13 July 2025: Clinical Research
Development and Validation of a Predictive Nomogram for Early Postoperative Recurrence in Non-Small Cell Lung Cancer
Zhi Liang ABCDEF 1, Wei Lin ABCD 1, Shipeng Fang BCDF 1, Jianhao Zhang BCDF 1, Jianhui Chen BCDF 1, Feng Yuan A 2*
DOI: 10.12659/MSM.948441
Med Sci Monit 2025; 31:e948441






Abstract
BACKGROUND: Early postoperative recurrence in non-small cell lung cancer (NSCLC) significantly impacts survival outcomes, yet current staging systems often fail to accurately predict recurrence risk. In this study, we analyzed the risk factors associated with early postoperative recurrence in NSCLC and developed a nomogram model to enhance individualized risk assessment.
MATERIAL AND METHODS: A retrospective analysis was conducted on data from 286 NSCLC patients who underwent R0 resection between January 2020 and December 2022, categorized into a control group (n=235) and an observation group (n=51). Demographic and clinicopathological data were collected, and multivariate logistic regression was used to identify independent risk factors. A nomogram was developed and validated using internal resampling. Discriminatory ability was assessed using the area under the receiver operating characteristic curve (AUC), and calibration performance was evaluated using the Hosmer-Lemeshow test and calibration curves.
RESULTS: Multivariate analysis identified elevated D-dimer levels (≥0.5 mg/L), pleural invasion, lymphovascular invasion, and lymph node metastasis as independent predictors of early recurrence. The nomogram achieved an AUC of 0.806, with a sensitivity of 78.9% and specificity of 80.1%. Internal validation yielded a corrected C-index of 0.689. Calibration curves demonstrated good agreement between predicted and observed recurrence probabilities. Decision curve analysis showed the model provided a higher net benefit compared to extreme intervention strategies.
CONCLUSIONS: Elevated D-dimer levels, pleural invasion, lymphovascular invasion, and lymph node metastasis were key risk factors predicting early postoperative recurrence in NSCLC. The nomogram demonstrated strong predictive accuracy and calibration, offering a useful tool for individualized risk assessment.
Keywords: Carcinoma, Non-Small-Cell Lung, Cerebral Small Vessel Diseases, lung neoplasms, Recurrence, Risk Factors, Humans, nomograms, Male, Female, Middle Aged, Retrospective Studies, Neoplasm Recurrence, Local, Aged, ROC Curve, Risk Assessment, Lymphatic Metastasis, Postoperative Period, adult
Introduction
Non-small cell lung cancer (NSCLC) constitutes approximately 85% of all lung cancer cases and remains a leading cause of cancer-related mortality worldwide [1]. Despite advances in diagnostic imaging, surgical techniques, and adjuvant therapies, early postoperative recurrence remains a significant clinical challenge, particularly in patients undergoing curative resection [2]. Early recurrence not only adversely impacts survival outcomes but also complicates the therapeutic landscape by limiting available treatment options [3]. Identifying high-risk patients and appropriately stratifying them is crucial for improving personalized treatment strategies and optimizing postoperative management [4].
Recurrence in NSCLC is influenced by a complex interplay of factors, including tumor biology, patient characteristics, and treatment-related variables [5,6]. Established risk factors include advanced pathological stage, lymphovascular invasion, poor tumor differentiation, and specific molecular markers, such as epidermal growth factor receptor (EGFR) mutations and anaplastic lymphoma kinase (ALK) rearrangements [7]. However, these markers alone are insufficient to accurately predict recurrence, particularly within the early postoperative period, defined as within 1 year after surgery [8,9]. The development of reliable quantitative tools to integrate these diverse factors is crucial for improving risk assessment. Nomogram models have emerged as valuable predictive tools in oncology, offering individualized risk predictions by incorporating multiple clinical and pathological variables. These models are particularly advantageous in providing graphical representations of complex multivariable equations, enabling clinicians to make data-driven decisions. In NSCLC, nomograms have been used to predict overall survival, recurrence-free survival, and distant metastasis risk [10]. However, many existing models are based on long-term outcomes or heterogeneous populations and may lack the sensitivity to detect early postoperative recurrence [11,12]. This gap highlights the need for a robust, validated nomogram model specifically tailored to early recurrence risk in NSCLC patients.
This study analyzed the key risk factors associated with early postoperative recurrence in NSCLC and evaluated the predictive performance of a newly developed nomogram model. The findings of this study could offer significant insights into the etiology of early recurrence, inform postoperative surveillance protocols, and pave the way for more personalized therapeutic interventions.
Material and Methods
STUDY DESIGN:
A retrospective study was conducted at our hospital from January 2020 to December 2022 to evaluate the risk factors and predictive value of a nomogram model for early postoperative recurrence in NSCLC. This study adhered to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines [13]. Patients were included if they were diagnosed with primary NSCLC confirmed by histopathology, underwent R0 resection with standard lymph node dissection, had preoperative imaging ruling out distant metastasis, and possessed comprehensive clinical and pathological data with complete postoperative follow-up information. Patients were excluded if they had histological subtypes other than adenocarcinoma or squamous cell carcinoma (as these are the most common NSCLC subtypes; excluding rarer subtypes reduces heterogeneity and ensures comparability among cases), received neoadjuvant radiotherapy, chemotherapy, or immune checkpoint inhibitors such as PD-1 or PD-L1 inhibitors before surgery, were diagnosed with other systemic malignancies or severe organ dysfunction (eg, cardiac, hepatic, or renal insufficiency), or had unconfirmed recurrence or follow-up durations of less than 1 month. A total of 286 patients met these criteria and were enrolled, with 235 patients categorized as the control group (no early recurrence) and 51 patients as the observation group (early postoperative recurrence). Informed consent was obtained from all subjects and/or their legal guardian(s). The study was reviewed and approved by the Ethics Committee of the First People’s Hospital of Linping District (2024 No. 010). All procedures adhered to relevant guidelines and regulations, in line with the Declaration of Helsinki. Data were handled confidentially, with personal identifiers removed to protect participant privacy.
COLLECTION AND CLASSIFICATION OF DEMOGRAPHIC AND CLINICOPATHOLOGICAL DATA:
Demographic and clinicopathological data were collected for all patients, including age, sex, smoking history, histological subtype, tumor differentiation grade, pathological TNM (pTNM) stage, pleural invasion, lymphovascular invasion, use of adjuvant chemotherapy, preoperative serum carcinoembryonic antigen (CEA), serum albumin, hemoglobin, and plasma D-dimer levels. Histological classification and differentiation grade were determined according to the 2015 World Health Organization (WHO) Classification of Tumors of the Lung [14]. Staging was performed using the 8th edition of the American Joint Committee on Cancer (AJCC) TNM staging system [15]. Lymphovascular invasion was assessed by D2–40 immunohistochemical staining for lymphatic vessels and Van Gieson’s staining for vascular elastic fibers [16]. Serum albumin levels <35 g/L were classified as hypoalbuminemia. Anemia was diagnosed based on hemoglobin levels, with thresholds defined as <120 g/L for adult males and <110 g/L for adult non-pregnant females, in accordance with the diagnostic criteria established for sea-level populations in China.
FOLLOW-UP PROTOCOL AND DEFINITION OF RECURRENCE:
All patients were followed up every 3 months during the first 2 years after surgery and every 6 months thereafter, for a total of 5 years. Follow-up evaluations included physical examinations, serum tumor marker assessments, chest and abdominal computed tomography (CT) scans, and whole-body bone scintigraphy or emission computed tomography (ECT), as necessary [17]. Early postoperative recurrence was defined as the occurrence of either local recurrence or distant metastasis within 2 years after surgery. Local recurrence was confirmed by imaging or pathological evidence of tumor regrowth at the ipsilateral bronchial stump or regional lymph nodes, including subdiaphragmatic, paraesophageal, supraclavicular, or hilar lymph nodes [18]. Distant metastasis was identified through imaging or pathological findings of tumor spread to the contralateral lung, bones, brain, liver, adrenal glands, or other distant organs. If both local recurrence and distant metastasis occurred, the event was classified as distant metastasis unless local recurrence preceded it [19]. Radiological criteria for diagnosing tumor recurrence or metastasis included chest CT or positron emission tomography-computed tomography (PET-CT) findings. Pathology confirmation was based on bronchoscopic examination and biopsy. Recurrence-free survival (RFS) was defined as the duration from surgery to the first documented tumor recurrence or metastasis, confirmed by imaging or pathological examination, and was used as the primary endpoint for survival analysis.
STATISTICAL ANALYSIS:
Statistical analyses were performed using SPSS version 27.0 and R version 4.3.3. Quantitative data are presented as mean±standard deviation (χ̄±s) and were compared between groups using independent-sample
Results
DEMOGRAPHIC AND CLINICAL CHARACTERISTICS OF PATIENTS:
The demographic and clinical characteristics of patients without early postoperative recurrence (control group, n=235) and those with early recurrence (observation group, n=51) were compared. No statistically significant differences were observed between the 2 groups regarding age, sex, smoking history, or histological type (P>0.05). Similarly, the use of adjuvant chemotherapy, hypoalbuminemia, and anemia showed no significant differences between the 2 groups (P>0.05). In contrast, significant differences were identified in key clinical characteristics associated with early recurrence. The observation group had a markedly higher prevalence of pleural invasion (49.0% vs 21.3%, P<0.001) and lymphovascular invasion (41.2% vs 26.0%, P=0.029) compared to the control group. Tumor differentiation also differed significantly, with poorly differentiated tumors being more frequent in the observation group (39.2% vs 23.0%, P=0.016). Patients with early recurrence were more likely to have advanced T stage (T2/T3: 51.0% vs 30.6%, P=0.006) and lymph node metastasis (56.9% vs 17.0%, P<0.001). Biomarkers were also significantly associated with recurrence: elevated D-dimer levels (≥0.5 mg/L) and elevated CEA levels (≥5.0 ng/mL) were observed more frequently in the observation group compared to the control group (D-dimer: 35.3% vs 17.4%, P=0.004; CEA: 37.3% vs 18.7%, P=0.004). These results suggest that pleural invasion, lymphovascular invasion, advanced T stage, lymph node metastasis, poor tumor differentiation, and elevated levels of D-dimer and CEA are significantly associated with early postoperative recurrence in non-small cell lung cancer (Table 1).
MULTIVARIATE LOGISTIC REGRESSION ANALYSIS OF FACTORS ASSOCIATED WITH EARLY POSTOPERATIVE RECURRENCE:
Multivariate logistic regression analysis identified several factors significantly associated with early postoperative recurrence in patients with non-small cell lung cancer. Among these, elevated D-dimer levels (≥0.5 mg/L) were found to be the strongest independent predictor of recurrence, with an OR of 3.718 (95% CI: 1.306–4.520, P=0.006). Similarly, pleural invasion demonstrated a significant association with recurrence, showing an OR of 2.642 (95% CI: 1.105–3.905, P=0.036). Lymphovascular invasion was another critical factor, with an OR of 3.194 (95% CI: 1.117–4.251, P=0.015), indicating its strong predictive value. Additionally, lymph node metastasis was significantly associated with early recurrence, with an OR of 2.088 (95% CI: 1.360–2.988, P=0.028). Conversely, T stage (T2/T3), low tumor differentiation, and elevated CEA levels (≥5.0 ng/mL) were not identified as statistically significant predictors in the multivariate analysis (P>0.05). Although elevated CEA levels approached statistical significance (P=0.061), their predictive value remained inconclusive in this model. These findings show that elevated D-dimer levels, pleural invasion, lymphovascular invasion, and lymph node metastasis are independent risk factors for early postoperative recurrence (Table 2).
DEVELOPMENT OF A NOMOGRAM PREDICTION MODEL FOR EARLY POSTOPERATIVE RECURRENCE IN NSCLC:
Based on the significant factors identified through multivariate logistic regression analysis, a nomogram prediction model was developed to estimate the probability of early postoperative recurrence in patients with NSCLC. The model incorporated 4 key predictors: elevated D-dimer levels, pleural invasion, lymphovascular invasion, and lymph node metastasis. Each variable was assigned a corresponding score, which, when summed, provided a total score for the patient. The total score was then mapped to a probability scale at the bottom of the nomogram, indicating the likelihood of early recurrence. Higher total scores were associated with an increased risk of early postoperative recurrence. This graphical representation allowed for individualized risk assessment, facilitating clinical decision-making regarding postoperative surveillance and management strategies (Figure 1).
DISCRIMINATION OF THE NOMOGRAM PREDICTION MODEL:
The nomogram prediction model for early postoperative recurrence in NSCLC demonstrated strong discriminatory ability, with an AUC of 0.806 (95% CI: 0.719–0.858). When the optimal cutoff was determined using the maximum Youden index, the model achieved a sensitivity of 78.9% and a specificity of 80.1%. These results indicate the model’s effectiveness in distinguishing between patients at high and low risk for early recurrence. Internal validation using the bootstrap resampling method, repeated 1000 times, yielded a corrected C-index of 0.689. The calibration curve revealed good agreement between predicted and observed recurrence probabilities, with an average absolute error of 0.011. This suggests that the model’s predictions closely approximate actual risks, highlighting its reliability and accuracy (Figure 2).
CALIBRATION OF THE NOMOGRAM PREDICTION MODEL:
The calibration of the nomogram prediction model for early postoperative recurrence in NSCLC was assessed using the Hosmer-Lemeshow goodness-of-fit test, which yielded a χ2 value of 2.869 and a P value of 0.915. These results indicate that the model demonstrates good calibration, with no significant difference between predicted and observed probabilities. The calibration curve further supported these findings, showing that the predicted probabilities closely aligned with the actual probabilities. The high degree of consistency suggests that the model provides reliable predictions for early postoperative recurrence (Figure 3).
CLINICAL UTILITY OF THE NOMOGRAM PREDICTION MODEL:
The clinical validity of the nomogram prediction model was evaluated using DCA. In the DCA, the horizontal line represented the assumption that no patients experienced early postoperative recurrence and thus received no intervention, with a net benefit of 0. The diagonal line reflected the assumption that all patients experienced early recurrence and underwent intervention, resulting in a negative net benefit with a slope corresponding to the intervention costs. The nomogram prediction model demonstrated a net benefit that was significantly higher than both extreme scenarios across a range of threshold probabilities. This indicates that the model effectively identifies patients at risk of early recurrence, guiding targeted interventions that provide greater clinical value (Figure 4).
POST HOC STATISTICAL POWER ANALYSIS FOR KEY PREDICTORS:
A post hoc power analysis was performed based on the observed sample size (n=286, with 51 patients experiencing early recurrence). Using an approximate weighted method, the overall statistical power of the study to detect associations between early postoperative recurrence and key risk factors (specifically D-dimer, pleural invasion, lymphovascular invasion, and lymph node metastasis) was estimated to be approximately 80%, assuming a significance level of 0.05 and moderate effect sizes. This suggests that the sample size was adequate to support the primary analyses.
Discussion
Non-small cell lung cancer (NSCLC) accounts for approximately 85% of all lung cancer cases globally [20,21]. Despite advances in surgery and adjuvant therapies, early postoperative recurrence remains a major challenge, underscoring the need for more accurate risk assessment tools, such as nomograms, to improve patient outcomes [22,23]. This study presents a novel nomogram-based prediction model for early postoperative recurrence in non-small cell lung cancer (NSCLC), integrating key clinical and pathological factors such as D-dimer levels, pleural invasion, lymphovascular invasion, and lymph node metastasis. Unlike traditional staging systems (eg, TNM), which often fail to fully capture the nuanced interactions between these risk factors, our model offers a personalized risk assessment that can more accurately predict early recurrence within the critical first 2 years after surgery. The study’s clinical value lies in its ability to stratify patients based on individual recurrence risk, providing clinicians with a valuable tool to inform postoperative management decisions. By accurately identifying high-risk patients, this model can guide targeted surveillance and early interventions, ultimately improving outcomes and reducing unnecessary treatments for low-risk patients. The validation of this nomogram, including high discriminatory ability (AUC = 0.806) and good calibration, further establishes its clinical robustness, ensuring reliable performance in diverse clinical settings. In addition, the model’s inclusion of D-dimer as a predictive biomarker highlights the growing importance of serum markers in the context of NSCLC recurrence, offering a non-invasive means of risk assessment that could complement existing diagnostic methods.
The identification of pleural invasion, lymphovascular invasion, elevated D-dimer levels, and lymph node metastasis as independent risk factors highlights the multifaceted nature of early recurrence in NSCLC. Pleural invasion reflects the tumor’s ability to breach anatomical barriers, facilitating both local and distant dissemination. Tumor cells invading the pleural cavity can spread via pleural effusion, thereby increasing the likelihood of recurrence. This finding emphasizes the need for aggressive surgical techniques to achieve complete resection and a thorough evaluation of pleural involvement during surgery. Lymphovascular invasion emerged as another critical predictor, signifying the entry of tumor cells into the vascular and lymphatic systems, which serve as gateways for hematogenous and lymphatic metastasis. The presence of tumor emboli within vessels likely contributes to the risk of micrometastases and subsequent recurrence [24,25]. The strong association between lymphovascular invasion and early recurrence underscores the importance of precise pathological evaluation and the potential use of adjuvant therapies targeting micrometastases. Elevated D-dimer levels were identified as the strongest independent predictor of early recurrence. D-dimer, a marker of fibrinolysis and systemic hypercoagulability, is often upregulated in cancer, as tumor cells activate coagulation pathways, forming microthrombi that facilitate vascular invasion and create a pro-tumorigenic microenvironment. Elevated D-dimer levels may thus reflect an aggressive tumor phenotype with enhanced metastatic potential. The significant role of lymph node metastasis aligns with the traditional understanding of NSCLC progression. Metastasis to regional lymph nodes indicates advanced disease and a higher likelihood of residual micro-metastatic disease after surgery [26,27]. This emphasizes the importance of comprehensive lymph node dissection and accurate staging in NSCLC patients.
The nomogram developed in this study demonstrated robust predictive performance, with an AUC of 0.806, indicating high discriminatory ability. This model enables clinicians to integrate multiple variables into a single risk score, facilitating individualized risk stratification. The strong calibration of the model, as confirmed by the Hosmer-Lemeshow test and calibration curve, suggests that the predicted probabilities closely align with actual outcomes. Such reliability is essential for clinical application, particularly in guiding postoperative surveillance and therapeutic decisions. The decision curve analysis (DCA) further validated the clinical utility of the nomogram, showing a higher net benefit across a range of threshold probabilities compared to extreme scenarios where all or no patients were treated. This underscores the model’s practical value in identifying high-risk patients who may benefit from targeted interventions while avoiding unnecessary treatments for low-risk patients. Although elevated CEA levels approached statistical significance (
T staging and tumor differentiation are generally considered important prognostic factors, particularly for predicting overall survival and recurrence risk in early-stage NSCLC [28]. However, there are exceptions in certain study contexts, particularly when T staging and tumor differentiation may not remain significant in multivariate analysis. This is observed in studies focusing on early recurrence (rather than long-term survival, such as 5-year survival rates) [29], in populations undergoing R0 resection (with good local control where T stage has a lesser impact on early recurrence) [30], or in cases where smaller sample sizes or collinearity between variables (such as the strong correlation between T stage and N stage, or vascular invasion) diminish the independent predictive value of these factors [31]. Furthermore, when pathological differentiation is concentrated (eg, predominantly moderate or high differentiation), T stage and tumor differentiation may not exhibit as much variance, reducing their predictive impact [31]. Additionally, when stronger competing risk factors such as D-dimer, lymph node metastasis, or vascular invasion are incorporated into the model, their effects may overshadow those of T stage and tumor differentiation [32]. In our study, the reasons for the lack of significance of T stage and tumor differentiation in predicting early recurrence are likely related to 3 main factors. T stage and tumor differentiation may be closely correlated with stronger predictors such as lymph node metastasis, pleural invasion, and lymphovascular invasion. When these more robust predictors are included in the multivariate model, the independent effect of T stage and differentiation may be diminished. Our study specifically targeted early postoperative recurrence (within 2 years of surgery). The key factors associated with early recurrence may be those related to tumor invasion and metastasis, such as lymph node involvement and vascular invasion, which are more predictive of early recurrence than T stage or differentiation. In our cohort, the distribution of T stage and tumor differentiation may have been relatively homogeneous, limiting the variability needed to detect significant associations after adjusting for other clinical factors.
This study has certain limitations. The retrospective, single-center design may have introduced selection bias, and the model’s generalizability remains to be validated in prospective, multicenter cohorts. Additionally, molecular and genomic variables – such as EGFR, ALK, KRAS mutations, PD-L1 expression, and circulating tumor DNA – were not included, which may limit the model’s predictive granularity. Although the nomogram demonstrated robust predictive performance, potential overfitting and biases inherent in the retrospective dataset may limit its generalizability, which needs validation using external datasets and prospective studies in future research. In future research, we plan to incorporate clinical variables associated with treatment response to enable more precise risk stratification. We will also expand the sample size through multicenter collaborations and apply robust cross-validation and external validation techniques to minimize potential overfitting and enhance reliability. Despite the nomogram’s strong discriminatory ability, future research could explore the integration of machine learning models or artificial intelligence to enhance its performance in diverse clinical settings. Integration of molecular and immunogenomic biomarkers will further refine predictive performance. The nomogram could be instrumental in guiding personalized adjuvant therapy decisions by identifying patients at high risk for recurrence, and future iterations could integrate treatment responses and post-surgical therapeutic strategies to improve its clinical applicability. External validation in diverse regional populations is planned to assess generalizability and support clinical translation.
Conclusions
This study identified elevated D-dimer levels, pleural invasion, lymphovascular invasion, and lymph node metastasis as key risk factors for early postoperative recurrence in NSCLC. The nomogram prediction model demonstrated strong discriminatory and calibration performance, offering a valuable tool for individualized risk assessment. However, further validation with larger, multicenter datasets is needed to confirm its generalizability and clinical utility.
Availability of Data and Materials
The datasets used and/or analyzed during this study are available upon reasonable request from the corresponding author.
Figures
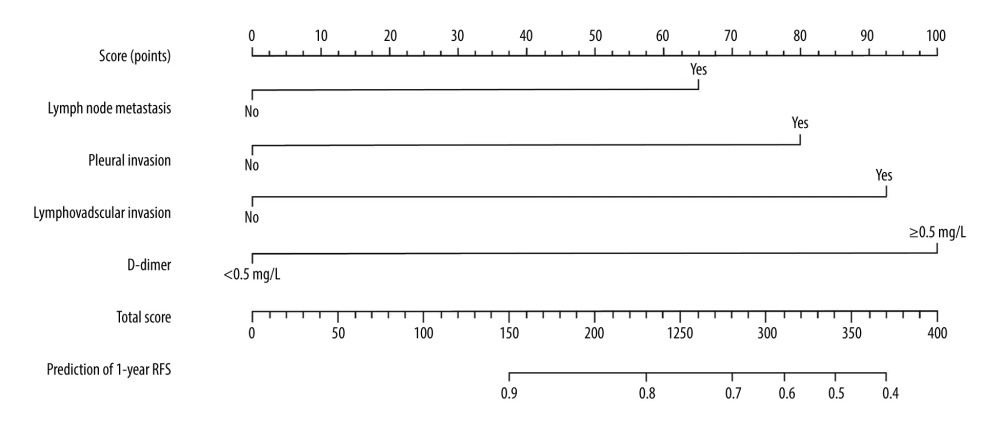 Figure 1. Nomogram prediction model for early postoperative recurrence in patients with NSCLC.
Figure 1. Nomogram prediction model for early postoperative recurrence in patients with NSCLC. 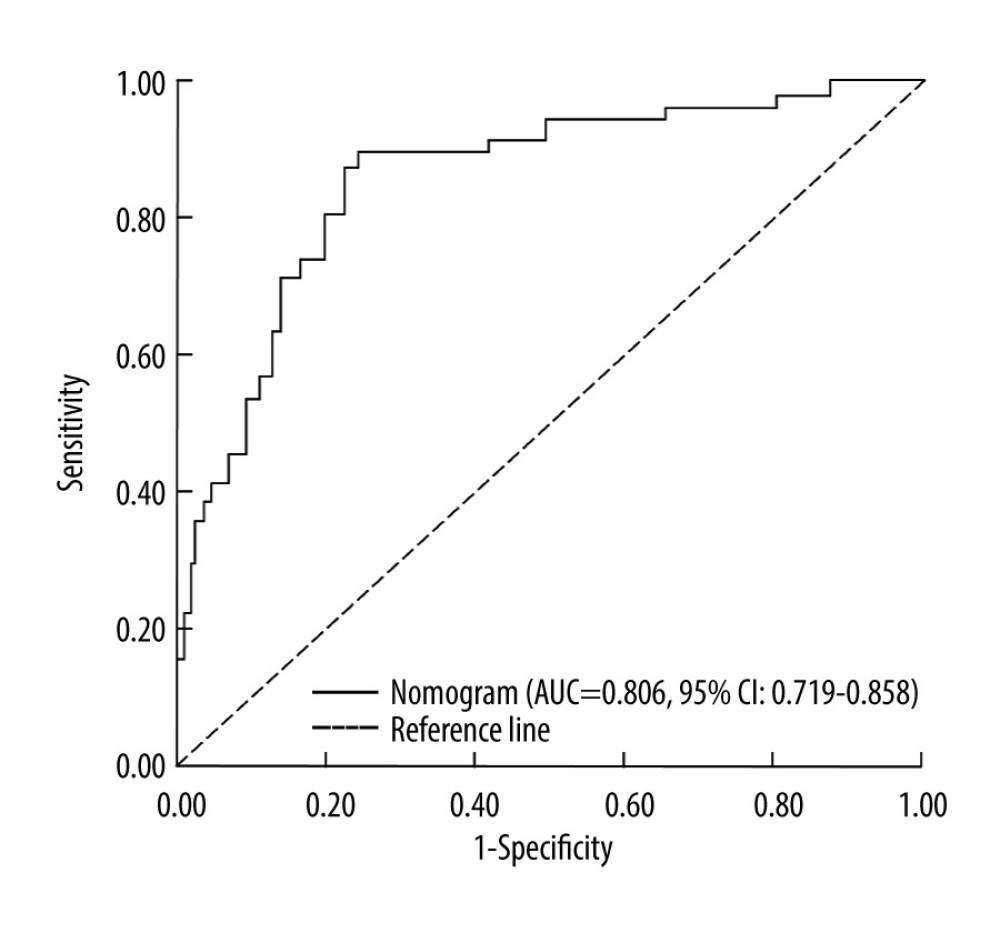 Figure 2. Receiver operating characteristic (ROC) curve illustrating the discriminatory ability of the nomogram prediction model for early postoperative recurrence in patients with NSCLC.
Figure 2. Receiver operating characteristic (ROC) curve illustrating the discriminatory ability of the nomogram prediction model for early postoperative recurrence in patients with NSCLC. 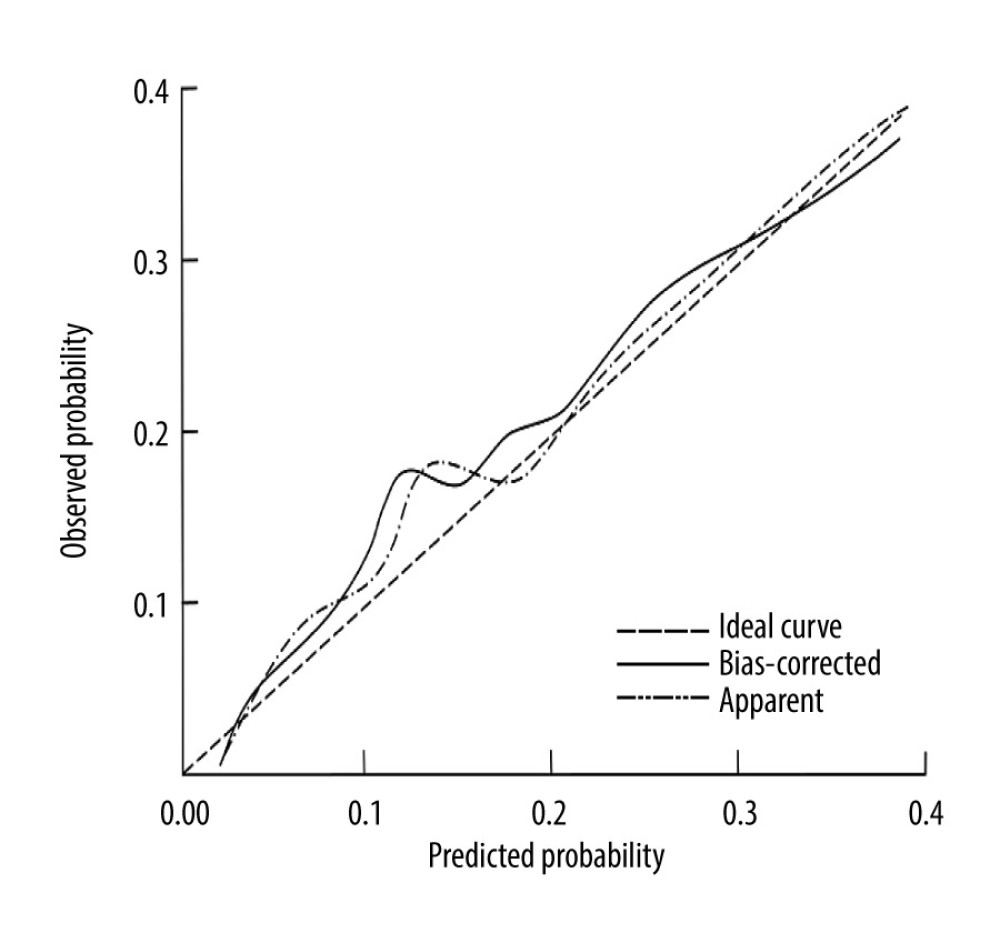 Figure 3. Calibration curve demonstrating the agreement between predicted and observed probabilities in the nomogram prediction model for early postoperative recurrence in patients with NSCLC.
Figure 3. Calibration curve demonstrating the agreement between predicted and observed probabilities in the nomogram prediction model for early postoperative recurrence in patients with NSCLC. 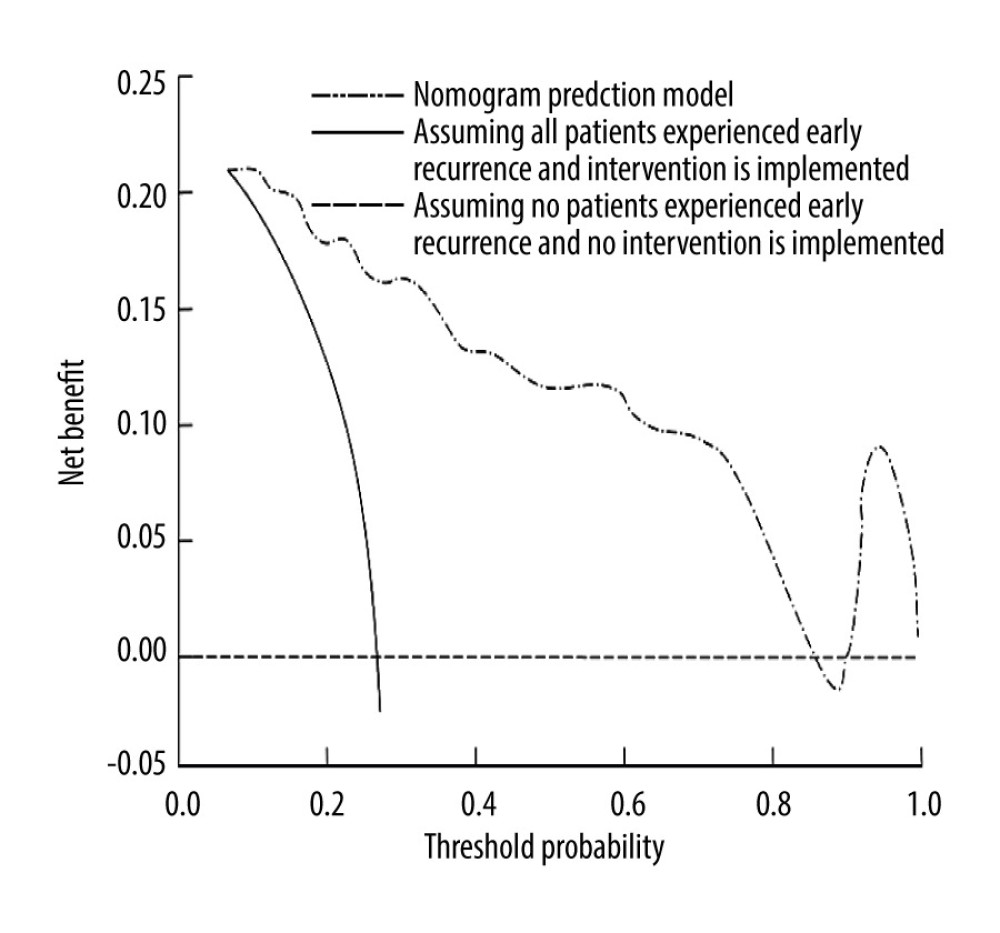 Figure 4. Decision curve analysis (DCA) evaluating the clinical utility of the nomogram prediction model for early postoperative recurrence in patients with NSCLC.
Figure 4. Decision curve analysis (DCA) evaluating the clinical utility of the nomogram prediction model for early postoperative recurrence in patients with NSCLC. References
1. Altorki N, Wang X, Kozono D, Lobar or sublobar resection for peripheral stage IA non-small-cell lung cancer: N Engl J Med, 2023; 388(6); 489-98
2. Ohtaki Y, Nagashima T, Okano N, Prognosis of non-small cell lung cancer with postoperative regional lymph node recurrence: Thorac Cancer, 2024; 15(11); 859-66
3. Hashimoto K, Ariyasu R, Ichinose J, Advances in the treatment of postoperative recurrence of non-small cell lung cancer and their impact on survival in Asian patients: J Thorac Cardiovasc Surg, 2023; 165(4); 1565-74.e1
4. Gutierrez-Sainz L, Cruz-Castellanos P, Higuera O, de Castro-Carpeño J, Neoadjuvant chemoimmunotherapy in patients with resectable non-small cell lung cancer: Curr Treat Options Oncol, 2021; 22(10); 91
5. Cai S, Yang G, Hu M, Spatial cell interplay networks of regulatory T cells predict recurrence in patients with operable non-small cell lung cancer: Cancer Immunol Immunother, 2024; 73(10); 189
6. Patnaik SK, Cortes EG, Kannisto ED, Lower airway bacterial microbiome may influence recurrence after resection of early-stage non-small cell lung cancer: J Thorac Cardiovasc Surg, 2021; 161(2); 419-29.e16
7. Wang C, Li J, Chen J, Multi-omics analyses reveal biological and clinical insights in recurrent stage I non-small cell lung cancer: Nat Commun, 2025; 16(1); 1477
8. Choe J, Kim MY, Yun JK, Sublobar resection in stage IA non-small cell lung cancer: role of preoperative CT features in predicting pathologic lymphovascular invasion and postoperative recurrence: Am J Roentgenol, 2021; 217(4); 871-81
9. Hu D, Li S, Huang Z, Wu N, Lu X, Predicting postoperative non-small cell lung cancer prognosis via long short-term relational regularization: Artif Intell Med, 2020; 107; 101921
10. Zhang J, Fan J, Yin R, A nomogram to predict overall survival of patients with early stage non-small cell lung cancer: J Thorac Dis, 2019; 11(12); 5407-16
11. Sun J, Wu S, Jin Z, Lymph node micrometastasis in non-small cell lung cancer: Biomed Pharmacother, 2022; 149; 112817
12. Guo W, Zhang T, Li R, Molecular risk factors for locoregional recurrence in resected non-small cell lung cancer: Cancer Med, 2023; 12(14); 15026-36
13. von Elm E, Altman DG, Egger M, The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies: J Clin Epidemiol, 2008; 61(4); 344-49
14. Travis WD, Brambilla E, Nicholson AG, The 2015 World Health Organization Classification of lung tumors: Impact of genetic, clinical and radiologic advances since the 2004 classification: J Thorac Oncol, 2015; 10(9); 1243-60
15. Detterbeck FC, Boffa DJ, Kim AW, Tanoue LT, The eighth edition lung cancer stage classification: Chest, 2017; 151(1); 193-203
16. Min KH, Park SJ, Lee KS, Clinical usefulness of D2–40 in non-small cell lung cancer: Lung, 2011; 189(1); 57-63
17. Ettinger DS, Wood DE, Aisner DL, Non-small cell lung cancer, Version 3.2022, NCCN clinical practice guidelines in oncology: J Natl Compr Canc Netw, 2022; 20(5); 497-530
18. Lou F, Huang J, Sima CS, Patterns of recurrence and second primary lung cancer in early-stage lung cancer survivors followed with routine computed tomography surveillance: J Thorac Cardiovasc Surg, 2013; 145(1); 75-81 discussion 81–82
19. Jeong WG, Choi H, Chae KJ, Kim J, Prognosis and recurrence patterns in patients with early stage lung cancer: A multi-state model approach: Transl Lung Cancer Res, 2022; 11(7); 1279-91
20. Lee S, Roknuggaman M, Son JA, Prognostic impact of postoperative complications in high-risk operable non-small cell lung cancer: J Chest Surg, 2022; 55(1); 20-29
21. Kawaguchi Y, Hanaoka J, Ohshio Y, Sarcopenia increases the risk of post-operative recurrence in patients with non-small cell lung cancer: PLoS One, 2021; 16(9); e0257594
22. Ryu H, Song C, Kim JS, Role of prognostic nutritional index in postoperative radiotherapy for non-small cell lung cancer: Thorac Cancer, 2023; 14(28); 2859-68
23. Tamura M, Matsumoto I, Tanaka Y, Prognostic factor and treatment strategy for clinical N1 non-small cell lung cancer: Gen Thorac Cardiovasc Surg, 2020; 68(3); 261-65
24. Akcam TI, Tekneci AK, Ergin TM, Factors influencing postoperative recurrence of early-stage non-small cell lung cancer: Acta Chir Belg, 2024; 124(2); 121-30
25. Wu CF, Fu JY, Yeh CJ, Recurrence risk factors analysis for stage I non-small cell lung cancer: Medicine (Baltimore), 2015; 94(32); e1337
26. Borghetti P, Barbera F, Bonù ML, Resected pN1 non-small cell lung cancer: Recurrence patterns and nodal risk factors may suggest selection criteria for post-operative radiotherapy: Radiol Med, 2016; 121(9); 696-703
27. Zhu W, Li S, Ji X, Tan H, Impact of anesthetic factors on prognosis of patients with non-small cell lung cancer after surgery: J Thorac Dis, 2023; 15(9); 4869-84
28. Hung J-J, Jeng W-J, Hsu W-H, Predictors of death, local recurrence, and distant metastasis in completely resected pathological stage-I non-small-cell lung cancer: J Thorac Oncol, 2012; 7(7); 1115-23
29. Zhang Y, Gao J, Zheng A, Definition and risk factors of early recurrence based on affecting prognosis of esophageal squamous cell carcinoma patients after radical resection: Transl Oncol, 2021; 14(6); 101066
30. Chen C, Wang L, Zhang R, Who benefits from R0 resection? A single-center analysis of patients with stage IV gallbladder cancer: Chronic Dis Transl Med, 2019; 5(3); 188-96
31. Derwinger K, Kodeda K, Bexe-Lindskog E, Taflin H, Tumour differentiation grade is associated with TNM staging and the risk of node metastasis in colorectal cancer: Acta Oncol, 2010; 49(1); 57-62
32. Wu T, Fang L, Ruan Y, Tumor aggression-defense index – a novel indicator to predicts recurrence and survival in stage II–III colorectal cancer: J Transl Med, 2025; 23(1); 107
Figures
Figure 1. Nomogram prediction model for early postoperative recurrence in patients with NSCLC.Figure 2. Receiver operating characteristic (ROC) curve illustrating the discriminatory ability of the nomogram prediction model for early postoperative recurrence in patients with NSCLC.Figure 3. Calibration curve demonstrating the agreement between predicted and observed probabilities in the nomogram prediction model for early postoperative recurrence in patients with NSCLC.Figure 4. Decision curve analysis (DCA) evaluating the clinical utility of the nomogram prediction model for early postoperative recurrence in patients with NSCLC. Tables
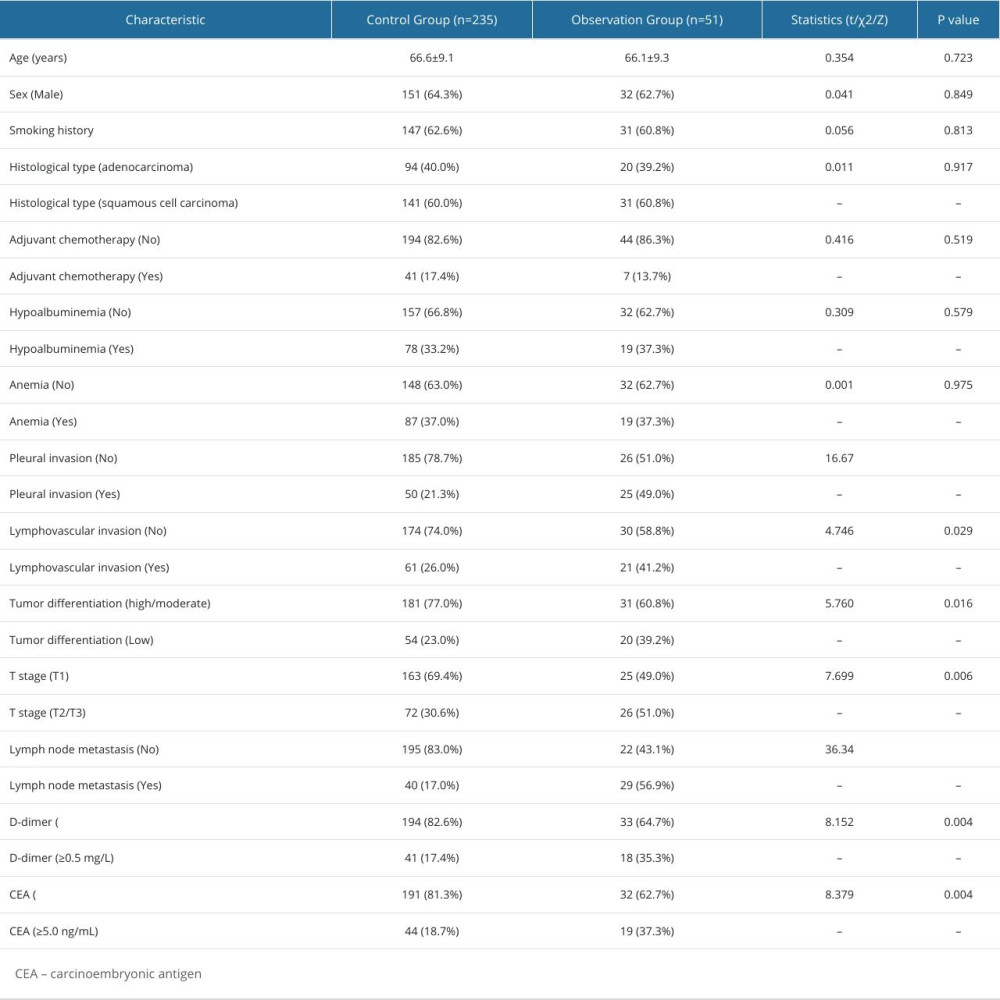 Table 1. Demographic and clinical characteristics of patients.
Table 1. Demographic and clinical characteristics of patients.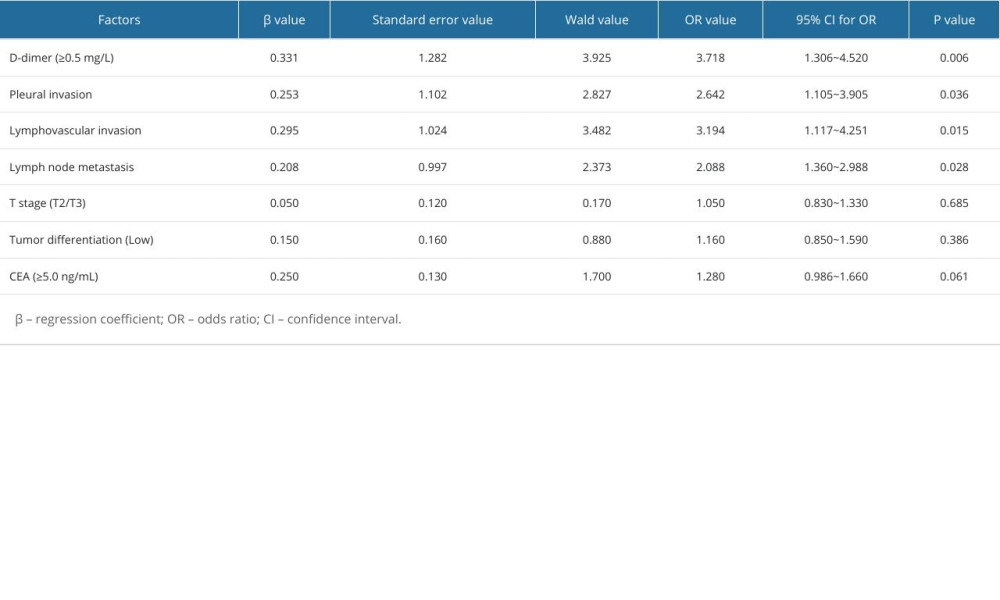 Table 2. Multivariate logistic regression analysis of factors associated with early postoperative recurrence.Table 1. Demographic and clinical characteristics of patients.Table 2. Multivariate logistic regression analysis of factors associated with early postoperative recurrence.
Table 2. Multivariate logistic regression analysis of factors associated with early postoperative recurrence.Table 1. Demographic and clinical characteristics of patients.Table 2. Multivariate logistic regression analysis of factors associated with early postoperative recurrence. In Press
Clinical Research
Association Between Total Cholesterol–to–High-Density Lipoprotein Ratio and Gestational Hypertension: A Cas...Med Sci Monit In Press; DOI: 10.12659/MSM.952395
Review article
Clinical Use of Endotracheal Intubation Without Neuromuscular Blockade: The Current Stage of KnowledgeMed Sci Monit In Press; DOI: 10.12659/MSM.951765
Clinical Research
Effect of Dexmedetomidine Hydrochloride Nasal Spray on Anxiety and Sleep in Patients Undergoing Gynecologic...Med Sci Monit In Press; DOI: 10.12659/MSM.952465
Clinical Research
Prognostic Value of Mortality Scoring Systems in Patients With Severe Burns: Identifying Key Predictors of ...Med Sci Monit In Press; DOI: 10.12659/MSM.951713
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,173
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,757,769
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,143
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,797
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387