19 January 2024: Clinical Research
The Impact of Type D Personality Traits on Quality of Life, Sleep, Anxiety, and Depression in Fibromyalgia Patients: A Comparative Study with Healthy Controls
İlknur TopalDOI: 10.12659/MSM.942606
Med Sci Monit 2024; 30:e942606






Abstract
BACKGROUND: Type D personality has been associated with adverse clinical outcomes and poor quality of life in many diseases. This study aimed to evaluate the effects of type D personality on pain, anxiety and depression, sleep quality, and quality of life in 50 patients with fibromyalgia syndrome.
MATERIAL AND METHODS: Fifty patients with fibromyalgia and 50 healthy controls were included in the study. Baseline and post-treatment evaluations encompassed a comprehensive battery of assessment tools: socio-demographic questionnaire, visual analog scale for pain, Beck Anxiety Inventory, Beck Depression Inventory, Fibromyalgia Impact Questionnaire, SF-36 Short Form Questionnaire, and Pittsburgh Sleep Quality Index. The effects of type D personality traits on clinical parameters were determined by evaluating the participants with the D-Type Personality Scale (DS-14).
RESULTS: Twelve participants (24%) in the control group and 30 patients (60%) in the fibromyalgia group had type D personality traits, and the difference was significant (P<0.001). The Beck Anxiety Inventory and Beck Depression Inventory scores were significantly higher, and the SF-36 domains of vitality and mental health were significantly lower in fibromyalgia patients with type D personality (P=0.023, P=0.036, P=0.002, P>0.001).
CONCLUSIONS: This study draws attention to the high prevalence of type D personality in patients with fibromyalgia and demonstrates that this personality trait has a negative impact on patients’ clinical parameters.
Keywords: Anxiety, Depression, fibromyalgia syndrome, sleep quality, Type D personality, Quality of Life
Background
Fibromyalgia syndrome is described as a persistent pain condition characterized by widespread bodily discomfort, fatigue, sleep disturbances, and various other symptoms [1]. Alongside these primary symptoms, individuals with fibromyalgia can also experience issues such as dizziness, mood disorders, cognitive impairment, anxiety, depression, tingling sensations, abdominal bloating, and shortness of breath [1]. The etiology of fibromyalgia is thought to involve central sensitization, which entails dysfunction within the locomotor system, affecting the perception, transmission, and processing of incoming pain signals [2]. Recent research has linked fibromyalgia to a range of other factors, including inflammatory, immune, endocrine, genetic, and psychosocial elements [2]. Pain, the primary symptom in fibromyalgia, falls under the category of nociplastic pain, which refers to pain arising from altered nociception without any damage to tissues or the somatosensory system, causing activation of peripheral nociceptors [3]. Fibromyalgia is more prevalent in women than men, and community incidence rates are reported between 7.3% and 12.9% [1].
The diagnosis of fibromyalgia has undergone changes over time. Initially, the American College of Rheumatology established diagnostic criteria that necessitated the presence of tender points. However, more recent research, as indicated by Wolfe et al [4], has demonstrated that a tender point examination is no longer a prerequisite for diagnosis. The 3 fibromyalgia criteria recommended by the American College of Rheumatology in 2010/2011 are as follows [5]: (1) Pain severity: The patient rates their pain on a scale from 0 to 10, reflecting the severity of their pain experienced in the past 7 days, allowing an assessment of pain intensity. (2) Generalized pain: The patient reports pain felt in at least 1 area of the body for a minimum of 1 month, involving the right and left sides, upper and lower halves, and front and back of the body. (3) Symptom severity: The patient assesses the severity of symptoms such as headaches, fatigue, cognitive difficulties, sleep disturbances, gastrointestinal issues, and depression experienced in the past 7 days on a scale from 0 to 3. A fibromyalgia diagnosis is based on the total of scores of generalized pain, symptom severity, and pain severity. If these criteria surpass a specific threshold, a diagnosis of fibromyalgia is made.
The National Institute for Health and Care Excellence has outlined general principles for the clinical management of fibromyalgia in its 2021 guidelines [6]. The primary objective of treating fibromyalgia is to alleviate symptoms and enhance the quality of life for affected individuals. Non-pharmacological interventions, including exercise, cognitive-behavioral therapy, and patient education, have demonstrated effectiveness in symptom management, as supported by Adams et al [7], Arnold et al [8], and the National Institute for Health and Care Excellence. In addition to non-pharmacological approaches, pharmacological treatments involving medications such as antidepressants, anticonvulsants, and analgesics have also been considered [6,8]. A comprehensive approach to the recovery of individuals with fibromyalgia encompasses 4 fundamental pillars: (1) patient education, (2) psychological therapy, (3) medication-based treatment, and (4) physical activity.
“Type D personality” (TDP) is derived from the initials of “distrustful” and “distressed”. TDP represents an individual’s internal state of being distrustful and distressed, with the individual frequently experiencing negative emotional responses [9]. TDP is defined as a personality disposition that predisposes individuals to chronic distress; it is characterized by the presence of negative affect and social inhibition [9]. Negative affect encompasses a susceptibility to experiencing negative emotions, such as anxiety, depression, dysphoria, and irritability, while social inhibition refers to the tendency to withhold the expression of emotions in social situations due to a fear of rejection [9,10]. Individuals exhibiting TDP tend to experience heightened levels of worry, nervousness, and self-blame. They also typically hold a pessimistic outlook on life, possess lower self-confidence, and report reduced overall life satisfaction [11,12]. Additionally, they often perceive social relationships negatively, have limited social support, and form weak connections with others [13]. TDP is associated with increased anxiety, depression, diminished quality of life, and a negative assessment of one’s own health [14]. Moreover, individuals with TDP traits are more susceptible to physical and mental health conditions [14]. Research suggests that TDP can elevate the risk of heart attacks and is more prevalent among individuals with heart disease, indicating a link between these personality traits and heart conditions [15]. Furthermore, patients with ankylosing spondylitis and TDP tend to experience more severe clinical symptoms [16].
The available body of literature concerning the influence of TDP on fibromyalgia is quite sparse. In the context of our research, we hypothesized that TDP could be linked to elevated levels of anxiety, depression, sleep disruptions, reduced quality of life, and heightened disease activity in individuals with fibromyalgia. Therefore, this study aimed to evaluate the effects of type D personality on pain, anxiety and depression, sleep quality, and quality of life in 50 patients with fibromyalgia syndrome. This way, early diagnosis of TDP in patients with fibromyalgia can facilitate interventions to improve patient well-being.
Material and Methods
SAMPLE:
We enrolled a total of 50 patients who sought treatment at our hospital’s physical therapy outpatient clinic. In our study, the diagnosis of fibromyalgia was made based on the updated American College of Rheumatology in 2010/2011 criteria, which require the presence of pain lasting for more than 3 months, a pain score of 17 or higher in at least 3 months of pain distribution, and a symptom impact score of 17 or higher [4]. Additionally, we recruited 50 healthy volunteers from the same age group to serve as a control group.
PARTICIPANT INCLUSION AND EXCLUSION CRITERIA:
Patients diagnosed with fibromyalgia according to the American College of Rheumatology 2010/2011 criteria and aged between 18 and 65 were included in our study. Those with inflammatory rheumatic disease, malignancy, and neurological disease were excluded. Healthy volunteers between the ages of 18 and 65 years were included in the control group.
INFORMED CONSENT:
Before being enrolled in the study, a comprehensive explanation of the research aims and procedures was given to all participants. Participation was contingent upon our obtaining written informed consent.
ETHICAL APPROVAL:
The study received approval from the Clinical Research Ethics Committee of the Faculty of Medicine at Medipol University (approval number: 10840098-6004.01.01-E.15458), ensuring compliance with ethical guidelines.
ASSESSMENT:
All study participants completed a comprehensive set of assessments, as follows:
The 14-item Type D Personality Scale (DS-14): We used the DS-14 scale to determine the presence of TDP traits [17]. This assessment comprises 2 sub-dimensions, which evaluate negative affect and social inhibition, for a total of 14 items. Each item is rated on a scale from 0 to 4, with some items requiring reverse scoring. Individuals who scored 10 or higher on both subdimensions were classified as demonstrating TDP characteristics.
Beck Anxiety Inventory: This assessment tool was employed to gauge the severity of anxiety [18]. It consists of a total of 21 questions, each scored between 0 and 3. The maximum achievable score on this scale is 63, with higher scores indicative of a greater degree of anxiety.
Beck Depression Inventory: This scale was used to assess the severity of depressive symptoms [19]. It comprises 21 questions, each scored between 0 and 3, with a maximum total score of 63. Elevated scores on this scale denote a higher level of depression.
Fibromyalgia Impact Questionnaire: This questionnaire was used to evaluate the impact of fibromyalgia on patients’ well-being and current status [20]. It encompasses 10 factors, including physical function, overall well-being, work-related issues, fatigue, morning fatigue, stiffness, anxiety, and depression. The first section has 10 items scored on a Likert scale from 0 to 3. In the second and third sections, participants were asked to indicate the frequency of “being affected by the disease” and “inability to attend work” on specified days, and scores were calculated accordingly. The remaining 7 questions involved marking the appropriate position on a visual analog scale. Higher scores on the scale indicate a greater level of impairment, with a maximum possible score of 100.
Visual Analogue Scale: This 10-point scale was used to assess pain levels, ranging from 0 (no pain) to 10 (unbearable pain). Pain severity was categorized [21] as mild (1–3), moderate (4–7), or severe (8–10).
SF-36 Short Form Questionnaire: We used the SF-36 as a tool to assess the well-being and quality of life of our research participants. This survey comprises 36 questions designed to measure 8 dimensions related to physical and mental health. These dimensions encompass physical function, role physical, role emotional, vitality, mental health, social function, body pain, and general health. Scores on these subscales can range from 0 to 100, with higher scores indicating a more positive quality of life [22].
STATISTICAL ANALYSIS:
Quantitative variables were described using measures of central tendency and variance, with mean±SD. The Fisher’s exact test (in cases of low sample size) and chi-squared test were used to determine differences between proportions or associations among categorical variables. To demonstrate differences in behavioral patterns of group means, the Mann-Whitney U test was used when the normality and homoscedasticity assumptions were not met. The Mann Whitney U test was also used to compare the distribution between specific categorical groups related to numerical values of the parameters. The chi-squared test or Fisher’s Exact test were used to assess the relationship between categorical variables. The G*Power program [23] was used to calculate the sample size. Significant high or low values at the 0.05 level were indicated based on ratios obtained when a similar independent relationship between groups was assumed. Statistical significance was set at P=0.05 for all cases. Statistical analyses were performed using the IBM SPSS (Statistical Package for the Social Sciences, Version 21.0, IBM Corp Armonk, NY, USA) software package for Windows.
Results
PARTICIPANT CHARACTERISTICS:
In this study, we investigated 50 patients with a diagnosis of fibromyalgia based on American College of Rheumatology criteria (FM group), alongside a matched control group of 50 healthy individuals. The FM group had an average disease duration of 40.2±42.6 months, a Fibromyalgia Impact Questionnaire score of 69.6±16.3, and a visual analog scale pain score of 7±1.8. Demographically, there were no statistically significant differences between the FM and control groups (Table 1).
TYPE D PERSONALITY PREVALENCE:
TDP traits were significantly more prevalent in the FM group, with 60% (n=30) of patients exhibiting these traits, compared with 24% (n=12) of participants in the control group (P<0.001**). Furthermore, scores in the FM group were significantly higher on the Pittsburgh Sleep Quality Index, Beck Anxiety Inventory, and Beck Depression Inventory than in the control group (P<0.001, P<0.001, P=0.001, respectively; Table 2).
QUALITY OF LIFE ASSESSMENT:
The FM group consistently reported lower scores across all dimensions of the SF-36 quality of life questionnaire than did the control group, as shown in Table 2.
IMPACT OF TYPE D PERSONALITY:
Analyzing sleep, depression, and quality of life in all participants, regardless of TDP status, revealed no statistically significant differences in sleep quality (P=0.086). However, individuals with TDP showed higher Beck Anxiety Inventory and Beck Depression Inventory scores (P=0.003, P=0.002, respectively) and lower scores in various SF-36 quality of life sub-domains, including physical function, vitality, mental health, social function, and general health, as detailed in Table 3.
In the FM group, there were no significant distinctions in sleep quality between patients with and without TDP. However, among patients in the FM group with TDP, Beck Anxiety Inventory and Beck Depression Inventory scores were significantly higher (P=0.02, P=0.036, respectively), and the quality of life was notably lower in the mental health and vitality domains of the SF-36, as detailed in Table 4.
Notably, among healthy individuals in the control group, regardless of TDP traits, no significant differences were found in sleep, depression, and quality of life levels (
Discussion
STUDY LIMITATIONS:
This study had several limitations. A relatively small sample size and a single-center setting may restrict generalizability. Furthermore, our cross-sectional study had some fundamental limitations. First, these types of studies cannot be used to establish causal relationships and rely solely on data from a specific point in time. Second, variability and memory errors can also limit data reliability. Lastly, observer effects and non-response issues can influence participant behavior and potentially lead to misleading outcomes. Therefore, these limitations should be considered when interpreting the results of this cross-sectional study.
Conclusions
This study has revealed a significant connection between TDP and the development of fibromyalgia. The study emphasizes that the FM group was more likely to exhibit TDP traits than was the control group. Additionally, fibromyalgia patients with TDP traits showed high levels of depression and anxiety, accompanied by a noticeable decline in overall quality of life. Recognizing TDP traits in patients with fibromyalgia and managing them through psychotherapeutic interventions can lead to the development of adaptive coping strategies. In light of the results obtained, expanding the sample size and conducting new studies can provide a clearer understanding of the relationship between fibromyalgia and TDP.
Tables
Table 1. Comparison of demographic data between groups. Table 2. Clinical comparison of fibromyalgia and control groups.
Table 2. Clinical comparison of fibromyalgia and control groups.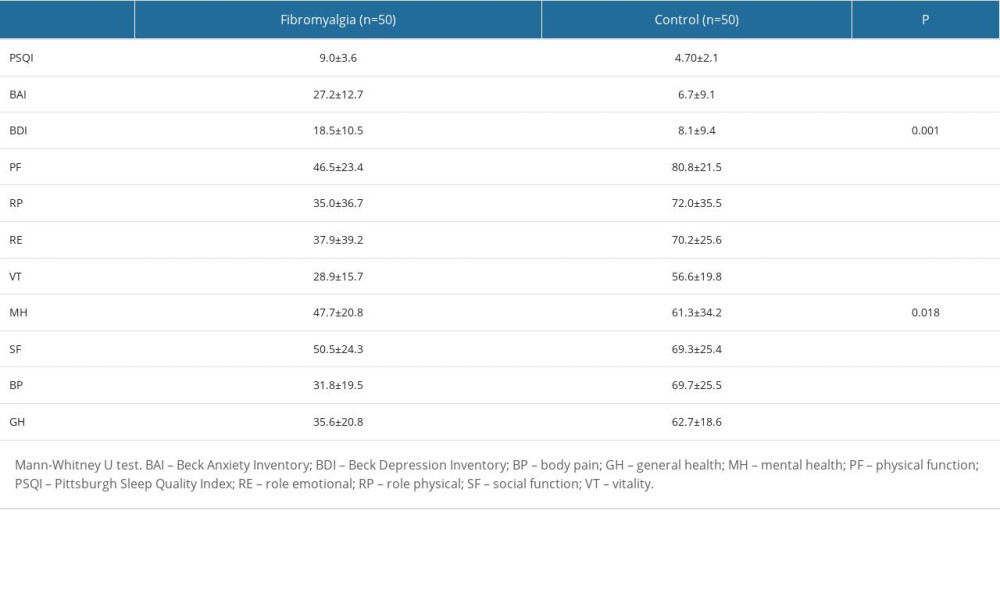 Table 3. Comparison of all participants in terms of sleep, depression, anxiety, and quality of life according to whether they have type D personality traits or not.
Table 3. Comparison of all participants in terms of sleep, depression, anxiety, and quality of life according to whether they have type D personality traits or not.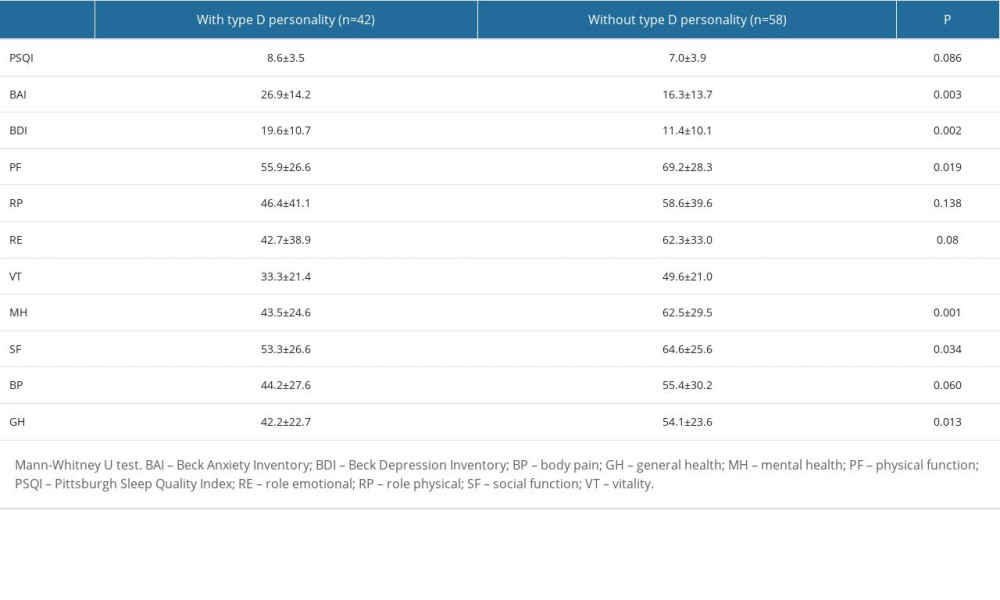 Table 4. Comparison of clinical parameters of fibromyalgia patients according to whether they have Type D personality or not.
Table 4. Comparison of clinical parameters of fibromyalgia patients according to whether they have Type D personality or not.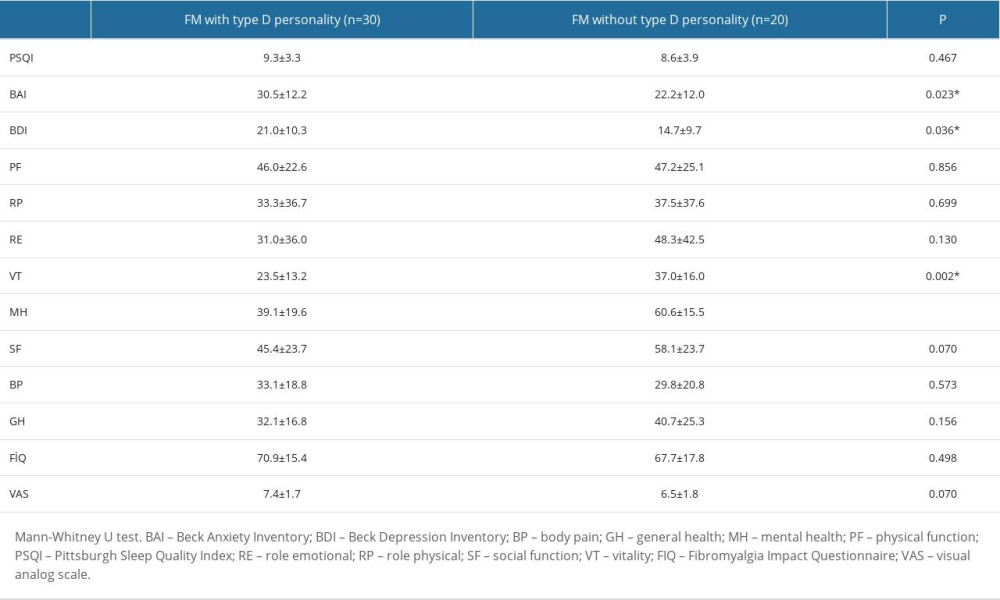
References
1. Neumann L, Buskila D, Epidemiology of fibromyalgia: Curr Pain Headache Rep, 2003; 7(5); 362-68
2. Meyer HP, Myofascial pain syndrome and its suggested role in the pathogenesis and treatment of fibromyalgia syndrome: Curr Pain Headache Rep, 2002; 6(4); 274-83
3. Wolfe F, Clauw DJ, Fitzcharles MA, The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity: Arthritis Care Res (Hoboken), 2010; 62(5); 600-10
4. Wolfe F, Clauw DJ, Fitzcharles MA, 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria: Semin Arthritis Rheum, 2016; 46(3); 319-29
5. : National Institute for Health and Care Excellence (NICE) Guideline NG193. Published 7 April 2021. Available from: https://www.nice.org.uk/guidance/ng193/resources/chronic-pain-primary-and-secondary-in-over-16s-assessment-of-all-chronic-pain-and-management-of-chronic-primary-pain-pdf-66142080468421
6. Adams N, McVeigh JG, Antonio Cuesta-Vargas A, Abokdeer S, Evidence-based approaches for the management of fibromyalgia syndrome: A scoping review: Phys Ther Rev, 2023; 28; 1-17
7. Arnold LM, Bennett RM, Crofford LJ, AAPT diagnostic criteria for fibromyalgia: J Pain, 2019; 20(6); 611-28
8. Denollet J, Type D personality. A potential risk factor refined: J Psychosom Res, 2000; 49; 255-66
9. Watson D, Pennebaker JW, Health complaints, stress and distress: Exploring the central role of negative affectivity: Psychol Rev, 1989; 96; 234-54
10. Mols F, Denollet J, Type D personality in the general population: A systematic review of health status, mechanisms of disease, and work-related problems: Health Qual Life Outcomes, 2010; 8; 9
11. Denollet J, Kupper N, Type D personality, depression and cardiac prognosis: Cortisol dysregulation as a mediating mechanism: J Psychosom Res, 2007; 62; 607-9
12. O’Riordan A, Howard S, Gallagher S, Type D personality and life event stress: The mediating effects of social support and negative social relationships: Anxiety Stress, 2020; 33; 452-65
13. Can İ, Tuman TC, The effect of type D personality on quality of life, sleep quality, anxiety and depression in patients with myofascial pain syndrome: Psychiatry and Behav Sci, 2020; 10(2); 90-95
14. Kupper N, Denollet J, Type D personality as a risk factor in coronary heart disease: A review of current evidence: Curr Cardiol Rep, 2018; 20(11); 104
15. Erkol İnal E, Demirci K, Doğru A, Şahin M, Ankylosing spondylitis patients with type D personality have worse clinical status: Mod Rheumatol, 2016; 26(1); 138-45
16. Denollet J, DS14: standard assessment of negative affectivity, social inhibition, and type D personality: Psychosom Med, 2005; 67(1); 89-97
17. Beck AT, Epstein N, Brown G, Steer RA, An inventory for measuring clinical anxiety: psychometric properties: J Consult Clin Psychol, 1988; 56(6); 893-97
18. Beck AT, Ward CH, Mendelson M, An inventory for measuring depression: Arch Gen Psychiatry, 1961; 4; 561-71
19. Sarmer S, Ergin S, Yavuzer G, The validity and reliability of the Turkish version of the Fibromyalgia Impact Questionnaire: Rheumatol Int, 2000; 20(1); 9-12
20. Huskisson EC, Visual analog scales: Pain, measurement and assessment, 1983, New York, Raven
21. Koçyiğit H, Aydemir Ö, Fişek G, Reliability and validity of the Turkish Version of Short Form-36 (SF-36) İlaç ve Tedavi Dergisi, 1999; 12; 102-6
22. Faul F, Erdfelder E, Lang AG, Buchner A, G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences: Behav Res Methods, 2007; 39(2); 175-91
23. Crofford LJ, Pillemer SR, Kalogeras KT, Hypothalamic-pituitary-adrenal axis perturbations in patients with fibromyalgia: Arthritis Rheum, 1994; 37(11); 1583-92
24. Kupper N, Gidron Y, Winter J, Denollet J, Association between type D personality, depression, and oxidative stress in patients with chronic heart failure: Psychosom Med, 2009; 71(9); 973-80
25. Conti C, Carrozzino D, Patierno C, The clinical link between type D personality and diabetes: Front Psychiatry, 2016; 7; 113
26. Ye Q, Liu L, Wang Y, Association of type D personality and mild cognitive impairment in patients with hypertension: Front Psychol, 2022; 13; 974430
27. Molina-Leyva A, Caparros-delMoral I, Ruiz-Carrascosa JC, Elevated prevalence of Type D (distressed) personality in moderate to severe psoriasis is associated with mood status and quality of life impairment: A comparative pilot study: J Eur Acad Dermatol Venereol, 2015; 29(9); 1710-17
28. Dubayova T, Krokavcova M, Nagyova I, Type D, anxiety and depression in association with quality of life in patients with Parkinson’s disease and patients with multiple sclerosis: Qual Life Res, 2013; 22(6); 1353-60
29. van Middendorp H, Kool MB, van Beugen S, Prevalence and relevance of type D personality in fibromyalgia: Gen Hosp Psychiatry, 2016; 39; 66-72
30. Ablin JN, Zohar AH, Zaraya-Blum R, Buskila D, Distinctive personality profiles of fibromyalgia and chronic fatigue syndrome patients: Peer J, 2016; 4; e2421
31. Garİp Y, GÜler T, Bozkurt Tuncer Ö, Önen S, Type D personality is associated with disease severity and poor quality of life in Turkish patients with fibromyalgia syndrome: A cross-sectional study: Arch Rheumatol, 2019; 35(1); 13-19
32. Demirci S, Demirci K, Demirci S, The effect of type D personality on quality of life in patients with multiple sclerosis: Noro Psikiyatr Ars, 2017; 54(3); 272-76
33. Cao X, Wang XH, Wong EM, Type D personality negatively associated with self-care in Chinese heart failure patients: J Geriatr Cardiol, 2016; 13(5); 401-17
34. Sánchez-Díaz M, Salazar-Nievas MC, Molina-Leyva A, Arias-Santiago S, Type D personality is associated with poorer quality of life in patients with chronic spontaneous urticaria: A cross-sectional study: Acta Derm Venereol, 2022; 102; adv00734
35. Dubayova T, Nagyova I, Havlikova E, The association of type D personality with quality of life in patients with Parkinson’s disease: Aging Ment Health, 2009; 13(6); 905-12
Tables
Table 1. Comparison of demographic data between groups.Table 2. Clinical comparison of fibromyalgia and control groups.Table 3. Comparison of all participants in terms of sleep, depression, anxiety, and quality of life according to whether they have type D personality traits or not.Table 4. Comparison of clinical parameters of fibromyalgia patients according to whether they have Type D personality or not. In Press
08 Mar 2024 : Animal Research
Modification of Experimental Model of Necrotizing Enterocolitis (NEC) in Rat Pups by Single Exposure to Hyp...Med Sci Monit In Press; DOI: 10.12659/MSM.943443
18 Apr 2024 : Clinical Research
Comparative Analysis of Open and Closed Sphincterotomy for the Treatment of Chronic Anal Fissure: Safety an...Med Sci Monit In Press; DOI: 10.12659/MSM.944127
08 Mar 2024 : Laboratory Research
Evaluation of Retentive Strength of 50 Endodontically-Treated Single-Rooted Mandibular Second Premolars Res...Med Sci Monit In Press; DOI: 10.12659/MSM.944110
11 Mar 2024 : Clinical Research
Comparison of Effects of Sugammadex and Neostigmine on Postoperative Neuromuscular Blockade Recovery in Pat...Med Sci Monit In Press; DOI: 10.12659/MSM.942773
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952