04 May 2020: Clinical Research
A Cross-Sectional Observational Study to Compare the Role of Ultrasound with Mammography in Women Identified at High Risk for Breast Cancer in a Population in China
Peili An1BCF, Shujuan Zhong1BCF, Rong Zhang1ACF, Xiaoxia Hou1ABC, Ruru Xi1ADF, Yingjin Wang1CEF*DOI: 10.12659/MSM.919777
Med Sci Monit 2020; 26:e919777






Abstract
BACKGROUND: Currently, there is no national breast cancer screening program in China. In countries that have screening programs, screening mammography is used. This study aimed to compare the imaging parameters and diagnostic findings between ultrasound and mammography in women at high risk who had a histologically confirmed diagnosis of breast cancer in a population in China.
MATERIAL AND METHODS: A cross-sectional observational study included 1,687 women with a risk score of ≥30, according to the cancer risk assessment model, who underwent breast ultrasound and mammography. Women who had a Breast Imaging-Reporting and Data System (BI-RADS) score of 4 or 5 were identified, and 155 women had breast cancer confirmed by breast biopsy and histology. The ultrasound and mammography findings were evaluated and compared.
RESULTS: Breast ultrasound resulted in significantly fewer inconclusive results (BI-RADS score, 0), when compared with mammography (p=0.046). In cases with a histologically confirmed diagnosis of breast cancer (BI-RADS score, 4), the diagnostic sensitivity of breast ultrasound and mammography were 0.989 and 0.859, respectively. In cases with a histologically confirmed diagnosis of breast cancer (BI-RADS score, 5), the diagnostic sensitivity of breast ultrasound and mammography were 1.000 and 0.984, respectively. In cases with a histologically confirmed diagnosis of benign breast lesions (BI-RADS score, 2), there was no significant difference between breast ultrasound and mammography.
CONCLUSIONS: In a population of women in China, breast ultrasound was a more sensitive diagnostic imaging method for women with high risk BI-RADS 4 and 5 breast lesions.
Keywords: Biopsy, Early Detection of Cancer, Histology, Inflammatory Breast Neoplasms, Mammography, Ultrasonography, Doppler, Breast, Breast Neoplasms, Mass Screening, Sensitivity and Specificity, Ultrasonography, Ultrasonography, Mammary
Background
Currently, there is no national breast cancer screening program in China. In countries that have screening programs, screening mammography is used. Ultrasound uses high-frequency sound waves to detect abnormalities in the breast, and mammography uses X-rays. During the last two decades, the incidence of breast cancer has increased worldwide [1]. Breast cancer is now the most common cancer in women [2,3], and is the leading cause of cancer-related death in Chinese women [1]. Breast cancer screening of women at 40 years and above reduces mortality from breast cancer by 30–50% [4]. The United States Preventive Services Task Force (USPSTF) recommends screening mammography every two years for women aged between 50–74 years [5].
Mammography is widely used for breast cancer screening [6,7]. However, Chinese women have been reported to have increased breast density with age [3]. Mammography has higher sensitivity for fatty breast tissue and lower sensitivity for dense breast tissue [6]. Also, the peak age for the diagnosis of breast cancer in Chinese women is 45–49 years, which is 10–20 years less than in Caucasian women [1,2]. However, mammography is less effective in younger women compared to older women, due to increased breast density with age [7,8].
The Breast Imaging-Reporting and Data System (BI-RADS) has been developed as a quality assurance and risk assessment method by the American College of Radiologists (ACR). BI-RADS is used in the reporting of breast ultrasound, mammography, and magnetic resonance imaging (MRI). In China, most women are diagnosed with breast cancer from fine-needle aspiration cytology (FNAC) or histology of core needle biopsy of the breast [9]. However, women who present with a palpable breast mass and are diagnosed with breast cancer by cytology or histology are more likely to have distant metastases at diagnosis [10], and to have local recurrence after diagnosis and treatment [11]. Therefore, there is a need for an accurate non-invasive method for the screening of breast cancer in Chinese women. Ultrasound is found to be sensitive for screening of breast cancer in Chinese women who are at high risk of breast cancer on imaging [6]. However, currently, there are no national guidelines for screening breast cancer in China [1,6].
This cross-sectional observational study aimed to compare the imaging parameters and diagnostic findings between ultrasound and mammography in women at high risk of breast cancer in a population in China, in women who had a diagnosis confirmed by breast histopathology.
Material and Methods
ETHICAL APPROVAL AND PATIENT CONSENT:
The study design and protocol were approved by the Human Ethics Committee of the Northwest Women’s and Children’s Hospital (Approval number: NWCH/CL/14/19, dated 24th July 2019). The study was conducted according to the legal requirements for human studies in China. The cross-sectional study was designed and conducted according to the strengthening of the reporting of observational studies in epidemiology (STROBE) statement [12], and the 2008 Helsinki Declaration. Informed consent was signed by all participating women or their relatives or their legally authorized person for diagnosis, anesthesia (if required), biopsies, histopathology, radiology, or performing additional diagnostic procedures as part of the study. Personal data and images in all formats were anonymized to ensure patient confidentiality.
STUDY PARTICIPANTS:
Between 1st June 2016 to 30th June 2019, a breast cancer screening program was conducted at the Northwest Women’s and Children’s Hospital, China, and the referring hospitals. A total of 3,579 women completed questionnaires regarding their breast health, their lifestyle, demographical characteristics, clinical conditions, and reproductive history. The risk of breast cancer was assessed using a model that was recommended by the Institutional Review Board, with a risk score that ranged from 0–100 [13]. There were 1,892 women who had a risk score of <30 who were considered to be at low risk for breast cancer. Therefore, these women were excluded from further investigations. There were 1,687 women who were screened with a risk score of 30 or more, and these women were advised to undergo either mammography or breast ultrasound.
DATA COLLECTION:
Data from the clinical questionnaires, mammography, breast ultrasound, and breast biopsy and histopathology were collected from the institutional medical records. The flowchart of the study design is shown in Figure 1. The mean age of women at the time of enrollment into the study was 45.45 years, 55% of women were <50 years, and 20% of women were postmenopausal. The demographic and clinical characteristics and the reproductive history of the women are presented in Table 1.
MAMMOGRAPHY:
A standard two-view (cranial-caudal and medial-lateral oblique) mammography was performed using Senographe™ Crystal full-field digital mammography (GE Healthcare, Chicago, IL, USA) [3]. The mammographs were reported by radiologists with a minimum of three years of experience who was unaware of the data in the clinical questionnaires.
BREAST ULTRASOUND:
Breast ultrasound was performed by color Doppler using a LOGIQ E9 XDclear 2.0 radiology ultrasound system (GE Healthcare, Chicago, IL, USA) using a 12 MHz XDclear 2.0 transducer (GE Healthcare, Chicago, IL, USA). Transverse and sagittal planes were scanned by ultrasound technologists with a minimum of three years of experience who were unaware of the data in the clinical questionnaires and the mammographic findings [6].
IMAGING ANALYSIS USING THE BREAST IMAGING-REPORTING AND DATA SYSTEM (BI-RADS):
Breast ultrasound and mammographic examinations were interpreted using the Breast Imaging-Reporting and Data System (BI-RADS) using scores between 0–5. BI-RADS 0, inconclusive results requiring further mammography; BI-RADS 1, no areas of architectural distortion, suspicious calcifications, or masses (tumor was absent); BI-RADS 2, simple cysts, secretory calcifications, calcified fibroadenomas, implants, fat-containing lesions, and intramammary lymph nodes (benign tumor); BI-RADS 3, a solitary mass of punctate calcifications, or a circumscribed and non-palpable mass, or focal asymmetry (probably benign); BI-RADS 4, suspicious for malignancy; and BI-RADS 5, highly suggestive of malignancy (Figures 2, 3) [6]. Radiologists and ultrasound technologists had a minimum of three years of experience and were unaware of the data in the clinical questionnaires.
BREAST BIOPSIES:
Women with BI-RADS scores of 4 or 5 (Figure 4) underwent breast biopsies and histopathology [8]. Breast sampling was ultrasound-guided using a LOGIQ™ E9 ultrasound system (GE Healthcare, Chicago, IL, USA) for fine-needle aspiration cytology (FNAC), core needle biopsy, using an 18 G biopsy needle (BD Biosciences, Chicago, IL, USA), and excision biopsy. Breast biopsies were performed by physicians with a minimum of three years of experience who were unaware of the data in the clinical questionnaires and the mammographic and ultrasound data [14].
BREAST HISTOPATHOLOGY:
The histological analysis was performed by histopathologists with a minimum of three years of experience who were unaware of the data in the clinical questionnaires and the mammographic and ultrasound data.
BENEFICIAL SCORE ANALYSIS:
The beneficial score for each diagnostic modality was evaluated according to Equation 1 of the BI-RADS level of evidence [15]:
Where,
Where, PCD is the true positive tumor detected; NCD, is the true negative tumor detected; N, is the total number of women included in the analysis.
COST ANALYSIS:
Cost data regarding imaging modalities and the biopsies and histopathology were obtained from the medical and institutional records.
STATISTICAL ANALYSIS:
Data were analyzed using InStat version 3.0 (GraphPad, San Diego, CA, USA). The study sample size was calculated on the basis that the sensitivity of each diagnostic method varied from 50–90% and the maximum missing data was estimated to be 30%. Categorical data were presented as the frequency (number), and continuous data were presented as the mean ± standard deviation (SD). Categorical data were analyzed by Fisher’s exact test or the chi-squared (χ2) test. Continuous data were analyzed by one-way analysis of variance (ANOVA) following Tukey’s post hoc test, with a critical value (q) >3.25 considered to be significant. Data were considered significant, with a 95% confidence level [6].
Results
DIAGNOSTIC PARAMETERS:
There were 141 women who were reported to have a Breast Imaging-Reporting and Data System (BI-RADS) score of 4 or 5 by mammography, and 155 women were reported to have a BI-RADS score of 4 or 5 by ultrasound. Breast biopsy and histopathology were performed in 155 women and included 98 fine-needle aspiration cytology (FNAC) samples, 32 core needle biopsies, and 25 excision biopsies. Breast ultrasound combined with mammography resulted in fewer inconclusive results (BI-RADS score, 0) than breast ultrasound (p=0.002) and mammography (p<0.0001). Breast ultrasonography resulted in fewer numbers of inconclusive results (BI-RADS score: 0) than mammography (p=0.046). The sensitivity of breast biopsy and histopathology for the detection of BI-RADS score 4 on breast ultrasound, mammography, and breast ultrasound plus mammography were 0.989, 0.859, and 1.000, respectively. The sensitivity of breast biopsy and histopathology for the detection of BI-RADS score 5 on breast ultrasound, mammography, and breast ultrasound plus mammography were 1.000, 0.984, and 1.000, respectively. Breast ultrasound and mammography both had the same specificity (p=0.34). The analysis of imaging and biopsy results are presented in Table 2. The histological diagnosis of breast cancers are presented in Table 3.
BENEFICIAL SCORE ANALYSIS:
For inconclusive results (BI-RADS score, 0), benign lesion or no tumor (BI-RADS score, 1), and highly suggestive of malignancy (BI-RADS score, 5), breast ultrasound and mammography had the same sensitivity. For the detection of benign lesions (BI-RADS score, 2), probably benign tumor (BI-RADS score, 3), and suspicious for malignancy (BI-RADS score, 4), the sensitivity for the detection of breast cancer was significantly greater for breast ultrasound than mammography. For the detection of benign breast lesions (BI-RADS score, 2), there was a significant difference between breast ultrasound and mammography (Figure 5). When breast ultrasound combined with mammography was considered as a reference standard, there was a significant difference between the results predicted by breast ultrasound and mammography (p<0.0001) (Table 4).
COST ANALYSIS:
Breast ultrasound (75±7 ¥ per patient) had a significantly lower cost than mammography (210±15 ¥/patient; p<0.0001; q=86.255) and biopsy and histopathology (315±35 ¥/patient, p<0.0001, q=153.34) (Figure 6).
Discussion
This study reported fewer numbers of inconclusive results for breast ultrasonography than mammography. Breast biopsy and histopathology had a sensitivity for the detection of Breast Imaging-Reporting and Data System (BI-RADS) scores of 4 and 5 tumors, which was significantly higher for breast ultrasound than mammography. The study results were consistent with a previously reported multicenter randomized trial of Chinese women [6] and a previously published retrospective cross-sectional study [16]. The low sensitivity of mammography may be due to the increased breast density of Chinese women [3], the younger age of the women enrolled in this study, and fewer postmenopausal women who had breast glandular tissue replaced by fat [6]. There has been previously reported to be an inverse relationship between age and breast density [8]. However, ultrasound scans of the breast are less affected by age [6]. The findings from the present study support that breast ultrasonography has a higher sensitivity than mammography in Chinese women.
Comparatively high numbers of inconclusive results, with a BI-RADS score of 0, were reported by both imaging modalities, and the results of the present study were consistent with these findings from breast cancer screening programs of Chinese women [6,16]. This study program for early detection of breast cancer included women who volunteered for the study who may or may not have required further imaging methods. There are several models available for breast cancer risk assessment. For example, the Claus model and extended formula and tables, the Gail model, the Gail-2 model, the BOADICEA model of the genetic susceptibility to breast cancer, the Jonker model, and the Tyrer-Cuzick model [13]. Therefore, there is a need to establish a suitable national breast cancer risk-prediction model in China to reduce inconclusive results.
In this study, for the detection of benign breast tumors (BI-RADS score, 2), breast ultrasound had a significantly higher detection rate than mammography. Ultrasound has previously been shown to have high specificity for the detection of malignant and benign lesions of the breast [15]. In premenopausal Chinese women, increased glandular breast tissue affects the mammographic findings [8], and mammography has a higher risk of overdiagnosis [17]. Breast cancer screening has a recognized limitation of underdiagnosis because life-threatening breast cancers may not be diagnosed easily with a single imaging modality [18]. Breast ultrasound may be the best diagnostic modality for the detection of slow-growing tumors in Chinese women, which have a better prognosis than the faster-growing tumors that women may identify by self-examination of the breasts.
The findings from the present study showed that breast ultrasound had the least cost for breast cancer screening, which was consistent with previous studies on breast cancer screening programs in China [6,16]. The cost factor is an important part of the screening of cancer in developing countries [6]. Digital mammography is more expensive than conventional mammography and breast ultrasound [4]. In China, a higher percentage of women do not participate in breast cancer screening programs because of family needs, financial issues, and social inconvenience [6]. Ultrasonography is more convenient for the screening of breast cancer in Chinese women compared with mammography.
The study has several limitations. This study was of short duration, and there was a lack of patient follow-up to determine survival data. Women with a low risk of breast cancer were excluded from the program, which may have affected the performance of the diagnostic imaging modalities. The women’s demographic and clinical conditions also are recognized to have effects on the results of imaging modalities [3]. The study did not evaluate the effects of demographic and clinical parameters on the results of the imaging modalities. Breast biopsy and histopathology were performed in only 155 women, and the observational period of the study was short.
Conclusions
This study aimed to compare the imaging parameters and diagnostic findings between ultrasound and mammography in women at high risk who had a histologically confirmed diagnosis of breast cancer in a population in China. Women who had a Breast Imaging-Reporting and Data System (BI-RADS) score of 4 or 5 were identified and 155 women had breast cancer confirmed by breast biopsy and histology. Breast ultrasound was a more sensitive diagnostic imaging method for women with high risk BI-RADS 4 and 5 breast lesions.
Figures
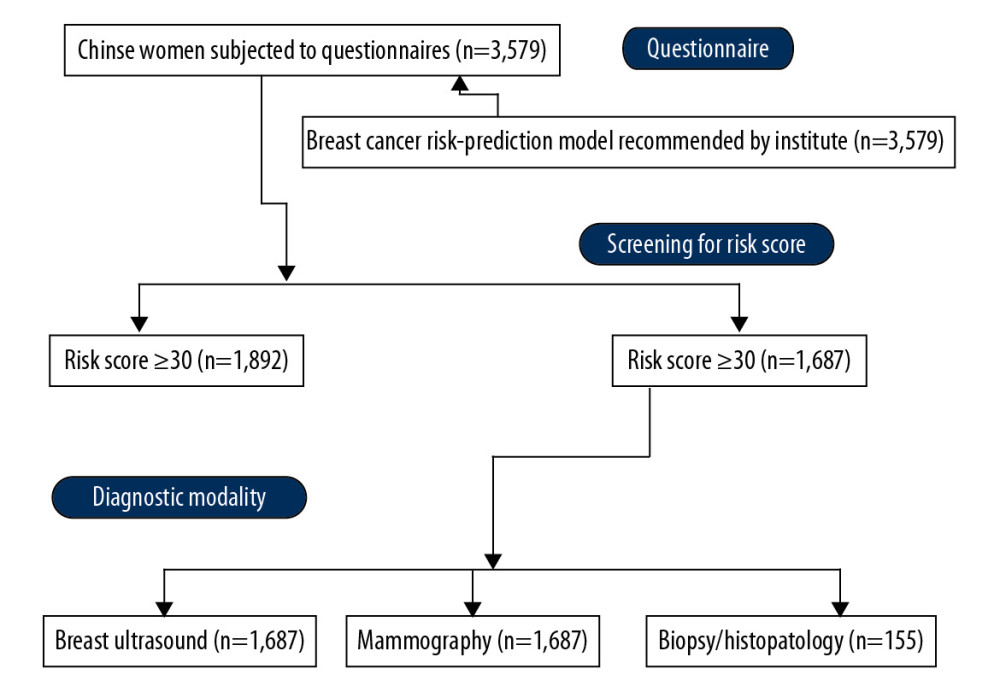 Figure 1. The flowchart of the study design.
Figure 1. The flowchart of the study design. 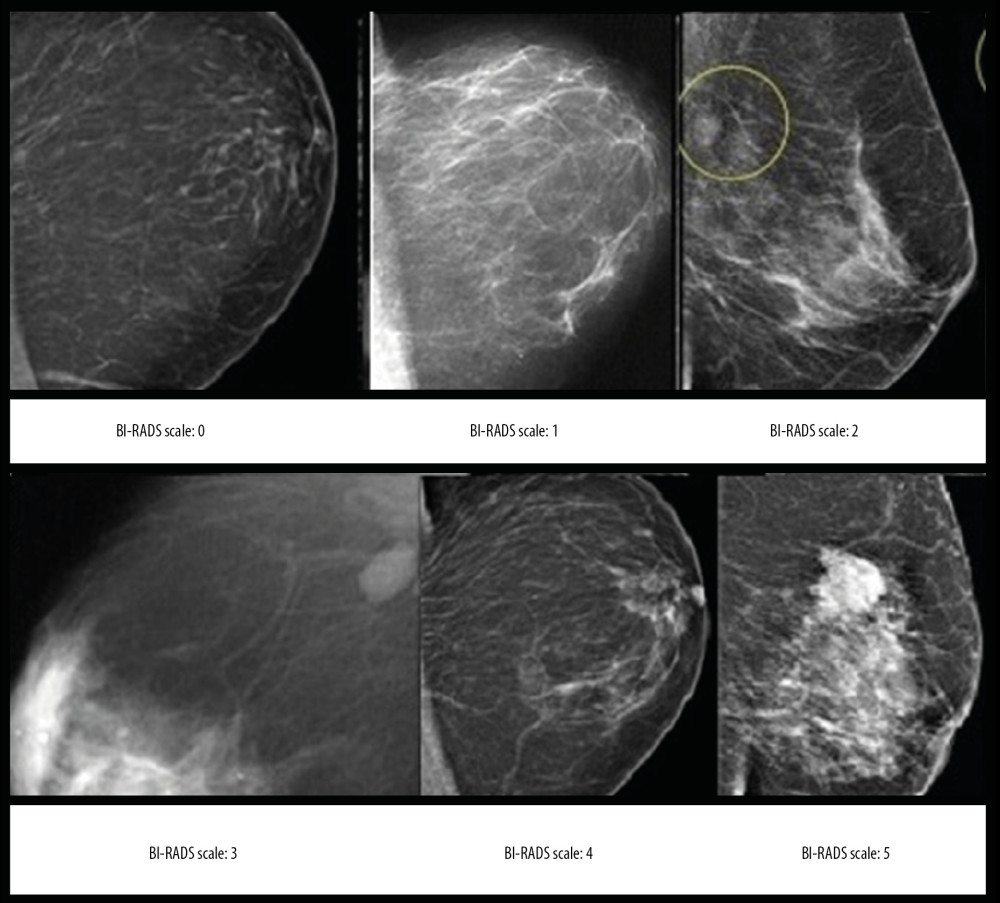 Figure 2. The Breast Imaging-Reporting and Data System (BI-RADS) scores according to the mammography.
Figure 2. The Breast Imaging-Reporting and Data System (BI-RADS) scores according to the mammography. 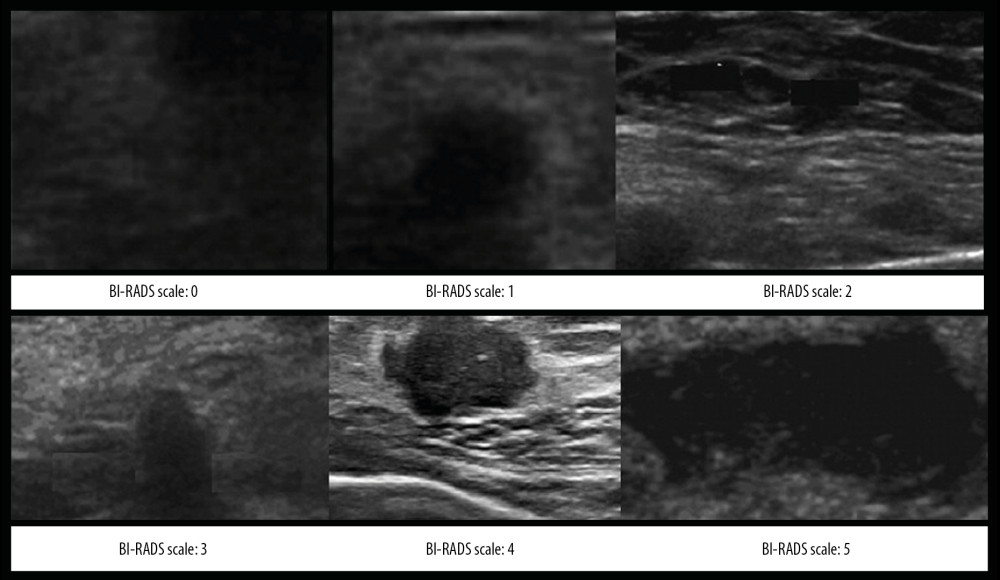 Figure 3. The Breast Imaging-Reporting and Data System (BI-RADS) scores according to the breast ultrasound.
Figure 3. The Breast Imaging-Reporting and Data System (BI-RADS) scores according to the breast ultrasound. 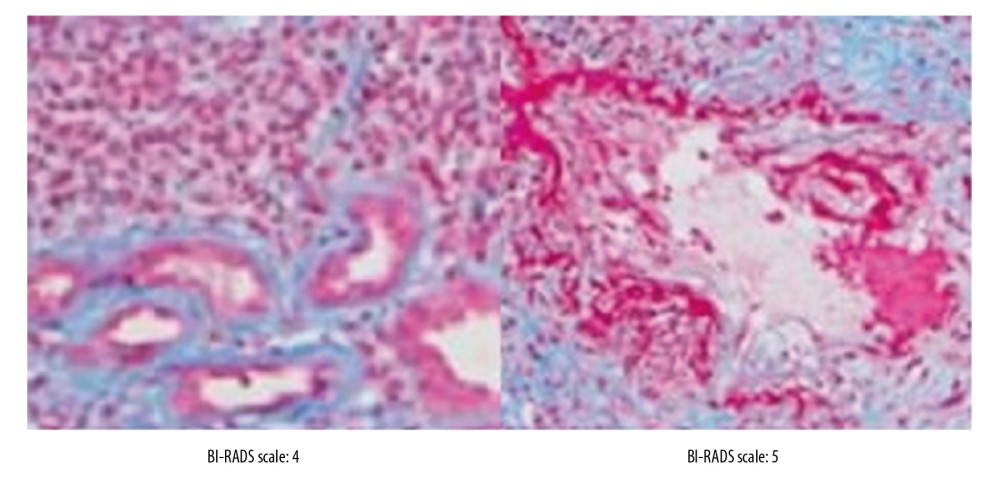 Figure 4. The Breast Imaging-Reporting and Data System (BI-RADS) scores according to the histopathology of the breast biopsies.
Figure 4. The Breast Imaging-Reporting and Data System (BI-RADS) scores according to the histopathology of the breast biopsies. 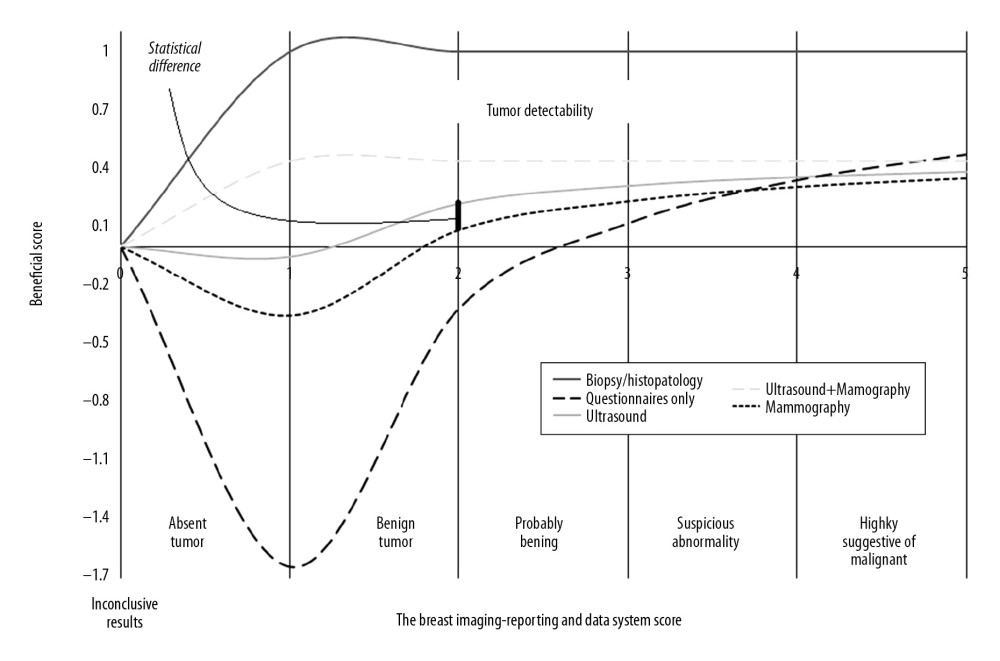 Figure 5. The beneficial score analysis. Physicians performed the biopsies. Pathologists performed the histological analysis. Radiologists performed the mammography. Ultrasound technologists performed breast ultrasound. All had a minimum of three years of experience. 0, inconclusive results; 1, tumor was absent; 2, benign tumor; 3, probably benign; 4, suspicious abnormality; 5, highly suggestive of malignancy.
Figure 5. The beneficial score analysis. Physicians performed the biopsies. Pathologists performed the histological analysis. Radiologists performed the mammography. Ultrasound technologists performed breast ultrasound. All had a minimum of three years of experience. 0, inconclusive results; 1, tumor was absent; 2, benign tumor; 3, probably benign; 4, suspicious abnormality; 5, highly suggestive of malignancy. 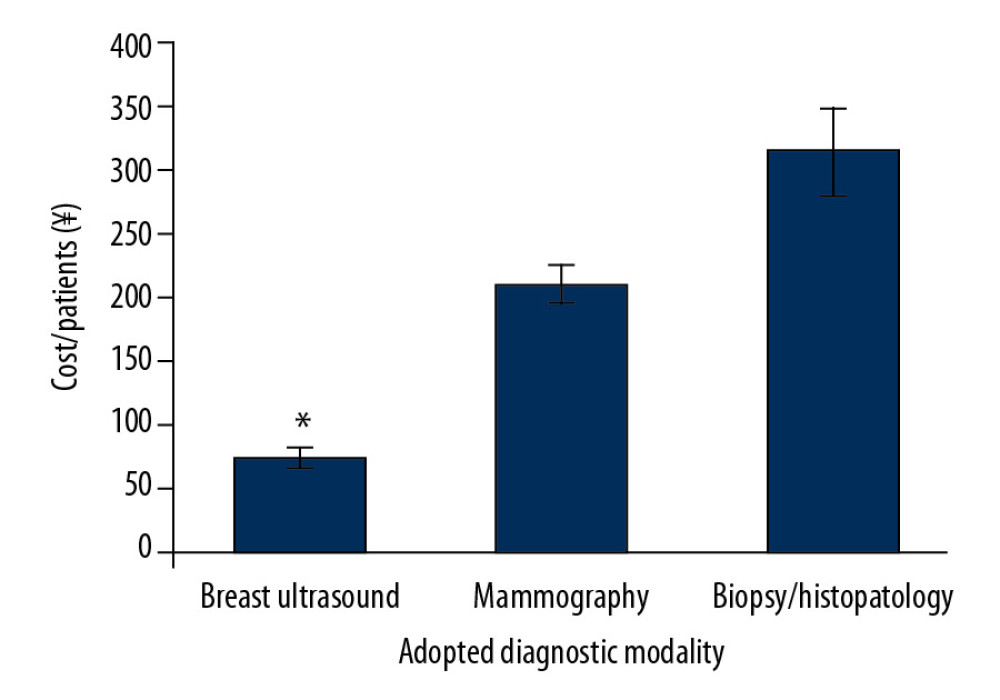 Figure 6. Cost analysis of the diagnosis. Data are presented as the mean±standard deviation (SD). Data were analyzed by one-way analysis of variance (ANOVA) following Tukey’s post hoc test. A p<0.05 and q>3.25 were considered significant. * Significantly lower than mammography and biopsy/histopathology.
Figure 6. Cost analysis of the diagnosis. Data are presented as the mean±standard deviation (SD). Data were analyzed by one-way analysis of variance (ANOVA) following Tukey’s post hoc test. A p<0.05 and q>3.25 were considered significant. * Significantly lower than mammography and biopsy/histopathology. References
1. Li J, Zhang BN, Fan JH, A nation-wide multicenter 10-year (1999–2008) retrospective clinical epidemiological study of female breast cancer in China: BMC Cancer, 2011; 11; 364
2. Fan L, Strasser-Weippl K, Li JJ, Breast cancer in China: Lancet Oncol, 2014; 15; e279-89
3. Zulfiqar M, Rohazly I, Rahmah M, Do the majority of Malaysian women have dense breasts on mammogram?: Biomed Imaging Interv J, 2011; 7(2); e14
4. Feig S, Comparison of costs and benefits of breast cancer screening with mammography, ultrasonography, and MRI: Obstet Gynecol Clin North Am, 2011; 38; 179-96
5. Niemczyk NA, Screening mammography may be less effective than thought: J Midwifery Womens Health, 2014; 59; 465-67
6. Shen S, Zhou Y, Xu Y: Br J Cancer, 2015; 112; 998-1004
7. Shen SJ, Sun Q, Xu YLComparative analysis of early diagnostic tools for breast cancer: Zhonghua Zhong Liu Za Zhi, 2012; 34(11); 877-80 [in Chinese]
8. Checka CM, Chun JE, Schnabel FR, The relationship of mammographic density and age: Implications for breast cancer screening: Am J Roentgenol, 2012; 198; W292-95
9. Wu X, Lin Q, Lu J, Comparison of mammography and ultrasound in detecting residual disease following bioptic lumpectomy in breast cancer patients: Mol Clin Oncol, 2016; 4; 419-24
10. Sennerstam RB, Franzen BS, Wiksell HO, Auer GU, Core-needle biopsy of breast cancer is associated with a higher rate of distant metastases 5 to 15 years after diagnosis than FNA biopsy: Cancer Cytopathol, 2017; 125; 748-56
11. Sanchez MA, Burga AM, Ljung BM, Primum non nocere: Cancer Cytopathol, 2017; 125; 745-47
12. Vandenbroucke JP, von Elm E, Altman DG, Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration: PLoS Med, 2007; 4; e297
13. Xu YL, Sun Q, Shan GL, A case-control study on risk factors of breast cancer in China: Arch Med Sci, 2012; 8; 303-9
14. Park CS, Kim SH, Jung NY, Interobserver variability of ultrasound elastography and the ultrasound BI-RADS lexicon of breast lesions: Breast Cancer, 2015; 22; 153-60
15. Zhao W, Yan K, Liu Y, Zhang Z, Contrast ultrasound versus ultrasound elastography for diagnosis of breast lumps: A cross-sectional study: Medicine (Baltimore), 2019; 98(26); e16132
16. Wang FL, Chen F, Yin H, Effects of age, breast density and volume on breast cancer diagnosis: a retrospective comparison of sensitivity of mammography and ultrasonography in China’s rural areas: Asian Pac J Cancer Prev, 2013; 14; 2277-82
17. Yaffe MJ, Pritchard KI, Overdiagnosing overdiagnosis: Oncologist, 2014; 19; 103-6
18. Bleyer A, Welch HG, Effect of three decades of screening mammography on breast-cancer incidence: N Engl J Med, 2012; 367; 1998-2005
Figures
Figure 1. The flowchart of the study design.Figure 2. The Breast Imaging-Reporting and Data System (BI-RADS) scores according to the mammography.Figure 3. The Breast Imaging-Reporting and Data System (BI-RADS) scores according to the breast ultrasound.Figure 4. The Breast Imaging-Reporting and Data System (BI-RADS) scores according to the histopathology of the breast biopsies.Figure 5. The beneficial score analysis. Physicians performed the biopsies. Pathologists performed the histological analysis. Radiologists performed the mammography. Ultrasound technologists performed breast ultrasound. All had a minimum of three years of experience. 0, inconclusive results; 1, tumor was absent; 2, benign tumor; 3, probably benign; 4, suspicious abnormality; 5, highly suggestive of malignancy.Figure 6. Cost analysis of the diagnosis. Data are presented as the mean±standard deviation (SD). Data were analyzed by one-way analysis of variance (ANOVA) following Tukey’s post hoc test. A p<0.05 and q>3.25 were considered significant. * Significantly lower than mammography and biopsy/histopathology. Tables
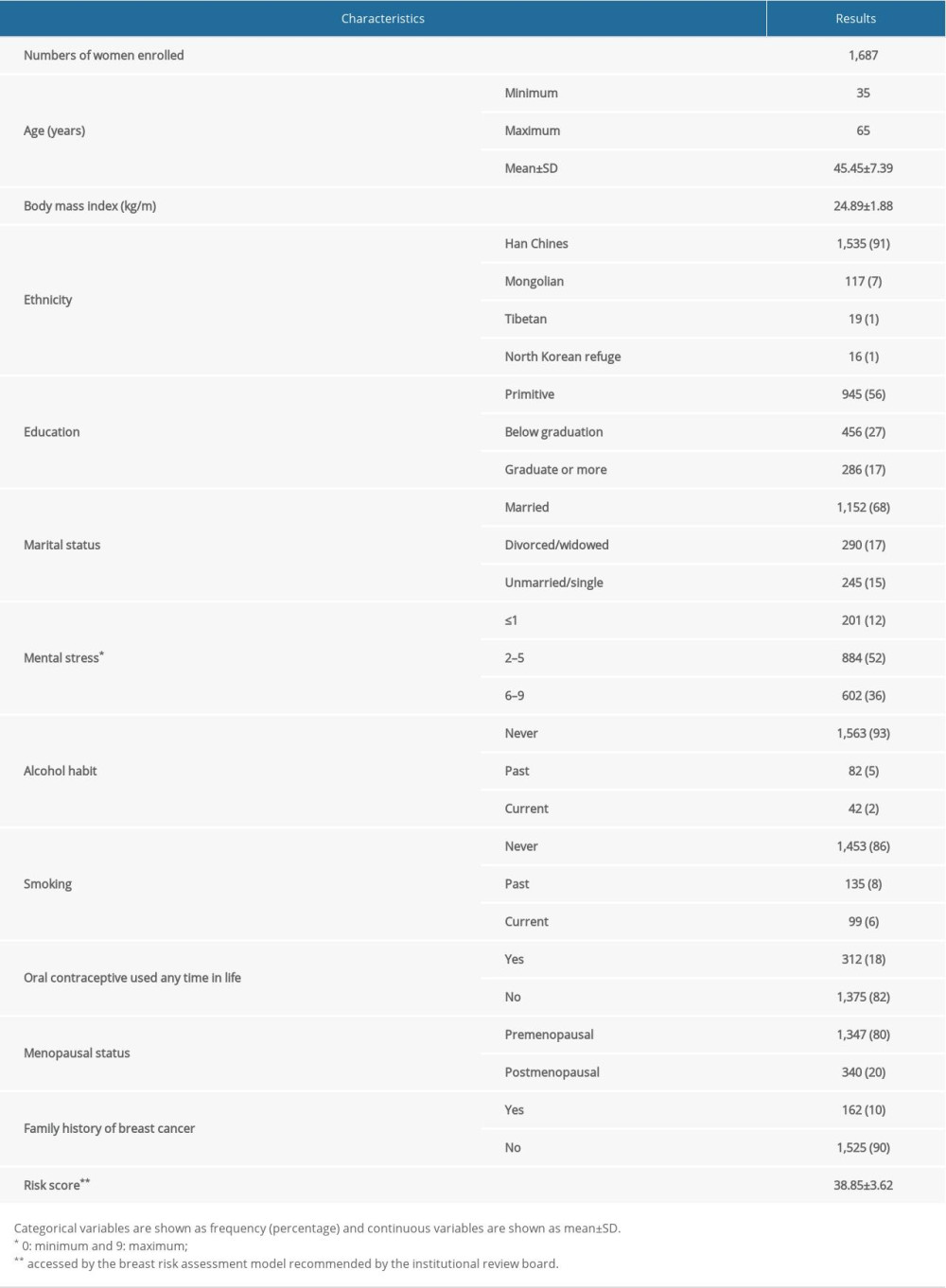 Table 1. Questionnaires results of the enrolled women.
Table 1. Questionnaires results of the enrolled women.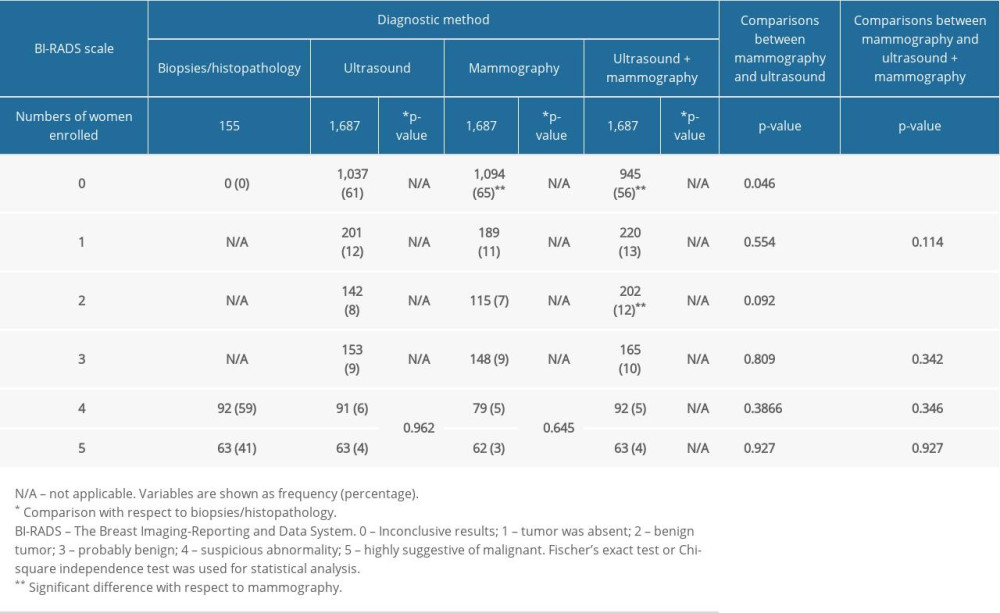 Table 2. Specification for diagnostic parameters of adopted modalities.
Table 2. Specification for diagnostic parameters of adopted modalities.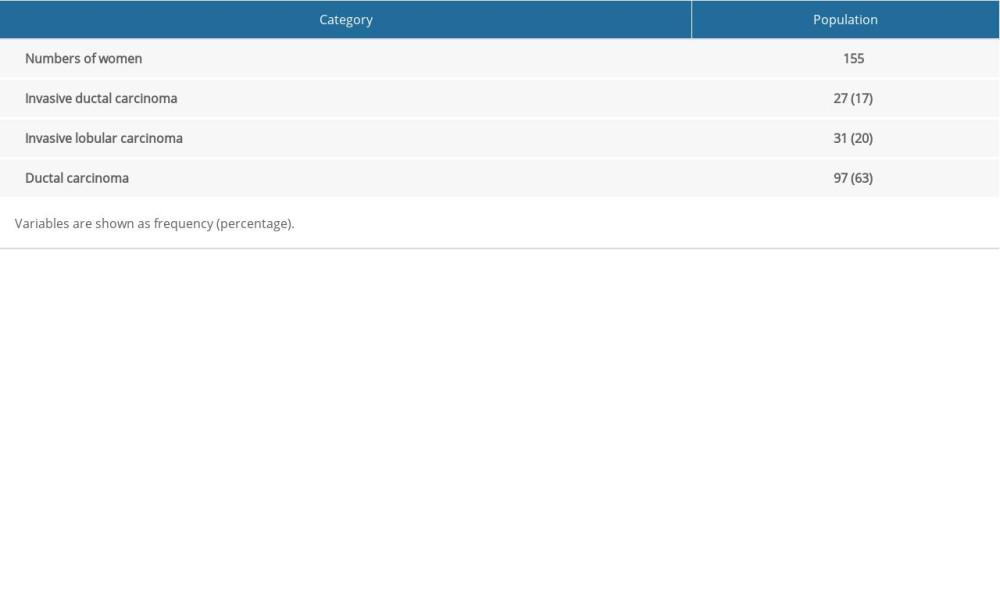 Table 3. The histological diagnosis of the breast cancers diagnosed.
Table 3. The histological diagnosis of the breast cancers diagnosed.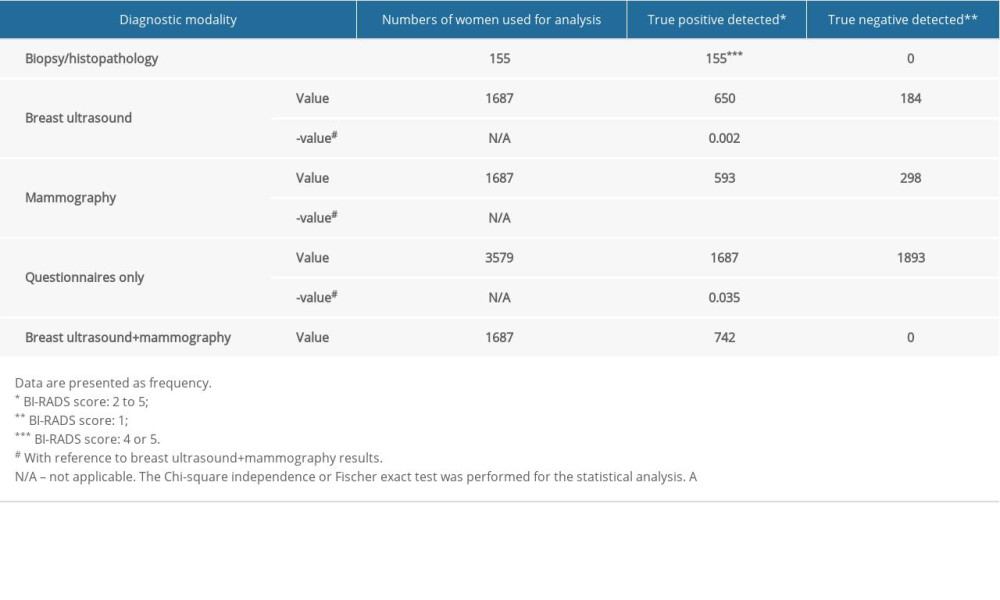 Table 4. Data of diagnostic parameters used in the analysis.Table 1. Questionnaires results of the enrolled women.Table 2. Specification for diagnostic parameters of adopted modalities.Table 3. The histological diagnosis of the breast cancers diagnosed.Table 4. Data of diagnostic parameters used in the analysis.
Table 4. Data of diagnostic parameters used in the analysis.Table 1. Questionnaires results of the enrolled women.Table 2. Specification for diagnostic parameters of adopted modalities.Table 3. The histological diagnosis of the breast cancers diagnosed.Table 4. Data of diagnostic parameters used in the analysis. In Press
Clinical Research
Body Weight and Insulin Resistance Indicators Among ChildrenMed Sci Monit In Press; DOI: 10.12659/MSM.951434
Clinical Research
Comparison of Radiographic Cervical Sagittal Alignment Parameters in Patients With Nonspecific Neck Pain, D...Med Sci Monit In Press; DOI: 10.12659/MSM.952950
Clinical Research
Combined Fibrinogen and Urinary α1-Microglobulin as Predictors of Respiratory Tract Infection in Children w...Med Sci Monit In Press; DOI: 10.12659/MSM.951066
Database Analysis
Evaluation of Salivary Total Oxidant Status (TOS) and Total Antioxidant Status (TAS) in Orthodontic Patient...Med Sci Monit In Press; DOI: 10.12659/MSM.952052
Most Viewed Current Articles
17 Jan 2024 : Review article 14,175,576
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,756,620
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,465,966
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,651
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387