17 July 2020: Lab/In Vitro Research
Expression of the C677T Polymorphism of the 5, 10-Methylenetetrahydrofolate Reductase (MTHFR) Gene in Patients with Carotid Artery Atherosclerosis
Anying Li1BG, Wei Huang1C, Qiong Yang1AE, Liping Peng1BD, Qiang Liu2ADE*DOI: 10.12659/MSM.920320
Med Sci Monit 2020; 26:e920320






Abstract
BACKGROUND: The C677T polymorphism of the 5,10-methylenetetrahydrofolate reductase (MTHFR) gene polymorphism has been associated with hypertension and coronary heart disease, but its relationship with carotid artery remains unknown. This study aimed to investigate the association between the C677T polymorphism of the MTHFR gene in patients with confirmed carotid artery atherosclerosis.
MATERIAL AND METHODS: This retrospective study included 210 patients with carotid artery atherosclerosis (the patient group) and 210 controls (the control group). Color Doppler ultrasound was used to identify carotid artery intimo-medial thickness and atherosclerotic plaques. Sanger sequencing using the polymerase chain reaction (PCR) was used to detect the MTHFR C677T gene polymorphism. Systolic blood pressure (SBP), diastolic blood pressure (DBP), fasting plasma glucose (FPG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglyceride (TG), glycosylated hemoglobin (HbA1c), and other laboratory indicators were measured.
RESULTS: SBP, DBP, FPG, TC, LDL-C, HbA1c, and intimo-medial thickness were significantly increased in the patient group compared with the control group, and HDL-C was significantly lower. The allele frequencies of the C667T locus of MTHFR gene were significantly different between the two groups (P<0.05), and the TT genotype and the T allele frequencies in the patient group were higher than in the control group. Logistic regression analysis showed that SBP, TC, LDL-C, and the C667T MTHFR gene polymorphism were risk factors for carotid artery atherosclerosis.
CONCLUSIONS: The C677T polymorphism of the MTHFR gene was expressed in patients with carotid artery atherosclerosis.
Keywords: 5,10-Methylenetetrahydrofolate Reductase (FADH2), atherosclerosis, Polymorphism, Genetic, Statistics as Topic, Blood Pressure, Carotid Arteries, Carotid Artery Diseases, Carotid Artery, Common, Gene Frequency, Genotype, Hypertension, Methylenetetrahydrofolate Reductase (NADPH2), Polymorphism, Single Nucleotide, Risk Factors
Background
With the improvement of living standards and the aging of the population, cerebrovascular diseases have become important diseases that endanger human health and life. Carotid artery atherosclerosis is a risk factor for ischemic stroke, particularly in older adults [1–3]. Atherosclerosis is a disease of muscular arteries and the aorta that begins in childhood and increases with age. Carotid artery atherosclerosis causes carotid artery stenosis, and when thrombosis is associated with the advanced atherosclerotic plaque, the artery can occlude, resulting in the loss of blood supply to the brain [4–6]. Previous studies have shown that smoking, stress, lifestyle, hypertension, diabetes, and abnormal lipid metabolism are associated with the pathogenesis of carotid artery atherosclerosis [7]. With the development of genetic testing, gene polymorphisms have been shown to affect the occurrence and development of atherosclerosis by affecting several risk factors. The susceptibility genes associated with atherosclerosis include genes associated with the renin-angiotensin system, including angiotensin-converting enzyme (ACE), apolipoprotein-related genes such as apolipoprotein L1 (APOLl), and interleukin-6 (IL-6) [8].
The 5, 10-methylenetetrahydrofolate reductase (MTHFR) gene encodes a key enzyme involved in folate metabolism. MTHFR gene polymorphisms affect the activity and thermal stability of the MTHFR protein, which changes the concentration of homocysteine and folic acid
Material and Methods
PATIENTS:
A total of 210 patients who were diagnosed with carotid artery atherosclerosis were enrolled in this study from the Department of Neurology of our hospital from February 2017 to September 2018. The study group included 103 men and 107 women with a mean age of 65.54±9.23 years. All patients were diagnosed with carotid artery atherosclerosis by ultrasonography. The control group included 210 healthy adults who underwent routine medical examinations in our hospital with no cardiovascular and cerebrovascular disease, liver, or kidney disease. The control group included 106 men and 104 women with a mean age of 64.83±10.81 years who had normal carotid arteries on ultrasound examination. The Ethics Committee of the Third Xiangya Hospital, Changsha, China, approved the study, and informed consent was obtained from all study participants.
REAGENTS AND INSTRUMENTS:
The Eppendorf gradient polymerase chain reaction (PCR) instrument (Eppendorf, Hamburg, Germany), a cryogenic 5424 high-speed centrifuge (Eppendorf, Hamburg, Germany), and the Nanodrop2000 spectrophotometer (Thermo Fisher Scientific, Waltham, MA, USA) were used. The S2000 Color Doppler ultrasound system (Siemens, Munich, Germany) was used for carotid artery imaging. An immunoassay analyzer (Beckman Coulter, Brea, CA, USA), an AU 600 automatic biochemical analyzer (Olympus, Tokyo, Japan), and LH750 blood cell analyzer (Beckman Coulter, Brea, CA, USA) were used. The polymerase chain reaction (PCR) was performed using the KOD-FX Neo (Toyobo Co. Ltd., Osaka, Japan). A blood genomic DNA extraction kit and agarose gel were obtained from Beijing Tiangen (Beijing, China). Primer synthesis and Sanger sequencing were performed by Shanghai Shenggong Biotechnology Co., Ltd. (Shanghai, China).
PATIENT CLINICAL AND DEMOGRAPHIC DATA:
Clinical and demographic data were collected for all subjects, including gender, age, family history, smoking history, alcohol consumption, diet, and exercise. Clinical measurements included systolic blood pressure (SBP), diastolic blood pressure (DBP), height, weight, and body mass index (BMI). Then, 4 mL of EDTA anticoagulated fasting venous blood was collected in the early morning. The fasting plasma glucose level was determined by the glucose oxidase method. Total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglyceride (TG), and glycosylated hemoglobin (HbA1c) were measured using an AU 600 fully automatic biochemical analyzer (Olympus, Tokyo, Japan).
CAROTID ULTRASOUND FOR CAROTID ARTERY ATHEROSCLEROSIS:
Carotid artery imaging was performed using color Doppler ultrasound to detect the distal part of the common carotid arteries below the bifurcation, the common carotid artery at the bifurcation, and the proximal part of the internal carotid artery to determine the intimo-medial thickness and the diameter of the vascular lumen. The intimo-medial thickness was the vertical distance between the lumen and the endocardial junction. The presence or absence of intimo-medial thickening was determined, and the shape, size, and properties of the atherosclerotic plaque were determined.
DIAGNOSIS OF CAROTID ATHEROSCLEROSIS AND PLAQUE CHARACTERISTICS:
An intimo-medial thickness of <1.0 mm was normal. The intimo-medial thickness was considered to be increased at between 1.0 mm and 1.2 mm. An intimo-medial thickness of >1.2 mm represented the formation of an atherosclerotic plaque. An intimo-medial thickness of ≥1.0 mm represented carotid atherosclerosis. The mixed plaques with low echogenic lipid content and uneven echogenicity were regarded as unstable plaques. The fibrous plaques with strong echogenicity or calcification were identified as stable plaques.
DNA EXTRACTION:
Anticoagulated blood (500 μL) was collected, and DNA extraction was performed according to the standard genomic DNA extraction method. Briefly, 1000 μL of red blood cell lysate was added to 500 μL of anticoagulant, mixed by inversion, incubated at room temperature for 5 min, and centrifuged at 3,000 rpm for 5 min. After discarding the supernatant, 200 μL of buffer solution, and 20 μL of proteinase K were added and mixed by shaking, followed by the addition of 200 μL of buffer solution, and incubation at 70°C for 10 min until the solution became clear. Then, 200 μL of absolute ethanol was added and mixed for 15 s followed by transfer to the CB3 adsorption column and centrifuged at 30°C for 30 sec. The column was washed twice, and the DNA was eluted with 50 μL of the buffer. The DNA purity was determined using a NanoDrop 2000 ultraviolet spectrophotometer (Thermofisher Scientific, Waltham, MA, USA). DNA was stored at −20°C for further study.
POLYMERASE CHAIN REACTION (PCR) AMPLIFICATION AND SEQUENCING:
The PCR reaction mixture contained 2×KOD PCR buffer (12.5 μL), dNTPs (4 μL), buffer F (0.5 μL), buffer R (0.5 μL), DNA (2 μL), and double-distilled H2O (5.5 μL). The PCR amplification cycles included denaturing at 94°C for 2 min, 94°C for 30 sec, 55°C for 30 sec, 72°C for 1 min, and 35 cycles at 72°C for 10 min. According to the MTHFR gene sequence (NG_013351.1), PCR primers were designed using Primer Premier version 5.0 software. The primer sequences used for PCR were:
The PCR amplification product size was 233 bp and was analyzed by agarose gel electrophoresis and sent to Shanghai Biotech (Shanghai, China) for Sanger sequencing.
STATISTICAL ANALYSIS:
Data were analyzed using SPSS version 17.0 software (IBM Corp., Armonk, NY, USA). Categorical data were presented as the mean±standard deviation (SD). Comparison between two groups was performed using the Student’s t-test. For two comparisons within the same group, one-way analysis of variance (ANOVA) with Bonferroni post hoc analysis were performed. The data included the number of cases of carotid artery atherosclerosis. The chi-squared (χ2) test was used for statistical analysis. The allele frequency=(2×homozygous+heterozygous)/(2×number of subjects) was analyzed. The balance of the MTHFR gene distribution was detected by the Hardy-Weinberg method. The risk factors for carotid atherosclerosis were analyzed by multiple logistic regression analysis of the binomial classification. A p-value <0.05 was considered to be statistically significant.
Results
COMPARISON OF GENERAL AND BIOCHEMICAL INDICATORS BETWEEN THE PATIENT GROUP AND THE CONTROL GROUP:
There were no significant differences in age, gender, body mass index (BMI), and plasma triglyceride (TG) levels between the patient group and the control group (p>0.05). However, the systolic blood pressure (SBP), diastolic blood pressure (DBP), fasting plasma glucose (FPG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), and glycosylated hemoglobin (HbA1c) in the patient group were significantly higher than those in the control group. In contrast, plasma levels of high-density lipoprotein cholesterol (HDL-C) were lower in the control group (Table 1).
MTHFR GENE POLYMORPHISMS:
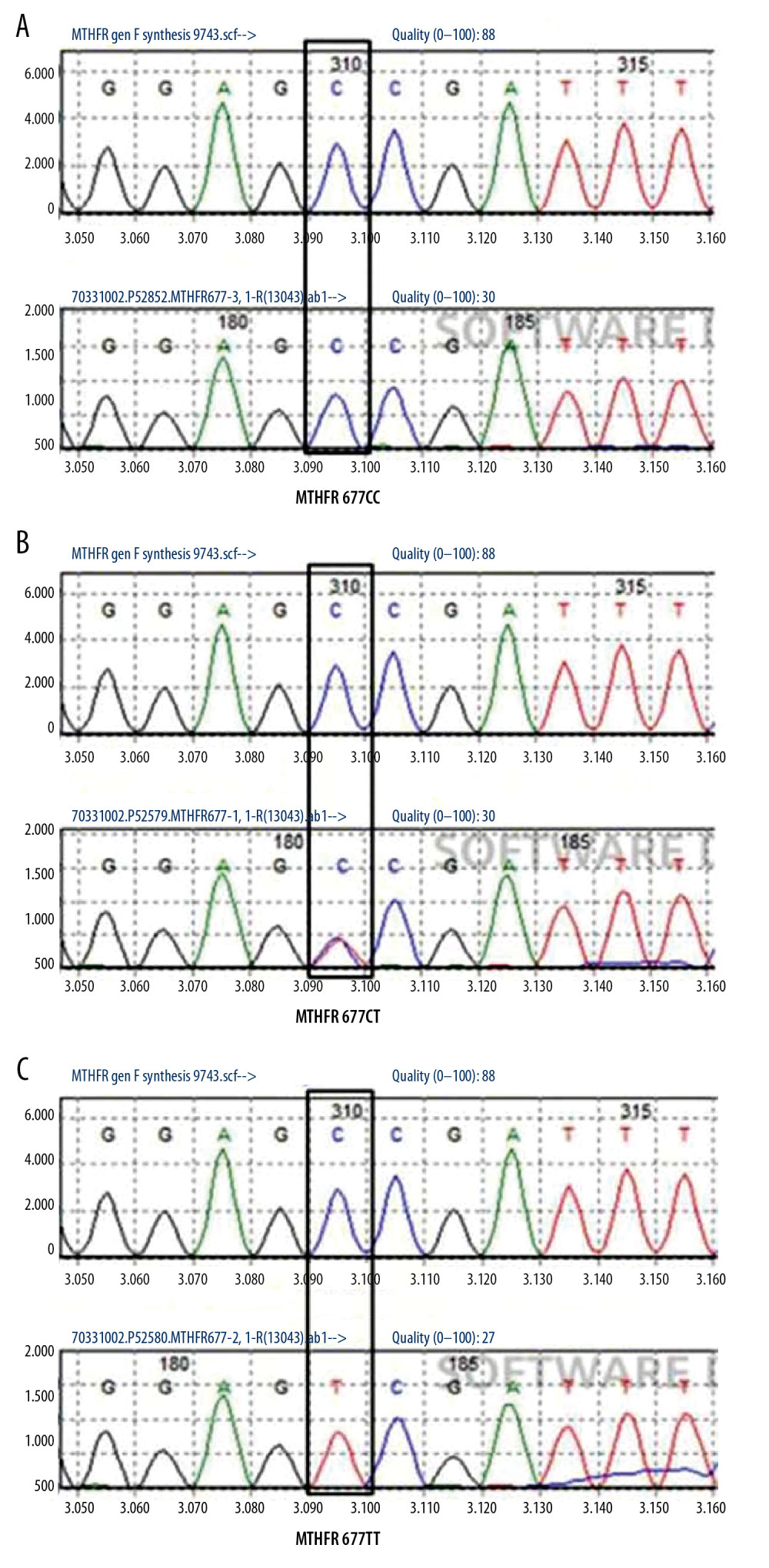
Three genotypes of the MTHFR gene were detected by Sanger sequencing: the wild type, CC genotype (Figure 1A); the heterozygous mutant, CT genotype (Figure 1B); and the homozygous mutant, TT genotype (Figure 1C). The gene distribution frequency of MTHFR gene C677T polymorphism was tested with the Hardy–Weinberg equilibrium and showed was consistent with genetic balance (P>0.05) (Table 2), suggesting that the selected samples were representative.
COMPARISON OF ALLELE FREQUENCIES AND GENOTYPE FREQUENCIES BETWEEN STUDY GROUPS:
The frequencies of three genotypes and allele frequencies of the C667 locus of the MTHFR gene were significantly different between the two groups (P<0.05). The frequency of the TT genotype and T allele in the patient group were significantly higher than in the control group (Table 3). In the patient group, 83 patients had stable carotid artery atherosclerotic plaques, and 127 patients had unstable carotid artery atherosclerotic plaques. The genotype frequencies and allele frequencies of the MTHFR gene C667 locus were compared between the two plaque types. The frequency of the TT and T alleles in unstable plaque group were significantly higher than those in stable plaque group (P<0.05) (Table 4).
LOGISTIC REGRESSION ANALYSIS OF RISK FACTORS FOR CAROTID ARTERY ATHEROSCLEROSIS:
The independent variables used were hypertension, TC, TG, HDL, and LDL to perform stepwise regression analysis to determine whether carotid artery atherosclerosis was a dependent variable. Hypertension and diabetes were not independent risk factors for carotid artery atherosclerosis (P>0.05), as shown by univariate analysis (Table 5). For 420 study participants, when carotid artery atherosclerosis was selected as the dependent variable, using atherosclerosis as a factor in the overall population, comparing atherosclerosis to non-atherosclerosis, age, gender, BMI, SBP, DBP, FPG, TG, TC, HDL-C, LDL-C, HbA1c, and the MTHFR gene C667T polymorphism were taken as independent variables. Logistic regression analysis of locus polymorphisms showed that SBP, TC, LDL-C, and the MTHFR gene C667T polymorphism were risk factors for carotid artery atherosclerosis (Table 6).
Discussion
Timely diagnosis and intervention for patients with carotid artery atherosclerosis have a positive clinical effect in the prevention of stroke and cardiovascular and cerebrovascular disease [18]. Carotid artery atherosclerosis is a vascular disease caused by a combination of genetic and acquired factors, including diet and lifestyle, hypertension, obesity, diabetes, and hyperlipidemia [19]. This study compared the clinical indicators of patients with carotid artery atherosclerosis and healthy control and showed that SBP, DBP, FPG, TC, LDL-C, HbA1c and the intimo-medial thickness were higher in the carotid artery atherosclerosis group than in the healthy control group, while HDL-C was lower than in the control group, which was consistent with previous studies [20]. However, there were no significant differences in body mass index (BMI) between the two groups in this study, which may be related to the selected population. All subjects in this study were generally older, with an average age of over 60 years.
Previous studies have shown that MTHFR is a key rate-limiting enzyme for homocysteine metabolism, and normal MTHFR activity can maintain normal metabolism of folic acid and homocysteine, maintaining its stable plasma concentration [21]. The C677T locus in the MTHFR gene occurs in the folate binding region, which increases the thermal instability of the MTHFR enzyme and reduces its enzymatic activity, resulting in abnormal homocysteine and folate metabolism [22]. Several studies have demonstrated the close association of folate metabolism in the pathogenesis of cardiovascular diseases with potential mechanisms include antioxidant actions, effects on cofactor availability, or direct interactions with the enzyme endothelial nitric oxide synthase (NOS) [23]. The MTHFR C677 locus gene polymorphism is closely related to the occurrence of several diseases [24,25]. McNulty et al. [26] showed that MTHFR 677C> T can increase the risk of hypertension by between 24% to 87%, and the authors showed that vitamin B2 supplementation had a better therapeutic effect on hypertensive patients with the MTHFR 677TT genotype. Ponomarenko et al. [27] showed that MTHFR C677T polymorphism was a new risk factor for atherosclerosis, in addition to traditional risk factors such as LDL-C, HDL-C, and smoking.
In 2015, a meta-analysis study by Zhu et al. identified an association of the MTHFR gene C677T polymorphism with ischemic stroke in the Chinese population [15]. Also, an association between plasma homocysteine and the C677T gene polymorphism and carotid intimal thickness in South Asian, Chinese, and European Canadians has been shown [16]. In the present study, the frequencies of the three genotypes and the allele frequencies of the C667 locus of MTHFR gene were significantly different between the patient group and the control group. The frequency of the TT genotype and T allele genotype in the carotid artery in the atherosclerosis group were significantly higher than in the control population. Comparing the genotype frequency and allele frequency of the MTHFR gene C667T locus in patients with stable plaque and unstable plaque, it was found that the frequency of TT genotype and T allele were significantly higher in patients with an unstable plaque than those in the stable plaque group. Further logistic regression analysis found that SBP increased the risk of carotid artery atherosclerosis by 3.514 times, suggesting that hypertension is an independent risk factor for carotid artery atherosclerosis, which is consistent with the literature [28]. TC and LDL-C are also risk factors for carotid artery atherosclerosis, and high levels of LDL can damage arterial endothelial cells, and lipid abnormalities make lipids easily deposited in blood vessels to form atheromatous plaques [29].
The findings from the present study showed that the C667T polymorphism of the MTHFR gene is closely related to the occurrence of carotid atherosclerosis, which can increase the risk of carotid artery atherosclerosis by 6.143 times, which is an independent risk factor for carotid artery atherosclerosis. High levels of homocysteine can damage endothelial cells, promote the proliferation of smooth muscle cells, and develop atherosclerosis, which may be because the MTHFR gene C667T polymorphism affects the pathogenesis of carotid atherosclerosis [30].
This study had several limitations. This study did not include an investigation into the molecular mechanisms involved in carotid atherosclerosis, and further investigation into how the C677T polymorphism of the MTHFR gene affects the carotid artery atherosclerotic plaque is required in the future. Also, this study included a small patient number from one center, which may have introduced bias into the study. Due to the limited number of patients enrolled, large cohort clinical studies are required to support the findings from this preliminary study.
Conclusions
This study aimed to investigate the association between the C677T polymorphism of the MTHFR gene in patients with confirmed carotid artery atherosclerosis. The findings showed that the C677T polymorphism of the MTHFR gene was expressed in patients with carotid artery atherosclerosis.
Tables
Table 1. Analysis of general data and biochemical indicators.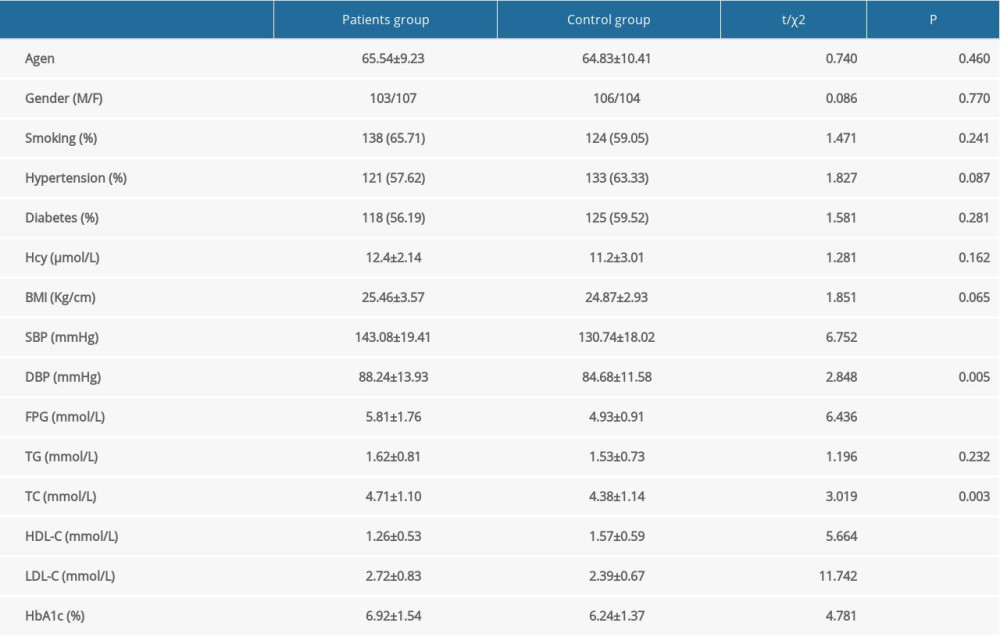 Table 2. Hardy-Weinberg equilibrium test for polymorphic loci.
Table 2. Hardy-Weinberg equilibrium test for polymorphic loci.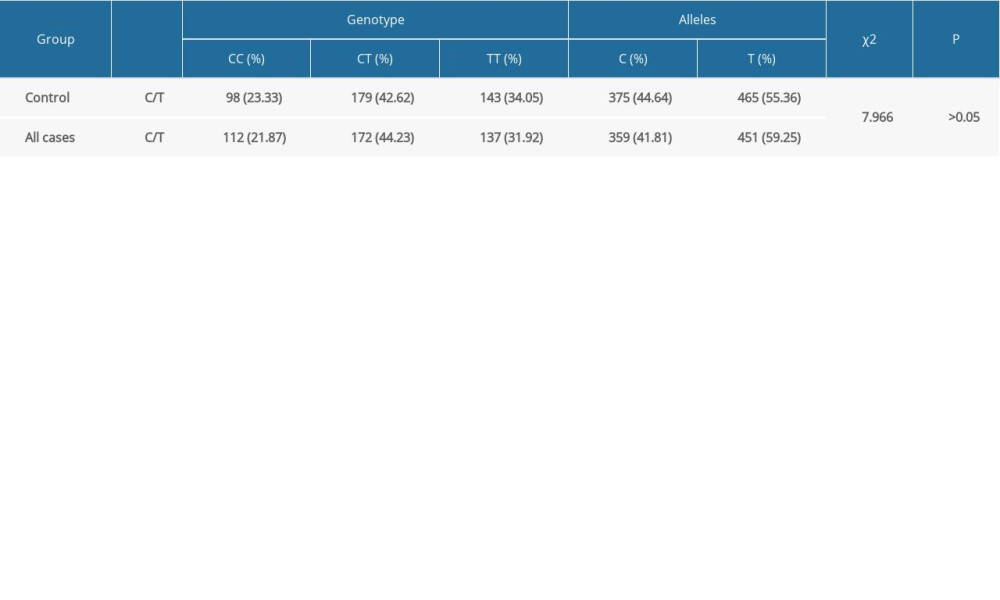 Table 3. Comparison of MTHFR C667 allele frequency and genotype frequency.
Table 3. Comparison of MTHFR C667 allele frequency and genotype frequency. Table 4. Comparison of MTHFR C667 allele frequency and genotype frequency.
Table 4. Comparison of MTHFR C667 allele frequency and genotype frequency.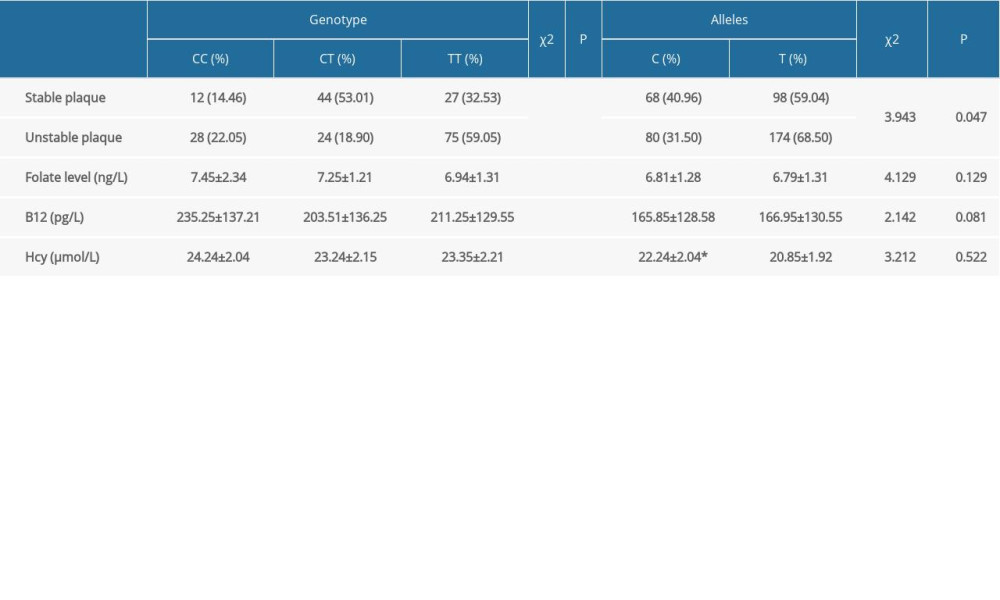 Table 5. Regression analysis of CAS risk factors.
Table 5. Regression analysis of CAS risk factors.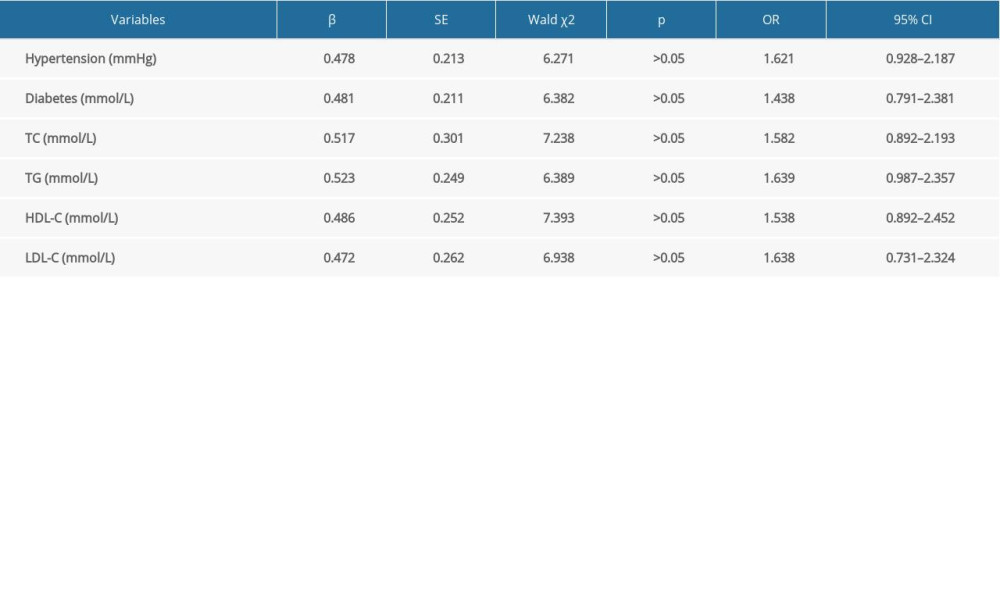 Table 6. Logistic regression analysis of risk factors for carotid atherosclerosis.
Table 6. Logistic regression analysis of risk factors for carotid atherosclerosis.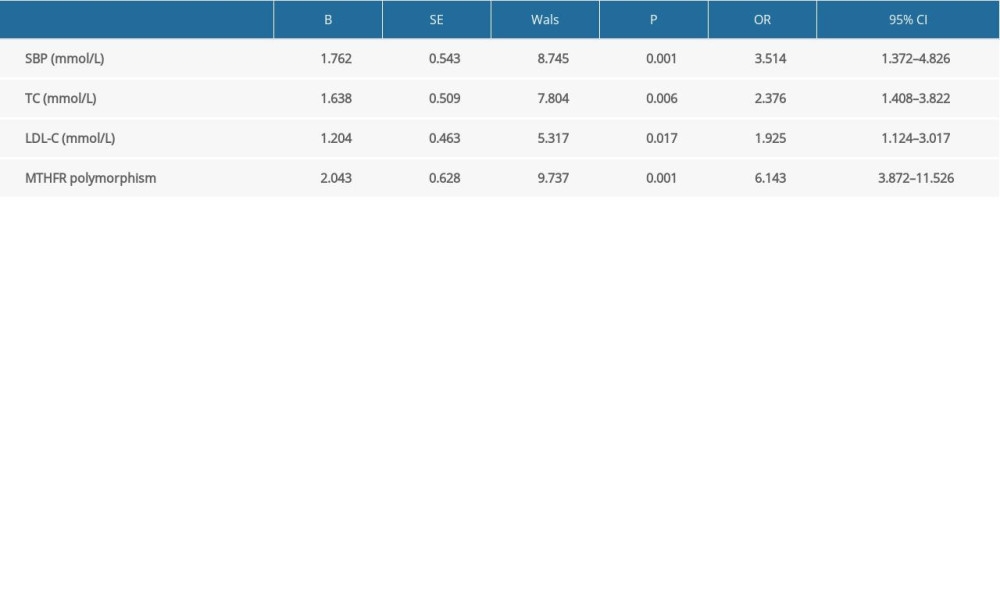
References
1. Jia H, Li H, Zhang Y, Association between red blood cell distribution width (RDW) and carotid artery atherosclerosis (CAS) in patients with primary ischemic stroke: Arch Gerontol Geriatr, 2015; 61(1); 72-75
2. Osawa K, Nakanishi R, McClelland RL, Ischemic stroke/transient ischemic attack events and carotid artery disease in the absence of or with minimal coronary artery calcification: Results from the Multi-Ethnic Study of Atherosclerosis: Atherosclerosis, 2018; 275; 22-27
3. Yahagi K, Kolodgie FD, Lutter C, Pathology of human coronary and carotid artery atherosclerosis and vascular calcification in diabetes mellitus: Arterioscler Thromb Vasc Biol, 2017; 37(2); 191-204
4. Bos D, Portegies ML, van der Lugt A, Intracranial carotid artery atherosclerosis and the risk of stroke in whites: The Rotterdam Study: JAMA Neurol, 2014; 71(4); 405-11
5. Finn C, Giambrone AE, Gialdini G, The association between carotid artery atherosclerosis and silent brain infarction: A systematic review and meta-analysis: J Stroke Cerebrovasc Dis, 2017; 26(7); 1594-601
6. Zhao D, Bi G, Feng J, Association of serum chemerin levels with acute ischemic stroke and carotid artery atherosclerosis in a Chinese population: Med Sci Monit, 2015; 21; 3121-28
7. Whayne TF, Prevention of carotid artery atherosclerosis: What is the evidence?: Angiology, 2017; 68(8); 661-68
8. Forgo B, Medda E, Hernyes A, Carotid artery atherosclerosis: A review on heritability and genetics: Twin Res Hum Genet, 2018; 21(5); 333-46
9. Hiraoka M, Kagawa Y, Genetic polymorphisms and folate status: Congenit Anom (Kyoto), 2017; 57(5); 142-49
10. Tang Z, Xiao L, Wang JQ, Zhang T, Analysis of metabolism-related indicators and MTHFR gene polymorphism in patients with H-type hypertension: Minerva Med, 2017; 108(2); 103-7
11. Reilly R, McNulty H, Pentieva K, MTHFR 677TT genotype and disease risk: Is there a modulating role for B-vitamins?: Proc Nutr Soc, 2014; 73(1); 47-56
12. Long S, Goldblatt J, MTHFR genetic testing: Controversy and clinical implications: Aust Fam Physician, 2016; 45(4); 237-40
13. Yang B, Fan S, Zhi X, Geographical and ethnic distribution of MTHFR gene polymorphisms and their associations with diseases among Chinese population: Clin Genet, 2017; 92(3); 243-58
14. Li ZH, Sun L, Zhang HY, Elevated plasma homocysteine was associated with hemorrhagic and ischemic stroke, but methylenetetrahydrofolate reductase gene C677T polymorphism was a risk factor for thrombotic stroke – A multicenter case-control study in China: Stroke, 2003; 34(9); 2085-90
15. Zhu XY, Hou RY, Pan XD, Association between the methylenetetrahydrofolate reductase (MTHFR) gene C677T polymorphism and ischemic stroke in the Chinese population: A meta-analysis: Int J Neurosci, 2015; 125(12); 885-94
16. Kelemen LE, Anand SS, Hegele RA, Associations of plasma homocysteine and the methylenetetrahydrofolate reductase C677T polymorphism with carotid intima media thickness among South Asian, Chinese and European Canadians: Atherosclerosis, 2004; 176(2); 361-70
17. Marcucci R, Sofi F, Fedi S, Thrombophilic risk factors in patients with severe carotid atherosclerosis: J Thromb Haemost, 2005; 3(3); 502-7
18. Madan SA, John F, Pyrsopoulos N, Pitchumoni CS, Nonalcoholic fatty liver disease and carotid artery atherosclerosis in children and adults: A meta-analysis: Eur J Gastroenterol Hepatol, 2015; 27(11); 1237-48
19. Clarke R, Du H, Kurmi Oand China Kadoorie Biobank Collaborative Group, Burden of carotid artery atherosclerosis in Chinese adults: Implications for future risk of cardiovascular diseases: Eur J Prev Cardiol, 2017; 24(6); 647-56
20. Skowronska M, Piorkowska A, Czlonkowska A, Differences in carotid artery atherosclerosis between men and women in the early phase after ischemic event: Neurol Neurochir Pol, 2018; 52(2); 162-67
21. Liew SC, Gupta ED, Methylenetetrahydrofolate reductase (MTHFR) C677T polymorphism: Epidemiology, metabolism and the associated diseases: Eur J Med Genet, 2015; 58(1); 1-10
22. Colson NJ, Naug HL, Nikbakht E, The impact of MTHFR 677 C/T genotypes on folate status markers: A meta-analysis of folic acid intervention studies: Eur J Nutr, 2017; 56(1); 247-60
23. Verhaar MC, Stroes E, Rabelink TJ, Folates and cardiovascular disease: Arterioscler Thromb Vasc Biol, 2002; 22(1); 6-13
24. Amare AT, Schubert KO, Klingler-Hoffmann M, The genetic overlap between mood disorders and cardiometabolic diseases: A systematic review of genome wide and candidate gene studies: Transl Psychiatry, 2017; 7(1); e1007
25. Shao W, Yuan Y, Li Y, Association between MTHFR C677T polymorphism and methotrexate treatment outcome in rheumatoid arthritis patients: A systematic review and meta-analysis: Genet Test Mol Biomarkers, 2017; 21(5); 275-85
26. McNulty H, Strain JJ, Hughes CF, Ward M, Riboflavin, MTHFR genotype and blood pressure: A personalized approach to prevention and treatment of hypertension: Mol Aspects Med, 2017; 53; 2-9
27. Ponomarenko IV, Sukmanova IAThrombosis risk factors and gene mutations in young age patients with acute coronary syndrome: Kardiologiia, 2019; 59(1S); 19-24 [in Russian]
28. Zhang Z, Fang X, Hua Y, Combined effect of hyperhomocysteinemia and hypertension on the presence of early carotid artery atherosclerosis: J Stroke Cerebrovasc Dis, 2016; 25(5); 1254-62
29. Zhang Q, Liu S, Liu Y, Achieving low density lipoprotein-cholesterol <70mg/dL may be associated with a trend of reduced progression of carotid artery atherosclerosis in ischemic stroke patients: J Neurol Sci, 2017; 378; 26-29
30. Pawlak K, Mysliwiec M, Pawlak D, Hyperhomocysteinemia and the presence of cardiovascular disease are associated with kynurenic acid levels and carotid atherosclerosis in patients undergoing continuous ambulatory peritoneal dialysis: Thromb Res, 2012; 129(6); 704-9
Tables
Table 1. Analysis of general data and biochemical indicators.Table 2. Hardy-Weinberg equilibrium test for polymorphic loci.Table 3. Comparison of MTHFR C667 allele frequency and genotype frequency.Table 4. Comparison of MTHFR C667 allele frequency and genotype frequency.Table 5. Regression analysis of CAS risk factors.Table 6. Logistic regression analysis of risk factors for carotid atherosclerosis.Table 1. Analysis of general data and biochemical indicators.Table 2. Hardy-Weinberg equilibrium test for polymorphic loci.Table 3. Comparison of MTHFR C667 allele frequency and genotype frequency.Table 4. Comparison of MTHFR C667 allele frequency and genotype frequency.Table 5. Regression analysis of CAS risk factors.Table 6. Logistic regression analysis of risk factors for carotid atherosclerosis. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387