18 October 2020: Clinical Research
Expression of Matrix Metalloproteinase-2, Matrix Metalloproteinase-9, Tissue Inhibitor of Metalloproteinase-1, and Changes in Alveolar Septa in Patients with Chronic Obstructive Pulmonary Disease
Yongxiang Zhang1ABCDE, Yuechuan Li1AEFG*, Zhen Ye1BD, Hui Ma1CFDOI: 10.12659/MSM.925278
Med Sci Monit 2020; 26:e925278






Abstract
BACKGROUND: This study investigated the relationship between the pathological alteration of alveolar septa and (1) pulmonary function and (2) matrix metalloproteinase (MMP)-2, MMP-9, and tissue inhibitor matrix metalloproteinase 1 (TIMP-1) expression in chronic obstructive pulmonary disease (COPD).
MATERIAL AND METHODS: Sixty patients with pulmonary disease were divided into control (n=20) and COPD (n=40) groups. Postoperative lung tissue specimens were examined. Hematoxylin and eosin and elastin van Gieson staining detected pathological alterations of pulmonary alveolar septa. Septa thickness was measured. MMP-2, MMP-9, and TIMP-1 expression levels were detected by immunohistochemical staining. Correlations were determined by Pearson analysis.
RESULTS: Forced expiratory volume in 1 s (FEV₁), forced vital capacity, FEV₁ percent predicted (FEV₁%pre), and diffusion capacity of carbon monoxide percent predicted (DLCO%pre) in COPD patients were significantly lower than in those of the control group (P<0.05). MMP-2, MMP-9, and TIMP-1 expression levels were significantly higher in the COPD group than in control, especially the severe group (P<0.05). Septa thickness was negatively correlated with FEV₁%pre (r=–0.335; P<0.05) and positively correlated with MMP-2 and TIMP-1 expression (P<0.05). Proportion of collagenous fiber was negatively correlated with FEV₁%pre and DLCO%pre (P<0.01), and positively correlated with MMP-2, MMP-9, and TIMP-1 expression (P<0.01). Proportion of elastic fibers was negatively correlated with collagenous fiber.
CONCLUSIONS: The pathological alteration of alveolar septa was correlated with pulmonary function and expression levels of MMP-2, MMP-9, and TIMP-1, which can play vital roles in COPD progression.
Keywords: Matrix Metalloproteinase 9, Pathological Conditions, Signs and Symptoms, Respiratory Function Tests, Gene Expression Regulation, Matrix Metalloproteinase 2, Pulmonary Alveoli, Pulmonary Disease, Chronic Obstructive, Tissue Inhibitor of Metalloproteinase-1
Background
Chronic obstructive pulmonary disease (COPD) is a common chronic illness marked by persistent respiratory symptoms and restricted airflow. It is caused by abnormalities of the airway or alveolar septa due to significant exposure to harmful particles or gases [1,2]. COPD is a complex disease that includes many clinical subtypes, such as the non-exacerbator phenotype, frequent exacerbator phenotype with emphysema, exacerbator phenotype with chronic bronchitis, and asthma-COPD overlap syndrome [3,4]. COPD severely affects human health and quality of life and ranks as the fourth leading cause of death worldwide [5]. Furthermore, COPD carries a significant financial burden worldwide [6]. In China, the prevalence of COPD among 40-year-olds is about 10% [7]. Therefore, it is important to study the pathogenesis and pathological changes of COPD to effectively prevent and treat the disease.
The expiratory movement during calm breathing is mainly produced by the relaxation of the diaphragm and external intercostal muscles and the elastic retraction of the lungs pulling the thoracic cage [8]. The increase of pulmonary volume in COPD patients is caused by the increase of expiratory resistance caused by airway lesions and an increase in residual air volume, while the decreased elastic retraction force of the lungs also has a very important role in the increase of pulmonary volume in patients with COPD [9]. The forced expiratory volume in 1 s percent predicted (FEV1%pre) and the carbon monoxide diffusing capacity percent predicted (DLCO%pre) are important indices of lung function, and the values of both FEV1%pre and DLCO%pre are decreased in patients with lung disease [10–12]. Previous studies on the pathological changes of COPD have primarily focused on the pathological changes of the airway, especially the small airway [13,14]. Studies have shown that vasculitis, vascular endothelium structural and functional changes, vascular remodeling, pulmonary lymphangiectasis, and an increase in the number of lobular lymphatic vessels are seen in the pulmonary interstitium of patients with COPD [15–17]. Bronchial angiogenesis and pulmonary vascular remodeling are increased, eventually leading to changes in bronchial and pulmonary circulation [18]. However, the mechanism of the pathological changes of pulmonary interstitial alveolar septa in patients with COPD has not been well characterized. Studies have found that the majority of patients with later-stage COPD have concomitant pulmonary interstitial fibrosis, aggravating the occurrence of persistent airway obstruction and ventilation disorders [19,20]. The alveolar walls are composed of a monolayer of squamous epithelium, including squamous epithelium (type I cells), secretory epithelium (type II cells), and septal cells. The alveolar septum, a structure between adjacent alveolar walls, consists of connective tissue and abundant capillaries. Because the alveolar septa are a significant part of the pulmonary interstitium, it is important to study their pathological changes in COPD to identify the pathological basis of the disease.
Matrix metalloproteinases (MMPs) are a set of enzymes which can degrade components of the extracellular matrix (ECM) [21]. MMP-2 and MMP-9 act on extracellular basement membrane turnover by preferentially degrading type IV collagen, a principal constituent of the basement membrane, thereby affecting the structural integrity of the pulmonary tissue [22,23]. Furthermore, a study showed that serum MMP-2, MMP-9, and MMP-12 levels were significantly increased in patients with COPD and positively correlated with disease severity [24]. Tissue inhibitor matrix metalloproteinase (TIMP) is a tissue depressor of MMPs and a particular depressor of MMP activity. Because MMPs play an important role in the pathogenesis and development of COPD, we further investigated the relationship between lung function and MMP-2, MMP-9, and TIMP-1 levels.
The aim of this study was to explore the relationship between pathological changes of alveolar septa in the pulmonary interstitium with pulmonary function and local expression levels of MMP-2, MMP-9, and TIMP-1 in patients with COPD.
Material and Methods
PATIENTS:
The study included 60 patients with pulmonary disease who were admitted to our hospital from May 2014 to December 2015 and underwent pulmonary lobectomy. All patients were carefully evaluated before surgery. Inclusion criteria were as follows: (1) pulmonary lesion ≤3 cm; (2) preoperative pulmonary function and chest high-resolution computed tomography (HRCT) examinations; (3) age between 50 and 70 years; and (4) Han ethnicity. Exclusion criteria were as follows: (1) history of bronchial asthma, pulmonary fibrosis, bronchiectasis, or tuberculosis; (2) history of connective tissue disease; (3) HRCT of the chest showed pulmonary interstitial lesions; and (4) incomplete clinical data.
The basic patient characteristics, including sex, age, and smoking history and smoking index, were collected. Smoking index=number of cigarettes smoked per day × years of smoking. Simultaneously, the preoperative pulmonary function measures (pulmonary function indicators after the dilation test) were collected, including FEV1/forced vital capacity (FVC), FEV1%pre, DLCO%pre, and pathological biopsy results. Ethics approval for the study was obtained from the Medical Ethics Committee of the Tianjin Chest Hospital. Written informed consent was collected from all participants in the study.
The patients were grouped according to preoperative pulmonary function as follows: the control group was defined as FEV1/FVC >70%; the COPD group was defined as FEV1/FVC <70%. According to the value of FEV1%pre, the COPD group was further divided into 3 groups: the mild COPD group was defined as FEV1%pre ≥80%; the moderate COPD group was defined as FEV1%pre 50–79%; and the severe COPD group was defined as FEV1%pre <50%. The flow diagram of patient enrollment is shown in Figure 1.
COLLECTION AND PREPARATION OF PATHOLOGICAL SPECIMENS:
The lung tissue samples analyzed in this study were postoperative lung tissue specimens of patients with lung tumors. Pathological specimens of patients after pulmonary lobectomy were collected by automatic microtome (Leica RM 2255, Leica Instruments, Nussloch, Germany). Specifically, for patients who met the inclusion and exclusion criteria, pathological specimens (10×5×5 mm) were excised from near the visceral pleura at a distance of >2 cm from the lesion. Specimens were dehydrated and embedded in paraffin wax and numbered. The thickness of the lung alveolar septa on light microscopy examination was measured by a stage micrometer measurement and image analysis software. Briefly, under a high-power microscope (10×40), 5 alveolar images were randomly selected from each specimen and the thicknesses of the alveolar septa was measured at 45° intervals (a total of 8 parts) with the center of each alveolar as the center. When a local measurement of one part was not possible, it was discarded and all other parts were used. The mean value of the alveolar septal thickness was then measured. The thickness of the specimens was 4 um, and 10 specimens were prepared for each sample. All specimens were prepared for hematoxylin and eosin (H&E) staining, elastin van Gieson (EVG) staining, and immunohistochemistry.
H&E STAINING:
An H&E staining kit (G1120, Solarbio, Beijing, China) was used to stain the tissue sections. The sections were deparaffinized in xylene twice (2–5 min each time), and rehydrated with successive washes in 100% ethanol for 1 min, 95% ethanol for 1 min, 95% ethanol for 2 min, 75% ethanol for 1 min, tap water for 2 min, and distilled water for 2 min. The tissue sections were then stained with hematoxylin for 5 min, rinsed with distilled water for 1 min, differentiated with 75% hydrochloric acid ethanol for 30 s, rinsed with 50°C tap water for 5 min, rinsed with distilled water for 5 min, then stained with eosin for 1–2 min, and rinsed again with distilled water. Furthermore, sections were dehydration with graded alcohol: 95% ethanol (2×1 min), 100% ethanol (2×1 min), and clearing in xylene (2×1 min). The mounted slides were then examined and photographed using an Olympus BX50 optical microscope (Olympus, Tokyo, Japan) with an ISCapture microscope imaging system (Tucsen Photonics). The staining intensity was analyzed by Image-Pro Plus 5.0 software and expressed as an integrated optical density value. Ten fields were randomly selected at 100× magnification for each section.
EVG STAINING:
The tissue sections were deparaffinized in xylene twice (2–5min each time), rehydrated, and then successively washed in 100% ethanol for 1 min, 95% ethanol for 1 min, 95% ethanol for 2 min, 75% ethanol for 1 min, tap water for 2 min, and distilled water for 2 min. The sections were then oxidized with potassium permanganate for 5 min, washed in distilled water, whitened with oxalic acid for 5 min, and washed in distilled water. Tissue sections were then stained with elastin for 8–24 h, and then differentiated with 95% ethanol. After washing thoroughly with tap and distilled water, van Gieson dye (Solarbio, Beijing, China) was used to stain for 1 min, and 95% ethanol was rapidly differentiated for 10 s. The sections were dehydrated with 95% ethanol (2×1 min), 100% ethanol (2×1 min), and cleared in xylene (2×1 min). The mounted slides were then examined and photographed using the Olympus BX50 microscope with the ISCapture microscope imaging system. Ten fields were randomly selected at 100× magnification for each section.
IMMUNOHISTOCHEMICAL STAINING:
The sections were deparaffinized and rehydrated, and washed with 0.01 M phosphate-buffered saline (PBS) (Servicebio, China) (3×5 min). The sections were then incubated with 0.3% methanol and hydrogen peroxide, incubated for 20 min at room temperature, and then washed with distilled water (3×5 min). The sections were incubated with 10% goat serum for 30 min at 37°C, the excess serum was absorbed by filter paper, and the primary monoclonal mouse antibodies to MMP-2 (Calbiochem-Novabiochem, Schwalbach, Germany; clone 42-5D11; dilution 1: 25), MMP-9 (Calbiochem-Novabiochem; clone 56-2A4; dilution 1: 50), TIMP-1(Calbiochem-Novabiochem; clone 10-2D1; dilution 1: 20) were added, then the sections were washed with 0.01 M PBS (3×5 min). The sections were then exposed to a secondary antibody, biotinylated goat anti-mouse antibody, and then to peroxidase conjugated streptavidin. Next, they were incubated with MMP-2, MMP-9, and TIMP-1 working solution for 30 min at 37°C, then sections were washed with 0.01 M PBS (3×5 min). The sections were next incubated with horseradish peroxidase to mark the working fluid for 30 min at 37°C, then the sections were washed with 0.01 M PBS (3×5 min) followed by diaminobenzidine (DAB) and hematoxylin staining. Next, the slides were examined and photographed using the Olympus BX50 optical microscope with the ISCapture microscope imaging system. The DAB staining was analyzed by Image-Pro Plus 5.0 software. Ten fields were randomly selected at 100× magnification for each section.
STATISTICS ANALYSIS:
SPSS 19.0 (SPSS, Inc, Chicago, IL, USA) statistical software was used for all data analyses, and measurement data were expressed as mean±standard deviation. The independent
Results
ANALYSIS OF CLINICAL CHARACTERISTICS:
A total of 60 patients who were admitted from May 2014 to December 2015, had pulmonary disease, and underwent pulmonary lobectomy were recruited into the study (Table 1). The patients were divided into 2 groups according to their levels of preoperative pulmonary function: the control group (n=20) and the COPD group (n=40). The control group had an average patient age of 58.05±9.33 years and included 18 patients with pulmonary cancer, 1 patient with pulmonary hamartoma, and 1 patient with teratoma. A total of 13/20 patients were men (65%). The COPD group had an average patient age of 60.50±4.30 years and included 37 patients with pulmonary cancer, 2 patients with pulmonary hamartoma, 1 patient with pulmonary lipoma, and 25 patients with emphysema. A total of 29/40 patients were men (72.5%). Patient sex, age, smoking history and smoking index and patient types in 2 groups showed no significant differences (P>0.05) between groups. Patients with pulmonary malignant tumor staging were type I. In addition, the exacerbation rate in 1 year and the Global Initiative for Obstructive Lung Disease (GOLD) groups of the patients with COPD are shown in Table 2.
COMPARISON OF PULMONARY FUNCTION:
Differences in pulmonary function in the control and COPD groups were analyzed (Table 3). According to the FEV1%pre value, the COPD group was further divided into a mild COPD group (n=8), a moderate COPD group (n= 24), and a severe COPD group (n=8). FEV1, FVC, FEV1/FVC, FEV1%pre, and DLCO%pre of patients in the COPD group were was all significantly lower compared to those in patients without COPD (t=−11.83, P<0.01; t=−2.67, P<0.01; t=−14.84, P<0.01; t=−2.29, P=0.03, respectively), and were decreased with the decrease in COPD severity. In particular, the severe group showed the lowest FEV1%pre (45.25±3.71) and DLCO%pre (61.51±12.83), which were significantly lower in the severe group than in the mild and moderate COPD groups and the control group (P<0.01).
PATHOLOGICAL ANALYSIS OF ALVEOLAR SEPTA:
The results of H&E and EVG staining showed disordered internal fibers and increased alveolar rupture in the COPD group in comparison with those of the control group (Figure 2). The alveolar septa thickness and the proportion of collagen fibers were significantly higher in the COPD group (t=2.29, P=0.03; t=2.54, P=0.01, respectively), while the proportion of elastic fibers and elasticity/collagen were significantly lower (t=−2.49, P=0.02; t=−3.70, P<0.01, respectively) (Table 4). Notably, in the severe group, the thickness and the proportion of collagen fibers were markedly higher (P<0.01), while the proportion of elastic fibers and elasticity/collagen were significantly lower compared to those of the control, mild, and moderate groups (P<0.05). Taken together, these results indicated that the pathological change in the pulmonary interstitium disease state developed progressively with the development of COPD disease, which was associated with the severe rupture of alveolar septa.
RELATIONSHIP BETWEEN PATHOLOGICAL CHANGES OF ALVEOLAR SEPTA AND PULMONARY FUNCTION:
As shown in Table 5, the relationship between the pathological changes of the alveolar septa and lung function was analyzed. Pearson correlation analysis revealed a significant negative relationship between collagenous fiber and FEV1 (r=−0.360; P=0.005) and FEV1/FVC (r=−0.267; P = 0.046). A significant positive relationship between FEV1/FVC and elastic fibers proportion (r=0.373; P=0.003) was observed. Significant negative relationships between FEV1%pre and alveolar septa thickness and collagen fibers (r=−0.335; P=0.035; r=−0.472, P=0.002, respectively) and a significant positive relationship between FEV1%pre and elastic fiber proportion (r=0.316, P=0.047) were observed. The change in fibers could have affected the ventilatory capacity of patients with COPD. Meanwhile, DLCO%pre showed a significant negative relationship between lung function and collagen fibers (r=−0.329, P=0.010) and a significant positive relationship with elastic fiber proportion (r=0.316, P=0.014). These results revealed that pathological changes of pulmonary interstitial alveolar septa were correlated with lung function changes in patients with COPD. This pathological change could have a negative effect on pulmonary function.
THE EXPRESSION LEVEL OF MMP-2, MMP-9, AND TIMP-1 IN PATIENTS WITH COPD:
The expression levels of MMP-2, MMP-9, and TIMP-1 in alveolar septa collagen fibers and elastic fibers in the COPD group were significantly higher than those in the control group (Figure 3, Table 6, t=7.97, P<0.01; t=6.33; P<0.01; t=2.74, P<0.01, respectively). The expression levels of MMP-2, MMP-9, and TIMP-1 in alveolar septa were significantly increased with the progression of COPD, and were the highest in the patients with severe COPD (P<0.05). However, the values of MMP-9/TIMP-1 and MMP-2/TIMP-1 were significantly lower in the severe COPD group (P<0.05). This indicated that the change of alveolar septa could lead to the expression of MMP-2, MMP-9, and TIMP-1 in alveolar septa, and MMP-2, MMP-9, and TIMP-1 played vital roles in the pulmonary interstitial metabolism of the COPD pathogenesis.
RELATIONSHIP BETWEEN PATHOLOGICAL CHANGES OF ALVEOLAR SEPTA AND EXPRESSION OF MMP-2, MMP-9, AND TIMP-1:
As shown in Table 7, the results of the correlation analysis showed that the thickness of alveolar septa was positively correlated with the expression levels of MMP-2 and TIMP-1 (r=0.289, P=0.025; r=0.417, P=0.001, respectively) and negatively correlated with the ratio of MMP-9/TIMP-1 (r=−0.302, P=0.019). The proportion of collagenous fiber was positively correlated with the expression levels of MMP-2, MMP-9, and TIMP-1 (r=0.353, P=0.006; r=0.386, P=0.002; r=0.563, P=0.001, respectively). Moreover, negative correlations were observed between the proportion of elastic fibers and the expression of MMP-2, MMP-9, and TIMP-1 (r=−0.271, P=0.037; r=−0.268, P=0.038; r=−0.295, P=0.022, respectively). The pathological changes of the pulmonary interstitial alveolar septa were related to MMP-2, MMP-9, and TIMP-1 in patients with COPD.
Discussion
COPD is a class of airway inflammatory diseases, and smoking is its most commonly recognized risk factor [6]. COPD is a highly endemic and heterogeneous disease with high morbidity and mortality, placing a heavy burden on health care providers worldwide. Treatment options that confer a mortality benefit to the patient are rare. Research on the pathogenesis and pathological changes of COPD is crucial to explore the effective prevention and treatment of the disease. However, to date, the pathogenesis of COPD is still not clear. In the present study, we investigated the relationship between the pathological alterations of the alveolar septa and lung function, and the levels of MMP-2, MMP-9, and TIMP-1 in patients with COPD.
In the present study, sex, age, and smoking index did not differ significantly in the 2 groups. The DLCO%pre and FEV1%pre values of the COPD group were significantly lower than that of the control group, and the severe COPD group showed markedly lower levels than in the mild and moderate COPD groups. Our results indicated that the pulmonary diffusion function in patients with COPD was lower, which is in agreement with a previous study [25]. Studies have demonstrated that patients present with a decrease in DLCO when alveolar septa and alveolar capillaries are damaged [26,27]. Furthermore, the decrease of DLCO in patients with COPD in the present study revealed that the patients’ alveolar septa may have changed. Also, alveolar septa rupture was increased in the COPD group in the present study. The reason might be that, with the restriction of airflow, the alveoli expand significantly, then the alveoli and alveolar septa rupture [28,29].
The fibrous components of the pulmonary interstitium include primarily elastic fibers and collagen fibers, which together form the elastic resistance of the lungs [30]. When the lungs expand, these fibers stretch and tend to retract. Collagen fibers are tough and can resist a pulling force. Elastic fibers give the lungs good elasticity, and the destruction of pulmonary elastic fibers leads to a decrease in the elastic retraction of the lungs. In the present study, we found that the alveolar septa were significantly thicker in patients with COPD, especially those with severe COPD. At the same time, pulmonary alveolar rupture occurred in patients with COPD. The reason may be that in patients with COPD, especially in those who have emphysema, the bronchial lumen dilates when inhaling, the air enters the alveoli, and the pulmonary cavity shrinks when exhaling. The air then remains, and the pressure in the alveoli increases continuously, leading to rupture of the alveolar walls. Furthermore, the alveolar septum thickens, elastic fibers decrease, and the alveolar walls are prone to rupture.
We further investigated the relationship between lung function and pathological changes. With the increase of alveolar septa thickness, the DLCO%pre and FEV1%pre levels were decreased, and FEV1%pre was decreased significantly. The reason can be that the alveolar septum is the nodular tissue between adjacent alveoli, which contains a capillary network, and the thickening of the alveolar septum will inevitably lead to an increase in the gas diffusion distance and reduce the pulmonary function of patients with COPD [31,32]. Furthermore, collagen fibers were increased in patients with COPD, and collagen fibers in the severe COPD group were significantly increased compared with that of the mild and moderate groups. Similarly, the DLCO%pre and FEV1%pre levels decreased with the increase of collagen fibers. A reason for this may be that the proportion of collagen fibers increased and the proportion of elastic fibers decreased, resulting in the decrease of pulmonary compliance and pulmonary elastic retraction [33,34]. The alteration of collagen fibers and elastic fibers raises the possibility of a remodeling process occurring in the connective matrix in alveolar walls, and connective tissue changes are part of the pathological events in emphysema [35]. Ultimately, airflow limitation in patients with COPD is more obvious, indicating that this pathological change in the alveolar septa may be a pathogenic mechanism in these patients. Similarly, the amount of collagen fibers in alveolar septa was increased in a model of COPD [36].
MMPs have been considered as latent therapeutic targets in a variety of pathological conditions involving abnormal MMP expression and activity [37]. The deposition of ECM has a crucial role in the development process of pulmonary fibrosis. However, ECM is primarily resolved by MMPs, and the conversion efficiency of MMPs is adjusted mainly by TIMPs [38]. It has been shown that the imbalance between MMPs and TIMPs can be an important mechanism in pulmonary fibrosis [39]. Meanwhile, the levels of MMPs and TIMPs were shown to be revised in pulmonary fibrosis [40,41]. Li et al. discovered that the expression and activity of MMPs, especially MMP-2 and MMP-9, were significantly increased in pulmonary tissues after injury [42]. MMP-9 and TIMP-1 expression can serve not only as the indicator to determine the pathological classification, metastasis, and prognosis of carcinoma, but can also help the targeted gene therapy of carcinoma [43,44]. In the present study, expressions levels of MMP-2 and MMP-9 were also significantly higher in patients with COPD. Also, the expression level of TIMP1 was notably increased in patients with COPD, while the values of MMP-2/TIMP-1 and MMP-9/TIMP-1 were increased, in particular the value of MMP-9/TIMP-1. Furthermore, the expression levels of MMP-2, MMP-9, and TIMP-1 in the alveolar septa were significantly higher in the severe COPD group, while the values of MMP-9/TIMP-1 and MMP-2/TIMP-1 were significantly lower in the severe COPD group. Smoking decreases the MMP-9/TIMP-1 ratio [45]. Mohamed et al. found that MMP-9 and TIMP-1 play important roles in the pathophysiology of asthma exacerbation and airway remodeling [46]. Uysal et al. found that MMP-9 concentration and the MMP-9/TIMP-1 ratio are the best predictors of emphysema in patients with COPD [47]. Overall, the results of that experiment are the same as those reported in an earlier study [42]. Yang et al. found the expression levels of MMP-2, MMP-9, and TIMP-1 were significantly upregulated in the pulmonary tissue of rats with pulmonary fibrosis [38]. Similarly, in the present study, we found that collagenous fiber and elastic fibers were correlated with the expression levels of MMP-2, MMP-9, and TIMP-1 in patients with COPD. We also found that pulmonary interstitial alveolar septa thickness was positively correlated with the expression of MMP-2 and TIMP-1 in patients with COPD. The enhanced expression of MMP can lead to increased degradation of EMC in the pulmonary interstitium and the destruction of broncho-lung structure. While inhibiting the activity of MMPS, TIMP promotes the increase of collagen synthesis and fibroblast proliferation, and the alveolar septum also thickens during the formation of pulmonary interstitial fibrosis.
The study has the following limitations: (1) the number of cases was small; (2) there are many pathogenic factors and influencing factors that cause COPD; (3) the use of drugs in patients was not considered; and (4) because of the more obvious lung changes in patients with severe COPD, no such patients were included in the study owing to poor lung function. Further studies are needed to assess the influence of these factors on FEV1 and DLCO.
Conclusions
In the present study, there were significant pathologic changes in the alveolar septa of patients with COPD. Alveolar septa rupture, alveolar septa thickness, and collagen fibers were significantly increased, and elastic fibers and elasticity/collagen were significantly decreased, especially in patients with severe COPD (
Figures
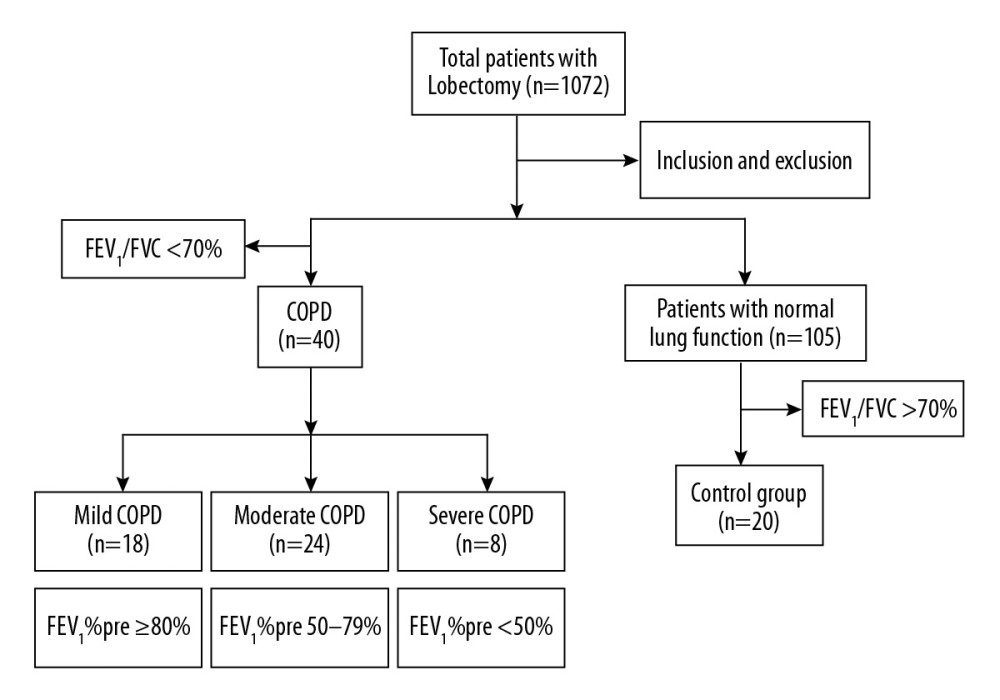 Figure 1. Flow diagram of patient enrollment.
Figure 1. Flow diagram of patient enrollment. 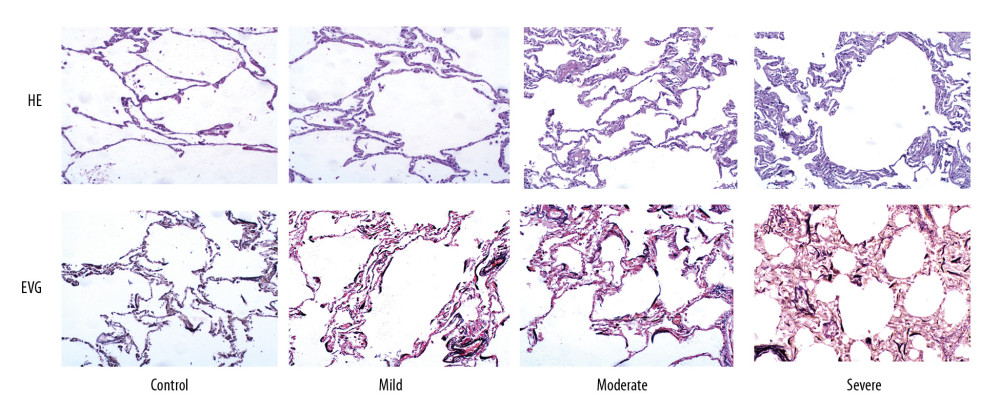 Figure 2. Comparison of alveolar septa thickness and fiber morphology (H&E, ×100 magnification; EVG, ×100 magnification).
Figure 2. Comparison of alveolar septa thickness and fiber morphology (H&E, ×100 magnification; EVG, ×100 magnification). 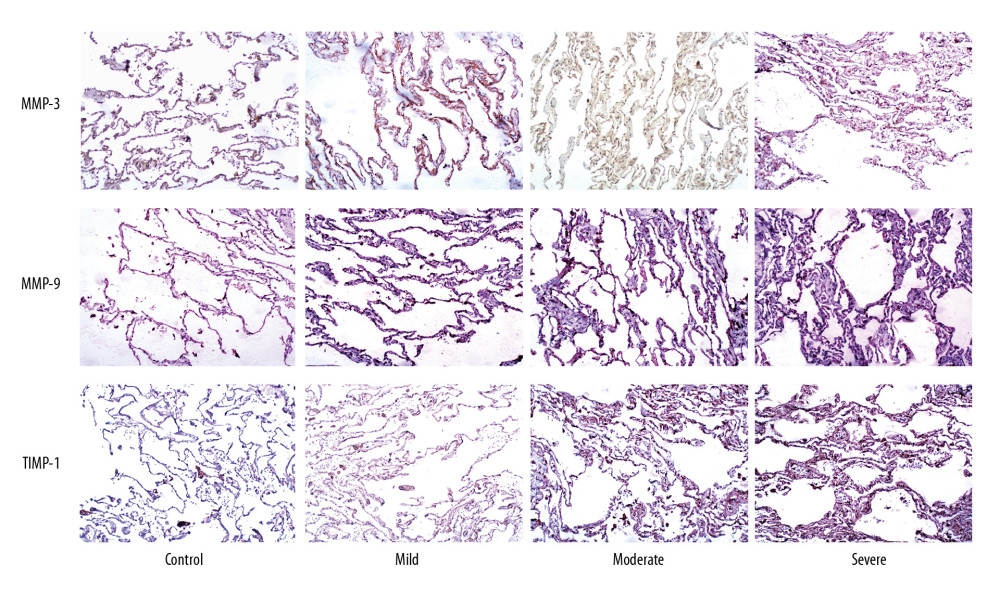 Figure 3. Immunohistochemical analysis of the expression of matrix metalloproteinase (MMP)-2, MMP-9, and tissue inhibitor of metalloproteinase (TIMP)-1 in alveolar septa (×100 magnification).
Figure 3. Immunohistochemical analysis of the expression of matrix metalloproteinase (MMP)-2, MMP-9, and tissue inhibitor of metalloproteinase (TIMP)-1 in alveolar septa (×100 magnification). Tables
Table 1. Analysis of general information of patients.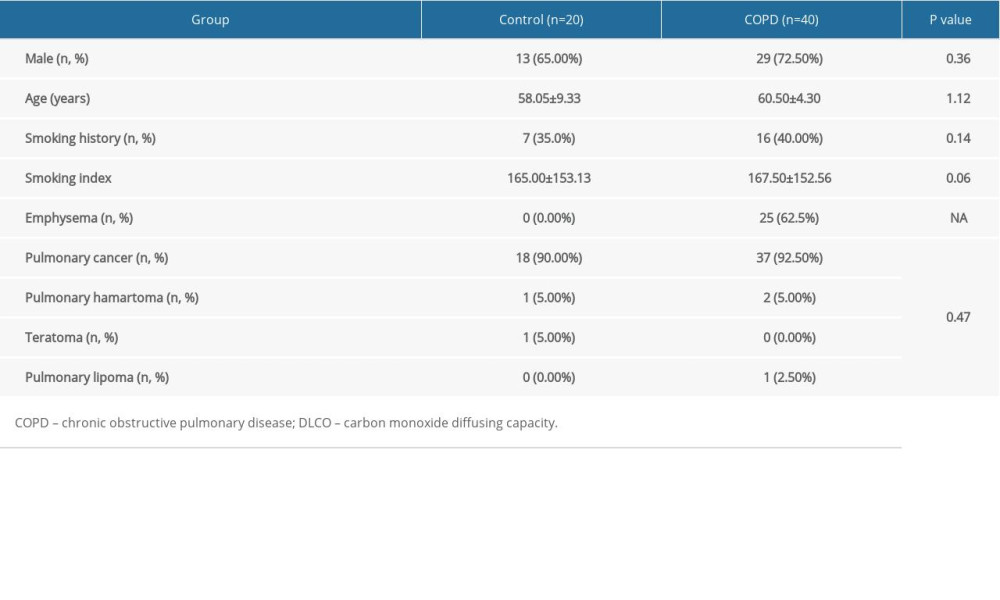 Table 2. The exacerbation rate in 1 year and GOLD groups in the patients with COPD.
Table 2. The exacerbation rate in 1 year and GOLD groups in the patients with COPD. Table 3. Comparison of pulmonary function between COPD group and control group.
Table 3. Comparison of pulmonary function between COPD group and control group.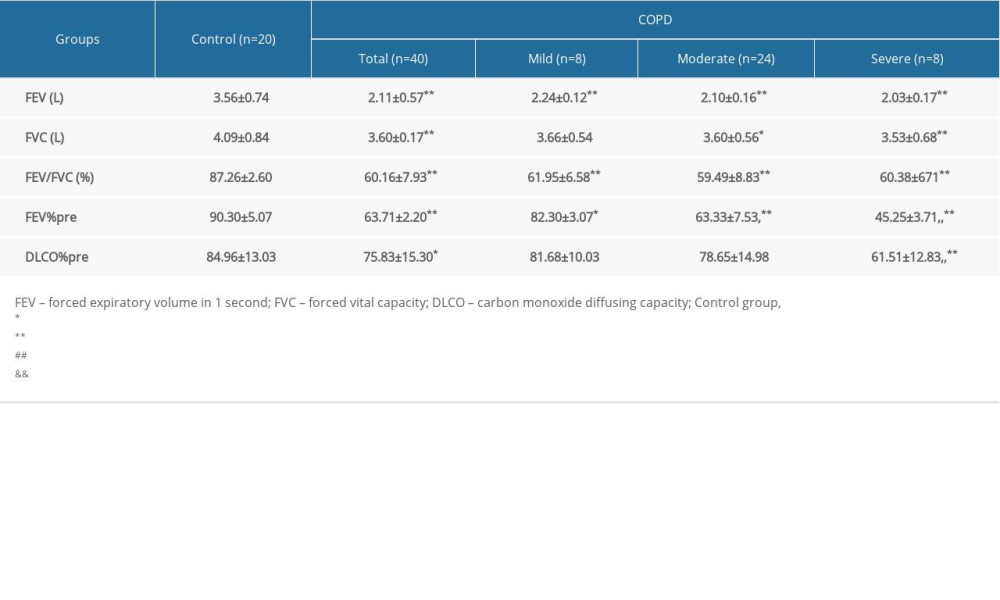 Table 4. Comparison of alveolar septum thickness and fiber ratio between COPD group and control group.
Table 4. Comparison of alveolar septum thickness and fiber ratio between COPD group and control group.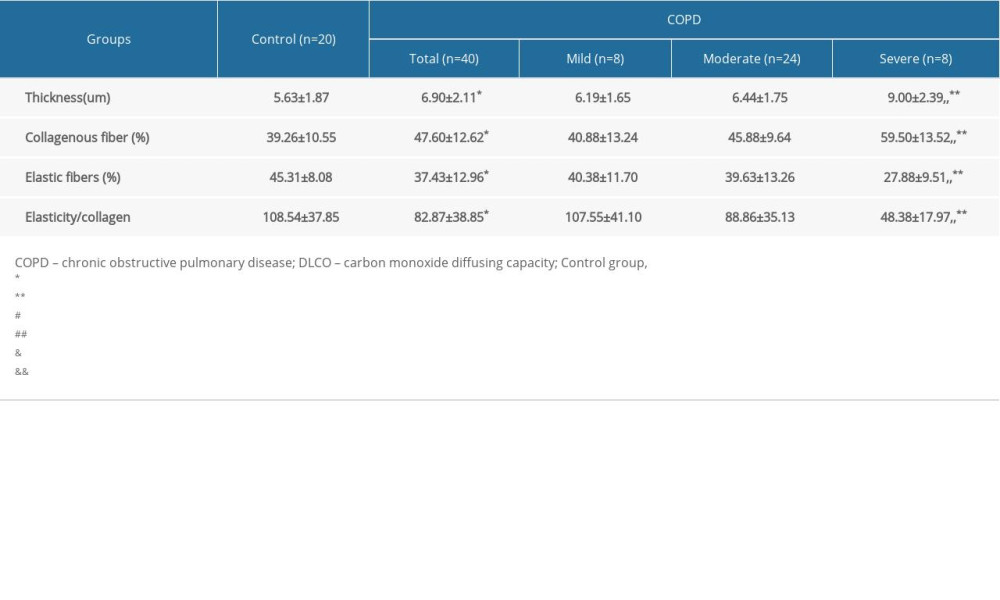 Table 5. Correlation between alveolar septum thickness and fiber composition ratio and lung function.
Table 5. Correlation between alveolar septum thickness and fiber composition ratio and lung function.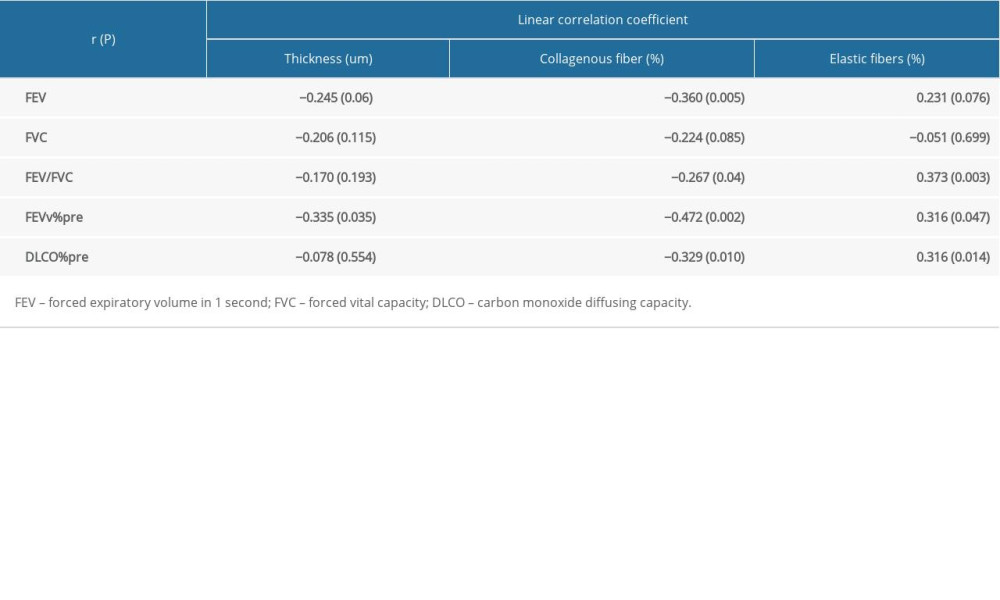 Table 6. Comparison of expression of MMP-2, MMP-9 and TIMP-1 in alveolar septa between COPD group and control group.
Table 6. Comparison of expression of MMP-2, MMP-9 and TIMP-1 in alveolar septa between COPD group and control group.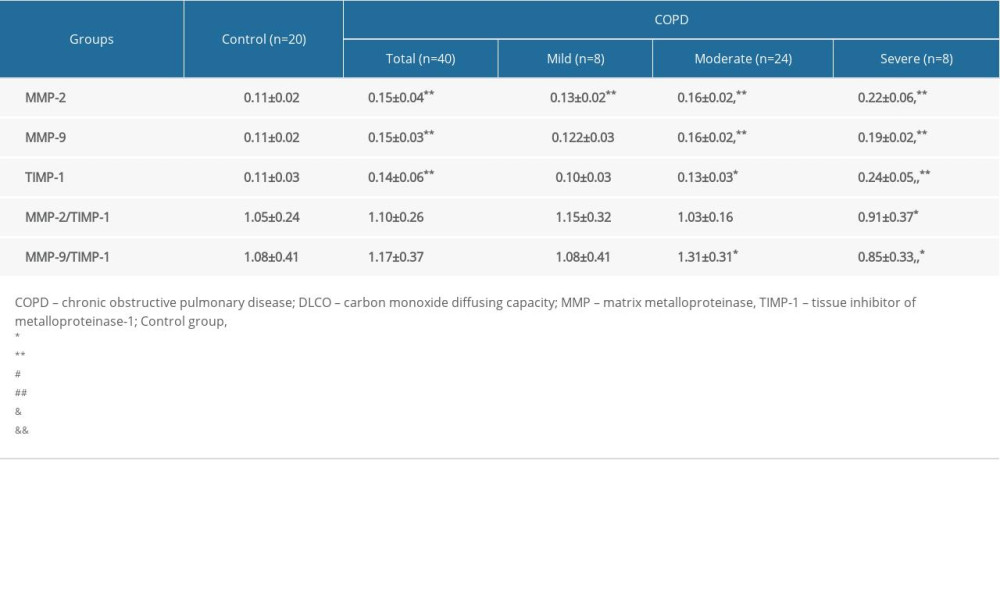 Table 7. Correlation between alveolar septum thickness and fiber composition ratio and the expression of MMP-2, MMP-9, and TIMP-1.
Table 7. Correlation between alveolar septum thickness and fiber composition ratio and the expression of MMP-2, MMP-9, and TIMP-1.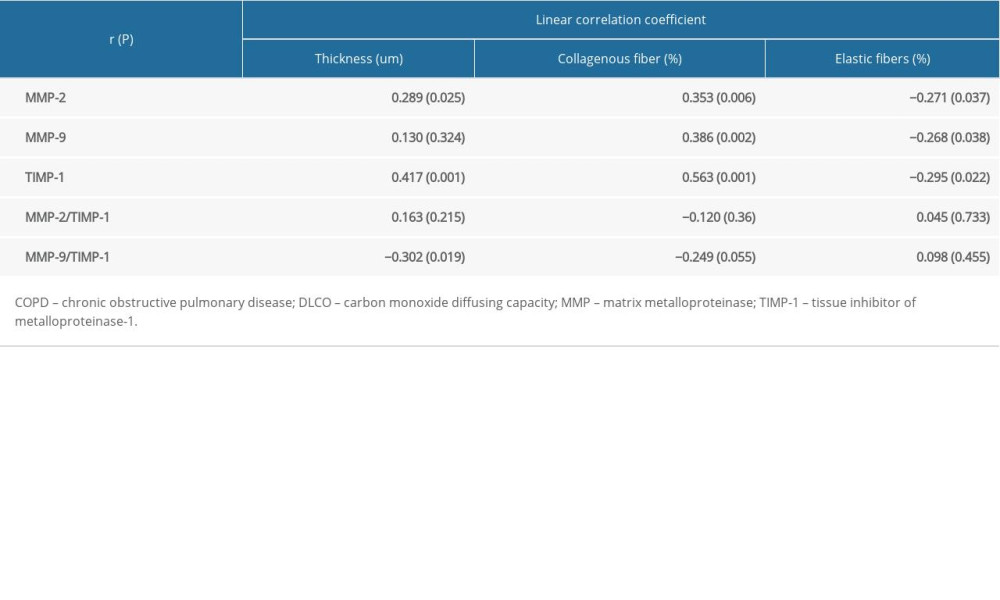
References
1. Kokturk N, Gurgun A, Sen E, The view of the Turkish Thoracic Society on the report of the GOLD 2017 global strategy for the diagnosis, management, and prevention of COPD: Turk Thorac J, 2017; 18; 57-64
2. Qaseem A, Wilt TJ, Weinberger SE, Diagnosis and management of stable chronic obstructive pulmonary disease: A clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society: Ann Intern Med, 2011; 155; 179-91
3. Singh D, Agusti A, Anzueto A, Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: The GOLD Science Committee Report 2019: Eur Respir J, 2019; 53; 1900164
4. Myriam CR, Ricard C, Marc M, Identification and distribution of COPD phenotypes in clinical practice according to Spanish COPD Guidelines: The FENEPOC study: Int J Chron Obstruct Pulmon Dis, 2017; 12; 2373-83
5. Lozano R, Naghavi M, Foreman K, Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010: Lancet, 2012; 380; 2095-128
6. Duffy SP, Criner GJ, Chronic obstructive pulmonary disease: Evaluation and management: Med Clin North Am, 2019; 103; 453-61
7. Bao HL, Wang LH, Prevalence of chronic obstructive pulmonary disease among community population aged ≥4 0 in China: A meta-analysis on studies published between 1990 and 2014: Chin J Epidemiol, 2016; 37; 119-24
8. Ramos E, Vanderlei L, Ramos D, Influence of pursed-lip breathing on heart rate variability and cardiorespiratory parameters in subjects with chronic obstructive pulmonary disease (COPD): Braz J Phys Ther, 2009; 13; 288-93
9. Zeng S, Zhang A, Vasudevan S, Changes in lung volumes across GOLD stages of COPD: Implications for mechanisms of air trapping: Ann Am Thorac Soc, 2019; A5780
10. Schubert J, Kruavit A, Mehra S, Prevalence and nature of lung function abnormalities among Indigenous Australians referred to specialist respiratory outreach clinics in the Northern Territory: Intern Med J, 2019; 49; 217-24
11. Attanasi M, Lucantoni M, Rapino D, Lung function in children with juvenile idiopathic arthritis: A cross-sectional analysis: Pediat Pulm, 2019; 54; 1242-49
12. van Dijk M, Hartman JE, Klooster K, Endobronchial valve treatment in emphysema patients with a very low DLCO: Respiration, 2020; 99; 163-70
13. Sun C, Zhu M, Yang Z, LL-37 secreted by epithelium promotes fibroblast collagen production: A potential mechanism of small airway remodeling in chronic obstructive pulmonary disease: Lab Invest, 2014; 94; 991-1002
14. MacNee W, Pathogenesis of chronic obstructive pulmonary disease: Proc Am Thorac Soc, 2005; 2; 258-66 discussion 290–91
15. Maclay JD, McAllister DA, Mills NL, Vascular dysfunction in chronic obstructive pulmonary disease: Am J Respir Crit Care Med, 2009; 180; 513-20
16. Cottin V, Nunes H, Brillet PY, Combined pulmonary fibrosis and emphysema: A distinct underrecognised entity: Eur Respir J, 2005; 26; 586-93
17. Ley-Zaporozhan J, van Beek EJ, Imaging phenotypes of chronic obstructive pulmonary disease: J Magn Reson Imaging, 2010; 32; 1340-52
18. Harkness LM, Kanabar V, Sharma HS, Pulmonary vascular changes in asthma and COPD: Pulm Pharmacol Ther, 2014; 29; 144-55
19. Guan S, Xu W, Han F, Ginsenoside Rg1 attenuates cigarette smoke-induced pulmonary epithelial-mesenchymal transition via inhibition of the TGF-β1/Smad pathway: Biomed Res Int, 2017; 2017 7171404
20. Gargani L, Interstitial syndrome: Thoracic Ultrasound, 2018; 79; 75
21. Gharib SA, Manicone AM, Parks WC, Matrix metalloproteinases in emphysema: Matrix Biol, 2018; 73; 34-51
22. Kim JY, Choeng HC, Ahn C, Early and late changes of MMP-2 and MMP-9 in bleomycin-induced pulmonary fibrosis: Yonsei Med J, 2009; 50; 68-77
23. Tan RJ, Fattman CL, Niehouse LM, Matrix metalloproteinases promote inflammation and fibrosis in asbestos-induced lung injury in mice: Am J Respir Cell Mol Biol, 2006; 35; 289-97
24. Hardavella G, Tzortzaki EG, Siozopoulou V, Lymphangiogenesis in COPD: Another link in the pathogenesis of the disease: Respir Med, 2012; 106; 687-93
25. Krishnan JK, Martinez FJ, Lung function trajectories and chronic obstructive pulmonary disease: Current understanding and knowledge gaps: Curr Opin Pulm Med, 2018; 24; 124-29
26. Velasco-Torres Y, Ruiz V, Montano M, Participation of the miR-22-HDAC4-DLCO axis in patients with COPD by tobacco and biomass: Biomolecules, 2019; 9; 837-45
27. Kobayashi H, Otsuki Y, Yamaguchi M, An autopsy case of pulmonary capillary hemangiomatosis with an electron microscopy study: Am J Case Rep, 2019; 20; 1551-57
28. Li Y, Xiong S, Xiong WEffects of IL-4 on cyclooxygenase-2 and platelet-derived growth factor in the lungs of COPD rats: J Nanjing Med Univ, 2007; 21; 169-74 [in Chinese]
29. Wang Y, Kayoumu A, Lu G, Experimental models in Syrian golden hamster replicate human acute pancreatitis: Sci Rep, 2016; 6; 28014
30. Ochs M, O’Brodovich H, The structural and physiologic basis of respiratory disease: Kendig’s Disorders of the Respiratory Tract in Children, 2019; 63; 100.e2
31. Gómez Correa GA, Osorno Serna J, Cáceres Acosta MF, Nodular pulmonary amyloidosis: A manifestation of Sjögren’s syndrome: Case Rep Pulmonol, 2018; 2018 9745935
32. Zhang N, Gao P, Yin B: PLoS One, 2019; 14; e0215408
33. Oliveira MV, Silva PL, Rocco PRM, Extracellular matrix components remodeling and lung function parameters in experimental emphysema and allergic asthma: Differences among the mouse strains: Drug Discov Today Dis Models, 2019; 52; 1-8
34. Kling KM, Lopez-Rodriguez E, Pfarrer C, Aging exacerbates acute lung injury induced changes of the air-blood barrier, lung function and inflammation in the mouse: Am J Physiol Lung Cell Moll Physiol, 2017; 312; L1-12
35. Vlahovic G, Russell ML, Mercer RR, Cellular and connective tissue changes in alveolar septal walls in emphysema: Am J Resp Crit Care, 1999; 160; 2086-92
36. De Oliveira MV, Rocha NN, Santos RS, Endotoxin-induced emphysema exacerbation: a novel model of COPD exacerbations causing cardiopulmonary impairment and diaphragm dysfunction: Front Physiol, 2019; 10; 664
37. Deb N, Mallick S, Jaiswal A, Role of MMPs and oxidants in lung diseases: Oxidative stress in lung diseases, 2019; 149-69
38. Yang L, Chen P-p, Luo M, Inhibitory effects of total ginsenoside on bleomycin-induced pulmonary fibrosis in mice: Biomed Pharmacother, 2019; 114; 108851
39. Craig VJ, Zhang L, Hagood JS, Matrix metalloproteinases as therapeutic targets for idiopathic pulmonary fibrosis: Am J Respir Cell Mol Biol, 2015; 53; 585-600
40. Yoshimura S, Nishimura Y, Nishiuma T, Overexpression of nitric oxide synthase by the endothelium attenuates bleomycin-induced lung fibrosis and impairs MMP-9/TIMP-1 balance: Respirology, 2006; 11; 546-56
41. Jin X, Dai H, Ding K, Rapamycin attenuates bleomycin-induced pulmonary fibrosis in rats and the expression of metalloproteinase-9 and tissue inhibitors of metalloproteinase-1 in lung tissue: Chin Med J (Engl), 2014; 127; 1304-9
42. Li X, Ma D, Zha X, Ilomastat, a synthetic inhibitor of MMPs, prevents lung injury induced by gamma-ray irradiation in mice: Oncotarget, 2017; 8; 60789-808
43. Iniesta P, Morán A, De Juan C, Biological and clinical significance of MMP-2, MMP-9, TIMP-1 and TIMP-2 in non-small cell lung cancer: Oncol Rep, 2007; 17; 217-23
44. Ozek E, Ozcan D, Celik SE, Matrix metalloprotease-9 expresssion in meningioma: correlation with growth fraction and role of gender. A pilot immunohistochemical study: Clin Neurol Neurosurg, 2018; 172; 169-73
45. Watson A, Benton AS, Rose MC: J Invest Med, 2010; 58; 725-29
46. Mohamed GM, Farres MN, Mahmoud HR, Interplay between matrix metalloproteinase-9 and tissue inhibitor of matrix metalloproteinase-1 in acute asthma exacerbation and airway remodeling: Egypt J Chest Dis Tuberc, 2012; 61; 35-39
47. Uysal P, Uzun H, Relationship between circulating Serpina3g, matrix Metalloproteinase-9, and tissue inhibitor of Metalloproteinase-1 and -2 with chronic obstructive pulmonary disease severity: Biomolecules, 2019; 9; 62-73
Figures
Figure 1. Flow diagram of patient enrollment.Figure 2. Comparison of alveolar septa thickness and fiber morphology (H&E, ×100 magnification; EVG, ×100 magnification).Figure 3. Immunohistochemical analysis of the expression of matrix metalloproteinase (MMP)-2, MMP-9, and tissue inhibitor of metalloproteinase (TIMP)-1 in alveolar septa (×100 magnification). Tables
Table 1. Analysis of general information of patients.Table 2. The exacerbation rate in 1 year and GOLD groups in the patients with COPD.Table 3. Comparison of pulmonary function between COPD group and control group.Table 4. Comparison of alveolar septum thickness and fiber ratio between COPD group and control group.Table 5. Correlation between alveolar septum thickness and fiber composition ratio and lung function.Table 6. Comparison of expression of MMP-2, MMP-9 and TIMP-1 in alveolar septa between COPD group and control group.Table 7. Correlation between alveolar septum thickness and fiber composition ratio and the expression of MMP-2, MMP-9, and TIMP-1.Table 1. Analysis of general information of patients.Table 2. The exacerbation rate in 1 year and GOLD groups in the patients with COPD.Table 3. Comparison of pulmonary function between COPD group and control group.Table 4. Comparison of alveolar septum thickness and fiber ratio between COPD group and control group.Table 5. Correlation between alveolar septum thickness and fiber composition ratio and lung function.Table 6. Comparison of expression of MMP-2, MMP-9 and TIMP-1 in alveolar septa between COPD group and control group.Table 7. Correlation between alveolar septum thickness and fiber composition ratio and the expression of MMP-2, MMP-9, and TIMP-1. In Press
Clinical Research
Body Weight and Insulin Resistance Indicators Among ChildrenMed Sci Monit In Press; DOI: 10.12659/MSM.951434
Clinical Research
Comparison of Radiographic Cervical Sagittal Alignment Parameters in Patients With Nonspecific Neck Pain, D...Med Sci Monit In Press; DOI: 10.12659/MSM.952950
Clinical Research
Combined Fibrinogen and Urinary α1-Microglobulin as Predictors of Respiratory Tract Infection in Children w...Med Sci Monit In Press; DOI: 10.12659/MSM.951066
Database Analysis
Evaluation of Salivary Total Oxidant Status (TOS) and Total Antioxidant Status (TAS) in Orthodontic Patient...Med Sci Monit In Press; DOI: 10.12659/MSM.952052
Most Viewed Current Articles
17 Jan 2024 : Review article 14,175,576
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,756,620
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,465,966
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,651
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387