11 September 2020: Clinical Research
Carcinoid Tumorlets Co-Existing with Chronic Pulmonary Inflammatory Processes: Imaging Findings and Histological Appearances
Jun Wang123EF, Shuai Ren134EFG, Yongkang Liu13BD, Kai Guo13DF, Xiao Chen13BC, Zhongqiu Wang13AG*, Rong Chen4DEDOI: 10.12659/MSM.926014
Med Sci Monit 2020; 26:e926014






Abstract
BACKGROUND: Pulmonary carcinoid tumorlets (PCT) are incidental histologic or radiologic discoveries that are localized neuroendocrine tumors whose proliferation is associated with chronic pulmonary inflammatory processes. This study assessed the imaging findings and histological appearances of PCT co-existing with chronic pulmonary inflammatory processes.
MATERIAL AND METHODS: We performed a retrospective study of 14 patients with incidentally-found PCT with co-existing chronic pulmonary inflammatory processes who underwent preoperative X-rays and CT between 1 January 2003 and 31 December 2012. The clinical symptoms, X-rays, CT imaging findings, and histological appearances were retrospectively evaluated.
RESULTS: Twelve women and 2 men were found to have PCT, with a mean age of 55.29±13.90 years (range 25–74 years) at diagnosis. Among these 14 patients, hemoptysis, cough, chest pain, expectoration, and chest tightness were found in 9 (64.3%), 5 (35.7%), 4 (28.6%), 3 (21.4%), and 1, respectively. For most patients, we could not find any small nodules on the X-ray or CT images. However, indirect imaging findings of bronchiectasis (85.7%, 12/14), atelectasis (57.1%, 8/14), inflammation (92.8%, 13/14), tuberculosis (7.1%, 1/14), and lung cancer (7.1%, 1/14) were found in all 14 patients.
CONCLUSIONS: PCT occurs most commonly in middle-aged women who have chronic pulmonary inflammatory processes such as bronchiectasis, atelectasis, and inflammation. Although there are no specific symptoms or direct imaging findings in these patients, our results showed that patients who have bronchiectasis, atelectasis, or recurrent pulmonary infection are at increased risk for PCT.
Keywords: Clinical Medicine, Lung Diseases, Pathology, Radiology, Tomography Scanners, X-Ray Computed, Carcinoid Tumor, Tomography, X-Ray Computed
Background
Pulmonary carcinoid tumorlet (PCT) is a rare incidental finding in histopathological examination, which appears to be always associated with other underlying chronic respiratory conditions, such as bronchiectasis and fibrosis [1–5]. PCT is benign in its biological behavior, being a tiny peripheral carcinoid (usually ≤5 mm) that differs mainly in size from carcinoid tumors (>5 mm) [1,5]. PCT develops from hyperplastic neuroendocrine cells originating from the bronchial and bronchiolar mucosa, which are also called Kulchitsky cells [2]. The histological and immunohistochemical features of PCT are similar to those of carcinoids [1,6], but with no obvious carcinoid syndrome. Cough and shortness of breath can occur in PCT patients; however, there are no specific symptoms. Notably, PCT is commonly associated with chronic pulmonary inflammatory processes, including fibrosis and bronchiectasis. It was suggested that hyperplastic neuroendocrine cells can secret neuropeptides, which can elicit a peribronchiolar fibrotic reaction contributing to chronic fibrotic lung disease [2].
The symptoms associated with PCT are insufficient to make a diagnosis of PCT. However, PCT is commonly associated with fibrosis and bronchiectasis, which can be diagnosed on computed tomography (CT) images. With increasing awareness of PCT, it is also occasionally concurrently found and diagnosed on CT images in cases of chronic pulmonary inflammatory processes. Ginsberg et al. [2] reported that most PCTs can be detected on CT when they were large enough to be mentioned in pathology reports. However, 90% of patients had a diagnosis of cancer in their study. Some case reports also demonstrated CT imaging findings of incidentally-detected PCT [1,6,7]. Lung biopsies are sometimes recommended and used in patients with multiple tumorlets when clinical manifestations failed to indicate a primary tumor [8]. Preoperative diagnosis of PCT is very important for choosing the optimal treatment and for prognosis prediction, and it can help relieve patient stress and discomfort. However, to the best of our knowledge, no other radiologic study has reported the histological appearance and associated imaging findings of chronic inflammatory process or bronchiectasis in patients with PCT.
In this study we investigated the histological appearance and associated imaging findings in patients with PCT.
Material and Methods
PATIENTS:
Patient data confidentiality was protected in accordance with the principles of the Declaration of Helsinki. The protocol was approved by our Institutional Review Board. Written informed consent was waived because this was a retrospective study. We retrospectively collected and analyzed the clinical data, CT images, and histopathological data from 14 patients diagnosed with PCT from 1 January 2003 to 31 December 2012. PCT was proved through lung surgery or biopsy, which was necessary due to symptoms such as dyspnea, recurrent lung infections, and severe bleeding caused by a chronic inflammatory process or recurrent bronchiectasis. PCT was incidentally detected during histopathological examination of the surgical or biopsy sample. Age, sex, clinical symptoms, tumor location, imaging findings, and histopathological information were recorded and analyzed.
CT TECHNIQUES:
A Philips Brilliance 64 scanner was used in CT examinations. The CT scanning parameters were: tube voltage, 120 KVp; tube current, 100–400 mA; helical pitch, 1.375: 1; section thickness, 3.0 mm; gantry rotation time, 0.5 s. The images were reconstructed with a 1.0-mm section thickness and 1.0-mm increments. All CT scans were performed within 30 days of when the resection or biopsy was performed. Of these 14 patients, 4 also underwent 3-phase contrast-enhanced CT scanning (arterial, portal venous, and delayed phases). Following unenhanced imaging, non-ionic contrast media Ultravist 300 (Bayer Schering Pharma AG, Berlin, Germany) was administrated intravenously (1.2–1.5 ml/kg) at a rate of 3.0 ml/s, followed by administration of 40 ml saline solution, using a power injector (Ulrich Medical, Ulm, Germany). Arterial, portal venous, and delayed phase scans were obtained at 30 s, 60 s, and 120 s.
HISTOLOGICAL AND IMMUNOCHEMICAL ASSAY:
The resected lung tissues were fixed in 10% neutral buffered formalin for 24 h. Then, the specimens were embedded in paraffin and sliced for hematoxylin and eosin (HE) staining (4-μm-thick for each sections). Immunohistochemistry was performed to confirm the presence of PCT by a board-certified pathologist with 15 years of experience. A comprehensive immunohistochemical analysis of synaptophysin (Syn), chromogranin A (CgA), thyroid transcription factor-1 (TTF-1), CD56, and neuron-specific enolase (NSE) was conducted. The presence of bronchiectasis, tuberculosis, atelectasis, chronic bronchiolitis, organizing pneumonia, and cancer was noted.
IMAGING ANALYSIS:
All X-ray and CT images were independently reviewed by 2 experienced thoracic radiologists. Disparities in image analysis were resolved by discussion with a senior radiologist with 12 years of experience in chest CT reading until consensus was reached. For CT images, each scan was reviewed at lung window settings on a dedicated picture archiving and communication system (PACS) workstation. The following imaging features were evaluated: the number of nodules, tumor location, size, edge, presence of calcification, and presence of other chronic pulmonary inflammatory processes, such as bronchiectasis, tuberculosis, and atelectasis. The tumor margin was defined as well-defined (a smooth and clearly visible margin) or ill-defined (spiculation or infiltration on >90° of tumor perimeter) [9]. Calcification was identified on an unenhanced mediastinal window.
STATISTICAL ANALYSIS:
Categorical variables are presented as the number of cases (percentage). Quantitative variables are presented as mean±SD. Kappa analysis was performed to measure the degree of agreement between the 2 readers: κ ≤0.2 indicates slight agreement; 0.2< κ ≤0.4 indicates fair agreement, 0.4< κ ≤0.6 indicates moderate agreement, 0.6< κ ≤0.8 indicates substantial agreement, and κ >0.8 indicates excellent agreement. Statistical analysis was performed using SPSS version 19.0 (IBM Corp., IBM SPSS Statistics for Windows).
Results
CLINICAL FEATURES:
Patient characteristics are listed in Table 1. Among the 14 subjects with PCT, the mean age at diagnosis was 55.29±13.90 years (range 25–74 years). Most of the patients were more than 50 years old (10/14, 71.4%). PCT was more common in women (86%, 12/14). Hemoptysis, cough, chest pain, expectoration, and chest tightness were found in 9 (64.3%), 5 (35.7%), 4 (28.6%), 3 (21.4%), and 1 out of 14 patients, respectively.
IMAGING FINDINGS AND DIAGNOSIS:
We found it was difficult to observe the small tumorlets nodules directly on X-ray or CT images. Imaging findings and diagnoses are shown in Table 2. For most patients, we could not find any small nodules on the X-ray or CT images. However, indirect imaging findings, such as dilated and beaded bronchi or a massive patchy shadow or multiple small patchy shadows, were found in 13 patients (Figures 1–3). Bronchiectasis was found in 12 patients (85.7%), atelectasis was found in 8 patients (57.1%), inflammation or organizing pneumonia was found in 13 patients (92.9%), and calcification was found in 3 patients. The Kappa values for those qualitative variables were >0.80.
Finally, 12 patients (85.7%) were diagnosed as having bronchiectasis with inflammation, 1 patient (7.1%) was diagnosed with lung cancer, and 1 patient (7.1%) was diagnosed with pulmonary tuberculosis (Figure 3). None of the patients were correctly diagnosed as having PCT; therefore, the rate of missed diagnosis from imaging findings was 100%.
HISTOLOGICAL FINDINGS:
Pathological diagnoses and immunochemical findings in patients with PCT are listed in Table 3. Histological sections showed that tumorlets filled the air spaces in the bronchi. Tumorlets consisted of uniform populations of cells with oval or spindle nuclei (Figures 1C, 2F, 3E). Tumor cells were arranged in nests and had stippled chromatin. Cellular atypia, mitoses, and necrosis were absent. For the 12 patients with bronchiectasis, dilated bronchi were also observed in tissue sections.
Immunochemical staining showed that neuroendocrine markers, such as CgA (Figure 1D), Syn (Figure 1E), CD56 (Figure 1F), and NSE (Figure 1G), were highly expressed in the tumorlets. CgA, Syn, CD56, and NSE were positive in 100% of patients and TTF-1 was positive in 77.8% (7/9) of patients.
Discussion
PCT is extremely rare and is usually an incidental finding in lung biopsy or at histopathological examination [1]. Although CT can detect tumorlets in some cancer patients [2], it is difficult to find the nodules in other patients who have bronchiectasis or chronic inflammations. This report shows that PCT is commonly associated with chronic pulmonary inflammatory processes such as fibrosis and bronchiectasis that can be diagnosed on computed tomography (CT) images. In addition, PCT was more commonly observed in middle-aged women in our study.
PCT develops from neuroendocrine cells (known as Kulchitsky cells), which are commonly present as single cells or small clusters in the bronchial and bronchiolar epithelium [10]. It has been reported that diffuse idiopathic pulmonary neuroendocrine cell hyperplasia (DIPNECH), carcinoid tumorlet, and typical carcinoid form a distinct subset of neuroendocrine tumors with distinct morphologic, immunochemical, and molecular features [1]. For DIPNECH, the proliferation of single, cluster, or linear arrays of neuroendocrine cells are confined within the basement membrane of respiratory epithelia [11,12]. DIPNECH is frequently associated with tumorlets and/or peripheral carcinoid tumors and is considered to be a precursor to pulmonary carcinoid tumorlets [13–15]. Carcinoid tumorlets are distinguished from DIPNECH by extension beyond the basement membrane of the epithelia, with a size of 5 mm or less [1,11,12,15]. The tumor can be diagnosed as an atypical carcinoid if the size is larger than 5 mm. Size is the only criterion with which to discriminate PCT from typical carcinoid tumors [1]. Aubry et al. [8] reported that neuroendocrine cell hyperplasia was not found in tumorlets or peripheral carcinoid tumors, which suggests that neuroendocrine cell hyperplasia is not an obligate precursor lesion. Very little is known about the molecular mechanism of PCT, and genetic alterations may be involved in its progression. Finkelstein et al. [16] reported that Int-2 allelic imbalance is involved in carcinoid tumor formation.
Clinical symptoms and imaging findings are insufficient to make a correct preoperative diagnosis of PCT, especially in patients with chronic pulmonary inflammatory processes such as bronchiectasis, tuberculosis, and atelectasis. Histological and immunochemical examinations are the criterion standard for diagnosis of PCT in clinical practice. PCT consists of a relatively uniform population cells with oval or spindle nuclei, which are present as clusters or small nests [1]. As the cells lack mitoses and cellular atypia, PCT usually lacks necrosis [17]. In comprehensive immunohistochemical analysis, CgA, Syn, NSE, and CD56 are regarded as neuroendocrine biomarkers of PCT [1,14]. In the present study, CgA, Syn, NSE, and CD56 were strongly positive in tumorlets.
PCT is usually an incidental finding and can occur at any age. However, most PCT patients are elderly and most are women [2,8,18]. Our results in the present study are consistent with these earlier reports. It is unclear why this disease occurs predominantly in women. In addition, it has been reported that PCT has no obvious correlation with smoking. Regarding clinical symptoms, there are no specific signs indicating PCT. Chronic cough, dyspnea, and hemoptysis can occur in PCT patients [8]. Normal or only mildly abnormal obstruction occurs in PCT patients [8]. However, hemoptysis, cough, and chest pain were frequently observed in PCT patients in the present study, and these clinical symptoms may be related to the accompanying bronchiectasis, fibrosis, and tuberculosis. Moreover, lymph node metastases and Cushing’s syndrome, which were reported in PCT patients earlier [8], were not noted in the patients in our study.
Interestingly, PCT is always associated with chronic pulmonary inflammatory processes such as bronchiectasis, fibrosis, chronic abscess, and tuberculosis [1,5]. A chronic pulmonary inflammatory process was found to be indicative of PCT in our study, which is consistent with previous reports [1,5], but the association between chronic lung disease and PCT is not completely understood. An earlier study reported that lung inflammatory progress, microstructure damage, and fibrosis can lead to hypoxia, which can induce the proliferation of neuroendocrine cells present in the airways [18]. On the contrary, we postulated that PCT can lead to fibrotic lung disease by secreting neuropeptides that can elicit a peribronchiolar fibrotic reaction [2,19,20]. This is because some case reports have demonstrated that PCT can also be found in pulmonary sequestration [7]. In the present study, 12 of 14 PCT patients had bronchiectasis and inflammation, 8 of 14 patients had atelectasis, and 1 patient also had tuberculosis, and these results are consistent with previous reports [1,5]. Several studies proved that vascular endothelial growth factor (VEGF) is expressed in tumorlets, resulting in pulmonary fibrosis due to profibrotic growth factors secreted by tumorlets [1,2,20,21].
Few radiologic studies have reported PCT findings from chest radiographs or CT appearance. Ginsberg et al. [2] showed CT imaging of PCT in 35 patients (31 were cancer patients) who underwent pulmonary resection. Round or oval lung nodules were observed in 33 patients on CT images by radiologists, and CT did not reveal any nodules in the remaining 2 patients due to diffused fibrosis or small size. Aubry et al. [8] showed that multiple or solitary nodules could be found in PCT patients based on CT images, but without specific CT imaging findings. In our study, no nodules were found in PCT patients on CT images, with the exception of 1 patient who had a history of lung cancer. Most of our PCT patients had obvious bronchiectasis and chronic inflammation. As a result, the indirect imaging findings of massive patchy shadow or multiple small patchy shadows were found in 13 patients. For those patients, chest radiographs and CT images could not reveal the typical tumorlet nodules. PCT can be obscured by local inflammation. Therefore, it is hard to observe the small nodules in these patients, which consequently results in a high rate of missed diagnoses. It was difficult to estimate the prevalence of tumorlets because the 14 patients in this study had pathologically documented tumorlets. Our study showed that patients who had bronchiectasis, chronic inflammation, or tuberculosis are more likely to have PCT, which may help radiologists diagnose this under-recognized condition.
The main limitation of our study is the relatively small number of enrolled patients. The main purpose in writing this paper was to increase the awareness that patients with recurrent bronchiectasis or chronic inflammation may also have PCT. A multi-center study including more PCT patients is needed to confirm our findings.
Conclusions
PCT occurs most commonly in middle-aged women who have chronic lung diseases such as bronchiectasis or inflammation. Our results show that patients with bronchiectasis, atelectasis, chronic inflammation, or tuberculosis are more likely to have PCT. This information may be useful for radiologists to consider in the differential diagnosis of PCT when they encounter recurrent chronic pulmonary inflammation or multiple tumorlets in clinical practice and could help make an accurate preoperative diagnosis.
Figures
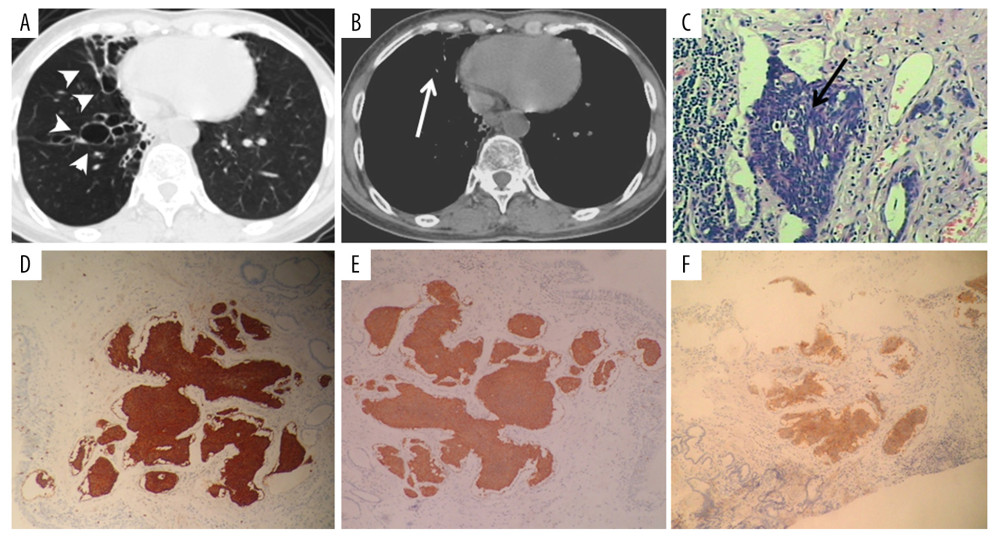 Figure 1. A 61-year-old woman with PCT and bronchiectasis. Dilated, beaded bronchi and cysts with defined borders can be observed in the lung window CT image (A, white arrowheads). Cord-like shadows can be observed in the mediastinal window (B, white arrows). PCT was evidenced by histopathological examination (C, black arrow). Tumorlets consisted of a comparatively uniform population of cells with oval or spindle nuclei. Mitoses were absent. Immunochemical staining revealed that the neuroendocrine markers CgA (D), Syn (E), CD56 (F), and NSE (G) were highly expressed in the tumorlets.
Figure 1. A 61-year-old woman with PCT and bronchiectasis. Dilated, beaded bronchi and cysts with defined borders can be observed in the lung window CT image (A, white arrowheads). Cord-like shadows can be observed in the mediastinal window (B, white arrows). PCT was evidenced by histopathological examination (C, black arrow). Tumorlets consisted of a comparatively uniform population of cells with oval or spindle nuclei. Mitoses were absent. Immunochemical staining revealed that the neuroendocrine markers CgA (D), Syn (E), CD56 (F), and NSE (G) were highly expressed in the tumorlets. 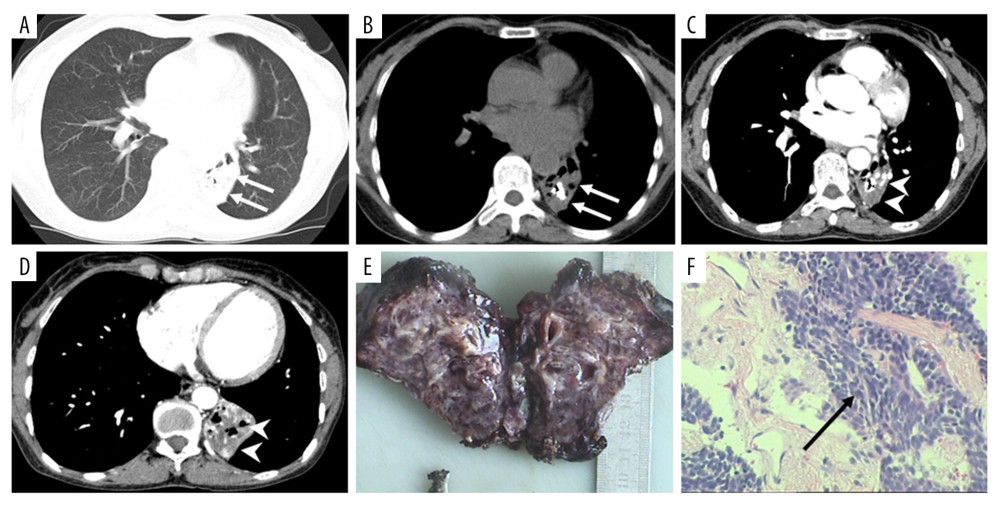 Figure 2. A 57-year-old woman with PCT and bronchiectasis and atelectasis. A patchy shadow was found in the left lower lobe on conventional CT image (long white arrows; A, lung window; B, mediastinal window) and contrast-enhanced CT images (white arrowheads; C, D). Obviously dilated and beaded bronchi were observed in the lung section (E). PCT was shown by histopathological examination (F, black arrow). Tumorlets consisted of a comparatively uniform population of cells with oval or spindle nuclei, without mitoses.
Figure 2. A 57-year-old woman with PCT and bronchiectasis and atelectasis. A patchy shadow was found in the left lower lobe on conventional CT image (long white arrows; A, lung window; B, mediastinal window) and contrast-enhanced CT images (white arrowheads; C, D). Obviously dilated and beaded bronchi were observed in the lung section (E). PCT was shown by histopathological examination (F, black arrow). Tumorlets consisted of a comparatively uniform population of cells with oval or spindle nuclei, without mitoses. 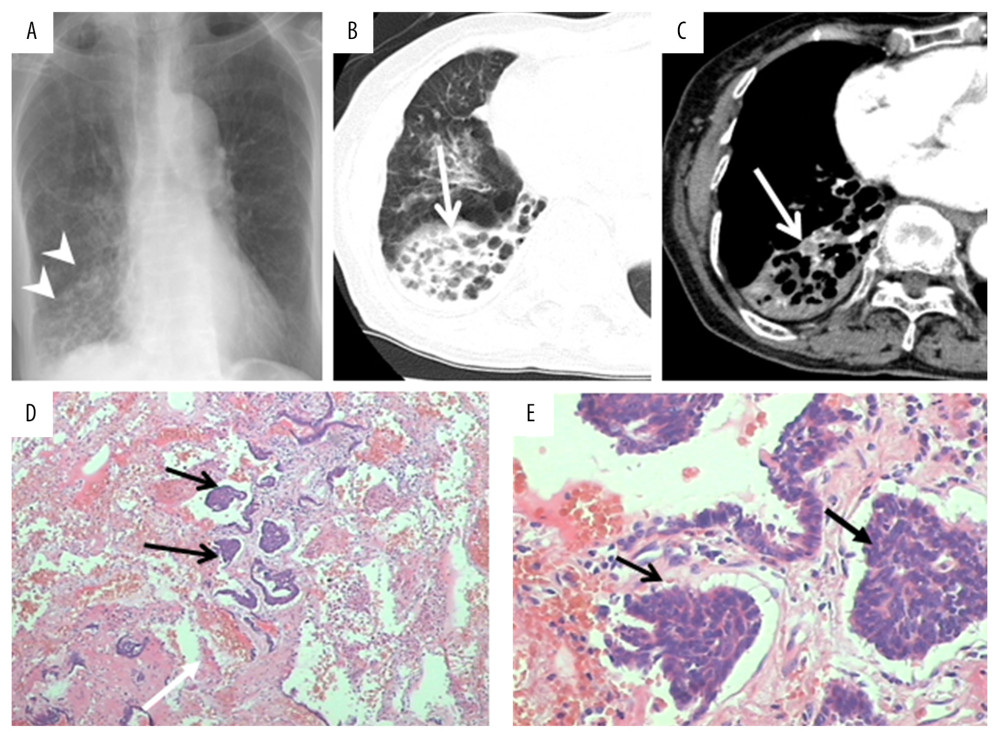 Figure 3. A 68-year-old woman with PCT and pulmonary tuberculosis. A patchy shadow was found in the middle right lobe on chest radiographs (A, white arrowheads) and CT images (long white arrows; B, lung window; C, mediastinal window). A 6.0×4.0×2.0 cm lung section was obtained and a sallow nodule was found. Several tuberculoid nodules and carcinoid tumorlets (D, E, black arrows) were observed in histopathological examination. Tumorlets consisted of a comparatively uniform population of cells with oval or spindle nuclei.
Figure 3. A 68-year-old woman with PCT and pulmonary tuberculosis. A patchy shadow was found in the middle right lobe on chest radiographs (A, white arrowheads) and CT images (long white arrows; B, lung window; C, mediastinal window). A 6.0×4.0×2.0 cm lung section was obtained and a sallow nodule was found. Several tuberculoid nodules and carcinoid tumorlets (D, E, black arrows) were observed in histopathological examination. Tumorlets consisted of a comparatively uniform population of cells with oval or spindle nuclei. References
1. He P, Gu X, Wu Q, Pulmonary carcinoid tumorlet without underlying lung disease: Analysis of its relationship to fibrosis: J Thorac Dis, 2012; 4; 655-58
2. Ginsberg MS, Akin O, Berger DM, Pulmonary tumorlets: CT findings: Am J Roentgenol, 2004; 183; 293-96
3. Travis WD, Advances in neuroendocrine lung tumors: Ann Oncol, 2012; 21; vii65-67
4. Kallianos A, Velentza L, Zarogoulidis P, Progressive dyspnea due to pulmonary carcinoid tumorlets: Respir Med Case Rep, 2017; 21; 84-85
5. Zhang Z, Hayreh H, Image diagnosis: Carcinoid tumorlets and pulmonary sequestration in a patient with chronic cough without a history of malignancy: Perm J, 2017; 21; 16-110
6. Gambino SL, King CS, Lettieri CJ, Multiple pulmonary nodules in a 70-year-old female with a history of breast cancer: Chest, 2009; 136; 938-41
7. Ye Y, Mu Z, Wu D, Carcinoid tumorlet in pulmonary sequestration with bronchiectasis after breast cancer: A case report: Oncol Lett, 2013; 5; 1546-48
8. Aubry MC, Thomas CF, Jett JR, Significance of multiple carcinoid tumors and tumorlets in surgical lung specimens: Analysis of 28 patients: Chest, 2007; 131; 1635-43
9. Ren S, Chen X, Wang Z, Differentiation of hypovascular pancreatic neuroendocrine tumors from pancreatic ductal adenocarcinoma using contrast-enhanced computed tomography: PLoS One, 2019; 14; e0211566
10. Linnoila RI, Functional facets of the pulmonary neuroendocrine system: Lab Investig, 2006; 86; 425-44
11. Rekhtman N, Neuroendocrine tumors of the lung: An update: Arch Pathol Lab Med, 2010; 134; 1628-38
12. Alrajhi N, Paramasivam M, Alboukai A, Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia: Unusual presentation: Ann Thorac Med, 2019; 14; 161-63
13. Jin L, Wang Z, Qi X, Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia: Case series and a review of the literature: Medicine (Baltimore), 2018; 97; e13806
14. Gorshtein A, Gross DJ, Barak D, Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia and the associated lung neuroendocrine tumors: Clinical experience with a rare entity: Cancer, 2012; 118; 612-19
15. Chassagnon G, Favelle O, Marchand-Adam S, DIPNECH: When to suggest this diagnosis on CT: Clin Radiol, 2015; 70; 317-25
16. Finkelstein SD, Hasegawa T, Colby T, 11q13 allelic imbalance discriminates pulmonary carcinoids from tumorlets: Am J Pathol, 1999; 155; 633-40
17. Pelosi G, Bianchi F, Dama E, Most high-grade neuroendocrine tumours of the lung are likely to secondarily develop from pre-existing carcinoids: Innovative findings skipping the current pathogenesis paradigm: Virchows Archiv, 2018; 472; 567-77
18. La Rosa S, Volante M, Uccella S, ACTH-producing tumorlets and carcinoids of the lung: clinico-pathologic study of 63 cases and review of the literature: Virchows Archiv, 2019; 475(5); 587-97
19. Dixon RK, Britt EJ, Netzer GA, Ten-year single center experience of pulmonary carcinoid tumors and diagnostic yield of bronchoscopic biopsy: Lung, 2016; 194; 905-10
20. Caliò A, Lever V, Rossi A, Increased frequency of bronchiolar histotypes in lung carcinomas associated with idiopathic pulmonary fibrosis: Histopathology, 2017; 71; 725-35
21. Sartelet H, Decaussin M, Devouassoux G, Expression of vascular endothelial growth factor (VEGF) and its receptors (VEGF-R1 [Flt-1] and VEGF-R2 [KDR/Flk-1]) in tumorlets and in neuroendocrine cell hyperplasia of the lung: Hum Pathol, 2004; 35; 1210-17
Figures
Figure 1. A 61-year-old woman with PCT and bronchiectasis. Dilated, beaded bronchi and cysts with defined borders can be observed in the lung window CT image (A, white arrowheads). Cord-like shadows can be observed in the mediastinal window (B, white arrows). PCT was evidenced by histopathological examination (C, black arrow). Tumorlets consisted of a comparatively uniform population of cells with oval or spindle nuclei. Mitoses were absent. Immunochemical staining revealed that the neuroendocrine markers CgA (D), Syn (E), CD56 (F), and NSE (G) were highly expressed in the tumorlets.Figure 2. A 57-year-old woman with PCT and bronchiectasis and atelectasis. A patchy shadow was found in the left lower lobe on conventional CT image (long white arrows; A, lung window; B, mediastinal window) and contrast-enhanced CT images (white arrowheads; C, D). Obviously dilated and beaded bronchi were observed in the lung section (E). PCT was shown by histopathological examination (F, black arrow). Tumorlets consisted of a comparatively uniform population of cells with oval or spindle nuclei, without mitoses.Figure 3. A 68-year-old woman with PCT and pulmonary tuberculosis. A patchy shadow was found in the middle right lobe on chest radiographs (A, white arrowheads) and CT images (long white arrows; B, lung window; C, mediastinal window). A 6.0×4.0×2.0 cm lung section was obtained and a sallow nodule was found. Several tuberculoid nodules and carcinoid tumorlets (D, E, black arrows) were observed in histopathological examination. Tumorlets consisted of a comparatively uniform population of cells with oval or spindle nuclei. Tables
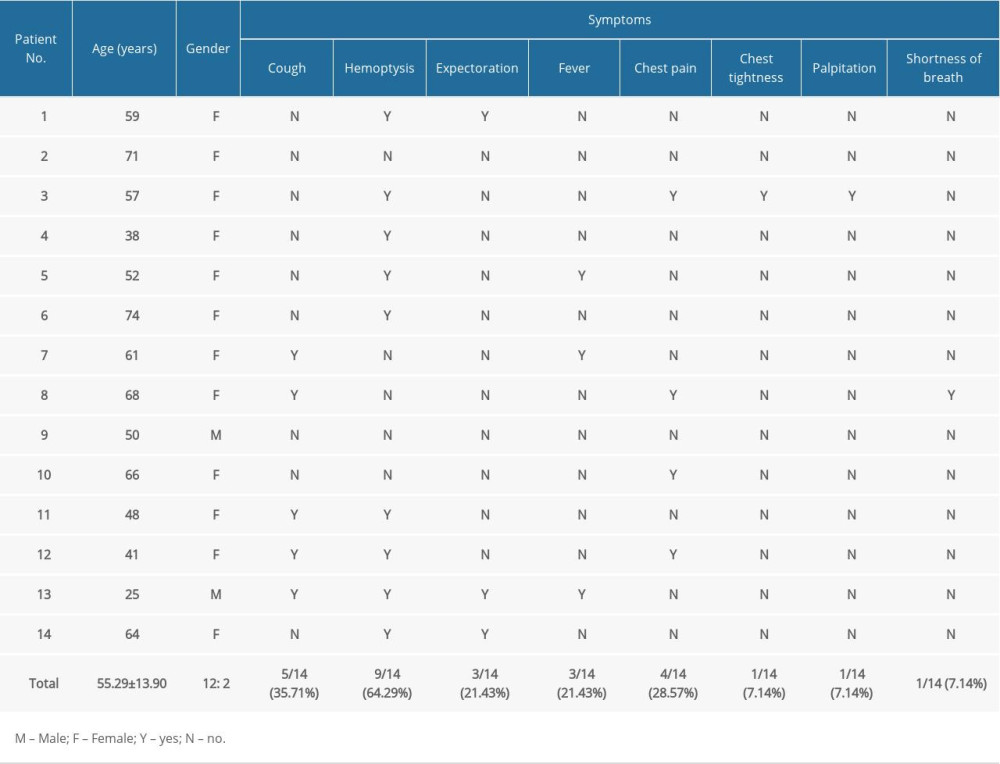 Table 1. Clinical symptoms in patients with pulmonary carcinoid tumorlets.
Table 1. Clinical symptoms in patients with pulmonary carcinoid tumorlets.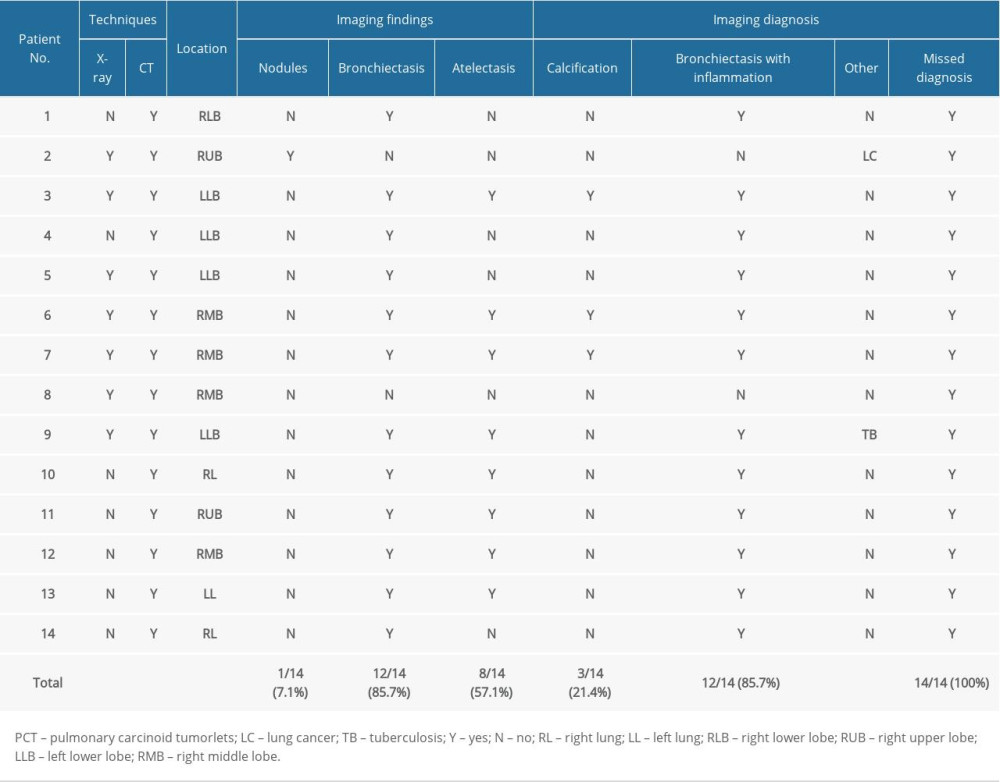 Table 2. Imaging findings and imaging diagnoses in patients with PCT.
Table 2. Imaging findings and imaging diagnoses in patients with PCT.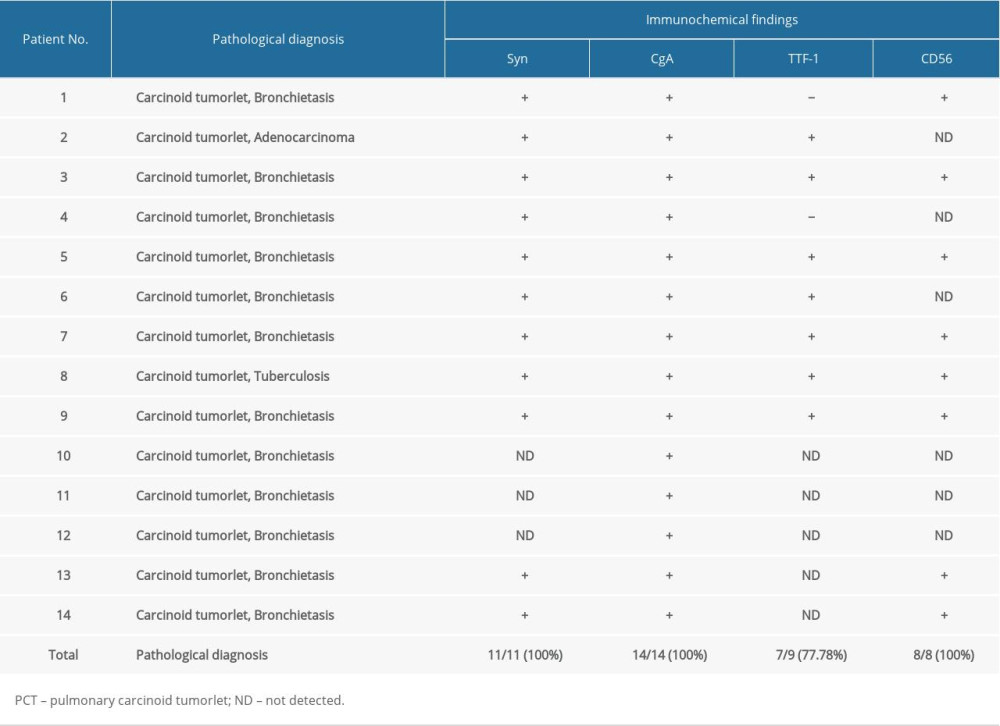 Table 3. Pathological diagnoses and immunochemical findings in patients with PCT.Table 1. Clinical symptoms in patients with pulmonary carcinoid tumorlets.Table 2. Imaging findings and imaging diagnoses in patients with PCT.Table 3. Pathological diagnoses and immunochemical findings in patients with PCT.
Table 3. Pathological diagnoses and immunochemical findings in patients with PCT.Table 1. Clinical symptoms in patients with pulmonary carcinoid tumorlets.Table 2. Imaging findings and imaging diagnoses in patients with PCT.Table 3. Pathological diagnoses and immunochemical findings in patients with PCT. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387