03 February 2021: Clinical Research
Efficacy of Beraprost Sodium Combined with Sildenafil and Its Effects on Vascular Endothelial Function and Inflammation in Patients Experiencing Left Heart Failure Complicated with Pulmonary Arterial Hypertension
Daoyuan Sun1ABE, Wenlan Yang2BDE, Zhenwei Wang3CDF, Beilan Gao4ACG*DOI: 10.12659/MSM.928413
Med Sci Monit 2021; 27:e928413






Abstract
BACKGROUND: To explore the efficacy of beraprost sodium combined with sildenafil and its effects on the vascular endothelial function and inflammation in left heart failure patients complicated with pulmonary arterial hypertension.
MATERIAL AND METHODS: A total of 80 patients with left heart failure complicated with pulmonary arterial hypertension was enrolled as the subjects of this study and assigned into an observation group (n=40) and a control group (n=40) using a random number table. The changes in pulmonary arterial hypertension-associated indicators at 3 months after treatment and the alterations in the levels of cardiac function-associated biochemical indicator brain natriuretic peptide (BNP), inflammatory factor tumor necrosis factor alpha (TNF-α), and mean pulmonary arterial pressure during treatment were compared between the 2 groups.
RESULTS: At 3 months after treatment, the pulmonary arterial hypertension-associated indicators human urotensin II and calcitonin gene-related peptide in the observation group were lower and higher, respectively, than those in control group. Moreover, the observation group had significantly lower BNP and TNF-α levels and mean pulmonary arterial pressure than the control group. After intervention, the echocardiographic parameters left ventricular ejection fraction (LVEF), cardiac output (CO), and stroke volume (SV) in both groups were significantly higher than those before intervention, and the observation group had significantly higher LVEF, SV, and CO than the control group after intervention.
CONCLUSIONS: Beraprost sodium combined with sildenafil for left heart failure complicated with pulmonary arterial hypertension can effectively improve pulmonary arterial hypertension, alleviate left heart failure, and reduce inflammatory responses, thereby achieving better clinical efficacy in patients.
Keywords: endothelial cells, Pulmonary Heart Disease, Aged, 80 and over, Echocardiography, Epoprostenol, Exercise Tolerance, pulmonary arterial hypertension, Pulmonary Artery, Sildenafil citrate, Stroke Volume, Ventricular Function, Left, Ventricular Function, Right
Background
In the pathogenesis of pulmonary arterial hypertension, elevated pulmonary vascular resistance-induced congestion in the pulmonary circulation can be diagnosed by measuring the mean pulmonary arterial pressure at rest or during exercise using right-heart catheterization [1]. Pulmonary arterial hypertension is a clinically common severe cardiovascular disease that can cause significant pulmonary vasoconstriction and thickening of the pulmonary artery intima, further increasing resistance in the pulmonary circulation, so it serves as a common risk factor for right heart failure. Chronic left heart failure can alter both structure and function of the heart in patients to obviously weaken cardiac filling and ejection, resulting in congestion in the pulmonary circulation [2]. Once patients have left heart failure complicated with pulmonary arterial hypertension, treatment is not satisfactory because of the critical disease conditions, and if no prompt and effective measures are performed, respiratory failure will occur in the early stages [3]. Calcium channel blockers used to be administered to the patients with left heart failure and pulmonary arterial hypertension to dilate blood vessels and reduce pulmonary arterial pressure, but the efficacy needs to be improved [4]. In recent years, great advances have been made in the treatment of pulmonary arterial hypertension with such drugs as prostacyclin and endothelin receptor antagonists. However, these drugs are far from satisfactory when administered alone to patients with left heart failure complicated by pulmonary arterial hypertension, so combined medication is necessary [5].
Beraprost sodium, the first oral prostacyclin derivative drug for humans, can selectively activate adenylate cyclase and raise the cyclic adenosine monophosphate level in cells, and it has certain antiplatelet, anti-inflammatory, and vasodilating effects as well [6]. Sildenafil, a 5-phosphodiesterase inhibitor, can effectively inactivate 5-phosphodiesterase and raise the level of cyclic guanosine monophosphate in the pulmonary vascular smooth muscle, thereby selectively dilating pulmonary vessels [7]. The present study mainly explored the clinical efficacy of beraprost sodium combined with sildenafil and its effects on vascular endothelial function and inflammatory responses in patients with left heart failure combined with pulmonary arterial hypertension so as to effectively improve the clinical treatment outcomes of such patients.
Material and Methods
GENERAL DATA:
A total of 80 patients with left heart failure complicated with pulmonary arterial hypertension who were treated in our hospital from January 2018 to December 2019 were enrolled as the subjects of this study. Consent documents for enrollment were signed. This study was approved by the Ethics Committee of Shanghai Pulmonary Hospital. Heart failure was definitively diagnosed by clinical manifestations and atrial brain natriuretic peptide (BNP) test results, whereas the diagnosis of pulmonary arterial hypertension was confirmed by past medical history combined with measurement results of pulmonary arterial pressure. Inclusion criteria: 1) patients with definitive diagnosis; 2) those with a predicted survival time of over 48 h; 3) those with normal mental conditions; and 4) those ≥50 years old. Exclusion criteria: 1) patients using bosentan, iloprost solution for inhalation, or other drugs for regulating pulmonary arterial pressure within 3 months before enrollment; 2) those with acute heart failure, respiratory failure, mental illness, congenital heart disease, myocardial infarction, respiratory system infection, tuberculosis, or malignant tumors; 3) those allergic to the drugs to be used in this study; or 4) those with stroke or severe liver or kidney dysfunction. The subjects were assigned into the following 2 groups using a random number table, with 40 patients in each group: Observation group: 27 men and 13 women, ages 50–88 years (mean 73.6±2.9 years). According to the New York Heart Association (NYHA) functional classification, 21 cases were in class III and 19 cases were in class IV at enrollment. The duration of left heart failure was 7–21 days (mean 15.3±1.2 days) and the duration of pulmonary arterial hypertension was 4 months-3 years (mean 17.5±1.5 months). Control group: 28 men and 12 women ages 50–87 years (mean 73.5±2.8 years). Among them, 20 patients were in NYHA class III and 20 patients were in NYHA class IV at enrollment. They experienced left heart failure for 7–20 days (mean 15.2±1.3 days) and pulmonary arterial hypertension for 4 months-3 years (mean 17.6±1.6 months). No statistically significant differences in the sex, age, NYHA functional class at enrollment, and duration of left heart failure and pulmonary arterial hypertension were observed between the 2 groups (
METHODS:
Upon enrollment, all the subjects were treated with cardiotonics, diuretics, vasodilators, and anticoagulant and antiplatelet drugs, and they were asked to lie in bed and inhale oxygen and received noninvasive mechanical ventilation therapy if necessary. For the special treatment of heart failure and pulmonary arterial hypertension, beraprost sodium tablets (40 μg each; Beijing Tide Pharmaceutical Co., Ltd., Beijing, China, NMP no. H20083589, batch no. 201711TH125) were orally taken 3 times daily after meals in the control group, whereas sildenafil citrate (20 mg each; Pfizer Inc., New York, NY, USA, NMP no. H20020528, batch no. 20171206) was orally administered 3 times daily in the observation group in addition to the treatment in the control group. The treatment in both groups lasted for 3 months (a treatment course).
OBSERVATION INDICATORS:
The changes in the pulmonary arterial hypertension-associated indicators at 3 months after treatment and the levels of cardiac function-associated biochemical indicator BNP, inflammatory factor tumor necrosis factor alpha (TNF-α), and mean pulmonary arterial pressure during treatment (before treatment and at 1 week, 1 month, and 3 months after treatment) were compared between the 2 groups. The alterations in the echocardiographic parameters before treatment and at 3 months after treatment and vascular endothelial function-related indicators at 3 months after treatment were also compared between the 2 groups. Finally, the correlations of mean pulmonary arterial pressure with the changes in levels of human urotensin II (hU-II), vascular endothelin-1, TNF-α, and BNP were analyzed.
EVALUATION CRITERIA:
Pulmonary arterial hypertension-associated indicator levels were determined for hU-II by drawing 5 mL of fasting blood from the elbow vein and centrifuging at 2500 revolutions per minute (rpm). The supernatant was collected and the level of hU-II was determined using an enzyme-linked immunosorbent assay kit (R&D Systems, Minneapolis, MN, USA; normal reference range in adults: 12.1–16.8 ng/L). For calcitonin gene-related peptide (CGRP), first, 5 mL of fasting blood was collected from the elbow vein and placed in anticoagulant-treated sterile test tubes and centrifuged at 2500 rpm. The supernatant was harvested, and the level of CGRP was measured using the chemiluminescence method (normal reference range in adults: 36–54 pg/mL). According to the classical diagnosis criteria of the European Society of Cardiology and European Respiratory Society in 2009, pulmonary arterial hypertension was diagnosed when the mean pulmonary arterial pressure recorded using an RM 6240B multichannel electrophysiological monitor was ≥25 mmHg at rest and ≥30 mmHg during exercise. Echocardiographic parameters included left ventricular ejection fraction (LVEF; normal reference value in adults: ≥50%), cardiac output (CO; normal reference value in adults: ≥4.5 L/min), and stroke volume (SV; normal reference value in adults: ≥60 mL). When the level of cardiac function-associated biochemical indicator BNP exceeded 500 mg/L (normal reference value in adults: ≤200 mg/L), heart failure was diagnosed. The normal reference range of inflammatory factor TNF-α in adults is 1–10 ηg/mL. Vascular endothelial function indicators included endothelin-1 (normal reference range: 3.5–58.4 ηg/L) and nitric oxide (normal reference range: 13.8–34.6 μmol/L).
STATISTICAL ANALYSIS:
Statistical Product and Service Solutions (SPSS) 20.0 (IBM, Armonk, NY, USA) was used for statistical processing. Such measurement data as pulmonary arterial hypertension-associated indicators, cardiac function-associated biochemical indicators, inflammatory indicators, and mean pulmonary arterial pressure were presented as mean±standard deviation (χ̆±
Results
COMPARISONS OF PULMONARY ARTERIAL HYPERTENSION-ASSOCIATED INDICATORS AT 3 MONTHS AFTER TREATMENT BETWEEN THE 2 GROUPS:
At 3 months after treatment, the observation group had a lower level of hU-II (P<0.05), but a higher level of CGRP (P<0.05) than the control group (Table 1).
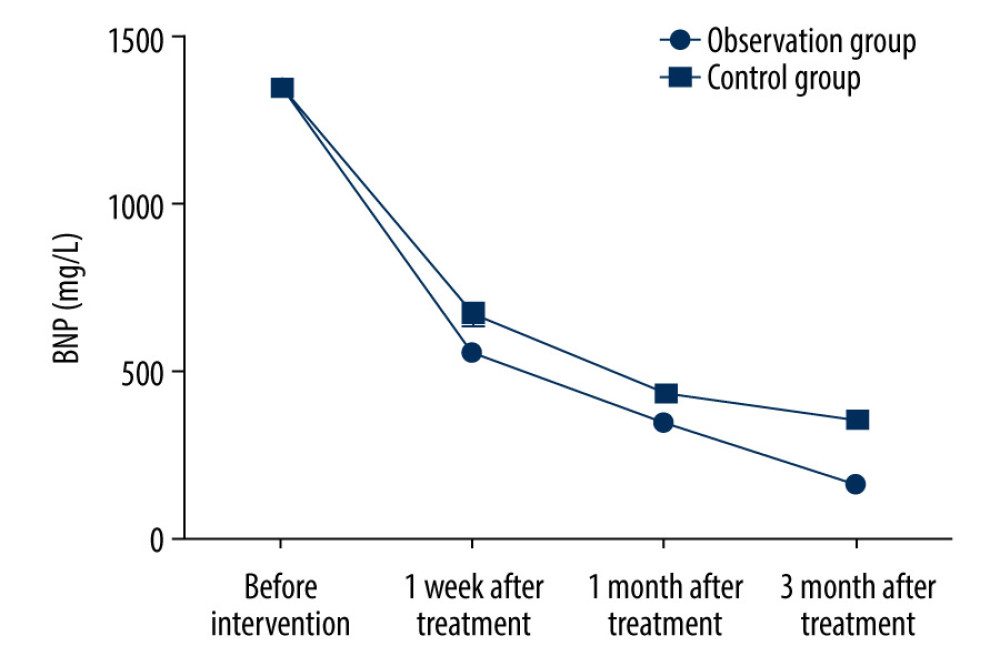
CHANGES IN LEVEL OF CARDIAC FUNCTION-ASSOCIATED BIOCHEMICAL INDICATOR BNP DURING TREATMENT:
Before treatment, no statistically significant difference in the level of BNP was observed between the 2 groups ([955.6±23.1] mg/L vs [956.1±23.0] mg/L; P>0.05). The levels of BNP at 1 week, 1 month, and 3 months after treatment in the observation group were significantly lower than those in the control group ([558.8±25.6] mg/L vs [678.8±31.8] mg/L, [359.6±19.2] mg/L vs [438.3±8.9] mg/L, [169.8±18.8] mg/L vs [359.5±16.3] mg/L; t=18.591, 23.520, and 48.218, P<0.05) (Figure 1).
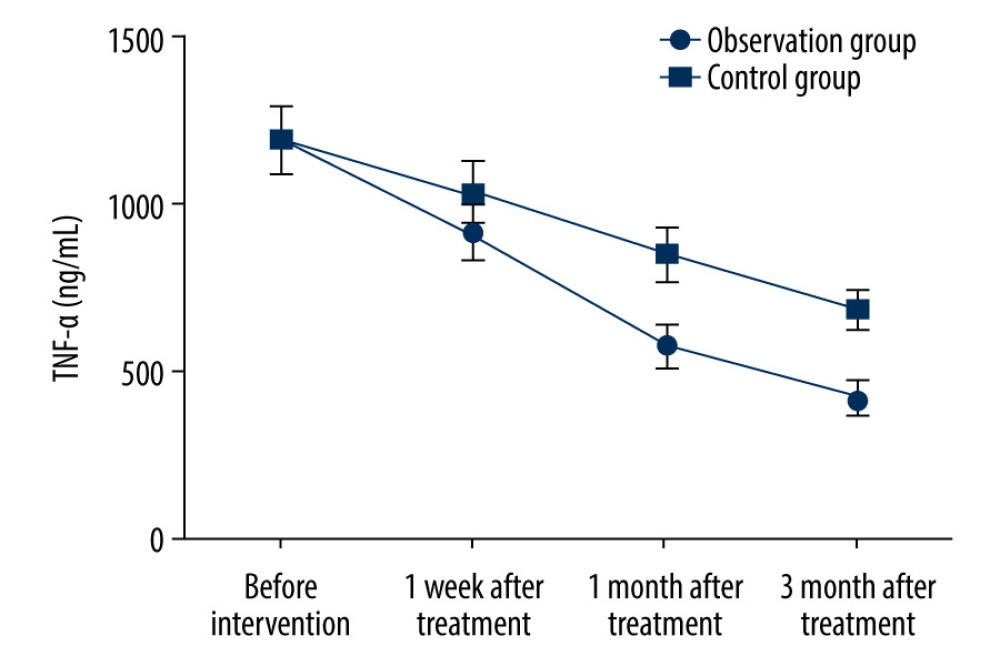
CHANGES IN LEVEL OF TNF-α DURING TREATMENT:
Before treatment, the level of TNF-α was not statistically significantly different between the 2 groups ([23.6±1.9] ng/mL vs [23.6±2.0] ng/mL; P>0.05). At 1 week, 1 month, and 3 months after treatment, the observation group had a significantly lower level of TNF-α than the control group ([18.1±1.7] ng/mL vs [20.4±1.8] ng/mL, [11.3±1.3] ng/mL vs [16.8±1.6] ng/mL, and [8.3±0.9] ng/mL vs [13.5±1.1] ng/mL; t=5.875, 16.873, and 23.140, P<0.05) (Figure 2).
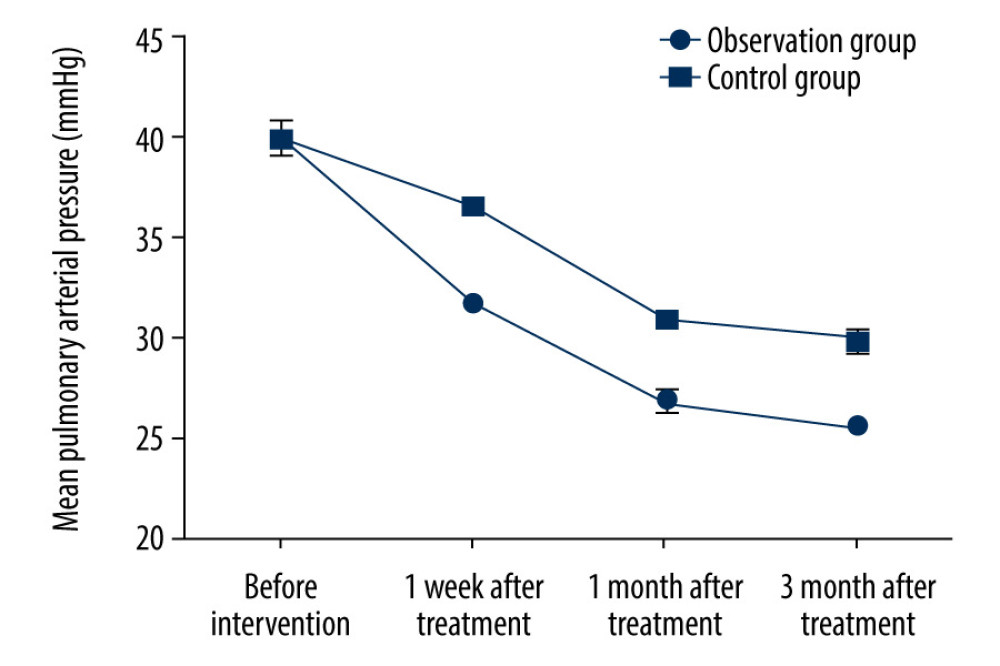
CHANGES IN MEAN PULMONARY ARTERIAL PRESSURE DURING FOLLOW-UP:
Before treatment, there was no statistically significant difference in the mean pulmonary arterial pressure between the 2 groups ([39.7±0.8] mmHg vs [39.8±0.8] mmHg; P>0.05). The mean pulmonary arterial pressure at 1 week, 1 month, and 3 months after treatment in the observation group was significantly lower than that in the control group ([31.6±0.2] mmHg vs [36.4±0.3] mmHg, [26.8±0.5] mmHg vs [30.8±0.3] mmHg, and [25.6±0.4] mmHg vs [29.8±0.5] mmHg; t=84.198, 43.386, and 41.485, P<0.05) (Figure 3).
COMPARISONS OF ECHOCARDIOGRAPHIC PARAMETERS BEFORE TREATMENT AND AT 3 MONTHS AFTER TREATMENT:
Before intervention, the echocardiographic parameters LVEF, SV, and CO were statistically significantly different between the 2 groups (P>0.05). After intervention, the LVEF, SV, and CO significantly rose in both groups compared with those before intervention (P<0.05), and the observation group had higher LVEF, SV, and CO than the control group after intervention (P<0.05) (Table 2).
COMPARISONS OF VASCULAR ENDOTHELIAL FUNCTION-RELATED INDICATORS AT 3 MONTHS AFTER TREATMENT:
At 3 months after treatment, the observation group had a higher level of nitric oxide (P<0.05) but a lower level of vascular endothelin-1 than the control group (P<0.05) (Table 3).
Discussion
Left heart failure, an impairment of cardiac function caused by multiple underlying heart diseases, can give rise to changes in myocardial structure and function [8], and it will progress until left heart pumping dysfunction, decreased filling capacity, and systolic dysfunction occur [9]. As the course is extended, left heart failure can induce water-sodium retention, congestion in the pulmonary and systemic circulation, elevated left ventricular preload and afterload, and even secondary pulmonary arterial hypertension [10]. Pulmonary arterial hypertension is a cardiovascular disease with a poor prognosis in which pulmonary vascular resistance and pressure tend to be increased by pulmonary artery occlusion. With the prolongation of the course of pulmonary arterial hypertension, pulmonary vascular remodeling will occur, further resulting in right heart failure and even clinical death [11]. Conventionally, the main symptomatic and supportive treatments for patients with left heart failure complicated with pulmonary arterial hypertension include oxygen therapy, cardiotonic therapy, diuretic treatment, vasodilation, and anti-infection [12]. Drugs for the targeted treatment of pulmonary arterial hypertension have been increasingly extensively used in clinical practice with the application of biological targeted therapy, but they are expensive [13]. Therefore, pulmonary arterial hypertension is clinically treated with beraprost sodium, a prostacyclin derivative. Although beraprost sodium can substantially inhibit prostacyclin in the vascular smooth muscle and restrain calcium influx, thereby dilating blood vessels [14], it alone has limited efficacy for left heart failure patients complicated with pulmonary arterial hypertension [15].
In this study, in addition to symptomatic and supportive treatments, beraprost sodium was administered in the control group, whereas beraprost sodium combined with sildenafil was given in the observation group. Then, the pulmonary arterial hypertension-associated indicators at 3 months after treatment were compared between the 2 groups, and it was found that the observation group had a lower level of hU-II but a higher level of CGRP than the control group. These findings suggest that beraprost sodium combined with sildenafil for left heart failure complicated with pulmonary arterial hypertension can considerably decrease pulmonary arterial hypertension-associated biochemical indicators. The changes in the levels of cardiac function-associated biochemical indicator BNP and inflammatory factor TNF-α and mean pulmonary arterial pressure during treatment were also compared between the 2 groups. It was discovered that the observation group had lower levels of BNP and TNF-α as well as mean pulmonary arterial pressure than the control group at 1 week, 1 month, and 3 months after treatment, indicating that beraprost sodium combined with sildenafil for left heart failure complicated with pulmonary arterial hypertension is significantly valuable in reducing heart failure-related factors and relieving body inflammatory responses and pulmonary arterial pressure. The echocardiographic parameters before treatment and at 3 months after treatment were compared between the 2 groups. According to the results, the LVEF, SV, and CO significantly rose in both groups after intervention compared with those before intervention, and the observation group had higher LVEF, SV, and CO than the control group after intervention. These results imply that beraprost sodium combined with sildenafil for left heart failure complicated with pulmonary arterial hypertension can reverse left ventricular remodeling to a certain extent, enhance cardiac pumping capacity, and alleviate left heart failure. The vascular endothelial function-related indicators were compared between the 2 groups at 3 months after treatment as well, and it was found that the observation group had a higher level of nitric oxide but a lower level of vascular endothelial-1 than the control group. The above results suggest that beraprost sodium combined with sildenafil for left heart failure complicated with pulmonary arterial hypertension has a significant protective effect on the vascular endothelium. Finally, the correlations of mean pulmonary arterial pressure with the changes in hU-II, vascular endothelin-1, TNF-α, and BNP levels were analyzed, and the results revealed that the mean pulmonary arterial pressure was positively correlated with the changes in the levels of hU-II, vascular endothelin-1, TNF-α, and BNP.
As a 5-phosphodiesterase inhibitor [16], sildenafil can effectively inactivate 5-phosphodiesterase to raise the level of cyclic guanosine monophosphate in the body [17], and selectively act on the pulmonary vascular smooth muscle to effectively dilate pulmonary vessels [18], so it is combined with beraprost sodium to treat left heart failure complicated with pulmonary arterial hypertension. Since lung tissues are rich in 5-phosphodiesterases, after oral administration, sildenafil has a long half-life, long duration of action, and high specificity and causes few adverse reactions. Additionally, this drug can reduce vascular endothelin-1 levels and raise nitric oxide levels, further dilating blood vessels [19]. Sildenafil in combination with beraprost sodium can also elevate the cyclic adenosine phosphate level in the body but does not compete with beraprost sodium for cytochrome P450 receptors. Therefore, their combination has an obvious synergistic effect [20].
On the basis of this randomized controlled trail, we believe that the combination of beraprost sodium with sildenafil was beneficial for patients experiencing left heart failure complicated with pulmonary arterial hypertension. The results of this study paved a new pathway for the treatment of left heart failure complicated with pulmonary arterial hypertension. However, the sample size of our study was too small, and this was a single center and nondouble-blind trial. The follow-up time was only 3 months. A randomized controlled, double-blind, multicenter trial needs to be carried out to further support our conclusions.
Conclusions
In conclusion, beraprost sodium combined with sildenafil can effectively improve pulmonary arterial hypertension, alleviate left heart failure, and relieve inflammatory responses in the body, thereby achieving better clinical efficacy in patients.
Tables
Table 1. Comparisons of pulmonary arterial hypertension-associated indicators at 3 months after treatment between the 2 groups (χ̆±s). Observation group: beraprost sodium combined with sildenafil; control group: beraprost sodium only. Table 2. Comparisons of echocardiographic parameters before treatment and at 3 months after treatment between the 2 groups (χ̆±s). Observation group: beraprost sodium combined with sildenafil; control group: beraprost sodium only.
Table 2. Comparisons of echocardiographic parameters before treatment and at 3 months after treatment between the 2 groups (χ̆±s). Observation group: beraprost sodium combined with sildenafil; control group: beraprost sodium only.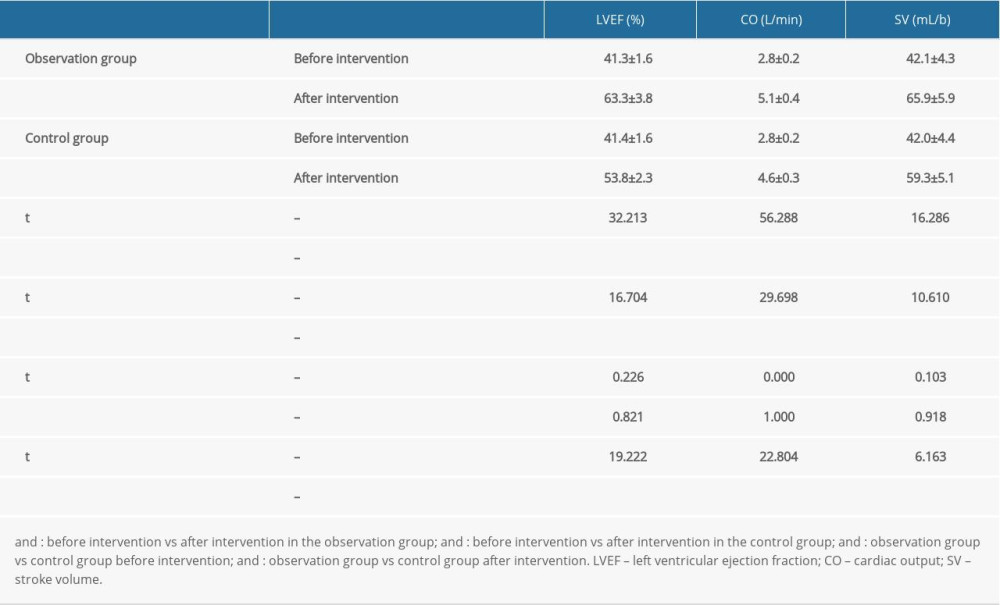 Table 3. Comparisons of vascular endothelial function-related indicators at 3 months after treatment between the 2 groups (χ̆±s). Observation group: beraprost sodium combined with sildenafil; control group: beraprost sodium only.
Table 3. Comparisons of vascular endothelial function-related indicators at 3 months after treatment between the 2 groups (χ̆±s). Observation group: beraprost sodium combined with sildenafil; control group: beraprost sodium only.
References
1. Maki H, Kubota K, Hatano M, Characteristics of pulmonary arterial hypertension in patients with systemic sclerosis and anticentriole autoantibodies: Int Heart J, 2020; 61; 413-18
2. Natali S, Palmieri M, Polidori C, Prevalence of pulmonary arterial hypertension in the Camerino area of central Italy and savings resulting from generic bosentan: Eur J Hosp Pharm, 2020; 27; 100-2
3. Akabane R, Sato T, Sakatani A, Pharmacokinetics of single dose sildenafil orally administered in canine models of chronic embolic pulmonary hypertension: J Vet Med Sci, 2020; 82; 446-51
4. Ren Z, Li J, Shen J, Therapeutic sildenafil inhibits pulmonary damage induced by cigarette smoke exposure and bacterial inhalation in rats: Pharm Biol, 2020; 58; 116-23
5. Russell S, Beghetti M, Oudiz R, A randomised trial: Open Heart, 2019; 6; e1149
6. Varghese N, Rios D, Pulmonary hypertension associated with bronchopulmonary dysplasia: A review: Pediatr Allergy Immunol Pulmonol, 2019; 32; 140-48
7. Johnson LR, Stern JA, Clinical features and outcome in 25 dogs with respiratory-associated pulmonary hypertension treated with sildenafil: J Vet Intern Med, 2020; 34; 65-73
8. Villanueva D, Agustin RD, Llanes EJ, Pre-operative sildenafil for patients with pulmonary hypertension undergoing mitral valve surgery: A systematic review and meta-analysis: Cardiol Res, 2019; 10; 369-77
9. Molloy S, McVea S, Thompson A, In the child with pulmonary hypertension, does treatment with enteral sildenafil compared with a slow wean from nitric oxide alone prevent rebound pulmonary hypertension and allow for discontinuation of nitric oxide?: Arch Dis Child, 2020; 105; 410-12
10. Allen J, Peterson N, Barrett K, A case report: J Vet Intern Med, 2020; 34; 283-88
11. Martinez C, Tsugu T, Sugimoto T, When to treat the valve disease and when to treat the pulmonary hypertension: Curr Cardiol Rep, 2019; 21; 151
12. Wang T, Lu J, Li Q, A retrospective observational case series study: Anesth Analg, 2019; 129; 1607-12
13. Cochius-den OS, Kipfmueller F, de Winter B, Pharmacokinetic modeling of intravenous sildenafil in newborns with congenital diaphragmatic hernia: Eur J Clin Pharmacol, 2020; 76; 219-27
14. Park SS, Kim TW, Kim CJ, Effect of sildenafil citrate on brain central fatigue after exhaustive swimming exercise in rats: J Exerc Rehabil, 2019; 15; 651-56
15. Lavie-Nevo K, Harris KC, Ting JY, Use of sildenafil in an infant with persistent pulmonary hypertension secondary to lung and renal hypoplasia – a case report: BMC Pediatr, 2019; 19; 416
16. Choi SH, Jung YK, Jang JA, Idiopathic pulmonary arterial hypertension associated with a novel frameshift mutation in the bone morphogenetic protein receptor II gene and enhanced bone morphogenetic protein signaling: A case report: Medicine (Baltimore), 2019; 98; e17594
17. Chanu P, Gao X, Bruno R, A modeling and simulation-based assessment of the impact of confounding factors on the readout of a sildenafil survival trial in pulmonary arterial hypertension: J Pharmacokinet Pharmacodyn, 2019; 46; 499-509
18. Stephanie P, Catherine B, Thierry S, Excluding NFU1 deficiency: Ann Pediatr Cardiol, 2019; 12; 325-28
19. Centorrino R, Shankar-Aguilera S, Foligno S, Life-threatening extreme methemoglobinemia during standard dose nitric oxide therapy: Neonatology, 2019; 116; 295-98
20. Khalil A, Sharp A, Cornforth C, Planned subgroup analysis from a multicenter randomized placebo-controlled double-blind trial: Ultrasound Obstet Gynecol, 2020; 55; 198-209
Figures
Tables
Table 1. Comparisons of pulmonary arterial hypertension-associated indicators at 3 months after treatment between the 2 groups (χ̆±s). Observation group: beraprost sodium combined with sildenafil; control group: beraprost sodium only.Table 2. Comparisons of echocardiographic parameters before treatment and at 3 months after treatment between the 2 groups (χ̆±s). Observation group: beraprost sodium combined with sildenafil; control group: beraprost sodium only.Table 3. Comparisons of vascular endothelial function-related indicators at 3 months after treatment between the 2 groups (χ̆±s). Observation group: beraprost sodium combined with sildenafil; control group: beraprost sodium only.Table 1. Comparisons of pulmonary arterial hypertension-associated indicators at 3 months after treatment between the 2 groups (χ̆±s). Observation group: beraprost sodium combined with sildenafil; control group: beraprost sodium only.Table 2. Comparisons of echocardiographic parameters before treatment and at 3 months after treatment between the 2 groups (χ̆±s). Observation group: beraprost sodium combined with sildenafil; control group: beraprost sodium only.Table 3. Comparisons of vascular endothelial function-related indicators at 3 months after treatment between the 2 groups (χ̆±s). Observation group: beraprost sodium combined with sildenafil; control group: beraprost sodium only. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387