13 February 2021: Clinical Research
Factors Affecting the Risk of Postpartum Hemorrhage in Pregnant Women in Tibet Health Facilities
Zhuo-Ma Pubu1BCE, Zhuo-Ma Bianba2CF, Ge Yang1DF, La-Mu CyRen1DF, De-Ji Pubu1DF, Ka-Zhu Suo Lang1F, Bian Zhen1CF, Qu-Zong Zhaxi1F, Zhuo-Ga Nyma1AE*DOI: 10.12659/MSM.928568
Med Sci Monit 2021; 27:e928568






Abstract
BACKGROUND: Postpartum hemorrhage (PPH), the leading cause of maternal death, is defined as a blood loss >500 mL within 24 h after vaginal delivery or >1000 mL within 24 h after cesarean section. This study aimed to investigate the incidence of PPH and assess its risk factors in pregnant women in Tibet to provide a reference for clinicians in this region.
MATERIAL AND METHODS: A total of 4796 pregnant women with gestational age ≥28 weeks who were admitted to hospitals in Tibet between December 2010 and December 2016 were involved in this study. Patient sociological and clinical data and pregnancy outcomes were collected. The related risk factors of PPH were analyzed by univariate and multivariable logistic regression. The area under the curve of the receiver operating characteristic curves was used to evaluate the effect of the PPH prediction model.
RESULTS: PPH occurred in 95 women, with an incidence of 1.98%. The following factors were associated with higher risk for PPH: maternal age ≥35 (odds ratio [OR]=1.96; 95% confidence interval [CI], 1.18–3.27; P=0.010), history of preterm birth (OR=2.66; 95% CI, 1.60–4.42; P<0.001), cesarean section (OR=6.69; 95% CI, 4.30–10.40; P<0.001), neonatal weight >4 kg (OR=3.92; 95% CI, 1.75–8.81; P<0.001) and occurrence of neonatal asphyxia (OR=5.52; 95% CI, 2.22–13.74; P<0.001).
CONCLUSIONS: Maternal age ≥35, history of preterm birth, cesarean section, newborn weight >4 kg, and neonatal asphyxia were risk factors of PPH, which can help evaluate PPH in Tibet.
Keywords: Delivery, Obstetric, Postpartum Hemorrhage, Pregnant Women, Risk Factors, Area Under Curve, Cesarean Section, Gestational Age, Health Facilities, Incidence, Infant, Infant, Newborn, Pregnancy, Pregnancy Outcome, Premature Birth, Tibet, young adult
Background
Postpartum hemorrhage (PPH) is defined as a loss of blood >500 mL within 24 h after vaginal delivery or > 1000 mL blood loss within 24 h after cesarean section. PPH remains a serious problem in pregnant women worldwide. Tibet is located in the Qinghai-Tibet Plateau and has an average altitude of more than 3000 meters above sea level. Low pressure and low oxygen decrease artery oxygen saturation. The incidence of PPH in pregnant women in the plateau is 2 to 7 times higher than that in plain areas [1]. As an obstetric emergency, PPH can cause sequelae such as hypotension, anemia, and fatigue, affecting puerperal recovery and even endangering the life of the puerpera in severe cases [2]. A previous study reported that PPH occurs in 18% of deliveries, which causes huge loss of life and property in society [3]. PPH is one of the major causes of maternal morbidity and mortality, despite major improvements in biomedicine and reproductive health services [4,5]. Recently, several studies have indicated that PPH results in 26.7% of severe adverse maternal outcomes and 29.3% of maternal deaths globally [6–8]; it is one of the main contributors to maternal death in the world and in China [9]. Therefore, giving attention to PPH is crucial for improving pregnancy outcomes.
The occurrence of PPH is influenced by various factors, including adherent placenta, uterine atony, genital tract injury, and coagulopathy [10–13]. Although obstetricians have taken some measures such as administering oxytocin during childbirth, the incidence of PPH remains high [14]. Fukami et al believe that regardless of the clinical etiology, the high incidence of PPH may result from characteristics of the maternal population [10]. Previous studies revealed that PPH history, multiple pregnancies, macrosomia, primiparity, multiple births, advanced maternal age, premature delivery, low education, cesarean section, and stillbirth are potential factors associated with PPH [15–17]. For obstetricians, the accurate identification of indicators affecting PPH in pregnant women and assessment of PPH risk aid in making timely intervention and preventing the occurrence of PPH. This study was conducted at Lhasa People’s Hospital from December 2010 to December 2016. The aim of this study was to clarify the incidence of PPH and the factors leading to it in pregnant women in Tibet. Our study findings could provide a reference for clinicians to prevent PPH in pregnant women in this region.
Material and Methods
STUDY DESIGN AND PATIENTS:
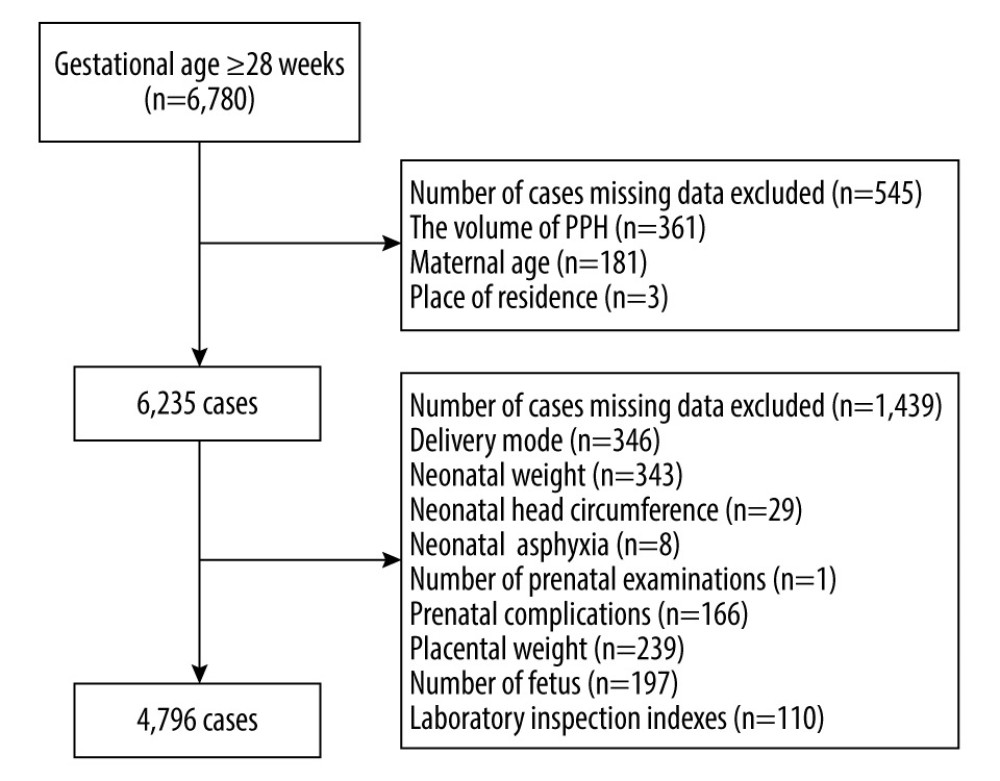
This was a retrospective study conducted at the Department of Obstetrics and Gynecology in Lhasa People’s Hospital from December 2010 to December 2016. A total of 6780 pregnant women who were registered in hospitals or health centers in Tibet were selected for the study. Among them, patients who met the inclusion criteria of gestational age of 28 weeks or more were included. Patients with missing data regarding the volume of PPH, delivery mode, maternal age, prenatal complications, neonatal weight, neonatal head circumference, placental weight, number of fetus, and laboratory inspection indexes were excluded. Ultimately, 4796 women were involved in this study. PPH was diagnosed based on the WHO diagnostic criteria: blood loss >500 mL within 24 h after vaginal delivery or blood loss >1000 mL within 24 h after cesarean section [18]. Participants were divided into a PPH group (n=95) and non-PPH group (n=4701) based on whether PPH occurred. Informed consent was collected from the patients, and the study was approved by the Ethics Committee of Lhasa People’s Hospital (approval No. SYLL2218005).
DATA COLLECTION:
Sociodemographic and clinical data were collected from all patients. Sociodemographic information included the patients’ age, place of residence, level of education, number of full-term births, history of preterm births, and history of abortion. Clinical data included prenatal laboratory indexes, prenatal complications, gestational age, number of fetuses, number of prenatal examinations, placental weight, prenatal length of hospital stay, mode of delivery, perineal condition, neonatal weight and head circumference, neonatal asphyxia, and amniotic fluid condition.
SAMPLING TECHNIQUES AND TOOLS:
The volumetric, gravimetric, and suction canister methods, 3 commonly used methods of measuring blood loss volume, were used in our study. The volumetric and gravimetric methods are suitable for vaginal delivery while the suction canister method is suitable for cesarean section.
The volumetric method was conducted as follows: after delivery, when the amniotic fluid was drained away, a special kidney basin was immediately placed close to the perineum of the puerpera. After 2 h, the blood container was taken out and the blood volume was measured using a measuring cup.
The gravimetric method was conducted as follows: after delivery, the blood-soaked dressing, sheets, and towels used were collected, sealed, and weighed. The weight of dressing before delivery was subtracted from the weight after delivery. The blood volume was calculated in line with a ratio of weight (g): volume (mL) of 1.05: 1.
After conversion into milliliters, the volume of blood for vaginal delivery was obtained by adding the volume of bleeding from the volumetric and gravimetric methods.
The suction canister method was conducted as follows: first, after cutting the uterine wall of the puerpera, the amniotic fluid was sucked out. Next, the blood was collected using suction canisters, poured into a measuring cylinder, and the volume of blood was measured.
STATISTICAL ANALYSIS:
For baseline data analysis, the normality of measurement data was evaluated using the Shapiro test. The measurements of normally distributed data were expressed as mean±standard deviation, and comparisons between groups were conducted using the
Results
OVERALL BASIC PATIENT INFORMATION:
In total, 6780 pregnant women in Tibet were involved in our study. After excluding patients with missing data on the volume of PPH (361), delivery mode (346), neonatal weight (343), neonatal head circumference (29), neonatal asphyxia (8), maternal age (181), place of residence (3), number of prenatal examinations (1), placental weight (239), prenatal complications (166), number of fetuses (197), and laboratory indexes (110), 4796 women participated in our study. The patient screening process is shown in Figure 1.
As presented in Table 1, among the 4796 patients, 90.43% were 18 to 35 years old and 9.57% were ≥35 years old. A total of 2265 patients (47.23%) came from urban areas and 2531 (52.77%) came from rural areas. A total of 2340 (48.79%) had a high school education or above and 2456 (51.21%) had junior high school education or below. Some patients (13.78%) had a history of preterm birth, 24.69% of patients had a history of abortion, and most patients had experienced from 1 to 3 full-term births (55.09%). PPH occurred in 95 women, with an incidence of 1.98%.
UNIVARIATE ANALYSIS FOR PPH:
We performed a univariate analysis for comparing the demographic and clinical characteristics of participants in the PPH and non-PPH groups. The results showed that the percentage of women with the following characteristics was markedly higher in the PPH group than in the non-PPH group: ≥35 years old (χ2=21.16, P<0.001), full-term birth (P=0.003), history of preterm birth (χ2=20.11, P=0.001), history of abortion (χ2=11.58, P=0.022), condition of the perineum (χ2=56.72, P<0.001), cesarean section (χ2=89.80, P<0.001), neonatal weight >4 kg (P<0.001), placenta weight ≥600 g (χ2=6.13, P=0.013), neonatal asphyxia (P=0.003), other inflammation (χ2=5.82, P=0.016), amniotic fluid meconium contamination (χ2=6.71, P<0.010), and prenatal length of hospital stay (t=−4.16, P<0.001) (Table 1).
MULTIVARIABLE LOGISTIC REGRESSION ANALYSIS FOR PPH:
Variables with statistically significant differences, according to the results of the univariate analysis, were included in the multivariable logistic regression analysis. As shown in Table 2, maternal age ≥35 years (odds ratio [OR]=1.96; 95% confidence interval [CI], 1.18–3.27; P=0.010); history of preterm birth (OR=2.66; 95% CI, 1.60–4.42; P<0.001); cesarean section (OR=6.69; 95% CI, 4.30–10.40; P<0.001), neonatal weight >4 kg (OR=3.92; 95% CI, 1.75–8.81; P<0.001), and occurrence of neonatal asphyxia (OR=5.52; 95% CI, 2.22–13.74; P<0.001) may elevate the risk of PPH in pregnant women.
CONSTRUCTION AND VALIDATION OF THE PPH PREDICTION MODEL:
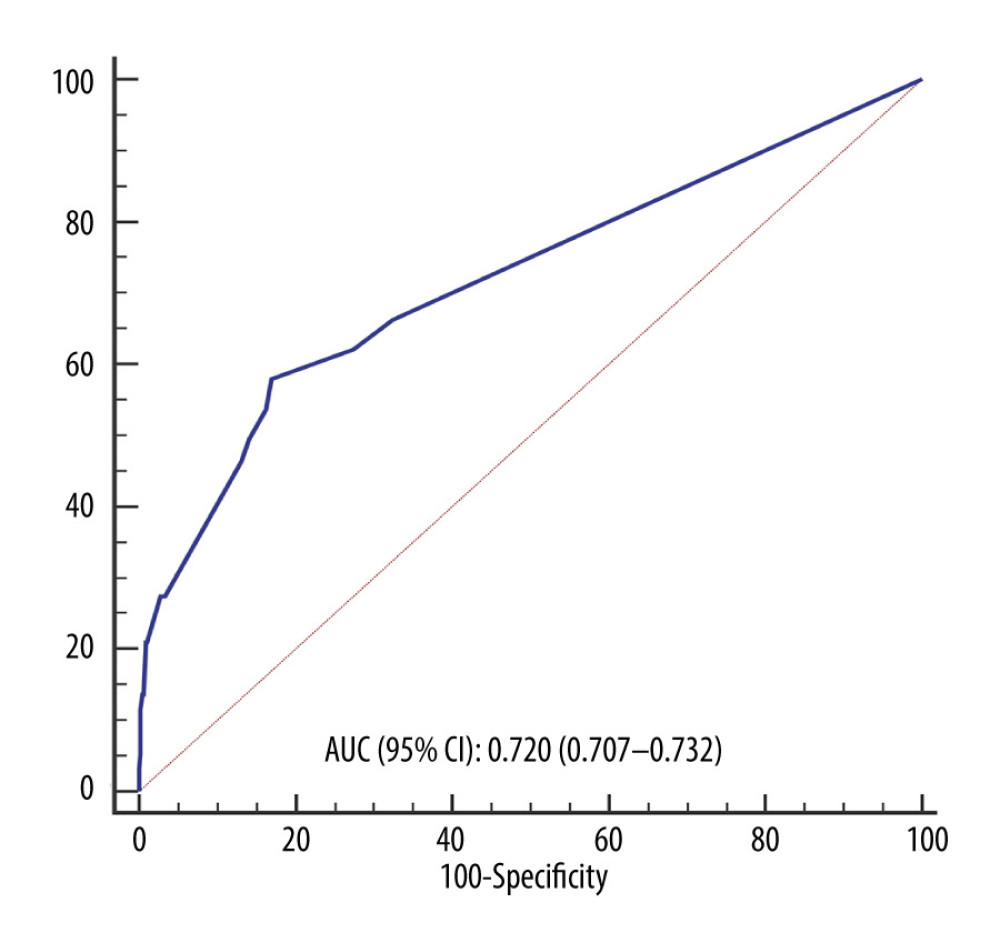
Independent risk factors including maternal age ≥35 years, history of preterm birth, cesarean section, neonatal weight >4 kg, and occurrence of neonatal asphyxia were used to establish the prediction model of PPH. As displayed in Table 2, the PPH prediction model was obtained as follows: Y=Logit (P)=−3.184+0.674×maternal age (≥35)+0.977×history of preterm birth (yes)+0.950×mode of delivery (cesarean section)+0.683×neonatal weight (>4 kg)+1.708×neonatal asphyxia (yes). When P>0.021, the model predicted that PPH would occur. The results from the ROC curve indicated that the area under the curve (AUC) value of this model was 0.720 (95% CI, 0.707–0.732; sensitivity, 57.89%; specificity, 83.02%) (Figure 2, Table 3).
Discussion
The sociodemographic and clinical data of 4796 pregnant women in Tibet were collected to measure the incidence of PPH and assess its risk factors in this region. The results showed that the incidence of PPH in Tibet was 1.98%, which was lower than that in some other developing countries, such as Pakistan (6%) [14], Uganda (7.4%) [19], and India (22.7%) [20], and some developed countries, such as Japan (8.7%) [10]. The incidence of PPH varies in different countries and regions owing to differences in economic and social development levels, living habits, ethnicity, and medical and health conditions. There were confounding and selection biases in the study samples because only patients registered in hospitals or health centers in Tibet were included to analyze the incidence of PPH, which might have caused the difference in incidence between Tibet and other areas. In this study, maternal age ≥35 years, history of preterm birth, cesarean section, neonatal weight >4 kg, and occurrence of neonatal asphyxia were identified as risk factors for PPH in pregnant women in Tibet.
In the present work, maternal age ≥35 was identified to increase the risk of PPH by 0.96 times. Advanced maternal age leads to a higher risk of PPH [21–23], which can be caused by the decrease in elasticity of the soft birth canal and worsening of uterine contraction with the increase of maternal age. Also, a higher risk of placenta previa and placental abruption occur with advanced maternal age, which increase the possibility of PPH [24]. In our present study, preterm birth was also a risk factor for PPH, and this was supported by the results of several previous studies [25–28]. The present results showed that women with a history of preterm birth exhibited 1.66 times higher risk of having PPH than those without a history of preterm birth. The reason may be that women with preterm deliveries often have pregnancy complications such as placenta previa and premature rupture of membranes, which cause endometrial damage and increase the risk of bleeding [29,30].
Cesarean section is a common choice for obstetricians when they face emergencies such as dystocia. However, the risk of a severe complication such as bleeding, thromboembolism, and infection is much higher in women delivering by cesarean section than by vaginal birth [31]. Previous studies have revealed that compared with vaginal delivery, cesarean section has a significantly higher risk of PPH [14,32], which supports the conclusion of our study. Cesarean section, as an invasive operation, can cause mechanical injury to the body and can cause irritable coagulation disorders. The timing of the cesarean section operation is an important factor affecting the volume of bleeding. Seligman et al indicated that women receiving cesarean sections during delivery often had a higher risk of PPH, compared with women having prenatal cesarean sections [33]. This may be because cesarean sections are often the choice after vaginal delivery failure due to various reasons, such as fetal asphyxia. A long stage of labor results in edema of uterine myofiber, brittleness and thinning of the lower segment of the uterus, and poor uterine contraction, which increase blood loss. In addition, cesarean section can prolong the operation time of parturient women, increasing the volume of blood loss.
In the present study, the data showed that neonatal weight >4 kg could increase the risk of PPH in pregnant women by 2.92 times and was an independent risk factor for PPH. Neonatal weight >4 kg, namely macrosomia, was identified as being associated with the risk of PPH in previous studies. A retrospective cohort study by Davey et al including all pregnant women in Victoria, Australia, demonstrated that macrosomia increases the risk of severe PPH in pregnant women [34]. Another prospective cohort study showed that macrosomia increases the risk of PPH in women in Uganda by 1.18 times [14]. A case-controlled study indicated that fetal macrosomia resulted in more frequent PPH in pregnant women in Tanzania [35]. With the development of the social economy, the living standards of people are generally improved, and pregnant women pay more attention to nutrition and supplementation during pregnancy. Improper nutrition and lack of enough physical exercise make not only pregnant women themselves gain excessive weight, but also increase the risk of macrosomia in the fetus. An oversized fetus is likely to lead to excessive distension of uterine fibers, thinning of the myometrial wall, and poor myofiber contraction, resulting in PPH [14,36]. During vaginal delivery, macrosomia may prolong the first and second stages of labor and result in severe perineal laceration or even perineal incision. When the laboring trial period is too long, obstetricians often choose cesarean section to avoid neonatal asphyxia. Another risk factor for PPH in pregnant women is neonatal asphyxia, which is one of the most serious situations encountered in the clinic [37]. Neonatal asphyxia is associated with advanced maternal age, malpresentation, and prolonged labor process, which all increase the rate of cesarean section and the risk of PPH [38,39]. Closely monitoring fetal heart changes and observing the amniotic fluid for meconium contamination can identify early fetal distress to prevent PPH in time.
A PPH prediction model was successfully established as follows: Y=Logit (
Our study has some limitations. This study included women who received care in different levels of medical institutions, including Grade A urban tertiary hospitals, ordinary county hospitals, and township health centers. The different conditions of the hospitals resulted in a difference in measured postpartum blood loss of the women included in this study. This might have been affected by the regional economies and whether a health care system was well established, among other factors.
Conclusions
Despite significant improvements in biomedicine and reproductive health services and measures such as oxytocin used by obstetricians, PPH rates remain high. In our study, we found maternal age ≥35 years, history of preterm birth, cesarean section, newborn weight >4 kg, and occurrence of neonatal asphyxia were risk factors for PPH in pregnant women in Tibet. These results should remind obstetricians to be especially alert to these risk factors in the prenatal and perinatal period and to provide timely intervention for pregnant women with a high risk of PPH. Obstetricians should make detailed assessments of pregnant women to prevent PPH and optimize pregnancy outcomes.
Tables
Table 1. Univariate analysis of influencing indicators of postpartum hemorrhage (PPH) in Tibet.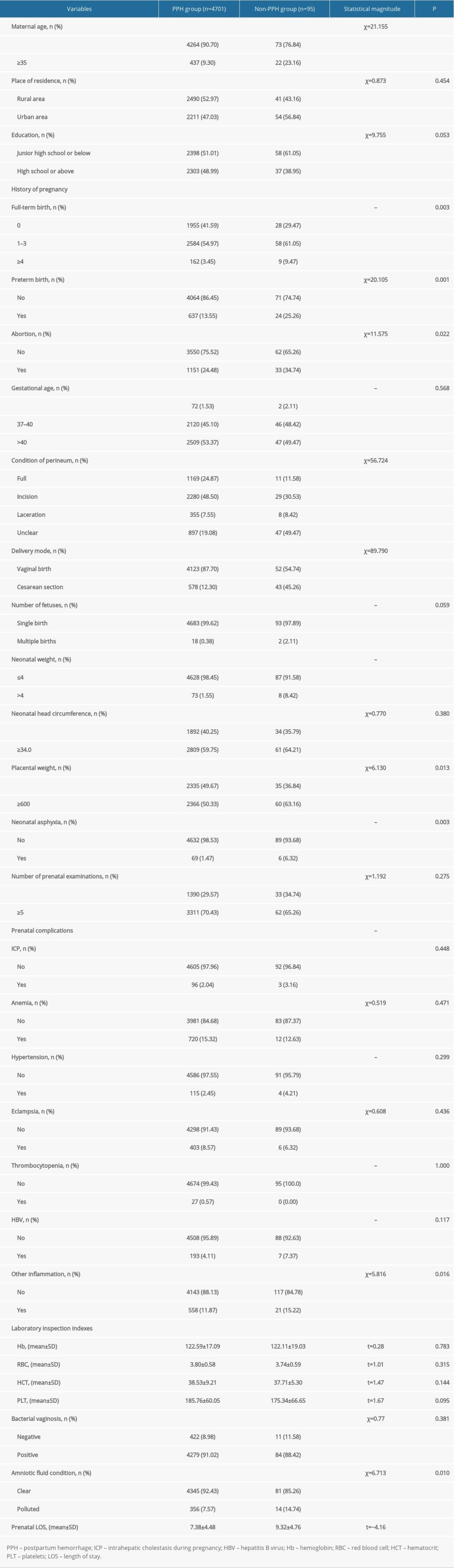 Table 2. Logistic regression analysis of influencing factors of postpartum hemorrhage (PPH) in Tibet.
Table 2. Logistic regression analysis of influencing factors of postpartum hemorrhage (PPH) in Tibet.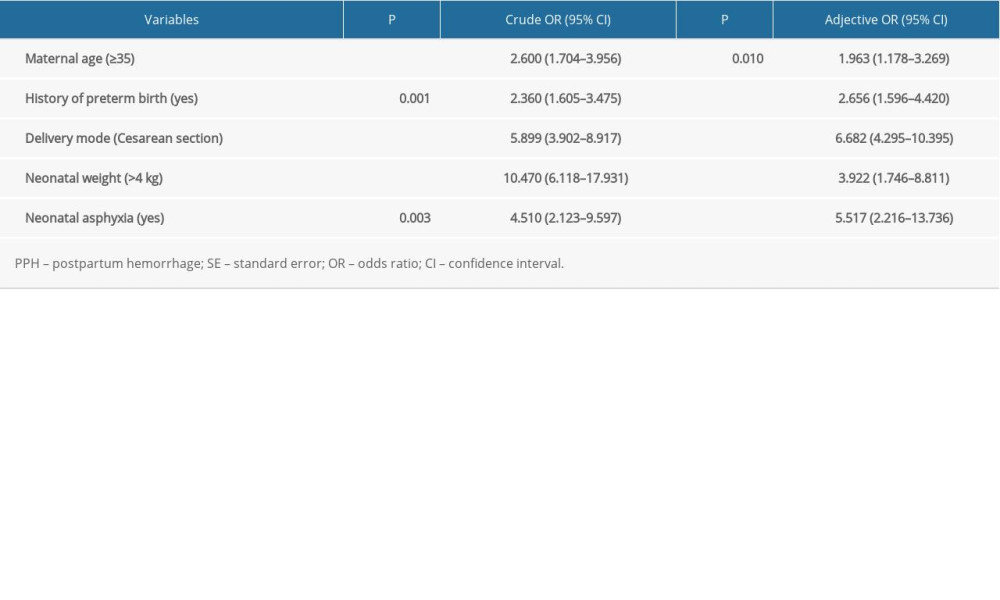 Table 3. The results of receiver operating characteristic (ROC) analysis of the prediction model of postpartum hemorrhage (PPH).
Table 3. The results of receiver operating characteristic (ROC) analysis of the prediction model of postpartum hemorrhage (PPH).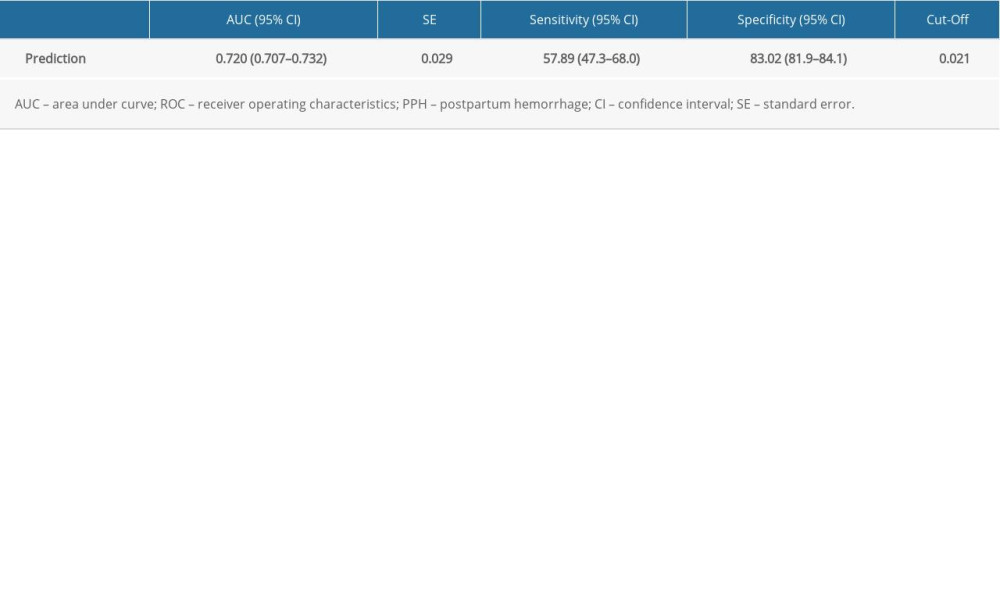
References
1. Zhang WThe influence of nursing intervention on maternal bad mood and postpartum hemorrhage: Journal of Qilu Nursing, 2015; 21(18); 19-21 [in Chinese]
2. Andrikopoulou M, D’Alton ME, Postpartum hemorrhage: Early identification challenges: Semin Perinatol, 2019; 43(1); 11-17
3. Durmaz A, Komurcu N, Relationship between maternal characteristics and postpartum hemorrhage. A meta-analysis study: J Nur Res, 2018; 26(5); 362-72
4. Higgins N, Patel SK, Toledo P, Postpartum hemorrhage revisited: New challenges and solutions: Curr Opinion Anaesthesiol, 2019; 32(3); 278-84
5. Hogan MC, Foreman KJ, Naghavi M, Maternal mortality for 181 countries, 1980–2008: A systematic analysis of progress towards Millennium Development Goal 5: Lancet (London, England), 2010; 375(9726); 1609-23
6. GBD 2015 Maternal Mortality Collaborators, Global, regional, and national levels of maternal mortality, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015: Lancet (London, England), 2016; 388(10053); 1775-812
7. Say L, Chou D, Gemmill A, Global causes of maternal death: A WHO systematic analysis: Lancet Glob Health, 2014; 2(6); e323-33
8. Souza JP, Gülmezoglu AM, Vogel J, Moving beyond essential interventions for reduction of maternal mortality (the WHO Multicountry Survey on Maternal and Newborn Health):A cross-sectional study: Lancet (London, England), 2013; 381(9879); 1747-55
9. Yang YY, Fang YH, Wang X, A retrospective cohort study of risk factors and pregnancy outcomes in 14,014 Chinese pregnant women: Medicine, 2018; 97(33); e11748
10. Fukami T, Koga H, Goto M, Incidence and risk factors for postpartum hemorrhage among transvaginal deliveries at a tertiary perinatal medical facility in Japan: PLoS One, 2019; 14(1); e0208873
11. Lutomski JE, Byrne BM, Devane D, Greene RA, Increasing trends in atonic postpartum haemorrhage in Ireland: An 11-year population-based cohort study: Int J Obstet Gynecol, 2012; 119(3); 306-14
12. Yu SCH, Cheng YKY, Tse WT, Perioperative prophylactic internal iliac artery balloon occlusion in the prevention of postpartum hemorrhage in placenta previa: A randomized controlled trial: Am J Obstet Gynecol, 2020; 223(1); 117.e111-13
13. Feduniw S, Warzecha D, Szymusik I, Wielgos M, Epidemiology, prevention and management of early postpartum hemorrhage – a systematic review: Ginekol Pol, 2020; 91(1); 38-44
14. Ononge S, Mirembe F, Wandabwa J, Campbell OM, Incidence and risk factors for postpartum hemorrhage in Uganda: Reprod Health, 2016; 13; 38
15. Oberg AS, Hernandez-Diaz S, Palmsten K, Patterns of recurrence of postpartum hemorrhage in a large population-based cohort: Am J Obstet Gynecol, 2014; 210(3); 229.e221-28
16. Firmin M, Carles G, Mence B, Postpartum hemorrhage: Incidence, risk factors, and causes in Western French Guiana: J Gynecol Obstet Hum Reprod, 2019; 48(1); 55-60
17. Hawker L, Weeks A, Postpartum haemorrhage (PPH) rates in randomized trials of PPH prophylactic interventions and the effect of underlying participant PPH risk: A meta-analysis: BMC Pregnancy Childbirth, 2020; 20(1); 107
18. Lumbreras-Marquez MI, Reale SC, Carusi DA, Introduction of a novel system for quantitating blood loss after vaginal delivery: A retrospective interrupted time series analysis with concurrent control group: Anesth Analg, 2020; 130(4); 857-68
19. Gani N, Ali TS, Prevalence and factors associated with maternal postpartum haemorrhage in Khyber Agency, Pakistan: J Ayub Med Coll Abbottabad, 2013; 25(1–2); 81-85
20. Ramachandra Bhat PB, Navada MH, Rao SV, Nagarathna G, Evaluation of obstetric admissions to Intensive Care Unit of a tertiary referral center in coastal India: Indian J Crit Care Med, 2013; 17(1); 34-37
21. Zhu C, Wang M, Niu G, Obstetric outcomes of twin pregnancies at advanced maternal age: A retrospective study: Taiwan J Obstet Gynecol, 2018; 57(1); 64-67
22. Lao TT, Sahota DS, Cheng YK, Advanced maternal age and postpartum hemorrhage – risk factor or red herring?: J Matern Fetal Neonatal Med, 2014; 27(3); 243-46
23. Sheen JJ, Wright JD, Goffman D, Maternal age and risk for adverse outcomes: Am J Obstet Gynecol, 2018; 219(4); 390.e1-15
24. Schimmel MS, Bromiker R, Hammerman C, The effects of maternal age and parity on maternal and neonatal outcome: Arch Gynecol Obstet, 2015; 291(4); 793-98
25. Choi SR, Yoon NR, Hwang SO, Is a cause of postpartum hemorrhage of using of tocolytic agents in preterm delivery?: J Matern Fetal Neonatal Med, 2017; 30(22); 2711-15
26. Zafran N, Gerszman E, Garmi G, The impact of postpartum cervical tear on the occurrence of preterm birth in subsequent pregnancy: Arch Gynecol Obstet, 2017; 296(2); 199-204
27. Glavind MT, Møllgaard MV, Iversen ML, Obstetrical outcome in women with endometriosis including spontaneous hemoperitoneum and bowel perforation: A systematic review: Best Pract Res Clin Obstet Gynaecol, 2018; 51; 41-52
28. Reddy UM, Rice MM, Grobman WA, Serious maternal complications after early preterm delivery (24–33 weeks’ gestation): Am J Obstet Gynecol, 2015; 213(4); 538.e531-39
29. Toijonen AE, Heinonen ST, Gissler MVM, Macharey G, A comparison of risk factors for breech presentation in preterm and term labor: A nationwide, population-based case-control study: Arch Gynecol Obstet, 2020; 301(2); 393-403
30. Park CW, Moon KC, Park JS, The frequency and clinical significance of intra-uterine infection and inflammation in patients with placenta previa and preterm labor and intact membranes: Placenta, 2009; 30(7); 613-18
31. Norhayati MN, Nik Hazlina NH, Aniza AA, Sulaiman Z, Factors associated with severe maternal morbidity in Kelantan, Malaysia: A comparative cross-sectional study: BMC Pregnancy Childbirth, 2016; 16(1); 185
32. Butwick AJ, Ramachandran B, Hegde P, Risk factors for severe postpartum hemorrhage after cesarean delivery: Case-control studies: Anesth Analg, 2017; 125(2); 523-32
33. Seligman K, Ramachandran B, Hegde P, Obstetric interventions and maternal morbidity among women who experience severe postpartum hemorrhage during cesarean delivery: Int J Obstet Anesth, 2017; 31; 27-36
34. Davey MA, Flood M, Pollock W, Risk factors for severe postpartum haemorrhage: A population-based retrospective cohort study: Aust NZJ Obstet Gynaecol, 2020; 60(4); 522-32
35. Said AS, Manji KP, Risk factors and outcomes of fetal macrosomia in a tertiary centre in Tanzania: A case-control study: BMC Pregnancy Childbirth, 2016; 16(1); 243
36. Prapawichar P, Ratinthorn A, Utriyaprasit K, Viwatwongkasem C, Maternal and health service predictors of postpartum hemorrhage across 14 district, general and regional hospitals in Thailand: BMC Pregnancy Childbirth, 2020; 20(1); 172
37. Paul V, Neonatal morbidity and mortality: Report of the national neonatal and perinatal database: Indian Pediatr, 1999; 36(2); 167-69
38. Abdo RA, Halil HM, Kebede BA, Prevalence and contributing factors of birth asphyxia among the neonates delivered at Nigist Eleni Mohammed memorial teaching hospital, Southern Ethiopia: A cross-sectional study: BMC Pregnancy Childbirth, 2019; 19(1); 536
39. Sun M, Song X, Shi W, Delayed umbilical cord clamping in cesarean section reduces postpartum bleeding and the rate of severe asphyxia: Clin Exp Obstet Gynecol, 2017; 44(1); 14-16
Figures
Tables
Table 1. Univariate analysis of influencing indicators of postpartum hemorrhage (PPH) in Tibet.Table 2. Logistic regression analysis of influencing factors of postpartum hemorrhage (PPH) in Tibet.Table 3. The results of receiver operating characteristic (ROC) analysis of the prediction model of postpartum hemorrhage (PPH).Table 1. Univariate analysis of influencing indicators of postpartum hemorrhage (PPH) in Tibet.Table 2. Logistic regression analysis of influencing factors of postpartum hemorrhage (PPH) in Tibet.Table 3. The results of receiver operating characteristic (ROC) analysis of the prediction model of postpartum hemorrhage (PPH). In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387