05 April 2021: Clinical Research
Extra-Thyroid Extension Prediction by Ultrasound Quantitative Method Based on Thyroid Capsule Response Evaluation
Minghang Lin12BF, Yiming Su3CDF, Weili Wei2BCE, Yiran Gong2BC, Yinan Huang2BCE, Jinshu Zeng2DEFG, Liya Li4BCF, Haihong Shi4B, Shuqiang Chen2ABCDEFG*DOI: 10.12659/MSM.929408
Med Sci Monit 2021; 27:e929408






Abstract
BACKGROUND: The aim of this study was to assess the interaction between thyroid malignancies and thyroid anterior capsule by ultrasound quantification to determine extra-capsular invasion.
MATERIAL AND METHODS: A total of 145 patients preoperatively diagnosed with malignant nodules under the thyroid anterior capsule were selected and routinely examined by ultrasound. The length of the nodules (from the junction of the nodule capsule to the deepest point of the nodule, vertical diameter, V) and the distance between the nodule protruding from thyroid capsule and the highest protruding (ledge length, L) nodule were used to obtain the L/V ratio. These parameters where then used to compare the efficacy of predicting extra-thyroid extension (ETE) between L/V, the aspect ratio of the tumor, and manual judgment.
RESULTS: Out of 145 nodules, there were 63 ETEs and 82 non-ETEs determined by ultrasound. Extra-capsular invasion was associated with L//V ratio, but there was no significant correlation between capsular invasion and AR (aspect ratio), age, location, or presence of clustered calcification. The ability of the ratio of L/V to predict extra-capsular invasion was superior to the predictive ability of the AR ratio. With a Youden index of 0.593, the L/V ratio was 0.2325. The use of the L/V ratio to determine the presence of ETE was superior to subjective visual judgment.
CONCLUSIONS: The calculation of L/V ratio by ultrasound could more precisely predict the ETE compared with manual judgment, which indirectly reflects the interaction between thyroid capsule and malignant nodules. The above conclusions need to be confirmed by a range of cases.
Keywords: Ultrasonography, Carcinoma, Papillary, Diagnosis, Differential, Thyroid Gland
Background
Compared with other malignant tumors, the incidence of thyroid cancer has increased significantly in the past 20 years. One of the important reasons for this spike is the widespread use of ultrasound for diagnosis [1]. Due to the continuous improvement of high-frequency probes, combined with elasticity, fine-needle aspiration (FNA), and gene detection, ultrasound can detect thyroid microcarcinomas as small as 2 mm in diameter, allowing an in-depth assessment of the invasiveness of the tumor [2]. Therefore, ultrasound has become the preferred and primary method for thyroid imaging [3]. Most thyroid papillary carcinomas are associated with a good prognosis, and those with marked invasiveness attract particular attention. On the other hand, studies have shown that the invasiveness and recurrence of thyroid papillary carcinoma with thyroid capsule protrusion is associated with a poor prognosis [4]. A prominent thyroid cancer known as extra-thyroid extension (ETE) has become one of the main indicators for evaluating patient prognosis, and it has been the focus of much clinical study. In the 8th edition of American Joint Committee on Cancer (AJCC)/Tumor Node Metastasis (TNM) staging system of thyroid cancer, T3b was introduced for tumors with macroscopic ETE limited to the strap muscles [5]. This focus on T3b involves paying more attention to the ETE. Comparatively, the judgment of ETE has been historically subjective, based on the thin thyroid capsule, and rife with error. Study have previously demonstrated that the degree of contact between the nodule and the capsule, the bulging of the thyroid capsule contour, echo disruption, etc are valuable for predicting extra-capsular invasion, though these indicators still mainly rely on the examiner’s subjective visual judgement [6]. There is no standardized index for the ultrasonographic evaluation of ETE at present. Furthermore, due to the aggressive growth of malignant thyroid nodules, various complex interactions of the tumor tissue with the thyroid capsule may occur during the invasion process, especially nodules close to capsule, such that the capsule may have various reactions to the infringement. This study intended to use the advantages of the spatial resolution of high-frequency ultrasound to evaluate ETE quantitatively, based on the relationship between the capsule and thyroid tumors.
Material and Methods
PATIENT INFORMATION:
This retrospective study was approved by the Institutional Ethics Review Board (with the instructions of FYYY-2017-201), who determined that informed consent from the enrolled patients was not required. All patients enrolled in the study were hospitalized for thyroid cancer as confirmed by FNA. A total of 145 patients were enrolled. Preoperative ultrasound examinations were performed routinely by trained personnel. The time interval between surgery and ultrasonography was less than 3 days. The enrolled patient’s nodules were located under the anterior capsule of thyroid gland. The term “subcapsular” was used to define the absence of thyroid tissue between the anterior capsule and the nodule, which is the marginal region. Exclusion criteria for enrollment included suspicion of having 2 or more malignant thyroid nodules.
EXAMINATION PROCEDURE:
The patient was placed in a supine position and the anterior cervical region was fully exposed. Routine scanning of the bilateral thyroid glands and isthmus was performed by two-dimensional ultrasound observation (GE LOGIC E9, using a 6–15 high-frequency linear array probe) including thyroid nodules site, size, shape, number, boundary, presence of sound halo, nodule internal echo, and calcification. Additional evaluation included rear echo attenuation, neck enlarged lymph nodes, and other abnormalities. At the same time, the aspect ratio (AR) was calculated and the relationship between the nodule and the capsule was observed. Sufficient couplant was applied to confirm that there was no echo between the probe and the skin to avoid pressure on the thyroid tissue. The vertical diameter of the nodule (vertical diameter, V) was measured from the junction of the nodule envelope to the deepest part of nodule, and the ledge length (L) of the protruding thyroid capsule from the nodule were measured. Each value was measured 3 times to get the average. Storage L/V value (measurement method shown in Figure 1) and nodule aspect ratio were measured for each nodule. Ultrasound images of thyroid nodules were collected by 2 sonographers with more than 10 years of working experience who were blinded to the pathological findings of the nodules. Take the average value of the measurement results and make the consistency test. Finally, pathological data were recorded after the initial examination, particularly pathological results such as tumor invasion of the thyroid capsule and extra-thyroid tissue.
STATEMENT OF ETHICS:
This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. This retrospective study was approved by the Institutional Ethics Review Board of the First Affiliated Hospital of Fujian Medical University, Fuzhou, China (with the instructions of FYYY-2017-201), which determined that informed consent from the enrolled patients was not required.
STATISTICS:
Data were coded and stored in an Excel file. Statistical analysis was performed using the SPSS 17 software package. Independent-sample
Results
CONSISTENCY TEST:
The ultrasonic analysis results of the 2 physicians were consistent (Kappa value=0.852, P<0.01) General features of the 2 groups (ETE and non-ETE) are listed in Table 1. The above table demonstrates the correlation between capsular invasion and LV ratio. There was no correlation between capsular invasion and AR, age, location, or presence of clustered calcified plaques.
ULTRASOUND AND INTRAOPERATIVE FEATURES OF CAPSULAR INVASION:
The extra-capsular violation manifested as the original smooth morphology of the capsule disappeared and the tumor contact surface of the capsule became stiff. The surrounding capsule bulge was not obvious during this phase, and the L/V ratio was relatively low (Figure 2A). In some of the more obviously invaded tumors, the continuity of the anterior capsule was interrupted, manifesting as an invasion within the anterior cervical muscles, where it was apparent that the capsule was disordered. Intraoperative pathology showed that the continuity of the thyroid capsule was interrupted. The fish-meat-like tumor tissue broke through the thyroid capsule on the cut surface (Figure 2B). In some severely invaded patients, the tumor invaded the neck muscles. Tumors that did not show extra-capsular invasion showed good continuity of the capsule that was in contact with the tumor. The capsule in these cases retained the original curvature, and the L/V was small (Figure 3A). The continuity of the capsule was apparent during surgery. The subcapsular tumor was observed by dissection of the capsule (Figure 3B).
L/V-AR RATIO ROC CURVE:
Two methods, L/V and A/R ratio, were used to determine ETE. The ROC curves (Figure 4) were produced to calculate the AUC. The AUC of L/V was 0.0872, which was superior to that of the A/R ratio (Z=13.597, P<0.01).
CHI-SQUARE EVALUATION OF MANUAL JUDGMENT VERSUS L/V:
In the inspection process, 3 ultrasound technicians with more than 10 years of experience in thyroid diagnosis were invited to jointly determine whether there was an occurrence of extra-thyroidal invasion. The group consensus was obtained as the final opinion. The L/V ratio of 0.2325 and Youden index of 0.593 were used as the cutoff values to determine the invasion criteria. These were then compared with the manual judgment by the chi-square test as shown in Table 2. The postoperative pathology was used as the criterion standard.
Chi-square test results showed that the accuracy of manual judgment was 79.31%, and the accuracy of L/V judgment was 88.27%. Chi-square testing showed that the difference between the 2 assessments was statistically significant (
Discussion
Most thyroid papillary carcinomas show a slow and inert growth pattern. Overall, the prognosis is good. The 5-year survival rate is currently over 90% [7,8]. However, there is a significant proportion of thyroid papillary carcinoma patients that experience recurrence. Due to different follow-up times, the recurrence rate ranges anywhere from 20% to 35% [9,10]. Numerous studies have reported that extra-capsular invasion in preoperative examination is one of the most important independent risk factors affecting the recurrence rate of thyroid cancer [4,8]. Minimal neck muscle invasion is common during surgery and although it does not significantly affect surgical strategies [4], the impact on its long-term (more than 10 years) relapse rate remains unknown. Whether or not an extra-thyroidal invasion has been found after the operation also helps determine whether to expand the range of surgery and whether iodine treatment is needed [5]. Therefore, giving sufficient attention can significantly reduce tumor recurrence rate and improve disease prognosis. Ultrasound is the most important imaging tool for assessing the nature of thyroid tumors before surgery as well as for providing references during surgery. Ultrasound can show the fine features of the thyroid tumors and show the relationship between the tumor and the adjacent tissues of the neck. In terms of ETE, ultrasound can also identify the relationship between the thyroid capsule and the anterior cervical muscle group.
The composition of the thyroid capsule is a double-layered envelope. The outer layer is called the surgical or pseudo-enveloped membrane, while the inner layer is called the true envelope. The thyroid gland is situated between the 2 envelopes. There is a certain amount of fat and other connective tissue between the 2 thyroid capsules or between the surgical capsule and the neck muscles [11]. Malignant nodules including thyroid cancer (papillary or medullary carcinoma, among others) are generally invasive. When the tumor is enlarged to the extent of the capsule, it invades the thyroid capsule and subsequently, the surrounding tissue (primarily the anterior cervical muscle group (neck), and the tissues around the trachea) [12]. Benign nodules, including thyroma and nodular goiters, are quite the opposite, exhibiting an inflated tumor with associated fiber capsule. Even when the tumor grows to touch the thyroid dorsal membrane, there is still a demarcation between the tumor tissue and the capsule. On the other hand, when extra-thyroid invasion occurs, the neck muscles are often the first to be invaded, followed by the nerves, trachea, and central lymph nodes. This can explain the results of this study, wherein the tumors with thyroid capsular invasion exhibited a less significant protrusion than those that did not invade. Studies have shown that the invasion of trachea and central lymph node tissues often indicates a sign of poor prognosis, being closely related to the stage of thyroid cancer and the scope of the expansion of surgery. Some scholars have also proposed the identification of skeletal muscle invasion as a more reliable histological criterion of ETE [13]. Therefore, it is particularly important to find out when invasion occurs only in the neck muscles versus those tumors that are likely to invade beyond the thyroid capsule.
In this study, the thyroid capsular connecting line was taken as the normal line, and the vertical distance between the apex of the thyroid capsular nodule and the normal line was considered as the degree of tumor extension. Considering the variable size of the thyroid nodule itself, in order to correct the maximum longitudinal diameter of the nodule, we used L/V ratio as a criterion. The results of this study show that tumors with extra-capsular invasion appear to be less prominent on ultrasound than non-encapsulated invasive tumors.
The aspect ratio (AR) has been recognized by the ATA (American Thyroid Association) and other agencies as one of the hallmarks of thyroid cancer, due to its indication of the growth pattern of the tumor. The AR ratio reflects the relationship between the thyroid tumor and capsule. The results of this study suggest that L/V ratio is more predictive than the AR ratio for EET detection, which is consistent with the biological characteristics of papillary thyroid carcinoma. In the course of this study, our experience was that the 2 parameters often agree with each other. If both L/V ratio and AR ratio have characteristic significance, we need to pay special attention to follow-up or suggest further treatment.
At present, the use of ultrasound to judge thyroid cancer extra-capsular invasion mostly depends on visual judgement and personal experiences [6]. Since thyroid tumors are close to the capsule, the relationship between the tumor, the capsule, and the neck muscles is difficult to distinguish with the naked eye, often prompting probing and squeezing by the examining physician and increasing the likelihood of error. In contrast, quantitative methods like ultrasound are very helpful for accurate assessment. Of course, in actual practice, it is not likely that the examining physician would rely solely on a single parameter, but would rather use multiple methods. In addition, some scholars have pointed out that ultrasonic texture features show great significance in predicting malignant potential, but their role in predicting ETE needs further study [14].
This study sought to gauge the value of ultrasound in quantitatively determining tumor invasion of the thyroid envelope. However, this ratio cannot be used as a cutoff value. As a non-standardized imaging method, there are some subjective errors in ultrasound, such as the choice of angle, maximum radial measurement of nodules, and the determination of the normal line. Another variable of ultrasound of the neck is the resulting differences in strength that are inherent due to scan probe placement. Error can be introduced with any of these factors and it should be considered that each can have a slight impact on the L/V value and should be thoughtfully considered as such. Additionally, some of the limitations of this study include the lack of a longitudinal follow-up period, wherein it could be possible to confirm the long-term recurrence rate and patient survival. It is suggested that multiple scanning measurements should be performed to obtain a weighted average.
Conclusions
The calculation of L/V ratio by ultrasound can more precisely predict the ETE compared with manual judgment, which indirectly reflects the interaction between thyroid capsule and malignant nodules. The above conclusions need to be confirmed by a range of cases.
Figures
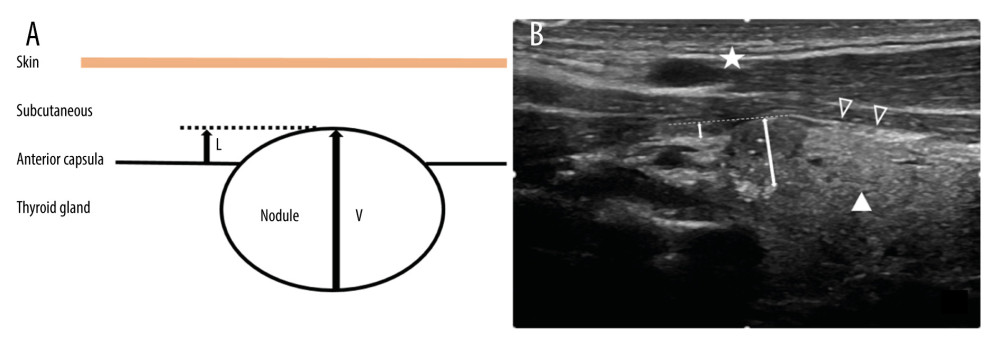 Figure 1. Schematic of the L/V measurement method (A). Actual diagram of L/V measurement method (B). The icons represent subcutaneous tissue (white pentagram), anterior capsula (white hollow triangle) and thyroid gland (white solid triangle) (B). The short double arrow represents the L value, which is the ledge length of the protruding thyroid capsule from the nodule. The long double arrow represents the V value, which is the vertical diameter of the nodule (B).
Figure 1. Schematic of the L/V measurement method (A). Actual diagram of L/V measurement method (B). The icons represent subcutaneous tissue (white pentagram), anterior capsula (white hollow triangle) and thyroid gland (white solid triangle) (B). The short double arrow represents the L value, which is the ledge length of the protruding thyroid capsule from the nodule. The long double arrow represents the V value, which is the vertical diameter of the nodule (B). 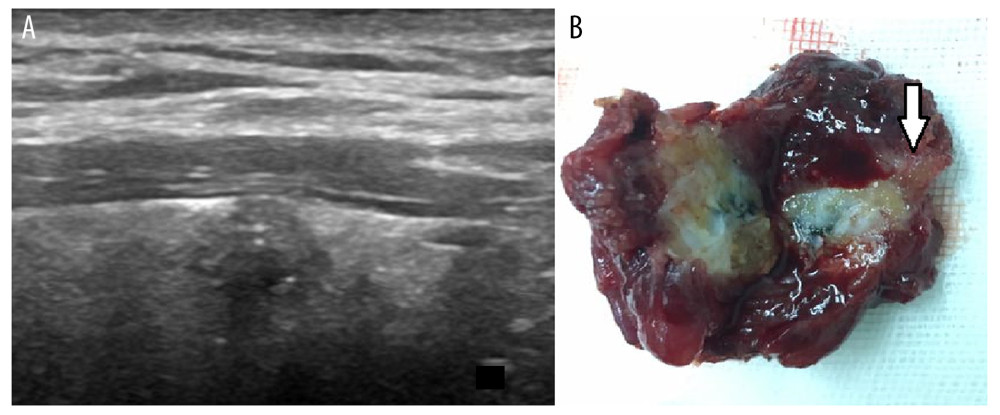 Figure 2. Papillary carcinoma of the thyroid gland with extra-capsular invasion (A). A flat nodule is seen in the thyroid gland with no prominent bulge, and the L/V ratio is 0.17, showing that the tumor invaded the thyroid capsule and the anterior cervical muscle (arrow) (B).
Figure 2. Papillary carcinoma of the thyroid gland with extra-capsular invasion (A). A flat nodule is seen in the thyroid gland with no prominent bulge, and the L/V ratio is 0.17, showing that the tumor invaded the thyroid capsule and the anterior cervical muscle (arrow) (B). 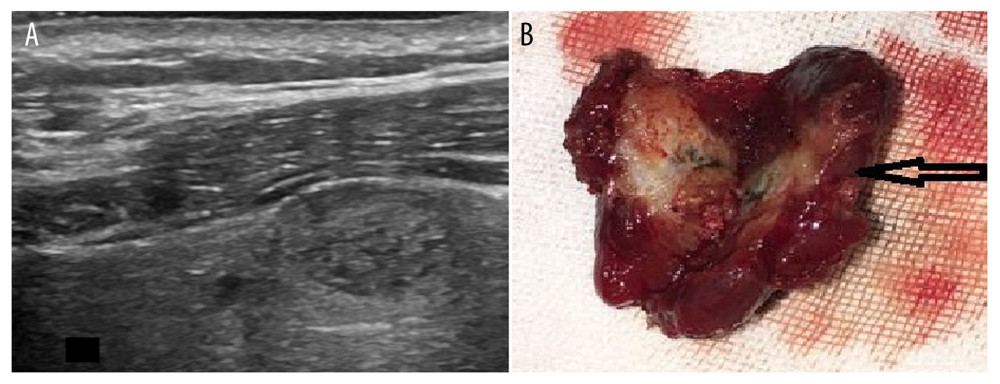 Figure 3. Papillary carcinoma of the thyroid gland without extra-capsular invasion. Ultrasonographic findings of the apparent uplift of the nodule, L/V ratio of 0.34 (A); intact thyroid capsule (B).
Figure 3. Papillary carcinoma of the thyroid gland without extra-capsular invasion. Ultrasonographic findings of the apparent uplift of the nodule, L/V ratio of 0.34 (A); intact thyroid capsule (B). 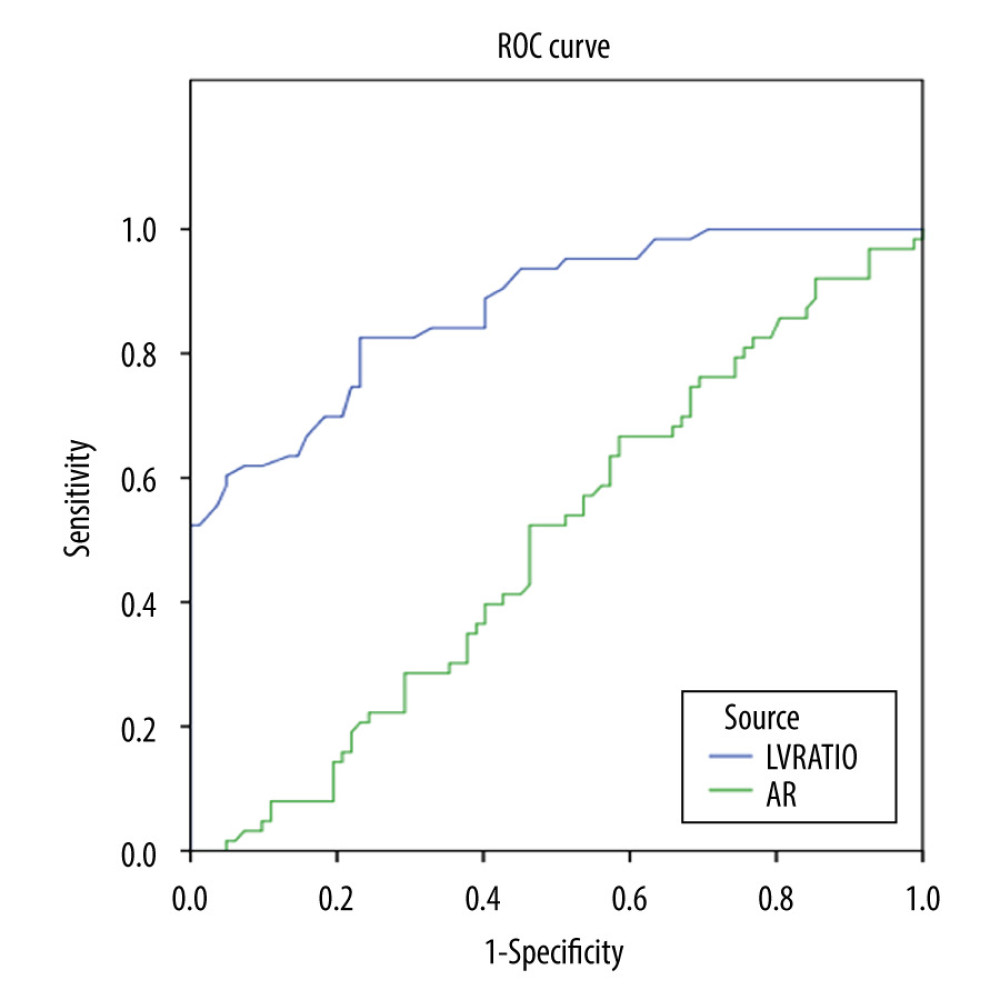 Figure 4. L/V-AR ratio ROC curve. The AUCs of AR and L/V ratios were 0.0872 and 0.496, respectively. After Z testing, the Z value was 13.597, P<0.01. Statistical analysis revealed that the efficacy of using the L/V ratio to judge extra-capsular invasion is better than use of the AR ratio. The Youden index was 0.593 and the L/V ratio was 0.2325.
Figure 4. L/V-AR ratio ROC curve. The AUCs of AR and L/V ratios were 0.0872 and 0.496, respectively. After Z testing, the Z value was 13.597, P<0.01. Statistical analysis revealed that the efficacy of using the L/V ratio to judge extra-capsular invasion is better than use of the AR ratio. The Youden index was 0.593 and the L/V ratio was 0.2325. Tables
Table 1. The correlation between capsular invasion and LV ratio. There was no correlation between capsular invasion and AR, age, location, or presence of clustered calcified plaques.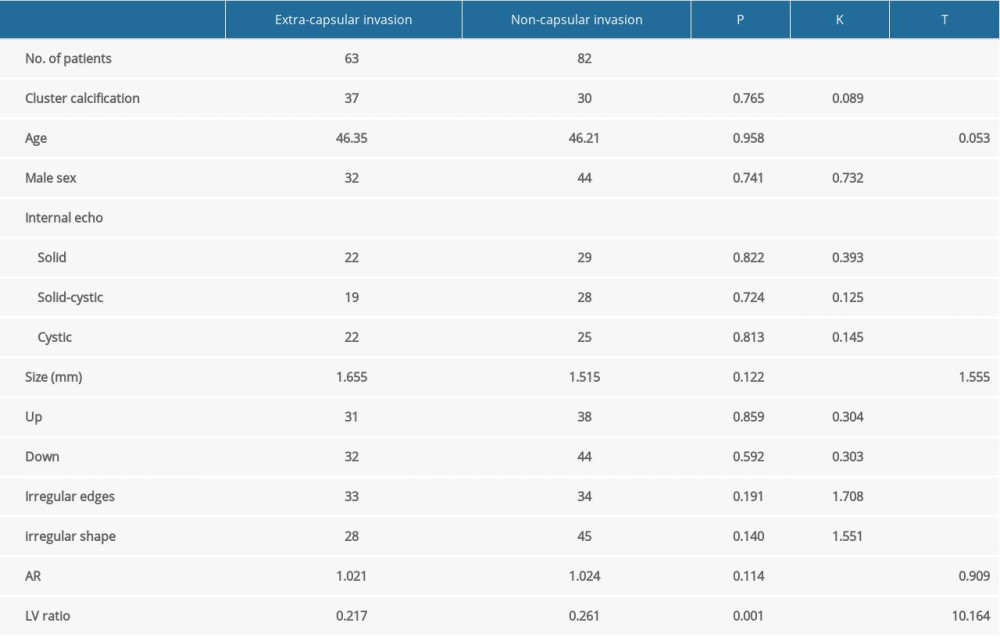 Table 2. Chi-square test: The accuracy of manual judgment was 79.31%, and the accuracy of LV judgment was 88.27%. Chi-square testing showed the difference between the 2 assessments was statistically significant (P<0.05).
Table 2. Chi-square test: The accuracy of manual judgment was 79.31%, and the accuracy of LV judgment was 88.27%. Chi-square testing showed the difference between the 2 assessments was statistically significant (P<0.05).
References
1. Vigneri R, Malandrino P, Vigneri P, The changing epidemiology of thyroid cancer: Curr Opin Oncol, 2015; 27(1); 1-7
2. Onenerk AM, Pusztaszeri MP, Canberk S, Faquin WC, Triage of the indeterminate thyroid aspirate: What are the options for the practicing cytopathologist?: Cancer, 2017; 125(S6); 477-85
3. Na DG, Baek JH, Sung JY, Thyroid imaging reporting and data system risk stratification of thyroid nodules: Categorization based on solidity and echogenicity: Thyroid, 2016; 26(4); 562-72
4. Kim SY, Kwak JY, Kim EK, Association of preoperative US features and recurrence in patients with classic papillary thyroid carcinoma: Radiology, 2015; 277(2); 574-83
5. Lamartina L, Borget I, Mirghani H, Surgery for neck recurrence of differentiated thyroid cancer: Outcomes and risk factors: J Clin Endocrinol Metab, 2017; 102(3); 1020-31
6. Kamaya A, Tahvildari AM, Patel BN, Sonographic detection of extra-capsular extension in papillary thyroid cancer: J Ultrasound Med, 2015; 34(12); 2225-30
7. Pires BP, Alves PA, Bordallo MA, Prognostic factors for early and long-term remission in pediatric differentiated thyroid carcinoma: The role of sex, age, clinical presentation, and the newly proposed american thyroid association risk stratification system: Thyroid, 2016; 26(10); 1480-87
8. Cooper DS, Doherty GM, Haugen BR, Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer: Thyroid, 2009; 19(11); 1167-214
9. Lee SG, Lee WK, Lee HS, Practical performance of the 2015 American Thyroid Association guidelines for predicting tumor recurrence in patients with papillary thyroid cancer in South Korea: Thyroid, 2017; 27(2); 174-81
10. Kim SH, Roh JL, Gong G, Differences in the recurrence and survival of patients with symptomatic and asymptomatic papillary thyroid carcinoma: An observational study of 11,265 person-years of follow-up: Thyroid, 2016; 26(10); 1472-79
11. Wang Q-C, Cheng W, Wen X, Shorter distance between the nodule and capsule has greater risk of cervical lymph node metastasis in papillary thyroid carcinoma: Asian Pac J Cancer Prev, 2014; 15; 855-60
12. Pacini F, Castagna MG, Approach to and treatment of differentiated thyroid carcinoma: Med Clin North Am, 2012; 96(2); 369-83
13. Mete O, Rotstein L, Asa SL, Controversies in thyroid pathology: Thyroid capsule invasion and extrathyroidal extension: Ann Surg Oncol, 2010; 17(2); 386-91
14. Nieniewski M, Chmielewski LJ, Study of classification of breast lesions using texture GLCM features obtained from the raw ultrasound signal: Image Analysis and Stereology, 2020; 39(2); 129-45
Figures
Figure 1. Schematic of the L/V measurement method (A). Actual diagram of L/V measurement method (B). The icons represent subcutaneous tissue (white pentagram), anterior capsula (white hollow triangle) and thyroid gland (white solid triangle) (B). The short double arrow represents the L value, which is the ledge length of the protruding thyroid capsule from the nodule. The long double arrow represents the V value, which is the vertical diameter of the nodule (B).Figure 2. Papillary carcinoma of the thyroid gland with extra-capsular invasion (A). A flat nodule is seen in the thyroid gland with no prominent bulge, and the L/V ratio is 0.17, showing that the tumor invaded the thyroid capsule and the anterior cervical muscle (arrow) (B).Figure 3. Papillary carcinoma of the thyroid gland without extra-capsular invasion. Ultrasonographic findings of the apparent uplift of the nodule, L/V ratio of 0.34 (A); intact thyroid capsule (B).Figure 4. L/V-AR ratio ROC curve. The AUCs of AR and L/V ratios were 0.0872 and 0.496, respectively. After Z testing, the Z value was 13.597, P<0.01. Statistical analysis revealed that the efficacy of using the L/V ratio to judge extra-capsular invasion is better than use of the AR ratio. The Youden index was 0.593 and the L/V ratio was 0.2325. Tables
Table 1. The correlation between capsular invasion and LV ratio. There was no correlation between capsular invasion and AR, age, location, or presence of clustered calcified plaques.Table 2. Chi-square test: The accuracy of manual judgment was 79.31%, and the accuracy of LV judgment was 88.27%. Chi-square testing showed the difference between the 2 assessments was statistically significant (P<0.05).Table 1. The correlation between capsular invasion and LV ratio. There was no correlation between capsular invasion and AR, age, location, or presence of clustered calcified plaques.Table 2. Chi-square test: The accuracy of manual judgment was 79.31%, and the accuracy of LV judgment was 88.27%. Chi-square testing showed the difference between the 2 assessments was statistically significant (P<0.05). In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387