03 January 2021: Clinical Research
Co-Infection with Common Respiratory Pathogens and SARS-CoV-2 in Patients with COVID-19 Pneumonia and Laboratory Biochemistry Findings: A Retrospective Cross-Sectional Study of 78 Patients from a Single Center in China
Man-Ling Tang1ABCDEF, Yue-Qiu Li2BCDF, Xiang Chen1BCDF, Hui Lin1BCD, Zhong-Chun Jiang2BCD, Dai-Li Gu2BCD, Xun Chen2BCF, Cai-Xi Tang2ACDF, Zhi-Qin Xie2ABCDEFG*DOI: 10.12659/MSM.929783
Med Sci Monit 2021; 27:e929783






Abstract
BACKGROUND: This retrospective study aimed to investigate co-infections with common respiratory pathogens and SARS-CoV-2 and laboratory biochemistry findings in patients with COVID-19 in the Zhuzhou area of China, in order to provide a reference for the disease assessment and clinical treatment of COVID-19.
MATERIAL AND METHODS: The clinical data of COVID-19 patients admitted to the hospital of Zhuzhou City from January 28 to March 15, 2020, as well as laboratory test results for respiratory pathogens and biochemical indicators, were collected to conduct correlation analyses. All patients were diagnosed based on fluorescence-based PCR assay for SARS-CoV-2.
RESULTS: Eleven of the 78 patients (14.1%) were co-infected with other respiratory pathogens, among which Mycoplasma pneumoniae (n=5, 45.5%) and respiratory syncytial virus (n=4, 36.4%) were the most frequent. There were 8 patients co-infected with 1 other pathogen and 3 patients co-infected with 2 other pathogens. Compared with mono-infected COVID-19 patients, patients with co-infections had significantly higher levels of procalcitonin (P=0.002).
CONCLUSIONS: The findings showed that Mycoplasma pneumonia and respiratory syncytial virus were the most common co-infections in patients with COVID-19 pneumonia. Increased levels of PCT in patients with COVID-19 pneumonia were associated with co-infection.
Keywords: coinfection, COVID-19, Mycoplasma pneumoniae, Respiratory Syncytial Viruses, SARS Virus, Adolescent, Aged, 80 and over, Anti-Infective Agents, C-Reactive Protein, COVID-19, COVID-19 Nucleic Acid Testing, Child, Child, Preschool, creatine kinase, Cross-Sectional Studies, L-Lactate Dehydrogenase, Pandemics, Pneumonia, Mycoplasma, procalcitonin, Respiratory Syncytial Virus Infections, Respiratory Tract Infections, SARS-CoV-2, Severity of Illness Index, young adult
Background
Coronavirus disease 2019 (COVID-19) is a new infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which is transmitted through respiratory droplets and physical contact, with a high level of susceptibility in humans [1]. The main manifestations of COVID-19 are fever, fatigue, and dry cough, and most patients have a good prognosis. Individuals with COVID-19 tend to have mild symptoms that can be easily overlooked in the early stages, while severely ill patients rapidly develop acute respiratory distress syndrome and sepsis, which can lead to death from multiple organ failure [2,3]. SARS-CoV-2 is a positive-sense, single-stranded ribonucleic acid virus belonging to the genus
Despite the high transmissibility of SARS-CoV-2, the vast majority of infected individuals are either mildly ill with mild clinical symptoms and no imaging manifestation of pneumonia or moderately ill with a fever and respiratory symptoms and imaging manifestations of pneumonia, while about 20% of those infected progress to severe illness [2,3,6]. In the Northern Hemisphere, the COVID-19 outbreak occurred during the high-incidence season of other respiratory infections, such as influenza, viral pneumonia, and community-acquired pneumonia. Many individuals with SARS-CoV-2 infection have co-infection with other respiratory pathogens [7,8], which complicates the diagnosis and treatment of COVID-19. Hence, the differentiation between SARS-CoV-2 mono-infection and SARS-CoV-2 co-infection with other pathogens is of great importance to clinical management. To this end, we investigated co-infections among hospitalized COVID-19 patients. This retrospective study investigated co-infections with common respiratory pathogens and SARS-CoV-2 and laboratory biochemistry findings in patients with COVID-19 pneumonia to provide a reference for the disease assessment and clinical treatment of COVID-19. Our study shows that
Material and Methods
RESEARCH PARTICIPANTS:
The study was approved by the Ethics Committee of Zhuzhou Central Hospital in 2020 (No. 2020216). All data used were obtained from the electronic medical record system and the paper medical record system. In order not to disturb the patients, we applied to the Ethics Committee for exemption from informed consent and obtained approval.
We performed a retrospective analysis of the clinical data of 78 consecutive COVID-19 patients who were admitted to the People’s Hospital of Lukou District in China, the designated hospital for the isolation and treatment of COVID-19 patients in Zhuzhou City, between January 28 and March 15, 2020. Those patients consisted of 41 men and 37 women with an average age of 47.7±17.2 years.
REAGENTS AND INSTRUMENTS:
SARS-CoV-2 infection was confirmed using the 2019-nCoV Nucleic Acid Detection Kit (fluorescence-based PCR assay) and fully automated nucleic acid extraction instrument (Sansure Biotech, Inc., Changsha, China) [9,10]. We used immunoglobulin M antibody detection kits for 9 other respiratory pathogens (Legionella pneumophila, Coxiella burnetii, influenza A virus, influenza B virus, M. pneumoniae, Chlamydia pneumoniae, RSV, adenoviruses, and human parainfluenza virus) (Autobio Diagnostics Co., Ltd., Zhengzhou, China); a SYSMEXN 1000 fully automated hematology analyzer and its supporting reagents (Sysmex Corp., Hyogo, Japan); a CS2000 fully automated coagulation analyzer and its supporting reagents (Sysmex Corporation, Hyogo, Japan); a Hitachi 7180 fully automated biochemical analyzer and its supporting reagents (Maccura Biotechnology Co., Ltd., Sichuan, China); and FS-301, a Finecare fully automated immunofluorescence quantitative test system (Guangzhou Wanfu Biotechnology Co., Ltd., Guangzhou, China).
DIAGNOSTIC METHODS AND CLINICAL SEVERITY CLASSIFICATION:
According to the criteria outlined in the Diagnosis and Treatment Protocol for COVID-19 (Trial Version 7) issued by the General Office of the National Health Commission on February 18, 2020 [10], we collected the clinical data of patients whose specimens (such as sputum, oropharyngeal swabs, and lower respiratory tract secretions) tested positive for SARS-CoV-2 nucleic acid via real-time fluorescence-based polymerase chain reaction (RT-PCR) assay. All 78 patients with COVID-19 in our hospital were tested for respiratory pathogens. If the patient was infected with COVID-19 and other respiratory pathogens, we diagnosed co-infection. If the patient was infected with COVID-19 but was not infected with other respiratory pathogens, we diagnosed mono-infection. The 78 patients were divided into mildly ill (8 patients), moderately ill (59 patients), severely ill (9 patients), and critically ill (2 patients) groups. The mildly ill group comprised patients who had mild clinical symptoms and showed no imaging manifestation of pneumonia. The moderately ill group comprised patients who had a fever and respiratory symptoms and showed imaging manifestations of pneumonia. The severely ill group comprised patients who met any of the following criteria: RDS with a respiratory rate of ≥30 breaths/min, blood oxygen saturation levels (SpO2) ≤93% at rest, or partial pressure of oxygen (paO2)/fraction of inspired oxygen (FiO2) in arterial blood ≤300 mmHg. The critically ill group comprised patients who met any of the following criteria: the need for mechanical ventilation due to respiratory failure, shock, or the need for monitoring and treatment in the Intensive Care Unit (ICU) due to failures of other organs.
STATISTICAL METHODS:
Descriptive analyses of the variables produced data expressed as the median and interquartile range (IQR), mean±standard deviation, or number (%), as appropriate. For comparisons between experimental groups, statistical data that met the assumption of homogeneity of variance (
Results
COMPARISONS OF CLINICAL CHARACTERISTICS BETWEEN CO-INFECTED AND MONO-INFECTED COVID-19 PATIENTS:
The 78 consecutive COVID-19 patients consisted of 41 men (52.6%) and 37 women (47.4%), ranging in age from 3 years to 88 years, with an average age of 47.7±17.2 years. There were 8 mildly ill patients (10.3%), 59 moderately ill patients (75.6%), and 11 severely/critically ill patients (14.1%). There were no statistically significant differences between the 2 groups in patient characteristics such as age, sex, epidemiological history, comorbidities, onset time, clinical symptom, physical examination, computerized tomography scan result, severity classification, and length of stay (P>0.05) (Table 1).
CO-INFECTIONS IN COVID-19 PATIENTS:
Eleven out of those 78 COVID-19 patients (14.1%) were co-infected with other respiratory pathogens, comprising 6 men and 5 women, with an average age of 42.7±14.9 years. According to the clinical severity classification, those co-infected patients comprised 2 mildly ill patient, 7 moderately ill patients, and 2 severely/critically ill patients. Among the co-infecting pathogens, M. pneumonia (45.5%) and RSV (36.4%) accounted for the highest rates of co-infection. There were 8 COVID-19 patients (72.7%) co-infected with 1 other pathogen, which included M. pneumonia (3 patients), RSV (3 patients), influenza B virus (1 patient), and adenoviruses (1 patient), while the remaining 3 COVID-19 patients (27.3%) were co-infected with 2 other pathogens, which included M. pneumoniae and C. pneumoniae (1 patient), M. pneumoniae and RSV (1 patient), and C. pneumoniae and L. pneumophila (1 patient). Almost all co-infected patients had unilateral or bilateral pulmonary lesions, with the exception of 1 moderately ill, influenza B virus-co-infected patient who showed no obvious lung abnormalities (Table 1). One of the severely ill patients was co-infected with M. pneumoniae and RSV and had underlying cardiovascular diseases, while the other severely ill patient was co-infected with adenoviruses and had hypertension and diabetes as underlying diseases. Other co-infected patients did not have any underlying disease.
COMPARISONS OF LABORATORY TEST RESULTS BETWEEN CO-INFECTED AND MONO-INFECTED COVID-19 PATIENTS:
The comparisons of laboratory test indicators between mono-infected COVID-19 patients and COVID-19 patients co-infected with other respiratory pathogens revealed that the co-infection group had no significantly lower levels of lactate dehydrogenase (LDH), creatine kinase (CK), and C-reactive protein (CRP) than in the mono-infection group (P 0.318, 0.692, 0.362, respectively). For inflammatory markers, there were 4 co-infected patients (36.4%) and 4 mono-infected patients (6.0%) with increased levels of procalcitonin (PCT), which differed significantly between the 2 groups of patients (P=0.002). Multivariate analysis also showed significant differences in the level of PCT between the 2 groups (P=0.003, OR=0.038,95%CI (0.004–0.341)). On the contrary, there were no statistically significant differences in other laboratory test results between the 2 groups of patients (Tables 2, 3).
Discussion
SARS-CoV-2 that has invaded the human body is highly contagious, with a long incubation period, and has clinical manifestations that are similar to other respiratory infections [11]. The outbreak of COVID-19 occurred during the high-incidence season of other respiratory infections, and patients are prone to co-infection with SARS-CoV-2 and other respiratory pathogens. As described in previous studies [12,13], co-infection of COVID-19 with other pathogens may lead to high rates of ICU stay and mortality.
Our study shows that
The dynamic profiling of cardiac enzymes is an important clinical diagnostic indicator for cardiac injury in COVID-19 patients [5,18,19]. Our study showed that co-infected COVID-19 patients had lower levels of LDH and CK than mono-infected patients in the early stages, indicating that co-infection does not aggravate myocardial injury in COVID-19 patients. This may be associated with cardiomyocyte damages caused directly by viral entry via the angiotensin-converting enzyme 2 (ACE2) receptor [20]. ACE2 receptors are ubiquitous in the human body, and co-infecting pathogens can affect the ACE2-related signaling pathways. Our results are consistent with the previously reported findings [21] showing no difference in the rate of co-infections among mildly, moderately, and severely ill COVID-19 patients. CRP and PCT play vital roles in the diagnosis and treatment of infectious diseases. The production of PCT is mainly triggered by bacterial toxins and inflammatory cytokines, while its activation and production are inhibited by the large amount of INF-γ produced during viral infections [22]. Our study found that the patients with co-infection were significantly more likely to have elevated PCT levels than those with mono-infection, suggesting greater severity of inflammatory responses in co-infected patients.
COVID-19 patients were treated with anti-inflammatory therapy according to the inflammatory index and clinical experience. Combination therapy with antiviral and antibiotic agents was recommended for definite COVID-19 patients and suspected COVID-19 patients [23,24]. In this study, 52 of 78 cases (66.7%) were treated with a single antibiotic (21 cases with levofloxacin, 22 cases with moxifloxacin, 5 cases with levofloxacin converted to moxifloxacin, 1 case from piperacillin sulbactam to moxifloxacin, 1 case to piperacillin tazobactam, 2 cases from levofloxacin/moxifloxacin to linezolid), and 7 cases (9.0%) with combined antibiotics (1 case of meropenem combined with vancomycin, 1 case of meropenem with linezolid, 2 cases of moxifloxacin with meropenem, 1 case of levofloxacin with cefoperazone sulbactam, 1 case of moxifloxacin combined with cefoperazone sulbactam, and 1 case of levofloxacin with piperacillin sulbactam). All 78 cases of infection were well controlled, and neither secondary infection nor adverse events occurred. According to the experience in the treatment of respiratory tract pathogens, quinolones such as levofloxacin or moxifloxacin are the first choice in the treatment of respiratory tract pathogens. Then, the curative effect of antibiotics should be further evaluated according to the development of the disease, inflammatory indicators, and etiological results, and the antibiotics needed further are selected according to the antibiotics sensitivity test. In the specific clinical work, the past medical history of patients, especially infection susceptibility factors, needs to be well considered.
Due to the situation of epidemic control in China, the number of COVID-19 patients in our area is limited. At the same time, as our hospital is the local designated treatment hospital, all patients in the region are treated there. These conditions may have prevented us from finding more differences between the co-infection and mono-infection groups. Large sample and multicenter studies in other regions are still needed. In addition, this study was conducted in the early stage of the epidemic, and the patient diagnosis and treatment process and hospital-related work flow were not yet perfect, so the clinical data were not comprehensive. More comprehensive research is needed to assess the influence of other conditions on infection.
Conclusions
The findings showed that
Tables
Table 1. Comparisons of clinical characteristics between co-infected and mono-infected COVID-19 patients with univariate analysis.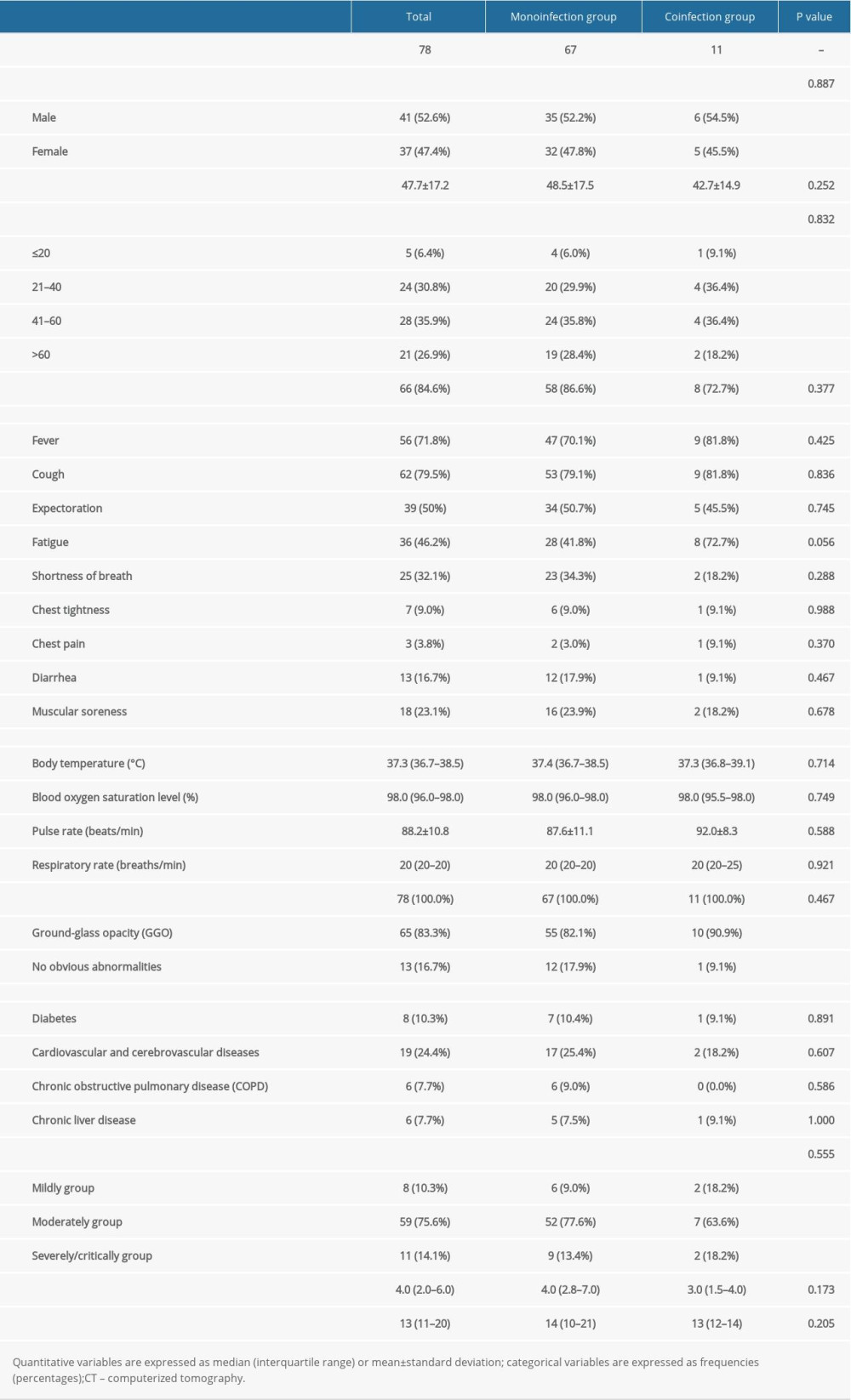 Table 2. Comparisons of laboratory test results between co-infected and mono-infected COVID-19 patients with univariate analysis.
Table 2. Comparisons of laboratory test results between co-infected and mono-infected COVID-19 patients with univariate analysis.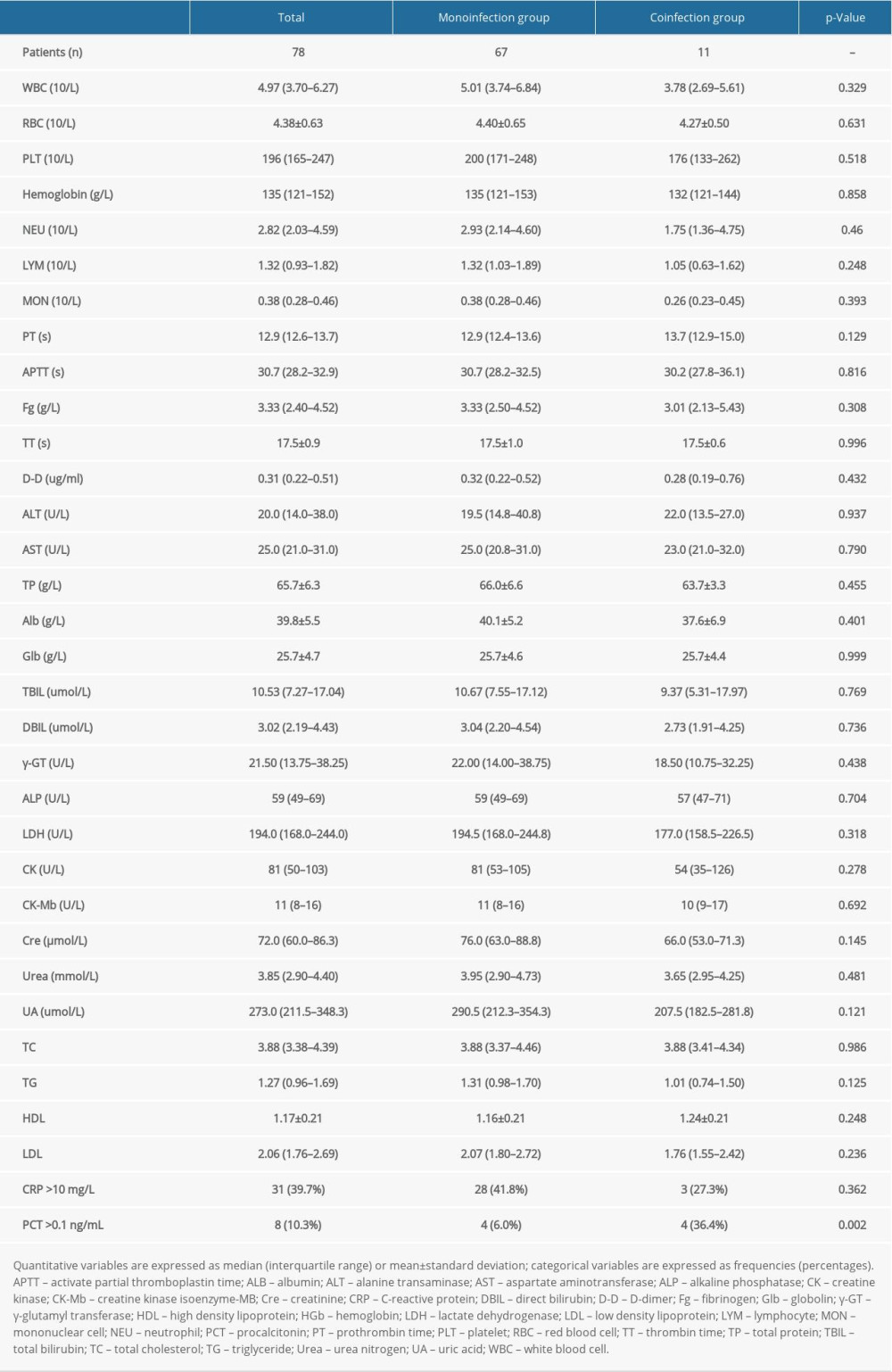 Table 3. Risk factors between co-infected and mono-infected COVID-19 patients with multivariate analysis.
Table 3. Risk factors between co-infected and mono-infected COVID-19 patients with multivariate analysis.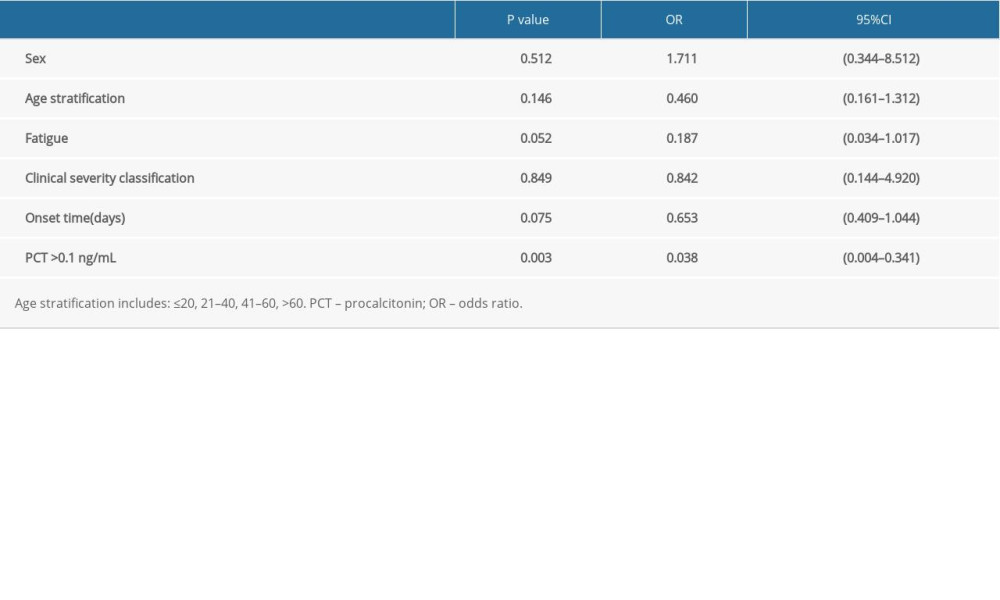
References
1. Gralinski LE, Menachery VD, Return of the coronavirus: 2019-nCoV: Viruses, 2020; 12(2); 135
2. Benvenuto D, Giovanetti M, Ciccozzi A, The 2019-new coronavirus epidemic: Evidence for virus evolution: J Med Virol, 2020; 92(4); 455-59
3. Guan WJ, Ni ZY, Hu Y, Clinical characteristics of coronavirus disease 2019 in China: N Engl J Med, 2020; 382(18); 1708-20
4. Wassenaar TM, Zou Y, 2019_nCoV/SARS-CoV-2: rapid classification of betacoronaviruses and identification of Traditional Chinese Medicine as potential origin of zoonotic coronaviruses: Lett Appl Microbiol, 2020; 70(5); 342-48
5. Zhou P, Yang XL, Wang XG, A pneumonia outbreak associated with a new coronavirus of probable bat origin: Nature, 2020; 579(7798); 270-73
6. Lu R, Zhao X, Li J, Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding: Lancet, 2020; 395(10224); 565-74
7. Khodamoradi Z, Moghadami M, Lotfi M, Co-infection of coronavirus disease 2019 and influenza A: A report from Iran: Arch Iran Med, 2020; 23(4); 239-43
8. Arashiro T, Nakamura S, Asami T, SARS-CoV-2 and Legionella co-infection in a person returning from a Nile cruise: J Travel Med, 2020; 27(3); taaa053
9. Ai T, Yang Z, Hou H, Correlation of chest CT and RT-PCR testing in coronavirus disease 2019 (COVID-19) in China: A report of 1014 cases: Radiology, 2020; 296(2); E32-40
10. National Health Commission & National Administration of Traditional Chinese Medicine, Diagnosis and treatment protocol for novel coronavirus pneumonia (Trial Version 7): Chinese Medical Journal, 2020; 133(9); 1087-95
11. Huang X, Wei F, Hu L, Epidemiology and clinical characteristics of COVID-19: Arch Iran Med, 2020; 23(4); 268-71
12. Cox MJ, Loman N, Bogaert D, Co-infections: potentially lethal and unexplored in COVID-19: Lancet Microbe, 2020; 1(1); e11
13. Li Z, Chen ZM, Chen LD, Coinfection with SARS-CoV-2 and other respiratory pathogens in patients with COVID-19 in Guangzhou, China: J Med Virol, 2020; 92(11); 2381-83
14. Zahariadis G, Gooley TA, Ryall P, Risk of ruling out severe acute respiratory syndrome by ruling in another diagnosis: Variable incidence of atypical bacteria coinfection based on diagnostic assays: Can Respir J, 2006; 13(1); 17-22
15. Kim D, Quinn J, Pinsky B, Rates of co-infection between SARS-CoV-2 and other respiratory pathogens: JAMA, 2020; 323(20); 2085-86
16. Richardson S, Hirsch JS, Narasimhan M, Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City Area: JAMA, 2020; 323(20); 2052-59
17. Hazra A, Collison M, Pisano J, Coinfections with SARS-CoV-2 and other respiratory pathogens: Infect Control Hosp Epidemiol, 2020; 41(10); 1228-29
18. Yang X, Yu Y, Xu J, Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study: Lancet Respir Med, 2020; 8(5); 475-81
19. Chen N, Zhou M, Dong X, Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study: Lancet, 2020; 395(10223); 507-13
20. Li R, Qiao S, Zhang G, Analysis of angiotensin-converting enzyme 2 (ACE2) from different species sheds some light on cross-species receptor usage of a novel coronavirus 2019-nCoV: J Infect, 2020; 80(4); 469-96
21. Ma L, Wang W, Le Grange JM, Coinfection of SARS-CoV-2 and other respiratory pathogens: Infect Drug Resist, 2020; 13; 3045-53
22. de Haan JJ, Lubbers T, Derikx JP, Rapid development of intestinal cell damage following severe trauma: A prospective observational cohort study: Crit Care, 2009; 13(3); R86
23. Lai CC, Wang CY, Hsueh PR, Co-infections among patients with COVID-19: The need for combination therapy with non-anti-SARS-CoV-2 agents?: J Microbiol Immunol Infect, 2020; 53(4); 505-12
24. Jin YH, Cai L, Cheng ZS, A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version): Mil Med Res, 2020; 7(1); 4
Tables
Table 1. Comparisons of clinical characteristics between co-infected and mono-infected COVID-19 patients with univariate analysis.Table 2. Comparisons of laboratory test results between co-infected and mono-infected COVID-19 patients with univariate analysis.Table 3. Risk factors between co-infected and mono-infected COVID-19 patients with multivariate analysis. In Press
Review article
Clinical Use of Endotracheal Intubation Without Neuromuscular Blockade: The Current Stage of KnowledgeMed Sci Monit In Press; DOI: 10.12659/MSM.951765
Clinical Research
Effect of Dexmedetomidine Hydrochloride Nasal Spray on Anxiety and Sleep in Patients Undergoing Gynecologic...Med Sci Monit In Press; DOI: 10.12659/MSM.952465
Clinical Research
Prognostic Value of Mortality Scoring Systems in Patients With Severe Burns: Identifying Key Predictors of ...Med Sci Monit In Press; DOI: 10.12659/MSM.951713
Laboratory Research
Evaluation of the Trueness and Precision of Cast, Milled-Cast, Milled, and 3D-Printed Post-and-Core Techniq...Med Sci Monit In Press; DOI: 10.12659/MSM.953491
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,214
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,757,839
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,153
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,809
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387