02 October 2021: Clinical Research
Preoperative Alkaline Phosphatase-to-Cholesterol Ratio as a Predictor of Overall Survival in Pancreatic Ductal Adenocarcinoma Patients Undergoing Radical Pancreaticoduodenectomy
Guotong Qiu1ABCDEF, Lipeng ZhangDOI: 10.12659/MSM.931868
Med Sci Monit 2021; 27:e931868






Abstract
BACKGROUND: The value of alkaline phosphatase and cholesterol for predicting overall survival (OS) in cancer patients has been previously studied. However, the predictive value of these variables in patients with pancreatic ductal adenocarcinoma (PDAC) was limited. Hence, we conducted this study to investigate the prognostic value of the alkaline phosphatase-to-cholesterol ratio (ACR) in patients undergoing radical pancreaticoduodenectomy (PD) for PDAC.
MATERIAL AND METHODS: A total of 102 PDAC patients undergoing radical PD at the Cancer Hospital Chinese Academy of Medical Sciences were retrospectively enrolled based on medical records from June 2009 to June 2019. R programming language was used for the optimal cutoff value of biological markers such as preoperative ACR. Kaplan-Meier method and log-rank test were used for univariate survival analysis, and a Cox regression model was used for multivariate survival analysis.
RESULTS: The optimal cutoff value of preoperative ACR was 32.988. Patients with higher preoperative ACR values had worse OS (P<0.001). Higher preoperative ACR was significantly correlated with the degree of tumor differentiation (P<0.018); levels of alanine aminotransferase (P<0.001), aspartate aminotransferase (P<0.001), total bilirubin (P<0.001), and carbohydrate antigen 19-9 (P=0.016); and clinical symptoms (P=0.001). Multivariate analysis showed that tumor differentiation (P<0.001), ACR value (hazard ratio [HR]: 2.225, 95% confidence interval [CI]: 1.33-3.724, P=0.002), and sex (HR, 1.725, 95% CI: 1.1-2.704, P=0.018) were independent factors associated with the prognosis of PDAC patients undergoing radical PD.
CONCLUSIONS: The preoperative ACR was correlated with OS in pancreatic cancer patients undergoing radical pancreaticoduodenectomy. Elevated ACR was correlated with poor OS.
Keywords: Alkaline Phosphatase, Cholesterol, Pancreaticoduodenectomy, Predictive Value of Tests, Pancreatic Cancer, Adult, Adenocarcinoma, adult, Aged, Carcinoma, Pancreatic Ductal, China, Female, Humans, Male, Middle Aged, Pancreatic Neoplasms, Preoperative Care, Prognosis, Sensitivity and Specificity, Survival Analysis
Background
Pancreatic cancer has the worst prognosis and the highest mortality rate among all malignancies. In China, pancreatic cancer takes sixth place in terms of mortality, with morbidity and mortality rates having increased in recent years [1]. In the United States, it ranks 10th for estimated new male cases, ninth for estimated new female cases, and fourth for estimated deaths among male and female cases, separately. Meanwhile, the 5-year survival rate of confirmed cases is reported to be less than 9%, with about 80%–85% of patients having distant metastases at the time of diagnosis [2]. According to a British study, pancreatic cancer is about to surpass breast cancer and become the third leading cause of death in the European Union [3]. Despite recent advances in pancreatic cancer diagnosis, preoperative management strategies, and surgical levels, no significant progress has been made in increasing the overall survival (OS) time of cancer patients [4]. In addition, a series of studies have been conducted on high-risk factors for pancreatic cancer, such as smoking [5], obesity [6], diabetes [7], and familial predisposition [8], without making any remarkable contribution to early diagnosis. Therefore, simple, economical, and effective predictors of OS time could help manage pancreatic carcinoma patients more efficiently.
Systemic inflammatory and immune responses occupy a key role in the tumorigenesis of many cancers, including pancreatic cancer [9]. Relevant reports have found that alkaline phosphatase (ALP) plays a major role in inflammation by affecting purine signal transduction, which can stop inflammatory signals and thus induce immunosuppression [10]. Furthermore, the predictive value of ALP combined with other biomarkers has been reported in resectable and nonresectable pancreatic carcinoma [11–13]. Additionally, in patients undergoing immunotherapy, higher cholesterol (CHO) levels are known to be associated with a better prognosis [14]. Therefore, ALP and CHO can be jointly used to predict OS in cancer patients.
Nonetheless, the relationship between the ALP-to-CHO ratio (ACR) and the prognosis of patients undergoing radical pancreaticoduodenectomy (PD) has not been investigated so far. Hence, we conducted a retrospective study to assess the predictive value of ACR in patients undergoing radical PD for pancreatic ductal adenocarcinoma (PDAC).
Material and Methods
DATA COLLECTION:
For each patient, the following data were collected: age; sex; body mass index; laboratory test results, including white blood cell (WBC) counts and plasma levels of alanine aminotransferase, aspartate transaminase, total bilirubin, albumin, globulin, carbohydrate antigen 19-9 (CA19-9), ALP, and CHO; clinical symptoms; history of diabetes, smoking, drinking, and familial predisposition to cancer; and tumor characteristics, including tumor differentiation, lymphovascular invasion, perineural invasion, capsular invasion, maximum tumor diameter, T-staging, N-staging, tumor-node-metastasis (TNM) staging, and adjuvant therapy. TNM staging was determined based on the pathology report. ACR was defined as ALP divided by CHO.
ETHICS:
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki published by the World Medical Association (July 9, 2018) and was approved by the Medical Ethics Committee of the National Cancer Center/Cancer Hospital Chinese Academy of Medical Sciences (approval No. 17-168/1424). All patients signed written informed consent forms before enrollment.
TREATMENT AND FOLLOW-UP:
All patients received radical PD following admission and were postoperatively followed up every 3 months for the first 2 years and every 6 months thereafter through outpatient medical records and telephone calls. The findings from physical examination and laboratory tests were recorded in detail. OS was calculated from the day of surgery to the date of death or last follow-up (ie, October 15, 2020).
DATA ANALYSIS:
Normally distributed data are expressed as mean ±standard deviation, nonnormally distributed data as median (minimum-maximum), and categorical variables as frequency and percentage. SPSS 26.0 was used for data analysis, and the optimal cutoff value was calculated using the R programming language (4.0.3). Chi-square test and independent samples
Results
DETERMINATION OF OPTIMAL CUTOFF VALUES FOR SURVIVAL ANALYSIS:
The optimal cutoff values of ALP, CHO, and ACR were calculated by the R programming language to be 108.5 U/L, 3.49 mmol/L, and 32.988, respectively.
The median ACR for all patients in this study was 45.0 (9.0–325.9) (Table 1). As is shown in Figure 1, the area under the receiver-operating characteristics curve of preoperative ACR is 0.737 (95% confidence interval [CI]: 0.615–0.859), which is higher than ALP (0.719, 95% CI: 0.578–0.859) and CHO (0.521, 95% CI: 0.365–0.678), with 75.0% sensitivity and 27.8% specificity. Based on this optimal cutoff value, 34 patients had a preoperative ACR ≤32.988, and 68 patients had a preoperative ACR >32.988, as detailed in Table 1. The survival curve for preoperative ACR reveals that the OS of patients with ACR > 32.988 was shorter than that of patients with ACR ≤0.08 (Figure 2).
ACR CORRELATION ANALYSIS:
Based on the best cutoff value of preoperative ACR, patients were divided into 2 groups, namely, low ACR (≤32.988) and high ACR (>32.988). High preoperative ACR values were found to be significantly correlated with alanine aminotransferase (P=0.001), aspartate transaminase (P=0.001), total bilirubin (P=0.001), CA19-9 (P=0.016), clinical symptoms (P=0.001), differentiation degree (P=0.049), and preoperative serum ALP (P=0.001), as detailed in Table 2.
UNIVARIATE AND MULTIVARIATE ANALYSES:
Univariate analysis showed that sex (hazard ratio [HR], 1.763; 95% CI, 1.142–2.72; P=0.01), preoperative WBC count (HR, 2.541; 95% CI, 1.264–5.109; P=0.009), alanine aminotransferase (HR, 3.169; 95% CI, 1.372–7.317; P=0.007), total bilirubin (HR, 2.071; 95% CI, 1.314–3.266; P=0.002), CA19-9 (HR, 2.043; 95% CI, 1.236–3.375; P=0.005), degree of differentiation (poorly vs well, HR=15.113, 95% CI, 3.99–57.239; moderately/well, HR=4.6, 95% CI=1.437–14.724), adjuvant therapy (HR, 1.55; 95% CI, 1.008–2.384; P=0.046), preoperative plasma ALP (HR, 2.247; 95% CI, 1.32–3.824; P=0.003), and preoperative ACR (HR, 2.609; 95% CI, 1.573–4.327; P=0.001) were independent predictors of OS in patients undergoing radical PD (Table 3).
In contrast, the following were not determined as independent factors associated with the OS of patients treated with radical PD: age, body mass index, aspartate transaminase, albumin, globulin, clinical symptoms, diabetes, hypertension, smoking status, alcohol consumption, family history of cancer, American Society of Anesthesiologists classification, lymphovascular invasion, perineural invasion, capsular invasion, maximum tumor diameter, T-stage, N-stage, TNM stage, and preoperative CHO level.
In multivariate regression analysis, tumor differentiation degree (P<0.001), sex (HR, 1.725; 95% CI, 1.1–2.704; P=0.018), and preoperative ACR (HR, 2.225; 95% CI, 1.33–3.724; P=0.002) were identified as independent prognosticators in patients undergoing radical PD (Table 4).
Discussion
Our results demonstrated that preoperative ACR was an independent predictor of OS in PDAC patients undergoing radical PD, with higher ACR values correlating with a worse prognosis. To our knowledge, this report is the first on the relationship between ACR and the prognosis of PDAC patients undergoing radical PD. Furthermore, multivariate analysis indicated that sex (
Despite being a currently accepted cancer staging system, TNM classification has been shown to have limited ability in cancer staging prediction [15]. A number of studies have focused on the predictors of OS in various tumors, including pancreatic carcinoma. For example, patients with a high neutrophil-to-lymphocyte ratio in the early stage of pancreatic cancer have been reported have poorer OS compared with those with a low neutrophil-to-lymphocyte ratio [16]. In addition, the prognosis of pancreatic carcinoma patients with a high glucose/lymphocyte ratio has been estimated to be worse than that of patients with a low glucose/lymphocyte ratio [17]. Another study has identified high serum albumin levels as a protective prognostic factor in advanced pancreatic carcinoma patients treated with gemcitabine and albumin-bound paclitaxel [18]. However, the predictive value of combined ALP and CHO in pancreatic carcinoma has not been studied yet.
ALP is an enzyme secreted by the liver and released from the biliary tract. It belongs to a protein superfamily [19], and it is widely distributed throughout the body and mainly found in skeletal muscles, intestine, kidney, and liver. Oxidative stress has been suggested to increase the activity of ALP and its sensitivity to levamisole, homoarginine, and heat in cells [20]. Tumors in the head of the pancreas can cause bilirubin stasis, which in turn leads to abnormal liver function and changes in serum ALP levels.
Studies have reported that ALP can improve tumor cell invasion, metastasis, and proliferation ability [21]. It has also been identified as a predictor of bone metastasis in both lung and kidney cancer patients, with higher ALP levels capable of promoting tumor bone metastasis [22,23]. Moreover, higher ALP levels have been demonstrated to serve as a risk factor for lymph node metastasis in esophageal cancer [24], correlate with a later stage in colon cancer [25], and promote cell invasion and metastasis in pancreatic carcinoma; whereas, decreased ALP activity can reportedly inhibit tumor cell metastasis and invasion [26]. Other studies have indicated that the ratios of ALP to serum albumin and ALP to lactate dehydrogenase might predict the OS of patients with resectable and unresectable pancreatic carcinoma, respectively [11,12].
CHO is an important raw material for the synthesis of physiological activators, such as adrenal cortex hormones, sex hormones, bile acids, and vitamin D. It is also the main component of cell membranes, and its serum concentration can be used as an indicator of lipid metabolism [27]. Recently, it was discovered that the PCSK9 protein, which regulates CHO metabolism, has immune regulation functions for tumors, and that inhibiting its activity can promote the intratumoral infiltration of cytotoxic T cells and thereby enhance the effect of immunotherapy [28]. In another study, it was found that the positive regulation of CHO levels could change the invasive and metastatic capabilities of mouse ovarian cancer cells, and that patients with higher serum CHO levels were more sensitive to immunosuppressive agents for tumors [29]. CHO has also been shown to downregulate interleukin-9-mediated CD8+ T-cell differentiation and antitumor activity [30]. Inhibition of CHO acyltransferase can promote the proliferation of CD8+ T cells, which might play a central role in antitumor immunity [31]. The antitumor effect of CHO has been confirmed in breast cancer, kidney cancer, and soft tissue sarcoma [32–34]. Additionally, a meta-analysis involving 24,655 patients confirmed CHO as a protective factor in patients with cancer [35].
Therefore, preoperative ACR, as an indicator reflecting both preoperative ALP and CHO concentrations, could simultaneously combine their roles in tumor genesis and progression. Compared with a single biomarker, ACR was better able to predict OS in patients undergoing radical PD for PDAC in the current study. Hence, ACR could be used as a prognosticator in PDAC patients undergoing radical PD.
There are some limitations in this study. First, it was a single-center retrospective study with a small sample size, which makes the study prone to selection bias. It will be necessary to design more scientific, multi-center, large-sample prospective studies to verify the conclusions drawn here. Second, due to the small number of patients, patients were not divided into training and experimental groups for statistical verification, and external verification was unavailable, which necessitates further study. Third, the predictive value of preoperative ACR was focused in this study, without taking into account the relationship between postoperative ACR changes and the prognosis of the patients. Finally, during follow-up, many patients received other treatments due to tumor recurrence, which affected OS.
Conclusions
In conclusion, this study, for the first time, proved the prognostic value of preoperative ACR for predicting OS after radical PD for PDAC. Moreover, ACR was shown to be a simple, easy-to-accept, and low-cost factor that could be used as a prognosticator in patients undergoing radical PD for pancreatic head ductal adenocarcinoma. This finding suggests that treatment plans should consider not only TNM stage but also the preoperative serum enzymes, making individualized therapy possible for patients with PDAC. However, the exact mechanisms and function of ALP and CHO in PDAC should be elucidated. Further research is needed to verify the findings of our study.
Figures
![Receiver-operating characteristic (ROC) curve analysis based on preoperative alkaline phosphatase (ALP) concentration, cholesterol (CHO) level, and ALP/CHO ratio (ACR) for overall survival. The area under the ROC curve (AUC) indicates the diagnostic power of ALP, CHO, and ACR. The optimum cutoff point for ALP concentration was 108.5 U/L, and AUC was 0.719 (95% confidence interval [CI], 0.578–0.859), with a sensitivity of 78.6% and a specificity of 33.3% by the Youden index. The optimum cutoff point for CHO level was 3.49 mmol/L, and AUC was 0.521 (95% CI, 0.365–0.678), with a sensitivity of 81.0% and a specificity of 66.7% by the Youden index. The optimum cutoff point for ACR was 32.988, and AUC was 0.737 (95% CI, 0.615–0.859), with a sensitivity of 75.0% and a specificity of 27.8% by the Youden index.](https://jours.isi-science.com/imageXml.php?i=medscimonit-27-e931868-g001.jpg&idArt=931868&w=1000) Figure 1. Receiver-operating characteristic (ROC) curve analysis based on preoperative alkaline phosphatase (ALP) concentration, cholesterol (CHO) level, and ALP/CHO ratio (ACR) for overall survival. The area under the ROC curve (AUC) indicates the diagnostic power of ALP, CHO, and ACR. The optimum cutoff point for ALP concentration was 108.5 U/L, and AUC was 0.719 (95% confidence interval [CI], 0.578–0.859), with a sensitivity of 78.6% and a specificity of 33.3% by the Youden index. The optimum cutoff point for CHO level was 3.49 mmol/L, and AUC was 0.521 (95% CI, 0.365–0.678), with a sensitivity of 81.0% and a specificity of 66.7% by the Youden index. The optimum cutoff point for ACR was 32.988, and AUC was 0.737 (95% CI, 0.615–0.859), with a sensitivity of 75.0% and a specificity of 27.8% by the Youden index.
Figure 1. Receiver-operating characteristic (ROC) curve analysis based on preoperative alkaline phosphatase (ALP) concentration, cholesterol (CHO) level, and ALP/CHO ratio (ACR) for overall survival. The area under the ROC curve (AUC) indicates the diagnostic power of ALP, CHO, and ACR. The optimum cutoff point for ALP concentration was 108.5 U/L, and AUC was 0.719 (95% confidence interval [CI], 0.578–0.859), with a sensitivity of 78.6% and a specificity of 33.3% by the Youden index. The optimum cutoff point for CHO level was 3.49 mmol/L, and AUC was 0.521 (95% CI, 0.365–0.678), with a sensitivity of 81.0% and a specificity of 66.7% by the Youden index. The optimum cutoff point for ACR was 32.988, and AUC was 0.737 (95% CI, 0.615–0.859), with a sensitivity of 75.0% and a specificity of 27.8% by the Youden index. 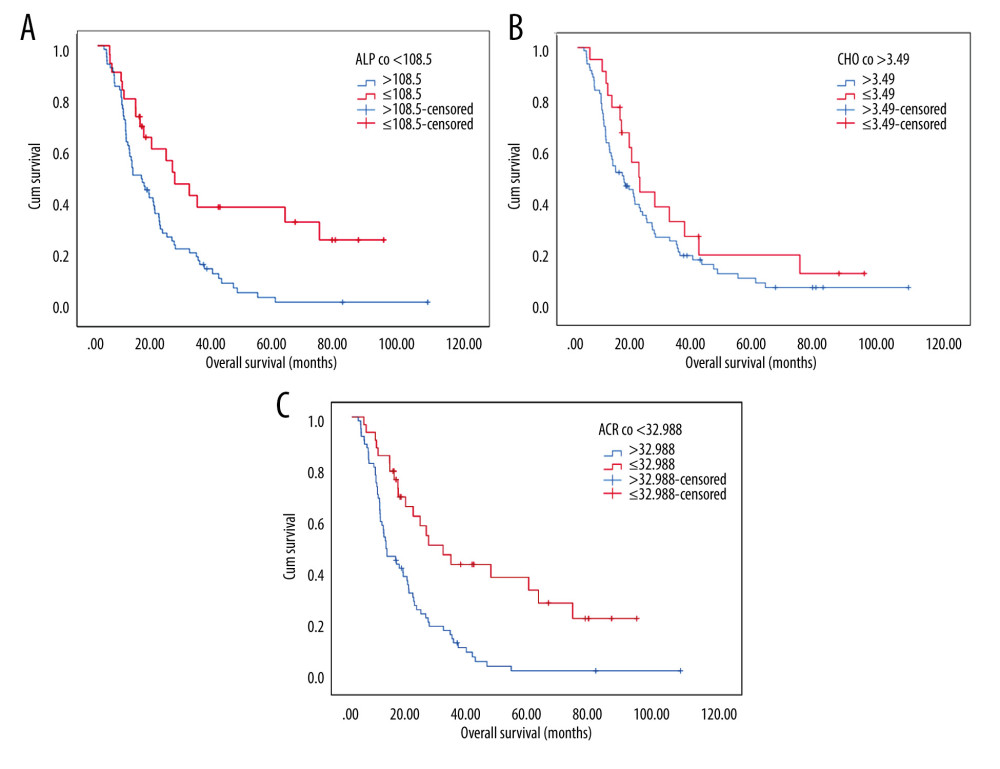 Figure 2. Kaplan-Meier curves generated by preoperative alkaline phosphatase (ALP) concentration, cholesterol (CHO) level, and ALP/CHO ratio (ACR) using the optimal cutoff values. (A) In the comparison of preoperative ALP concentration >108.5 U/L with preoperative ALP concentration ≤108.5 U/L (P<0.05), the blue line represents the >108.5 U/L group and the red line represents the ≤108.5 U/L group. (B) In the comparison of preoperative cholesterol level >3.49 mmol/L and preoperative cholesterol level ≤3.49 mmol/L (P=0,181), the blue line represents the >3.49 mmol/L group and the red line represents the ≤3.49 mmol/L group. (C) In the comparison of preoperative ACR >32.988 with preoperative ACR ≤32.988 (P<0.05), the blue line represents the ACR >32.988 group and the red line represents the ACR ≤32.988 group.
Figure 2. Kaplan-Meier curves generated by preoperative alkaline phosphatase (ALP) concentration, cholesterol (CHO) level, and ALP/CHO ratio (ACR) using the optimal cutoff values. (A) In the comparison of preoperative ALP concentration >108.5 U/L with preoperative ALP concentration ≤108.5 U/L (P<0.05), the blue line represents the >108.5 U/L group and the red line represents the ≤108.5 U/L group. (B) In the comparison of preoperative cholesterol level >3.49 mmol/L and preoperative cholesterol level ≤3.49 mmol/L (P=0,181), the blue line represents the >3.49 mmol/L group and the red line represents the ≤3.49 mmol/L group. (C) In the comparison of preoperative ACR >32.988 with preoperative ACR ≤32.988 (P<0.05), the blue line represents the ACR >32.988 group and the red line represents the ACR ≤32.988 group. Tables
Table 1. Baseline characteristics of 102 pancreatic ductal adenocarcinoma patients who underwent radical pancreaticoduodenectomy, n (%).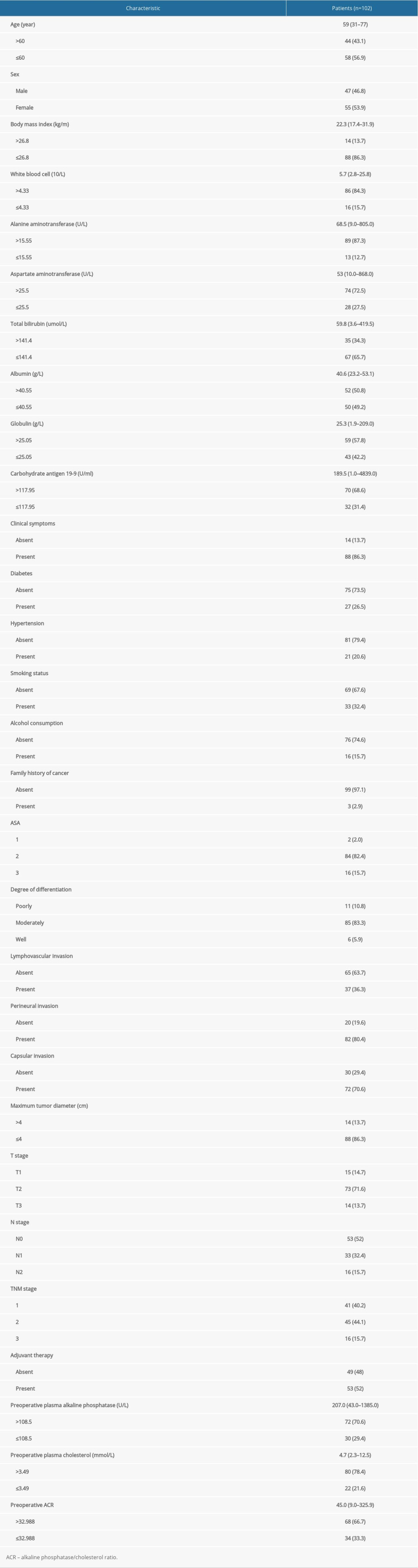 Table 2. Correlation between preoperative alkaline phosphatase-to-cholesterol ratio (ACR) and clinicopathological characteristics in pancreatic ductal adenocarcinoma patients who underwent radical pancreaticoduodenectomy, n (%).
Table 2. Correlation between preoperative alkaline phosphatase-to-cholesterol ratio (ACR) and clinicopathological characteristics in pancreatic ductal adenocarcinoma patients who underwent radical pancreaticoduodenectomy, n (%).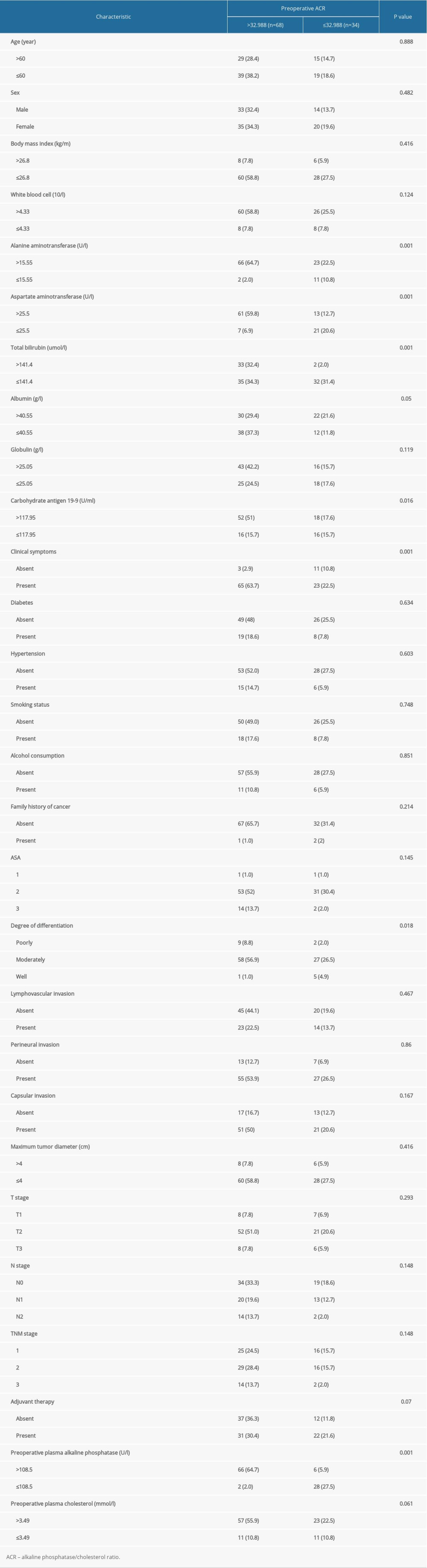 Table 3. Univariate analysis for overall survival in pancreatic ductal adenocarcinoma patients who underwent radical pancreaticoduodenectomy.
Table 3. Univariate analysis for overall survival in pancreatic ductal adenocarcinoma patients who underwent radical pancreaticoduodenectomy.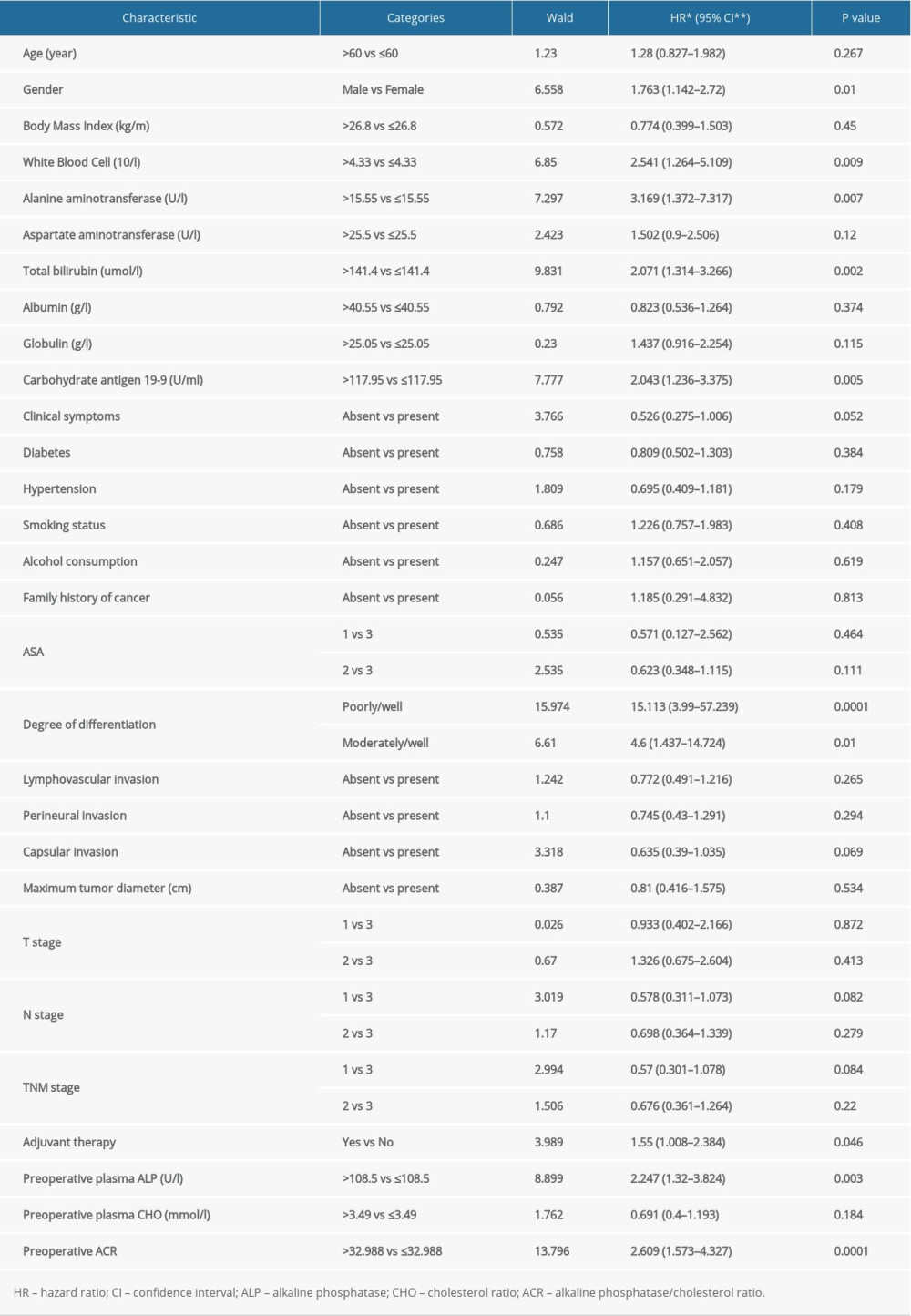 Table 4. Multivariate analysis for overall survival in pancreatic ductal adenocarcinoma patients who underwent radical pancreaticoduodenectomy.
Table 4. Multivariate analysis for overall survival in pancreatic ductal adenocarcinoma patients who underwent radical pancreaticoduodenectomy.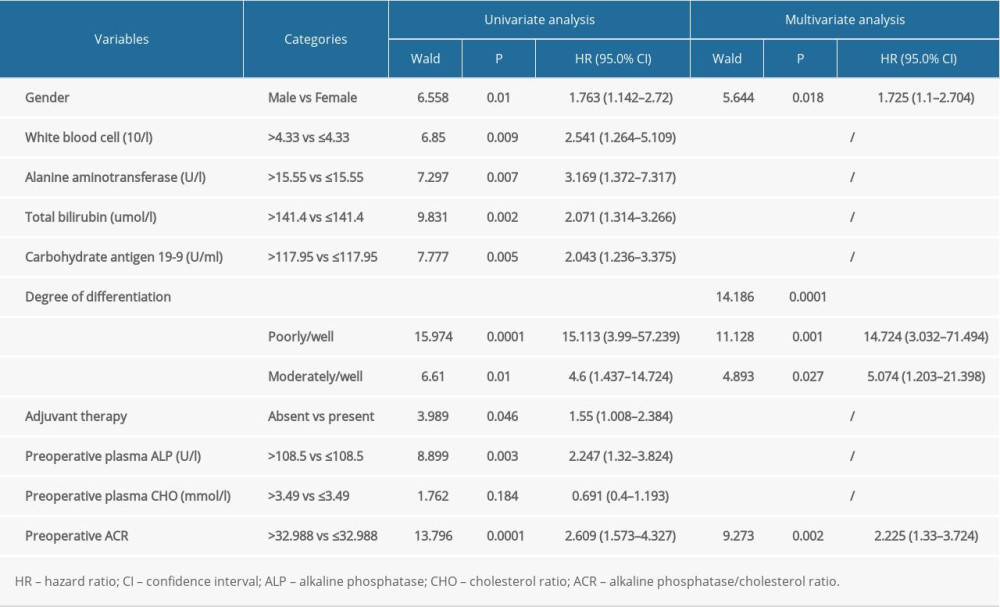
References
1. Chen W, Zheng R, Baade PD, Cancer statistics in China, 2015: Cancer J Clin, 2016; 66; 115-32
2. Siegel RL, Miller KD, Jemal A, Cancer statistics, 2020: Cancer J Clin, 2020; 70; 7-30
3. Bray F, Ferlay J, Soerjomataram I, Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries: Cancer J Clin, 2018; 68; 394-424
4. Mizrahi JD, Surana R, Valle JW, Shroff RT, Pancreatic cancer: Lancet, 2020; 395; 2008-20
5. Blackford A, Parmigiani G, Kensler TW, Genetic mutations associated with cigarette smoking in pancreatic cancer: Cancer Res, 2009; 69; 3681-88
6. Stolzenberg-Solomon RZ, Schairer C, Moore S, Lifetime adiposity and risk of pancreatic cancer in the NIH-AARP Diet and Health Study cohort: Am J Clin Nutr, 2013; 98; 1057-65
7. Andersen DK, Korc M, Petersen GM, Diabetes, pancreatogenic diabetes, and pancreatic cancer: Diabetes, 2017; 66; 1103-10
8. Bang YJ, Ruiz EY, Van Cutsem E, Phase III, randomised trial of avelumab versus physician’s choice of chemotherapy as third-line treatment of patients with advanced gastric or gastro-oesophageal junction cancer: Primary analysis of JAVELIN Gastric 300: Ann Oncol, 2018; 29; 2052-60
9. Grivennikov SI, Greten FR, Karin M, Immunity, inflammation, and cancer: Cell, 2010; 140; 883-99
10. Rader BA, Alkaline phosphatase, an unconventional immune protein: Front Immunol, 2017; 8; 897
11. Zhang K, Dong S, Jing YH, Albumin-to-alkaline phosphatase ratio serves as a prognostic indicator in unresectable pancreatic ductal adenocarcinoma: A propensity score matching analysis: BMC Cancer, 2020; 20; 541
12. Pu N, Gao S, Xu Y, Alkaline phosphatase-to-albumin ratio as a prognostic indicator in pancreatic ductal adenocarcinoma after curative resection: J Cancer, 2017; 8; 3362-70
13. Xiao Y, Lu J, Chang W, Dynamic serum alkaline phosphatase is an indicator of overall survival in pancreatic cancer: BMC Cancer, 2019; 19; 785
14. Perrone F, Minari R, Bersanelli M, The prognostic role of high blood cholesterol in advanced cancer patients treated with immune checkpoint inhibitors: J Immunother, 2020; 43; 196-203
15. Rochefort MM, Ankeny JS, Kadera BE, Impact of tumor grade on pancreatic cancer prognosis: validation of a novel TNMG staging system: Ann Surg Oncol, 2013; 20; 4322-29
16. Abe T, Amano H, Kobayashi T, Preoperative neutrophil-to-lymphocyte ratio as a prognosticator in early-stage pancreatic ductal adenocarcinoma: Eur J Surg Oncol, 2018; 44; 1573-79
17. Zhong A, Cheng CS, Kai J, Clinical significance of glucose to lymphocyte ratio (GLR) as a prognostic marker for patients with pancreatic cancer: Front Oncol, 2020; 10; 520330
18. Blomstrand H, Green H, Fredrikson M, Clinical characteristics and blood/serum bound prognostic biomarkers in advanced pancreatic cancer treated with gemcitabine and nab-paclitaxel: BMC Cancer, 2020; 20; 950
19. Galperin MY, Bairoch A, Koonin EV, A superfamily of metalloenzymes unifies phosphopentomutase and cofactor-independent phosphoglycerate mutase with alkaline phosphatases and sulfatases: Protein Sci, 1998; 7; 1829-35
20. López-Posadas R, González R, Ballester I, Tissue-nonspecific alkaline phosphatase is activated in enterocytes by oxidative stress via changes in glycosylation: Inflamm Bowel Dis, 2011; 17; 543-56
21. Yamamoto K, Awogi T, Okuyama K, Takahashi N, Nuclear localization of alkaline phosphatase in cultured human cancer cells: Med Electron Microsc, 2003; 36; 47-51
22. Zhang L, Gong Z, Clinical characteristics and prognostic factors in bone metastases from lung cancer: Med Sci Monit, 2017; 23; 4087-94
23. Chen XY, Lan M, Zhou Y, Risk factors for bone metastasis from renal cell cancer: J Bone Oncol, 2017; 9; 29-33
24. Aminian A, Karimian F, Mirsharifi R, Correlation of serum alkaline phosphatase with clinicopathological characteristics of patients with oesophageal cancer: East Mediterr Health J, 2011; 17; 862-66
25. Hung HY, Chen JS, Chien-Yuh Y, Preoperative alkaline phosphatase elevation was associated with poor survival in colorectal cancer patients: Int J Colorectal Dis, 2017; 32; 1775-78
26. Rao SR, Snaith AE, Marino D, Tumour-derived alkaline phosphatase regulates tumour growth, epithelial plasticity and disease-free survival in metastatic prostate cancer: Br J Cancer, 2017; 116; 227-36
27. Luo J, Yang H, Song BL, Mechanisms and regulation of cholesterol homeostasis: Nat Rev Mol Cell Biol, 2020; 21; 225-45
28. Liu X, Bao X, Hu M, Inhibition of PCSK9 potentiates immune checkpoint therapy for cancer: Nature, 2020; 588(7839); 693-98
29. Reverter M, Rentero C, Garcia-Melero A, Cholesterol regulates Syntaxin 6 trafficking at trans-Golgi network endosomal boundaries: Cell Rep, 2014; 7; 883-97
30. Ma X, Bi E, Huang C: J Exp Med, 2018; 215; 1555-69
31. Yang W, Bai Y, Xiong Y, Potentiating the antitumour response of CD8(+) T cells by modulating cholesterol metabolism: Nature, 2016; 531; 651-55
32. Munir MT, Ponce C, Powell CA, The contribution of cholesterol and epigenetic changes to the pathophysiology of breast cancer: J Steroid Biochem Mol Biol, 2018; 183; 1-9
33. de Martino M, Leitner CV, Seemann C, Preoperative serum cholesterol is an independent prognostic factor for patients with renal cell carcinoma (RCC): BJU Int, 2015; 115; 397-404
34. Que Y, Jiang F, Liu L, Clinical significance of preoperative serum high density lipoprotein cholesterol levels in soft tissue sarcoma: Medicine (Baltimore), 2015; 94; e844
35. Zhou P, Li B, Liu B, Prognostic role of serum total cholesterol and high-density lipoprotein cholesterol in cancer survivors: A systematic review and meta-analysis: Clin Chim Acta, 2018; 477; 94-104
Figures
Figure 1. Receiver-operating characteristic (ROC) curve analysis based on preoperative alkaline phosphatase (ALP) concentration, cholesterol (CHO) level, and ALP/CHO ratio (ACR) for overall survival. The area under the ROC curve (AUC) indicates the diagnostic power of ALP, CHO, and ACR. The optimum cutoff point for ALP concentration was 108.5 U/L, and AUC was 0.719 (95% confidence interval [CI], 0.578–0.859), with a sensitivity of 78.6% and a specificity of 33.3% by the Youden index. The optimum cutoff point for CHO level was 3.49 mmol/L, and AUC was 0.521 (95% CI, 0.365–0.678), with a sensitivity of 81.0% and a specificity of 66.7% by the Youden index. The optimum cutoff point for ACR was 32.988, and AUC was 0.737 (95% CI, 0.615–0.859), with a sensitivity of 75.0% and a specificity of 27.8% by the Youden index.Figure 2. Kaplan-Meier curves generated by preoperative alkaline phosphatase (ALP) concentration, cholesterol (CHO) level, and ALP/CHO ratio (ACR) using the optimal cutoff values. (A) In the comparison of preoperative ALP concentration >108.5 U/L with preoperative ALP concentration ≤108.5 U/L (P<0.05), the blue line represents the >108.5 U/L group and the red line represents the ≤108.5 U/L group. (B) In the comparison of preoperative cholesterol level >3.49 mmol/L and preoperative cholesterol level ≤3.49 mmol/L (P=0,181), the blue line represents the >3.49 mmol/L group and the red line represents the ≤3.49 mmol/L group. (C) In the comparison of preoperative ACR >32.988 with preoperative ACR ≤32.988 (P<0.05), the blue line represents the ACR >32.988 group and the red line represents the ACR ≤32.988 group. Tables
Table 1. Baseline characteristics of 102 pancreatic ductal adenocarcinoma patients who underwent radical pancreaticoduodenectomy, n (%).Table 2. Correlation between preoperative alkaline phosphatase-to-cholesterol ratio (ACR) and clinicopathological characteristics in pancreatic ductal adenocarcinoma patients who underwent radical pancreaticoduodenectomy, n (%).Table 3. Univariate analysis for overall survival in pancreatic ductal adenocarcinoma patients who underwent radical pancreaticoduodenectomy.Table 4. Multivariate analysis for overall survival in pancreatic ductal adenocarcinoma patients who underwent radical pancreaticoduodenectomy.Table 1. Baseline characteristics of 102 pancreatic ductal adenocarcinoma patients who underwent radical pancreaticoduodenectomy, n (%).Table 2. Correlation between preoperative alkaline phosphatase-to-cholesterol ratio (ACR) and clinicopathological characteristics in pancreatic ductal adenocarcinoma patients who underwent radical pancreaticoduodenectomy, n (%).Table 3. Univariate analysis for overall survival in pancreatic ductal adenocarcinoma patients who underwent radical pancreaticoduodenectomy.Table 4. Multivariate analysis for overall survival in pancreatic ductal adenocarcinoma patients who underwent radical pancreaticoduodenectomy. In Press
Clinical Research
Body Weight and Insulin Resistance Indicators Among ChildrenMed Sci Monit In Press; DOI: 10.12659/MSM.951434
Clinical Research
Comparison of Radiographic Cervical Sagittal Alignment Parameters in Patients With Nonspecific Neck Pain, D...Med Sci Monit In Press; DOI: 10.12659/MSM.952950
Clinical Research
Combined Fibrinogen and Urinary α1-Microglobulin as Predictors of Respiratory Tract Infection in Children w...Med Sci Monit In Press; DOI: 10.12659/MSM.951066
Database Analysis
Evaluation of Salivary Total Oxidant Status (TOS) and Total Antioxidant Status (TAS) in Orthodontic Patient...Med Sci Monit In Press; DOI: 10.12659/MSM.952052
Most Viewed Current Articles
17 Jan 2024 : Review article 14,175,576
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,756,620
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,465,966
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,651
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387