23 September 2021: Review Articles
A Review of the Role of the S-Detect Computer-Aided Diagnostic Ultrasound System in the Evaluation of Benign and Malignant Breast and Thyroid Masses
Di Zhang1CE, Fan Jiang2BC, Rui Yin3CF, Ge-Ge Wu4B, Qi Wei4CD, Xin-Wu Cui4G, Shu-E Zeng5AB*, Xue-Jun Ni1AE, Christoph F. Dietrich6FDOI: 10.12659/MSM.931957
Med Sci Monit 2021; 27:e931957






Abstract
ABSTRACT: Computer-aided diagnosis (CAD) systems have attracted extensive attention owing to their performance in the field of image diagnosis and are rapidly becoming a promising auxiliary tool in medical imaging tasks. These systems can quantitatively evaluate complex medical imaging features and achieve efficient and high-diagnostic accuracy. Deep learning is a representation learning method. As a major branch of artificial intelligence technology, it can directly process original image data by simulating the structure of the human brain neural network, thus independently completing the task of image recognition. S-Detect is a novel and interactive CAD system based on a deep learning algorithm, which has been integrated into ultrasound equipment and can help radiologists identify benign and malignant nodules, reduce physician workload, and optimize the ultrasound clinical workflow. S-Detect is becoming one of the most commonly used CAD systems for ultrasound evaluation of breast and thyroid nodules. In this review, we describe the S-Detect workflow and outline its application in breast and thyroid nodule detection. Finally, we discuss the difficulties and challenges faced by S-Detect as a precision medical tool in clinical practice and its prospects.
Keywords: Breast, Image Processing, Computer-Assisted, Thyroid Neoplasms, Ultrasonography, Doppler, Breast Neoplasms, Diagnosis, Computer-Assisted, Female, Humans, Image Interpretation, Computer-Assisted, Sensitivity and Specificity, Thyroid Gland, Ultrasonography
Background
Ultrasound (US) is widely available in clinical practice because of advantages such as its radiation-free, low-cost, and real-time imaging and its easy integration into interventional procedures for patient treatment [1]. However, US is highly dependent on operator experience and cannot quantitatively analyze image features, problems that lead to insufficient repeatability and objectivity [2,3]. To address these limitations, the American College of Radiology published the Breast Imaging Reporting and Data System (BI-RADS) and the Thyroid Imaging Reporting and Data System (TI-RADS), which provide standardized terminology to describe the characteristics and final assessment categories of breast and thyroid lesions [4,5]. Currently, the tools are widely used to facilitate communication between radiologists and clinicians and to regulate the management of patients with breast and thyroid lesions. However, because some US features are present in both malignant and benign masses, the subjectivity and diversity of these features can lead to differences in the operator’s final assessment, especially for medical residents with limited clinical experience [6,7]. A study by Lee et al showed that the sensitivity and specificity of experts in evaluating breast lesions according to the BI-RADS lexicon were as high as 98% and 58.6%, but those of residents were 66% and 52.9%, respectively [6]. To improve diagnostic accuracy and confidence in consensus recommendations, new technologies have been developed for clinical applications, such as US elastography [8], contrast-enhanced ultrasonography [9], 3-dimensional US [10], and computer-aided diagnosis (CAD) systems [11].
The CAD system can make quantitative evaluations by effectively analyzing a large number of images. This computer-based method aids interpretation and diagnosis and can also decrease intra-observer and inter-observer variability [12]. The development of CAD algorithms and software has become an area of intense research in the medical field. Conventional CAD processes based on traditional machine learning consist of preprocessing, image segmentation, feature extraction, selection, and classification, of which the most critical step is feature extraction [13]. Effective feature extraction is a complex task that is highly dependent on the quality of each intermediate result in the image processing step, and recursive trial and error is required to achieve satisfactory results [14,15]. Therefore, obtaining satisfactory results with conventional CAD systems based on traditional machine learning is time-consuming and complicated. In contrast to conventional CAD systems that rely on hand-crafted features, deep learning algorithms can directly generate a set of transformation functions and image features from data, reducing the burden of feature selection and classification [16]. Recently, deep learning has achieved good results in clinical practice and has rapidly become a promising auxiliary tool in medical imaging tasks [17,18].
S-Detect (Samsung Medison, Co., Ltd., Seoul, Korea) is a novel and more interactive CAD system based on a deep learning algorithm, which provides a second objective opinion to assist operators in the interpretation and diagnosis of breast and thyroid cancer [19,20]. S-Detect has attracted extensive attention owing to its compelling performance in image recognition tasks and has the potential to become a useful diagnostic tool for radiologists [21]. However, because it is a new tool, doctors still have many concerns about the application of S-Detect in clinical practice. In a study by Choi et al, the specificity of S-Detect in identifying benign and malignant breast nodules was 95.4% [22]. However, Xia et al reported that S-Detect was only 41.2% specific for thyroid nodules [23]. Therefore, a thorough review of the research status of this technology is needed to guide its application. In this review, we describe the clinical diagnostic performance of S-Detect in the clinic and discuss its limitations and future prospects.
S-Detect Workflow
S-Detect is a commercial CAD system based on convolutional neural networks, which is a deep learning algorithm consisting of input layers, hidden layers, and output layers. By learning a large amount of training data, high-order statistics are extracted, and the balance of input and output data is optimized through a plurality of hidden layers, thus realizing accurate decisions and distinguishing malignant tumors from benign tumors. The data used to develop S-Detect were original US signals that did not undergo image postprocessing, and therefore human bias did not contribute to its development [24]. When a breast or thyroid mass is selected by a clinician who touches the screen and places a marker in the center of the target nodule, S-Detect automatically draws a region of interest along the boundary of the mass. When the nodule boundary automatically drawn by S-Detect is considered insufficient for evaluation, the operator can manually readjust the outline (Figure 1). When satisfactory lesion segmentation is completed, S-Detect analyzes the morphological characteristics of the breast or thyroid nodule according to the BI-RADS or TI-RADS lexicon, respectively, and provides a detailed report of each US descriptor. The US features, including shape, orientation, margin, echo pattern, and posterior acoustic features, are used for breast nodule analysis (Figure 2), while the characteristics of composition, shape, orientation, margins, echogenicity, and spongiform appearance are used to describe thyroid nodules (Figure 3). For other features, manual insertion is required. S-Detect finally provides the evaluation result as “possibly benign” or “possibly malignant” in dichotomy form, and a structured report is assigned as a reference to assist radiologists in their final diagnosis. The procedure for a complete S-Detect examination including B-mode scanning takes approximately 2 minutes [20,24]. S-Detect can make an instant judgement on the frozen image on the US system [25].
Application of S-Detect in the Breast
Breast cancer is the most common malignant tumor in women worldwide [26]. Accurate and early diagnosis of breast cancer for appropriate local and systemic treatment is of vital importance to improve the survival rate [27]. In addition to mammography, US plays an important role in the early diagnosis of breast cancer. Currently, the BI-RADS lexicon is used as a standard protocol for evaluating breast lesions by US imaging. As a supplementary method to the BI-RADS lexicon, S-Detect was developed to increase diagnostic accuracy and decrease inter-observer variability. According to the meta-analysis of Li et al, S-Detect may have the potential to help radiologists improve the diagnosis of breast masses and can be considered as a useful supplement to conventional US [28]. Kimet al evaluated the diagnostic performance of S-Detect to distinguish between benign and malignant breast masses. When the cutoff value was set at category 4a according to BI-RADS, S-Detect had significantly higher specificity, positive predictive value (PPV), and accuracy than did the radiologist (all
Choi et al also compared the changes in diagnostic performance of 2 experienced radiologists and 2 inexperienced radiologists before and after using S-Detect. After combining the results of S-Detect, the specificity, accuracy, and PPV of both experienced radiologists and 1 inexperienced radiologist were significantly improved without reducing sensitivity. Moreover, S-Detect significantly increased the AUC values for all radiologists using the BI-RADS lexicon to predict the risk of malignancy. The study found that regardless of the experience of radiologists, S-Detect has the potential to improve their diagnostic performance [22].
In a study by Lee et al, 500 solid breast lesions in 413 patients were retrospectively assessed by 2 groups of radiologists and S-Detect, and the agreement of US features according to the BI-RADS lexicon was compared between S-Detect and each group of radiologists. For the interpretation of each US descriptor, the kappa value showed that the agreement between S-Detect and the experienced group was higher than the kappa value between S-Detect and the inexperienced group. After the radiologists took the S-Detect results into account, the kappa value increased in both groups and the increase in the inexperienced group was more prominent [31]. This suggested that S-Detect can be used as a teaching tool to help inexperienced radiologists become familiar with and understand various US features in US examinations. For experienced radiologists, S-Detect can provide a second opinion in a cost-effective manner. In addition, S-Detect improves the inter-observer agreement of benign and malignant diagnoses among radiologists, which can prevent novice radiologists from making misdiagnoses due to lack of experience.
A retrospective study of 100 breast masses was performed by Park et al. When the final assessment of the breast mass by radiologists was inconsistent with S-Detect, they modified their final assessment according to the conclusion of S-Detect. Among all cases reclassified by 5 radiologists, 89% to 100% of cases that were originally classified as BI-RADS grade 4 or 5 were correctly downgraded to BI-RADS grade 3 [32]. Bartolotta et al also confirmed that S-Detect helped radiologists correctly change the initial BI-RADS classification in more than 1 of 4 breast lesions, and the percentage of correct reclassification (81%) was statistically significant [33]. According to the diagnostic recommendations of BI-RADS, biopsy is recommended for breast masses of category 4 or higher. However, many US features used in BI-RADS are described in both benign and malignant breast masses, especially in category 4 lesions, which indicates a wide range of malignant risk (2–95%) [34]. Therefore, with the assistance of S-Detect, the high rate of correct downgrading reduces misdiagnosis and unnecessary breast biopsies. The rate of correct downgrading is more significant for inexperienced radiologists because these operators tend to overestimate lesion characteristics.
Wu et al conducted a prospective study to evaluate factors that can cause false-positive or false-negative results in S-Detect. They found that larger benign lesions, the presence of lesion calcifications detected by B-mode US, and high degrees of vascularity were likely to lead to false-positive S-Detect results. Smaller malignant lesions and the absence of calcifications detected by B-mode US were likely to lead to false-negative S-Detect results [19]. These influencing factors must be taken into consideration when applying S-Detect in clinical practice. S-Detect can be used as an auxiliary tool for radiologists but it cannot completely replace grayscale US at present.
Application of S-Detect in the Thyroid
The global incidence rate of thyroid cancer in women is 10.2 per 100 000, which is 3 times higher than that of men. In 2018, thyroid cancer accounted for 5.1% of the total estimated female cancer burden, or 1 in 20 cancer diagnoses [26]. US has become the primary imaging choice for the examination of thyroid diseases and facilitates decision making for fine-needle aspiration (FNA) [35,36]. However, due to the slow growth of thyroid cancer and its lower invasiveness than other malignant tumors, overdiagnosis and overtreatment are a concern [37]. Given the good prognostic outcome of early-stage thyroid cancer, a high-performance CAD system can help radiologists improve the accuracy and consistency of radiological diagnoses and avoid unnecessary FNA procedures.
According to Choi et al, S-Detect showed a fairly high sensitivity (90.7%) and negative predictive value (91.7%), which was similar to an experienced radiologist in identifying benign and malignant thyroid nodules. However, the specificity and AUC were lower (specificity, 74.6% vs 94.9%,
Choi et al further demonstrated that the inter-observer agreement between experienced radiologists and S-Detect for the characterization of thyroid nodules was acceptable, and classifications of the US characteristics, including composition, orientation, echogenicity, and spongiform, showed substantial agreement (kappa=0.659, 0.740, 0.733, and 0.658, respectively) [20], compared with previous studies [39,40], in which the inter-observer agreement on the US features classification of thyroid nodules between S-Detect and radiologists may be similar or higher than that between experienced and inexperienced radiologists. Partially different from the results of Choi et al, a prospective study by Yoo et al showed that the sensitivity, specificity, PPV, negative predictive value, and accuracy of S-Detect in detecting thyroid cancer were 80.0%, 88.1%, 83.3%, 85.5%, and 84.6%, respectively, and there was no significant difference in diagnostic performance between S-Detect and radiologists. Moreover, the radiologists who utilized S-Detect exhibited better diagnostic sensitivity than those who did not (92.0% vs 84.0%); however, their specificity and PPV were lower (85.1% vs 95.5%, and 82.1% vs 93.3%, respectively) [41]. The enhanced diagnostic sensitivity from the aid of CAD enables radiologists to identify actual thyroid malignant tumors and reduces the missed diagnosis rate. This suggests that S-Detect is helpful for inexperienced or non-thyroid radiologists. However, the reduced diagnostic specificity when radiologists use S-Detect needs to be considered in clinical use.
Xia et al evaluated the diagnostic performance of S-Detect for thyroid nodules of different pathological subtypes. Among all thyroid nodules, the sensitivity of S-Detect to identify malignant thyroid nodules was higher than that of experienced radiologists, but the specificity was lower. The sensitivity of S-Detect to detect papillary thyroid cancer was higher than that of experienced radiologists, but the specificity and accuracy were lower. Compared with the diagnostic ability of experienced radiologists, S-Detect had relatively low diagnostic performance in identifying follicular thyroid carcinoma [23]. The study found that S-Detect has different diagnostic capabilities for thyroid nodules in different pathological subtypes, but radiologists can still benefit from the overall high sensitivity.
Conclusions
As a recently developed commercial US CAD system, S-Detect has the considerable advantages of convenient and fast clinical adaptability and good diagnostic performance. In clinical practice, this tool can be used to improve the diagnostic performance of radiologists and can be used as a teaching tool for novice or non-professional radiologists. S-Detect not only provides a classification model for the final diagnosis but also describes the US characteristics of the mass.
For the diagnosis of breast cancer, most studies showed that the specificity and PPV of S-Detect were equivalent or higher than those of expert radiologists. Radiologists can screen out real benign lesions according to the final assessments of S-Detect, reducing the rate of misdiagnosis. However, for thyroid nodules, S-Detect has a high sensitivity and low specificity. Radiologists can detect a higher proportion of genuine malignant tumors according to the final assessments of S-Detect, reducing the missed diagnosis rate. Therefore, radiologists can obtain different types of benefits from S-Detect.
For young doctors, the assistance of S-Detect can greatly improve their diagnostic performance and confidence and can be used as a training mechanism for residents. S-Detect can be used in top-level hospitals as well as in smaller local hospitals. This tool can help small hospitals improve their diagnostic performance of malignant breast and thyroid tumors.
Challenges and Future Perspectives
As a commercial CAD system, S-Detect has excellent clinical performance, although there are still some limitations to its use. To fully integrate future S-Detect technology into the work of clinicians and apply it worldwide, the following issues should be addressed. First, for S-Detect, the imaging information of grayscale US is the only reference for evaluating mass lesions. However, the classification of lesions by radiologists is based on the comprehensive evaluation of all patient information, including medical history and other auxiliary imaging methods such as color Doppler flow imaging and US elastography. Therefore, the development of multi-modal training CAD models (B-mode, color Doppler, contrast-enhanced ultrasonography, and elastography) based on various imaging data can provide complete lesion information, thus improving the diagnostic accuracy of CAD models. Second, US-based diagnosis is still limited in part by operator experience. Input images acquired by highly experienced radiologists and novices can be different, resulting in inconsistent output results of S-Detect. Enabling the CAD system to automatically obtain the best quality static images of lesions needs to be established. Third, S-Detect has a poor ability to distinguish non-mass lesions (eg, architectural distortion, calcifications, enlarged lymph nodes, and diffuse inflammation). It is hard to clarify the margins of non-mass lesions; thus, it is difficult for S-Detect to determine the region of interest of non-mass lesions. The effective identification of all features of the lesion, including calcification, must be considered in the future development of S-Detect systems. We believe that future commercial CAD systems will not only be able to distinguish benign and malignant masses but also further classify specific benign diseases, such as inflammatory masses, cysts, and abscesses.
The development of future commercial CAD systems must focus on how the progress of artificial intelligence can be implemented in a way that maximizes its clinical benefit.
Figures
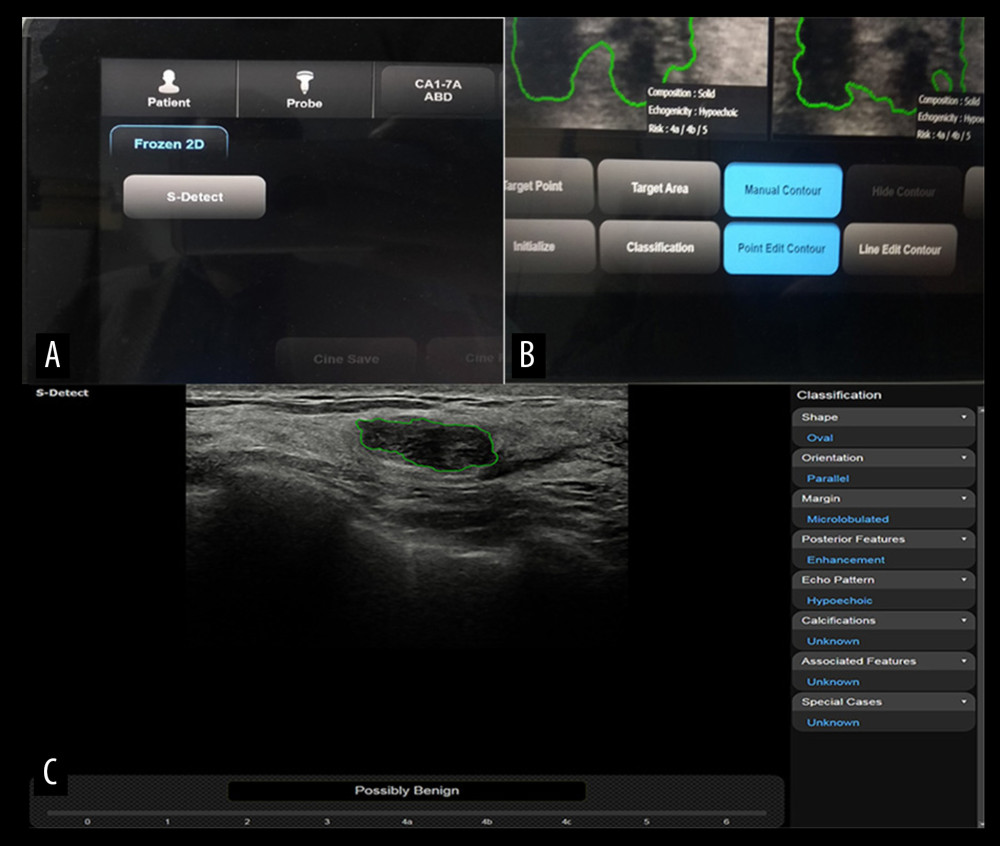 Figure 1. The assessment process with S-Detect(A) When a lesion is selected, “S-Detect” is pressed to initiate the analysis. (B) If the outline drawn automatically by the system is not satisfactory, the border of the lesion can be redrawn by pressing the “Manual Contour” button. (C) S-Detect presents ultrasonographic features on the right of the screen and a final assessment at the bottom.
Figure 1. The assessment process with S-Detect(A) When a lesion is selected, “S-Detect” is pressed to initiate the analysis. (B) If the outline drawn automatically by the system is not satisfactory, the border of the lesion can be redrawn by pressing the “Manual Contour” button. (C) S-Detect presents ultrasonographic features on the right of the screen and a final assessment at the bottom. 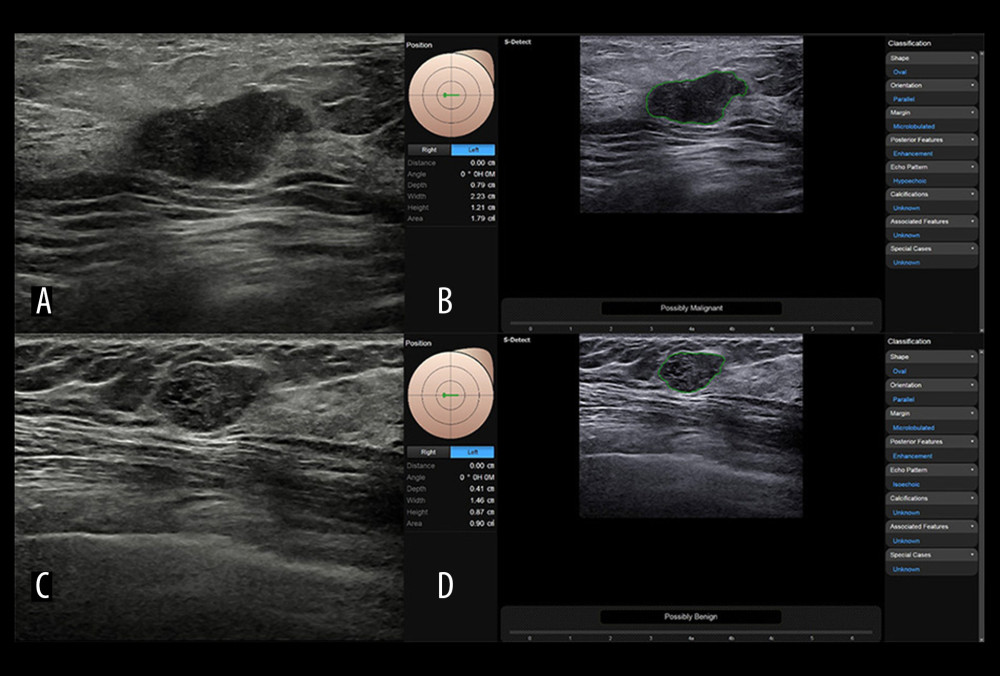 Figure 2. Representative case of (A, B) malignant and (C, D) benign breast nodulesImages of (A) B-mode US and (B) S-Detect result of a 67-year-old woman with invasive cancer in her right breast. After the region of interest was set, S-Detect automatically analyzed the ultrasound features of the lesion and displayed a final assessment of “possibly malignant” based on the lesion features listed in the right column: oval shape, parallel orientation, microlobulated margin, hypoechoic echo pattern, and posterior features enhancement. Images of (C) B-mode US and (D) S-Detect result of a 47-year-old woman with fibroadenoma in her right breast. After the region of interest was set, S-Detect automatically analyzed the ultrasound features of the lesion and displayed a final assessment of “possibly benign” based on the lesion features listed in the right column: oval shape, parallel orientation, microlobulated margin, isoechoic echo pattern, and posterior features enhancement.
Figure 2. Representative case of (A, B) malignant and (C, D) benign breast nodulesImages of (A) B-mode US and (B) S-Detect result of a 67-year-old woman with invasive cancer in her right breast. After the region of interest was set, S-Detect automatically analyzed the ultrasound features of the lesion and displayed a final assessment of “possibly malignant” based on the lesion features listed in the right column: oval shape, parallel orientation, microlobulated margin, hypoechoic echo pattern, and posterior features enhancement. Images of (C) B-mode US and (D) S-Detect result of a 47-year-old woman with fibroadenoma in her right breast. After the region of interest was set, S-Detect automatically analyzed the ultrasound features of the lesion and displayed a final assessment of “possibly benign” based on the lesion features listed in the right column: oval shape, parallel orientation, microlobulated margin, isoechoic echo pattern, and posterior features enhancement. 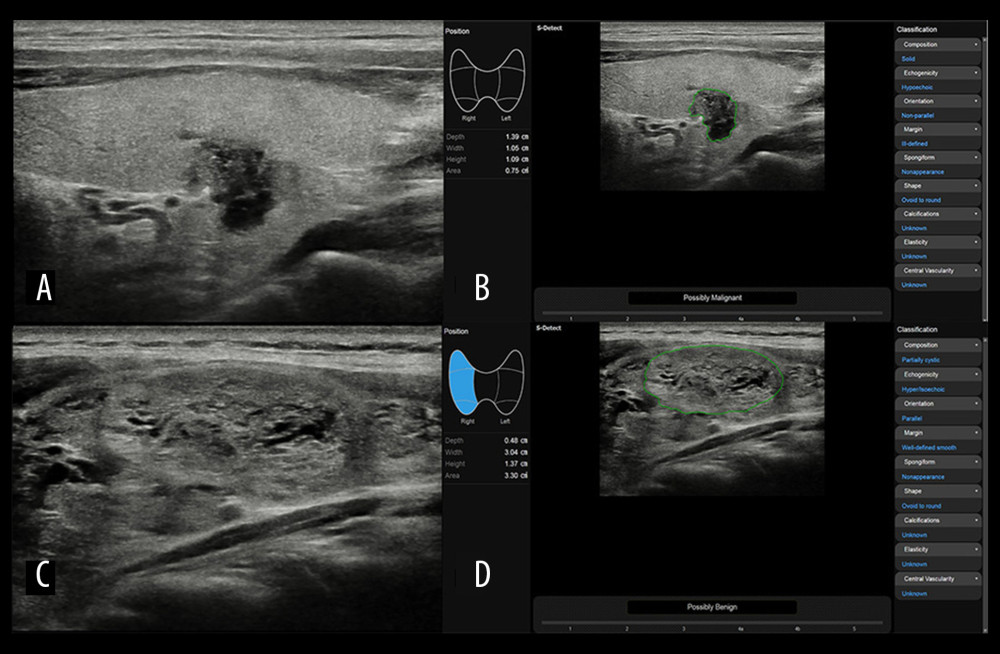 Figure 3. Representative case of (A, B) malignant and (C, D) benign thyroid nodulesImages of (A) B-mode US and (B) S-Detect result of a 39-year-old man with papillary thyroid carcinoma. After the region of interest was set, S-Detect automatically analyzed the ultrasound features of the lesion and displayed a final assessment of “possibly malignant” based on the lesion features listed in the right column: solid composition, non-parallel orientation, hypoechoic echogenicity, ill-defined margin, nonappearance spongiform, and ovoid to round shape. Images of (C) B-mode US and (D) S-Detect result of a 43-year-old woman with follicular adenoma. After the region of interest was set, S-Detect automatically analyzed the ultrasound features of the lesion and displayed final assessment of “possibly benign” based on the lesion features listed in the right column: partially cystic composition, parallel orientation, hyper/isoechoic echogenicity, well-defined smooth margin, nonappearance spongiform, and ovoid to round shape.
Figure 3. Representative case of (A, B) malignant and (C, D) benign thyroid nodulesImages of (A) B-mode US and (B) S-Detect result of a 39-year-old man with papillary thyroid carcinoma. After the region of interest was set, S-Detect automatically analyzed the ultrasound features of the lesion and displayed a final assessment of “possibly malignant” based on the lesion features listed in the right column: solid composition, non-parallel orientation, hypoechoic echogenicity, ill-defined margin, nonappearance spongiform, and ovoid to round shape. Images of (C) B-mode US and (D) S-Detect result of a 43-year-old woman with follicular adenoma. After the region of interest was set, S-Detect automatically analyzed the ultrasound features of the lesion and displayed final assessment of “possibly benign” based on the lesion features listed in the right column: partially cystic composition, parallel orientation, hyper/isoechoic echogenicity, well-defined smooth margin, nonappearance spongiform, and ovoid to round shape. References
1. Mann RM, Hooley R, Barr RG, Moy L, Novel approaches to screening for breast cancer: Radiology, 2020; 297; 266-85
2. Ko SY, Kim EK, Sung JM, Diagnostic performance of ultrasound and ultrasound elastography with respect to physician experience: Ultrasound Med Biol, 2014; 40; 854-63
3. Rix A, Lederle W, Theek B, Advanced ultrasound technologies for diagnosis and therapy: J Nucl Med, 2018; 59; 740-46
4. Zheng Y, Xu S, Kang H, Zhan W, A single-center retrospective validation study of the American College of Radiology Thyroid Imaging Reporting and Data System: Ultrasound Q, 2018; 34; 77-83
5. Tessler FN, Middleton WD, Grant EG, Thyroid Imaging Reporting and Data System (TI-RADS): A user’s guide: Radiology, 2018; 287; 29-36
6. Lee YJ, Choi SY, Kim KS, Yang PS, Variability in observer performance between faculty members and residents using Breast Imaging Reporting and Data System (BI-RADS)-Ultrasound, Fifth Edition (2013): Iran J Radiol, 2016; 13; e28281
7. Persichetti A, Di Stasio E, Coccaro C, Inter- and intraobserver agreement in the assessment of thyroid nodule ultrasound features and classification systems: A blinded multicenter study: Thyroid, 2020; 30; 237-42
8. Wang Y, Liu Y, Zheng X, Added value of different types of elastography in evaluating ultrasonography detected breast lesions: A compared study with mammography: Clin Breast Cancer, 2020; 20; e366-e72
9. Balleyguier C, Opolon P, Mathieu MC, New potential and applications of contrast-enhanced ultrasound of the breast: Own investigations and review of the literature: Eur J Radiol, 2009; 69; 14-23
10. Alcazar JL, Jurado M, Three-dimensional ultrasound for assessing women with gynecological cancer: A systematic review: Gynecol Oncol, 2011; 120; 340-46
11. Shen J, Zhang CJP, Jiang B, Artificial intelligence versus clinicians in disease diagnosis: Systematic review: JMIR Med Inform, 2019; 7; e10010
12. Singh S, Maxwell J, Baker JA, Nicholas JL, Lo JY, Computer-aided classification of breast masses: Performance and interobserver variability of expert radiologists versus residents: Radiology, 2011; 258; 73-80
13. Jalalian A, Mashohor SB, Mahmud HR, Computer-aided detection/diagnosis of breast cancer in mammography and ultrasound: A review: Clin Imaging, 2013; 37; 420-26
14. Han S, Kang HK, Jeong JY, A deep learning framework for supporting the classification of breast lesions in ultrasound images: Phys Med Biol, 2017; 62; 7714-28
15. Cheng JZ, Chou YH, Huang CS, Computer-aided US diagnosis of breast lesions by using cell-based contour grouping: Radiology, 2010; 255; 746-54
16. Lee JG, Jun S, Cho YW, Deep learning in medical imaging: general overview: Korean J Radiol, 2017; 18; 570-84
17. Zhou LQ, Wang JY, Yu SY, Artificial intelligence in medical imaging of the liver: World J Gastroenterol, 2019; 25; 672-82
18. Li X, Zhang S, Zhang Q, Diagnosis of thyroid cancer using deep convolutional neural network models applied to sonographic images: A retrospective, multicohort, diagnostic study: Lancet Oncol, 2019; 20; 193-201
19. Wu JY, Zhao ZZ, Zhang WY, Computer-aided diagnosis of solid breast lesions with ultrasound: Factors associated with false-negative and false-positive results: J Ultrasound Med, 2019; 38; 3193-202
20. Choi YJ, Baek JH, Park HS, A Computer-aided diagnosis system using artificial intelligence for the diagnosis and characterization of thyroid nodules on ultrasound: initial clinical assessment: Thyroid, 2017; 27; 546-52
21. Choi JH, Kang BJ, Baek JE, Application of computer-aided diagnosis in breast ultrasound interpretation: Improvements in diagnostic performance according to reader experience: Ultrasonography, 2018; 37; 217-25
22. Choi JS, Han BK, Ko ES, Effect of a deep learning framework-based computer-aided diagnosis system on the diagnostic performance of radiologists in differentiating between malignant and benign masses on breast ultrasonography: Korean J Radiol, 2019; 20; 749-58
23. Xia S, Yao J, Zhou W, A computer-aided diagnosing system in the evaluation of thyroid nodules-experience in a specialized thyroid center: World J Surg Oncol, 2019; 17; 210
24. Zhao C, Xiao M, Jiang Y, Feasibility of computer-assisted diagnosis for breast ultrasound: The results of the diagnostic performance of S-detect from a single center in China: Cancer Manag Res, 2019; 11; 921-30
25. Wu GG, Zhou LQ, Xu JW, Artificial intelligence in breast ultrasound: World J Radiol, 2019; 11; 19-26
26. Bray F, Ferlay J, Soerjomataram I, Global cancer statistics. 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries: Cancer J Clin, 2018; 68; 394-424
27. Jacobs MA, Wolff AC, Macura KJ, Multiparametric and multimodality functional radiological imaging for breast cancer diagnosis and early treatment response assessment: J Natl Cancer Inst Monogr, 2015; 2015; 40-46
28. Li J, Sang T, Yu WH, The value of S-Detect for the differential diagnosis of breast masses on ultrasound: A systematic review and pooled meta-analysis: Med Ultrason, 2020; 22; 211-19
29. Kim K, Song MK, Kim EK, Yoon JH, Clinical application of S-Detect to breast masses on ultrasonography: A study evaluating the diagnostic performance and agreement with a dedicated breast radiologist: Ultrasonography, 2017; 36; 3-9
30. Lee SE, Moon JE, Rho YH, Which supplementary imaging modality should be used for breast ultrasonography? Comparison of the diagnostic performance of elastography and computer-aided diagnosis: Ultrasonography, 2017; 36; 153-59
31. Lee J, Kim S, Kang BJ, Evaluation of the effect of computer aided diagnosis system on breast ultrasound for inexperienced radiologists in describing and determining breast lesions: Med Ultrason, 2019; 21; 239-45
32. Park HJ, Kim SM, La Yun B, A computer-aided diagnosis system using artificial intelligence for the diagnosis and characterization of breast masses on ultrasound: Added value for the inexperienced breast radiologist: Medicine (Baltimore), 2019; 98; e14146
33. Bartolotta TV, Orlando A, Cantisani V, Focal breast lesion characterization according to the BI-RADS US lexicon: Role of a computer-aided decision-making support: Radiol Med, 2018; 123; 498-506
34. Yoon JH, Kim MJ, Moon HJ, Subcategorization of ultrasonographic BI-RADS category 4: Positive predictive value and clinical factors affecting it: Ultrasound Med Biol, 2011; 37; 693-99
35. Shin JH, Baek JH, Chung J, Ultrasonography diagnosis and imaging-based management of thyroid nodules: Revised Korean Society of Thyroid Radiology consensus statement and recommendations: Korean J Radiol, 2016; 17; 370-95
36. Lee YH, Baek JH, Jung SL, Ultrasound-guided fine needle aspiration of thyroid nodules: A consensus statement by the korean society of thyroid radiology: Korean J Radiol, 2015; 16; 391-401
37. Jegerlehner S, Bulliard JL, Aujesky D, Overdiagnosis and overtreatment of thyroid cancer: A population-based temporal trend study: PLoS One, 2017; 12; e0179387
38. Wei Q, Zeng SE, Wang LP, The value of S-Detect in improving the diagnostic performance of radiologists for the differential diagnosis of thyroid nodules: Med Ultrason, 2020; 22; 415-23
39. Choi SH, Kim EK, Kwak JY, Kim MJ, Son EJ, Interobserver and intraobserver variations in ultrasound assessment of thyroid nodules: Thyroid, 2010; 20; 167-72
40. Park CS, Kim SH, Jung SL, Observer variability in the sonographic evaluation of thyroid nodules: J Clin Ultrasound, 2010; 38; 287-93
41. Yoo YJ, Ha EJ, Cho YJ, Kim HL, Han M, Kang SY, Computer-aided diagnosis of thyroid nodules via ultrasonography: Initial clinical experience: Korean J Radiol, 2018; 19; 665-72
Figures
Figure 1. The assessment process with S-Detect(A) When a lesion is selected, “S-Detect” is pressed to initiate the analysis. (B) If the outline drawn automatically by the system is not satisfactory, the border of the lesion can be redrawn by pressing the “Manual Contour” button. (C) S-Detect presents ultrasonographic features on the right of the screen and a final assessment at the bottom.Figure 2. Representative case of (A, B) malignant and (C, D) benign breast nodulesImages of (A) B-mode US and (B) S-Detect result of a 67-year-old woman with invasive cancer in her right breast. After the region of interest was set, S-Detect automatically analyzed the ultrasound features of the lesion and displayed a final assessment of “possibly malignant” based on the lesion features listed in the right column: oval shape, parallel orientation, microlobulated margin, hypoechoic echo pattern, and posterior features enhancement. Images of (C) B-mode US and (D) S-Detect result of a 47-year-old woman with fibroadenoma in her right breast. After the region of interest was set, S-Detect automatically analyzed the ultrasound features of the lesion and displayed a final assessment of “possibly benign” based on the lesion features listed in the right column: oval shape, parallel orientation, microlobulated margin, isoechoic echo pattern, and posterior features enhancement.Figure 3. Representative case of (A, B) malignant and (C, D) benign thyroid nodulesImages of (A) B-mode US and (B) S-Detect result of a 39-year-old man with papillary thyroid carcinoma. After the region of interest was set, S-Detect automatically analyzed the ultrasound features of the lesion and displayed a final assessment of “possibly malignant” based on the lesion features listed in the right column: solid composition, non-parallel orientation, hypoechoic echogenicity, ill-defined margin, nonappearance spongiform, and ovoid to round shape. Images of (C) B-mode US and (D) S-Detect result of a 43-year-old woman with follicular adenoma. After the region of interest was set, S-Detect automatically analyzed the ultrasound features of the lesion and displayed final assessment of “possibly benign” based on the lesion features listed in the right column: partially cystic composition, parallel orientation, hyper/isoechoic echogenicity, well-defined smooth margin, nonappearance spongiform, and ovoid to round shape. In Press
Clinical Research
Body Weight and Insulin Resistance Indicators Among ChildrenMed Sci Monit In Press; DOI: 10.12659/MSM.951434
Clinical Research
Comparison of Radiographic Cervical Sagittal Alignment Parameters in Patients With Nonspecific Neck Pain, D...Med Sci Monit In Press; DOI: 10.12659/MSM.952950
Clinical Research
Combined Fibrinogen and Urinary α1-Microglobulin as Predictors of Respiratory Tract Infection in Children w...Med Sci Monit In Press; DOI: 10.12659/MSM.951066
Database Analysis
Evaluation of Salivary Total Oxidant Status (TOS) and Total Antioxidant Status (TAS) in Orthodontic Patient...Med Sci Monit In Press; DOI: 10.12659/MSM.952052
Most Viewed Current Articles
17 Jan 2024 : Review article 14,175,576
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,756,620
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,465,966
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,651
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387