25 December 2021: Clinical Research
Association of Perioperative Myocardial Injury with 30-Day and Long-Term Mortality in Older Adult Patients Undergoing Orthopedic Surgery in China
Wenlan Hu1BCDE, Youzhou Chen1BCD, Kaiping Zhao2BCD, Jihong Wang1BCD, Mei Zheng1BCD, Ying Zhao1BCD, Hao Han1BCD, Qiong Zhao3AE, Xingshan Zhao1AE*DOI: 10.12659/MSM.932036
Med Sci Monit 2021; 27:e932036






Abstract
BACKGROUND: Myocardial injury after noncardiac surgery (MINS) is common and associated with postoperative mortality. We assessed MINS occurrence and association with 30-day and long-term mortality in older adult patients undergoing orthopedic surgery in China.
MATERIAL AND METHODS: This was a retrospective study of consecutive patients who underwent orthopedic surgery between January 1, 2009, and December 31, 2017, at Beijing Jishuitan Hospital. MINS was defined as postoperative troponin I peak elevation above the 99th percentile upper reference limit (>0.034 µg/L) within 30 days after surgery. Outcomes were 30-day postoperative mortality and long-term all-cause mortality.
RESULTS: From 34 901 patients, 5897 (16.9%) had serial troponin I measurements, and 266 (4.5%) had MINS after surgery. Mean patient age was 71.1±9.2 years; 32.9% were male. Among patients with MINS, 180 had myocardial infarction (MI) (3.2%). Patients with MI had higher 30-day and long-term mortality than those without MI (8.9% vs 1.2%; P<0.016 and 18.9% vs 3.5%; P=0.001). Male sex (OR 5.87, 95% CI 1.75-19.67; P=0.004), RCRI ≥2 (OR 5.05, 95% CI 1.67-15.31; P=0.004), and MI (OR 9.13, 95% CI 1.13-73.63; P=0.011) were independently associated with 30-day mortality. Age (HR 1.07, 95% CI 1.03-1.11; P=0.001), male sex (HR 2.96, 95% CI 1.51-5.80; P=0.002), RCRI ≥2 (HR 2.01, 95% CI 1.03-3.94; P=0.041), orthopedic trauma (HR 3.40, 95% CI 1.00-11.44; P=0.049), and MI (HR 7.33, 95% CI 2.22-24.20; P=0.001) were predictors of 2-year mortality.
CONCLUSIONS: Perioperative MI was independently associated with 30-day and long-term mortality after orthopedic surgery, providing a potential indicator of high risk of mortality in patients who could benefit from targeted prevention and intervention.
Keywords: Mortality, Orthopedics, perioperative period, Aged, 80 and over, Cause of Death, Electrocardiography, Female, Humans, Male, Myocardial Ischemia, Orthopedic Procedures, Postoperative Complications, troponin I
Background
Perioperative mortality in patients undergoing noncardiac surgery is a significant global burden [1], and cardiovascular complications are significant causes of perioperative mortality. In the perioperative setting, cardiac troponin values are frequently elevated; however, their pathophysiology is not yet fully understood. Recent studies have demonstrated that 5% to 25% of patients have elevation of troponin levels after noncardiac surgery [2–5]. An isolated elevation of cardiac troponin is associated with a higher mortality risk [2,6,7]. Myocardial injury, defined as an increased cardiac troponin level, has recently been introduced by the Fourth Universal Definition of Myocardial Infarction (UDMI) [6]. Perioperative myocardial injury is estimated to affect about 8 million patients worldwide annually [2,8] and is independently correlated with a significant risk of cardiovascular complication and death in the first 2 years after surgery [2,4,8]. As a result, a new concept termed myocardial injury after noncardiac surgery (MINS) was proposed, which includes myocardial infarction (MI) and ischemic myocardial injury that does not satisfy the definition of MI [2,8]. MINS has been shown to be common and an independent predictor of 30-day mortality after surgery. While the relationship between MINS and short-term mortality has been confirmed in large prospective studies [2,8], data regarding its relationship with long-term mortality are limited.
Orthopedic surgery is the most common noncardiac major surgical procedure performed in adults, especially in older adults. Orthopedic surgery is considered an intermediate-risk procedure with an intermediate risk of cardiac death and MI [9]. Previous studies reported an incidence of perioperative cardiac events of 0.2% to 10.2% after orthopedic surgery [10–14]. China has the largest and most rapidly growing elderly population in the world. With advances in anesthetic and surgical techniques, orthopedic surgery is performed with increasing frequency, especially in those older patients with multiple comorbidities and a high risk of falls and fractures. Therefore, perioperative cardiac complications are an important clinical concern.
To date, most studies reported in the literature focused on patients from Western countries. The rates of perioperative major adverse cardiovascular events vary by race and ethnicity [15], and no study has investigated MINS in elderly Chinese patients undergoing orthopedic surgery. Therefore, we performed the present study of adult patients treated with orthopedic surgery in an attempt to determine (1) the incidence of MINS, (2) the clinical characteristics of patients with MINS, (3) the 30-day and long-term (2-year) mortality rate after orthopedic surgery in patients with and without fulfilling the definition of MI, and (4) the predictors of 30-day and long-term mortality after orthopedic surgery.
Material and Methods
STUDY DESIGN:
We conducted a retrospective single-center cohort study involving patients who underwent orthopedic surgery between January 1, 2009, and December 31, 2017, at Beijing Jishuitan Hospital, a 1500-bed tertiary center of orthopedics. This article adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Supplementary Material). This study protocol was approved by the Ethics Committee of Beijing Jishuitan Hospital (no. 201905-05), and all included patients gave their informed consent.
PATIENTS:
Eligible patients were ≥50 years of age and underwent hip, knee, spine, or orthopedic trauma surgical procedures, received general or regional anesthesia, had serial perioperative troponin measurements, and stayed in the hospital for at least 1 night after surgery. We excluded patients who were incorrectly screened as follows: <50 years, <24-h hospital stay, surgery under local anesthesia, cardiac surgery or MI within 14 days before surgery, only 1 measured troponin value or elevated postoperative troponin values without a dynamic change, and missing or incomplete preoperative baseline level data.
Routine perioperative troponin I measurements were recommended in at-risk patients before surgery and on postoperative days 1 and 2, and later if clinically indicated. These patients had at least 1 major cardiovascular risk factor, such as a history of ischemic heart disease, heart failure, stroke, diabetes mellitus, or chronic kidney disease, based on current guidelines [16]. In patients with minor risk factors, serial troponin I measurements were ordered by the treating clinician, considering elderly age or recently suspected symptoms of ischemic disease. For each patient, the peak value of postoperative troponin I measurements was used in the analysis.
TROPONIN I MEASUREMENTS:
Troponin I levels were determined by a troponin I assay (chemiluminescent immunoassay, Beckman Coulter, CA, USA), and the recommended diagnostic threshold of 0.034 μg/L was used to evaluate troponin I elevation. The laboratory platform used was the Access 2 Immunoassay system. The assays limit of detection was 0.01 μg/L, limit of blank was 0.01 μg/L, and 99th percentile of healthy reference population was 0.02 μg/L.
DATA COLLECTION AND GROUPING:
Patient baseline demographics, medical history, electrocardiography (ECG), echocardiography, coronary angiography, comorbidities, and serial laboratory measurements, including troponin I, were obtained from the hospital administrative database. The Revised Cardiac Risk Index (RCRI) was calculated for all patients [17]. Each patient was assigned an American Society of Anesthesiologists physical status class. Data on ischemia symptoms, ECG changes, and treatment initiated by the consultant cardiologist were collected in those patients who had a cardiology consultation.
Large studies have defined MINS as a peak level of ≥0.03 μg/L on conventional troponin T testing that occurs during or within 30 days after noncardiac surgery [2]. When using high-sensitivity cTnT (hs-cTnT) assays, MINS was defined as a concentration of at least 20 ng/L, combined with an absolute change of at least 5 ng/L or an absolute postoperative hs-cTnT of at least 65 ng/L [8,18,19]. However the cut-off value of troponin I for myocardial injury ranges from 0.03 to 0.07 μg/L [18,19]. In the current study, we defined MINS as an elevation above the 99th percentile upper reference limit (>0.034 μg/L) for troponin I assay within 30 days after surgery, based on current guidelines [6]. An elevation with evidence of a nonischemic etiology, such as sepsis, pulmonary embolus, atrial fibrillation, cardioversion, or chronic elevation, was not regarded as MINS [16,18].
All patient cases with an elevated troponin I measurement were adjudicated by 2 independent investigators based on all clinical information obtained during index hospitalization. We further characterized patients as to whether the MINS also fulfilled at least 1 of the additional criteria required for the diagnosis of MI [6]. The patients were divided into MI and no-MI groups. Because all cases of MINS necessarily fulfilled the troponin criteria, ≥1 of the following defining features was required: the presence of ischemic symptoms, ischemic ECG changes (new or presumed new ST-segment or T-wave changes, new left bundle-branch block, or development of pathological Q waves), or new or presumed new ischemic abnormality on cardiac imaging. In cases of disagreement between the 2 investigators, consensus was sought by discussion with a third senior physician.
OUTCOMES AND FOLLOW-UP:
The main outcome was long-term (2-year) all-cause mortality, which was defined as all-cause mortality until the last follow-up. The secondary outcome was all-cause mortality 30 days after surgery. Follow-up time was calculated from surgery until June 30, 2018. All patients were routinely followed according to their treating physicians’ discretion. The information about survival status was retrieved by phone.
STATISTICAL ANALYSIS:
Data were analyzed using SPSS version 20.0 (IBM, Armonk, NY, USA). Normally distributed continuous data were presented as means±standard deviation and compared using the
Results
CHARACTERISTICS OF STUDY PATIENTS:
The baseline characteristics of the 266 patients with MINS are presented in Table 1. The mean age of the patients was 71.1±9.2 years, and 87 (32.9%) patients were male. The median peak troponin I level was 0.23 (0.08–1.32) μg/L.
A total of 180 (67.7%) patients had at least 1 ischemic feature (ischemic symptom or ECG changes suggestive of new ischemia) and were in the MI group, and 86 (32.3%) patients had isolated troponin I elevation without an ischemic feature and were in the no-MI group. The incidence of perioperative MI was 3.2% of orthopedic patients with troponin detection. The MI group had significantly more frequent coronary heart disease (46.7% vs 19.8%;
Among the 180 patients with perioperative MI, chest pain was present in only 24 (13.3%) patients. Atypical ischemic symptoms such as palpitation (15.0%), shortness of breath (29.4%), and dyspnea (14.4%) were observed. ECG findings suggestive of new myocardial ischemia, especially ST-segment changes or T-wave inversion, were observed in 108 patients (60.0%). A total of 14 (7.8%) of the 180 patients’ ECGs showed ST-segment elevation (≥1 mm), 59 (32.8%) showed ST-segment depression (≥1 mm), and 35 (19.4%) showed minimal ST-segment depression (<1 mm) or T-wave inversion. A total of 14 patients had a primary diagnosis of ST-segment elevation myocardial infarction (STEMI) (7.8%), and 166 patients were recorded to have non-ST-segment elevation myocardial infarction (NSTEMI) (92.2%). NSTEMI was more common than STEMI.
MINS occurred from surgery to 14 days after surgery. The occurrence peaked on postoperative day 2 (62.4%), and 80.8% and 95.9% occurred by postoperative days 3 and 5, respectively. In the 14 patients with postoperative STEMI, 1 patient had prior coronary stenting twice, at 7 and 4 months before surgery. Two patients were considered as NSTEMI by postoperative days 3 but experienced STEMI on days 10 and 12 after surgery. At 30-day follow-up, there were 7 (50.0%) deaths in the STEMI group; most deaths were from cardiac shock. During the 3-year follow-up, there were 8 (53.3%) deaths.
TIME-EVENT ANALYSIS OF THE 2 GROUPS:
The median follow-up was 42 (range, 12–70) months after surgery, all-cause death occurred in 52 patients (19.5%). A total of 229 patients were censored at the follow-up time of 2 years. Using Kaplan-Meier survival analysis, we determined the 30-day mortality was 6.4% and 2-year mortality was 19.2% in the patients with MINS. Patients who developed MI had significantly higher 30-day mortality than those who did not develop MI (8.9% vs 1.2%; P<0.016). The 2-year mortality in patients with MI was remarkably higher during the follow-up (18.9% vs 3.5%; P=0.001), as shown in Figure 2.
PREDICTORS OF MORTALITY AFTER MINS:
Table 2 shows results from the logistic regression analysis, with 30-day mortality treated as the index outcome. Male sex, coronary heart disease, RCRI ≥2, troponin I, and MI were associated with 30-day mortality in univariate analysis. When adjusted for age, coronary heart disease, procedure type, troponin I level, and MI, the stepwise logistic regression model revealed the following factors as strong predictors of 30-day mortality: male sex (OR 5.87, 95% CI 1.75–19.67; P=0.004), RCRI ≥2 (OR 5.05, 95% CI 1.67–15.31; P=0.004), and MI (OR 9.13, 95% CI 1.13–73.63; P=0.011).
The variables age, coronary heart disease, RCRI ≥2, orthopedic trauma, troponin level, and MI were the associated factors for 2-year mortality. Cox proportional hazard analysis was also performed to determine the predictors of 2-year mortality in the study population. Stepwise modeling was carried out using forward selection (P<0.05) to determine the most significant predictors. Age (HR 1.07, 95% CI 1.03–1.11; P=0.001), male sex (HR 2.96, 95% CI 1.51–5.80; P=0.002), RCRI ≥2 (HR 2.01, 95% CI 1.03–3.94; P=0.041),orthopedic trauma (HR 3.40, 95% CI 1.00–11.44; P=0.049), and MI (HR 7.33, 95% CI 2.22–24.20; P=0.001) were significant predictors of 2-year mortality after orthopedic surgery (Table 3). Figure 3 presents the adjusted Kaplan-Meier survival curves for the patients with and without MI over long-term follow-up.
Postoperative troponin peak was significantly associated with 30-day (OR 1.03, 95% CI 1.01–1.06;
Postoperative coronary angiography was performed in 14 patients, and 11 patients had postoperative MI. Thirteen patients had significant coronary stenosis and underwent coronary revascularization. Only 3 patients with STEMI underwent postoperative coronary angiography; 1 of them had an acute plaque rupture and thrombus in the right coronary artery, experienced cardiac arrest in the catheterization room, and died in the Coronary Intensive Care Unit within 24 h after percutaneous coronary intervention. The other 2 patients had significant occlusion lesions and underwent coronary revascularization.
Discussion
Our study provides clinicians with valuable information on all-cause mortality in older adult patients undergoing orthopedic surgery in China. In this retrospective study, we assessed the incidence of MINS in older adult patients undergoing orthopedic surgery. A total of 266 patients (4.5%) had MINS within 30 days after orthopedic surgery, and the incidence of perioperative MI was 3.2% of patients with troponin detection. Patients who developed perioperative MI were at higher risk for substantial 30-day and long-term mortality.
Myocardial ischemic injury is a leading cause of 30-day mortality after noncardiac surgery [2,8]. Recently, MINS was established as a diagnosis, underlining the prognostic relevance of postoperative ischemic troponin elevations [2,8]. Large prospective cohort studies of patients undergoing noncardiac surgery that had routine troponin measurements after surgery have shown that 13% to 18% develop MINS within 30 days after surgery [4,8]. Among the patients with MINS, about 22% to 29% fulfilled the universal definition of myocardial infarction [18].
Orthopedic surgery is associated with a number of conditions that cause bleeding, inflammation, and significant physiologic stresses [7]. The incidence of troponin elevation and cardiac complication varies with different types of orthopedic surgery. Several previous small studies have demonstrated that 3.1% to 8.7% of patients developed myocardial injury after hip, knee, or spine surgery [13,15]. The incidence of perioperative cardiac events (including MI) ranged from 0.2% to 2% for joint and spine surgeries [9–13]. Our data support the findings of these orthopedic surgery studies.
Recently, Thomas et al performed a large, prospective VISION substudy of patients undergoing orthopedic surgery and found that MINS occurred in 11.9% of patients who underwent these orthopedic procedures, with 52% of patients who developed MINS having ischemic features (fulfilled additional criteria required for MI). In their substudy of orthopedic surgery, MINS was associated independently with 30-day mortality, and the 30-day mortality rate increased significantly for patients with MINS who had an ischemic feature (OR 18.25, 95% CI 10.06–33.10) and for those who did not have an ischemic feature (OR 7.35, 95% CI 3.37–16.01); however, long-term outcomes were not reported [20]. Our data showed that MINS occurred in 4.5% of patients with measured troponin levels, and more than half (67.7%) of patients fulfilled the criteria for the universal definition of MI. The differences in study patients and research design could possibly explain the lower incidence of MINS observed in our study when compared with the large prospective VISION study. In addition, the troponin measurements in that study were performed routinely in the first 3 days after surgery. In the present study, serum troponin levels were tested in the perioperative setting if there was suspicion of acute coronary syndrome in some patients. Therefore, it is possible that we missed additional asymptomatic postoperative myocardial ischemia and underestimated the incidence of MINS.
MINS has been reported to be associated with a higher risk of morality at 30 days and up to 2 years after noncardiac surgery [18]. Puelacher et al conducted a prospective study of 2018 consecutive adults who underwent noncardiac surgery with systematic hs-TnT measurements and demonstrated that MINS was independently associated with an increased risk of 1-year mortality (adjusted HR 1.48, 95% CI 1.07–2.06). The 30-day and 1-year mortality rates were comparable among patients with MINS who fulfilled no additional criteria required for MI compared with those with at least 1 additional criterion [4]. In the present study, patients with perioperative MI had significantly higher 30-day mortality and 2-year mortality rates than did patients with MINS who did not fulfill additional criteria for MI.
A previous study showed that risk of death is dependent on the degree of troponin I elevation [5]. In the POISE study, the highest quartile of troponin value was an independent predictor of 30-day mortality [21]. The VISION study also showed that peak measurements of troponin were independently correlated with 30-day mortality in multivariable analyses [2]. As previously suggested by van Waes et al, a troponin increase is associated with a significant risk of 30-day mortality [5]. However, Vallet et al showed that an isolated cardiac troponin increase was not predictive of 6-month mortality in elderly patients with hip fracture [22]. In the present study, we found that perioperative troponin I levels in patients who underwent orthopedic surgeries were associated with a significantly increased risk of short-term (OR 1.03, 95% CI 1.01–1.06) and long-term mortality (OR 1.02, 95% CI 1.00–1.04) in the univariate analysis. After adjustment for perioperative MI, troponin I was not independently associated with a higher risk of death. In contrast, the 30-day and long-term mortality rates were significantly increased in the perioperative MI group compared with those patients with MINS but no MI. The diagnosis of perioperative MI in the present study was based on the UDMI guideline, which highlights the prognostic significance of troponin elevation in association with evidence of myocardial ischemia. Our study emphasizes the need for active surveillance of clinical symptoms and perioperative monitoring of cardiac troponin together with ECG changes in at-risk patients to detect perioperative MI early.
Although MINS is strongly linked with mortality, the etiology and pathophysiology mechanism of MINS is incompletely understood, and it remains unclear whether thrombosis or an oxygen supply-demand mismatch dominates [23]. Perioperative MIs after noncardiac surgery are dominantly caused by a supply-demand imbalance (type 2 MI) [23,24]. The OPTIMUS study investigated the ischemia mechanism in 30 patients who had NSTEMI after noncardiac surgery and 30 matched patients who had a nonoperative NSTEMI. Thrombus was the culprit lesion in 13% of the perioperative myocardial infarctions and in 67% of the nonoperative myocardial infarctions (
This study has some limitations. First, regarding the definition of MINS, large epidemiological studies have established the diagnostic criteria of a non-high-sensitivity troponin T [2] and hs-TnT cut-off threshold [8,18,19], while no study has established optimal troponin I thresholds for MINS [18,19]. Our criteria for MINS is supported by the Fourth UDMI, but still require approval by expert groups [6]. Second, this was a single-center retrospective study; therefore, there are limitations inherent to the retrospective design and methodology, and the results may not be generalizable to populations of other countries. Third, perioperative troponin measurements are not included in the routine clinical practice of our institution. Therefore, not all patients had troponin measurements, which could lead to selection bias. Because the majority of MINS occur without any ischemic symptoms and would go unrecognized without troponin monitoring [8,19], the true incidence of MINS might be underestimated.
Conclusions
MINS and perioperative MI are common in older adult patients undergoing orthopedic surgery in China. Perioperative MI is an independent predictor of short-term and long-term mortality. Our data can raise clinician awareness of the current situation of MINS in the Chinese population so that patients can be recognized, evaluated, and treated earlier. It also may be helpful in improving the prognosis of older adult patients following orthopedic surgery.
Figures
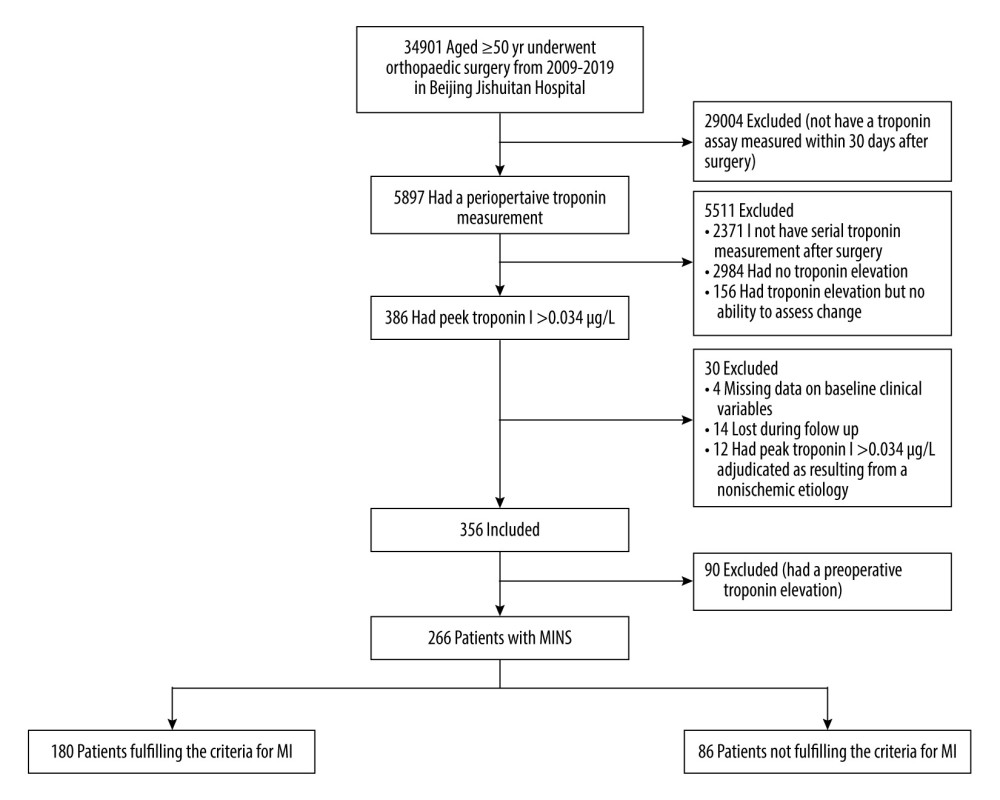 Figure 1. Study flow chart. The diagram shows the numbers of patients screened and the final study population. MI – myocardial infarction.
Figure 1. Study flow chart. The diagram shows the numbers of patients screened and the final study population. MI – myocardial infarction. 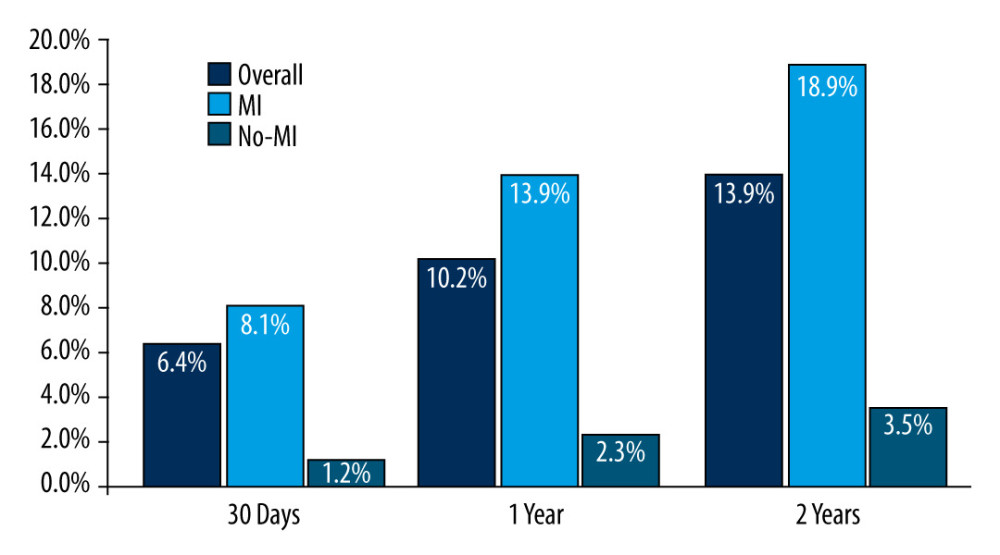 Figure 2. Mortality (%) at different time intervals derived from Kaplan-Meier analysis.
Figure 2. Mortality (%) at different time intervals derived from Kaplan-Meier analysis. 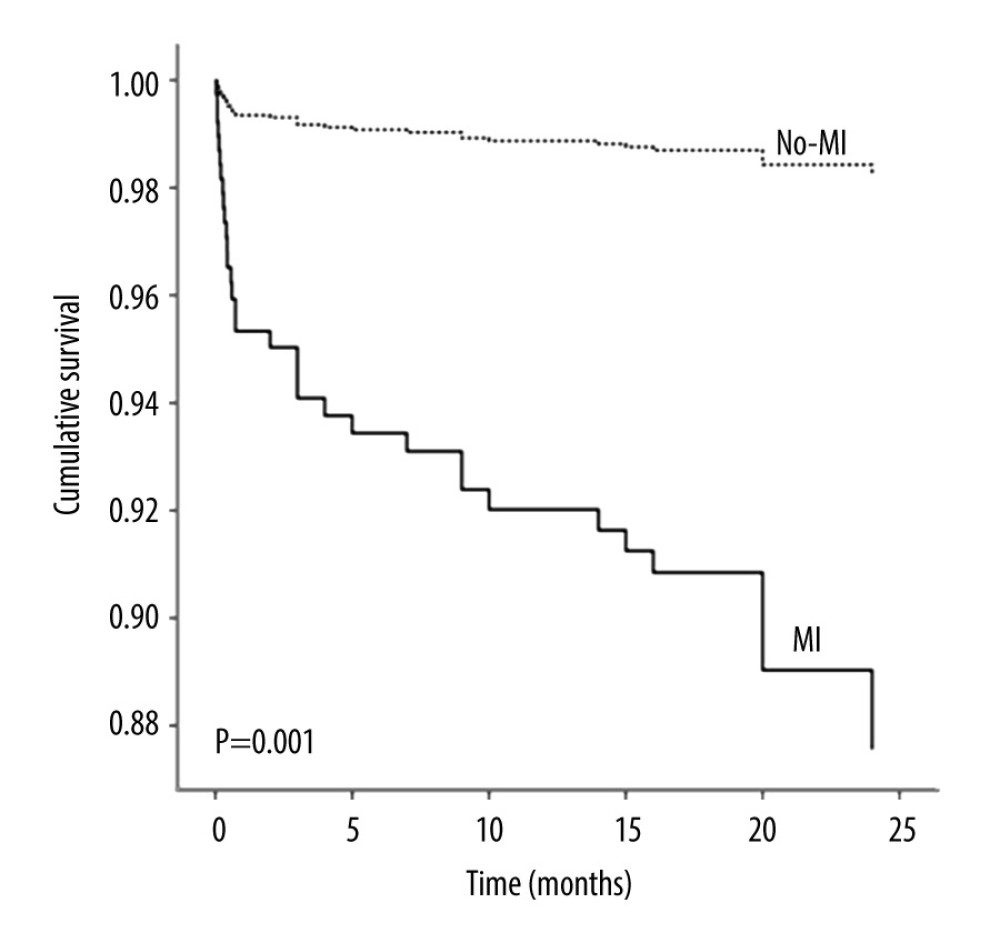 Figure 3. Kaplan-Meier survival curves illustrating risk of long-term death from any cause, shown for patients myocardial infarction and with no myocardial infarction.
Figure 3. Kaplan-Meier survival curves illustrating risk of long-term death from any cause, shown for patients myocardial infarction and with no myocardial infarction. Tables
Table 1. Baseline characteristics of patients with myocardial injury after noncardiac orthopedic surgery.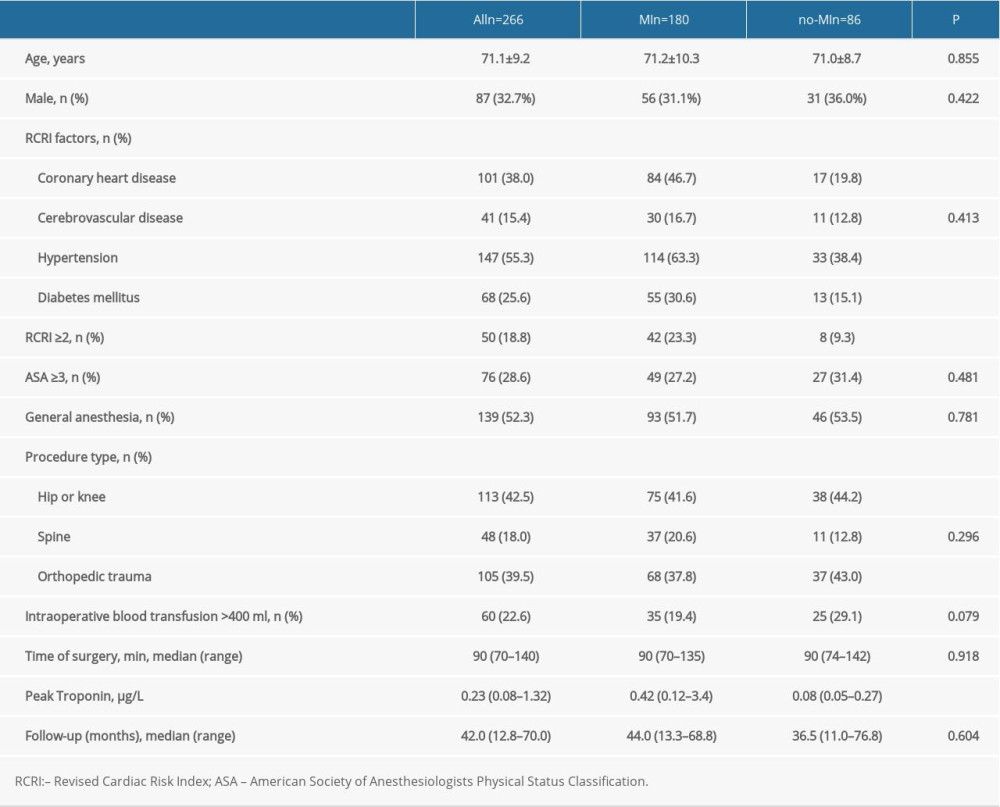 Table 2. Univariable and multivariable associated factors of 30-day mortality.
Table 2. Univariable and multivariable associated factors of 30-day mortality.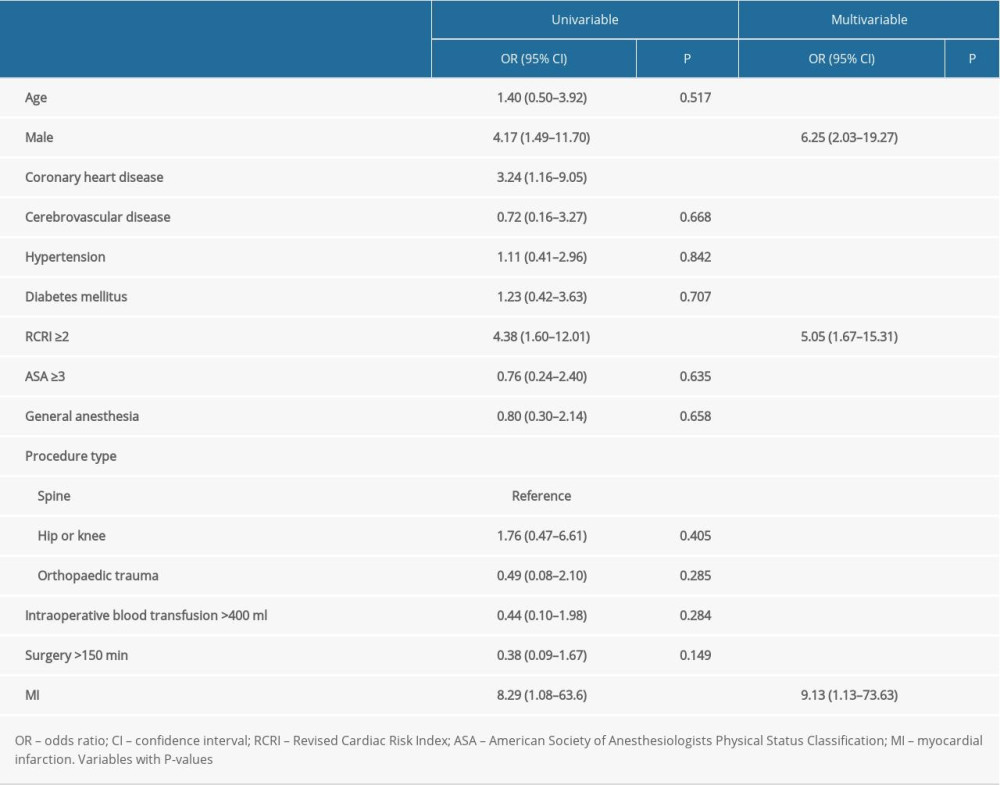 Table 3. Univariable and multivariable Cox proportional hazards model for long-term mortality.
Table 3. Univariable and multivariable Cox proportional hazards model for long-term mortality.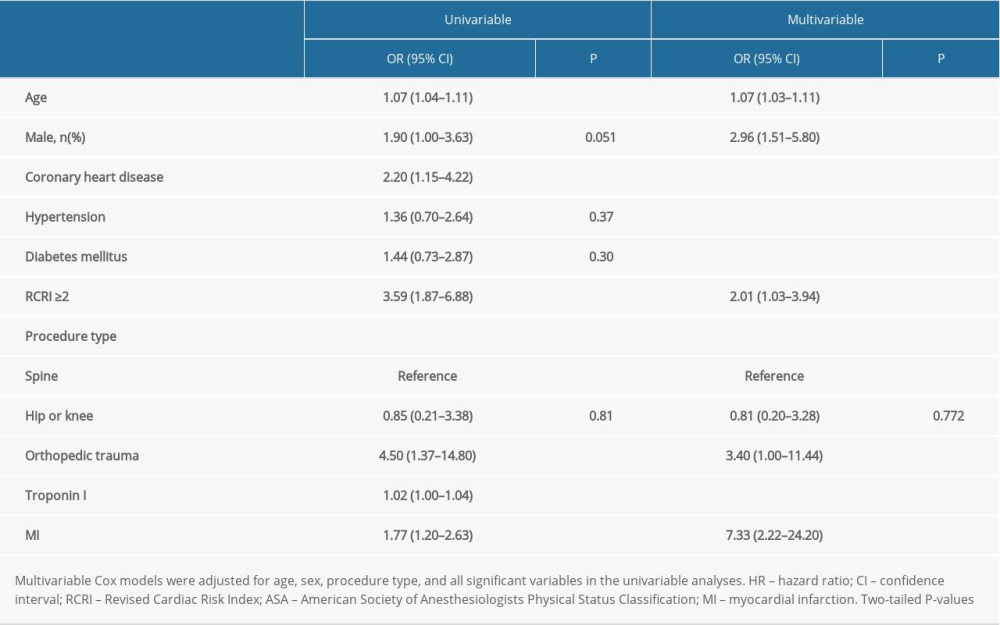 . STROBE Statement – checklist of items that should be included in reports of observational studies.
. STROBE Statement – checklist of items that should be included in reports of observational studies.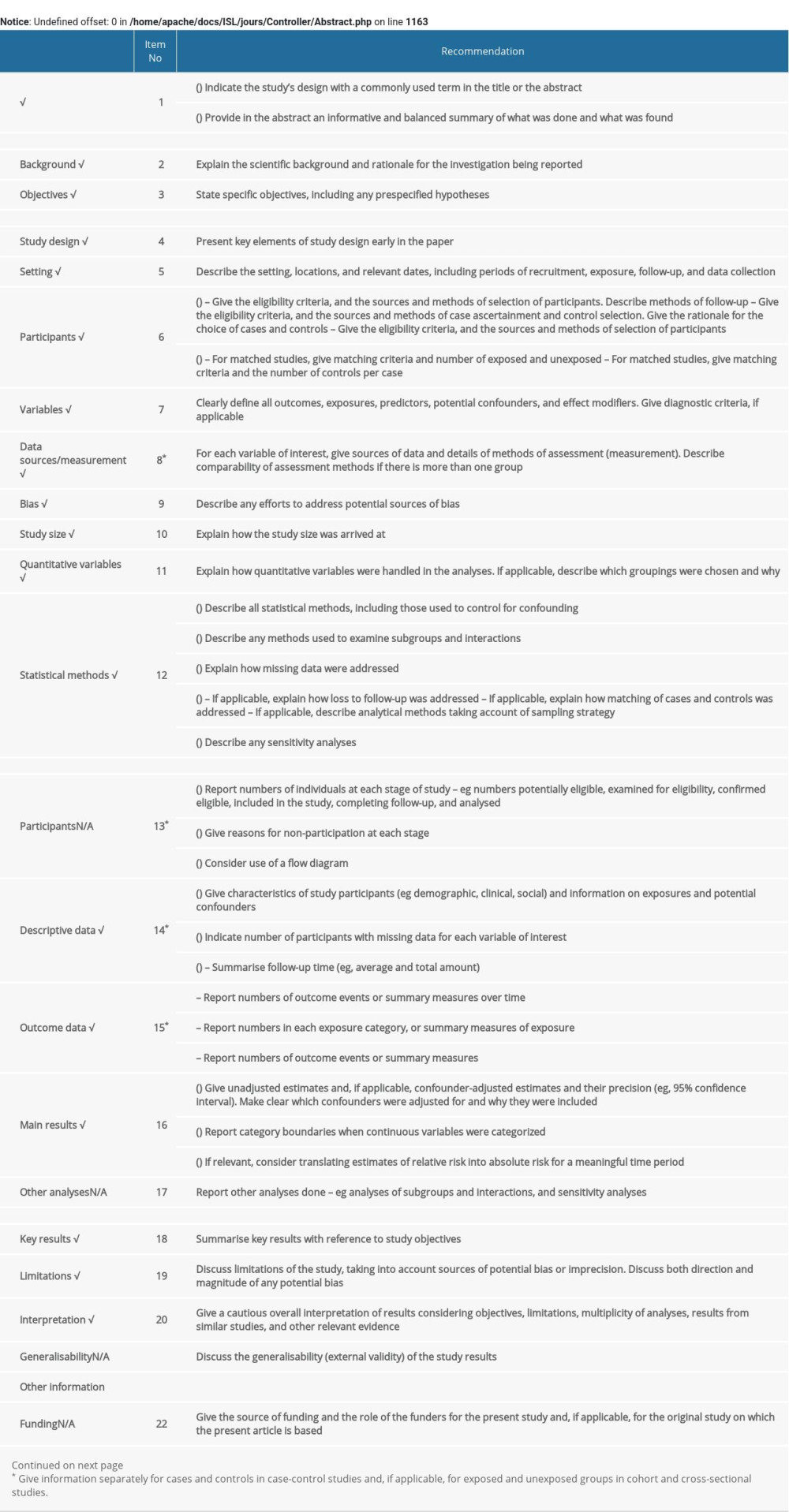
References
1. Weiser TG, Regenbogen SE, Thompson KD, An estimation of the global volume of surgery: A modelling strategy based on available data: Lancet, 2008; 372; 139-44
2. Botto F, Alonso-Coello P, Chan MT, Myocardial injury after noncardiac surgery: A large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes: Anesthesiology, 2014; 120; 564-78
3. Horr S, Reed G, Menon V, Troponin elevation after noncardiac surgery: Significance and management: Cleve Clin J Med, 2015; 82; 595-602
4. Puelacher C, Lurati Buse G, Seeberger D, Perioperative myocardial injury after noncardiac surgery: Incidence, mortality, and characterization: Circulation, 2018; 137; 1221-32
5. van Waes JA, Nathoe HM, de Graaff JC, Myocardial injury after noncardiac surgery and its association with short-term mortality: Circulation, 2013; 127; 2264-71
6. Thygesen K, Alpert JS, Jaffe AS, Fourth Universal Definition of Myocardial Infarction (2018): Circulation, 2018; 138; e618-e51
7. Devereaux PJ, Chan MTVascular Events In Noncardiac Surgery Patients Cohort Evaluation (VISION) Study Investigators, Association between postoperative troponin levels and 30-day mortality among patients undergoing noncardiac surgery: JAMA, 2012; 307; 2295-304
8. Devereaux PJ, Biccard BMWriting Committee for the VSI, Association of postoperative high-sensitivity troponin levels with myocardial injury and 30-day mortality among patients undergoing noncardiac surgery: JAMA, 2017; 317; 1642-51
9. Menendez ME, Memtsoudis SG, Opperer M, A nationwide analysis of risk factors for in-hospital myocardial infarction after total joint arthroplasty: Int Orthop, 2015; 39; 777-86
10. Dodd AC, Lakomkin N, Sathiyakumar V, Do orthopaedic trauma patients develop higher rates of cardiac complications? An analysis of 56,000 patients: Eur J Trauma Emerg Surg, 2017; 43; 329-36
11. Urban MK, Wolfe SW, Sanghavi NM, The incidence of perioperative cardiac events after orthopedic surgery: A single institutional experience of cases performed over one year: HSS J, 2017; 13; 248-54
12. Belmont PJ, Goodman GP, Kusnezov NA, Postoperative myocardial infarction and cardiac arrest following primary total knee and hip arthroplasty: Rates, risk factors, and time of occurrence: J Bone Joint Surg Am, 2014; 96; 2025-31
13. Oberweis BS, Smilowitz NR, Nukala S, Relation of perioperative elevation of troponin to long-term mortality after orthopedic surgery: Am J Cardiol, 2015; 115; 1643-48
14. Huddleston JM, Gullerud RE, Smither F, Myocardial infarction after hip fracture repair: A population-based study: J Am Geriatr Soc, 2012; 60; 2020-26
15. Smilowitz NR, Gupta N, Ramakrishna H, Perioperative major adverse cardiovascular and cerebrovascular events associated with noncardiac surgery: JAMA Cardiol, 2017; 2; 181-87
16. Kristensen SD, Knuuti J, New ESC/ESA Guidelines on noncardiac surgery: Cardiovascular assessment and management: Eur Heart J, 2014; 35; 2344-45
17. Lee TH, Marcantonio ER, Mangione CM, Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery: Circulation, 1999; 100; 1043-49
18. Devereaux PJ, Szczeklik W, Myocardial injury after noncardiac surgery: Diagnosis and management: Eur Heart J, 2020; 41; 3083-91
19. Puelacher C, Bollen Pinto B, Mills NL, Expert consensus on peri-operative myocardial injury screening in noncardiac surgery: A literature review: Eur J Anaesthesiol, 2021; 38; 600-8
20. Thomas S, Borges F, Bhandari M, Association between myocardial injury and cardiovascular outcomes of orthopaedic surgery: A vascular events in noncardiac surgery patients cohort evaluation (VISION) substudy: JBJS, 2020; 102; 880-88
21. Devereaux PJ, Xavier D, Pogue J, Characteristics and short-term prognosis of perioperative myocardial infarction in patients undergoing noncardiac surgery: A cohort study: Ann Intern Med, 2011; 154; 523-28
22. Vallet H, Breining A, Le Manach Y, Isolated cardiac troponin rise does not modify the prognosis in elderly patients with hip fracture: Medicine (Baltimore), 2017; 96; e6169
23. Helwani MA, Amin A, Lavigne P, Etiology of acute coronary syndrome after noncardiac surgery: Anesthesiology, 2018; 128; 1084-91
24. Sheth T, Natarajan MK, Hsieh V, Incidence of thrombosis in perioperative and nonoperative myocardial infarction: Br J Anaesth, 2018; 120; 725-33
25. Duvall WL, Sealove B, Pungoti C, Angiographic investigation of the pathophysiology of perioperative myocardial infarction: Catheter Cardiovasc Interv, 2012; 80; 768-76
26. Gualandro DM, Campos CA, Calderaro D, Coronary plaque rupture in patients with myocardial infarction after noncardiac surgery: Frequent and dangerous: Atherosclerosis, 2012; 222; 191-95
Figures
Figure 1. Study flow chart. The diagram shows the numbers of patients screened and the final study population. MI – myocardial infarction.Figure 2. Mortality (%) at different time intervals derived from Kaplan-Meier analysis.Figure 3. Kaplan-Meier survival curves illustrating risk of long-term death from any cause, shown for patients myocardial infarction and with no myocardial infarction. Tables
Table 1. Baseline characteristics of patients with myocardial injury after noncardiac orthopedic surgery.Table 2. Univariable and multivariable associated factors of 30-day mortality.Table 3. Univariable and multivariable Cox proportional hazards model for long-term mortality.Table 1. Baseline characteristics of patients with myocardial injury after noncardiac orthopedic surgery.Table 2. Univariable and multivariable associated factors of 30-day mortality.Table 3. Univariable and multivariable Cox proportional hazards model for long-term mortality.. STROBE Statement – checklist of items that should be included in reports of observational studies. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387