21 January 2022: Clinical Research
A Resting-State Functional Magnetic Resonance Imaging Study of Abnormal Frontoparietal Network Function in Migraine without Aura
Wen-Qiang Cui1ABCDEF, Si-Shuo Zhang12BE, Fei Xu3BCE, Hai-Tao Li1BE, Hong-Wei Zhi1BE, Ya-Han Wang1CE, Yong-Jun Huo4CE, Xiang-Qing Xu1AEFG*, Hong-Yun Wu1ACEGDOI: 10.12659/MSM.934975
Med Sci Monit 2022; 28:e934975






Abstract
BACKGROUND: This study aimed to investigate frontoparietal network (FPN) dysfunction in participants with migraine without aura (MwoA).
MATERIAL AND METHODS: We selected 48 age-, sex-, and education level-matched graduate students (24 participants with MwoA [MwoA group] and 24 healthy controls). RS-fMRI and independent component analysis were used to examine the FPN and to compare abnormal encephalic regional homogeneity values. The Mindful Attention Awareness Scale (MAAS), Self-Rating Anxiety Scale (SAS), Self-Rating Depression Scale (SDS), and Self-Rating Scale of Sleep (SRSS) were used to evaluate attention, anxiety, depression, and sleep, respectively. Pearson’s correlation was applied to evaluate the association between abnormal brain areas and the scores for each scale.
RESULTS: Neural function activity in encephalic regions of FPN showed abnormal changes in the MwoA group. The MwoA group had significantly lower MAAS scores (P<0.001), higher SAS scores (P<0.001), and higher SDS (P=0.06) and SRSS scores (P=0.26). In the MwoA group, functional activity of the right parietal lobule in the left FPN was positively correlated with MAAS scores (P=0.01) and negatively correlated with SAS (P=0.02). The orbital part of left inferior frontal gyrus activity in the right FPN was positively correlated with SDS (P=0.04) and SRSS (P<0.001). Right superior marginal gyrus activity in the right FPN was positively correlated with SDS (P=0.02).
CONCLUSIONS: Abnormal FPN function was correlated with attention, anxiety, depression, and sleep status in the MwoA group. These results offer further insights into the evaluation and treatment of MwoA.
Keywords: Brain Injuries, Magnetic Resonance Imaging, migraine without aura, Neuronal Plasticity, Polymicrogyria, Bilateral Frontoparietal, Adult, Brain Mapping, Female, Humans, Male, young adult
Background
Migraine is the most common form of disabling primary headache globally [1]. The onset of migraine usually manifests as a unilateral throbbing headache, accompanied with nausea, hypersensitivity, and significant fatigue. Approximately 2.5% of patients with episodic migraine have been reported to progress to chronic migraine (CM) each year [1], with CM reportingly affecting 1–2% of the global population [1]. CM, including migraine with aura (MA) and migraine without aura (MwoA), often triggers medical comorbidities such as anxiety, depression, and sleep disorders [2,3]. CM severely reduces the quality of life in those affected and imposes a significant financial burden on patients.
As a non-invasive technique, resting-state functional magnetic resonance imaging (RS-fMRI) reflects in vivo changes in brain function, which can be scanned repeatedly. RS-fMRI has been widely used to study the pathophysiological mechanisms of migraine and to identify imaging markers of migraine [4]. With advanced imaging techniques, migraine has been shown to be associated with not only abnormalities of the pain-brain network but also abnormalities of other related brain networks, such as the sensorimotor, visual processing, executive control, dorsal attention, and auditory networks [5].
The frontoparietal network (FPN), divided into the left FPN (lFPN) and right FPN (rFPN), involves the temporoparietal junction and the sub-frontal region, which are essentially mirror-image distributions [6]. One study showed that the functional connectivity between the FPN and the rostral anterior cingulate cortex/medial prefrontal cortex was positively associated with cue effects on pain rating changes [7]. The results of that study indicated that the FPN played an important role in cognitive modulation of pain. However, it remains unclear whether FPN dysfunction occurs in MwoA. To further enhance understanding of the brain network mechanisms of MwoA, we analyzed FPN abnormalities in MwoA using RS-fMRI.
Attention deficits have been observed in many patients with migraine [8]. Furthermore, MwoA often triggers anxiety and depression [2], and participants with MwoA have a considerably higher prevalence of sleep disorders [3]. These comorbidities complicate the treatment of migraine and need to be considered when studying the mechanisms of MwoA. Therefore, we used related scales to evaluate the attention, anxiety, depression, and sleep status of participants with MwoA, and we analyzed the correlation between the scores of various scales and abnormalities of the FPN. These findings will provide useful starting points at which to determine the mechanisms and provide some targets for neuroregulatory therapy of MwoA.
Material and Methods
STUDY POPULATION AND PROTOCOL:
The trial was registered in the CTR platform (ChiCTR2100051770). With reference to International Classification of Headache Diseases, 3rd Edition (Code 1.1, 2013) [9] diagnostic criteria for MwoA, we recruited participants with MwoA between January and June 2021. All participants were assessed by Professors Wu and Xu, who are neurologists specializing in the diagnosis and treatment of migraine. The study population comprised volunteer graduate students aged from 25 to 30 years who had been diagnosed with MwoA (the MwoA group) or those who were healthy (healthy controls [HCs]). All participants were right-handed. Enrolled participants with MwoA had a disease duration of >6 months and had experienced migraine attacks within the last month. Some participants were permitted to take analgesic medication for migraine prevention or treatment, as recommended by physicians and when necessary (Visual Analog Scale [VAS], >7); however, they were not permitted to take any medication for at least 3 days prior to the MRI examination. Similar to our previous study [10], we included HCs (i) who had not experienced from headache attacks in the past year; (ii) who had neither been ill nor had taken any medication for 1 month; and (iii) whose family members had no history of migraine or other headaches. Study participants were requested not to consume alcohol or caffeine or take nicotine or other chemically similar substances for at least 3 months prior to the MRI examination.
Participants who took opioid analgesics, antipsychotics or ergotamine, and participants with alcoholism or other drug abuse issues were excluded. Patients with chronic systemic diseases and illnesses that might confound data interpretation (eg, heart, brain, liver, kidney, and hematopoietic system primary diseases; mental diseases; pregnancy; and lactation) were also excluded. None of the participants had contraindications for fMRI. Informed consent was provided by all study participants. The study was approved by the Ethics Committee of the Affiliated Hospital of Shandong University of Traditional Chinese Medicine (approval number: 2014-028).
After screening, we recruited 24 individuals with MwoA and 24 HCs for this study. An RS-fMRI scan was performed during the interictal stage in the MwoA group, at least 3 days after a migraine attack. The RS-fMRI was performed for 1 healthy participant on the same day. Independent component analysis (ICA), a data-driven analysis method that breaks a signal down into multiple independent components without the need for prior model assumptions, was applied to analyze the RS-fMRI results. The FPN dysfunction in participants with MwoA was investigated using regional homogeneity (ReHo), which is an analysis method based on region of interest (ROI).
THE VAS SCORE: The VAS score is designed as a 10-cm scale with pain descriptors marking “no pain” (scored as 0) on the left and “the worst pain imaginable” (scored as 10) on the right. This score is used to assess patients’ pain intensity. VAS-based assessments are a valid and reliable method for patients with migraines [11]. At each assessment, subjects’ perceived level of pain for the most recent attack was recorded by marking the VAS with a perpendicular line.
THE MINDFUL ATTENTION AWARENESS SCALE (MAAS) SCORE: The MAAS, a 15-item single-dimension questionnaire, has good internal consistency and high test-retest reliability [12]. It is designed to assess a core characteristic of mindfulness, namely, attention. Items include statements such as “I rush through activities without being really attentive to them” and “I find myself doing things without paying attention.” During a session prior to the MRI scanning date, participants were asked to indicate how frequently or infrequently such experiences occurred. The response options were recorded on a 6-point Likert scale: 1, almost always; 2, very frequently; 3, somewhat frequently; 4, somewhat infrequently; 5, very infrequently; and 6, almost never. Higher scores indicated high trait mindfulness.
THE SELF-RATING ANXIETY SCALE (SAS) SCORE: The SAS was used to measure participants’ affective and somatic symptoms of current anxiety [13]. The SAS consists of 20 items, and its ratings cover the week prior to the evaluation. Each item is rated for severity, duration, and frequency of each symptom. A 4-point Likert scale is used, ranging from 1 (none or insignificant) to 4 (severe). The sum of the 20 items produces a score ranging between 20 and 80, with a cut-off value of ≥40 suggesting the presence of a clinically relevant anxiety disorder [13].
THE SELF-RATING DEPRESSION SCALE (SDS) SCORE: The SDS was used to assess participants’ current symptoms of depression [14]. The structure and calculation method of the SDS is similar to that of the SAS. Participants were asked to rate each item according to how they felt during the preceding 7 days. The sum of the 20 items produces a score ranging between 20 and 80, with a value ≥40 suggesting clinically relevant depression [14].
THE SELF-RATING SCALE OF SLEEP (SRSS) SCORE: The SRSS has been applied to a wide range of screenings for sleep disorders in various populations [15]. It was used to assess the subjects’ sleep quality in our study. It consists of 10 items, and each item has a 5-point scale (range, 1–5). In our study, all participants were asked to rate each item according to their sleep state in the preceding 7 days prior to undergoing the MRI. The sum of the 10 items produces a score ranging between 10 (essentially no sleep problems) and 50 (severe sleep disturbance). The higher the score, the more serious the sleep disturbance. A cut-off value ≥23 indicates sleep disturbance [15].
RS-FMRI: In our study, the Philips Achieva 3.0T MRI scanner and 12-channel matrix head coil were used to collect the RS-fMRI data dependent on the blood oxygen level. According to our previous study [10], during the MRI scan, subjects should remain stationary, close their eyes, and to continue breathing evenly. Structural MRI images were obtained by using a high-resolution, T1-weighted, three-dimensional (3D) magnetization-prepared acquisition gradient-echo pulse sequence [10]. The parameters were the same as in previous studies: 1) the repetition time (TR) and echo time (TE) are 8.0 ms and 3.8 ms, respectively; 2) the size of thickness and gap is 1 mm and 0 mm, respectively; 3) the flip angle is about 12°; 4) the matrix is set to 512×512; and 5) the field of view (FOV) is 250×250 mm [10]. The procedure for the structural sequence took approximately 5 min 30 s. A GRE-EPI sequence was applied to perform functional imaging. The parameters for scanning were as follows: 1) the TR and TE are 3000 ms and 35 ms, respectively; 2) the size of thickness and gap is 5 mm and 0 mm, respectively; 3) the flip angle is 90°; 4) the matrix is set to 128×128; and 5) the FOV is 230×230 mm [10]. Functional imaging was captured continuously for 10 min. The scanning range included the supratentorial brain, the cerebellum, and the brain stem.
DATA PREPROCESSING: This process was the same as in our previous study [10]. Firstly, we transformed the format of MRI scan data from Digital Imaging and Communications in Medicine (DICOM) to Neuroimaging Informatics Technology Initiative (Nifti). Secondly; noise, error, and other factors that have some influence on the results of ICA were eliminated. DPABI v4.3 software was applied to preprocess the RS-fMRI data relying on the MATLAB 2017a platform [16]. The steps are as follows: 1) the first 10 time points of data were removed, 2) the time layer, head movements, spatial standardization, and smoothing space were corrected, and 3) linear drift and filtering were removed. For spatial smoothing, signals ranging from 0.01 to 0.08 Hz were selected and a Gaussian kernel function of 4×4×4 mm3 with half height and full width was applied.
DETERMINATION OF FPN FUNCTION: ICA was performed on the preprocessed RS-fMRI data of 2 groups by using the GIFT software V3.0b (Group ICA/IVA of fMRI Toolbox, https://trendscenter.org/software/), relying on the MATLAB 2017a platform [10]. The number of components was set at 20, and the number of independent components was obtained by using a GIG-ICA algorithm. The calculation was repeated 50 times using Rand Init and bootstrap methods [17]. Based on Smith et al’s resting-state brain network (rs-BN) template, which was created using a large number of healthy individuals [18], we selected the FPN related to MwoA to guide the generation of resting-state FPN in new participants in this study. Similar to the previous study [10], the selected resting-state FPN and preprocessed fMRI data were input into the GIG-ICA algorithm simultaneously to produce the 3D spatial components of the participants and the corresponding 1D time series. In the above process, no threshold was set. Therefore, the rs-BN of all participants was retained. Three resting-state visual networks were selected, as demonstrated in Figure 1. The inter-group t test was conducted for the FPN of the 2 groups by using the REST v1.8 (Resting-State fMRI Data Analysis Toolkit) relying on the MATLAB 2017a platform [19]. P values <0.01 were used as the threshold of significance. Alphasim correction was performed by setting a voxel threshold of 256 and a connection rule of RMM=4. The differential brain regions in the FPN of the 2 groups were obtained using this connection.
REHO ANALYSES: We preprocessed the MRI data and then analyzed the ReHo using DPABI v4.3 software. Kendall’s coefficient of concordance was calculated for the time sequence of a given voxel concerning its 26 nearest neighbors [20], and then an individual ReHo map was generated. To mitigate the effects of individual diversification, the ReHo value of each voxel was converted into a z-score by subtracting and dividing the standard deviation of the whole-brain ReHo map [10]. The brain regions where ReHo obviously changed were defined as the center of the sphere, and the formed sphere region (6 mm in radius) was set as the ROI. According to the sequence, ROIs were recorded as ROI1, ROI2, ROI3, ROI4, ROIn, etc.
STATISTICAL ANALYSIS:
GraphPad Prism 6 (GraphPad Software, Inc., San Diego, CA, USA) software was used for all statistical analyses. A
Results
PARTICIPANTS AND BASELINE CHARACTERISTICS:
After screening 96 individuals (42 HC volunteers and 54 individuals with MwoA), 24 participants with MwoA and 24 HCs were included in this study. There were no significant differences in sex, age, educational qualifications, and dominant hand between the 2 groups (P=1.00, 0.49, 1.00, and 1.00, respectively, Table 1). The 24 participants with MwoA had a disease duration of >6 months, an average attack frequency of >1 attack/month, and an average attack duration of ≥4 h (Table 1).
VAS OUTCOMES:
The VAS scores in the MwoA group were 6.06±1.47 (Table 1), with results indicating that these participants were experiencing pain.
MAAS, SAS, SDS, AND SRSS OUTCOMES:
The MAAS scores in the MwoA group (76.96±5.40) were significantly lower than those of the HCs (85.13±2.86; t test, P<0.0001; Figure 2A). The SAS scores in the MwoA group (44.21±9.87) were significantly higher than in the HCs (34.29±7.38; t test, P=0.0003; Figure 2B). However, the SDS scores (38.92±7.24) and SRSS scores (23.88±6.41) in the MwoA group increased compared with those of the HCs (35.21±6.27 and 21.42±8.38, respectively), but there was no significant difference between them (t test, P=0.06 and P=0.26, respectively; Figure 2C, 2D). These results indicated that participants with MwoA were significantly less attentive than the HCs and that they had a clinically relevant anxiety disorder.
RS-FMRI RESULTS:
In the lFPN, MwoA group participants showed decreased functional activity in the brain regions of the right inferior semilunar lobule, the left fusiform gyrus, the orbital part of the right inferior frontal gyrus, the right parietal lobule, and the left supra-marginal gyrus, and they had enhanced functional activity in the left orbital middle frontal gyrus and the right middle frontal gyrus compared with the HCs (Figure 3). In the rFPN, the MwoA group had higher functional activity in the left inferior semilunar lobule, the right middle frontal gyrus, the orbital part of the left inferior frontal gyrus, the right parahippocampal gyrus, the right supraoccipital gyrus, and the right superior marginal gyrus compared with the HCs (Figure 4).
CORRELATION ANALYSIS RESULTS:
The results of a Pearson’s correlation analysis showed that the ReHo value of the right parietal lobule in the lFPN was positively correlated with the MAAS (r=0.39, P=0.01; Table 2), indicating that attention deficit disorder in patients may be related to decreased consistency in local neuronal activity in the right parietal lobule. There was a negative correlation between the ReHo value of the right parietal lobule in the lFPN and the SAS score (r=−0.37, P=0.02, Table 2), and the ReHo value of the orbital part of the left inferior frontal gyrus and the right superior marginal gyrus in the rFPN was positively correlated with the SDS score (r=0.32 and 0.37, P=0.04 and 0.02, respectively; Table 2). These results indicated that anxiety in participants with MwoA was related to decreased functional activity in the right parietal lobule in the lFPN. Moreover, the depression trend in participants with MwoA was related to increased functional activity of the orbital part of the left inferior frontal gyrus and the right superior marginal gyrus in the rFPN. The ReHo value of the orbital part of the left inferior frontal gyrus in the rFPN was positively correlated with the SRSS score (r=0.44, P<0.001; Table 2). This finding indicated that the decreased quality of sleep in MwoA participants might be related to the increased neuronal consistency in the orbital part of the left inferior frontal gyrus in the rFPN.
Discussion
In this study, we enrolled participants with MwoA whose sex, age, education levels, and dominant hand matched that of HCs. The FPN abnormalities were assessed using the RS-fMRI scans and ICA methods in the interictal phase of MwoA. Our RS-fMRI results demonstrated that functional activity in the left inferior semilunar lobule, the right middle frontal gyrus, the orbital part of the left inferior frontal gyrus, the right parahippocampal gyrus, the right supraoccipital gyrus, the right superior marginal gyrus of the rFPN, and the left orbital middle frontal gyrus and the right middle frontal gyrus of the lFPN was stronger in the MwoA group, whereas functional activity in the right inferior semilunar lobule, the left fusiform gyrus, the orbital part of the right inferior frontal gyrus, the right parietal lobule, and the left supra-marginal gyrus of the lFPN was weaker than that in the HC group. These results supported our hypothesis that participants with MwoA have FPN abnormalities.
One study reported that attention function had lateralization characteristics [21] and that selective impairment of attention function was observed in patients with MA with left aura [21]. Differences in rFPN and lFPN functions have also been reported. The rFPN has been found to be closely related to perception and pain, whereas the lFPN has been shown to be related to cognition and language [22]. Consistent with these findings, our results showed that the brain regions involving bilateral differences in FPN were almost mirror-image symmetrical. The functional activity of some brain regions of the lFPN were decreased, whereas the functional activity of some brain regions of the rFPN were enhanced. The increased functional activity of the rFPN related to perception and pain in participants with MwoA in the interictal stage suggested that they were prone to headache attacks when stimulated using external stimuli such as light and sound. This possibility was also supported through the high VAS scores in these participants. The decreased functional activity of the lFPN related to cognition and language indicated that participants with MwoA had potential risks for cognitive and language impairments.
Attention deficit, one of the clinical manifestations of aura, has been reported to occur in the prodrome hours or days before the onset of migraine in patients with MA [4]. Studies concerning migraine comorbid with attention deficit hyperactivity disorder (ADHD) have suggested that both adult and pediatric patients with migraine were more likely to show hyperactivity/impulsivity and inattention than those without migraine [23–25]. Selective attention is a core cognitive function in effective information processing, and is related to attention selection, working memory, and decision-making. FPN has been reported to be involved in the process of selective attention, which has also been confirmed in studies concerning Chinese tones [26,27]. In our study, the lower MAAS scores in the MwoA group indicated that they had poor attention function. The ReHo value of the right parietal lobule in the lFPN was positively correlated with the MAAS scores, indicating that the weakened consistency in local neuronal activity in the right parietal lobule is positively correlated with attention deficit in participants with MwoA. Our results further confirmed that the functional activity of the FPN was involved in the regulation of attentional selection function. Interestingly, although one of the mechanisms involved in attention difficulties in the MwoA group was found to be hypersensitivity to stimulus, the functional activity of the rFPN that related to perception and pain was not related to the MAAS scores.
The pathogenesis of migraine is closely related to serotonin, and serotonin levels in platelets are decreased during acute migraine attacks [28]. A decrease in serotonin is a key factor triggering the occurrence of anxiety and depression. Recurring migraine-induced anxiety and depression in patients with MoA and MwoA and negative emotion amplify patients’ pain [29,30]. These interrelated factors influence each other and seriously affect a patient’s work, life, and learning. In our study, we also found that participants in the MwoA group presented with clinically relevant anxiety disorders and depression-like tendencies, but without meeting the clinical depression criteria. These results are consistent with our clinical observation that many participants showed symptoms of anxiety, but only a small number developed depression.
Although MwoA and negative emotion have been found to be related, the mechanisms concerning these comorbidities remain unclear; therefore, treating such comorbidities remains challenging. Neuroimaging studies have shown that abnormal structural and functional connections in some brain regions could be associated with the structural basis of comorbidities related to migraine and negative emotions [31,32]. After patients with depressive disorders received the selective 5-HT and norepinephrine reuptake inhibitors (SNRIs) such as venlafaxine, the density of pain network connections in the thalamus-cortex-periaqueductal gray decreased, and this was positively associated with their pain scores [33–35], suggesting the presence of pain pathway abnormalities in depressive disorders. Our RS-fMRI and correlation analysis results indicated that anxiety disorders and the depression trend were related to the abnormal function of the FPN in MwoA. In addition, rFPN functional connectivity decreased in patients with primary insomnia, and functional connectivity between the right middle temporal gyrus and the right occipital cortex and the FPN was significantly positively correlated with the course of disease and self-rated anxiety, respectively [36]. In our study, an SRSS assessment scatter diagram showed no significant difference between participants in the MwoA and HC groups; however, there were large individual differences in participants with MwoA, and some participants’ sleep quality was very poor. In future studies, increasing the sample size is likely to help further verify whether patients have decreased sleep quality. Our study also found a correlation between the local consistency of neurons in the orbital part of the left inferior frontal gyrus in the rFPN and sleep quality in participants with MwoA. These findings provide useful starting points at which to determine comorbidity mechanisms and provide some targets for neuroregulatory therapy.
Interestingly, the functions of the cerebral cortex and deep nuclei can be modulated by neuromodulation technology with no adverse effects [37]. Many types of neuromodulation equipment have been used to treat MA in clinical practice [38]. This will also facilitate the clinical application of our research results. There were no significant differences in the demographic characteristics of the 2 groups. However, males and females were not studied separately and the number of males and females was unbalanced in each group, with fewer male than female participants (males, 11; females, 13), although the proportion of males and females was similar between the 2 groups. Whether this affected our results remains unclear. Meanwhile, 6 participants with MwoA took treatment measures in response to MwoA attacks in the month before MRI scanning, comprising 3 participants who took ibuprofen and 3 participants who took zolmitriptan. In addition, 3 subjects used precautions (including medicine and traditional Chinese medicine) in the 2 months preceding the MRI scans. Although they no longer took treatment 3 days before MRI scanning and stopped using preventive measures 1 month prior to the MRI, this might have had an impact on MRI results. These uncertainties need to be further addressed in a larger-sample study and more rigorously designed neuroimaging experiments.
Conclusions
This study showed that, in the interictal stage, MwoA participants had FPN abnormalities, including enhanced functional activity in the left inferior semilunar lobule, the right middle frontal gyrus, the orbital part of the left inferior frontal gyrus, the right parahippocampal gyrus, the right supraoccipital gyrus, the right superior marginal gyrus of the rFPN, and the left orbital middle frontal gyrus and the right middle frontal gyrus of the lFPN, as well as weakened functional activity in the right inferior semilunar lobule, the left fusiform gyrus, the orbital part of the right inferior frontal gyrus, the right parietal lobule, and the left supra-marginal gyrus of the lFPN. Weakened functional activity in the right parietal lobule in the lFPN was associated with decrease in attention and the anxiety disorders in participants with MwoA, whereas enhanced functional activity in the orbital part of the left inferior frontal gyrus and the right superior marginal gyrus in the rFPN was associated with the depression trend in these participants. Further, enhanced functional activity of the orbital part of the left inferior frontal gyrus in the rFPN was associated with decreased quality of sleep for participants with MwoA. These brain regions are potential targets for neuro-regulatory therapy in MwoA. Regulating the functional activity of these brain regions may improve the patients’ attention, emotion, and sleep. However, the role and neural mechanisms of FPN in MwoA need to be further explored in clinical and animal studies.
Figures
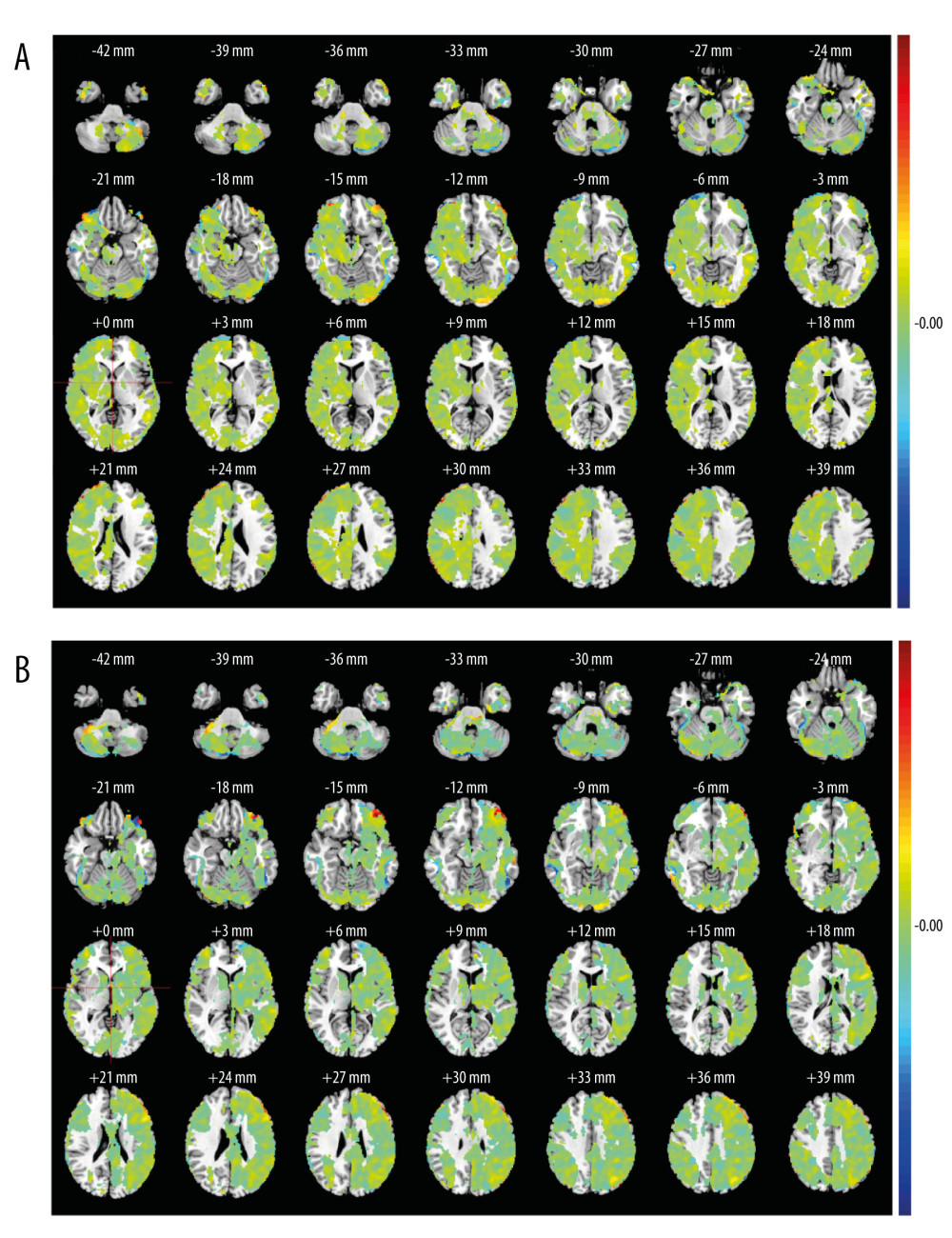 Figure 1. The selected resting-state frontoparietal network in this studyFPN included left FPN and right FPN. Left FPN (A) included the right inferior semilunar lobule, left fusiform gyrus, the orbital part of right inferior frontal gyrus, right parietal lobule, left supra-marginal gyrus, the left orbital middle frontal gyrus, right middle frontal gyrus, etc. Right FPN (B) included the left inferior semilunar lobule, right middle frontal gyrus, the orbital part of left inferior frontal gyrus, right parahippocampal gyrus, right supraoccipital gyrus, right superior marginal gyrus, etc. MATLAB R2017a (MathWorks, Inc., USA) was used to create this figure.
Figure 1. The selected resting-state frontoparietal network in this studyFPN included left FPN and right FPN. Left FPN (A) included the right inferior semilunar lobule, left fusiform gyrus, the orbital part of right inferior frontal gyrus, right parietal lobule, left supra-marginal gyrus, the left orbital middle frontal gyrus, right middle frontal gyrus, etc. Right FPN (B) included the left inferior semilunar lobule, right middle frontal gyrus, the orbital part of left inferior frontal gyrus, right parahippocampal gyrus, right supraoccipital gyrus, right superior marginal gyrus, etc. MATLAB R2017a (MathWorks, Inc., USA) was used to create this figure. 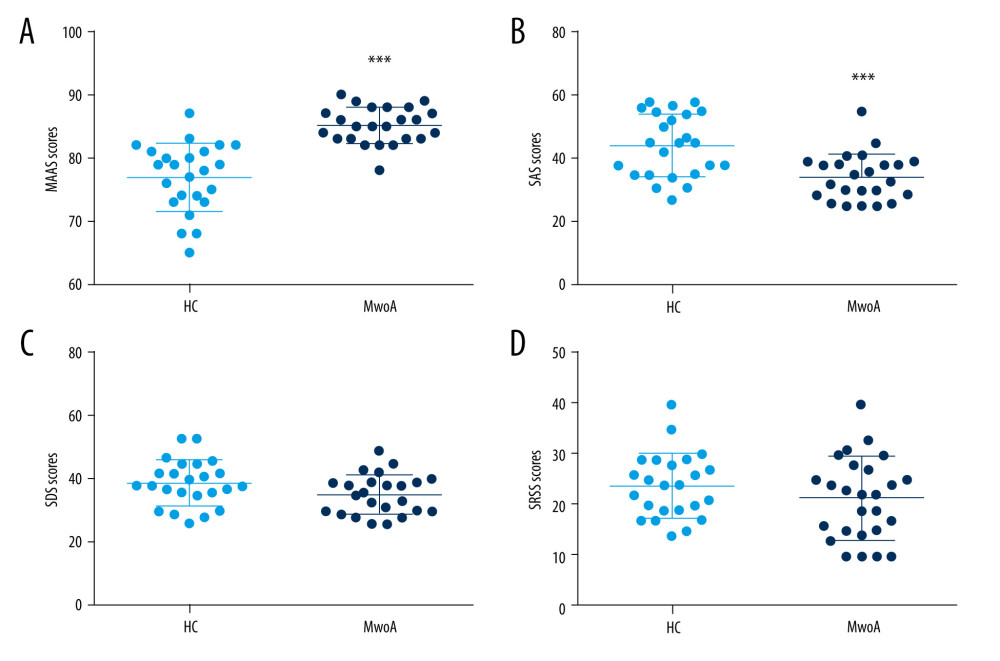 Figure 2. Comparison of MAAS, SAS, SDS and SRSS scores between the MwoA group and the HC groupThe scatter diagram of MAAS (A), SAS (B), SDS (C), and SRSS (D) scores in 2 groups. This figure was created using GraphPad Prism 6 (GraphPad Software, Inc., San Diego, CA, USA).
Figure 2. Comparison of MAAS, SAS, SDS and SRSS scores between the MwoA group and the HC groupThe scatter diagram of MAAS (A), SAS (B), SDS (C), and SRSS (D) scores in 2 groups. This figure was created using GraphPad Prism 6 (GraphPad Software, Inc., San Diego, CA, USA). ![Comparison of lFPN functional activity between the MwoA group and the HC groupThe functional activity peak of the right inferior semilunar lobule [Coordinates (38, −72, 46), T-value (−18.60), Voxel values (2283)], left fusiform gyrus [Coordinates (−54, −56, −10), T-value (−15.55), Voxel values (463)], the orbital part of right inferior frontal gyrus [Coordinates (48, 44, −14), T-value (−14.86), Voxel values (302)], right parietal lobule [Coordinates (36, −68, 52), T-value (−14.70), Voxel values (377)] and left supra-marginal gyrus [Coordinates (−48, −62, 46), T-value (−14.47), Voxel values (733)] were weaker in the MwoA group. The functional activity peak of the left orbital middle frontal gyrus [Coordinates (−38, 42, −14), T-value (18.30), Voxel values (2469)] and right middle frontal gyrus [Coordinates (54, 34, 22), T-value (9.06), Voxel values (291)] were higher in the MwoA group. The warmer colors represent a stronger functional activity, while the cold colors represent a weakened functional activity. MATLAB R2017a (MathWorks, Inc., USA) was used to create this figure.](https://jours.isi-science.com/imageXml.php?i=medscimonit-28-e934975-g003.jpg&idArt=934975&w=1000) Figure 3. Comparison of lFPN functional activity between the MwoA group and the HC groupThe functional activity peak of the right inferior semilunar lobule [Coordinates (38, −72, 46), T-value (−18.60), Voxel values (2283)], left fusiform gyrus [Coordinates (−54, −56, −10), T-value (−15.55), Voxel values (463)], the orbital part of right inferior frontal gyrus [Coordinates (48, 44, −14), T-value (−14.86), Voxel values (302)], right parietal lobule [Coordinates (36, −68, 52), T-value (−14.70), Voxel values (377)] and left supra-marginal gyrus [Coordinates (−48, −62, 46), T-value (−14.47), Voxel values (733)] were weaker in the MwoA group. The functional activity peak of the left orbital middle frontal gyrus [Coordinates (−38, 42, −14), T-value (18.30), Voxel values (2469)] and right middle frontal gyrus [Coordinates (54, 34, 22), T-value (9.06), Voxel values (291)] were higher in the MwoA group. The warmer colors represent a stronger functional activity, while the cold colors represent a weakened functional activity. MATLAB R2017a (MathWorks, Inc., USA) was used to create this figure.
Figure 3. Comparison of lFPN functional activity between the MwoA group and the HC groupThe functional activity peak of the right inferior semilunar lobule [Coordinates (38, −72, 46), T-value (−18.60), Voxel values (2283)], left fusiform gyrus [Coordinates (−54, −56, −10), T-value (−15.55), Voxel values (463)], the orbital part of right inferior frontal gyrus [Coordinates (48, 44, −14), T-value (−14.86), Voxel values (302)], right parietal lobule [Coordinates (36, −68, 52), T-value (−14.70), Voxel values (377)] and left supra-marginal gyrus [Coordinates (−48, −62, 46), T-value (−14.47), Voxel values (733)] were weaker in the MwoA group. The functional activity peak of the left orbital middle frontal gyrus [Coordinates (−38, 42, −14), T-value (18.30), Voxel values (2469)] and right middle frontal gyrus [Coordinates (54, 34, 22), T-value (9.06), Voxel values (291)] were higher in the MwoA group. The warmer colors represent a stronger functional activity, while the cold colors represent a weakened functional activity. MATLAB R2017a (MathWorks, Inc., USA) was used to create this figure. ![The comparison of rFPN functional activity between the MwoA group and the HC groupThe functional activity peak of the left inferior semilunar lobule [Coordinates (−38, −74, −48), T-value (18.71), Voxel values (4383)], right middle frontal gyrus [Coordinates (44, 36, 34), T-value (21.64), Voxel values (3364)], the orbital part of left inferior frontal gyrus [Coordinates (−44, 50, −12), T-value (14.83), Voxel values (664)], right parahippocampal gyrus [Coordinates (18, −26, −14), T-value (5.04), Voxel values (427)], right supraoccipital gyrus [Coordinates (24, −74, 20), T-value (4.56), Voxel values (277)] and right superior marginal gyrus [Coordinates (60, −52, 38), T-value (23.11), Voxel values (2184)] were stronger in the MwoA group. The warmer colors represent a stronger functional activity. MATLAB R2017a (MathWorks, Inc., USA) was used to create this figure.](https://jours.isi-science.com/imageXml.php?i=medscimonit-28-e934975-g004.jpg&idArt=934975&w=1000) Figure 4. The comparison of rFPN functional activity between the MwoA group and the HC groupThe functional activity peak of the left inferior semilunar lobule [Coordinates (−38, −74, −48), T-value (18.71), Voxel values (4383)], right middle frontal gyrus [Coordinates (44, 36, 34), T-value (21.64), Voxel values (3364)], the orbital part of left inferior frontal gyrus [Coordinates (−44, 50, −12), T-value (14.83), Voxel values (664)], right parahippocampal gyrus [Coordinates (18, −26, −14), T-value (5.04), Voxel values (427)], right supraoccipital gyrus [Coordinates (24, −74, 20), T-value (4.56), Voxel values (277)] and right superior marginal gyrus [Coordinates (60, −52, 38), T-value (23.11), Voxel values (2184)] were stronger in the MwoA group. The warmer colors represent a stronger functional activity. MATLAB R2017a (MathWorks, Inc., USA) was used to create this figure.
Figure 4. The comparison of rFPN functional activity between the MwoA group and the HC groupThe functional activity peak of the left inferior semilunar lobule [Coordinates (−38, −74, −48), T-value (18.71), Voxel values (4383)], right middle frontal gyrus [Coordinates (44, 36, 34), T-value (21.64), Voxel values (3364)], the orbital part of left inferior frontal gyrus [Coordinates (−44, 50, −12), T-value (14.83), Voxel values (664)], right parahippocampal gyrus [Coordinates (18, −26, −14), T-value (5.04), Voxel values (427)], right supraoccipital gyrus [Coordinates (24, −74, 20), T-value (4.56), Voxel values (277)] and right superior marginal gyrus [Coordinates (60, −52, 38), T-value (23.11), Voxel values (2184)] were stronger in the MwoA group. The warmer colors represent a stronger functional activity. MATLAB R2017a (MathWorks, Inc., USA) was used to create this figure. References
1. Burch RC, Buse DC, Lipton RB, Migraine: Epidemiology, burden, and comorbidity: Neurol Clin, 2019; 37(4); 631-49
2. Blumenfeld AM, Tepper SJ, Robbins LD, Effects of onabotulinumtoxinA treatment for chronic migraine on common comorbidities including depression and anxiety: J Neurol Neurosurg Psychiatry, 2019; 90(3); 353-60
3. Rains JC, Sleep and migraine: Assessment and treatment of comorbid sleep disorders: Headache, 2018; 58(7); 1074-91
4. Goadsby PJ, Holland PR, An update: Pathophysiology of migraine: Neurol Clin, 2019; 37(4); 651-71
5. Chwedt TJ, Chong CD, Functional imaging and migraine: New connections?: Curr Opin Neurol, 2015; 28(3); 265-70
6. Brunetti M, Della PS, Ferretti A, A frontoparietal network for spatial attention reorienting in the auditory domain: A human fMRI/MEG study of functional and temporal dynamics: CEREB Cortex, 2008; 18(5); 1139-47
7. Kong J, Jensen K, Loiotile R, Functional connectivity of the frontoparietal network predicts cognitive modulation of pain: Pain, 2013; 154(3); 459-67
8. Latysheva NV, Filatova EG, Osipova DV, Memory and attention deficit in migraine: Overlooked symptoms: Zh Nevrol Psikhiatr Im SS Korsakova, 2019; 119(2); 39-43
9. Headache Classification Committee of the International Headache Society (IHS), The international classification of headache disorders: Cephalalgia, 2013; 33(9); 629-808
10. Cui WQ, Zhang JW, Xu F, MRI evaluation of the relationship between abnormalities in vision-related brain networks and quality of life in patients with migraine without aura: Neuropsychiatr Dis Treat, 2021; 17; 3569-79
11. Demir YP, Sumer MM, Effects of smartphone overuse on headache, sleep and quality of life in migraine patients: Neurosciences (Riyadh), 2019; 24(2); 115-21
12. Brown KW, Ryan RM, The benefits of being present: Mindfulness and its role in psychological well-being: J Pers Soc Psychol, 2003; 84(4); 822-48
13. Zung WW, A rating instrument for anxiety disorders: Psychosomatics, 1971; 12(6); 371-79
14. Zung WW, A self-rating depression scale: Arch Gen Psychiat, 1965; 12; 63-70
15. Li JM, Self-rating scale of sleep: Chin J Health Psychol, 2012; 020; 1851
16. Yan CG, Wang XD, Zuo XN, Zang YF, DPABI: Data processing & analysis for (resting-state) brain imaging: Neuroinformatics, 2016; 14(3); 339-51
17. Bell AJ, Sejnowski TJ, An information-maximization approach to blind separation and blind deconvolution: Neural Comput, 1995; 7(6); 1129-59
18. Smith SM, Fox PT, Miller KL, Correspondence of the brain’s functional architecture during activation and rest: Proc Natl Acad Sci USA, 2009; 106(31); 13040-45
19. Song XW, Dong ZY, Long XY, REST: A toolkit for resting-state functional magnetic resonance imaging data processing: PLoS One, 2011; 6(9); e25031
20. Zang Y, Jiang T, Lu Y, Regional homogeneity approach to fMRI data analysis: Neuroimage, 2004; 22(1); 394-400
21. Sinforiani E, Zinelli P, Faglia L, Lateralization of visual attention in patients with classic migraine and unilateral prodromes: Funct Neurol, 1989; 4(3); 247-52
22. Smith SM, Fox PT, Miller KL, Correspondence of the brain’s functional architecture during activation and rest: Proc Natl Acad Sci USA, 2009; 106(31); 13040-45
23. Fasmer OB, Halmøy A, Oedegaard KJ, Haavik J, Adult attention deficit hyperactivity disorder is associated with migraine headaches: Eur Arch Psychiatry Clin Neurosci, 2011; 261(8); 595-602
24. Carpenet C, Guichard E, Tzourio C, Kurth T, Self-perceived attention deficit and hyperactivity symptom levels and risk of non-migraine and migraine headaches among university students: A cross-sectional study: Cephalalgia, 2019; 39(6); 711-21
25. Attygalle UR, Hewawitharana G, Wijesinghe CJ, Migraine, attention deficit hyperactivity disorder and screen time in children attending a Sri Lankan tertiary care facility: Are they associated?: BMC Neurol, 2020; 20(1); 275
26. Gong M, Liu T, Biased neural representation of feature-based attention in the human frontoparietal network. J: Neurosci, 2020; 40(43); 8386-95
27. Li X, Gandour J, Talavage T, Selective attention to lexical tones recruits left dorsal frontoparietal network: Neuroreport, 2003; 14(17); 2263-66
28. Johnson KW, Phebus LA, Cohen ML, Serotonin in migraine: Theories, animal models and emerging therapies: Prog Drug Res, 1998; 51; 219-44
29. Melek LN, Smith JG, Karamat A, Renton T, Comparison of the neuropathic pain symptoms and psychosocial impacts of trigeminal neuralgia and painful posttraumatic trigeminal neuropathy: J Oral Facial Pain Headache, 2019; 33(1); 77-88
30. Zheng YJ, Zhang TJ, Yang XQ, A survey of chronic pain in China: Libyan Journal of Medicine, 2020; 15(1); 1730550
31. Liu HY, Chou KH, Chen WT, Migraine and the hippocampus: Curr Pain Headache Rep, 2018; 22(2); 13
32. Ma M, Zhang J, Chen N, Exploration of intrinsic brain activity in migraine with and without comorbid depression: J Headache Pain, 2018; 19(1); 48
33. Hansen TM, Lelic D, Olesen AE, Differential effects of oxycodone and venlafaxine on resting state functional connectivity – a randomized placebo-controlled magnetic resonance imaging study: CNS Neurosci Ther, 2018; 24(9); 820-27
34. Gallagher HC, Gallagher RM, Butler M, Venlafaxine for neuropathic pain in adults: Cochrane Database Syst Rev, 2015; 2015(8); CD011091
35. Lelic D, Fischer IW, Olesen AE, Venlafaxine and oxycodone effects on human spinal and supraspinal pain processing: A randomized cross-over trial: Eur J Neurosci, 2016; 44(11); 2966-74
36. Li S, Tian J, Li M, Altered resting state connectivity in right side frontoparietal network in primary insomnia patients: Eur Radiol, 2018; 28(2); 664-72
37. Vigano A, Toscano M, Puledda F, Di Piero V, Treating chronic migraine with neuromodulation: the role of neurophysiological abnormalities and maladaptive plasticity: Front Pharmacol, 2019; 10; 32
38. Halker SR, Ailani J, Robbins MS, Neuromodulation for the acute and preventive therapy of migraine and cluster headache: Headache, 2019; 59(Suppl 2); 33-49
Figures
Figure 1. The selected resting-state frontoparietal network in this studyFPN included left FPN and right FPN. Left FPN (A) included the right inferior semilunar lobule, left fusiform gyrus, the orbital part of right inferior frontal gyrus, right parietal lobule, left supra-marginal gyrus, the left orbital middle frontal gyrus, right middle frontal gyrus, etc. Right FPN (B) included the left inferior semilunar lobule, right middle frontal gyrus, the orbital part of left inferior frontal gyrus, right parahippocampal gyrus, right supraoccipital gyrus, right superior marginal gyrus, etc. MATLAB R2017a (MathWorks, Inc., USA) was used to create this figure.Figure 2. Comparison of MAAS, SAS, SDS and SRSS scores between the MwoA group and the HC groupThe scatter diagram of MAAS (A), SAS (B), SDS (C), and SRSS (D) scores in 2 groups. This figure was created using GraphPad Prism 6 (GraphPad Software, Inc., San Diego, CA, USA).Figure 3. Comparison of lFPN functional activity between the MwoA group and the HC groupThe functional activity peak of the right inferior semilunar lobule [Coordinates (38, −72, 46), T-value (−18.60), Voxel values (2283)], left fusiform gyrus [Coordinates (−54, −56, −10), T-value (−15.55), Voxel values (463)], the orbital part of right inferior frontal gyrus [Coordinates (48, 44, −14), T-value (−14.86), Voxel values (302)], right parietal lobule [Coordinates (36, −68, 52), T-value (−14.70), Voxel values (377)] and left supra-marginal gyrus [Coordinates (−48, −62, 46), T-value (−14.47), Voxel values (733)] were weaker in the MwoA group. The functional activity peak of the left orbital middle frontal gyrus [Coordinates (−38, 42, −14), T-value (18.30), Voxel values (2469)] and right middle frontal gyrus [Coordinates (54, 34, 22), T-value (9.06), Voxel values (291)] were higher in the MwoA group. The warmer colors represent a stronger functional activity, while the cold colors represent a weakened functional activity. MATLAB R2017a (MathWorks, Inc., USA) was used to create this figure.Figure 4. The comparison of rFPN functional activity between the MwoA group and the HC groupThe functional activity peak of the left inferior semilunar lobule [Coordinates (−38, −74, −48), T-value (18.71), Voxel values (4383)], right middle frontal gyrus [Coordinates (44, 36, 34), T-value (21.64), Voxel values (3364)], the orbital part of left inferior frontal gyrus [Coordinates (−44, 50, −12), T-value (14.83), Voxel values (664)], right parahippocampal gyrus [Coordinates (18, −26, −14), T-value (5.04), Voxel values (427)], right supraoccipital gyrus [Coordinates (24, −74, 20), T-value (4.56), Voxel values (277)] and right superior marginal gyrus [Coordinates (60, −52, 38), T-value (23.11), Voxel values (2184)] were stronger in the MwoA group. The warmer colors represent a stronger functional activity. MATLAB R2017a (MathWorks, Inc., USA) was used to create this figure. Tables
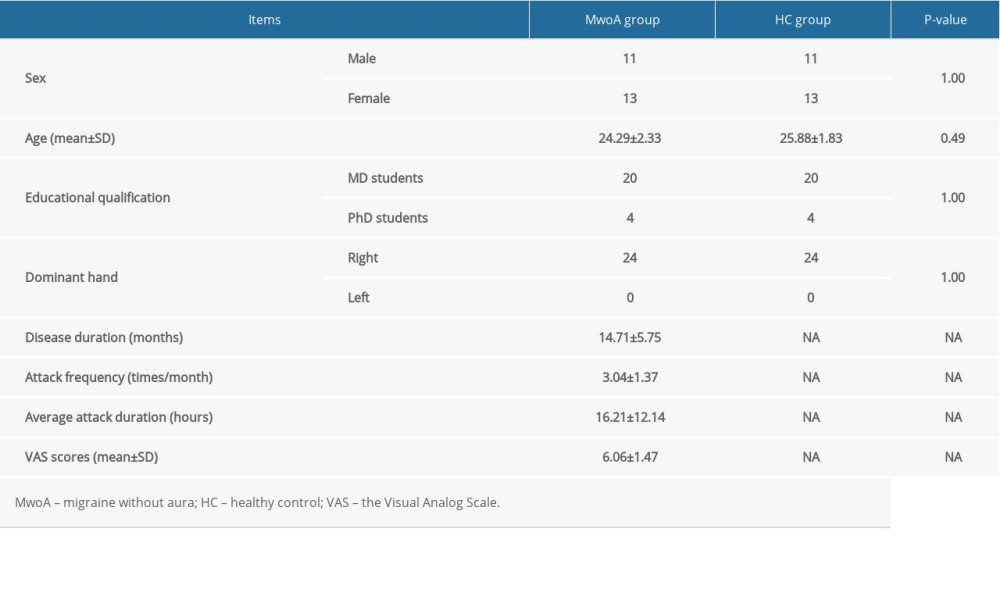 Table 1. Baseline characteristics and VAS scores of participants.
Table 1. Baseline characteristics and VAS scores of participants.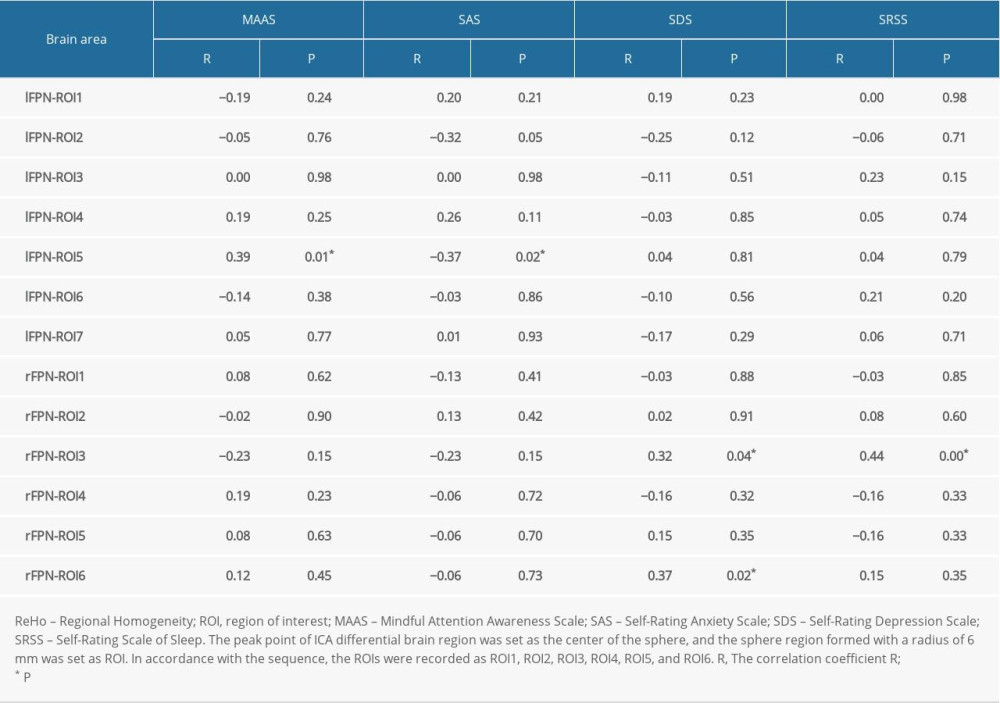 Table 2. Correlation analysis of the ReHo value of ROIs and MAAS, SAS, SDS, and SRSS scores.Table 1. Baseline characteristics and VAS scores of participants.Table 2. Correlation analysis of the ReHo value of ROIs and MAAS, SAS, SDS, and SRSS scores.
Table 2. Correlation analysis of the ReHo value of ROIs and MAAS, SAS, SDS, and SRSS scores.Table 1. Baseline characteristics and VAS scores of participants.Table 2. Correlation analysis of the ReHo value of ROIs and MAAS, SAS, SDS, and SRSS scores. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387