10 April 2022: Clinical Research
Organ-Sparing Pancreatectomy for Benign or Low-Grade Malignant Pancreatic Tumors: A Single-Center Experience with 101 Consecutive Patients
Kang Fang1ABCE, Gen Sun1ACE, Ming Zha1BF, Shuju Tu1CD, Yuanpeng Xiong1DF, Siqing Yi1BF, Yonghao Ouyang2BC, Yong Li1AD, Weidong Xiao1ACEG*DOI: 10.12659/MSM.935685
Med Sci Monit 2022; 28:e935685






Abstract
BACKGROUND: Pancreaticoduodenectomy (PD) and distal pancreatectomy with splenectomy (DPS) are considered the standard procedures for pancreatic lesions. However, long-term metabolic consequences of PD and DPS applied for benign or low-grade malignant tumors need to be addressed. This study aimed to investigate the short- and long-term outcomes of organ-sparing pancreatectomy for benign or low-grade malignant pancreatic tumors in our institution.
MATERIAL AND METHODS: The clinical data of 101 patients with benign or low-grade malignant pancreatic tumors who underwent organ-sparing pancreatectomy from January 2009 to September 2021 were retrospectively analyzed, including 40 tumor enucleations (EN), 22 central pancreatectomies (CP), 25 spleen-preserving distal pancreatectomies (SPDP), 7 pylorus-preserving pancreaticoduodenectomies (PPPD) and 7 duodenum-preserving pancreatic head resections (DPPHR).
RESULTS: The mean operative time, intraoperative blood loss, and length of hospital stay were 182.9±74.6 min, 191.9±127.8 mL, and 11.6±8.1 days, respectively. EN had the shortest operative time, while DPPHR had the longest operative time. The mean intraoperative blood loss of DPPHR and PPPD was significantly greater than the others (all P<0.05). The length of hospital stay of PPPD was longest. The overall morbidity was 33.6%. The reoperation rate was 1.0% and there was no mortality. The incidence of pancreatic endocrine insufficiency and exocrine insufficiency were 5.9% and 6.9%, respectively. None patients had tumor recurrence during the follow-up period.
CONCLUSIONS: Organ-sparing pancreatectomy is associated with acceptable perioperative risk and postoperative complications and better long-term outcomes in the aspects of preservation of function and curability in benign or low-grade malignant pancreatic tumors.
Keywords: Non Functioning Pancreatic Endocrine Tumor, Pancreatectomy, Therapeutic Equivalency, Blood Loss, Surgical, Humans, Neoplasm Recurrence, Local, Pancreatic Neoplasms, Postoperative Complications
Background
With the development of imaging technology and endoscopic ultrasonography, benign or low-grade malignant pancreatic tumors have been diagnosed more frequently in recent years. Most of these patients need to be treated by surgery because of clinical symptoms or the potential of malignancy [1]. However, the surgical treatment of benign or low-grade malignant pancreatic tumors is still challenging to pancreatic surgeons, as there is no consensus on selected surgical procedures. Pancreaticoduodenectomy (PD) and distal pancreatectomy with splenectomy (DPS) are considered as the standard procedures for tumors located at the pancreatic head or body-tail, respectively. These 2 procedures have the advantages of radical resection and decreasing the risk of tumor recurrence. However, these approaches result in an unnecessary loss of normal pancreatic parenchyma, with subsequent impairment of pancreatic exocrine and endocrine functions [2–4]. Moreover, the disadvantages of these standard procedures include the destruction of normal anatomy of the upper gastrointestinal and biliary tract in PD and the sacrifice of the spleen in DPS. As a fact, the quality of life following surgical intervention should be considered for patients with benign or low-grade-malignant pancreatic lesions having excellent long-term survival. In recent years, there has been a growing interest in organ-sparing pancreatectomy to achieve better functional results without compromising oncological radicality for treating benign or low-grade malignant tumors [5–8]. This study aimed to investigate the short- and long-term outcomes of organ-sparing pancreatectomy for benign or low-grade malignant pancreatic tumors in a single center over 12 years.
Material and Methods
STUDY DESIGN:
We performed a retrospective cohort study using a prospectively collected database including all consecutive patients with benign or low-grade malignant pancreatic tumors undergoing organ-sparing pancreatectomy in our institution from January 2009 to September 2021. All patients underwent an abdominal enhanced CT or MRI scan before surgery. A multidisciplinary team specializing in pancreatic surgery made a diagnosis and devised an individualized therapeutic strategy. All patients provided informed consent to the treatment. The Ethics Review Board of the First Affiliated Hospital of Nanchang University approved this study. All patients’ characteristics, surgical features, and intraoperative and postoperative outcomes were retrospectively reviewed.
PATIENTS:
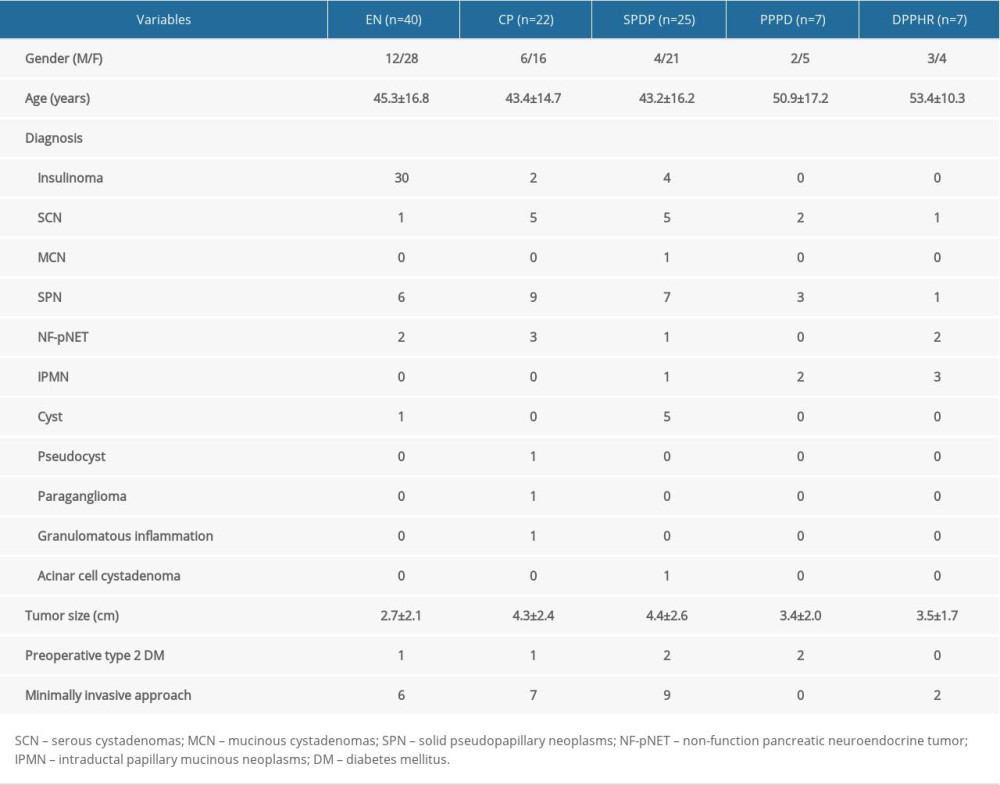
A total of 101 patients were enrolled in this retrospective study. There were 27 men and 74 women with a median age of 45.3±15.9 (range, 10–75) years. Twenty-two of the tumors were located at the head, 19 at the neck, and 60 at the body or tail of the pancreas. The mean tumor size was 3.6±2.4 cm (range, 1.0–13.0 cm). The pathological diagnosis included insulinoma (n=36), solid pseudopapillary neoplasms (SPN, n=26), serous cystadenomas (SCN, n=14), cyst (n=6), intraductal papillary mucinous neoplasms (IPMN, n=6), grade G1 or G2 nonfunctional pancreatic neuroendocrine tumors (NF-pNET, n=8), mucinous cystadenomas (MCN, n=1), paraganglioma (n=1), pseudocyst (n=1), acinar cell cystadenoma (n=1), and granulomatous inflammation (n=1).
SURGICAL PROCEDURES:
The surgical procedures included tumor enucleation (EN, n=40), central pancreatectomy (CP, n=22), spleen-preserving distal pancreatectomy (SPDP, n=25), pylorus-preserving pancreaticoduodenectomy (PPPD, n=7), and duodenum-preserving pancreatic head resection (DPPHR, n=7). Minimally invasive approaches were performed in 24 patients, including 3 laparoscopic ENs, 3 laparoscopic CPs, 7 laparoscopic SPDPs, 3 robotic-assisted ENs, 4 robotic-assisted CPs, 2 robot-assisted SPDPs, and 2 robot-assisted DPPHRs. Pancreaticogastrostomy reconstruction was performed in 2 laparoscopic CPs, 4 robot-assisted CPs, and 2 robot-assisted DPPHRs. Pancreaticojejunostomy reconstruction was performed in the rest of the CPs and DPPHRs and all PPPDs. The patients’ characteristics, pathological diagnosis, and surgical procedures are shown in Table 1.
POSTOPERATIVE MANAGEMENT:
Postoperative treatments included antibiotics, proton pump inhibitors, somatostatin analogs, water-electrolyte balance, and nutritional support treatments. Somatostatin analogs were administered intravenously for the first 7 days after the operation. An analysis of abdominal drain fluid amylase concentration to identify pancreatic fistula was performed on postoperative days 1, 3, 5, and 7. The total bilirubin level of drain fluid was measured if suspicious for complicated biliary leakage. The drainage tube was typically removed between days 5 and 7 in the absence of clinically relevant postoperative pancreatic fistula (CR-POPF) and biliary leakage. The nasogastric tube was removed after recovery of intestinal function, and a liquid diet intake orally was started.
DATA COLLECTION AND STUDY OUTCOMES:
Perioperative data, including operative time, intraoperative blood loss, length of hospital stay, reoperation, readmission, morbidity, and mortality (within 30 days after surgery) were collected and analyzed. Postoperative pancreatic fistula (POPF), delayed gastric emptying (DGE), and post-pancreatectomy hemorrhage (PPH) were assessed according to the criteria of the International Study Group of Pancreatic Surgery [9–11]. Grade B and C pancreatic fistulas were defined as CR-POPF. Intra-abdominal infection or abscess was diagnosed when signs of peritonitis, increased white blood cell count, and positive drainage-fluid culture was present or identified by abdominal puncture and a CT scan [12]. The severity of complications was scored according to the Clavien-Dindo classification system [13].
FOLLOW-UP:
All patients received follow-up every 3 to 6 months at outpatient clinics or by telephone interview. The long-term outcomes included pancreatic endocrine and exocrine functions, and tumor recurrence. Pancreatic endocrine insufficiency was defined as new-onset diabetes mellitus (NODM) or worsening previous diabetes mellitus. NODM was diagnosed according to the criteria of the World Health Organization [14]. Pancreatic exocrine insufficiency (PEI) was defined as patients with symptoms of diarrhea, steatorrhea, or weight loss, and need for pancreatic enzyme replacement therapy (PERT), and/or an abnormal pancreatic exocrine function test (with a 13C-labeled mixed triglyceride breath test, fecal elastase determination, or fat absorption test) [15]. Routine blood tests and portal vein system thrombosis were evaluated in patients after SPDP.
STATISTICAL ANALYSIS:
Data were analyzed with SPSS 26.0 for windows (SPSS, Chicago, IL). Quantitative data were presented as mean±standard deviation (SD) and compared using the
Results
PERIOPERATIVE OUTCOMES:
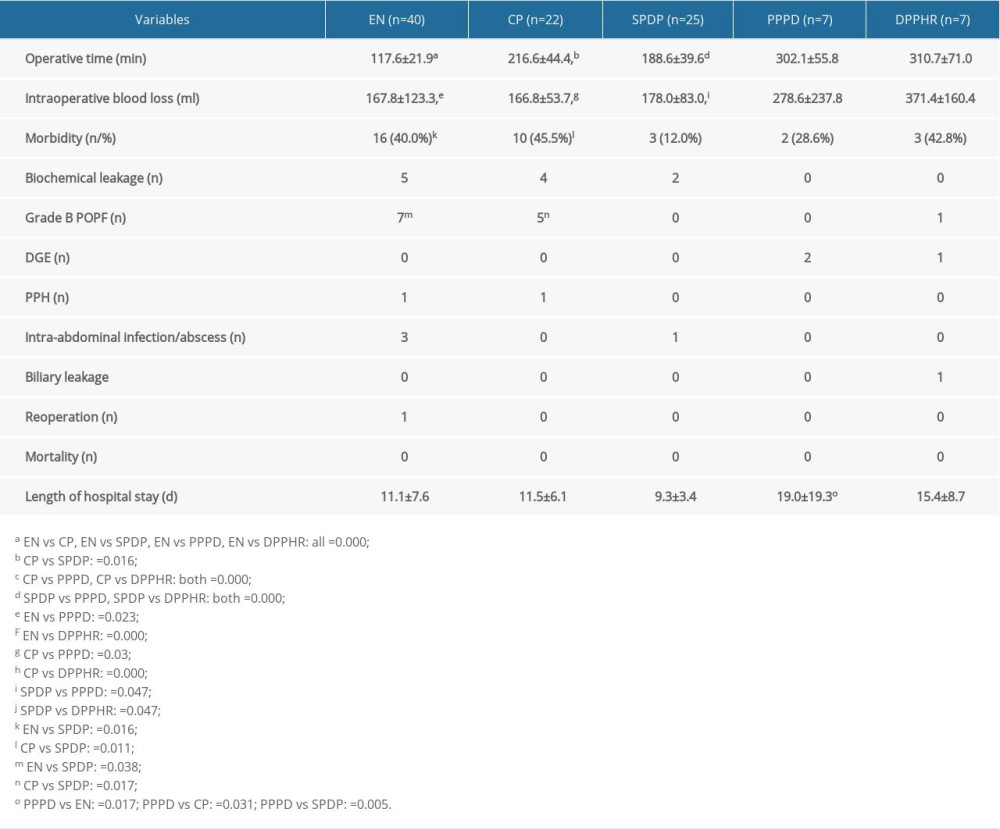
The mean operative time, intraoperative blood loss, and length of hospital stay were 182.9±74.6 min (range, 75–420 min), 191.9±127.8 mL (range, 50–800 mL), and 11.6±8.1 days (range, 4–61 days), respectively. Perioperative outcomes of different surgical procedures are listed in Table 2. EN had the shortest operative time, while DPPHR had the longest operative time. The mean intraoperative blood loss of DPPHR and PPPD was significantly greater than those of EN, CP, and SPDP (all P<0.05). The length of hospital stay of PPPD was significantly longer than those of EN, CP, and SPDP (all P<0.05).
The overall morbidity was 33.6% (34/101), including 11 (10.9%) biochemical pancreatic leakages, 13 (12.9%) grade B POPFs, 4 (4.0%) intra-abdominal infection/abscesses, 3 (3.0%) DGEs, 2 (2.0%) PPHs, and 1 (1.0%) biliary leakage. CP had the highest morbidity (45.5%), while SPDP had the lowest morbidity (12.0%). One patient (1.0%) underwent reoperation due to intra-abdominal hemorrhage after robot-assisted EN. According to the Clavien-Dindo classification, 8 patients were grade I, 21 patients were grade II, 4 patients were grade IIIa, and 1 patient was grade IIIb. There were no grade C POPFs or and mortalities.
LONG-TERM OUTCOMES:
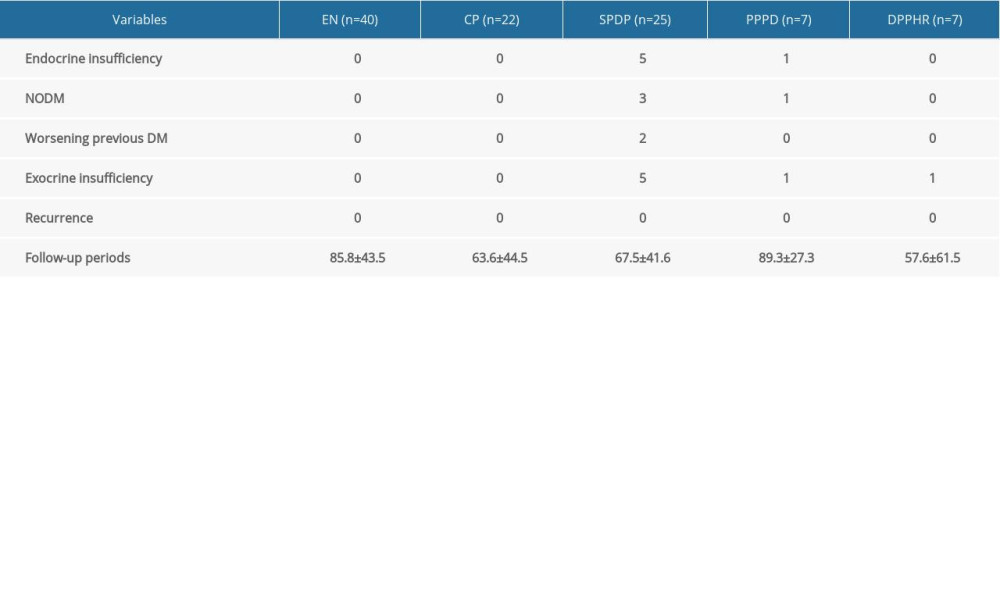
Up to October 2021, all patients were followed up for an average of 74.7±44.3 months (1–153 months). The long-term outcomes of different surgical procedures are listed in Table 3. Six (5.9%, 6/101) patients had pancreatic endocrine insufficiency, including 5 in the SPDP group and 1 in the PPPD group. Seven (6.9%, 7/101) patients had PEI, including 5 in the SPDP group, 1 in the PPPD group, and 1 in the DPPHR group. There was no abnormal elevation of platelet count or portal vein system thrombosis in patients after SPDP. No patients had tumor recurrence during the follow-up period.
Discussion
In general, PD and DPS are considered the standard procedures for the treatment of pancreatic lesions. However, long-term metabolic consequences of PD and DPS applied for benign or low-grade malignant tumors need to be addressed, because these patients have a longer life expectancy. It was reported that persistence of NODM after PD for benign tumors was observed in 14.5% of cases, and for malignant tumors in 15.5% of patients. PEI was found after PD for benign tumors in 25.2% and malignant tumors in 49.1% of patients [2]. Following distal pancreatectomy (DP), 12.6–30.2% of patients developed endocrine insufficiency, and 20.2% of patients developed PEI [3,4]. Compared with PD and DPS, organ-sparing pancreatectomy seems a more reasonable procedure for the treatment of benign or low-grade tumors. The most important advantage is their ability to preserve pancreatic endocrine and exocrine functions in the long-term outcome [16–19]. Although there is no uniform definition of organ-sparing pancreatectomy, EN, CP, SPDP, DPPHR, PPPD, middle-preserving pancreatectomy (MPP), and pancreatic head resection with segmental duodenectomy (PHRSD) can be categorized as organ-sparing procedures. This study aimed to assess the short- and long-term outcomes of organ-sparing pancreatectomy for benign or low-grade malignant pancreatic tumors in our institution. We enrolled 101 patients who underwent 5 different types of organ-sparing pancreatectomy, including EN, CP, SPDP, DPPHR, and PPPD. Our data showed that the overall morbidity was 33.7%, the incidence of CR-POPF was 25.8%, the reoperation rate was 1%, and the mortality was 0. As for the long-term outcomes, the incidence of pancreatic endocrine insufficiency and PEI were 5.9% and 6.9%, respectively, with an average of 74.7 months follow-up. Moreover, no patients had tumor recurrence during the follow-up period. Obviously, these organ-sparing procedures are safe and feasible in the treatment of benign or low-grade malignant pancreatic tumors.
EN is suitable for benign or low-grade malignant pancreatic tumors with a diameter less than 3 cm, located on the surface of the pancreas, and located a certain distance from the main pancreatic duct. This procedure can preserve the normal pancreatic tissue as much as possible and shorten the operation time; however, it is accompanied by a higher incidence of POPF. Faitot et al reported that among 126 patients who underwent EN, the morbidity and mortality were 63% and 0.8%, respectively. The incidence of grade B/C POPF was 41%, and the reoperation rate was 3%. Postoperative NODM was 0.8% and without PEI [20]. Forty cases of EN were included in the current study. The main indication was insulinoma, which is the most common functional pNET. EN had the shortest operative time when compared with other organ-sparing procedures. The morbidity was 40%, and the incidence of CR-POPF was 17.5%, which was higher than that of SPDP and comparable with CP. Our follow-up data showed that no patients had pancreatic endocrine or exocrine insufficiency after EN. These results suggest EN could be an alternative to standard resection for small, benign, and low-grade lesions located far from the main pancreatic duct.
CP, which was first used by Guillemin and Bessot in 1957 [21], is considered an ideal procedure for benign or low-grade malignant lesions located at the pancreatic neck and proximal body which are not suitable for EN. The most evident advantage of CP is to preserve the normal pancreatic tissue as much as possible and reduce the risk of pancreatic endocrine and exocrine insufficiency [22,23]. Furthermore, CP can preserve the structure and function of the gastrointestinal and biliary tract when compared with PD, and better preserve the spleen when compared with DPS, which avoids the risk of overwhelming post-splenectomy infection and hematological disorders. However, CP is associated with a higher risk of POPF, due to 2 pancreatic cutting edges, and most patients have a normal pancreatic texture and small pancreatic duct. Generally, there are 3 types of reconstruction for the pancreatic stump following central resection: PJ, PG, and “Ω” anastomosis, and there is no significant difference in the incidence of POPF after PJ and PG [17]. Therefore, the choice of a PJ or PG reconstruction after CP should be based on the surgeon’s preference, skill, and experience. We prefer to use PG in minimally invasive CP, because it is easier in technique and can preserve the normal structure of the upper digestive tract. In this study, 22 CPs were performed, including 7 minimally invasive procedures. Although the POPF rate was higher than that of SPDP, PPPD, and DPPHR, there were no reoperations or deaths related to POPF. Most importantly, the endocrine and exocrine functions of the pancreas were well preserved in long-term outcomes. Thus, our results reinforce the existing evidence of good long-term outcomes of CP for the treatment of benign or low-grade malignant tumors located at the pancreatic neck and proximal body.
SPDP is an alternative operation for lesions located at the body and tail of the pancreas. Splenic preservation has the advantages of less blood loss, fewer postoperative complications, shorter length of hospitalization, and avoidance of the long-term risk of post-splenectomy sepsis. In a meta-analysis, 521 SPDP patients were compared with 1131 DPS patients. SPDP patients were found to have significantly less operative blood loss, shorter duration of hospitalization, lower incidence of fluid collection and abscess, lower incidence of postoperative splenic and portal vein thrombosis, less grade B/C POPF, and lower incidence of postoperative NODM [24]. According to whether there is preservation of the splenic vessel, SPDP is divided into Kimura’s technique (preserving the splenic vessel) and Warshaw’s technique (resecting the splenic vessel but carefully preserving the short gastric and left gastroepiploic vessels) [25,26]. The latter technique is faster and easier; however, it carries the risk of postoperative splenic infarction and development of gastric varices [27,28]. Therefore, Kimura’s technique is considered the best choice for splenic preservation. In the present study, 25 patients underwent SPDP, including 21 with Kimura’s technique and 4 with Warshaw’s technique. Three patients had complications and fully recovered through conservative management. In long-term outcomes, both pancreatic endocrine insufficiency and PEI rate were 20%, which is consistent with previous reports [3,4]. No patients had an abnormal elevation of platelet count and portal vein system thrombosis, which suggests that SPDP can reduce abnormal hematological changes caused by splenectomy.
DPPHR and PPPD are organ-sparing procedures for lesions located at the head of the pancreas. DPPHR, which was first introduced by Beger in 1972, is mainly applied for chronic pancreatitis and benign or low-grade malignant tumors of the pancreatic head [29]. DPPHR has the advantages of shorter operation time, shorter duration of hospital stay, and lower cost of hospitalization when compared with PD [30,31]. Furthermore, DPPHR has the advantages of lower incidence of morbidity and higher postoperative quality of life, all while achieving the same surgical outcome. A systematic review analyzed the clinical data of 416 patients who underwent duodenum-preserving total or partial pancreatic head resection (DPPHRt/p). The frequencies of POPF, reoperation rate, and mortality were 19.2%, 1.7%, and 0.48%, respectively. Meanwhile, this meta-analysis suggested that DPPHRt/p significantly preserved the level of exocrine and endocrine pancreatic functions compared to PD, and the frequency of POPF, DGE, or mortality was comparable [32]. In our group, DPPHR was performed in 7 cases, with a morbidity rate of 42.8%. SPN, NF-pNET, and IPMN were the main indications. The operative time and intraoperative blood loss using DPPHR were significantly higher than those of EN, CP, and SPDP and comparable to PPPD, indicating that the complication rate of DPPHR was not inferior to that of PPPD. PPPD was first introduced by Watson in 1944 [33], but this technique was not widely accepted until 1978 when Traverso and Longmire republished it [34]. The expected advantages of PPPD over standard PD are considered to be as follows: less dumping, improved gastrointestinal function, reduced jejunal ulceration, and improved postoperative quality of life. PPPD is comparable to standard PD in terms of operative time, number of blood transfusions, and intraoperative blood loss, but is associated with a higher incidence of DGE [35–37]. In the present study, 2 patients were complicated with DGE in 7 PPPD, which was accompanied by prolonged hospital stay.
This study has several limitations, which should be taken into account when interpreting the results. First, our data were from multiple surgery teams, so the heterogeneity of surgical technique was inevitable. Second, comparison between the outcomes of patients who received standard treatment (PD and DPS) and those who underwent organ-sparing pancreatomy would be useful, and we intend to do this in further research. Finally, as this is only a retrospective study from a single institution with a limited number of cases, additional large-scale, multi-center randomized controlled trials are needed to further define our results.
Conclusions
Our data confirm that organ-sparing pancreatectomy is associated with acceptable perioperative risk and postoperative complications and good long-term outcomes in preservation of function and curability in benign or low-grade malignant tumors.
References
1. Beger HG, Poch B, Vasilescu C, Benign cystic neoplasm and endocrine tumours of the pancreas – when and how to operate – an overview: Int J Surg, 2014; 12(6); 606-14
2. Beger HG, Poch B, Mayer B, Siech M, New onset of diabetes and pancreatic exocrine insufficiency after pancreaticoduodenectomy for benign and malignant tumors: A systematic review and meta-analysis of long-term results: Ann Surg, 2018; 267(2); 259-70
3. Kusakabe J, Anderson B, Liu J, Long-term endocrine and exocrine insufficiency after pancreatectomy: J Gastrointest Surg, 2019; 23(8); 1604-13
4. Hallac A, Aleassa EM, Rogers M, Exocrine pancreatic insufficiency in distal pancreatectomy: Incidence and risk factors: HPB (Oxford), 2020; 22(2); 275-81
5. Sperti C, Beltrame V, Milanetto AC, Parenchyma-sparing pancreatectomies for benign or border-line tumors of the pancreas: World J Gastrointest Oncol, 2010; 2(6); 272-81
6. Lee SE, Jang JY, Hwang DW, Clinical efficacy of organ-preserving pancreatectomy for benign or low-grade malignant potential lesion: J Korean Med Sci, 2010; 25(1); 97-103
7. Beger HG, Benign tumors of the pancreas-radical surgery versus parenchyma-sparing local resection-the challenge facing surgeons: J Gastrointest Surg, 2018; 22(3); 562-66
8. Zhang RC, Ma J, Mou YP, Short- and long-term outcomes of laparoscopic organ-sparing resection for pancreatic neuroendocrine neoplasms: World J Surg, 2020; 44(11); 3795-800
9. Bassi C, Marchegiani G, Dervenis C, The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 years after: Surgery, 2017; 161(3); 584-91
10. Wente MN, Bassi C, Dervenis C, Delayed gastric emptying (DGE) after pancreatic surgery: A suggested definition by the International Study Group of Pancreatic Surgery (ISGPS): Surgery, 2007; 142(5); 761-68
11. Wente MN, Veit JA, Bassi C, Postpancreatectomy hemorrhage (PPH): An International Study Group of Pancreatic Surgery (ISGPS) definition: Surgery, 2007; 142(1); 20-25
12. Zhang GQ, Li XH, Ye XJ, Internal versus external drainage with a pancreatic duct stent for pancreaticojejunostomy during pancreaticoduodenectomy for patients at high risk for pancreatic fistula: A comparative study: J Surg Res, 2018; 232; 247-56
13. Dindo D, Demartines N, Clavien PA, Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey: Ann Surg, 2004; 240(2); 205-13
14. Alberti KG, Zimmet PZ, Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus provisional report of a WHO consultation: Diabet Med, 1998; 15(7); 539-53
15. Roeyen G, Jansen M, Ruyssinck L, Pancreatic exocrine insufficiency after pancreaticoduodenectomy is more prevalent with pancreaticogastrostomy than with pancreaticojejunostomy. A retrospective multicentre observational cohort study: HPB (Oxford), 2016; 18(12); 1017-22
16. Li Y, Wu W, Zhang T, Comparison of long-term benefits of organ-preserving pancreatectomy techniques for benign or low-grade malignant tumors at the pancreatic head: Medicine (Baltimore), 2017; 96(51); e9420
17. Xiao W, Zhu J, Peng L, The role of central pancreatectomy in pancreatic surgery: A systematic review and meta-analysis: HPB (Oxford), 2018; 20(10); 896-904
18. Cienfuegos JA, Salguero J, Núñez-Córdoba JM, Short- and long-term outcomes of laparoscopic organ-sparing resection in pancreatic neuroendocrine tumors: A single-center experience: Surg Endosc, 2017; 31(10); 3847-57
19. Song KB, Kim SC, Hwang DW, Enucleation for benign or low-grade malignant lesions of the pancreas: Single-center experience with 65 consecutive patients: Surgery, 2015; 158(5); 1203-10
20. Faitot F, Gaujoux S, Barbier , Reappraisal of pancreatic enucleations: A single-center experience of 126 procedures: Surgery, 2015; 158(1); 201-10
21. Guillemin P, Bessot M, Chronic calcifying pancreatitis in renal tuberculosis: Pancreatojejunostomy using an original technic: Mem Acad Chir (Paris), 1957; 83(27–28); 869-71
22. Paiella S, De PM, Faustini F, Central pancreatectomy for benign or low-grade malignant pancreatic lesions – a single-center retrospective analysis of 116 cases: Eur J Surg Oncol, 2019; 45(5); 788-92
23. Shi Y, Jin J, Huo Z, An 8-year single-center study: 170 cases of middle pancreatectomy, including 110 cases of robot-assisted middle pancreatectomy: Surgery, 2020; 167(2); 436-41
24. Pendola F, Gadde R, Ripat C, Distal pancreatectomy for benign and low-grade malignant tumors: Short-term postoperative outcomes of spleen preservation-A systematic review and update meta-analysis: J Surg Oncol, 2017; 115(2); 137-43
25. Warshaw AL, Conservation of the spleen with distal pancreatectomy: Arch Surg, 1988; 123(5); 550-53
26. Kimura W, Inoue T, Futakawa N, Spleen-preserving distal pancreatectomy with conservation of the splenic artery and vein: Surgery, 1996; 120(5); 885-90
27. Miura F, Takada T, Asano T, Hemodynamic changes of splenogastric circulation after spleen-preserving pancreatectomy with excision of splenic artery and vein: Surgery, 2005; 138(3); 518-22
28. Warshaw AL, Distal pancreatectomy with preservation of the spleen: J Hepatobiliary Pancreat Sci, 2010; 17(6); 808-12
29. Beger HG, Witte C, Krautzberger W, Bittner R, Experiences with duodenum-sparing pancreas head resection in chronic pancreatitis: Chirurg, 1980; 51(5); 303-7
30. Zhao Y, Zhang J, Lan Z, Duodenum-preserving resection of the pancreatic head versus pancreaticoduodenectomy for treatment of chronic pancreatitis with enlargement of the pancreatic head: Systematic review and meta-analysis: Biomed Res Int, 2017; 2017; 3565438
31. Sun YH, Ding N, Cheng K, Comparative analysis of duodenum-preserving pancreatic head resection and pancreaticoduodenectomy: Chin Med J (Engl), 2020; 133(17); 2112-13
32. Beger HG, Nakao A, Mayer B, Poch B, Duodenum-preserving total and partial pancreatic head resection for benign tumors – systematic review and meta-analysis: Pancreatology, 2015; 15(2); 167-78
33. Kenneth W, Carcinoma of the ampulla of Vater: Successful radical resection: Br J Surg, 1944; 31; 368-73
34. Traverso LW, Longmire WP, Preservation of the pylorus in pancreaticodenectomy: Surg Gynecol Obstet, 1978; 146(6); 959-62
35. Zhou Y, Lin L, Wu L, Xu D, Li B, A case-matched comparison and meta-analysis comparing pylorus-resecting pancreaticoduodenectomy with pylorus-preserving pancreaticoduodenectomy for the incidence of postoperative delayed gastric emptying: HPB(Oxford), 2015; 17(4); 337-43
36. Cai X, Zhang M, Liang C, Delayed gastric emptying after Pancreaticoduodenectomy: A propensity score-matched analysis and clinical Nomogram study: BMC Surg, 2020; 20(1); 149
37. Lee YH, Hur YH, Kim HJ, Is delayed gastric emptying associated with pylorus ring preservation in patients undergoing pancreaticoduodenectomy?: Asian J Surg, 2021; 44(1); 137-42
In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387