01 June 2022: Clinical Research
Assessment of Functional Performance in Children with Cerebral Palsy Receiving Treatment in a Day Care Facility: An Observational Study
Andżelina Wolan-Nieroda1ABCE*, Aleksandra Łukasiewicz1CF, Justyna Leszczak1DEF, Mariusz DrużbickiDOI: 10.12659/MSM.936207
Med Sci Monit 2022; 28:e936207






Abstract
BACKGROUND: The study assessed changes in functional performance of children with cerebral palsy (CP), immediately following treatment and 2 months later, in addition to investigating the relationship between therapy effect and sex, age, or comorbidities.
MATERIAL AND METHODS: Functional performance of 32 children with spastic diplegia CP, aged 9-16 years, was assessed for: 1) manual function (Box and Block test), motor capacities (Gross Motor Function Measure), sensory capacities (Finger Identification [FI] and Localisation of Tactile Stimuli test [LTC]), and 2) activity and participation, ie, independence in essential and more complex daily activities (Barthel Index; Paediatric Evaluation of Disability Inventory). Measurements were conducted before the start (Month 0), immediately after 6-month rehabilitation program (Month 6), and following a 2-month period with no therapy, ie, 8 months after baseline measurement (Month 8).
RESULTS: Comparison of Month 0 and Month 6 scores showed significant differences (P<0.001) in all measures. However, Month 8 scores were significantly worse in all the measures, except for sensory capacities assessed using FI and LTC (P<0.001).
CONCLUSIONS: Functional performance of children with CP was positively affected by 6-month therapy, but 2 months later these effects significantly deteriorated, except for the sensory capacities. This suggests that therapy focusing on functional performance should be included as a permanent component of rehabilitation programs. These findings may be important for clinical practice as they show that therapy of children with CP should be continuous and systematic, and this should be taken into account by those designing therapeutic programs.
Keywords: Cerebral Palsy, Motor Skills, Motor Skills Disorders, Physical Functional Performance, Rehabilitation, Child, Day Care, Medical, Humans, Upper Extremity
Background
Cerebral palsy (CP), is a heterogeneous group of disorders caused by early brain damage that lasts a lifetime. According to various authors, the incidence of CP is estimated at 1.5–3.3 cases per 1000 live births [1]. In Poland, the incidence of CP is estimated at 2.0–2.5 per 1000 live births [1,2]. CP resulting from a non-progressive lesion occurring in an immature brain is recognized as a disorder most severely affecting motor and postural control [3]. Due to this, therapy of children with CP aims to improve their independent mobility, performance of daily activities, and participation in social life. There are many factors promoting motor improvement in children with CP [4,5]. Effectiveness of various types of therapy intended for patients with CP was assessed in many studies [4–13]. However, most of these did not provide solid evidence related to effectiveness due to the heterogeneity of the study groups, other limitations associated with the type of therapy provided, and the duration of the rehabilitation program [4–8]. This observation encouraged us to investigate this subject matter more extensively.
Functional barriers faced by patients with CP are to a greater or lesser extent associated with their abilities related to gross and fine motor skills [14–16]. Additionally, motor disorders in children with CP are often accompanied by abnormalities connected with sensory integration, body schema, tactile function, communication, perception and behavior [14].
Identification and assessment of functional impairments in children with CP are facilitated by appropriate diagnostic tools, which can also be used to evaluate effects of therapies. The tools most commonly used to identify abnormalities in fine and gross motor skills presented by children with CP include the Gross Motor Function Classification System (GMFCS), Gross Motor Function Measure (GMFM), Manual Ability Classification System (MACS), and Paediatric Evaluation of Disability Inventory (PEDI) [17].
Today, rehabilitation of patients with CP is largely based on neurodevelopmental methods, such as Neurodevelopmental Treatment Bobath (NDT/Bobath), Proprioceptive Neuromuscular Facilitation (PNF), and Sensory Integration (SI), involving sensory stimulation and activation and affecting the patient’s proprioception and kinaesthesia [18–23].
We were also motivated to investigate long-term effects of rehabilitation – to assess patients’ status at baseline, at the end of a 6-month program, and after 2 months without therapy – by the fact that there is a lack of research reports evaluating various therapeutic methods for durability of effects and applying various tools measuring the therapeutic effects in children with CP. Furthermore, no research reports have presented unequivocal conclusions related to the effects of continued therapy versus rehabilitation programs including periods with no therapy on performance of children with CP [6]. The expected implications of our study for the clinical practice include the fact that the findings may provide information which will be helpful for therapists and parents planning therapy of children in CP, and may also be important in the process of designing therapeutic programs in facilities providing treatment to this population of children.
Many studies present information on the relationship between age, sex, or comorbidities and motor performance, physical activity, or quality of life in children with CP [24–32]. Age may be an important factor associated with delayed development of balance, postural control, and selective motor control in younger children with CP; this may adversely affect acquisition of certain skills. On the other hand, adolescents may have more advanced soft tissue contractures and deformities in joints, preventing improvement in gait and other functions, irrespective of muscle strength [24]. Also, comorbidities such as obesity and cardiovascular diseases can lead to reduced activity and impair the quality of life in children with CP [24,25]. Given the above, we believe there is a need to investigate whether the effect of therapy is related to sex, age, and coexisting conditions.
The aim of this study was to assess changes in the functional performance of children with spastic diplegia CP, at the end of treatment and 2 months later, in addition to investigating whether the effect of therapy is related to sex, age, and coexisting conditions. In connection to this we formulated the following hypotheses:
Material and Methods
ETHICS STATEMENT:
The project was approved by the local Bioethics Commission of the Medical Faculty (11/01/2021). Written consent was obtained from all the parents or legal guardians of the children, after they were informed of the study objectives. Participants aged 16 signed an informed consent form as well. Experimental conditions conformed to the Declaration of Helsinki.
DESIGN:
The prospective longitudinal non-randomized study involved a single group.
PROCEDURE:
The study was carried out in a special educational facility in the Podkarpackie Region, Poland. The children’s functional performance associated with manual, motor, and sensory capacities, as well as essential and complex activities of daily living, were measured 3 times. The consecutive measurements were conducted in 3 points of time, ie, before the start of the rehabilitation (Month 0), immediately after the 6-month rehabilitation program was completed (Month 6), and 2 months after the therapy was completed (2-month period with no therapy), ie, 8 months after the baseline measurement, (Month 8). All the children were provided with orthopedic braces worn on the lower limbs as a support for the therapy process. The braces were selected specifically for each child. Three-time assessment of each participant was carried out in the same conditions. All the participants received treatment from the same physiotherapist, and were assessed by one examiner who performed measurements 3 times, at time intervals as described above. Rater calibration was performed using the Kappa coefficient. The acquired result exceeded a value of 0.91, which showed measurement repeatability of over 91%, reflecting high reliability and agreement of the measurements.
PARTICIPANTS:
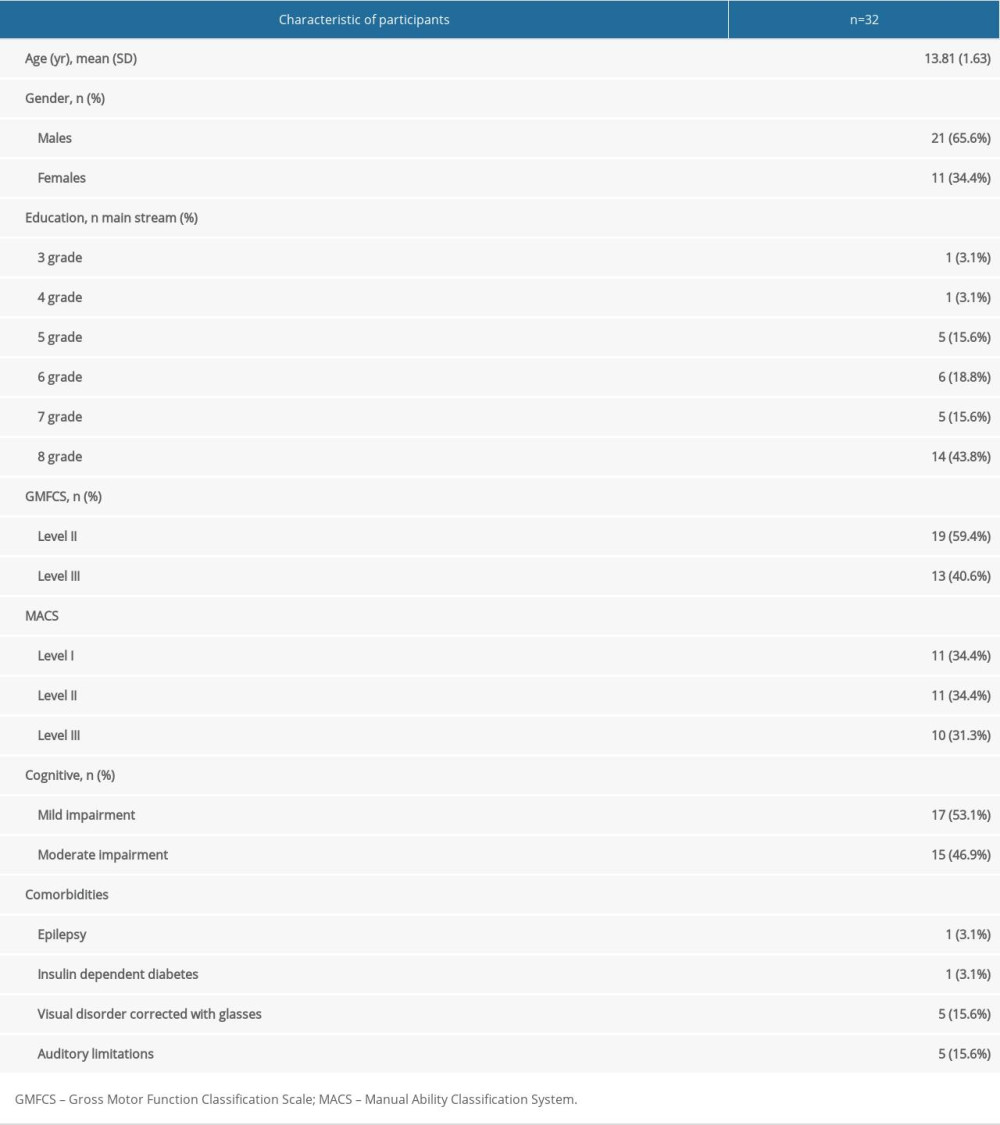
The study group comprised 32 children with spastic diplegia cerebral palsy, and mild to moderate intellectual disability, presenting GMFCS level II–III. Table 1 presents the characteristics of the study group.
INTERVENTION:
The therapy was conducted for 6 months, with 45-minute sessions taking place 5 times per week; the program included individual therapy based on NDT/Bobath and PNF methods (4 times per week) and sensory integration therapy (once a week) (Table 2). The sessions were designed specifically for each participant and aimed to improve motor functions, balance, gait, fine motor skills, and performance in activities of daily living, and to develop the spatial and body schema orientation by stimulating the senses (touch, proprioception). The sessions were held in a therapy room at the facility. No therapy session had to be ended earlier, and no undesired incidents occurred.
OUTCOME MEASURES:
The assessment, based on International Classification of Functioning, Disability and Health (ICF) and taking into account the 3 components – body functions, activity and participation – was carried out with the use of the tools which have been validated and recommended for use in research studies [24,32–37]. All the tests were applied in conformity with the instructions for the questionnaires and tests, described below, by certified therapists authorized to perform them.
SAMPLE SIZE:
The minimum sample size for the population investigated was determined using a sample size calculator (“PLUS module” from Statistica 13.3 software), taking into account the number of children with spastic diplegia CP attending the special educational facility in the Podkarpackie Region, Poland. A fraction size of 0.8 was used, with a maximum error of 5%, and a 95% confidence level, and a sample size of 30 patients was obtained. The study involved 32 children. The following formula was applied to determine the minimum sample size:
STATISTICAL ANALYSIS:
The research material was subjected to statistical analyses using Statistica 13.1. Non-parametric tests were applied in analyses of the variables and the values. This type of testing was performed due to the failure to achieve primary assumptions of parametric tests, ie, compatibility of the distributions of the relevant variables with the normal distributions, which were examined and verified using the Shapiro-Wilk W test. For most of the numerical variables, the following descriptive statistics were calculated: arithmetic mean, minimum, maximum, standard deviation, median, and 1st and the 3rd quartile. The statistical interpretation of the evaluations in the 3 consecutive periods was verified using non-parametric Friedman’s ANOVA. Because a statistically significant disproportion was identified, a subsequent post hoc test was run; in the case of Friedman’s ANOVA, it was Dunn’s test. It confirmed or contradicted the presence of statistically significant disparities between the results of the consecutive measurements. The Mann-Whitney U test was applied to assess the typically differentiated numerical characteristics of the 2 populations. To interpret the differences in the statistical level of a numerical characteristic in more than 2 populations, the Kruskal-Wallis ANOVA was applied. In this case, multiple comparisons were run as the post hoc test. The relationship of 2 unknowns failing to meet normal distribution criteria was assessed using Spearman’s rank correlation coefficient. Kappa coefficient was applied to assess agreement among 3 measurements performed by the examiner. Statistical significance was assumed for
Results
STUDY PARTICIPANTS:
The study group included 11 (34.4%) girls and 21 (65.6%) boys diagnosed with spastic diplegia CP and mild to moderate intellectual disability, ranging in age from 9 to 16 years (13.81 years±1.64 month), participating in a rehabilitation program carried out in a special educational facility. All the children were in primary school, most in the 8th grade (14 [43.8%]), and decreasing numbers were in the lower grades. Assessment with GMFCS showed that 19 children (59.4%) were at Level II, and 13 (40.6%) were at Level III. MACS Level I and II each were identified in 11 children (34.4%), while 10 (31.3%) children were at Level III. Mild and moderate intellectual disability was identified in 17 (53.1%) and in 15 (46.9%) children, respectively (Table 1).
CHANGES IN THE FUNCTIONAL PERFORMANCE AT THE END OF TREATMENT AND 2 MONTHS LATER:
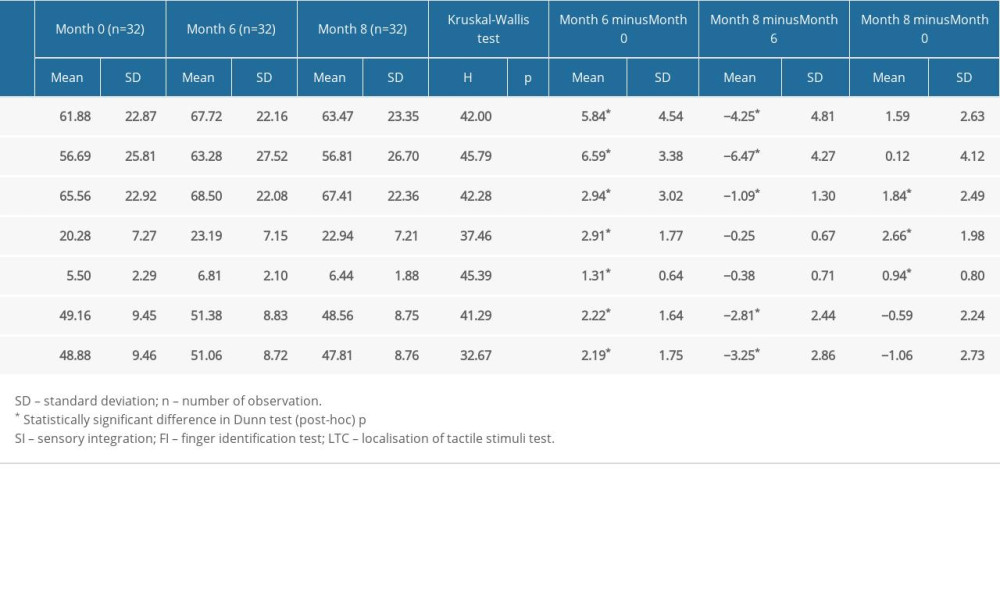
The results in all the scales and functional tests applied in the consecutive measurements, ie, before the rehabilitation – Month 0, immediately after the 6-month therapy – Month 6, and at the end of the two-month period with no therapy, ie, 8 months after the baseline measurement – Month 8, were examined using Kruskal-Wallis ANOVA test, which showed the scores were not equal (
RESULTS FOR BARTHEL INDEX, GMFM AS WELL AS BOX AND BLOCK (MONTH 0, MONTH 6, MONTH 8):
The interpretation of post hoc test results for Barthel Index, GMFM, as well as Box and Block for the right and the left limb was uniform. A statistically significant change was observed in the results measured immediately after the 6-month therapy, compared to Month 0 and the change was associated with improvement in the scores obtained by the children in the consecutive scales/functional test (the difference: Month 6 minus Month 0). Furthermore, the abovementioned tests showed a statistically significant change in the results achieved by the children in the measurement at the end of the 2-month period with no therapy relative to the measurement performed immediately after the 6-month therapy. This time the change was negative. This means that the 2-month break in the therapy resulted in a significant deterioration of the scores identified immediately after the therapy (Month 8 vs Month 6). In the case of these tests, no differences were found between Month 0 and Month 8 measurements. This means that the results in Month 8 did not differ from the baseline identified before the therapy, which shows that because the rehabilitation was discontinued (the period between Month 8 and Month 6), the children’s functional status was the same as before the therapy (Table 2).
RESULTS FOR SI TESTS (MONTH 0, MONTH 6, MONTH 8):
The interpretation for 2 other tests, ie, SI (FI and LTC) was also uniform. This time there were statistically significant changes in the results obtained by the children in the measurement immediately after the 6-month therapy relative to the baseline (Month 6 minus Month 0) and in the scores identified at the end of the 2-month period with no therapy relative to the baseline (Month 8 minus Month 0). No significant differences were found between the scores obtained by the children immediately after the 6-month therapy and at the end of the 2-month period with no therapy (Month 8 vs Month 6). This means that the scores in SI tests reflected a statistically significant improvement achieved by the children immediately after the therapy and that this effect was maintained in the measurement 2 months after the therapy ended. Despite a slight decrease, the scores were still significantly higher compared to the baseline (Table 2).
RESULTS FOR PEDI TEST (MONTH 0, MONTH 6, MONTH 8):
Finally, the scores in PEDI test were significantly improved immediately after the 6-month therapy relative to the baseline (Month 6 minus Month 0), and subsequently there was a significant decrease in the scores identified at the end of the two-month period with no therapy relative to the results identified in measurements immediately after the 6-month therapy (Month 8 minus Month 6). Although the latter decrease was significant, it was lower than the previous increase (ie, improvement identified immediately after the therapy relative to the baseline). Hence, despite this significant decrease, the children’s scores were still significantly higher than those identified at the baseline (Month 8 vs Month 0), Table 3.
RELATIONSHIP BETWEEN THE EFFECT OF THERAPY AND SEX, AGE, OR COEXISTING CONDITIONS:
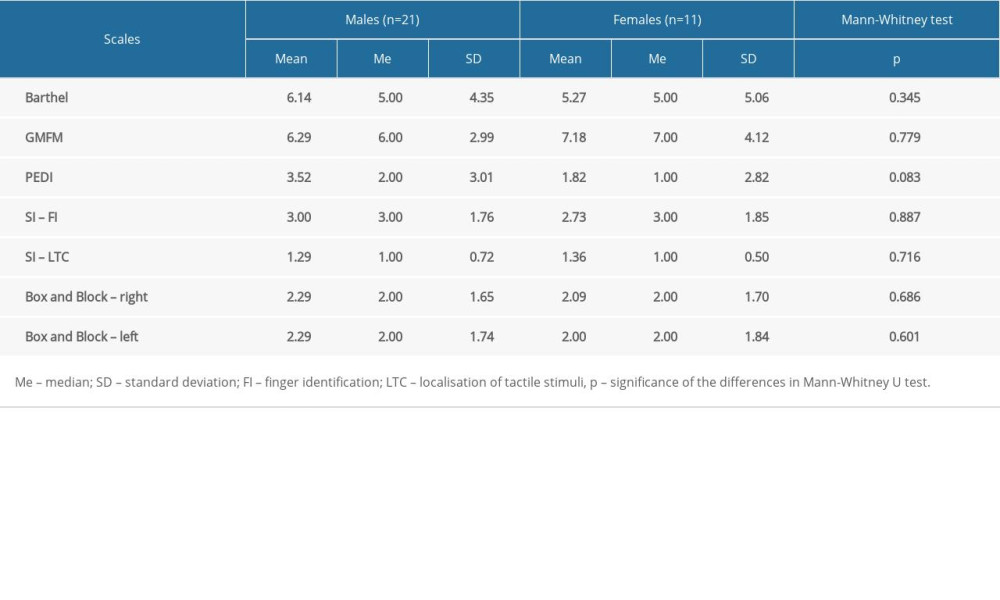
The effects of therapy were not related to the children’s sex (P>0.05) –Table 4.
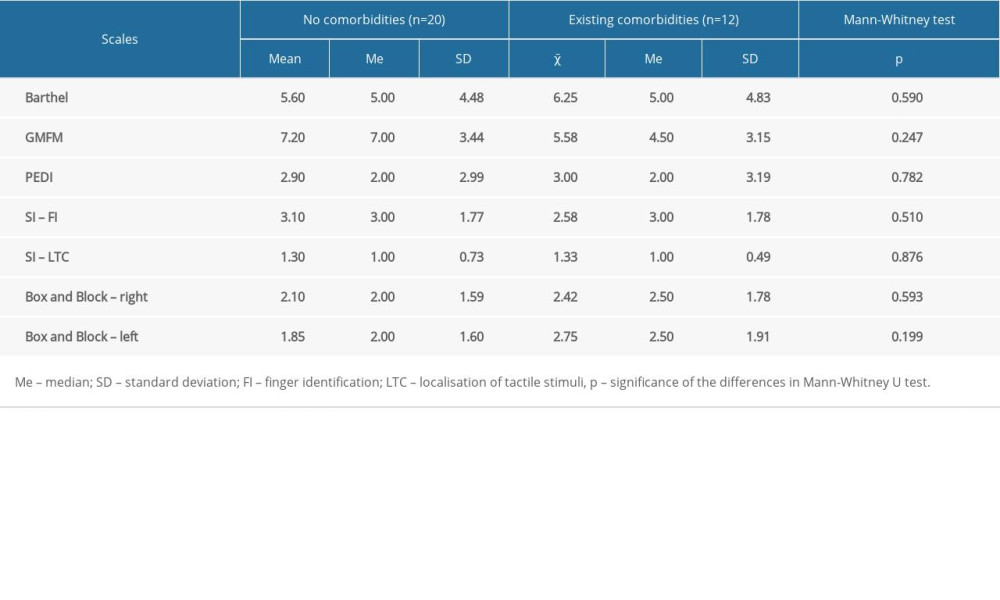
The effects of the therapy did not differ between children with and without comorbidities (P>0.05) – Table 5.
The effect of the therapy was not related to the children’s age – Table 6.
Discussion
The aim of the study was to assess changes in the functional performance of children with spastic diplegia CP at the end of treatment and 2 months later, in addition to investigating whether the effect of therapy is related to sex, age, and coexisting conditions. The findings of the present study show that immediately after the 6-month therapy program children with CP showed significant improvement in manual, motor and sensory capacities and in essential as well as complex activities of daily living. Later, following a 2-month period with no therapy, the children’s functional performance deteriorated significantly as reflected by all the measures, except for the sensory capacities: tactile perception and spatial orientation. Additionally, the findings do not support the hypothesis that the effect of therapy the children with spastic diplegia CP is related to their sex, age, or comorbidities.
The rehabilitation program applied in the current study was based on a combination of NDT/Bobath, PNF, and SI therapies. The results identified immediately after the 6-month therapy showed a considerable improvement in the children, reflected by all the measures. We assume that one of the mechanisms potentially contributing to improvement in functional performance in the participants involves neuroplastic changes induced by intensive motor training [38,39]. Another mechanism positively affecting functional performance is linked to physical training, which leads to strengthening of muscles as a result of neuromuscular adaptation [40]. This is consistent with other studies which reported improvement in motor capacities in children with diplegia regularly participating in physical training [41–43]. In the present study, the effects of rehabilitation were assessed using the following research tools: GMFM, PEDI, Index Barthel Box and Block, and Southern California Sensory Integration tests. In a study by Knox et al, effectiveness of Bobath therapy applied to 15 children with CP was assessed using GMFM and PEDI questionnaires. After a 6-week rehabilitation program, improvement was achieved by all the subjects in motor abilities and self-care skills [44]. Shamsoddini and Hollisaz assessed the effect of SI therapy on gross motor skills of children with CP. The 12-week therapy results were assessed with GMFM. The authors concluded that sensory integration and vestibular stimulation produced positive results in children with CP [45]. The present findings also show satisfying results of SI therapy. The analyses showed improved sensory integration in the children with CP; the effect was identified immediately after the 6-month rehabilitation and retained at a similar level after 2-month period with no therapy.
However, the current findings show that 2 months after the therapy was discontinued there was a significant decrease in the scores, compared to those identified immediately after the therapy, with an exception of the scores in Localisation of tactile stimuli test and Finger identification test. These findings of our study may be linked to the persistent primary impairments resulting from the damage to the central nervous system (eg, muscle spasticity) [46]. It appears that effects of therapy in children with spastic diplegia CP deteriorate rapidly due to increased muscle tightness if treatment is not provided on a regular basis. Lack of exercise frequently leads to mechanical changes in muscles and tendons, reduced range of motion in joints (ie, contractures) and bone deformities [27–29]. Effects produced by lack of physical activity in individuals with CP also include decreased muscle strength, which adversely affects performance of motor tasks, such as walking or climbing stairs [24–30]. It is likely that the above observations explain our findings proving the hypothesis, which says that a 2-month period with no therapy will negatively affect functional performance of children with spastic diplegia CP. Hence, it can be argued that well-targeted continuous and systematic therapy alleviates secondary problems, allowing patients to maintain normal motor functions which lead to independent mobility of children with spastic diplegia CP, and this fact should be taken into account by those designing therapeutic programs in facilities providing treatment to this population of children.
The current findings do not prove the hypothesis about the relationship between age, sex or comorbidities and effects of therapy. This may be linked with the fact that the groups, which were compared, were not equal in size. There were significantly more boys than girls (21 vs 11) in our study group and more children without comorbidities such as epilepsy, diabetes, visual disorder, or auditory limitations (20 vs 12). Therefore, the related research should be continued in equal-size groups representing the specific characteristics, because it seems that children’s age may indeed considerably impact therapy effects. This is associated with the specificity of problems experienced at different stages of development, and affecting individuals’ ability to acquire certain skills or improve certain functions, eg, the delayed development of balance, postural control and selective motor control in younger children with CP versus more advanced soft tissue contractures and deformities in joints in adolescents with CP [46]. It has also been reported that comorbidities can lead to reduced level of activity and poorer quality of life in subjects with CP [46–48].
To recapitulate the above observations and the present findings and to ensure the best quality of treatment and the most beneficial effects of therapy for the child, it is necessary to perform detailed and accurate functional assessment of the child, by using tests and scales tailored to and designed for patients with CP. As a result, therapists can adjust the treatment specifically to an individual patient, taking into account his/her capabilities and limitations. Various therapeutic methods have been shown to produce significant changes in fine and gross motor skills. In the related literature it is difficult to find studies focusing on long-term effects of therapies applied to children with CP. The current findings show that at the end of the 6-month therapy, the children’s functional performance was improved, which was reflected by all the outcome measures. However, the acquired skills were not retained after the 2-month period with no therapy, as shown by the measurements performed using GMFM, PEDI, Box and Block, and Index Barthel. Hence, to decrease a risk of regression in their functional performance it is necessary to reinforce effects of therapy by ensuring continuous and systematic rehabilitation of children with CP. On the other hand, the assessments carried out using SI tests showed that the effects of the 6-month therapy were sustained at a similar level 2 months after the program ended. This suggests that therapy focusing on sensory functions such as tactile perception, somatognosis, and spatial orientation could be included as a permanent component of rehabilitation programs in day care centers providing treatments to children with CP.
There are certain limitations of the study. Considering that the study sample was based on the population of a specific educational center that works with a certain rehabilitation technique and that the participants had a specific type of CP (ie, spastic diplegia CP), these findings cannot be easily applied to other settings and do not represent all individuals with CP. Therefore, further research concerning other types of CP and rehabilitation techniques are required. In accordance with the design of the current study, there was no control group, which would have enabled a comparative analysis. This limitation is linked with the fact that all children in this particular day care center receive rehabilitation, so we could not select a control group of subjects receiving no therapy. We are aware that this is a considerable weakness of the study, but, to partly compensate for this limitation, we performed the third examination (a follow-up) 2 months after therapy, which enabled assessment of the long-term effects of rehabilitation. It is necessary to continue research focusing on assessment of functional performance relative to the duration, type, and intensity of therapy provided to children with CP which would take into account a control group. The small sample size is the next limitation of this study. However, the sample size calculation process that was carried out showed that our sample of participants was adequately powered for the feasibility study. Moreover, the present study was continued for a relatively short time (8 months only); further research should be designed to monitor therapy effects during a longer period of time.
Despite these limitations, the study also presents some strengths. This was an observational study focusing on a uniform group of subjects presenting similar characteristics at baseline. Furthermore, all the study participants received treatment from the same physiotherapist and were then assessed by one examiner who performed 3 measurements at different time points to assess the long-term effects of the therapy. Rater calibration was performed and showed good reliability of the measurements performed by the examiner. Furthermore, the rehabilitation program applied in the current study was based on multi-targeted approach combining NDT/Bobath, PNF, and SI therapies (detailed description of the therapies is included in Table 2). All the above factors suggest that the outcome of this study can be applied to other settings. As for the functional implications of this study, the findings may be of importance for clinical practice as they support the evidence showing that a lack of systematic therapy provided to children with CP adversely affects their functional capacities, and this fact should be taken into account by those designing therapeutic programs in facilities providing treatment to this population of children.
Conclusions
Considering the limitations of the present study, the following conclusions can be made. Immediately after the 6-month therapy program the children with CP showed significant improvement in manual, motor, and sensory capacities and in essential as well as complex activities of daily living. Later, following a 2-month period with no therapy, the children’s functional performance deteriorated significantly as reflected by all the measures, except for the sensory capacities: tactile perception and spatial orientation. This suggests that therapy focusing on functional performance could be included as a permanent component of rehabilitation programs in day care centers providing treatments to children with CP. As regards the broader implications of this study, the findings may be of importance for clinical practice since they show it is necessary to provide continuous and systematic therapy to children with CP in order to reduce a risk of regression in their functional capacities. This information may be helpful for therapists working in day care facilities, and for parents/guardians planning effective therapy of children with CP, and it should be taken into account by those designing therapeutic programs in facilities providing treatment to this population of children. Effectiveness of the 6-month therapy program in children with CP was not related to their age, sex, or comorbidities.


References
1. Gomulska K, Sadowska L, Krefft A, Early prognostication of the development of infantile cerebral palsy (ICP) in the aspect of synthetic analysis of risk factors: Eur J Clin Exp Med, 2006; 4(1); 47-58
2. Jóźwiak S, Neurological basis of motor deficits in Cerebral Palsy: Ortop Traumatol Rehabil, 2001; 3(4); 472-75
3. Bailes AF, Greve K, Schmitt LC, Changes in two children with cerebral palsy after intensive suit therapy: A case report: Pediatr Phys Ther, 2010; 22(1); 76-85
4. Christy JB, Saleem N, Turner PH, Wilson J, Parent and therapist perceptions of an intense model of physical therapy: Pediatr Phys Ther, 2010; 22(2); 207-13
5. Ryan JM, Cassidy EE, Noorduyn SG, O’Connell NE, Exercise interventions for cerebral palsy: Cochrane Database Syst Rev, 2017; 6(6); CD011660
6. Gillett JG, Lichtwark GA, Boyd RN, Barber LA, FAST CP: Protocol of a randomised controlled trial of the efficacy of a 12-week combined Functional Anaerobic and Strength Training programme on muscle properties and mechanical gait deficiencies in adolescents and young adults with spastic-type cerebral palsy, 2015; 5(6); e008059 [published correction appears in BMJ Open. 2015;5(7):e008059corr1]
7. Novak I, McIntyre S, Morgan C, A systematic review of interventions for children with cerebral palsy: state of the evidence: Dev Med Child Neurol, 2013; 55(10); 885-910
8. Nusselder WJ, Looman CW, Mackenbach JP, Nondisease factors affected trajectories of disability in a prospective study: J Clin Epidemiol, 2005; 58(5); 484-94
9. James S, Ziviani J, Ware RS, Boyd RN, Randomized controlled trial of web-based multimodal therapy for unilateral cerebral palsy to improve occupational performance: Dev Med Child Neurol, 2015; 57(6); 530-38
10. Mitchell LE, Ziviani J, Boyd RN, A randomized controlled trial of web-based training to increase activity in children with cerebral palsy: Dev Med Child Neurol, 2016; 58(7); 767-73
11. Olama KA, Endurance exercises versus treadmill training in improving muscle strength and functional activities in hemiparetic cerebral palsy: The Egyptian Journal of Medical Human Genetics, 2011; 12(2); 193-99
12. Jung JW, Her JG, Ko J, Effect of strength training of ankle plantarflexors on selective voluntary motor control, gait parameters, and Gross Motor Function of children with cerebral palsy: J Phys Ther Sci, 2013; 25; 1259-63
13. Mattern-Baxter K, McNeil S, Mansoor JK, Effects of home-based locomotor treadmill training on gross motor function in young children with cerebral palsy: A quasi-randomized controlled trial: Arch Phys Med Rehabil, 2013; 94(11); 2061-67
14. Aisen ML, Kerkovich D, Mast J, Cerebral palsy: Clinical care and neurological rehabilitation: Lancet Neurol, 2011; 10(9); 844-52
15. Anttila H, Autti-Rämö I, Suoranta J, Effectiveness of physical therapy interventions for children with cerebral palsy: A systematic review: BMC Pediatr, 2008; 8; 14
16. Dean E, Cerebral palsy: Nurs Child Young People, 2017; 29(3); 11
17. Ko J, Sensitivity to functional improvements of GMFM-88, GMFM-66, and PEDI mobility scores in young children with cerebral palsy: Percept Mot Skills, 2014; 119(1); 305-19
18. Czochowska M, Zgorzalewicz-Stachowiak M, Sereda-Wiszowaty E, The impact of selected factors on the effectiveness of NDT-Bobath in improving children with cerebral palsy: Physiotherapy, 2008; 16(3); 8-24
19. Bagnowska K, Falkowski M, Selected methods of improving children with cerebral palsy: Publishing House New Pediatrics, 2013; 119-20
20. Wood E, Rosenbaum P, The gross motor function classification system for cerebral palsy: A study of reliability and stability over time: Dev Med Child Neurol, 2000; 42; 292-96
21. Gajewska E, Diagnostic instruments for assessing early motor development in child physiotherapy: ChildNeurol, 2011; 20(40); 55-58
22. Michalska A, Wendrorff J, Functional classification systems in cerebral palsy – Communication Function Classification System: Child Neurol, 2014; 23(46); 35-38
23. Kontson K, Marcus I, Myklebust B, Civillico E, Targeted box and blocks test: Normative data and comparison to standard tests: PLOS One, 2017; 12(5); e0177965
24. Gunel MK, Mutlu A, Tarsuslu T, Livanelioglu A, Relationship among the Manual Ability Classification System (MACS), the Gross Motor Function Classification System (GMFCS), and the functional status (WeeFIM) in children with spastic cerebral palsy: Eur J Pediatr, 2009; 168(4); 477-85
25. Scholtes VA, Becher JG, Comuth A, Effectiveness of functional progressive resistance exercise strength training on muscle strength and mobility in children with cerebral palsy: A randomized controlled trial: Dev Med Child Neurol, 2010; 52(6); e107-13
26. Scholtes VA, Becher JG, Janssen-Potten YJ, Effectiveness of functional progressive resistance exercise training on walking ability in children with cerebral palsy: A randomized controlled trial: Res Dev Disabil, 2012; 33(1); 181-88
27. Bania TA, Dodd KJ, Baker RJ, The effects of progressive resistance training on daily physical activity in young people with cerebral palsy: A randomised controlled trial: Disabil Rehabil, 2016; 38(7); 620-26
28. Park EY, Kim WH, Meta-analysis of the effect of strengthening interventions in individuals with cerebral palsy: Res Dev Disabil, 2014; 35(2); 239-49
29. Park EY, Kim WH, Structural equation modeling of motor impairment, gross motor function, and the functional outcome in children with cerebral palsy: Res Dev Disabil, 2013; 34(5); 1731-39
30. Peterson MD, Ryan JM, Hurvitz EA, Mahmoudi E, Chronic conditions in adults with cerebral palsy: JAMA, 2015; 314(21); 2303-5
31. Mathiowetz V, Volland G, Kashman N, Weber K, Adult norms for the Box and Block Test of manual dexterity: Am J Occup Ther, 1985; 39(6); 386-91
32. Palisano RJ, Rosenbaum P, Bartlett D, Livingston MH, Content validity of the expanded and revised Gross Motor Function Classification System: Dev Med Child Neurol, 2008; 50(10); 744-50
33. Ayres JA: Southern California Sensory Integration Tests, 2012; 15-18, Warsaw, Polish Association of Sensory Integration Therapists
34. May-Benson TA, Roley SS, Mailloux Z, Interrater reliability and discriminative validity of the structural elements of the Ayres Sensory Integration Fidelity Measure: Am J Occup Ther, 2014; 68(5); 506-13
35. Mahoney FI, Barthel DW, Functional evaluation: The Barthel Index: Stan Md Med J, 1965; 14; 61-65
36. Kramer JM, Schwartz AE, Davies DK, Usability and reliability of an accessible Patient-Reported Outcome Measure (PROM) software: The Pediatric Evaluation of Disability Inventory-Patient-Reported Outcome (PEDI-PRO): Am J Occup Ther, 2021; 75(1); 7501205010p1-10
37. Dietvorst M, van de Kerkhof TM, Janssen RPA, Translation and transcultural validation of the Dutch hospital for special surgery paediatric functional activity brief scale (HSS Pedi-FABS): BMC Musculoskelet Disord, 2021; 22(1); 853
38. Harvey A, Robin J, Morris ME, A systematic review of measures of activity limitation for children with cerebral palsy: Dev Med Child Neurol, 2008; 50(3); 190-98
39. Juenger H, Linder-Lucht M, Walther M, Cortical neuromodulation by constraint-induced movement therapy in congenital hemiparesis: An FMRI study: Neuropediatrics, 2007; 38(3); 130-36
40. Bleyenheuft Y, Dricot L, Gilis N, Capturing neuroplastic changes after bimanual intensive rehabilitation in children with unilateral spastic cerebral palsy: A combined DTI, TMS and fMRI pilot study: Res Dev Disabil, 2015; 43–44; 136-49
41. Moreau NG, Holthaus K, Marlow N, Differential adaptations of muscle architecture to high-velocity versus traditional strength training in cerebral palsy: Neurorehabil Neural Repair, 2013; 27(4); 325-34
42. Pandey DP, Tyagi V, Effect of functional strength training on functional motor performance in young children with cerebral palsy: Indian Journal of Physiotherapy and Occupational Therapy, 2011; 5(1); 52-55
43. Nsenga AL, Shephard RJ, Ahmaidi S, Aerobic training in children with cerebral palsy: Int J Sports Med, 2013; 34(6); 533-37 [published correction appears in Int J Sports Med. 2013;34(7):667]
44. Knox V, Evans AL, Evaluation of the functional effects of a course of Bobath therapy in children with cerebral palsy: A preliminary study: Dev Med Child Neurol, 2002; 44(7); 447-60
45. Shamsoddini AR, Hollisaz MT, Effect of sensory integration therapy on gross motor function in children with cerebral palsy: Iran J Child Neurology, 2009; 3; 43-48
46. Nooijen C, Slaman J, van der Slot W, Health-related physical fitness of ambulatory adolescents and young adults with spastic cerebral palsy: J Rehabil Med, 2014; 46(7); 642-47
47. Nieuwenhuijsen C, van der Slot WM, Dallmeijer AJ, Physical fitness, everyday physical activity, and fatigue in ambulatory adults with bilateral spastic cerebral palsy: Scand J Med Sci Sports, 2011; 21(4); 535-42
48. Schroeder AS, Homburg M, Warken B, Prospective controlled cohort study to evaluate changes of function, activity and participation in patients with bilateral spastic cerebral palsy after Robot-enhanced repetitive treadmill therapy: Eur J Paediatr Neurol, 2014; 18(4); 502-10
In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387