11 August 2022: Clinical Research
Surgical Management of 48 Patients with Retrosternal Goiter and Tracheal Stenosis: A Retrospective Clinical Study from a Single Surgical Center
Tao Zuo1234ADEFG, Zhaoming Gao5346BC, Zhiguo Chen2BC, Bin Wen53BC, Baojun Chen2CDF, Zhenfa Zhang534ADEF*DOI: 10.12659/MSM.936637
Med Sci Monit 2022; 28:e936637






Abstract
BACKGROUND: Benign retrosternal thyroid goiters can become large enough to compress the trachea and result in tracheomalacia and stenosis. This retrospective study from a single surgical center aimed to study the surgical management of 48 patients with retrosternal goiter and tracheal stenosis diagnosed and treated from January 2017 to December 2021.
MATERIAL AND METHODS: All preoperative contrast-enhanced CT scans showed retrosternal goiter and tracheal stenosis. RG was classified into type I in 28 patients, type II in 12 patients, and type III in 8 patients. TS was classified into grade I in 31 patients, grade II in 11 patients, and grade III in 6 patients. All patients were referred for surgery. Clinicopathologic features and surgical outcomes were recorded.
RESULTS: All operations were successfully performed. There were 41 patients with transcervical incision, 4 with cervical incision+sternotomy, 2 with cervical incision and thoracoscopic surgery, and 1 with cervical incision and surgery via the subxiphoid approach. Two patients presented recurrent laryngeal nerve injury. One patient showed short-term hand and foot numbness. The patients were pathologically diagnosed as simple nodular goiter (n=27), nodular goiter combined with cystic change (n=6), adenomatous nodular goiter (n=10), and thyroid adenoma (n=5). There was no prominent tumor recurrence or gradual TS remission.
CONCLUSIONS: This study has highlighted that patients with retrosternal goiter and tracheal stenosis may have comorbidities and require a multidisciplinary approach to management. The choice of anesthesia, surgical approach, and maintenance of the airway during and after surgery should be individualized.
Keywords: Thoracic Surgery, tracheal stenosis, Goiter, Substernal, Goiter, Nodular, Humans, Thyroidectomy
Background
Retrosternal goiter (RG) is defined as an enlarged thyroid gland extending downwards, with over 50% below the sternal notch, or the lower pole is greater than 3 cm below the suprasternal notch [1]. It can cause displacement and narrowing of great vessels and trachea in the neck, leading to high difficulty and risk of surgery and many complications [2].
According to the chest X-ray and computed tomography (CT) images and clinical signs of RG extending into the sternum, it can be divided into 3 types [2]: type I, after over half of the cervical goiter enters the sternum, the lower pole reaches the superior margin of the aortic arch (Figure 1A); type II, the goiter is almost entirely posterior to the sternum, with the lower pole behind the aortic arch or entering the postmediastinum (Figure 1B); and type III, a huge intrathoracic goiter protrudes into the thorax, which may be accompanied by superior vena cava compression syndrome (Figure 1C). Based on the range of involvement, it can be divided into limited type and diffuse type.
Although cervical goiters are easily recognized, the initial presentation of mainly substernal goiters may be unusual [3]. RG is occasionally detected by chest X-ray or CT scanning, or obstructive symptoms such as dyspnea, asthma, or coughing. The most common obstructive symptom is exertional dyspnea [4] caused by a retrosternal goiter and tracheal stenosis. In RG patients, the enlarged thyroid compresses the trachea for a long time, resulting in insufficient local blood supply and loss of elasticity of the fibrous tracheal ring, which causes cartilage degeneration and atrophy [5]. As a consequence of tracheal compression and tracheomalacia, concurrent upper respiratory infections may lead to acute respiratory failure during the perioperative period [5]. The size of the goiter was reported to be positively correlated with the degree of compression of the trachea [6].
The current classification of tracheal stenosis (TS) is based on the classification system of subglottic TS. The Cotton-Myer classification system is based on endoscopic estimates of the airspace cross-sectional area (CSA) at the subglottis and classifies obstruction severity as follows: grade I stenosis, less than 50% obstruction(Figure 2A); grade II stenosis, 51% to 70% obstruction (Figure 2B); grade III stenosis, 71% to 99% obstruction (Figure 2C); and grade IV stenosis, no detectable lumen or complete stenosis [7]. In retrosternal goiter and tracheal stenosis, grade I TS is defined as mild, grade II as moderate, and grades III and IV as severe. Airway obstruction in retrosternal goiter and tracheal stenosis can occur as a result of acute intracapsular hemorrhage of tumors, anesthesia induction, extubation, surgical resection, or simple body position change. Severe obstruction and complications are the major causes of death in such patients. The Surgical Affairs Committee of the American Thyroid Association recommend surgical management for goiters with compressive symptoms [4]. Careful preoperative testing, thoughtful consideration of the type of anesthesia (intravenous induction of muscle relaxant using laryngoscopy or Glidescope), and planning the extent of surgery and postoperative care are necessary to achieve optimal results [4,8]. Intravenous induction of muscle relaxant using laryngoscopy or Glidescope is feasible in patients with massive benign retrosternal goiters.
Therefore, this retrospective study from a single surgical center aimed to study the surgical management of 48 patients with retrosternal goiter and tracheal stenosis diagnosed and treated from January 2017 to December 2021.
Material and Methods
ETHICAL STATEMENT:
The study was conducted in accordance with the Declaration of Helsinki. Ethics approval was obtained from Ethics Committee of the Central Hospital of Wuhan, Tongji Medical College, Huazhong University of Science and Technology, and written informed consent for participation was obtained from the patients. A copy of the written consent is available for review from the Editor of this journal.
PATIENT SELECTION:
This retrospective study from a single surgical center aimed to study the surgical management of 48 consecutive patients with retrosternal goiter and tracheal stenosis diagnosed and treated from January 2017 to December 2021. There was no control group in this study. Inclusion criteria were: retrosternal goiter and tracheal stenosis in CT images, age <80 years, no obvious cardiopulmonary diseases, no serious complications, and signed consent for surgery. Exclusion criteria were: thyroid malignant tumor with systemic metastasis or incomplete resection; patients with systemic conditions who could not tolerate surgery (eg, cardiopulmonary dysfunction, shock, cachexia), and lack of consent.
IMAGING DIAGNOSIS:
All patients underwent enhanced CT examination (Shanghai United Imaging Healthcare Co., Ltd, Shanghai, China) of the neck and chest before surgery with plain scan and triphasic scan, including 3 phases: arterial, venous, and delayed with 3D reconstruction. The types and grades were determined by evaluation of CT images.
HISTOPATHOLOGY DIAGNOSIS:
All the pathological sections were independently reviewed by more than 2 intermediate-level pathologists, and the pathological diagnosis was reviewed and released by senior-level pathologists.
ANESTHESIA: The intubation method was selected according to the condition of TS [8]. The patients with grade I TS were treated with routine single-lumen intubation or non-intubated surgery with spontaneous respiration. In patients with grade II TS, appropriate intubation was selected according to the inner diameter of the stenosis. The patients with grade III TS underwent bronchoscopy (Olympus Corporation, Tokyo, Japan)-guided transoral endotracheal intubation in conscious state. Non-intubated surgery with spontaneous respiration was performed after tracheal stent (Boston Scientific Corporation, Natick, USA) implantation.
SURGICAL PROCEDURE: The skin was separated along the deep layer of the platysma myoides, and the muscle layer was cut open along the linea alba cervicalis. The strap muscle on 1 side was cut off based on actual condition. The sternocleidomastoid was separated and pulled outwards to expose the thyroid. The middle thyroid vein was treated first, and then the upper pole of the gland was dissociated and the superior thyroid artery, superior vein, and suspensory ligament were ligated. For large masses, the isthmus of the thyroid was cut off first to separate the thyroid from the trachea. Next, blunt dissection was performed with fingers along the mass envelope, and the tumor was gradually dragged to the neck. In large masses that were difficult to drag to the neck, the isthmus was firstly cut off, then the thyroid was dissociated, the recurrent laryngeal nerve was dissected, and the mass was resected together with the thyroid lobe [2]. For cystic masses, the liquid in the capsule was extracted first to reduce the volume for easier removal. After surgery, the TS site was assessed for softness. In case of severe tracheomalacia, tracheal suspension was conducted. Median sternotomy was carried out if the mass could not be removed or if TS and tracheal softening could not be treated via the cervical incision. A longitudinal midline skin incision was made in the chest, and the sternum was split lengthwise in the middle to expose the superior mediastinal vessels and mass. The major surrounding blood vessels and nerves were carefully separated from the mass, and the tumor was completely resected. After sufficient hemostasis, the local pleural damage was repaired by suturing, a indwelling negative-pressure drainage tube was placed, and the incision was closed.
POSTOPERATIVE MULTIDISCIPLINARY MANAGEMENT:
Patients with retrosternal goiter and tracheal stenosis often have a variety of perioperative comorbidities and complications, and it is necessary to have a full multidisciplinary team in place, including specialists in thoracic surgery, thyroid surgery, otolaryngology, anesthesiology, endocrinology, radiology, pathology, cardiology, vascular surgery, gastroenterology, intensive care, and nursing coordination. After surgery, respiration and serum calcium concentration were closely observed. In patients with nodular goiter and thyroid cancer, dry thyroxine preparation (Merck KGaA, Darmstadt, Germany) was orally administered after surgery. For the former, medication was adjusted according to triiodothyronine (T3), thyroxine (T4), and thyroid-stimulating hormone (TSH) monitoring until drug withdrawal. One month after airway stent implantation, the stent was removed under endoscopy.
DATA ANALYSIS:
We performed the statistical analysis using commercially available statistical software – IBM SPSS Statistics software version 20.0 (IBM Corp., Armonk, NY, USA).
Results
PATIENT SELECTION:
The clinical data of 48 patients with retrosternal goiter and tracheal stenosis treated by thoracic surgery and thyroid surgery from January 2017 to December 2021 were retrospectively analyzed (Table 1). Among them, there were 10 males and 38 females, ages 42–76 years (median age: 50). Their clinical manifestations included asymptomatic neck mass (n=22), chest tightness and coughing (n=15), swallowing obstruction (n=6), and dyspnea (n=5). One patient received tracheal stent implantation before surgery, and 4 had a history of thyroid surgery. Masses of different degrees were observed in 41 patients, and obvious tracheal deviation was found in 8 patients.
IMAGING DIAGNOSIS:
All preoperative contrast-enhanced CT scans showed retrosternal goiter and tracheal stenosis. Among them, 27 patients had cystic thyroid masses and 21 had solid masses. In 2 patients, the masses dropped into the postmediastinum. RG was classified into type I in 28 patients, type II in 12 patients, and type III in 8 patients. TS was classified as grade I in 31 patients, grade II in 11 patients, and grade III in 6 patients (Table 1).
HISTOPATHOLOGY DIAGNOSIS:
The patients were pathologically diagnosed as having simple nodular goiter (n=27), nodular goiter combined with cystic change (n=6), adenomatous nodular goiter (n=10), and thyroid adenoma (n=5) (Table 2).
SURGICAL MANAGEMENT:
There were no deaths during surgery or hospitalization, or intraoperative or postoperative hemorrhage. Preoperative tracheal stent implantation was performed in 1 patient. There were 41 patients with transcervical incision, 4 with cervical incision+sternotomy, 2 with cervical incision+thoracoscopic surgery, and 1 with cervical incision+surgery via the subxiphoid approach (Table 2).
MULTIDISCIPLINARY MANAGEMENT:
All patients received multidisciplinary management the during perioperative period from disciplines including thoracic surgery, thyroid surgery, otolaryngology, anesthesiology, endocrinology, radiology, pathology, cardiology, vascular surgery, gastroenterology, intensive care, and nursing coordination. Two patients presented recurrent laryngeal nerve injury, and the voice was improved 3 months after surgery. One patient showed short-term hand and foot numbness, which was improved 1 month after calcium supplementation, and then the supplementation was stopped.
Outcomes
The patients were followed up for 1–48 months, revealing no prominent tumor recurrence or gradual TS remission.
Discussion
SELECTION OF ANESTHESIA METHOD:
Selection criteria include airway obstruction has existed before retrosternal goiter and tracheal stenosis surgery, and patients with severe stenosis have dyspnea. Moreover, preoperative anesthesia induction, intraoperative secretions blocking the trachea, and changes in body position may all lead to severe hypoxia and cardiac arrest. Therefore, the correct selection of anesthesia methods is helpful to improve the success rate of surgery and the postoperative quality of life.
Before surgery, anesthesiologists must understand the position (including the distance from the glottis), size and lower pole of RG, degree of tracheal compression, invasion of the inner wall of the trachea, degree of tracheomalacia, and the relationship between dyspnea and body position in detail, so as to formulate a reasonable anesthesia plan and emergency management measures. A reasonable anesthesia plan is composed of preoperative determination of the way of anesthesia induction, prudent use of sedative and analgesic drugs, and preparation of an aspirator. It is believed that awake endotracheal intubation preserves spontaneous respiration, which can greatly increase the safety of patients and reduce the occurrence of severe complications caused by endotracheal intubation failure. Bronchoscopy-guided endotracheal intubation does not require adequate head hypsokinesis, and the whole intubation process is carried out under bronchoscopic monitoring, which can enhance the safety of intubation. Emergency management measures include laryngeal mask ventilation or endotracheal tube ventilation in the upper part of the stenosis, endotracheal tube placement into the trachea under the incision for ventilation after tracheotomy, or ventilation by extending a high-frequency ventilation tube under the incision through the catheter.
APPLICATION OF NON-TRACHEAL INTUBATION:
With the progress achieved in anesthetic techniques and perioperative risk management, the application of non-tracheal intubation in video-assisted thoracic surgery (VATS) has become possible. Tracheal surgery is one of the most complex thoracic surgery procedures; it has been proved to be successful in non-intubated anesthesia with spontaneous respiration in multiple centers [10–12]. However, the risk of intraoperative anesthesia and surgery is relatively high. Moreover, experience in non-intubated surgery is limited in our center. Therefore, before non-tracheal intubation in this study, it was confirmed that the stenotic ring was located 2 cm below the glottis, the tracheomalacia test was negative, and the stenosis was grade I–II in the Cotton-Myer grading system. For patients with TS grade III or above, stent implantation under tracheoscopy can be performed first to open and stabilize the airway, followed by non-intubated surgery with spontaneous respiration.
SELECTION OF SURGICAL INCISION:
With comprehensive preoperative examination, planning and multidisciplinary evaluation, as well as intraoperative delicate operation, most RG can be safely resected through a “collar-like” cervical incision (Figure 3A). According to a previous report, more than 95% can be removed by a cervical approach [13]. In this study, 85.41% of cases underwent surgery through transcervical incision. During surgery, it is very important to tilt the head back as far as possible. In surgery via the cervical incision, our experience suggests that head hypsokinesis with shoulder padding can fully expose the surgical area. The mass can be pulled from the mediastinum to the neck by blunt dissection and delicate operation. Padding the shoulder also provides adequate preparation for possible median sternotomy. For patients complicated with cystic lesions, a cyst puncture can be performed first. After the cystic fluid is sucked out, the cyst shrinks and the space for surgical operation is enlarged. In this study, 3 patients with cystic lesions were detected. With the discharge of cystic fluid, cervical surgery is easier. Additionally, intraoperative rapid-frozen section is helpful to determine the surgical method and resection range.
However, huge tumors compress the trachea, and often compress or involve the esophagus and lung tissue, and even invade the great mediastinal vessels or nerves, thus leading to severe complications such as superior vena cava syndrome (SVCS). Intraoperative full exposure of the surgical field is critical in such patients. Especially for patients with invasion of the innominate vein, subclavian artery, and other organs in the top of the thorax, the entire thoracic and mediastinal region from the top of the thorax to the diaphragm should be exposed during surgery. If great vessels such as the innominate veins need to be replaced, the whole course of the vessels to be replaced should be exposed horizontally. Consequently, proper selection of surgical incisions is important for safe and rapid resection of such tumors and improvement in prognosis. In these cases, a transcervical incision becomes particularly important.
A cervical incision in the proper body position+median sternotomy is a common surgical method for the extra-cervical approach (Figure 3B). A median sternotomy incision is always required for cases such as the lesion exceeding the aortic arch [14], intraoperative hemorrhage [9], tumor surrounding the recurrent laryngeal nerve, and close adhesion of the surgical part [15]. Another possible cause for the transthoracic approach is a malignant thyroid tumor [16]. It has been shown that preoperative CT-based calculation of the volume of the mediastinal mass ≥162 cm3 is an important basis for extra-cervical incision, and the negative predictive value is 100% [17]. Reports also held that in the extended neck position, the goiter was located 19 mm superior to its position without neck extension [18]. An extra-cervical approach often depends on the CT scan-based depth of goiter expansion in the mediastinum and extension beyond the aortic arch [19].We also think that patients with grade III TS or type III RG may be more suitable for an extra-cervical incision. The influence of intraoperative body position on the depth of the mass into the mediastinum should be considered in the preoperative evaluation of the extra-cervical approach. Complications of median sternotomy include sternal osteomyelitis, foreign-body infection, sternal dehiscence, arrhythmias and sternal instability. In addition, median sternotomy can also lead to internal mammary vessel injury and brachial plexus traction injury, resulting in prolonged postoperative pain.
There is evidence that thyroidectomy via the cervical incision combined with video-assisted or robot-assisted thoracoscopic surgery (VATS/RATS) obtains the optimal efficacy in some locally advanced malignancies [19]. Mediastinoscopy and hemostasis can help avoid sternotomy without additional incisions in cases of mild but uncontrollable bleeding from the cervical incision [20]. Surgery via the subxiphoid approach has been confirmed to reduce intercostal nerve injury (Figure 3C). Subxiphoid single-port thymectomy needs no sternotomy, contributing to less pain. Due to no intercostal nerve injury, it provides an excellent cosmetic effect. Subxiphoid uniportal video-assisted thoracoscopic surgery may also be a solution when RG cannot be resected via a cervical incision [21].
Some scholars believe that transverse cervical and thoracic hemi-clamshell (HCS) incision is suitable for the resection of dumbbell-shaped malignant tumors in the neck and thorax [22]. The HCS approach is also an option for the sternum and goiter with malignant behavior or outward invasion. The HCS approach consists of partial sternotomy with antero-lateral thoracotomy, which can better expose the anatomical structure at the cervicothoracic junction [23].
STRATEGIES FOR COMPLEX INTRAOPERATIVE PROBLEMS:
Tracheomalacia is a rare complication that may occur after trauma (long-term intubation], infection and chronic tracheal compression [24]. Dynamic tracheal collapse under bronchoscopy is the criterion standard in the diagnosis of tracheomalacia. Despite its low sensitivity, the tracheomalacia test has high specificity and is an effective adjunctive to bronchoscopy [25]. There are also centers using tracheobronchography as a supplement for bronchoscopy [26].
Based on the degree of disease and other relevant conditions, tracheomalacia can be treated conservatively, interventionally, or surgically. Mild localized tracheomalacia may disappear spontaneously, and these patients should be treated conservatively, monitored adequately, and followed up regularly. Aggressive surgical intervention is recommended for the patients with involvement of more than half of the cartilage rings or diffuse organ softening. Sulaiman et al reported a low incidence of tracheomalacia after thyroidectomy+sternotomy, and multivariate logistic regression analysis revealed no significant correlation between any relevant factors and the development of tracheomalacia [27]. For the treatment of tracheomalacia, one patient required tracheal resection with anastomosis, and 2 patients required tracheostomy [27].
Tracheal suspension is an effective method to treat tracheomalacia, it is simple, practical, and easy to master. We sutured the tracheal wall using a 4-0 Prolene suture. After piercing the presternal skin, it was inserted into a rubber tube to reduce tension, with a certain length reserved for adjustment. Moreover, tracheal suspension is an effective measure to rescue intraoperative asphyxia and prevent postoperative asphyxia.
Severe tracheomalacia or severe irreversible TS may require tracheal resection and reconstruction. For patients who undergo tracheal resection, preoperative high-resolution CT scanning of the neck and
Tracheal sleeve resection is carried out by resecting the tracheal segment with lesions, followed by end-to-end anastomosis. It is generally believed that the safe length for tracheal resection is 4 cm [28]. The complication rate after tracheal reconstruction can reach 40% [29]. Common complications include anastomotic fistula, anastomotic restenosis, recurrent laryngeal nerve injury, mediastinal emphysema, and abscess [30]. However, the possibility of tracheal resection and reconstruction for retrosternal goiter and tracheal stenosis is relatively low. In our study, none of the patients required tracheal reconstruction.
Stent implantation is also an option for severe tracheomalacia or severe stenosis [31]. It has been confirmed that the insertion of a tracheobronchial stent results in an immediate and significant improvement in fatal dyspnea in 70–100% of patients with TS [32], thus providing better preparation for surgery. In this study, 1 patient had acute TS before surgery (Figure 4A, 4B). After tracheoscopic tracheal stent implantation, tracheal wall oppression was detected intraoperatively (Figures 4C, 4D, 5A). The operation went smoothly, and tracheomalacia does not occur during surgery (Figure 5C, 5D). The trachea was well supported by the stent after the operation. One month after surgery, tracheoscopic removal of the stent was performed, and no noticeable tracheomalacia was found endoscopically (Figures 4E, 4F, 5B). The incidence of tracheal stent-related complications is reported to be as high as 18% [33]. The most common and severe complications include granulation tissue formation and secretory obstruction. Other stent-related problems include migration, incorrect position, infection, slippage, and bleeding. Piao et al suggested that the optimal tracheal management for RG resection is temporary placement of tracheobronchial stents before surgery [34]. We believe that although stent implantation has these problems to be solved, it is safe, effective, and more minimally invasive for tracheomalacia caused by the external pressure of benign tumors such as RG. However, the relevant complications and timing of stent removal should be further evaluated.
EXTENT OF THYROIDECTOMY:
The extent of thyroidectomy is determined by preoperative thyroid function examination and intraoperative lesion involvement. Preoperative multidisciplinary consultation involving thyroid surgery and endocrinology is necessary. Total thyroidectomy is recommended for patients with bilateral diffuse enlargement. Hemi-thyroidectomy can be considered for patients with an enlarged thyroid on one side and a normal thyroid on the other. In partial RG with an intact envelope, only the enlarged lesion should be resected.
TREATMENT AND NURSING OF POSTOPERATIVE COMPLICATIONS:
For patients with secondary hyperthyroidism after surgery, drugs should be adjusted routinely to prevent thyroid crisis. Routine calcium supplements are recommended for patients with hypothyroidism. With laryngeal edema, hormones can be used prophylactically. Patients with postoperative tracheomalacia inducing respiratory failure should be treated with tracheotomy, endotracheal intubation, or stent implantation.
We acknowledge that this retrospective study has some limitations. First, not enough cases were included. In addition, our study did not compare the time, amount of blood loss, and complications of different surgical methods. We are aware of some potential technical biases in our research. Despite these limitations, the results of this study on retrosternal goiter provides additional important experience.
Conclusions
It is necessary to have a full multidisciplinary team in surgical management of retrosternal goiter and tracheal stenosis. The multidisciplinary collaboration will develop individualized anesthesia and surgical plans, allow quality care and minimization of perioperative risks and complications.
Figures
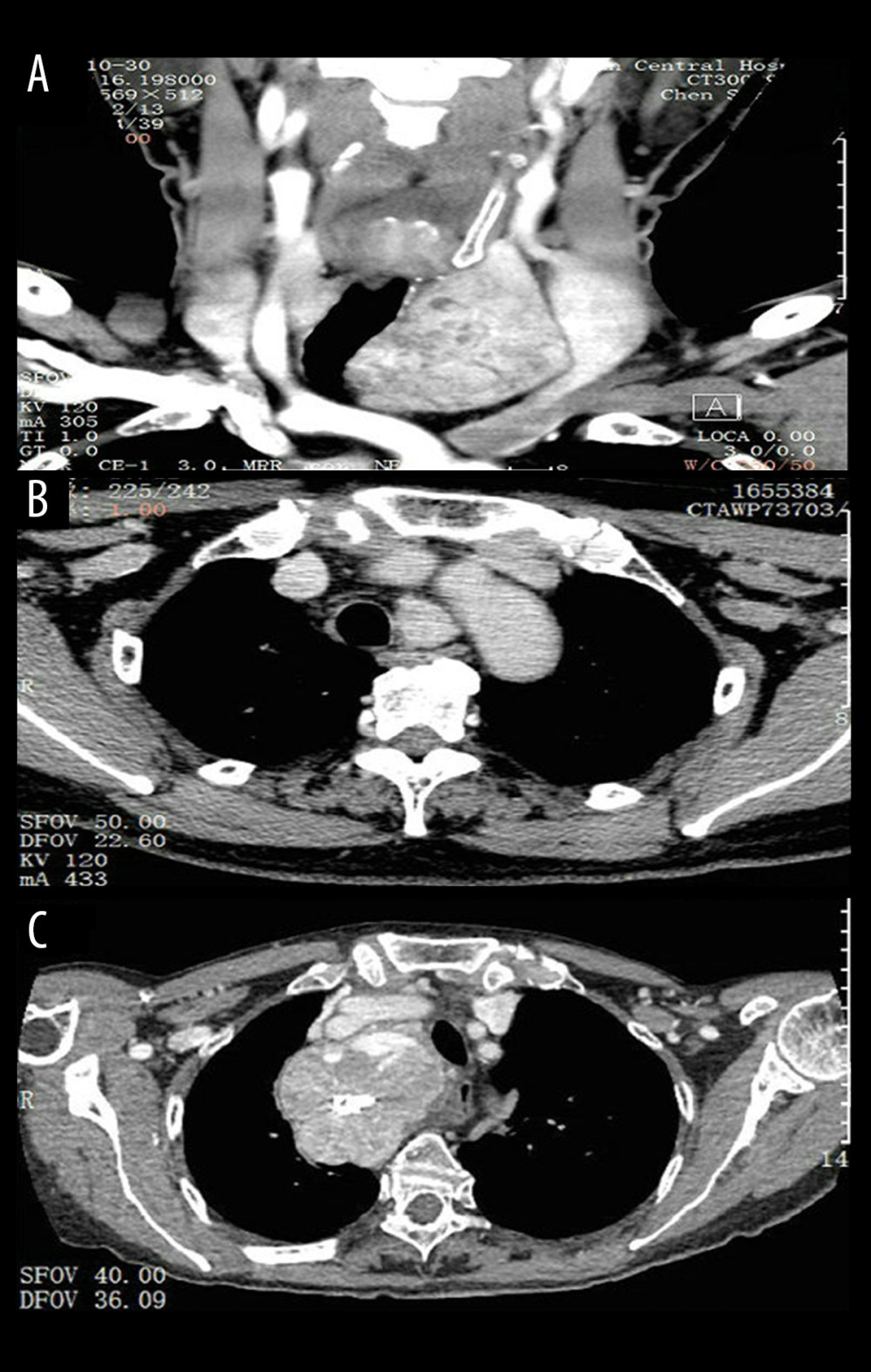 Figure 1. Three types of Retrosternal goiter are detected on computed tomographic (CT) scans. (A) Type I, after over half of the cervical goiter enters the sternum, the lower pole reaches the superior margin of the aortic arch; (B) Type II, the goiter is almost entirely posterior to the sternum, with the lower pole behind the aortic arch or entering the postmediastinum; (C) Type III, a huge intrathoracic goiter protrudes into the thorax, which may be accompanied by superior vena cava compression syndrome.
Figure 1. Three types of Retrosternal goiter are detected on computed tomographic (CT) scans. (A) Type I, after over half of the cervical goiter enters the sternum, the lower pole reaches the superior margin of the aortic arch; (B) Type II, the goiter is almost entirely posterior to the sternum, with the lower pole behind the aortic arch or entering the postmediastinum; (C) Type III, a huge intrathoracic goiter protrudes into the thorax, which may be accompanied by superior vena cava compression syndrome. 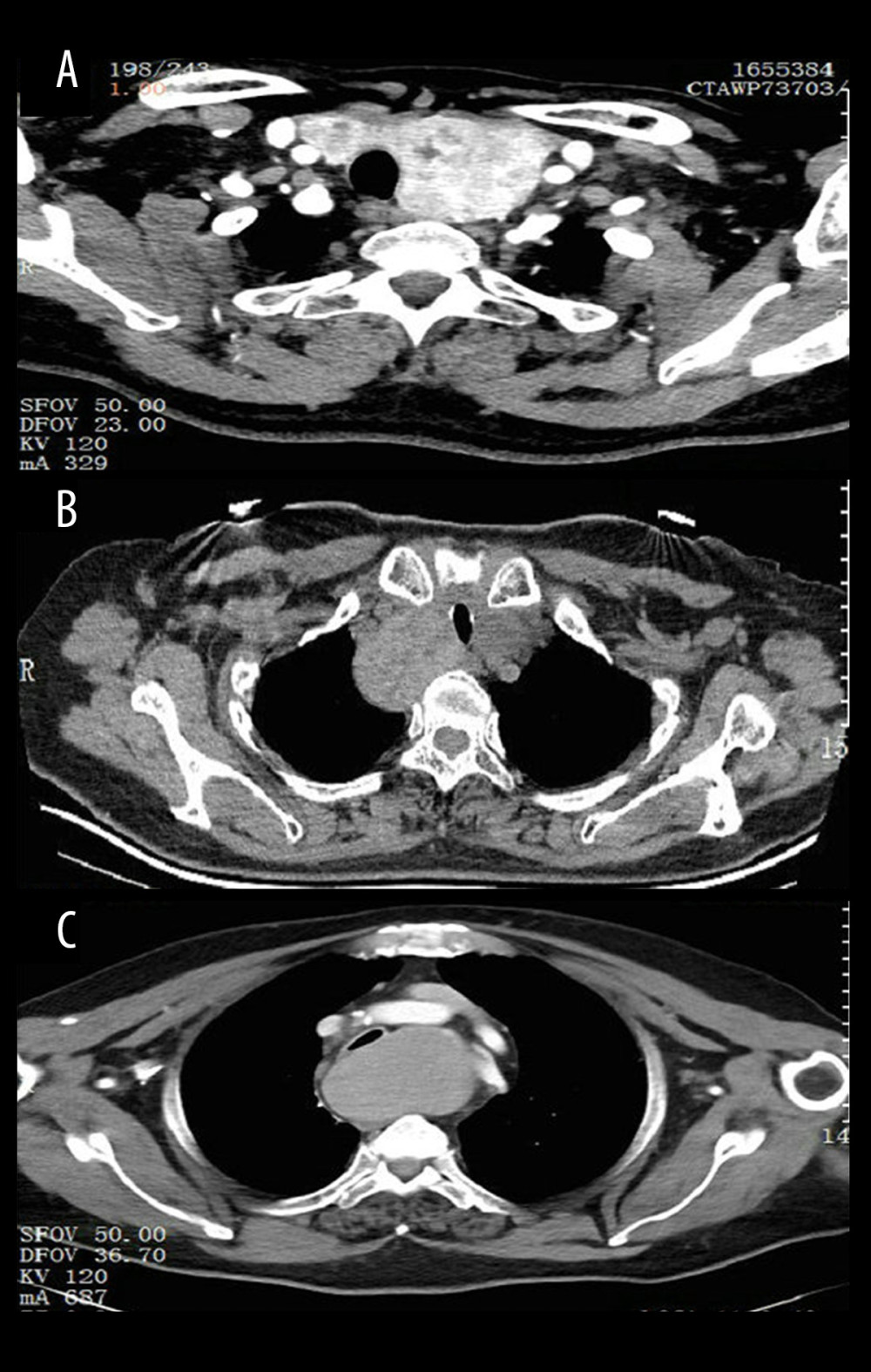 Figure 2. Three grades of retrosternal goiter were detected on CT scans. (A) grade I stenosis, less than 50% obstruction; (B) grade II stenosis, 51% to 70% obstruction; (C) grade III stenosis, 71% to 99% obstruction. There were no cases of grade IV stenosis.
Figure 2. Three grades of retrosternal goiter were detected on CT scans. (A) grade I stenosis, less than 50% obstruction; (B) grade II stenosis, 51% to 70% obstruction; (C) grade III stenosis, 71% to 99% obstruction. There were no cases of grade IV stenosis.  Figure 3. Surgical incision selection in different patients. (A) “Collar-like” cervical incision. (B) Cervical incision and median sternotomy. (C) Subxiphoid approach.
Figure 3. Surgical incision selection in different patients. (A) “Collar-like” cervical incision. (B) Cervical incision and median sternotomy. (C) Subxiphoid approach. 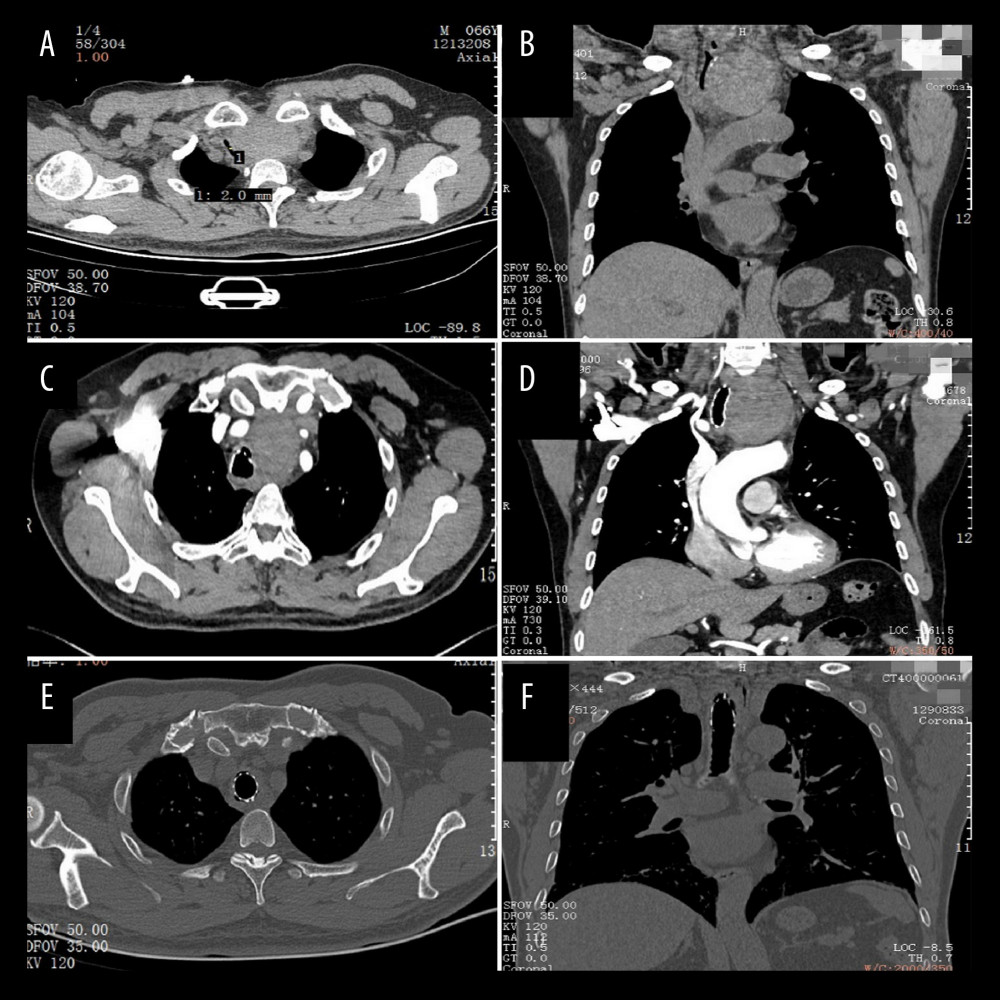 Figure 4. A patent of CT images before and after operation. The CT findings from a 66-year-old male patient revealed a type 1 RG with grade III tracheal stenosis. Axial (A) and coronal (B) images in soft-tissue windows are shown. Axial (C) and coronal (D) images in soft-tissue windows are shown after tracheoscopy. Intraoperative frozen sections suggested benign lesions. Axial (E) and coronal (F) images in soft-tissue windows are shown after surgery.
Figure 4. A patent of CT images before and after operation. The CT findings from a 66-year-old male patient revealed a type 1 RG with grade III tracheal stenosis. Axial (A) and coronal (B) images in soft-tissue windows are shown. Axial (C) and coronal (D) images in soft-tissue windows are shown after tracheoscopy. Intraoperative frozen sections suggested benign lesions. Axial (E) and coronal (F) images in soft-tissue windows are shown after surgery. 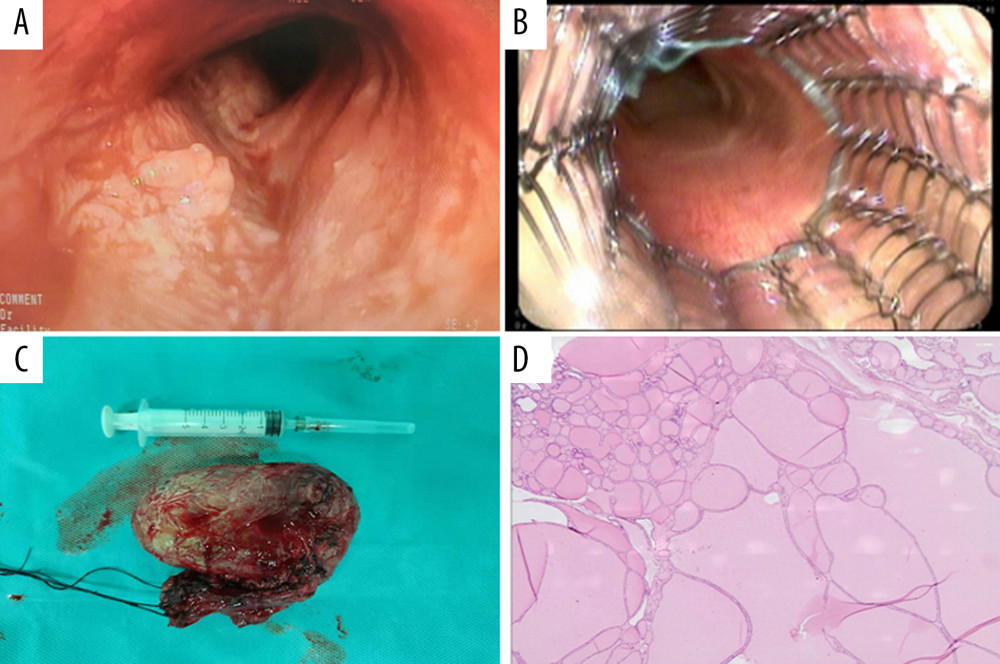 Figure 5. The same patient underwent a stent placement and operation. Based on progressive dyspnea, the respiratory physicians successfully implanted an airway stent under tracheoscopy to open the airway (A). Then, the patient’s vital signs were stable, relevant examination results were improved, and no contraindications were found. Surgical removal of the RG through a cervical approach (C). Postoperative pathological indication: Goiter with cystic lesions (hematoxylin and eosin,10×magnification) (D). One month after surgery, respiratory physicians removed the stent and found no tracheomalacia or tracheal stenosis (B).
Figure 5. The same patient underwent a stent placement and operation. Based on progressive dyspnea, the respiratory physicians successfully implanted an airway stent under tracheoscopy to open the airway (A). Then, the patient’s vital signs were stable, relevant examination results were improved, and no contraindications were found. Surgical removal of the RG through a cervical approach (C). Postoperative pathological indication: Goiter with cystic lesions (hematoxylin and eosin,10×magnification) (D). One month after surgery, respiratory physicians removed the stent and found no tracheomalacia or tracheal stenosis (B). 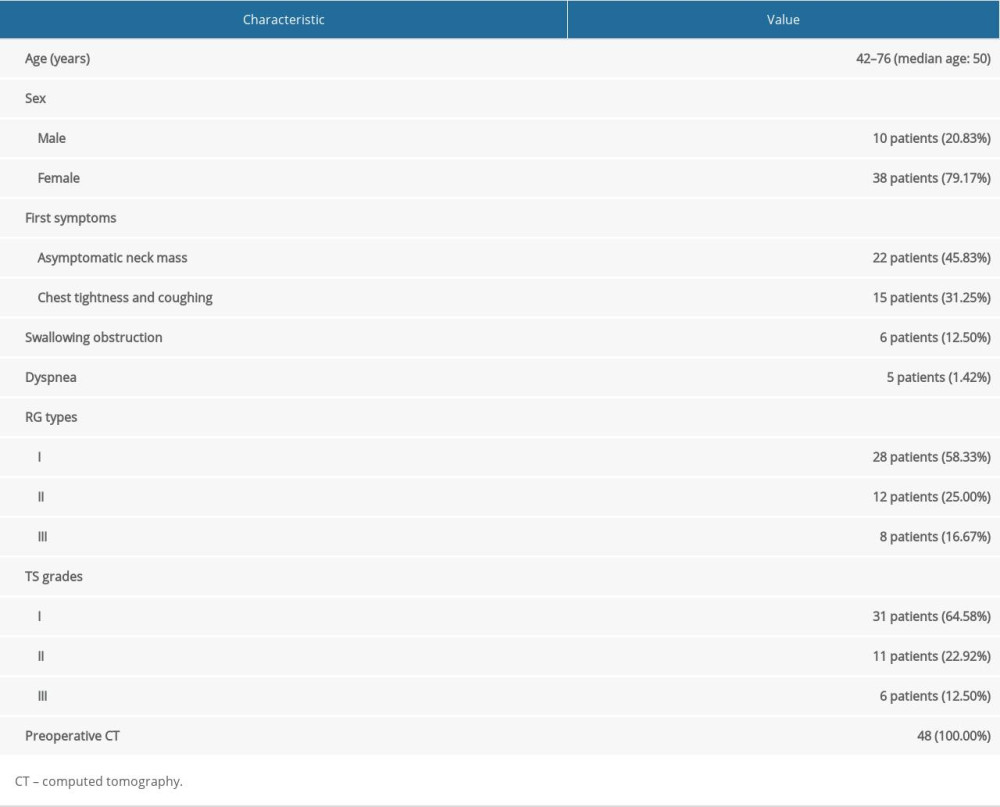

References
1. Shaha AR, Substernal goiter: What is in a definition?: Surgery, 2010; 147(2); 239-40
2. Wu Y, Qi Y, Tang PSurgical approach for intrathoracic goiter: Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi, 2006; 41(7); 528-31 [in Chinesse]
3. Anders HJ, Compression syndromes caused by substernal goiters: Postgrad Med J, 1998; 74(872); 327-29
4. Chen AY, Bernet VJ, Carty SE, American Thyroid Association statement on optimal surgical management of goiter: Thyroid, 2014; 24; 181-89
5. Batra YK, Gupta SK, Rajeev S, Tracheomalacia due to short term ventilation after total hip arthroplasty in an adult with long standing goiter: Anesth Analg, 2007; 105(6); 1867-68
6. Binar M, Serindere M, Bozlar U, Determining the thyroid gland volume causing tracheal compression: A semiautomated 3D CT volumetry study: Medicina (Kaunas), 2019; 55(5); 143
7. Myer CM, O’Connor DM, Cotton RT, Proposed grading system for subglottic stenosis based on endotracheal tube sizes: Ann Otol Rhinol Laryngol, 1994; 103; 319-23
8. Pan Y, Chen C, Yu L, Airway management of retrosternal goiters in 22 cases in a tertiary referral center: Ther Clin Risk Manag, 2020; 16; 1267-73
9. Li S, Ai Q, Liang H, Nonintubated robotic-assisted thoracic surgery for tracheal/airway resection and reconstruction: Technique description and preliminary results: Ann Surg, 2022; 275(2); e534-36
10. Jiang L, Liu J, Gonzalez-Rivas D, Thoracoscopic surgery for tracheal and carinal resection and reconstruction under spontaneous ventilation: J Thorac Cardiovasc Surg, 2018; 155(6); 2746-54
11. Okuda K, Moriyama S, Haneda H, Recent advances in video-assisted transthoracic tracheal resection followed by reconstruction under non-intubated anesthesia with spontaneous breathing: J Thorac Dis, 2017; 9(9); 2891-94
12. Ríos A, Sitges-Serra A, Surgical treatment of intrathoracic goiter: Cir Esp, 2012; 90; 421-28
13. Riffat F, Del Pero MM, Fish B, Radiologically predicting when a sternotomy may be required in the management of retrosternal goiters: Ann Otol Rhinol Laryngol, 2013; 122; 15-19
14. Wang X, Zhou Y, Li C, Surgery for retrosternal goiter: cervical approach: Gland Surg, 2020; 9(2); 392-400
15. Cichoń S, Anielski R, Konturek A, Surgical management of mediastinal goiter: Risk factors for sternotomy: Langenbecks Arch Surg, 2008; 393; 751-57
16. Yan HX, Du J, Fu J, Microarray-based differential expression profiling of long noncoding RNAs and messenger RNAs in formalin-fixed paraffin-embedded human papillary thyroid carcinoma samples: Transl Cancer Res, 2019; 8; 439-51
17. Sormaz İC, Uymaz DS, İşcan AY, The value of preoperative volumetric analysis by computerised tomography of retrosternal goiter to predict the need for an extra-cervical approach: Balkan Med J, 2018; 35(1); 36-42
18. Yano T, Okada T, Sato H, Preoperative evaluation of substernal goiter by computed tomography in the extended neck position: Case Rep Oncol, 2021; 14(3); 1353-58
19. Lin YS, Wu HY, Lee CW, Surgical management of substernal goiters at a tertiary referral centre: A retrospective cohort study of 2,104 patients: Int J Surg, 2016; 27; 46-52
20. Migliore M, Costanzo M, Cannizzaro MA, Cervico-mediastinal goiter: Is telescopic exploration of the mediastinum (video mediastinoscopy) useful?: Interactive Cardiovascular and Thoracic Surgery, 2010; 10; 439-40
21. Suda T, Subxiphoid uniportal video-assisted thoracoscopic surgery procedure: Thorac Surg Clin, 2017; 27(4); 381-86
22. Kuroda Y, Fukuzawa H, Kawahara I, Morita K, Hemi-Clamshell approach for fetal lung interstitial tumor resection in a neonate: A case report: Eur J Pediatr Surg Rep, 2021; 9(1); e72-e75
23. Shintani Y, Kanzaki R, Kawamura T, Surgical resection for advanced lung cancer using the hemi-clamshell approach: Interact Cardiovasc Thorac Surg, 2017; 25(3); 462-68
24. Carden KA, Boiselle PM, Waltz DA, Tracheomalacia and tracheobronchomalacia in children and adults: An in-depth review: Chest, 2005; 127; 984-1005
25. Sanchez MO, Greer MC, Masters IB, A comparison of fluoroscopic airway screening with flexible bronchoscopy for diagnosing tracheomalacia: Pediatr Pulmonol, 2012; 47(1); 63-67
26. Manimtim WM, Rivard DC, Sherman AK, Tracheobronchomalacia diagnosed by tracheobronchography in ventilator-dependent infants: Pediatr Radiol, 2016; 46(13); 1813-21
27. Sulaiman A, Lutfi A, Ikram M, Tracheomalacia after thyroidectomy for retrosternal goitres requiring sternotomy – a myth or reality?: Ann R Coll Surg Engl, 2021; 103(7); 504-7
28. Jamil A, Still S, Schwartz GS, Tracheal resection for tracheal stenosis: Proc (Bayl Univ Med Cent), 2019; 33(1); 15-18
29. Wertz A, Fuller SM, Mascio C, Slide tracheoplasty: Predictors of outcomes and literature review: Int J Pediatr Otorhinolaryngol, 2020; 130; 109814
30. Tapias LF, Mathisen DJ, Prevention and management of complications following tracheal resections-lessons learned at the Massachusetts General Hospital: Ann Cardiothorac Surg, 2018; 7(2); 237-43
31. Serio P, Fainardi V, Leone R, Tracheobronchial obstruction: follow-up study of 100 children treated with airway stenting: Eur J Cardiothorac Surg, 2014; 45(4); e100-9
32. Saad CP, Murthy S, Krizmanich G, Self-expandable metallic airway stents and flexible bronchoscopy: Long-term outcomes analysis: Chest, 2003; 124; 1993-99
33. Tanigawa N, Sawada S, Okuda Y, Symptomatic improvement in dyspnea following tracheobronchial metallic stenting for malignant airway obstruction: Acta Radiol, 2000; 41; 425-28
34. Piao M, Yuan Y, Wang Y, Feng C, Successful management of trachea stenosis with massive substernal goiter via thacheobronchial stent: J Cardiothorac Surg, 2013; 8; 212
Figures
Figure 1. Three types of Retrosternal goiter are detected on computed tomographic (CT) scans. (A) Type I, after over half of the cervical goiter enters the sternum, the lower pole reaches the superior margin of the aortic arch; (B) Type II, the goiter is almost entirely posterior to the sternum, with the lower pole behind the aortic arch or entering the postmediastinum; (C) Type III, a huge intrathoracic goiter protrudes into the thorax, which may be accompanied by superior vena cava compression syndrome.Figure 2. Three grades of retrosternal goiter were detected on CT scans. (A) grade I stenosis, less than 50% obstruction; (B) grade II stenosis, 51% to 70% obstruction; (C) grade III stenosis, 71% to 99% obstruction. There were no cases of grade IV stenosis.Figure 3. Surgical incision selection in different patients. (A) “Collar-like” cervical incision. (B) Cervical incision and median sternotomy. (C) Subxiphoid approach.Figure 4. A patent of CT images before and after operation. The CT findings from a 66-year-old male patient revealed a type 1 RG with grade III tracheal stenosis. Axial (A) and coronal (B) images in soft-tissue windows are shown. Axial (C) and coronal (D) images in soft-tissue windows are shown after tracheoscopy. Intraoperative frozen sections suggested benign lesions. Axial (E) and coronal (F) images in soft-tissue windows are shown after surgery.Figure 5. The same patient underwent a stent placement and operation. Based on progressive dyspnea, the respiratory physicians successfully implanted an airway stent under tracheoscopy to open the airway (A). Then, the patient’s vital signs were stable, relevant examination results were improved, and no contraindications were found. Surgical removal of the RG through a cervical approach (C). Postoperative pathological indication: Goiter with cystic lesions (hematoxylin and eosin,10×magnification) (D). One month after surgery, respiratory physicians removed the stent and found no tracheomalacia or tracheal stenosis (B). In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387