28 July 2022: Clinical Research
Discordant Subjective Perception of Sleep in Patients with Obstructive Sleep Apnea and Insomnia: A Retrospective Study
Xiaofan Zhuang1BCE, Xin ZhangDOI: 10.12659/MSM.937134
Med Sci Monit 2022; 28:e937134






Abstract
BACKGROUND: Factors affecting subjective perception of sleep are unclear but clinically important. We investigated the differences in subjective sleep perception of patients with obstructive sleep apnea (OSA) and insomnia disorder (ID).
MATERIAL AND METHODS: From our Sleep Medicine Center database, 33 patients with OSA and 69 with ID were selected and assessed with the Pittsburgh Sleep Quality Index (PSQI), Generalized Anxiety Disorder screen, Patient Health Questionnaire-9, Epworth Sleepiness Scale, Pre-sleep Arousal Scale (PSAS), and polysomnography.
RESULTS: In subjective sleep tests, PSQI total score, sleep quality, sleep onset latency (SOL), total sleep time, and sleep efficiency (SE) were higher in patients with ID. In objective sleep tests, patients with OSA had longer total sleep time, shorter SOL, lower percentage of stage N3, less SE, higher percentage of stage N1, more arousals, and higher arousal index. Hyperarousal state evaluation showed cognitive hyperarousal significantly higher with ID. Subjective sleep perception with OSA correlated positively with PSAS total score, cognitive hyperarousal, and percentage of stage N2 and negatively with percentage of REM, apnea-hypopnea index, and desaturation index. Subjective sleep perception of patients with ID correlated positively with PSAS total score, cognitive hyperarousal, SOL, N3 sleep latency, and REM sleep latency and negatively with SE.
CONCLUSIONS: Subjective sleep perception of OSA patients was mainly related to sleep structure and respiratory events, and that of ID patients, to sleep latency. Individual cognitive hyperarousal levels may be involved in negative subjective sleep perception. Clinicians should be aware that OSA patients may not actually experience adequate sleep.
Keywords: Polysomnography, Sleep Apnea Syndromes, Sleep Initiation and Maintenance Disorders, Humans, Perception, Sleep, Sleep apnea, obstructive
Background
Insomnia is the most prevalent sleep disorder, affecting 10% to 25% of adults in the general population [1]. It is a risk factor for dementia and various medical and psychiatric disorders, including heart failure, anxiety, and depression, and contributes to increased healthcare costs [2–4]. According to the International Classification of Sleep Disorders, 3rd edition (ICSD-3), insomnia is characterized by symptoms such as irritability and fatigue during wakefulness [5]. Thus, a diagnosis of insomnia mainly depends on clinical symptoms. In the field of sleep medicine, polysomnography is considered the criterion standard for objective and quantitative assessments of sleep, but data from the insomnia population have not been fully analyzed. Moreover, objective sleep measures of sleep continuity obtained by polysomnography are often inconsistent with subjective measures [6] because sleep perception, or sleep quality, is influenced by a combination of more than 1 sleep parameter.
Sleep perception is the self-assessment of sleep status, which is an important index in the clinical diagnosis of sleep disorders and determination of the efficacy of therapy. Abnormal sleep perception is a common finding in patients with a variety of medical, sleep, and psychiatric disorders [7,8]. Contrary to expectations, the perception of normal sleep often does not align with objective evaluations. For instance, long-term cocaine users experience positive sleep misperceptions during abstinence, with underestimations of sleep onset latency (SOL) and awakening after sleep onset being responsible for this difference [9]. Discordant sleep perception has also been reported in patients with obstructive sleep apnea (OSA) [10]. A major study showed that the prevalence of OSA was as high as 24% in men and 9% in women, based on an apnea-hypopnea index (AHI) criterion of ≥5/h. OSA is characterized by abnormalities of respiration during sleep and by upper airway narrowing or closure during sleep while respiratory effort continues. Most patients awaken in the morning feeling tired and unrefreshed regardless of the duration of their time in bed. In addition, OSA is frequently observed in patients with systemic hypertension, cardiovascular disease, and type 2 diabetes, and it may be an independent risk factor for these conditions [11,12].
Polysomnography is an objective diagnostic tool for OSA. A study suggested that patients with OSA have better sleep perception than do patients with insomnia, even if they sleep less, and that neither a decrease in oxyhemoglobin saturation nor microarousals during the occurrence of respiratory events seem to interfere with sleep perception [13]. In contrast to patients with OSA, patients with insomnia have difficulty recognizing their sleep state, with a tendency to overestimate awake time and underestimate asleep time [13]. Both are related to the ability to subjectively estimate time intervals and to differentiate states of consciousness (sleeping and wakefulness). Nevertheless, sleep misperception cannot be easily quantified, and the intrinsic mechanism of time perception during sleep that determines subjective sleep perception is still largely unknown.
In this study, we investigated the differences in subjective sleep perception between patients with OSA and those with insomnia. Also, taking into account hyperarousal theory, we investigated the possible factors related to subjective sleep perception to provide guidelines for the diagnosis and treatment of sleep-related disorders.
Material and Methods
PARTICIPANTS:
Patients with OSA and patients with insomnia were included in this retrospective study. Data were collected at the Sleep Medicine Center of Hangzhou Seventh People’s Hospital, China, from patients who visited the hospital for sleep disorders between October 2018 and September 2019. All patients underwent overnight polysomnography and were instructed to complete self-report questionnaires before and after the sleep study. Ethics approval for the study was obtained from Hangzhou Seventh People’s Hospital (approval no. 2018003-03).
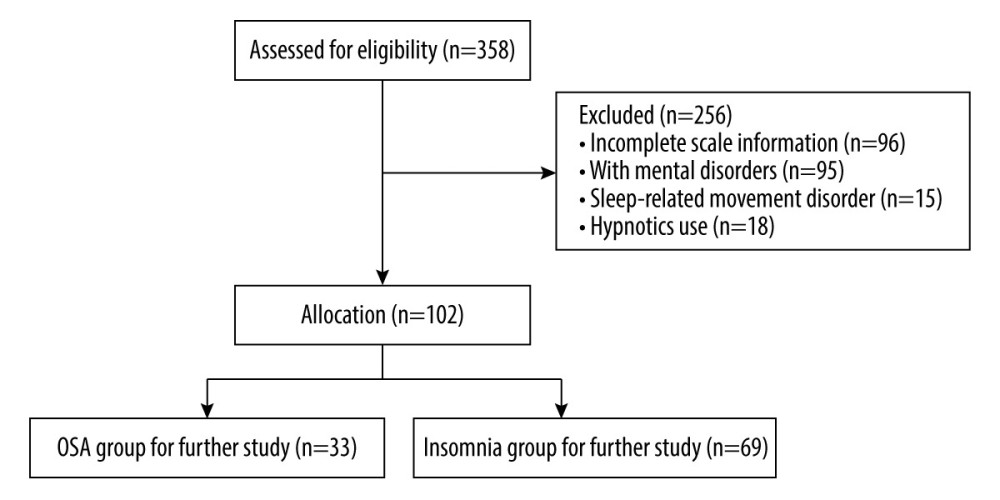
Inclusion criteria for the study were as follows: insomnia and OSA diagnosis consistent with ICSD-3; patients with OSA (AHI ≥5/h) with snoring but without insomnia-related symptoms; age ≥18 and ≤65 years; education level beyond primary school; ability to independently use a smartphone application (app) for scale evaluation; no medication; and drug abstinence for >2 weeks. Exclusion criteria were short-term insomnia disorders due to another mental disorder; a medical condition; drug or substance use; other sleep disorder or a serious medical, mental, or neurological condition; and shift workers. Data from 358 patients were screened and 102 eligible patients were eventually included (Figure 1). The 102 patients were divided into 2 groups: patients with insomnia disorder without OSA (ID, n=69) and patients with OSA without insomnia (OSA, n=33) (Table 1).
MEASURES:
The responses to the self-report questionnaires were assessed using the smartphone app Good Sleep 365. The sociodemographic characteristics of the patients (sex, age, educational level) were also collected. The Pittsburgh Sleep Quality Index (PSQI) was used to evaluate subjective sleep condition [14], the Epworth Sleepiness Scale (ESS) was used to assess daytime sleepiness [15], the Generalized Anxiety Disorder (GAD-7) scale and the Patient Health Questionnaire (PHQ-9) were used to measure emotional state [16,17], and the Pre-Sleep Arousal Scale (PSAS), including cognitive and somatic subscales, was used to evaluate hyperarousal levels [18].
The structural parameters of the polysomnography were used to evaluate the objective sleep condition. Electroencephalography electrodes were applied at C3-A2, C4-A1, F3-A2, F4-A1, O1-A2, and O2-A1, in accordance with the International 10–20 System. Bilateral vertical electrooculography, chin and bilateral anterior tibialis surface electromyography, electrocardiography sensors, nasal and oral airflow, thoracic and abdominal excursion, and finger oximetry were applied. Synchronized video monitoring was used to monitor abnormal sleep breathing or movements. A Grael polysomnography (Compumedics, Australia) was used to obtain data on the following sleep structural parameters: sleep efficiency (SE), total sleep time (TST), SOL, N3 sleep latency, REM sleep latency, sleep stage (N1, N2, N1+N2, N3, REM sleep,%), arousal number, arousal index (AI), AHI, and desaturation index (DI). The scoring standard was that of the American Academy of Sleep Medicine.
PROCEDURE:
All patients were asked to attend the Sleep Medicine Center before 4: 00 P.M. on the day of sleep monitoring. A semi-structured clinical interview to assess comorbid psychopathological disorders and sleep condition was conducted by 2 appropriately trained psychiatrists. Polysomnography sleep studies were recorded overnight, and the self-report questionnaires (PSQI, GAD-7, PHQ-9, PSAS) were completed prior to polysomnography using the Good Sleep 365 app. To match the patients’ habitual sleep time, sleep was monitored during their respective usual bedtimes.
STATISTICAL ANALYSES:
Data management and statistical analyses were performed using IBM-SPSS statistics software version 24 (Armonk, NY, USA). Categorical variables were analyzed using chi-square tests. Continuous variables conforming to a normal distribution were analyzed using independent sample
Results
The demographic characteristics of the participants are summarized in Table 1. There was a higher percentage of male patients in the OSA group than in the ID group, whereas the difference in the mean age (OSA: 45.1 [10.78]; ID: 41.3 [11.53]) and educational level of the 2 groups was not significant.
Among the 6 factor scores, in addition to the use of hypnotic drugs, the scores of sleep quality, sleep latency, TST, and SE significantly differed between the 2 groups (
The results of Spearman correlation analyses of factors related to subjective sleep perception, as indicated by the PSQI total score, are presented in Table 5. Sex served as the control variable. The subjective sleep perception of the OSA group correlated positively with the PSAS total score (r=0.403,
Discussion
The clinical diagnosis and treatment of sleep disorders such as insomnia largely depends on the subjective self-report of the sleep condition. However, objective measures of sleep are often inconsistent with subjective patient reports, particularly in patients with insomnia, and both subjective and objective differences in TST are very common. This mismatch has an impact on the diagnosis and treatment of insomnia [19]. Patients with OSA, by contrast, with disrupted sleep continuity, incomplete sleep structure, and in some cases hypoxemia, also tend to deny that they have poor sleep. Pinto et al found that sleep perception is best among good sleepers, followed by patients with OSA, and finally patients with insomnia [13], but the factors related to sleep perception were not mentioned in their study. Therefore, we explored the differences in subjective sleep perception by comparing OSA and insomnia.
The differences in subjective sleep perception in people with different sleep disorders have been explored in previous studies. A comparison of TST perception among patients with OSA, patients with insomnia, and normal controls based on polysomnography parameters and subjective estimation showed that median sleep perception as evaluated using TST was lowest in patients with insomnia (80.3%) and highest in patients with OSA (92.9%), with normal controls in the middle (91.4%) [20]. The PSQI scale is a frequently used subjective sleep assessment scale [21], and in the present study the PSQI total score served as an indicator of subjective sleep perception. Our results similarly showed that subjective perception of sleep was better in patients with OSA than in those with insomnia, particularly in terms of SOL and SE (Table 2). Patients in both groups experienced similar daytime dysfunction, which in OSA patients may have been related to excessive daytime sleepiness. The latter is a major presenting complaint in many but not all patients with OSA.
Our assessment of objective measures showed that the subjective sleep perception of patients with insomnia correlated positively with sleep latency, including SOL, N3 sleep latency, and REM sleep latency. In patients with insomnia, this could be attributed to the correlation of the backward shift of each sleep period with the poor sleep experience, whereas this was not the case in patients with OSA. Previous imaging studies have shown that the negative subjective sleep perception of SOL in patients with insomnia is related to a relatively high glucose metabolism in brain networks involved in consciousness during non-REM sleep [22]. Our assessment of objective sleep efficiency revealed a significantly lower SE in patients with OSA than in patients with insomnia, although the TST of the OSA group was longer. Bianchi et al also concluded that a low SE was not responsible for poor sleep perception [23]. In that study, subjective sleep estimates after 4 h of daytime sleep were associated with the percentage of REM and percentage of N3 stage, while after 12 h of continuous night-time sleep the correlation with N2 sleep was negative. Indeed, sleep structure is another important aspect of subjective sleep perception research. In our study, the subjective sleep perception of patients with OSA correlated positively with the percentage of of N2 stage and negatively with the percentage of REM sleep, while there was no obvious correlation between subjective sleep perception and the percentage of N1 and percentage of N3 sleep stage in patients with OSA. Previous studies have similarly found an association between the percentage of decline in REM sleep and negative subjective sleep perception [10]. Others have reported that slow-wave sleep is most readily perceived as sleep, followed by REM sleep, and N2 stage sleep [24,25], but this was not the case in our patients with insomnia. It may be because REM is often accompanied by vivid dreams, and patients may consider REM stage as an awake state when they wake up from this period; however, this remains to be confirmed.
A correlation between a higher AHI and both greater sleep fragmentation and a worse sleep perception was expected, and the sleep perception in the present study was evaluated by a sleep perception index [26,27]. When exploring polysomnography correlates of subjective TST, the subjective and objective TST values are significantly correlated [26,28]. In our study, the subjective sleep perception (PSQI score) and objective sleep time of patients with OSA were not completely consistent, possibly because the patients we included had more serious sleep-breathing events (AHI=47.4 (25.3, 83.6); Table 4); and OSA patients with insomnia were excluded. Matt et al compared the mismatch by first quantifying the subjective-objective difference within individuals, with results showing that OSA patients and OSA patients with insomnia had less sleep mismatch than did patients with insomnia alone [28], which was similar to our results. We found that sleep perception in patients with OSA correlated negatively with AHI and desaturation index. The perception of a poor sleep experience was possibly weakened by severe sleep-related breathing events. Interestingly, in a study that used continuous positive airway pressure titrations in patients with insomnia and OSA, sleep latency was generally over-estimated, while wake after sleep onset and number of awakenings were under-estimated [29]. None of these estimations differed between diagnostic and treatment polysomnography. This suggests that comorbidities of insomnia are more likely to be involved in affecting sleep perception, which is why we excluded OSA patients who had insomnia as their main concern. Laranjeira et al showed that in addition to the STOP-BANG questionnaire, the subjective evaluation of sleepiness, sleep quality, sleep perception, and TST does not necessarily indicate the severity of OSA, and self-reported good sleep does not mean the absence of fewer sleep-related breathing problems [30]. Based on these findings, it was concluded that patients with sleep disorders should undergo polysomnography to elucidate the disorder subtype and obtain appropriate treatment. Our evaluation of sleep fragmentation showed a higher arousal number and AI among patients with OSA than in those with insomnia, as was the case for the percentage of N1 stage. However, our OSA patients frequently described a good sleep experience. Bianchi et al concluded that sleep fragmentation was not the basis of sleep misperception, showing that neither a subjective estimate of total sleep time nor the accuracy of the sleep estimate was associated with indicators such as N1 sleep and arousal number [31]. Our study confirmed those findings, as it showed that subjective sleep perception did not correlate with arousal number or AI.
Neurophysiological research suggests that hyperarousal of the cognitive level of the central nervous system damages the brain’s inhibitory processes during sleep, and that sleep deprivation affects local brain regions and is among the underlying mechanisms of negative sleep perception. Other studies have shown that negative sleep perception in patients with insomnia is associated with increased brain activity during sleep, as determined by polysomnography [32]. To exclude the interactive effects of anxiety and depression on hyperarousal, we included the GAD-7 and PHQ-9 in this study, which showed that the anxiety level between the 2 groups did not significantly differ, whereas the depression level was higher in patients with insomnia than in patients with OSA. However, this can also be explained by the presence of sleep-related items in the PHQ-9 scale. Our results suggest that hyperarousal, particularly the level of cognitive arousal, is an important cause of subjective negative sleep perception. The higher cognitive arousal level in the ID group than in the OSA group indicated that pre-sleep cognitive arousal is an intrinsic mechanism of the perception of time during sleep. The high level of hyperarousal in patients with insomnia may be an important factor explaining the greater disparity in subjective sleep perception in these patients than in OSA patients.
Conclusions
In conclusion, the factors affecting subjective sleep perception in patients with OSA are not the same as those in patients with insomnia, although in both conditions the sleep structure is disrupted and SE is decreased. Prolonged SOL is an important factor in the poor subjective perception of sleep in patients with insomnia, while increased sleep-breathing events may lessen the experience of poor sleep in patients with OSA. Hyperarousal may be a key mechanism regulating sleep perception, with hyperarousal at the cognitive level as a possible factor explaining the difference in subjective sleep perception between OSA and insomnia patients. Thus, in clinical practice, improving indicators such as the time needed to fall asleep and decreasing the cognitive arousal level may effectively improve patients’ positive subjective perception of sleep. Patients with suspected sleep breathing events, as determined by physical examination and questionnaires, particularly patients who feel that they have slept well, should undergo a polysomnography examination to provide an accurate picture of the patient’s true sleep condition. As shown in our patients with OSA, those who self-reported good sleep may not necessarily have less severe OSA.
Tables
Table 1. Demographic characteristics of the participants. Table 2. PSQI, Pittsburgh Sleep Quality Index total score and factor score of patients in the obstructive sleep apnea (OSA) and insomnia disorder (ID) groups.
Table 2. PSQI, Pittsburgh Sleep Quality Index total score and factor score of patients in the obstructive sleep apnea (OSA) and insomnia disorder (ID) groups. Table 3. GAD-7, PHQ-9, ESS, and PSAS scores of patients with obstructive sleep apnea (OSA) and insomnia disorder (ID).
Table 3. GAD-7, PHQ-9, ESS, and PSAS scores of patients with obstructive sleep apnea (OSA) and insomnia disorder (ID).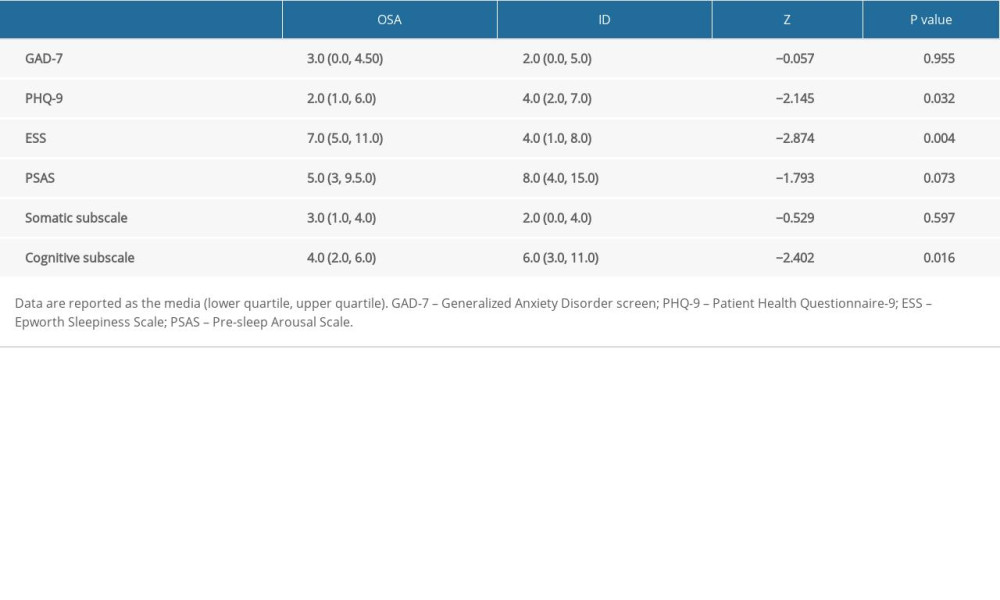 Table 4. Polysomnography sleep parameters of patients with obstructive sleep apnea (OSA) and insomnia (ID).
Table 4. Polysomnography sleep parameters of patients with obstructive sleep apnea (OSA) and insomnia (ID).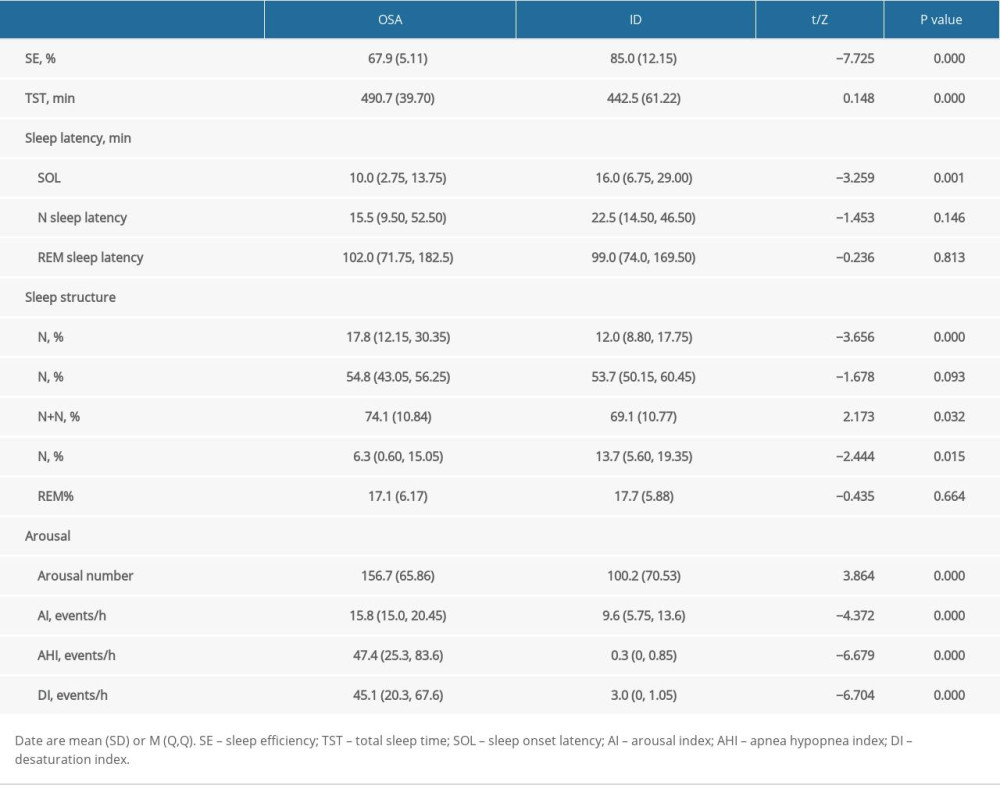 Table 5. Spearman correlation analyses of factors related to subjective sleep perception.
Table 5. Spearman correlation analyses of factors related to subjective sleep perception.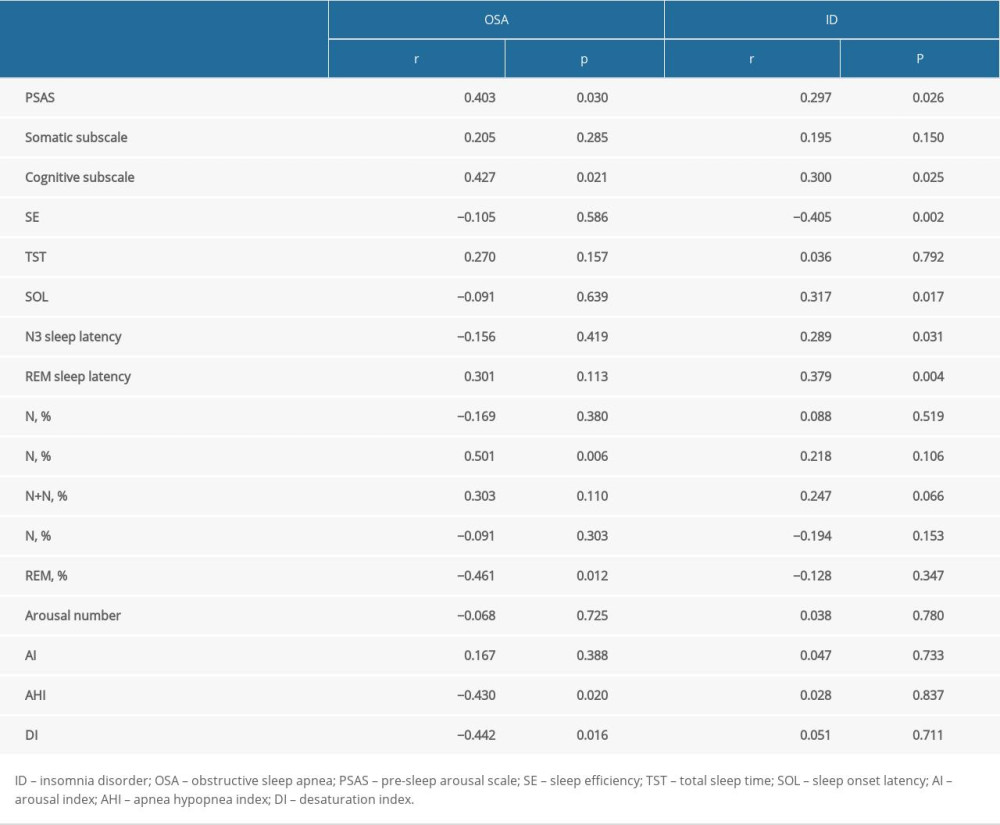
References
1. Ohayon MM, Epidemiology of insomnia: What we know and what we still need to learn: Sleep Med Rev, 2002; 6(2); 97-111
2. de Almondes KM, Costa MV, Malloy-Diniz LF, Insomnia and risk of dementia in older adults: Systematic review and meta-analysis: J Psychiatr Res, 2016; 77; 109-15
3. Hertenstein E, Feige B, Gmeiner T, Insomnia as a predictor of mental disorders: A systematic review and meta-analysis: Sleep Med Rev, 2019; 43; 96-105
4. Khan MS, Aouad R, The effects of insomnia and sleep loss on cardiovascular disease: Sleep Med Clin, 2017; 12(2); 167-77
5. Rezaie L, Khazaie H, Yazdani F, Exploration of the experience of living with chronic insomnia: A qualitative study: Sleep Sci, 2016; 9(3); 179-85
6. Means MK, Edinger JD, Glenn DM, Accuracy of sleep perceptions among insomnia sufferers and normal sleepers: Sleep Med, 2003; 4(4); 285-96
7. Schneider-Helmert D, Asymptomatic insomnia: Sleep Med, 2007; 8(2); 107-10
8. Rezaie L, Fobian AD, McCall WV, Paradoxical insomnia and subjective-objective sleep discrepancy: A review: Sleep Med Rev, 2018; 40; 196-202
9. Hodges SE, Pittman B, Morgan PT, Sleep perception and misperception in chronic cocaine users during abstinence: Sleep, 2017; L40(3); zsw069
10. Nam H, Lim JS, Kim JS, Sleep perception in obstructive sleep apnea: A study using polysomnography and the multiple sleep latency test: J Clin Neurol, 2016; 12(2); 230-35
11. Pugliese G, Barrea L, Laudisio D, Sleep apnea, obesity, and disturbed glucose homeostasis: Epidemiologic evidence, biologic insights, and therapeutic strategies: Curr Obes Rep, 2020; 9(1); 30-38
12. Collen J, Lettieri C, Wickwire E, Obstructive sleep apnea and cardiovascular disease, a story of confounders: Sleep Breath, 2020; 24(4); 1299-313
13. Pinto LR, Pinto MC, Goulart LI, Sleep perception in insomniacs, sleep-disordered breathing patients, and healthy volunteers – an important biologic parameter of sleep: Sleep Med, 2009; 10(8); 865-68
14. Mollayeva T, Thurairajah P, Burton K, The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis: Sleep Med Rev, 2016; 25; 52-73
15. Walker NA, Sunderram J, Zhang P, Lu SE, Clinical utility of the Epworth sleepiness scale: Sleep Breath, 2020; 24(4); 1759-65
16. Spitzer RL, Kroenke K, Williams JB, A brief measure for assessing generalized anxiety disorder: the GAD-7: Arch Intern Med, 2006; 166(10); 1092-97
17. Kroenke K, Spitzer RL, Williams JB, The PHQ-9: Validity of a brief depression severity measure: J Gen Intern Med, 2001; 16(9); 606-13
18. Ruivo Marques D, Allen Gomes A, Nicassio PM, Pre-Sleep Arousal Scale (PSAS): Psychometric study of a European Portuguese version: Sleep Med, 2018; 43; 60-65
19. Harvey AG, Tang NK, (Mis)perception of sleep in insomnia: A puzzle and a resolution: Psychol Bull, 2012; 138(1); 77-101
20. Choi SJ, Suh S, Ong J, Sleep misperception in chronic insomnia patients with obstructive sleep apnea syndrome: Implications for clinical assessment: J Clin Sleep Med, 2016; 12(11); 1517-25
21. Bei B, Milgrom J, Ericksen J, Subjective perception of sleep, but not its objective quality, is associated with immediate postpartum mood disturbances in healthy women: Sleep, 2010; 33(4); 531-38
22. Kay DB, Karim HT, Soehner AM, Subjective-objective sleep discrepancy is associated with alterations in regional glucose metabolism in patients with insomnia and good sleeper controls: Sleep, 2017; 40(11); zsx155
23. Bianchi MT, Wang W, Klerman EB, Sleep misperception in healthy adults: Implications for insomnia diagnosis: J Clin Sleep Med, 2012; 8(5); 547-54
24. Goulart LI, Pinto LR, Perlis ML, Effects of different sleep deprivation protocols on sleep perception in healthy volunteers: Sleep Med, 2014; 15(10); 1219-24
25. Aritake-Okada S, Uchiyama M, Suzuki H, Time estimation during sleep relates to the amount of slow wave sleep in humans: Neurosci Res, 2009; 63(2); 115-21
26. Duarte RLM, Mendes BA, Oliveira-E-Sá TS, Perception of sleep duration in adult patients with suspected obstructive sleep apnea: PLoS One, 2020; 15(8); e0238083
27. Khan Z, Bachan M, Taweesdt P, Arousal perception/misperception and total sleep time misperception in subjects with sleep disorders: Int J Med Med Sci, 2019; 11(5); 43-50
28. Bianchi MT, Williams KL, McKinney S, The subjective-objective mismatch in sleep perception among those with insomnia and sleep apnea: J Sleep Res, 2013; 22(5); 557-68
29. Castillo J, Goparaju B, Bianchi MT, Sleep-wake misperception in sleep apnea patients undergoing diagnostic versus titration polysomnography: J Psychosom Res, 2014; 76(5); 361-67
30. Laranjeira CM, Barbosa E, Rabahi MF, Is subjective sleep evaluation a good predictor for obstructive sleep apnea: Clinics (Sao Paulo), 2018; 73; e355
31. Saline A, Goparaju B, Bianchi MT, Sleep fragmentation does not explain misperception of latency or total sleep time: J Clin Sleep Med, 2016; 12(9); 1245-55
32. Turcotte I, St-Jean G, Bastien CH, Are individuals with paradoxical insomnia more hyperaroused than individuals with psychophysiological insomnia? Event-related potentials measures at the peri-onset of sleep: Int J Psychophysiol, 2011; 81(3); 177-90
Tables
Table 1. Demographic characteristics of the participants.Table 2. PSQI, Pittsburgh Sleep Quality Index total score and factor score of patients in the obstructive sleep apnea (OSA) and insomnia disorder (ID) groups.Table 3. GAD-7, PHQ-9, ESS, and PSAS scores of patients with obstructive sleep apnea (OSA) and insomnia disorder (ID).Table 4. Polysomnography sleep parameters of patients with obstructive sleep apnea (OSA) and insomnia (ID).Table 5. Spearman correlation analyses of factors related to subjective sleep perception.Table 1. Demographic characteristics of the participants.Table 2. PSQI, Pittsburgh Sleep Quality Index total score and factor score of patients in the obstructive sleep apnea (OSA) and insomnia disorder (ID) groups.Table 3. GAD-7, PHQ-9, ESS, and PSAS scores of patients with obstructive sleep apnea (OSA) and insomnia disorder (ID).Table 4. Polysomnography sleep parameters of patients with obstructive sleep apnea (OSA) and insomnia (ID).Table 5. Spearman correlation analyses of factors related to subjective sleep perception. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387