17 November 2022: Clinical Research
Identification and Validation of a Novel Model: Predicting Short-Term Complications After Local Flap Surgery for Skin Tumor Removal
Zhengnan Zhao1ABCDEF, Yue Tao1B, Xinjian Xiang1C, Zexu Liang1B, Yu Zhao1A*DOI: 10.12659/MSM.938002
Med Sci Monit 2022; 28:e938002






Abstract
BACKGROUND: The aim was to analyze the risk factors for the occurrence of complications after local flap transfer and to construct a simple prediction model to help surgeons in the perioperative screening of high-risk patients.
MATERIAL AND METHODS: Short-term complications were defined as any postoperative infection, dehiscence, bleeding, subcutaneous effusion, fat liquefaction, arteriovenous crisis, and tissue necrosis that required medical consultation or intervention. To explore 16 factors influencing short-term complications after local flap transfer, least absolute shrinkage and selection operator (LASSO) logistic regression was used to reduce the dimensionality of the data and to screen for predictors. Independent risk factors affecting the development of complications after local flap transfer were analyzed using logistic multiple regression models. The consistency (C-)index, receiver operating characteristic (ROC) curves, and calibration curves were used to check the model’s discrimination and calibration. Decision curve analysis (DCA) curves were used to evaluate the clinical applicability of this model, and internal validation was assessed using bootstrap validation.
RESULTS: The C-index of the nomogram model to predict short-term complications after local flap transfer was 0.763 (95% CI: 0.702-0.824), the area under the ROC curve was 0.763, and the internal validation C-index was 0.747. The calibration curve showed good agreement between observed and predicted values, and the DCA showed the model can benefit patients.
CONCLUSIONS: The model identified the relevant factors influencing short-term complications after local flap transfer, facilitating the identification and targeted intervention of patients at high risk of flap complications after surgery.
Keywords: nomograms, Surgical Flaps, Validation study, Humans, Reproducibility of Results, Skin, Skin Neoplasms
Background
Skin tumors are very common, and whether malignant tumors are represented by squamous cell carcinomas, basal cell carcinomas, or benign lesions such as nevi, solar keratoses, or keloid scars, surgical excision is the most effective treatment modality. For skin defect wounds left after surgical excision, the use of local flap repair is the preferred modality to achieve similar thickness and color [1]. However, whether postoperative flaps can be subjected to complications and whether they can heal properly is a concern for most physicians.
Therefore, the analysis of risk factors affecting flap healing is an important task for surgeons. Relevant studies on exploring the influencing factors related to flap necrosis have been conducted. Some scholars [2–6] concluded that a higher body mass index (BMI) or obesity is detrimental to normal flap healing, while Crippen [7] et al argued that obesity had a protective effect on flaps in some cases. Smoking and lower protein levels were more consistently identified as risk factors for flap healing [8–13]. Other factors considered to be associated with flap prognosis include radiation history [14], diabetes [15], age [16], defect site and flap size [17], and hypertension [8]. In our clinical work, we cannot reject patients with histories including smoking, advanced age, or poor nutritional status. When faced with these patients, we can be aware that the incidence of adverse postoperative outcomes will be higher. During surgery, conditions such as deeper tumor invasion, fewer distal flap bleeding sites, and wound sutures with tension can raise concerns about the flap’s ability to heal successfully. Therefore, a model that can predict flap outcomes is needed. However, most previous studies were limited to the reconstruction of breast defects, and the type of flap studied was mostly the free flap; few studies were conducted on the local transposition flap, which is more widely used in clinical practice. In this review, we conducted a retrospective analysis of 416 patients who underwent local flap transposition. We aimed to identify risk factors after local transposition flap reconstruction and to construct a simple and intuitive risk prediction model to assist surgeons in perioperative clinical decision-making and to reduce the occurrence of postoperative complications. The aim of this paper was to analyze the risk factors for the occurrence of complications after local flap transfer and to construct a simple prediction model to help surgeons in the perioperative screening of high-risk patients.
Material and Methods
We consecutively collected clinical data related to patients with various skin lesions admitted to the institution from July 2019 to March 2022 who underwent excision of skin lesions combined with local flap grafting. The inclusion criteria were (1) all patients who underwent local flap grafting in the institution from July 2019 to March 2022 and (2) the surgical procedure was performed by the same surgical team in the institution. The exclusion criteria were preoperative trauma or infection around the surgical incision, preoperative systemic infectious disease, and incomplete clinical information. We collected the following variables: demographic characteristics of age, sex, BMI, and smoking history and basic disease conditions, such as diabetes, hypertension, anemia, low prealbumin levels, and hypoproteinemia. Characteristics of the surgery that were collected were whether it was a secondary operation or not, surgical position, pathological nature of the lesion, residual defect-area, whether the bone was infringed, and laboratory indicators, glucose (GLU) and white blood cell (WBC) count. The definition of a secondary surgery was the same operative area received a second surgery within 1 month. Hypoproteinemia was defined as a serum albumin level below 35 g/L. A low prealbumin level was considered as serum prealbumin <150 mg/L. The definition of smoking history was smoking more than 1 cigarette per day for more than 6 months. The study was approved by the ethics committee of the institution, and informed consent was obtained from all patients or their legal guardians.
In the case of a normal data distribution, the quantitative variables were expressed as the mean ± standard deviation using the
Results
CLINICAL BASELINE DATA:
A total of 416 patients were included, 203 men and 213 women, with a mean age of 59.10±27.30 years, of whom 344 were in the group without complications and 72 in the group with complications. The complication rate was 17.3%. Statistically significant differences existed between the 2 groups in terms of whether secondary surgery was performed, defect area, smoking history, hypoproteinemia, low prealbumin level, BMI, whether the bone was infringed, surgical position, and pathological nature of the lesion (P<0.05). There were no statistical differences in terms of sex, age, diabetes, hypertension, anemia, GLU, and WBC (P>0.05). Detailed information is shown in Tables 1 and 2.
INDEPENDENT RISK FACTORS FOR SHORT-TERM COMPLICATIONS AFTER FLAP TRANSFER:
The screening was performed from the 16 variables collected based on the non-zero coefficients of the LASSO regression analysis, thus reducing the complexity of the prediction model. Six potential predictors were selected when the log(lambada) was taken as a minimum; namely, secondary operation, hypoproteinemia, smoking history, infringement of bone, BMI, and defect area, as shown in Figure 1. Incorporating these 6 predictors into a multifactorial logistic regression showed that hypoproteinemia, smoking history, infringement of bone, BMI, and defect area were independently associated with the occurrence of complications (Table 3).
CONSTRUCTION AND VALIDATION OF THE NOMOGRAM:
The independent risk factors for the complications hypoproteinemia, smoking history, infringement of bone, BMI, and defect area were incorporated into the model to construct a nomogram for the prediction of postoperative complications after local flap surgery. Considering the extensive nature of secondary operations in the removal of body surface tumors, the same was included in the model (Figure 2). The stability of the model was evaluated using the C-index, calibration curve, and ROC curve. The C-index of the model constructed in this study was 0.763 (95% CI: 0.702–0.824), the internal validation C-index was 0.747, and the area under the ROC curve was 0.763 (Figure 3A), indicating the model had good discrimination. The calibration correction curve showed a good agreement between the actual and simulated prediction curves (Figure 3B), suggesting that the model had good prediction performance. The DCA curve showed that thresholds in the 4% to 69% interval had a significant net benefit in using this model to predict postoperative complications of the local flap (Figure 4).
Discussion
Proximity flap transfer is an effective method for repairing body surface soft tissue defects; however, its postoperative complications include infection, dehiscence, bleeding, subcutaneous effusion, fat liquefaction, arteriovenous crisis, and tissue necrosis, which result in poor health outcomes and increased health care costs. In contrast to short-term complications, long-term complications of the flap are often related to the appearance of the flap, such as scar contracture, hyperpigmentation, and flap bloat, and this is also a topic worth investigating; however, the focus of this study was on short-term complications to aid in early intervention. LASSO regression is considered suitable for approximate subtraction screening of high-dimensional data [18] and has been widely used clinically to select the best characteristics among risk factors. Nomograms have been widely used in clinical studies as convenient risk prediction tools due to their intuitiveness and accuracy. We developed and validated a new nomogram based on patient-related clinical variables. This model contained 6 variables: secondary surgery, hypoproteinemia, smoking history, whether or not the bone was infringed, BMI, and defect area. Coincidentally, the distribution of the variables we screened were statistically significantly different in the 2 groups (Table 1), which we believe reflects the rationality of our screening process. We believe that this model can help physicians assess patients at high risk of complications on the day after surgery, visually present patients with relevant risk factors, and improve patient awareness of the treatment process.
According to our results, hypoproteinemia was retained in LASSO regression, and the inclusion of multifactorial logistics regression showed that patients with hypoproteinemia were 3.517 times more likely to have postoperative complications than were patients without hypoproteinemia, indicating that hypoproteinemia can significantly influence the occurrence of postoperative complications in the local flap. The clinical role of albumin as a marker for the evaluation of nutritional status has received increasing attention for its functions of maintaining colloid osmotic pressure, cell membrane integrity, and acid-base balance. Hypoproteinemia has been widely demonstrated to be associated with the prognosis of flap reconstruction, with Fang et al [8] suggesting that postoperative hypoproteinemia is a risk factor for poor flap healing complications, and Shum et al [9] suggesting that lower prealbumin levels are a risk factor for microvascular free flap failure. In a study by Xu et al [10], supplementation of albumin in the perioperative period to increase albumin levels was effective in reducing local flap complications and shortening the length of hospital stay. The redox properties possessed by albumin can effectively resist tissue damage or the increase of inflammatory reactive oxygen species [19], which may be related to the mechanism by which albumin promotes wound healing and reduces flap complications. Therefore, serum albumin levels in patients undergoing local flap transfer should be regulated to the normal range whenever possible to minimize adverse flap outcomes.
In our study, bone invasion was screened as an independent risk factor for complications of local flaps when multifactorial logistics regression was performed. Few previous investigators have seen this as an influential factor in flap prognosis, and we believe that the inclusion of this factor in the prediction model would facilitate a better and more accurate prediction of flap prognostic outcomes. When the lesion is resected to the bone, or even when the periosteum needs to be removed to ensure negative cut margins, the flap used to cover the defect will not have a blood supply from the base due to the lack of vascularity on the bone surface, which will increase the risk of graft ischemia. Free tissue grafts are an alternative but require a high level of microvascular expertise [20]. Artificial dermis can be applied when large areas of bone are exposed, but this also requires burring of the bone until there is sufficient bleeding for sarcomere to obtain a well-vascularized wound bed [25]. The blood flow of a local flap is not entirely dependent on the base, but mainly on the tip, which makes it an option for defect repair when the resection depth reaches the bone. However, again, local flap transposition over bone faces a higher risk of poor outcomes due to the poor blood supply to the periosteal surface.
We also found that smoking was detrimental to normal flap healing, which is consistent with previous study results. Smoking can lead to more complications, and the mechanism may be related to the induction of skin vasoconstriction and increased platelet aggregation. In a report by Hwang et al [11], the incidence of necrosis, hematoma, and fat necrosis after flap grafting was higher in smokers than in nonsmokers. Wang et al [12] demonstrated that both current and previous smoking can contribute to the development of acute complications after flap surgery. The mechanisms by which smoking is detrimental to tissue grafting have also been extensively studied: nicotine is thought to have adrenergic effects that induce peripheral vasoconstriction, thereby decreasing tissue blood flow, oxygen tension, and aerobic metabolism [22,23]. In an animal study, Lawrence et al [24] observed a significant decrease in flap survival in rats exposed to cigarette smoke, supporting the idea that smoking after surgery is also detrimental to flap survival.
Another factor considered is patient weight. In the present study, due to higher patient age and history of tumors, patients often did not reach the criteria of overweight in terms of BMI, so it is inaccurate to conclude on this basis that obesity was a risk factor. We did not classify the overall BMI of patients as normal, overweight, or obese. Instead, we used it as a numerical variable and, after testing normality, we applied the
During this study, the association between the size of the defect area and the risk of postoperative complications was quantified to more accurately predict the extent to which an increase in defect size affected the rate of complications. It is easy to understand that the defect area becomes a predictor of prognosis in local flap surgery. A larger defect area implies a larger flap area and a more distant proximal tip of the flap from the distal marginal tissues, which poses a challenge to the blood supply to the distal tissues of the flap. Also, the marginal tissues will need to establish de novo capillaries with the surrounding tissues or base to obtain oxygen supply. Defects and flap size were also found to be associated with postoperative complications of flap reconstruction in a study by Lee et al [26].
The results of our study showed a higher risk of postoperative complications in patients undergoing the second surgery than in those undergoing an initial surgery. This can be easily explained as follows. The blood supply to the flap is affected by the second surgery due to the destruction of local blood vessels during the initial surgery, the probability of complications, such as infection and delayed healing are increased, and the tension of the surrounding tissues is increased by performing multiple local flap translocations, which is also a risk factor [27]. Although the variable of secondary surgery was excluded during multifactorial logistic regression, we reintroduced it into the model, considering the prevalence of secondary surgery in the removal of body surface tumors. The timing of secondary surgery should be chosen more carefully to account for the limitations of the first surgery and the evolution of the patient’s general condition. In the vast majority of our cases, secondary surgery was undertaken because postoperative pathology after the first conventional excision of the lesion suggested unexpected malignancy or the presence of malignant residual tumor at the margins of the excised specimen, making a second extended excision and local flap transfer necessary.
In fact, there are more factors than just patient-related factors that affect flap outcomes. A study by Kraemer et al [28] showed that a decrease in peripheral temperature significantly reduced mean microcirculatory capillary blood flow, which led to arterial thrombosis or venous compromise. Another factor is the method of packing. In order for the flap to fit securely to the base, we usually applied appropriate pressure bandaging, and care must be taken not to compress the tip of the flap, which is an important source of blood supply to the flap. The level of care has also been reported to have an impact on the prognosis of the flap [29]. More factors are still to be discovered.
There were limitations to our study. For example, due to imperfect clinical data, we were unable to obtain an accurate geometry of the defect remaining after lesion excision. Therefore, the same defect area with different geometries would result in different flap designs, such as a narrow-shaped defect, implying a larger aspect ratio of the flap, which would put pressure on the distal blood supply to the flap. Nevertheless, the model we developed is still of good clinical interest.
Conclusions
In this study, we established a predictive model containing 6 variables, facilitating the identification and targeted intervention of patients at high risk of flap complications after surgery.
Figures
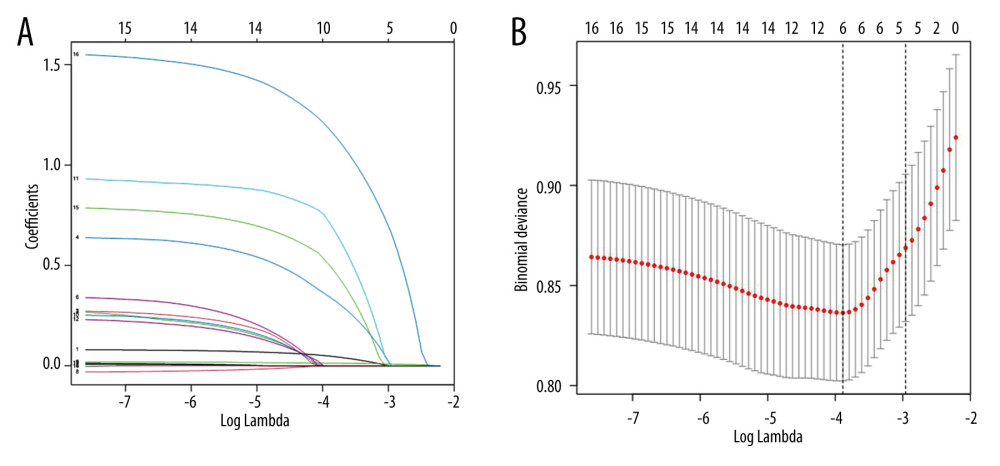 Figure 1. Predictor selection using a LASSO logistic regression model. (A) Penalty profile of scalar coefficients of 16 possible influencing factors. The 5-fold cross-validation of the minimum criterion was used to identify the optimal penalty coefficient in the LASSO model. (B) A dotted vertical line is drawn at the best value using the minimum standard and 1 standard error of the minimum standard (1-SE standard). Six features with non-zero coefficients resulted in the optimal lambda. Figure created with R software (version 4.2.0).
Figure 1. Predictor selection using a LASSO logistic regression model. (A) Penalty profile of scalar coefficients of 16 possible influencing factors. The 5-fold cross-validation of the minimum criterion was used to identify the optimal penalty coefficient in the LASSO model. (B) A dotted vertical line is drawn at the best value using the minimum standard and 1 standard error of the minimum standard (1-SE standard). Six features with non-zero coefficients resulted in the optimal lambda. Figure created with R software (version 4.2.0). 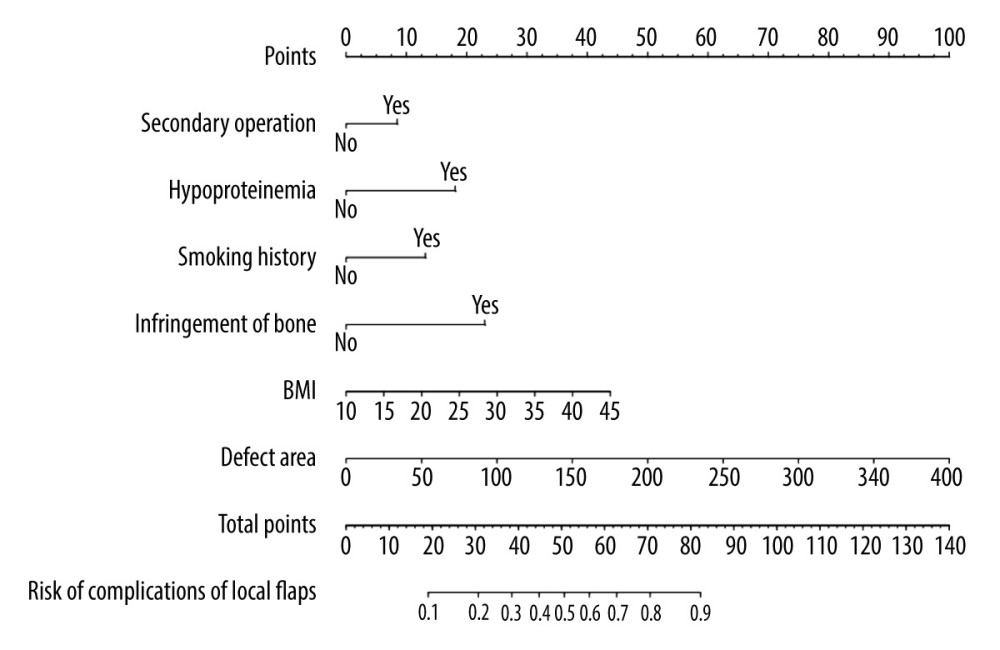 Figure 2. The nomogram for complications of the local flap is shown. The complications of the local flap risk nomogram were developed by incorporating the following characteristics: secondary operation, hypoproteinemia, smoking history, infringement of bone, body mass index, and defect area. Figure created with R software (version 4.2.0).
Figure 2. The nomogram for complications of the local flap is shown. The complications of the local flap risk nomogram were developed by incorporating the following characteristics: secondary operation, hypoproteinemia, smoking history, infringement of bone, body mass index, and defect area. Figure created with R software (version 4.2.0). 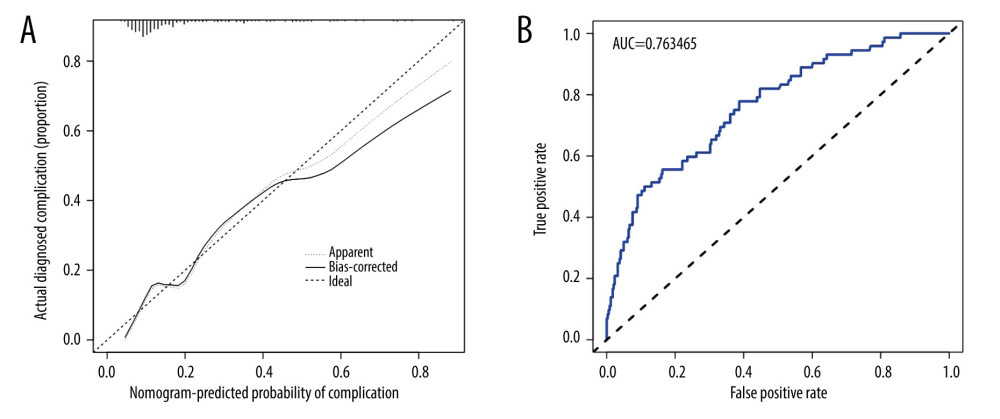 Figure 3. Internal validation of the nomogram. (A) Calibration diagram of the line diagram. The Y-axis is the actual incidence of complications diagnosis. The X-axis is the complication’s predicted risk. The dashed diagonal line represents the perfect prediction of the ideal model. The solid line shows the bias correction performance of the nomogram, whereas the dotted line closer to the diagonal shows a better prediction. (B) Area under the receiver operating characteristic curve analysis was used to determine the accuracy of the identification model for complications. Figure created with R software (version 4.2.0).
Figure 3. Internal validation of the nomogram. (A) Calibration diagram of the line diagram. The Y-axis is the actual incidence of complications diagnosis. The X-axis is the complication’s predicted risk. The dashed diagonal line represents the perfect prediction of the ideal model. The solid line shows the bias correction performance of the nomogram, whereas the dotted line closer to the diagonal shows a better prediction. (B) Area under the receiver operating characteristic curve analysis was used to determine the accuracy of the identification model for complications. Figure created with R software (version 4.2.0). 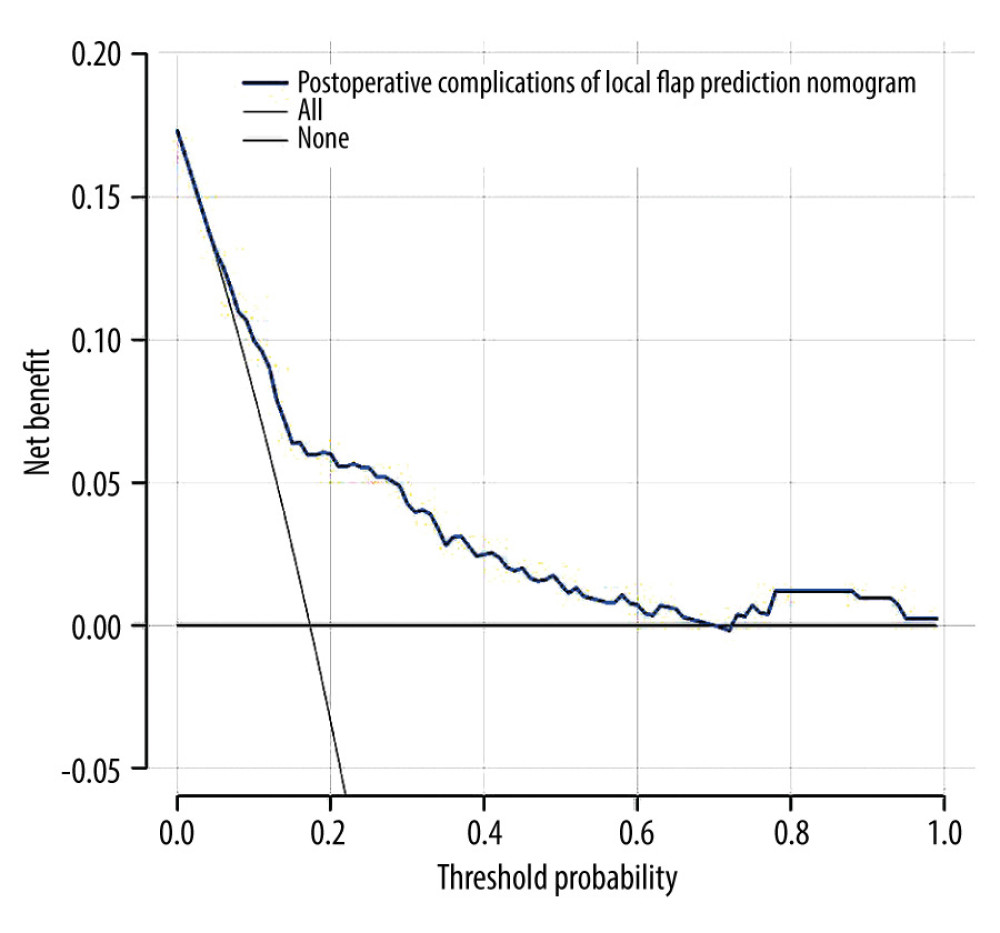 Figure 4. Decision curve analysis for the nomogram. Decision curve analysis demonstrates the clinical usefulness of the nomogram. The Y-axis measures the net benefit. The blue line is the nomogram predicting the risk of complications. The solid gray line assumes that complications will occur in all patients. The thin solid black line assumes that no patient will develop complications. In this analysis, the decision curve provided greater net benefits across the range of 4% to 69%. Figure created with R software (version 4.2.0).
Figure 4. Decision curve analysis for the nomogram. Decision curve analysis demonstrates the clinical usefulness of the nomogram. The Y-axis measures the net benefit. The blue line is the nomogram predicting the risk of complications. The solid gray line assumes that complications will occur in all patients. The thin solid black line assumes that no patient will develop complications. In this analysis, the decision curve provided greater net benefits across the range of 4% to 69%. Figure created with R software (version 4.2.0). References
1. Kruter L, Rohrer T, Advancement flaps: Dermatol Surg, 2015; 41(10); S239-46
2. Ito H, Ueno T, Suga H, Risk factors for skin flap necrosis in breast cancer patients treated with mastectomy followed by immediate breast reconstruction: World J Surg, 2019; 43(3); 846-52
3. Fertsch S, Munder B, Andree C, Risk factor analysis for flap and donor site related complications in 1274 DIEP flaps – retrospective single center study: Chirurgia (Bucharest, Romania: 1990), 2021; 116(2 Suppl); 5-15
4. Chang DW, Wang B, Robb GL, Effect of obesity on flap and donor-site complications in free transverse rectus abdominis myocutaneous flap breast reconstruction: Plast Reconstr Surg, 2000; 105(5); 1640-48
5. Heidekrueger PI, Fritschen U, Moellhoff N, Impact of body mass index on free DIEP flap breast reconstruction: A multicenter cohort study: J Plast Reconstr Aesthet Surg, 2021; 74(8); 1718-24
6. Hultman CS, Daiza S, Skin-sparing mastectomy flap complications after breast reconstruction: Review of incidence, management, and outcome: Ann Plast Surg, 2003; 50(3); 249-55
7. Crippen MM, Brady JS, Mozeika AM, Impact of body mass index on operative outcomes in head and neck free flap surgery: Otolaryngol Head Neck Surg, 2018; 159(5); 817-23
8. Fang Z, Tian Z, Zhang C, Risk factors for pedicle flap complications in 251 elderly Chinese patients who underwent oral and maxillofacial reconstruction: J Oral Maxillofac Surg, 2016; 74(10); 2073-80
9. Shum J, Markiewicz MR, Park E, Low prealbumin level is a risk factor for microvascular free flap failure: J Oral Maxillofac Surg, 2014; 72(1); 169-77
10. Xu H, Han Z, Ma W, Perioperative albumin supplementation is associated with decreased risk of complications following microvascular head and neck reconstruction: J Oral Maxillofac Surg, 2021; 79(10); 2155-61
11. Hwang K, Son JS, Ryu WK, Smoking and flap survival: Plast Surg, 2018; 26(4); 280-85
12. Wang CY, Dudzinski J, Nguyen D, Association of smoking and other factors with the outcome of mohs reconstruction using flaps or grafts: JAMA Facial Plast Surg, 2019; 21(5); 407-13
13. Kinsella JB, Rassekh CH, Wassmuth ZD, Smoking increases facial skin flap complications: Ann Otol Rhinol Laryngol, 1999; 108(2); 139-42
14. Zhou W, Zhang WB, Yu Y, Risk factors for free flap failure: A retrospective analysis of 881 free flaps for head and neck defect reconstruction: International J Oral Maxillofac Surg, 2017; 46(8); 941-45
15. Bozikov K, Arnez ZM, Factors predicting free flap complications in head and neck reconstruction: J Plast Reconstr Aesthet Surg, 2006; 59(7); 737-42
16. Liu S, Zhang W-b, Yu Y, Free flap transfer for pediatric head and neck reconstruction: What factors influence flap survival?: Laryngoscope, 2019; 129(8); 1915-21
17. Gong X, Cui J, Jiang Z, Risk factors for pedicled flap necrosis in hand soft tissue reconstruction: A multivariate logistic regression analysis: ANZ J Surg, 2018; 88(3); E127-E31
18. Sauerbrei W, Royston P, Binder H, Selection of important variables and determination of functional form for continuous predictors in multivariable model building: Stat Med, 2007; 26(30); 5512-28
19. Candiano G, Petretto A, Bruschi M, The oxido-redox potential of albumin Methodological approach and relevance to human diseases: J Proteomics, 2009; 73(2); 188-95
20. Sosin M, De la Cruz C, Bojovic B, Microsurgical reconstruction of complex scalp defects: An appraisal of flap selection and the timing of complications: J Craniofac Surg, 2015; 26(4); 1186-91
21. Park S, Han KT, Kim MC, Lim JS, Immediate near-total scalp reconstruction with artificial dermis on exposed calvarium: Arch Craniofac Surg, 2016; 17(4); 233-36
22. Jensen JA, Goodson WH, Hopf HW, Hunt TK, Cigarette smoking decreases tissue oxygen: Arch Surg (Chicago, Ill: 1960), 1991; 126(9); 1131-34
23. Sorensen LT, Jorgensen S, Petersen LJ, Acute effects of nicotine and smoking on blood flow, tissue oxygen, and aerobe metabolism of the skin and subcutis: J Surg Res, 2009; 152(2); 224-30
24. Lawrence WT, Murphy RC, Robson MC, Heggers JP, The detrimental effect of cigarette smoking on flap survival: An experimental study in the rat: Br J Plast Surg, 1984; 37(2); 216-19
25. Abedi N, Ho AL, Knox A, Predictors of mastectomy flap necrosis in patients undergoing immediate breast reconstruction: A review of 718 patients: Ann Plast Surg, 2016; 76(6); 629-34
26. Lee ZH, Abdou SA, Ramly EP, Larger free flap size is associated with increased complications in lower extremity trauma reconstruction: Microsurgery, 2020; 40(4); 473-78
27. Liu S, Zhang W-b, Yu Y, Free flap transfer for pediatric head and neck reconstruction: What factors influence flap survival?: Laryngoscope, 2019; 129(8); 1915-21
28. Kraemer R, Lorenzen J, Knobloch K, Free flap microcirculatory monitoring correlates to free flap temperature assessment: J Plast Reconstr Aesthet Surg, 2011; 64(10); 1353-58
29. Varadarajan VV, Arshad H, Dziegielewski PT, Head and neck free flap reconstruction: what is the appropriate post-operative level of care?: Oral Oncol, 2017; 75; 61-66
Figures
Figure 1. Predictor selection using a LASSO logistic regression model. (A) Penalty profile of scalar coefficients of 16 possible influencing factors. The 5-fold cross-validation of the minimum criterion was used to identify the optimal penalty coefficient in the LASSO model. (B) A dotted vertical line is drawn at the best value using the minimum standard and 1 standard error of the minimum standard (1-SE standard). Six features with non-zero coefficients resulted in the optimal lambda. Figure created with R software (version 4.2.0).Figure 2. The nomogram for complications of the local flap is shown. The complications of the local flap risk nomogram were developed by incorporating the following characteristics: secondary operation, hypoproteinemia, smoking history, infringement of bone, body mass index, and defect area. Figure created with R software (version 4.2.0).Figure 3. Internal validation of the nomogram. (A) Calibration diagram of the line diagram. The Y-axis is the actual incidence of complications diagnosis. The X-axis is the complication’s predicted risk. The dashed diagonal line represents the perfect prediction of the ideal model. The solid line shows the bias correction performance of the nomogram, whereas the dotted line closer to the diagonal shows a better prediction. (B) Area under the receiver operating characteristic curve analysis was used to determine the accuracy of the identification model for complications. Figure created with R software (version 4.2.0).Figure 4. Decision curve analysis for the nomogram. Decision curve analysis demonstrates the clinical usefulness of the nomogram. The Y-axis measures the net benefit. The blue line is the nomogram predicting the risk of complications. The solid gray line assumes that complications will occur in all patients. The thin solid black line assumes that no patient will develop complications. In this analysis, the decision curve provided greater net benefits across the range of 4% to 69%. Figure created with R software (version 4.2.0). Tables
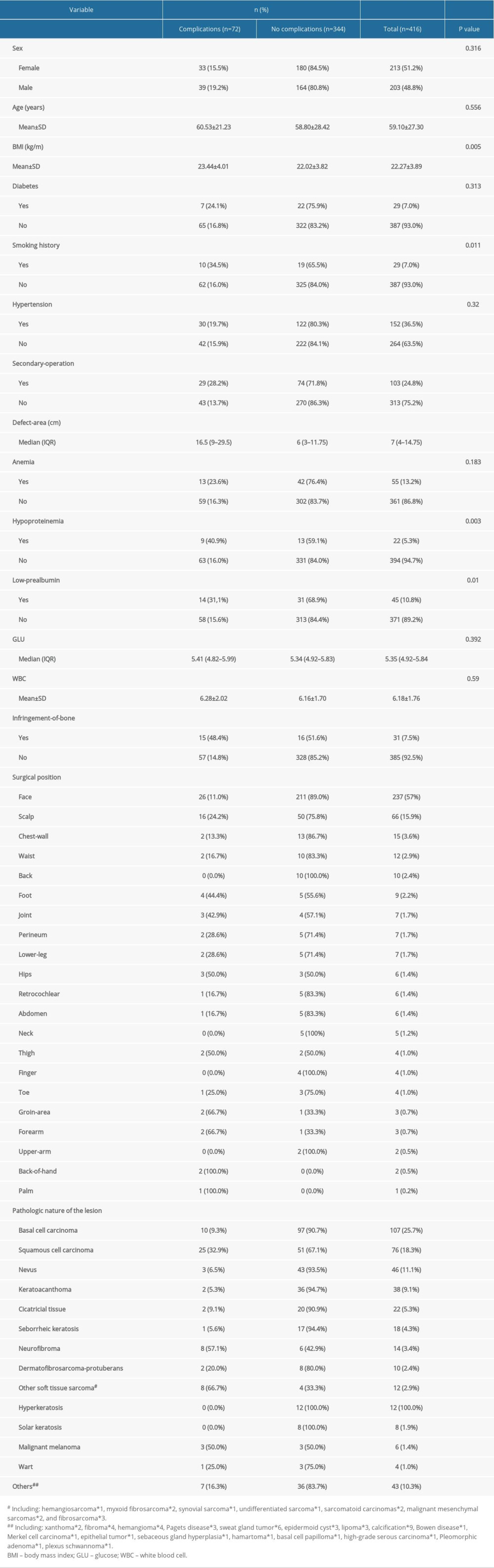 Table 1. Demographic and clinical characteristics of the complications group and no complications group.
Table 1. Demographic and clinical characteristics of the complications group and no complications group. Table 2. Distribution of postoperative complications.
Table 2. Distribution of postoperative complications. Table 3. Prediction factors for postoperative complications of local flap.Table 1. Demographic and clinical characteristics of the complications group and no complications group.Table 2. Distribution of postoperative complications.Table 3. Prediction factors for postoperative complications of local flap.
Table 3. Prediction factors for postoperative complications of local flap.Table 1. Demographic and clinical characteristics of the complications group and no complications group.Table 2. Distribution of postoperative complications.Table 3. Prediction factors for postoperative complications of local flap. In Press
Meta-Analysis
Effectiveness of Cardiac Telerehabilitation in Improving Functional Capacity, Quality Of Life and Cardiovas...Med Sci Monit In Press; DOI: 10.12659/MSM.953366
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,468
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,759,966
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,248
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,898
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387