08 November 2022: Database Analysis
Clinical Characteristics and Factors Associated with In-Hospital Mortality in 66 755 Patients Hospitalized Due to Diabetes in Poland, January to December 2019
Kuba Sękowski1ABCDEF*, Justyna Grudziąż-Sękowska1ADE, Paweł Goryński2ABE, Jarosław Pinkas1ADE, Mateusz Jankowski1ACEDOI: 10.12659/MSM.938550
Med Sci Monit 2022; 28:e938550






Abstract
BACKGROUND: The global burden of diabetes mellitus is increasing, and diabetes poses a serious problem for the healthcare system. We aimed to characterize patients hospitalized due to diabetes in Poland in 2019 and identify factors associated with the risk of in-hospital death and prolonged hospitalization.
MATERIAL AND METHODS: Data on all patients hospitalized due to diabetes in Poland in 2019 were taken from hospital discharge records collected by the National Institute of Public Health, Warsaw, Poland. The presence of comorbidities, in-hospital mortality rate, and duration of hospitalization were analyzed separately for type 1 and type 2 diabetes.
RESULTS: In 2019, a total of 28 617 patients were admitted to the hospital due to type 1 diabetes and 38 138 patients due to type 2 diabetes. The prevalence of comorbidities was 55.2% among patients with type 1 diabetes and 78.9% among those with type 2 diabetes. The in-hospital mortality rates were 2.1% and 3.3%, respectively. For emergency admissions, the in-hospital mortality rate was 4.0% and 4.5%, respectively. Over 30% of patients were hospitalized for more than 7 days. Older age and respiratory diseases were the most critical factors associated with higher risk of in-hospital death in patients with type 1 or type 2 diabetes (P<0.001). Male sex, age, and presence of at least 1 comorbidity were associated (P<0.001) with a higher risk of prolonged hospitalization.
CONCLUSIONS: Effective management of respiratory diseases in patients hospitalized due to diabetes, especially those admitted in an emergency, seems crucial to reduce the risk of in-hospital death.
Keywords: Diabetes Mellitus, Hospital Mortality, Hospitalization, Poland, Registries, Humans, Male, Diabetes Mellitus, Type 2, Diabetes Mellitus, Type 1, Comorbidity
Background
Diabetes mellitus is a chronic non-communicable disease characterized by prolonged hyperglycemia that can lead to long-term health complications [1,2]. It is estimated that more than 400 million people worldwide have diabetes [2]. The most common (>90%) is type 2 diabetes, which usually occurs in adults over 40 years of age [2–4]. Being overweight or obese is the significant risk factor of type 2 diabetes [5,6]. Approximately 5% to 10% of patients with diabetes have type 1 diabetes [2,7]. The most common age at diagnosis of type 1 diabetes is between the ages of 4 to 6 years and early puberty (10 to 14 years) [7,8]. Because the exact cause of type 1 diabetes is unknown, genetics and environmental factors are considered significant risk factors for developing type 1 diabetes [9,10].
Diabetes is mainly managed in outpatient settings and requires a high level of therapeutic compliance by patients [11,12]. Patients with diabetes must make regular blood sugar checks and keep blood sugar levels as close to target as possible to prevent or delay diabetes-related complications [13]. Uncontrolled diabetes causes life-threatening events and requires hospitalization [14]. Most patients with diabetes have comorbidities that can also influence the risk of hospitalization [15]. Moreover, diabetes-related hospitalization can include scheduled admissions to diagnose the patient’s health condition, especially in the case of children with newly diagnosed type 1 diabetes. It is estimated that patients with diabetes have a 3 times higher risk of hospitalization than individuals without diabetes [16,17]. Diabetes-related hospitalizations generate significant economic costs [18].
The estimated prevalence of diabetes in Europe varies from 15.3%, in Germany, to 4.4%, in Ireland [19]. Diabetes poses a severe problem for the healthcare systems in Central and Eastern European countries, like Poland [19,20]. After the communist collapse in 1989, Poland’s social, economic, and demographic changes evoked lifestyle changes that significantly contributed to the increase in diabetes incidence [21]. The estimated crude prevalence of diabetes in Poland is 7.0% [22]. However, it is estimated that between 2010 and 2030, the prevalence of diabetes in Poland will rise by at least 20% [20]. In Poland, more than 70 000 diabetes-related hospitalizations are reported annually [23,24].
Public registries can generate national data on diabetes-related hospitalizations and their course and outcome. These data can be helpful for clinicians and policymakers to improve the management of diabetes in Poland. However, a limited amount of research on diabetes is based on national registries [22–26]. Most of the previously published data are focused on epidemiological analyses aimed at the prevalence of diabetes [22,25]. Goryński et al showed significant differences in the in-hospital mortality rate by sex, age, or year of admission [24]. Kozioł et al analyzed the predictors of rehospitalization and post-discharge death (up to 90 days) among the patients hospitalized due to all types of diabetes [26]. However, there is a lack of data on the impact of comorbidities on the risk of in-hospital death among patients hospitalized due to type 1 or type 2 diabetes. Moreover, factors associated with prolonged hospitalization among patients with type 1 and type 2 diabetes have not been studied yet.
Therefore, this study aimed to characterize patients hospitalized due to diabetes from January to December 2019, and to identify factors associated with the risk of in-hospital death and prolonged hospitalization among patients hospitalized due to diabetes.
Material and Methods
DATA SOURCE:
This was a retrospective database analysis. Data on patients hospitalized due to diabetes were taken from the hospital discharge records collected and aggregated by the National Institute of Public Health-National Institute of Hygiene (NIZP-PZH). Data collection is carried out as part of the population-based hospital morbidity study [27], and the data on numbers and the reason for hospitalization are used for the annual publications in Public Statistics of the Republic of Poland. Public and private hospitals in Poland (with the exclusion of psychiatric hospitals) are legally obligated to report hospitalization data using discharge report templates provided by the NIZP-PZH. Hospital discharge records are anonymous. The template includes the following data: sex, age, location of place of residence, hospital admission, and discharge, as well as the primary (reason for hospitalization) and secondary (comorbidities) diagnosis. Moreover, data on the outcome of hospitalization, whether death or survival, are provided. Data on medical conditions and diagnoses are reported by physicians using the ICD-10 classification [28]. All the hospitals were trained in the data reporting process, and the coding rules are constantly updated to maintain the data collection quality. Data submitted by the hospitals are regularly checked by the scientific team tasked with managing the registry [27].
DIABETES REPORTING AND OUTCOMES:
In this database analysis, all patients hospitalized due to diabetes in 2019 (diabetes was declared as a cause of hospitalization in discharge reports) were included. Patients hospitalized due to type 1 diabetes (E10 insulin-dependent diabetes mellitus) and type 2 diabetes (E11 non-insulin-dependent diabetes mellitus) were identified through the ICD-10 admission diagnosis codes. When a patient was hospitalized due to diabetes complications, the primary reason for hospitalization was reported as diabetes and the diabetes exacerbation was defined as a coexisting disease.
The inclusion criteria were diabetes diagnosed by a doctor; hospitalization due to diabetes; and diabetes as a reason for hospitalization, according to the discharge report.
The exclusion criteria were patients diagnosed with diabetes but hospitalized due to health reasons other than diabetes; E12 malnutrition-related diabetes mellitus; and E13 other specified diabetes mellitus.
In-hospital mortality was defined as the percentage of fatal cases out of all hospitalizations due to diabetes. Moreover, additional analysis was carried out for the duration of hospitalization. Prolonged hospitalization was defined as hospitalization for more than 7 days.
The following groups of comorbidities were analyzed: (1) endocrine, nutritional, metabolic diseases (E00-9; E15-90; other than diabetes); cardiovascular diseases (I00-99); genitourinary disorders (N00-99); diseases of the digestive system (K00-93); respiratory diseases (J00-99); diseases of the skin and subcutaneous tissue (L00-99); and diseases of the nervous system (G00-99).
STATISTICAL ANALYSIS:
The data were analyzed with SPSS v.28 (IBM Corp, Armonk, NY, USA). The normality of distributions of continuous variables was assessed by the Shapiro-Wilk test. The statistical significance of differences between mean values of continuous variables was analyzed by the Kruskal-Wallis test. Descriptive statistics (counts, percentages) were used to present the distribution of categorical variables. Moreover, the chi-square test of independence was used to compare categorical variables. Associations between personal characteristics (sex, age, presence of comorbidities) and (1) outcome of hospitalization (death/survival), and (2) duration of hospitalization (≤7 days/8 days and over) were analyzed using multivariable logistic regression models. Data were analyzed separately for emergency and scheduled admissions. As there were no deaths among children with diabetes, the pediatric population (0–18 years) was excluded from the analysis of factors associated with in-hospital mortality. The odds ratio (OR) and 95% confidence intervals (95% CI) were used to measure the strength of association. The statistical significance level was set at
ETHICS:
The datasets used in this study were anonymous. Patient consent was waived because this study was a retrospective database analysis. The study protocol was approved by the Ethics Board of the Centre of Postgraduate Medical Education in Warsaw, Poland (approval no. 70/2022).
Results
HOSPITALIZATIONS DUE TO DIABETES IN 2019:
In 2019, a total of 28 617 patients were admitted to the hospital due to type 1 diabetes, and 38 138 patients were admitted to the hospital due to type 2 diabetes. The highest number of diabetes-related hospitalization was observed in January, and the lowest was in December (Table 1). Most of the hospitalizations (58.7% due to type 1 diabetes and 68.1% due to type 2 diabetes) were emergency hospital admissions (Table 1). The average duration of hospitalization was 7.2±8.7 days (a median of 5 days) for type 1 diabetes and 7.7±7.5 days (a median of 6 days) for type 2 diabetes. Duration of hospitalization (P<0.001) differed by the admission date, wherein the lowest period of hospitalization was observed in December (Table 1). In December, 82.2% of patients hospitalized due to type 1 diabetes and 83.5% of patients hospitalized due to type 2 diabetes were discharged before December 24. Most of the patients (84.5%) with type 1 diabetes stayed in 1 ward during hospitalization, 14.1% of patients were admitted to 2 wards, and 1.4% were hospitalized in at least 3 wards. Most children hospitalized due to type 1 diabetes (41.2%) were admitted to pediatric diabetology wards, 24.6% were admitted to pediatrics wards, and 18.6% were admitted to pediatric endocrinology wards. Over one-third of adults hospitalized due to type 1 diabetes were admitted to internal medicine wards (37.5%), 17.6% were admitted to emergency departments, and only 13% were admitted to diabetology wards. Most patients hospitalized due to type 2 diabetes (84.2%) stayed in 1 ward during the hospitalization, 14.6% were hospitalized in 2 wards, and 1.4% were hospitalized in at least 3 wards. Over one-half of patients hospitalized due to type 2 diabetes (52%) were admitted to internal medicine wards, 14.1% were admitted to emergency departments, and 8.7% were admitted to diabetology wards.
Of the 28 617 patients hospitalized due to type 1 diabetes, 609 deaths were reported (in-hospital mortality rate, 2.1%), without seasonal differences (P=0.4) in the in-hospital mortality rate. Of 38 138 patients hospitalized due to type 2 diabetes, 1277 deaths were reported (in-hospital mortality rate, 3.3%). Among patients hospitalized due to type 2 diabetes, the highest in-hospital mortality rate was observed during the winter season, with 4% in January and February (P=0.03). Details are presented in Table 1.
CLINICAL CHARACTERISTICS OF PATIENTS HOSPITALIZED DUE TO TYPE 1 DIABETES:
The mean age of patients hospitalized due to type 1 diabetes was 43.0±25.7 years. The in-hospital mortality rate was significantly higher in female (F) than male (M) patients (F: 2.3% vs M: 2.0%; P=0.03). Among adults hospitalized due to type 1 diabetes, the in-hospital mortality rate was 4.0% for emergency admissions and 0.8% for scheduled admissions. Almost one-third of patients hospitalized due to type 1 diabetes were under 18 years of age (Table 2). More than one-half of patients (55.2%) hospitalized due to type 1 diabetes had comorbidities, with significant differences by sex (M: 52.7%; F: 57.1%; P<0.001). There were significant differences in the prevalence of comorbidities between fatal cases and survivors (Table 2).
CLINICAL CHARACTERISTICS OF PATIENTS HOSPITALIZED DUE TO TYPE 2 DIABETES:
The mean age of patients admitted due to type 2 diabetes was 67.7±13.9 years. The in-hospital mortality rate was significantly higher among females (F: 3.8% vs M: 2.9%; P<0.001). Among adults hospitalized due to type 2 diabetes, the in-hospital mortality rate was 4.5% for emergency admissions and 0.8% for scheduled admissions. More than three-fourths of patients (76.7%) were over 60 years of age and had comorbidities (78.9%). The percentage of patients with at least 1 chronic condition (except diabetes) was significantly higher among females than males (F: 80.8% vs M: 77.1%; P<0.001). Almost half of the patients (49.0%) hospitalized due to type 2 diabetes had at least 1 cardiovascular disease and over one-fourth of patients (27.7%) had at least 1 endocrine disease (Table 3). Almost one-tenth of patients hospitalized due to type 2 diabetes had a digestive system (8.8%) or skin and subcutaneous tissue (9.1%) disease.
There were significant differences in the prevalence of comorbidities between fatal cases and survivors (Table 3).
FACTORS ASSOCIATED WITH THE IN-HOSPITAL MORTALITY IN DIABETES:
Findings from the multivariable logistic regression analysis are presented in Tables 4 and 5.
Among adult patients hospitalized in an emergency due to type 1 diabetes, age (OR: 1.05; 95% CI: 1.04–1.05; P<0.001), presence of at least 1 disease of the respiratory system (OR: 4.40; 95% CI: 3.44–5.62; P<0.001), cardiovascular disease (OR: 2.08; 95% CI: 1.73–2.51; P<0.001), genitourinary disorder (OR: 2.14; 95% CI: 1.74–2.62; P<0.001), or disease of the skin and subcutaneous tissue (OR: 1.52; 95% CI: 1.19–1.94; P<0.001) were significantly associated with the higher odds for in-hospital death (Table 5). Among adults hospitalized on schedule due to type 1 diabetes, only age (OR: 1.06; 95% CI: 1.03–1.09; P<0.001), presence of at least 1 disease of the respiratory system (OR: 8.95; 95% CI: 4.23–18.95; P<0.001), and cardiovascular disease (OR: 3.16; 95% CI: 1.65–6.04; P<0.001) were significantly associated with the higher odds for in-hospital death (Table 4).
Among adults admitted due to type 2 diabetes (Table 5), age (OR: 1.06; 95% CI: 1.05–1.07; P<0.001), presence of at least one disease of the respiratory system (OR: 4.65; 95% CI: 4.03–5.37; P<0.001), cardiovascular disease (OR: 1.31; 95% CI: 1.16–1.48; P<0.001), genitourinary disorder (OR: 1.53; 95% CI: 1.35–1.74; P<0.001), or condition of the skin and subcutaneous tissue (OR: 1.61; 95% CI: 1.34–1.94; P<0.001) were significantly associated with the higher risk of in-hospital mortality in diabetes. Moreover, presence of the neurological diseases (OR: 1.66; 95% CI: 1.19–2.30; P=0.003) was also significantly associated with the higher risk of in-hospital mortality in type 2 diabetes (Table 5). There were no differences in factors related to the risk of in-hospital mortality in type 2 diabetes between scheduled and emergency hospitalizations, except for the neurological diseases that were associated with a higher risk of death only in the case of emergency hospitalizations (Table 5).
FACTORS ASSOCIATED WITH PROLONGED HOSPITALIZATION:
Among patients hospitalized due to type 1 diabetes, 68.6% were hospitalized for up to 7 days. Most patients with type 2 diabetes (64.4%) were hospitalized for up to 7 days. Among children hospitalized due to type 1 diabetes (Table 6), the presence of at least 1 comorbidity significantly increased the odds for prolonged hospitalization among those hospitalized on schedule (OR: 1.74; 95% CI: 1.34–2.24; P<0.001). The risk of prolonged hospitalization among children hospitalized on schedule and in an emergency setting decreased with age (Table 6). Among adults hospitalized due to type 1 diabetes, at least 1 comorbidity, older age, and male sex were significantly associated with a higher risk of prolonged hospitalization (Table 6). Among adults hospitalized due to type 2 diabetes, the presence of at least 1 comorbidity (OR: 1.36; 95% CI: 1.29–1.43; P<0.001), older age (OR: 1.02; 95% CI: 1.01–1.02; P<0.001), and male sex (OR: 1.12; 95% CI: 1.07–1.17; P<0.001) were significantly associated with a higher risk of prolonged hospitalization (Table 7). Factors related to the risk of prolonged hospitalization differed by type of admission (Table 7).
Discussion
This public registry-based study presented the detailed clinical characteristics of 66 755 patients hospitalized due to diabetes type 1 or type 2. This study provided data on comorbidities among patients hospitalized due to diabetes, wherein the prevalence of comorbidities was higher among female patients in both types of diabetes. The presence of respiratory diseases was the most essential factor associated with the higher risk of in-hospital death among patients with diabetes. Moreover, factors related to prolonged hospitalization were identified.
Seasonal variations in hospital admissions were proven for cardiovascular, genitourinary, or respiratory diseases [29–31]. In the present study, the highest number of diabetes-related hospitalizations (in both types of diabetes) was observed in January and the lowest in December. Moreover, December was identified as the month with the shortest duration of hospitalization. We can hypothesize, that due to the winter holidays and Christmas in the last week of December, physicians tend to discharge patients and new admissions are less likely to happen. Over 80% of patients with diabetes hospitalized in December were discharged before December 24, 2019. Among patients hospitalized due to type 2 diabetes, the highest in-hospital mortality rate was observed in January and February. We can hypothesize that the weather, air pollution, and limited psychical activity level during winter can increase the risk of in-hospital mortality among patients with type 2 diabetes [30,31].
Findings from this study showed that children with type 1 diabetes were admitted mainly to pediatric diabetology or endocrinology wards. We hypothesize that these hospitalizations were among newly diagnosed cases, as recommended by the national guidelines [32]. Most adults with diabetes were hospitalized in internal medicine wards, and less than one-tenth were admitted to diabetic wards. This finding confirms that diabetes is an interdisciplinary health problem.
In this study, emergency hospital admissions varied from 58.7% among patients with type 1 diabetes to 68.1% among patients with type 2 diabetes. Type 1 diabetes-related hospital admission may partially result from the national guidelines and may be related to newly diagnosed cases and “educational” hospitalizations, as observed by Grudziąż-Sękowska et al [33]. Nevertheless, the percentage of type 2 diabetes scheduled hospital admissions in Poland seems to be higher than in other high-income countries [19,34]. Such a high percentage of scheduled hospital admissions may result from poor diabetes management in outpatient settings, as accessibility to specialist treatment remains one of the critical problems of the Polish health system [35]. Policymakers and key stakeholders should consider revising the current standards of diabetes management and evaluating the effectiveness of diabetes management in particular outpatient clinics, as well as evaluating the effectiveness of diabetes management in particular outpatient clinics [36].
In this study, one-third of patients hospitalized due to type 1 diabetes were under 18 years of age, which is in line with the epidemiology data on the age of onset of type 1 diabetes [7,8]. The prevalence of comorbidities observed in this study (55.2%) was higher than reported in 2009 (53.4%), when a study based on a similar methodology was performed by Gajewska et al [23].
Findings from this study showed that more than three-fourths of patients hospitalized due to type 2 diabetes were more than 60 years of age. This finding aligns with data on diabetes-related hospital admission in other countries [6,37,38]. Between 2009 and 2019, the prevalence of comorbidities among patients with type 2 diabetes increased from 75.2% to 78.9% [23]. Both in 2009 and 2019, the prevalence of comorbidities in patients with diabetes was higher among female patients [23]. However, the prevalence of the endocrine, nutritional, and metabolic diseases among patients hospitalized due to diabetes was lower (27%) compared with global data on comorbidities in diabetic patients [39–41]. It is estimated that 30% to 60% of patients with type 2 diabetes have dyslipidemia [39,40], and most of them have overweight or obesity [41]. We can hypothesize that endocrine, nutritional, and metabolic disease were underreported. Retrospective analyses of electronic medical records in the United States revealed that an overwhelming percentage of patients had never had weight status documented during their hospital admission [42,43]. A similar phenomenon may occur in Poland and indicates an urgent need to improve the quality of data reporting, especially related to the weight status of hospitalized individuals.
Uncontrolled or poorly controlled diabetes can cause damage to vital organs, increase the risk of infection, and worsen outcomes of respiratory diseases [44–46]. Goryński et al showed that between 2010 and 2018, the type 1 diabetes in-hospital mortality rate increased from 1.49% to 2.2% among male patients and from 1.86% to 2.58% among female patients [24]. A similar phenomenon was observed among those hospitalized due to type 2 diabetes: between 2010 and 2018, the in-hospital mortality rate increased from 1.9% to 2.76% among male patients and from 2.37% to 3.37% among female patients [24]. Moreover, Kozioł et al showed that of 74 248 diabetes-related hospitalizations in 2017, 7.3% resulted in death within 90 days following discharge [26]. Findings from this study showed differences in in-hospital mortality rates in type 1 (2.1%) and type 2 (3.3%) diabetes. However, the in-hospital mortality rate was over 5 times higher among emergency admissions than scheduled admissions.
Out of 6 different groups of diseases analyzed in this study, respiratory diseases were the most important factor associated with the risk of in-hospital mortality in type 1 and type 2 diabetes. This finding underlines the importance of managing respiratory diseases in patients hospitalized due to diabetes. Physicians should take particular care of diabetes patients admitted to the hospital with respiratory diseases, as this group is at the most significant risk of in-hospital death.
Findings from this study showed the male sex was significantly associated with prolonged hospitalization in adults with type 1 diabetes. Moreover, male sex increased the risk of prolonged hospitalization in adults with type 2 diabetes with emergency admissions to the hospital. The differences in the duration of hospitalization according to patient sex require further investigations.
Clinicians and policymakers should consider the following practical implications of this study. First, the comprehensive clinical characteristics of patients hospitalized due to diabetes were presented. Comorbidities among patients with diabetes have a significant impact on disease management and outcomes. Characteristics of the factors associated with the risk of in-hospital death and prolonged hospitalization given in this study can be used by a clinician to screen diabetic patients admitted to the hospital and identify groups at higher risk of a fatal course of hospitalization. Moreover, the relatively high percentage of scheduled hospital admissions among patients with type 2 diabetes should be analyzed by policymakers to identify factors that influence insufficient ambulatory-based diabetes management in a fairly large group of patients. An enhancement of primary health care could reduce the number of potentially preventable hospitalizations.
Our study had several limitations. The scope of the analysis presented in this study was limited to data available in the public registry led by the NIZP-PZH. The analysis of comorbidities was limited to the whole group based on the ICD-10 codes, and the impact of individual diseases on the risk of in-hospital mortality or prolonged hospitalization was not assessed. As all the data were anonymous, an assessment of the post-discharge mortality rate was impossible. Moreover, data on the pharmacological treatment of patients were not available. The geographical distribution of hospital admissions was also missed.
Conclusions
In conclusion, this study showed that most patients hospitalized due to diabetes have comorbidities, and the prevalence of comorbidities was higher in female patients. Seasonal differences in the number of diabetes-related hospital admissions and the duration of hospitalization were observed. The presence of respiratory diseases was found to be the most essential factor associated with the higher risk of in-hospital death in patients hospitalized due to diabetes. Among patients with type 1 diabetes, factors associated with in-hospital death differed by type of admission (emergency or scheduled). However, these differences were not observed among patients with type 2 diabetes. Age and comorbidities were significantly associated with the duration of hospitalization.
Tables
Table 1. Diabetes-associated hospitalizations by month in Poland, January to December 2019.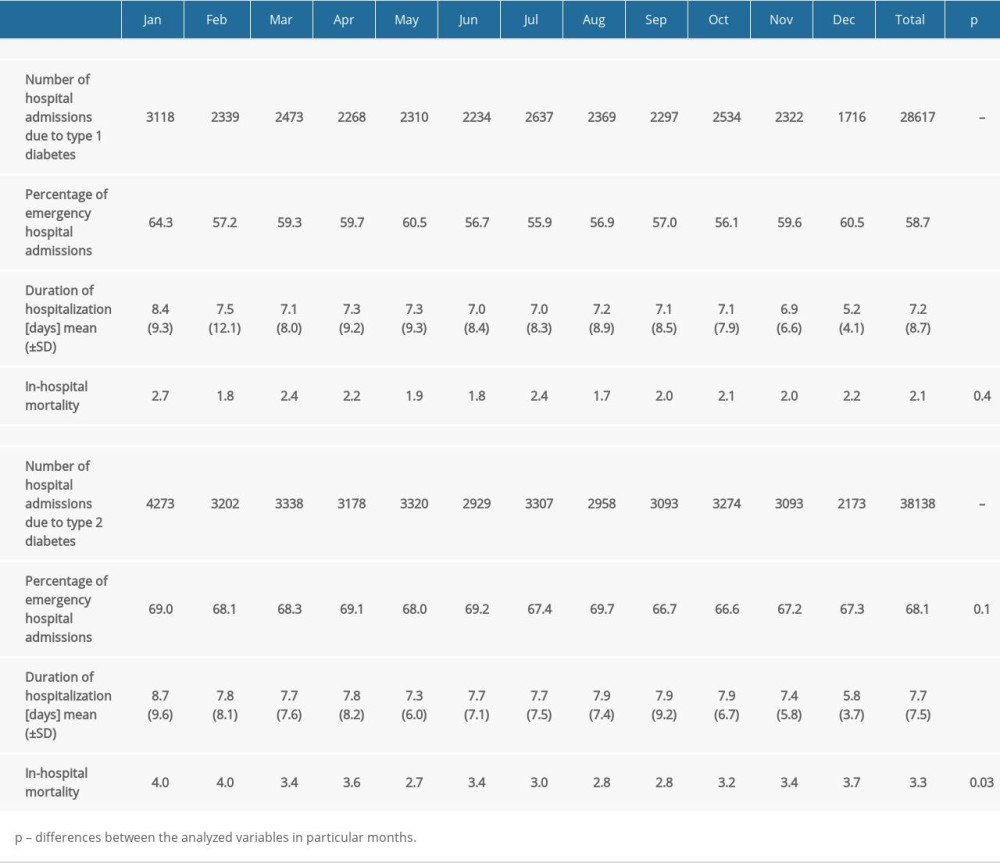 Table 2. Characteristics of 28 617 patients hospitalized due to type 1 diabetes in Poland, January to December 2019.
Table 2. Characteristics of 28 617 patients hospitalized due to type 1 diabetes in Poland, January to December 2019.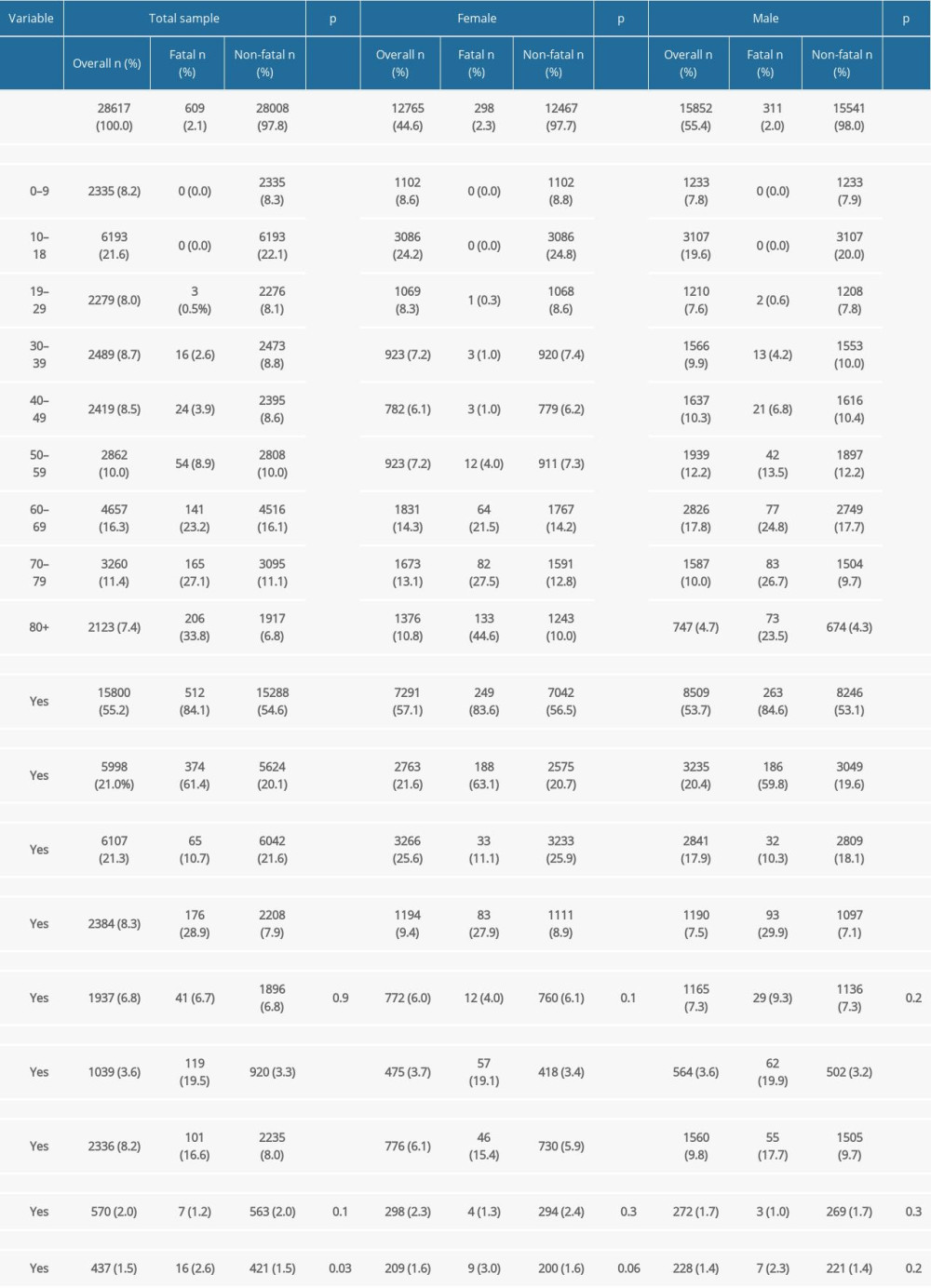 Table 3. Characteristics of 38 138 patients hospitalized due to type 2 diabetes in Poland, January to December 2019.
Table 3. Characteristics of 38 138 patients hospitalized due to type 2 diabetes in Poland, January to December 2019.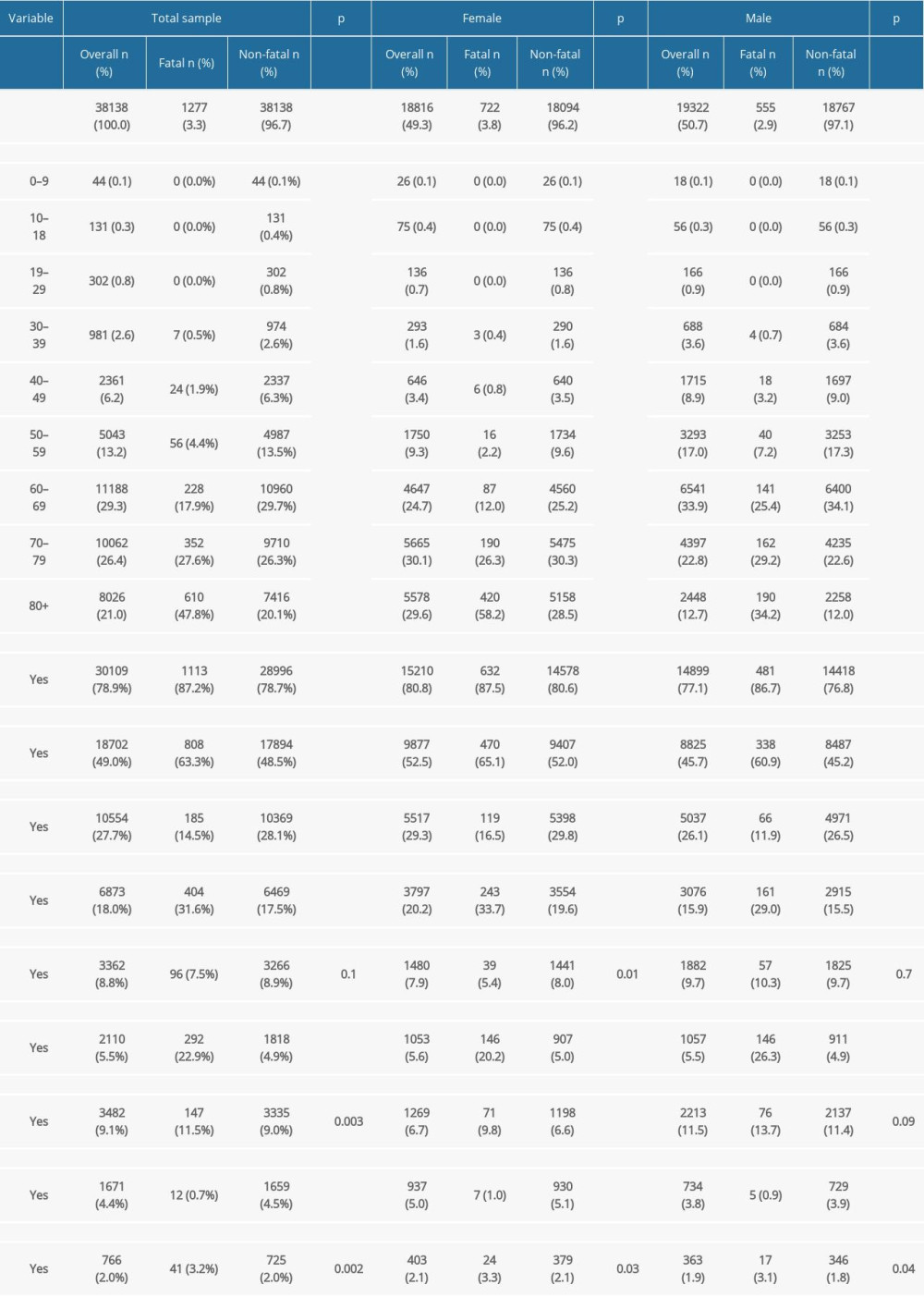 Table 4. Factors associated with the in-hospital mortality in type 1 diabetes by multivariable logistic regression models.
Table 4. Factors associated with the in-hospital mortality in type 1 diabetes by multivariable logistic regression models.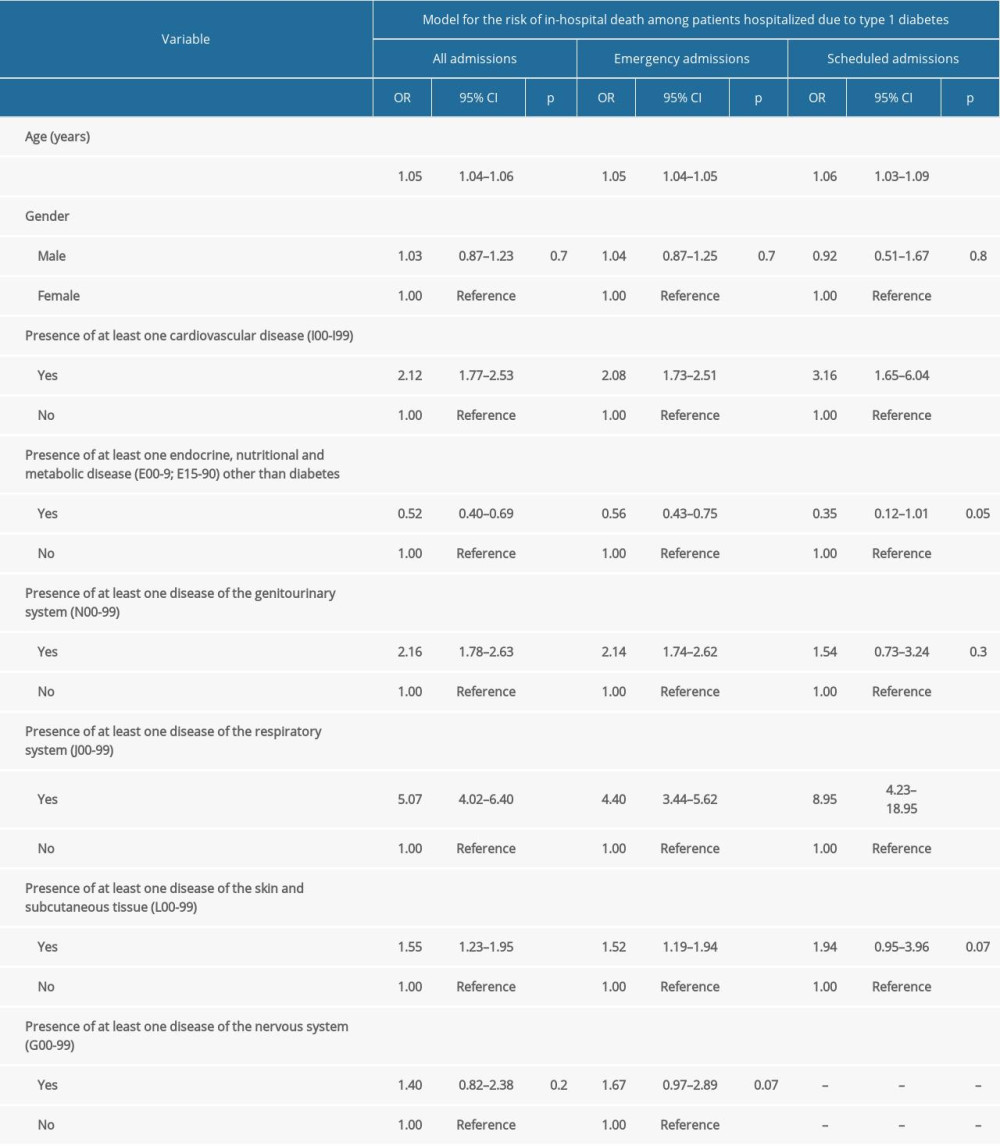 Table 5. Factors associated with the in-hospital mortality in type 2 diabetes by multivariable logistic regression models.
Table 5. Factors associated with the in-hospital mortality in type 2 diabetes by multivariable logistic regression models.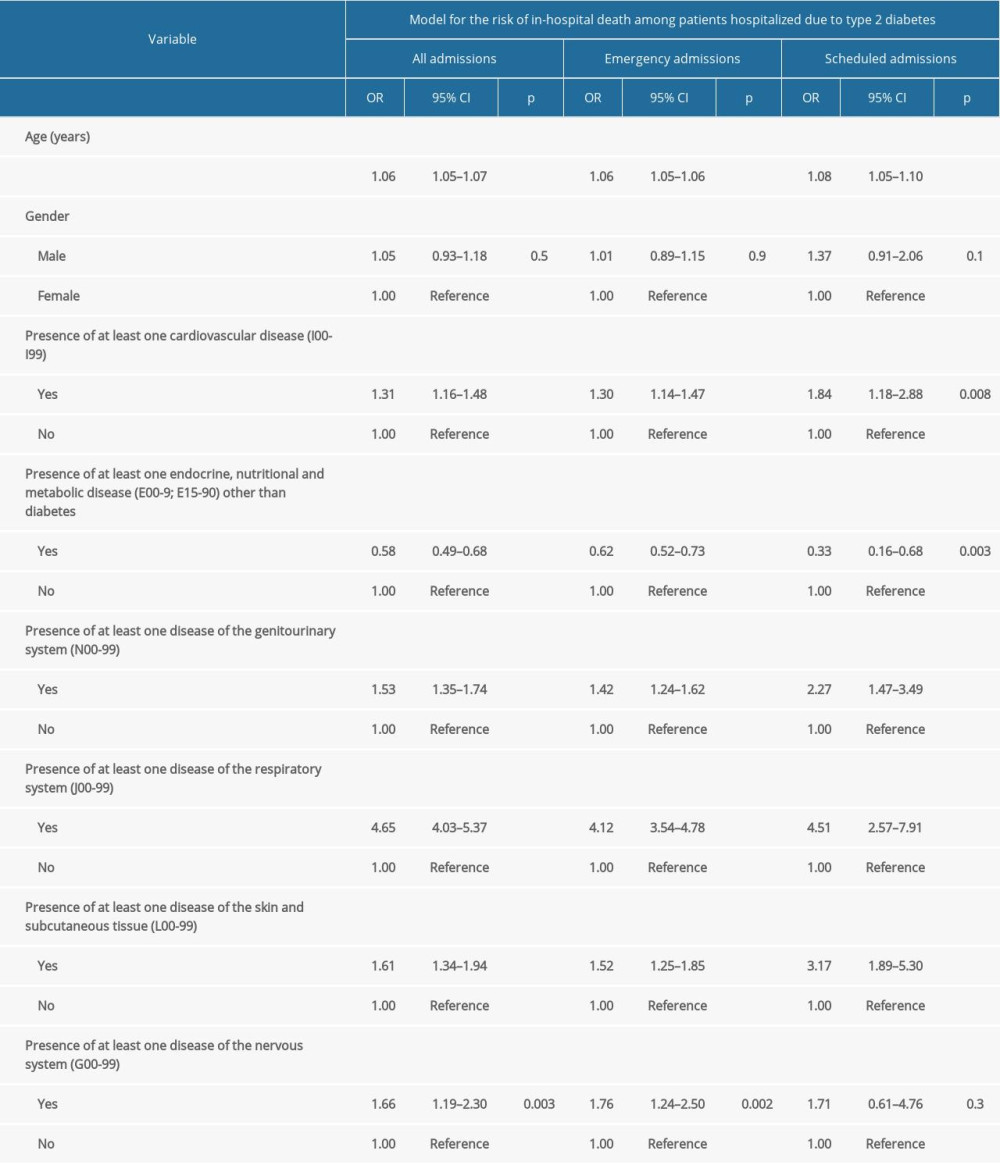 Table 6. Factors associated with prolonged hospitalization due to type 1 diabetes.
Table 6. Factors associated with prolonged hospitalization due to type 1 diabetes.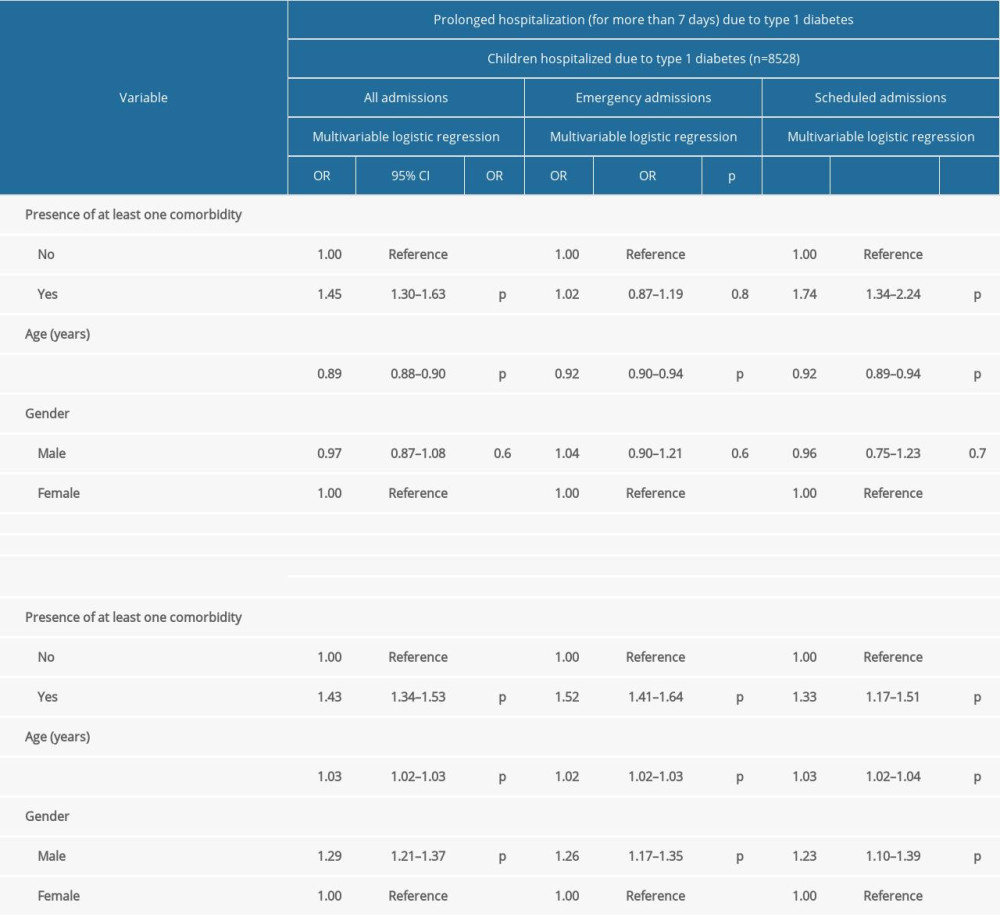 Table 7. Factors associated with prolonged hospitalization due to type 2 diabetes (adult population; n=37 963).
Table 7. Factors associated with prolonged hospitalization due to type 2 diabetes (adult population; n=37 963).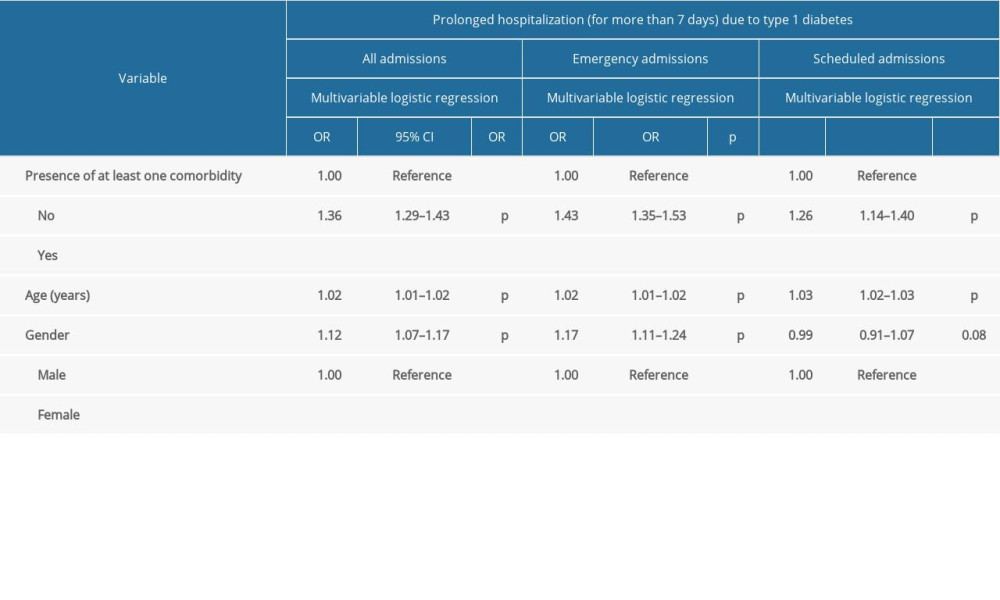
References
1. Skyler JS, Bakris GL, Bonifacio E, Differentiation of diabetes by pathophysiology, natural history, and prognosis: Diabetes, 2017; 66(2); 241-55
2. World Health Organization: Diabetes [Internet] September, 2022 Available from: https://www.who.int/health-topics/diabetes#tab=tab_1
3. Galicia-Garcia U, Benito-Vicente A, Jebari S, Pathophysiology of type 2 diabetes mellitus: Int J Mol Sci, 2020; 21(17); 6275
4. Stumvoll M, Goldstein BJ, van Haeften TW, Type 2 diabetes: Principles of pathogenesis and therapy: Lancet, 2005; 365(9467); 1333-46
5. Chatterjee S, Khunti K, Davies MJ, Type 2 diabetes: Lancet, 2017; 389(10085); 2239-51
6. Bellou V, Belbasis L, Tzoulaki I, Risk factors for type 2 diabetes mellitus: An exposure-wide umbrella review of meta-analyses: PLoS One, 2018; 13(3); e0194127
7. DiMeglio LA, Evans-Molina C, Oram RA, Type 1 diabetes: Lancet, 2018; 391(10138); 2449-62
8. Giwa AM, Ahmed R, Omidian Z, Current understandings of the pathogenesis of type 1 diabetes: Genetics to environment: World J Diabetes, 2020; 11(1); 13-25
9. Pociot F, Lernmark Å, Genetic risk factors for type 1 diabetes: Lancet, 2016; 387(10035); 2331-39
10. Simmons KM, Michels AW, Type 1 diabetes: A predictable disease: World J Diabetes, 2015; 6(3); 380-90
11. Seidu S, Cos X, Brunton S, 2022 update to the position statement by Primary Care Diabetes Europe: A disease state approach to the pharmacological management of type 2 diabetes in primary care: Prim Care Diabetes, 2022; 16(2); 223-44
12. Spence MM, Makarem AF, Reyes SL, Evaluation of an outpatient pharmacy clinical services program on adherence and clinical outcomes among patients with diabetes and/or coronary artery disease: J Manag Care Spec Pharm, 2014; 20(10); 1036-45
13. Centers for Disease Control and Prevention: What is type 1 diabetes? [Internet] March 11, 2022 Available from:https://www.cdc.gov/diabetes/basics/what-is-type-1-diabetes.html
14. Kim S, Burden of hospitalizations primarily due to uncontrolled diabetes: Implications of inadequate primary health care in the United States: Diabetes Care, 2007; 30(5); 1281-82
15. Iglay K, Hannachi H, Joseph Howie P, Prevalence and co-prevalence of comorbidities among patients with type 2 diabetes mellitus: Curr Med Res Opin, 2016; 32(7); 1243-52
16. Dhatariya K, Corsino L, Umpierrez GE: Management of diabetes and hyperglycemia in hospitalized patients, 2000, South Dartmouth (MA), MDText.com, Inc
17. Moss SE, Klein R, Klein BEK, Risk factors for hospitalization in people with diabetes: Arch Intern Med, 1999; 159(17); 2053-57
18. Cheng SW, Wang CY, Ko Y, Costs and length of stay of hospitalizations due to diabetes-related complications: J Diabetes Res, 2019; 2019; 2363292
19. Statista: Prevalence of diabetes in adult population in Europe 2019 by country [Internet] November, 2019 Available fromhttps://www.statista.com/statistics/1081006/prevalence-of-diabetes-in-europe/
20. Shaw JE, Sicree RA, Zimmet PZ, Global estimates of the prevalence of diabetes for 2010 and 2030: Diabetes Res Clin Pract, 2010; 87(1); 4-14
21. Kalinowski P, Changes in health status of the Polish population after 1990: Ann Univ Mariae Curie Sklodowska Med, 2002; 57(1); 285-91
22. Topor-Madry R, Wojtyniak B, Strojek K, Prevalence of diabetes in Poland: A combined analysis of national databases: Diabet Med, 2019; 36(10); 1209-16
23. Gajewska M, Gebska-Kuczerowska A, Gorynski P, Analyses of hospitalization of diabetes mellitus patients in Poland by gender, age and place of residence: Ann Agric Environ Med, 2013; 20(1); 61-67
24. Goryński P, Moskalewicz B, Seroka W, Analysis of diabetic patients hospitalizations in Poland by gender, age and place of residence: Rocz Panstw Zakl Hig, 2022; 73(1); 99-108
25. Walicka M, Chlebus M, Brzozowska M, Prevalence of diabetes in Poland in the years 2010–2014: Clin Diabetol, 2015; 4(6); 232-37
26. Kozioł M, Towpik I, Żurek M, Predictors of rehospitalization and mortality in diabetes-related hospital admissions: J Clin Med, 2021; 10(24); 5814
27. Poznańska A, Goryński P, Seroka W, Nationwide General Hospital Morbidity Study as a source of data about Polish population health: Przegl Epidemiol, 2019; 73(1); 69-80
28. World Health Organization: ICD-10 Version: 2010 [Internet] September, 2022 Available from: https://icd.who.int/browse10/2010/en
29. Slama A, Śliwczyński A, Woźnica J, Impact of air pollution on hospital admissions with a focus on respiratory diseases: A time-series multi-city analysis: Environ Sci Pollut Res Int, 2019; 26(17); 16998-7009
30. Bochenek B, Jankowski M, Gruszczynska M, Weather as a potential cause of regional differences in the dynamics of COVID-19 transmission in Poland: Implications for epidemic forecasting: Pol Arch Intern Med, 2022; 132(1); 16110
31. Lu P, Xia G, Zhao Q, Attributable risks of hospitalizations for urologic diseases due to heat exposure in Queensland, Australia, 1995–2016: Int J Epidemiol, 2022; 51(1); 144-54
32. Diabetes Poland, 2022 Guidelines on the management of patients with diabetes A position of Diabetes Poland: Curr Top Diabetes, 2022; 2(1); 1-130
33. Grudziąż-Sękowska J, Sękowski K, Kobuszewski B, Healthcare utilization and adherence to treatment recommendations among children with type 1 diabetes in Poland during the COVID-19 pandemic: Int J Environ Res Public Health, 2022; 19(8); 4798
34. Eurostat: Hospital discharges and length of stay statistics [Internet] August, 2020 Available from: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Hospital_discharges_and_length_of_stay_statistics
35. Polak P, Świątkiewicz-Mośny M, Wagner A, Much Ado about nothing? The responsiveness of the healthcare system in Poland through patients’ eyes: Health Policy, 2019; 123(12); 1259-66
36. Comino EJ, Islam MF, Tran DT, Association of processes of primary care and hospitalisation for people with diabetes: A record linkage study: Diabetes Res Clin Pract, 2015; 108(2); 296-305
37. Lee DC, Young T, Koziatek CA, Age disparities among patients with type 2 diabetes and associated rates of hospital use and diabetic complications: Prev Chronic Dis, 2019; 16; E101
38. Quilliam BJ, Simeone JC, Ozbay AB, Risk factors for hypoglycemia-related hospitalization in patients with type 2 diabetes: A nested case-control study: Clin Ther, 2011; 33(11); 1781-91
39. Taskinen MR, Borén J, New insights into the pathophysiology of dyslipidemia in type 2 diabetes: Atherosclerosis, 2015; 239(2); 483-95
40. Low Wang CC, Hess CN, Hiatt WR, Clinical update: Cardiovascular disease in diabetes mellitus: Atherosclerotic cardiovascular disease and heart failure in type 2 diabetes mellitus – mechanisms, management, and clinical considerations: Circulation, 2016; 133(24); 2459-502
41. Daousi C, Casson IF, Gill GV, Prevalence of obesity in type 2 diabetes in secondary care: Association with cardiovascular risk factors: Postgrad Med J, 2006; 82(966); 280-84
42. Mattar A, Carlston D, Sariol G, The prevalence of obesity documentation in Primary Care Electronic Medical Records. Are we acknowledging the problem?: Appl Clin Inform, 2017; 8(1); 67-79
43. Hossain MA, Amin A, Paul A, Recognizing obesity in adult hospitalized patients: a retrospective cohort study assessing rates of documentation and prevalence of obesity: J Clin Med, 2018; 7(8); 203
44. Navarro-Pérez J, Orozco-Beltran D, Gil-Guillen V, Mortality and cardiovascular disease burden of uncontrolled diabetes in a registry-based cohort: The ESCARVAL-risk study: BMC Cardiovasc Disord, 2018; 18(1); 180
45. Unnikrishnan R, Misra A, Infections and diabetes: Risks and mitigation with reference to India: Diabetes Metab Syndr, 2020; 14(6); 1889-94
46. Archuleta S, Gharamti AA, Sillau S, Increased mortality associated with uncontrolled diabetes mellitus in patients with pulmonary cryptococcosis: A single US cohort study: Ther Adv Infect Dis, 2021; 8; 20499361211004367
Tables
Table 1. Diabetes-associated hospitalizations by month in Poland, January to December 2019.Table 2. Characteristics of 28 617 patients hospitalized due to type 1 diabetes in Poland, January to December 2019.Table 3. Characteristics of 38 138 patients hospitalized due to type 2 diabetes in Poland, January to December 2019.Table 4. Factors associated with the in-hospital mortality in type 1 diabetes by multivariable logistic regression models.Table 5. Factors associated with the in-hospital mortality in type 2 diabetes by multivariable logistic regression models.Table 6. Factors associated with prolonged hospitalization due to type 1 diabetes.Table 7. Factors associated with prolonged hospitalization due to type 2 diabetes (adult population; n=37 963). In Press
Meta-Analysis
Effectiveness of Cardiac Telerehabilitation in Improving Functional Capacity, Quality Of Life and Cardiovas...Med Sci Monit In Press; DOI: 10.12659/MSM.953366
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,468
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,759,966
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,248
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,898
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387