12 April 2023: Clinical Research
Clinical Evaluation of Continuous Renal Replacement Therapy Combined with Peritoneal Lavage for Severe Acute Pancreatitis: A Retrospective Cohort Study
Wen-zhu Jiang1EF, Hong-jie Zhao2BC, Lu Chen3DF, Xiao-dong Tang3DF, Zhicheng Deng3AE*DOI: 10.12659/MSM.939314
Med Sci Monit 2023; 29:e939314






Abstract
BACKGROUND: We aimed to investigate the clinical efficacy of continuous renal replacement therapy (CRRT) in combination with peritoneal lavage for the treatment of severe acute pancreatitis.
MATERIAL AND METHODS: We retrospectively reviewed data from 52 patients with severe acute pancreatitis between January 2014 and December 2021 at Jiangyin People’s Hospital. The patients were divided into 2 groups: CRRT (n=26) and CRRT in combination with peritoneal lavage (n=26). The following results and outcomes were retrospectively compared: procalcitonin, interleukin-6, and C-reactive protein levels, duration of systemic inflammatory response, Acute Physiology and Chronic Health Evaluation II (APACHE II) scores, abdominal distention relief time, abdominal pain relief time, length of intensive care unit stay, length of hospital stay, inpatient hospital costs, incidence of complications, and mortality.
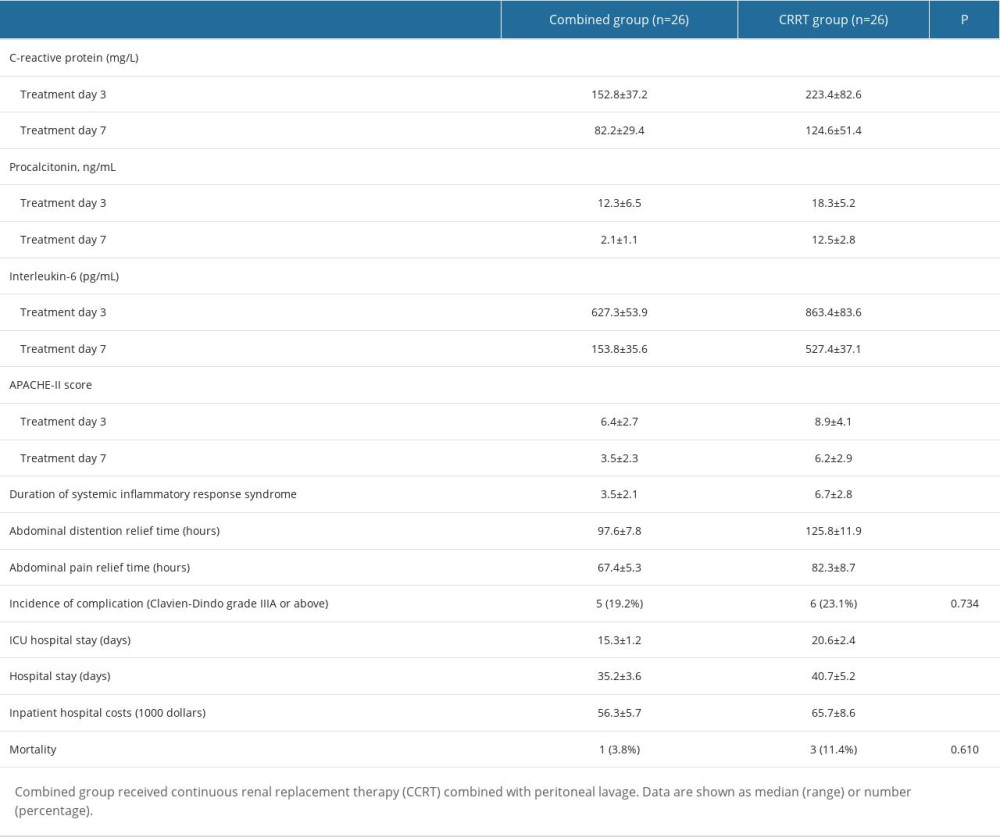
RESULTS: There were significant differences in interleukin-6 and procalcitonin levels and APACHE-II scores after 3 and 7 days of treatment. The duration of systemic inflammatory response, abdominal distention relief time, abdominal pain relief time, length of intensive care unit stay, and length of hospital stay were considerably shorter in the combination group than in the CRRT group (P<0.01). Inpatient hospital costs were significantly lower in the combination group than in the CRRT group (P<0.01). However, incidence of complications and mortality showed no significant differences between the 2 groups.
CONCLUSIONS: CRRT combined with peritoneal lavage is an important adjuvant therapy in the early stages of acute severe acute pancreatitis and has better clinical efficacy than CRRT alone.
Keywords: Peritoneal Lavage, Severity of Illness Index, Acute Disease, Pancreas, Humans, Continuous Renal Replacement Therapy, Pancreatitis, Interleukin-6, procalcitonin, Abdominal Pain, Systemic Inflammatory Response Syndrome
Background
Severe acute pancreatitis (SAP) is an inflammatory disorder of the pancreas that results in a hyperdynamic and hypermetabolic process caused by the self-digestion of pancreatic acinar cells and other factors, such as pro-inflammatory cytokines and chemokines. It is a dangerous gastrointestinal condition characterized by sustained organ failure for >48 h and has a high mortality rate [1–3]. The production of a substantial number of inflammatory mediators in the early stages of SAP can result in a systemic inflammatory response syndrome (SIRS) [4] and inflammatory cell infiltration [5–8].
Early organ failure, defined as organ failure occurring within the first 3 days after onset, is linked to mortality in patients with SAP. According to a report [9], the death rate of patients with SAP with early organ failure can be 15% to 20%. It is well known that a treatment window of 48 to 72 h after commencement is required to avoid additional harm, by neutralizing inflammatory cytokines [10]. It is critical to provide suitable early treatment, correct severity assessment, sufficient infusion therapy, and a more comprehensive treatment according to the patient’s circulation and breathing, which can increase the treatment success rate. Clinical physicians often adopt less invasive techniques, including continuous renal replacement therapy (CRRT) or peritoneal lavage (PL) to treat SAP.
CRRT is commonly performed in the Intensive Care Unit (ICU) [11–13]. CRRT is advantageous for cytokine elimination [14] and cardiovascular function [15–17], in addition to supporting failing kidneys. Although multiple studies [6,13,18] showed that early application can enhance outcomes, the benefits of CRRT remain controversial. Xu et al reported that early CRRT had no benefit for patients with SAP with early organ failure [19]. Lin et al demonstrated that it is unclear whether CRRT could reduce mortality and avoid local or systemic complications [20].
PL has been used for patients with SAP and intraperitoneal fluids. It can eliminate toxins and metabolites from the peritoneal cavity, reduce systemic absorption, and influence SIRS and organ failure [21–23]. Some reports have demonstrated that PL can reduce cardiopulmonary complications [24–28]; however, a comprehensive evaluation of 10 randomized controlled trials including 469 patients showed that PL did not lead to a significant change in death and complications [23]. Dong et al demonstrated that PL did not confer clinical benefit in patients with SAP [29].
Because previous studies demonstrated that CRRT or PL monotherapy was controversial in critically ill patients with SAP, we combined these 2 technologies to treat SAP. To investigate the impact of CRRT combined with PL, we retrospectively analyzed the data of patients with SAP in our department.
Material and Methods
From January 2014 to December 2021, a total of 52 patients with SAP were admitted to our hospital. SAP was diagnosed in accordance with the Atlanta criteria [2]. According to the Declaration of Helsinki and its amendments, informed written consent was obtained from each patient. This study was approved by the Medical Ethics Committee of the hospital.
Patients in both groups were treated with nil by mouth, oxygen administration, nasogastric aspiration, intravenous fluid resuscitation, nutritional support, prophylactic antibiotics, and appropriate analgesic-antispasmodic therapy. CRRT was initiated when the SIRS score was >2 and/or persistent organ failure occurred (>48 h), stage 3 acute kidney injury developed complications, or when fluid overload caused respiratory compromise (PaO2/FiO2 <200) [30].
We percutaneously inserted a double-lumen catheter into the femoral vein or right internal jugular vein to establish temporary vascular access. The blood flow rate was 200 to 220 mL/min. The dialyzer was changed every 4 to 12 h using the predilution mode. The surface area was set to 1.8 to 2.1 m2. Hemofiltration was continuously performed for 24 h; we used 3000 mL 0.9% saline (Baxter) as the replacement solution. According to the specific conditions of the patients, the electrolyte composition was adjusted and the acid-base imbalance was modified. Low-molecular-weight heparin was administered at the start of continuous venovenous hemofiltration to prevent clotting. In patients with a bleeding tendency, heparin was replaced with potassium citrate.
For PL, a 12 F pigtail catheter was inserted into the pelvic cavity and peritoneal dialysate was changed every 2 to 4 h. The process was continued for approximately 7 days.
The selection criteria were as follows: according to the Atlanta criteria, SAP as defined by persistent organ failure that persists for >48 h; organ failure as defined by the presence of at least 1 of the following: renal, pulmonary, or circulatory failure; Ranson score >3 [31]; and Acute Physiology and Chronic Health Evaluation II (APACHE-II) score >8 [32].
Exclusion criteria included biliary pancreatitis with need for emergency surgery, endoscopic retrograde cholangiopancreatography, percutaneous transhepatic gallbladder drainage, and abdominal compartment syndrome.
CT Severity Index score [33] and biochemical and hematologic characteristics, including procalcitonin (PCT), interleukin-6 (IL-6), and C-reactive protein (CRP) levels were reviewed. The following clinical parameters were recorded: duration of SIRS, APACHE-II scores, abdominal distention relief time, abdominal pain relief time, length of ICU stay, length of hospital stay, inpatient hospital costs, incidence of complication, and mortality.
All data were statistically analyzed using SPSS 19.0 software. The
Results
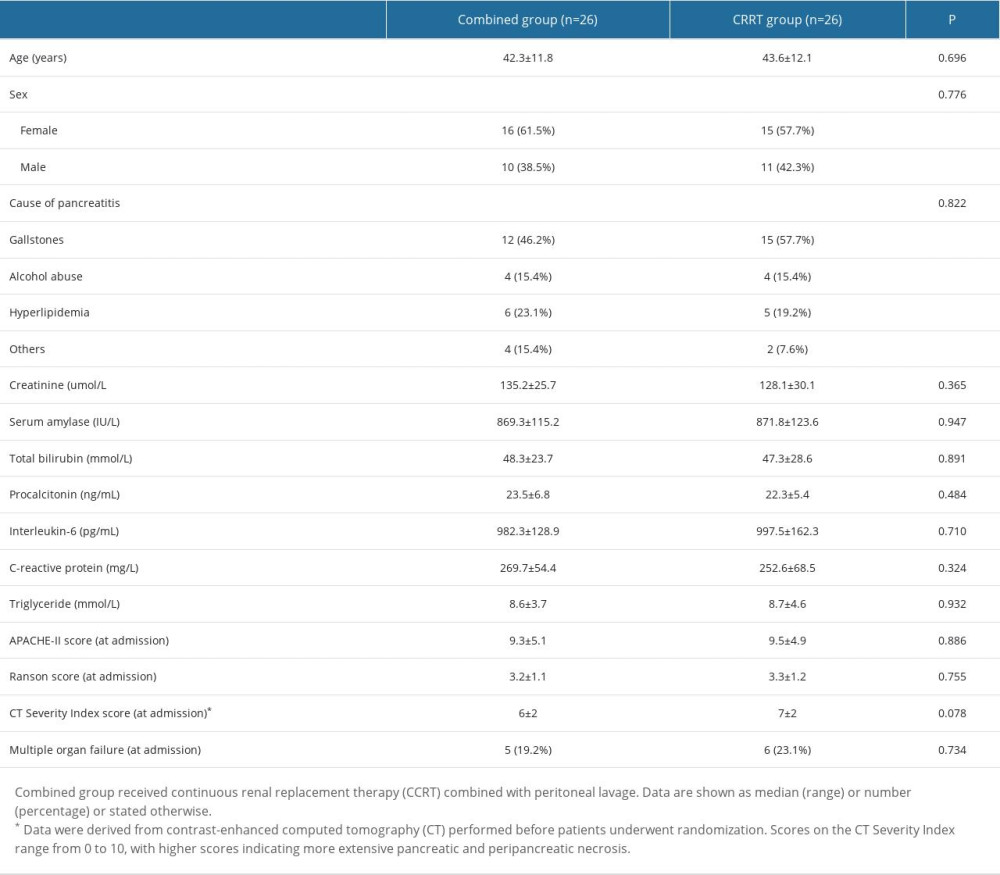
Table 1 displays the intergroup comparison of patients’ baseline clinical characteristics. At admission, the 2 groups were compared in terms of age, sex, body mass index, etiology, creatinine, serum amylase, total-bilirubin, PCT, IL-6, CRP, triglycerides, APACHE-II, Ranson scores, CT Severity Index score, and multiple organ failure. The patients in the combined group were 42.3±11.8 years old and the CRRT group was 43.6±12.1 years old (
Discussion
The first peak of death in SAP occurs during the acute response period because of multiple organ insufficiency or MOF [34,35]. Less invasive techniques, including CRRT and PL, have been gradually used to attenuate the “hits” of SAP by clinical physicians for patients with SAP. We used CRRT combined with PL to treat SAP. The advantage of PL is that it has not only the ability to purify ascites but also to treat peritoneal exudate [36]. Physicians can observe and calculate the retained fluid accurately. It is simple and easy to perform at the bedside in critically ill patients.
Several studies reported that, when performed early, CRRT was beneficial in critically ill patients [11,37]. CRRT can remove some inflammatory mediators, including endotoxins and IL-6, in the blood through adsorption and convection, which can prevent the response process of inflammatory factors, restore the dynamic balance of anti-inflammatory and pro-inflammatory factors, and improve the internal environment. For patients with hyperlipidemia, CRRT not only removes the etiology, but is also a comprehensive treatment. However, a previous study suggested that CRRT has no benefit on the prognosis of critically ill patients [19].
In this study, we combined CRRT and PL to treat SAP patients with a Ranson score >3 points and an APACHE-II score >8 points. We found that CRP, PCT, and IL-6 levels in the combined group were significantly lower than those in the CRRT group, and the duration of SIRS, abdominal distention relief time, and abdominal pain relief time were shorter. This indicated that the combined application of CRRT and PL not only quickly removed harmful and toxic substances and various chemical media in ascites and blood, but also purified blood and maintained hemodynamic stability compared with CRRT alone. The Ranson and APACHE-II scores are currently widely used clinically to evaluate the severity of acute pancreatitis. In this study, we found that the APACHE-II scores in the combined group were considerably lower than those in the CRRT group. Only 1 patient died of MOF, and the rest were free of the risk of early death in the combination group. In the CRRT group, 2 patients died of MOF and 1 died because of circulatory failure. Patients in the combined group had shorter ICU and hospital stays and lower hospital costs than patients in the CRRP group, which indicated that CRRT and the combined application of PL could help improve the prognosis of patients. However, this study also demonstrated that CRP, PCT, and IL-6 levels did not completely return to normal after early combined treatment, and we further found that CRP, PCT, and IL-6 levels increased after treatment in some cases, which suggested that pancreatic necrosis may exist. Regular enhanced CT and fine-needle aspiration might be used for the early detection of local pancreatic complications and to re-evaluate the extent of pancreatic necrosis, infection, combined organ dysfunction, and disease progression. Appropriate treatment methods, including percutaneous drainage and necrotic tissue debridement, were performed in the later phase. In this study, there were 2 cases of lung infection and sepsis, 1 case of pancreatic abscess and intestinal fistula, and 2 cases of infectious pancreatic necrosis in the later stages in the combined group, while 1 case of lung infection and sepsis, 2 cases of bleeding, 4 cases of infectious pancreatic necrosis happened in the CRRT group, which demonstrated that SAP required integrated treatment after the acute phase.
This study has some limitations. The number of samples included in this research was limited. This is a retrospective study and more research, for example a prospective study, is needed to prove the point of this paper. However, this study indicated that CRRT with PL was beneficial in patients with SAP compared with CRRT alone.
Conclusions
CRRT combined with PL is an important adjuvant therapy in the early stage of acute severe pancreatitis and has good clinical efficacy.
In the future, well-designed large-scale comparison studies will be necessary to acquire a better understanding of this issue.
References
1. Halonen KI, Pettilä V, Leppäniemi AK, Multiple organ dysfunction associated with severe acute pancreatitis: Crit Care Med, 2002; 30(6); 1274-79
2. Banks PA, Bollen TL, Dervenis C, Classification of acute pancreatitis – 2012: Revision of the Atlanta classification and definitions by international consensus: Gut, 2013; 62(1); 102-11
3. Petrov MS, Shanbhag S, Chakraborty M, Organ failure and infection of pancreatic necrosis as determinants of mortality in patients with acute pancreatitis: Gastroenterology, 2010; 139(3); 813-20
4. Chakraborty RK, Burns B, Systemic inflammatory response syndrome: StatPearls, 2022, Treasure Island (FL), StatPearls Publishing LLC
5. Kambhampati S, Park W, Habtezion A, Pharmacologic therapy for acute pancreatitis: World J Gastroenterol, 2014; 20(45); 16868-80
6. Meher S, Mishra TS, Sasmal PK, Role of biomarkers in diagnosis and prognostic evaluation of acute pancreatitis: J Biomark, 2015; 2015; 519534
7. Gukovsky I, Li N, Todoric J, Inflammation, autophagy, and obesity: Common features in the pathogenesis of pancreatitis and pancreatic cancer: Gastroenterology, 2013; 144(6); 1199-209e4
8. Kang R, Lotze MT, Zeh HJ, Cell death and DAMPs in acute pancreatitis: Mol Med, 2014; 20(1); 466-77
9. Sternby H, Bolado F, Canaval-Zuleta HJ, Determinants of severity in acute pancreatitis: A nation-wide multicenter prospective cohort study: Ann Surg, 2019; 270(2); 348-55
10. Norman J, The role of cytokines in the pathogenesis of acute pancreatitis: Am J Surg, 1998; 175(1); 76-83
11. Tandukar S, Palevsky PM, Continuous renal replacement therapy: Who, when, why, and how: Chest, 2019; 155(3); 626-38
12. Nash DM, Przech S, Wald R, O’Reilly D, Systematic review and meta-analysis of renal replacement therapy modalities for acute kidney injury in the intensive care unit: J Crit Care, 2017; 41; 138-44
13. Oda S, Hirasawa H, Shiga H, Continuous hemofiltration/hemodiafiltration in critical care: Ther Apher, 2002; 6(3); 193-98
14. Yekebas EF, Treede H, Knoefel WT, Influence of zero-balanced hemofiltration on the course of severe experimental pancreatitis in pigs: Ann Surg, 1999; 229(4); 514-22
15. Heering P, Morgera S, Schmitz FJ, Cytokine removal and cardiovascular hemodynamics in septic patients with continuous venovenous hemofiltration: Intensive Care Med, 1997; 23(3); 288-96
16. Dunham CM, Clinical impact of continuous renal replacement therapy on multiple organ failure: World J Surg, 2001; 25(5); 669-76
17. Yang Z, Wang C, Tao J, Effect of early hemofiltration on pro- and anti-inflammatory responses and multiple organ failure in severe acute pancreatitis: J Huazhong Univ Sci Technology Med Sci, 2004; 24(5); 456-59
18. Isenmann R, Rau B, Beger HG, Early severe acute pancreatitis: Characteristics of a new subgroup: Pancreas, 2001; 22(3); 274-78
19. Zhang X, Sun S, Li S, Early classic hemofiltration exhibits no benefits in severe acute pancreatitis with early organ failure: A retrospective case-matched study: Artif Organs, 2014; 38(4); 335-41
20. Lin Y, He S, Gong J, Continuous veno-venous hemofiltration for severe acute pancreatitis: Cochrane Database Syst Rev, 2019; 10(10); CD012959
21. Wang G, Liu H, Xu L, Effect of laparoscopic peritoneal lavage and drainage and continuous venovenous diahemofiltration on severe acute pancreatitis: J Laparoendosc Adv Surg Tech A, 2017; 27(11); 1145-50
22. Hines OJ, Pandol SJ, Management of severe acute pancreatitis: Br Med J, 2019; 367; l6227
23. Li Z, Xia C, Zhang L, Peritoneal lavage for severe acute pancreatitis: A meta-analysis and systematic review: Pancreas, 2016; 45(6); 806-13
24. Teerenhovi O, Nordback I, Eskola J, High volume lesser sac lavage in acute necrotizing pancreatitis: Br J Surg, 1989; 76(4); 370-73
25. Ihse I, Evander A, Gustafson I, Holmberg JT, Influence of peritoneal lavage on objective prognostic signs in acute pancreatitis: Ann Surg, 1986; 204(2); 122-27
26. Mayer AD, McMahon MJ, Corfield AP, Controlled clinical trial of peritoneal lavage for the treatment of severe acute pancreatitis: N Engl J Med, 1985; 312(7); 399-404
27. Ranson JH, Berman RS, Long peritoneal lavage decreases pancreatic sepsis in acute pancreatitis: Ann Surg, 1990; 211(6); 708-16 discussion 716–18
28. He WH, Xion ZJ, Zhu Y, Percutaneous drainage versus peritoneal lavage for pancreatic ascites in severe acute pancreatitis: A prospective randomized trial: Pancreas, 2019; 48(3); 343-49
29. Dong Z, Petrov MS, Xu J, Peritoneal lavage for severe acute pancreatitis: A systematic review of randomised trials: World J Surg, 2010; 34(9); 2103-8
30. Bagshaw SM, Wald R, Adhikari NKJ, Timing of initiation of renal-replacement therapy in acute kidney injury: N Engl J Med, 2020; 383(3); 240-51
31. Ong Y, Shelat VG, Ranson score to stratify severity in acute pancreatitis remains valid – old is gold: Expert Rev Gastroenterol Hepatol, 2021; 15(8); 865-77
32. Akavipat P, Thinkhamrop J, Thinkhamrop B, Sriraj W, Acute Physiology and Chronic Health Evaluation (APACHE) II Score – the clinical predictor in Neurosurgical Intensive Care Unit: Acta Clin Croat, 2019; 58(1); 50-56
33. Huang H, Chen W, Tang G, Optimal timing of contrast-enhanced computed tomography in an evaluation of severe acute pancreatitis-associated complications: Exp Ther Med, 2019; 18(2); 1029-38
34. Zhang Y, Yu WQ, Zhang J, Efficacy of early percutaneous catheter drainage in acute pancreatitis of varying severity associated with sterile acute inflammatory pancreatic fluid collection: Pancreas, 2020; 49(9); 1246-54
35. Johnson CD, Abu-Hilal M, Persistent organ failure during the first week as a marker of fatal outcome in acute pancreatitis: Gut, 2004; 53(9); 1340-44
36. Pérez S, Finamor I, Martí-Andrés P, Role of obesity in the release of extracellular nucleosomes in acute pancreatitis: A clinical and experimental study: Int J Obes (Lond), 2019; 43(1); 158-68
37. Honore PM, Jamez J, Wauthier M, Prospective evaluation of short-term, high-volume isovolemic hemofiltration on the hemodynamic course and outcome in patients with intractable circulatory failure resulting from septic shock: Crit Care Med, 2000; 28(11); 3581-87
In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387