29 March 2023: Clinical Research
Clinical Comparison of Anterior or Posterior Placental Location with Placenta Previa and History of Previous Cesarean Section Delivery
Fatih Mehmet FindikDOI: 10.12659/MSM.939326
Med Sci Monit 2023; 29:e939326






Abstract
BACKGROUND: Placenta previa is defined as a placenta that grows from the anterior or posterior wall of the uterus and covers the cervix. The incidence of placenta previa has been increasing in recent years. It is thought that bleeding is more common during surgery in cases with anterior placenta that is closing the cervix. This study investigated the importance of placental location in pregnant women with placenta previa who had a previous cesarean section.
MATERIAL AND METHODS: This study covered the period from July 2017 to June 2020. The 116 patients included in the study were divided into 2 groups according to placental location: anterior (group 1) and posterior (group 2). All patients had previously delivered via cesarean section. Operation time, presence of invasion, estimated blood loss during surgery, and transfused erythrocyte volume were evaluated. Medical records were used to access the relevant data.
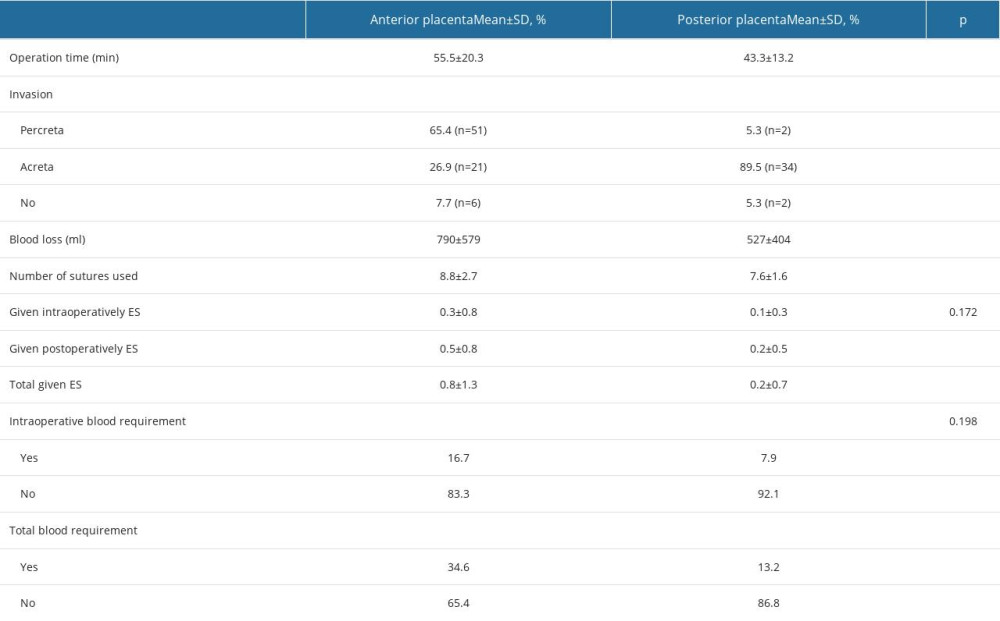
RESULTS: The patients in group 1 and group 2 had an average of 2.71 and 2.01 previous cesarean sections, respectively (P=0.002). The placental invasion (percreta) rate was significantly higher in group 1 than in group 2 (65.4 vs 5.3%, P<0.001), as was the estimated blood loss during surgery (790 vs 527 mL, P=0.014). The total erythrocyte suspension was considerably higher in group 1 than in group 2 patients (0.8 vs 0.2, P=0.014), both during and after surgery.
CONCLUSIONS: In patients with placenta previa, the location of the placenta should always be examined with ultrasonography to allow better preoperative planning.
Keywords: Cesarean Section, Cesarean Section, Repeat, Placenta Accreta, Placenta Previa, Pregnancy, Female, Humans, Placenta, Uterus
Background
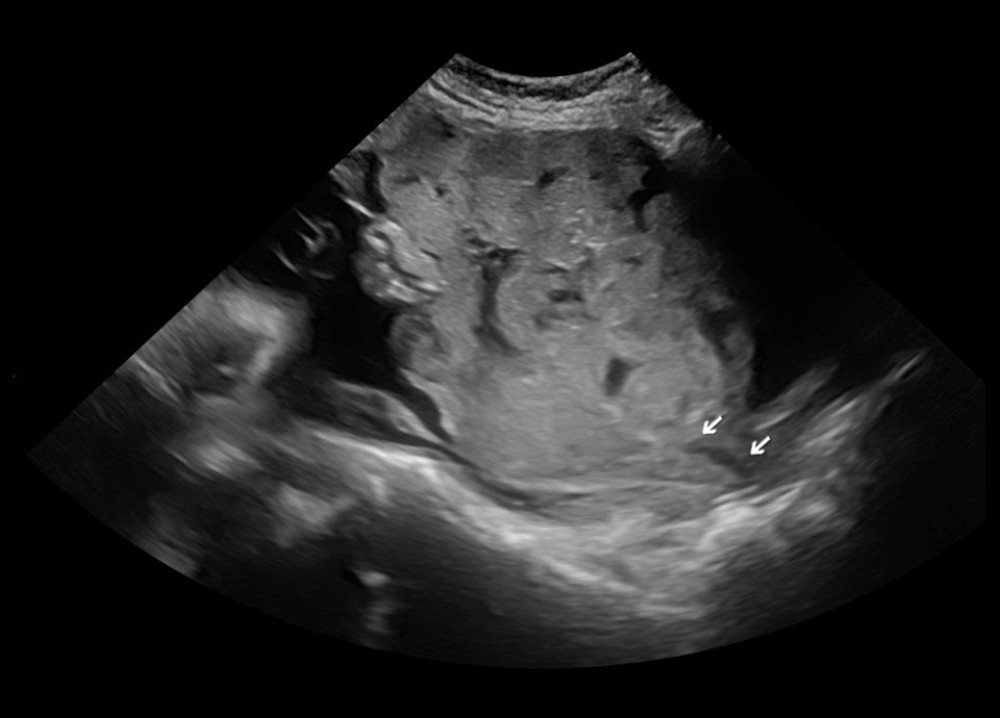
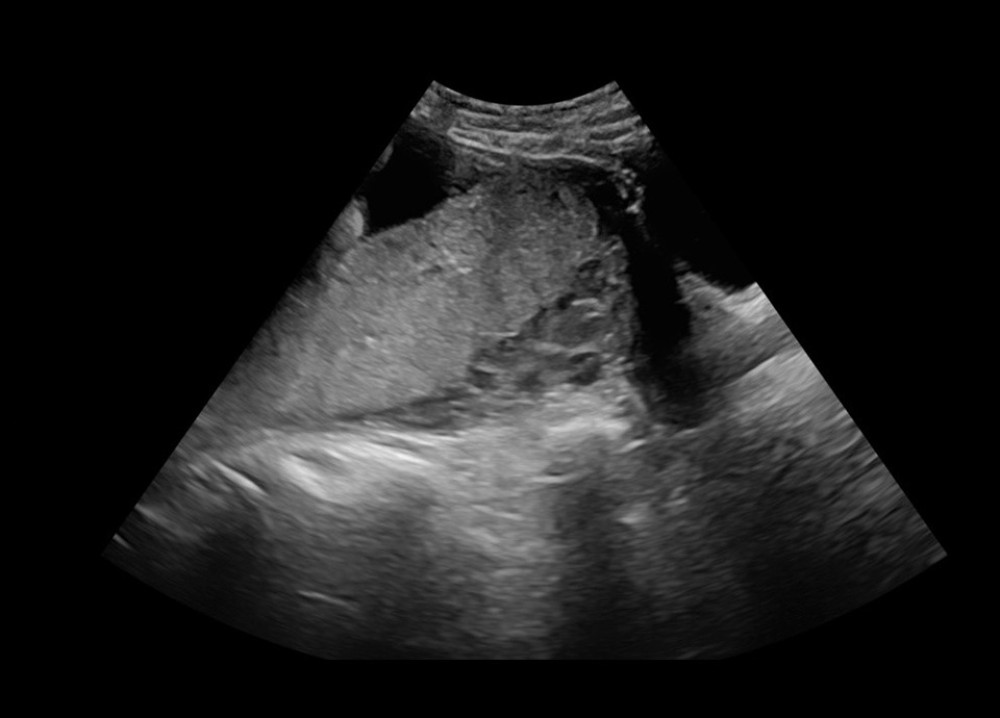
Placenta previa is defined as a placenta that grows from the anterior or posterior wall of the uterus and covers the cervix. The recent rise in the incidence of placenta previa has been attributed to the increased number of cesarean sections [1,2]. In Turkey, this rate is around 8% [3]. Diagnosis of placenta previa can be made based on a standard ultrasonographic examination. In these patients, massive bleeding, organ injury or death can occur during surgery [4,5]. Thus, in these high-risk pregnancies, it is critical to determine whether the placenta is positioned anteriorly or posteriorly. In pregnant women with an anterior placenta in which placenta percreta is present and can include bladder involvement, the surgical procedure for delivery can be more complicated [6]. In addition, intraoperative bleeding occurs more often in patients with placenta previa with an anterior placenta [7]. The present study seeks to compare clinical outcomes between anterior and posterior placental location in the setting of placenta previa and history of prior cesarean section delivery. Differences in placental location may be integral for preoperative surgical preparation and intraoperative surgical management.
Material and Methods
INCLUSION AND EXCLUSION CRITERIA:
All patients had had at least 1 previous cesarean section. Patients in whom the placenta completely covered the cervical os, as determined on preoperative ultrasonography, were included in the study. Patients with a low-lying placenta and patients operated on before the 20th week of pregnancy were excluded from the study. In addition, patients diagnosed with placenta previa were excluded from the study if they did not have a previous cesarean section.
STATISTICAL ANALYSIS:
Statistical analysis was performed using SPSS software (IBM SPSS 21.0 for Mac OS; IBM Corp., Armonk, NY). The data are presented as the mean±standard deviation or median and interquartile range. The Mann-Whitney U test or Fisher’s exact test was used to compare data between groups. A
Prior to the study, approval was obtained from the ethics committee of our university (no. 2020–90). The study was conducted in accordance with the principles of the 2013 Helsinki Declaration.
Results
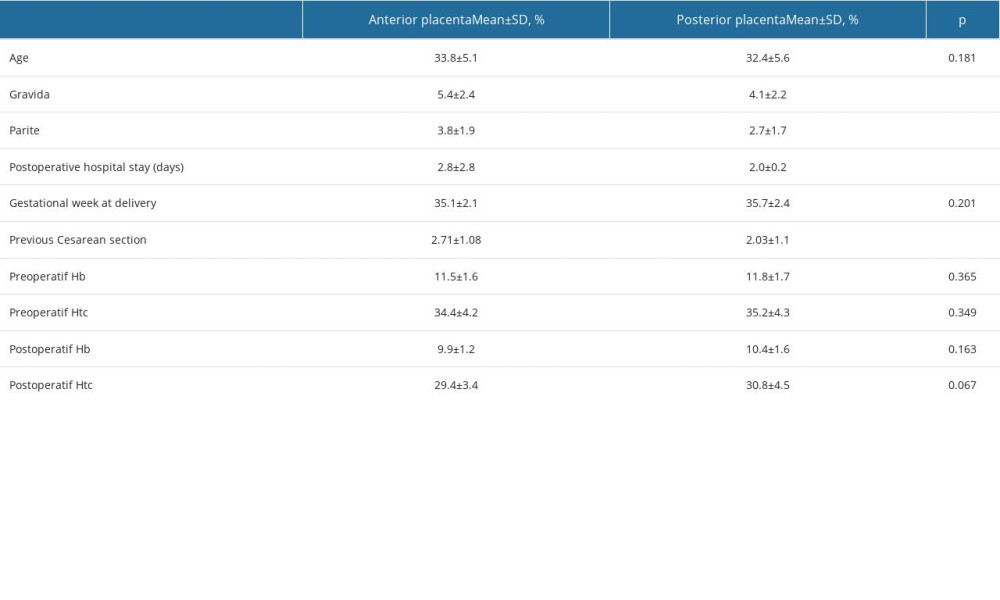
Of the 116 patients included in the study, 78 were in group 1 and 38 in group 2. The mean age in groups 1 and 2 was 33.8±5.1 years and 32.4±5.6 years, respectively (
The mean duration of surgery was 55.5 min in group 1 and 43.3 min in group 2 (
Discussion
Placenta previa, the most significant complication of pregnancy, is associated with the number of previous cesarean sections [1,2,9]. In Turkey, the number of cesarean sections is increasing, and so is the incidence of placenta previa [3]. Placenta previa can lead to life-threatening bleeding during pregnancy or at the time of cesarean section delivery, possibly requiring blood transfusion, hysterectomy, or intensive care or leading to maternal death [10–12]. Given the high risk of mortality and morbidity associated with placenta previa, localization of the placenta (anterior vs posterior) is an important step in its determination and in preoperative planning in terms of the preoperative preparation of blood products and the potential surgical procedures.
In this study, the patients were divided into 2 groups depending on placental location. In group 1, the placenta was located at the anterior wall and in group 2 at the posterior wall. In both groups, the placenta blocked the cervical os. Only patients with a previous cesarean section were included in the study, with a significantly higher number of previous cesarean sections in group 1 (
Placenta previa is the most common cause of postpartum hemorrhage [9]. A study investigating severe postpartum bleeding in placenta previa identified an anterior placenta as an important risk factor [14]. In another study investigating the risk of cesarean hysterectomy, bleeding was found to be higher in patients with an anterior placenta [15]. Similar results were obtained in a study investigating the causes of massive bleeding in patients with placenta previa [16]. That study also reported previous cesarean section as a risk factor. These results are consistent with our finding of a larger volume of bleeding in group 1 patients (
Patients with excessive bleeding during surgery often need a blood transfusion. In this study, 4 units of ES were prepared before surgery, as described in another study [17]. Among our patients, the volume of erythrocytes transfused was higher in group 1 than in group 2 patients (0.8 units higher;
In a study investigating the risk factors for antepartum bleeding in patients with placenta previa, an anterior placenta, but not a posterior placenta, was found to be a risk factor for antepartum hemorrhage [18].
Most studies in the literature have evaluated only the amounts of blood transfused. This was not the case in our study, which also considered the number of patients given ES. In this study, while the need for intraoperative blood was the same in both groups, the total ES needed (intraoperative and postoperative) was 35% higher in group 1 (
In a study comparing uterine incision methods in patients with placenta accreta spectrum, both the invasion rate and the estimated amount of bleeding were higher in the group with an anterior placenta. In these patients, the operation time was significantly longer and more ES units were used [19].
The duration of cesarean section surgery is longer in patients with placenta previa than in those without [20,21]. In the present study, the duration of surgery was significantly longer in the group with an anterior placenta (
A larger number of intraoperative sutures was needed in group 1 (8.8 sutures) than in group 2 (7.6 sutures), with
In our study, the rate of invasion (percreta) was significantly higher in group 1 than in group 2 (65.4% vs 5.3%,
In our study, it is seen that placental invasion rates are higher than those of previous studies. We did not find any data to explain the reason for this. However, in our clinic, if there is at least one previous cesarean section in placenta previa patients, we prepare as if there is placental invasion. As a result, the high rate of invasion supports the necessity of preoperative preparation. This information shows us that more studies are needed on placental invasion rates.
The hospital stay is generally longer in patients with placenta previa, and specifically in those with an anterior placenta [1,21]. Similarly, patients in group 1 had a longer postoperative hospital stay (2.8 days longer) than did those in group 2 (
One of the limitations of our study was to study a subject with a relatively low incidence, such as placenta previa. Another is that it is a single-center study. We think that multicenter studies with more patients will contribute to the literature.
Conclusions
The location of the placenta is critical in patients with placenta previa, particularly in those who have had a previous cesarean section, as it can determine the risk of postpartum bleeding. It is therefore crucial to determine the position of the placenta before surgery to inform patients about the risk of bleeding and to prepare the blood products that might be needed during surgery. The presence of placental invasion, amount of bleeding, and number of sutures required will vary depending on the placental location. Thus, during routine prenatal care, ultrasonography should be used to check for placenta previa as well as for the anterior or posterior placement of the placenta.
References
1. Titapant V, Tongdee T, Pooliam J, Retrospective analysis of 113 consecutive cases of placenta accreta spectrum from a single tertiary care center: J Matern Fetal Neonatal Med, 2020; 33; 3324-31
2. Zhang L, Bi S, Du L, Effect of previous placenta previa on outcome of next pregnancy: A 10-year retrospective cohort study: BMC Pregnancy Childbirth, 2020; 20; 212
3. Findik FM, Içen MS, Tunç SY, Evaluation of patients with previous C/S+ placenta previa totalis in 2017: Dicle Tıp Dergisi, 2020; 47; 630-67
4. Esakoff TF, Sparks TN, Kaimal AJ, Diagnosis and morbidity of placentaaccreta: Ultrasound Obstet Gynecol, 2011; 37; 324-27
5. Habek D, Becareviç R, Emergency peripartum hysterectomy in a tertiary obstetric center: 8-year evaluation: Fetal Diagn Ther, 2007; 22; 139-42
6. Palacios Jaraquemada JM, Pesaresi M, Nassif JC, Anterior placenta percreta: Surgical approach, hemostasis and uterine repair: Acta Obstet Gynecol Scand, 2004; 83; 738-44
7. Baba Y, Matsubara S, Ohkuchi A, Anterior placentation as a risk factor for massive hemorrhage during cesarean section in patients with placenta previa: J Obstet Gynaecol Res, 2014; 40; 1243-48
8. Jauniaux E, Ayres-de-Campos D, Langhoff-Roos J, FIGO placenta accreta diagnosis and management expert consensus panel. FIGO classification for the clinical diagnosis of placenta accreta spectrum disorders: Int J Gynaecol Obstet, 2019; 146; 20-24
9. Jing L, Wei G, Mengfan S, Effect of site of placentation on pregnancy outcomes in patients with placenta previa: PLoS One, 2018; 13; e0200252
10. Silver RM, Abnormal placentation: placenta previa, vasa previa, and placenta accreta: Obstet Gynecol, 2015; 126; 654-68
11. Baumfeld Y, Herskovitz R, Niv ZB, Placenta associated pregnancy complications in pregnancies complicated with placenta previa: Taiwan J Obstet Gynecol, 2017; 56; 331-35
12. Lyu B, Chen M, Liu XXRisk factors of peripartum hysterectomy in placenta previa: A retrospective study of 3840 cases: Zhonghua Fu Chan Ke Za Zhi, 2016; 51; 498-502 [in Chinese]
13. Rac MW, Dashe JS, Wells CE, Ultrasound predictors of placental invasion: The Placenta Accreta Index: Am J Obstet Gynecol, 2015; 212; 343.e1-7
14. Kong CW, To WWK, Risk factors for severe postpartum haemorrhage during caesarean section for placenta praevia: J Obstet Gynaecol, 2020; 40; 479-84
15. Liu B, Deng S, Lin M, Prediction of cesarean hysterectomy in placenta previa complicated with prior cesarean: A retrospective study: BMC Pregnancy Childbirth, 2020; 20; 81
16. Hasegawa J, Matsuoka R, Ichizuka K, Predisposing factors for massive hemorrhage during Cesarean section in patients with placenta previa: Ultrasound Obstet Gynecol, 2009; 34; 80-84
17. Titapant V, Chongsomboonsuk T, Associated factors of blood transfusion for Caesarean sections in pure placenta praevia pregnancies: Singapore Med J, 2019; 60; 409-13
18. Long SY, Yang Q, Chi R, Maternal and neonatal outcomes resulting from antepartum hemorrhage in women with placenta previa and its associated risk factors: A single-center retrospective study: Ther Clin Risk Manag, 2021; 17; 31-38
19. Liu Z, Fan D, Lin D, Double-uterine-incision in the management of placenta previa complicated by placenta accreta spectrum: Am J Transl Res, 2021; 13; 13017-23
20. Maher MA, Abdelaziz A, Comparison between two management protocols for postpartum hemorrhage during cesarean section in placenta previa: Balloon protocol versus non-balloon protocol: J Obstet Gynaecol Res, 2017; 43; 447-55
21. Rauf M, Ebru C, Sevil E, Conservative management of post-partum hemorrhage secondary to placenta previa-accreta with hypogastric artery ligation and endo-uterine hemostatic suture: J Obstet Gynaecol Res, 2017; 43; 265-71
Figures
In Press
Clinical Research
Comparative Effectiveness of a Nurse-Led Care Model vs Usual Care in Rheumatoid Arthritis: A Longitudinal C...Med Sci Monit In Press; DOI: 10.12659/MSM.953211
Clinical Research
Impact of Treatment Modality on Pain, Sexual Function, and Psychological Well-Being in Patients With Bartho...Med Sci Monit In Press; DOI: 10.12659/MSM.952422
Clinical Research
Association Between Radiographic Knee Osteoarthritis, Pre-Fracture Mobility, and Hip Fracture Patterns in O...Med Sci Monit In Press; DOI: 10.12659/MSM.952678
Clinical Research
Association Between Total Cholesterol–to–High-Density Lipoprotein Ratio and Gestational Hypertension: A Cas...Med Sci Monit In Press; DOI: 10.12659/MSM.952395
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,084
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,757,530
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,116
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,768
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387