19 June 2023: Clinical Research
A Case-Control Study of Cognitive Function in Patients with End-Stage Renal Disease Before and After Hemodialysis in Southern Spain
María Mar Sánchez-Fernández1ABCDEF*, María José Fernández-Serrano2ACDEFG, Antonio S. Moreno-Salazar3ADEF, Pedro L. Quirós-Ganga4ABDEF, Gustavo A. Reyes del PasoDOI: 10.12659/MSM.940409
Med Sci Monit 2023; 29:e940409






Abstract
BACKGROUND: Cognitive problems are frequent in patients with end-stage renal disease (ESRD) treated with hemodialysis. However, previous studies used only a single cognitive screening test or a small number of cognitive indices, which is inadequate for an exhaustive evaluation of cognitive deficits. This case-control study aimed to evaluate cognitive function in patients with ESRD before and after hemodialysis at centers in southern Spain, and included analysis of associations between cognitive function and duration of hemodialysis, biochemistry, body composition, and treatment variables.
MATERIAL AND METHODS: Cognitive performance was evaluated in 42 healthy participants (HPs) and in 43 ESRD patients, before and after hemodialysis. The tests measured verbal and visual memory, sustained/selective attention, and processing speed. The diagnostic criterion for ESRD was a glomerular filtration rate <15 mL/min/1.73 m². Correlation and multiple regression analyses were used to explore the relationships between cognitive and clinical variables, controlling for age, schooling, mood, and blood pressure.
RESULTS: Scores for verbal memory, sustained/selective attention, and processing speed were lower in patients with ESRD treated with hemodialysis than in HPs, with no between-group differences in visual memory. No acute hemodialysis-specific effect on performance was observed. Several biochemistry variables were associated with performance, both negatively (eg total cholesterol, calcium, and total protein) and positively (eg sodium, phosphorus, and creatinine).
CONCLUSIONS: Patients with ESRD treated with hemodialysis showed cognitive deficits in verbal memory, sustained/selective attention, and processing speed. Performance was not significantly different between tests administered before and after hemodialysis. An adequate diet as well as physical exercise could be useful to improve cognitive performance in this population.
Keywords: Neuropsychological Tests, Renal Dialysis, Renal Insufficiency, Chronic, Humans, Case-Control Studies, Spain, Kidney Failure, Chronic, Cognition
Background
Cognitive problems are frequently observed in patients with end-stage renal disease (ESRD) treated with hemodialysis [1–3], including disorders in processing speed, attention, visual and verbal memory, language, logical memory, cognitive change, and planning [4–7]. Disorders in components of executive functions were also recently observed in ESRD patients treated with hemodialysis, including working memory, fluency, cognitive flexibility, inhibitory control, and decision-making [8]. However, many of these studies used only a single cognitive screening test [9–11] or only a small number of cognitive performance indices [12–14], which is inadequate for a complete evaluation of associated deficits [15]. Cognitive disorders in these patients have been associated with a higher mortality risk [16–19]. For this, it is of great interest to exhaustively study these cognitive deficits in this population.
Discrepant findings have been observed in studies examining the acute effect of hemodialysis on cognitive domains, which are likely attributable to differences in the timing of evaluations. Costa et al [6] observed slower reaction times in alertness and interference tasks and worse verbal memory scores immediately after hemodialysis in comparison with those recorded the day before, contrasting with the improvement shown by healthy controls between a first and second evaluation. Researchers conducting evaluations after longer post-hemodialysis intervals observed improvements in: attention, concentration, visual/verbal memory, and psychomotor speed at 24 h post-hemodialysis [20]; visual and logical memory, psychomotor speed, planning, and concentration at 19 h post-hemodialysis [4]; and inhibition of working memory at 20 h post-hemodialysis [8]. In this last case, no post-hemodialysis improvement was observed in planning, decision-making, figurative and verbal fluency, or cognitive flexibility and reasoning. Hence, the timing of evaluations may be a crucial factor to consider in assessing cognitive disorders and the acute effects of hemodialysis in these patients.
Previous findings about the associations between cognitive performance and clinical variables in ESRD patients treated with hemodialysis have been, in some cases, contradictory and inconclusive. Regarding the renal replacement therapy received, recent findings using screening measures (Brief Cognitive State Examination) have shown worse cognitive performance in ESRD patients treated with hemodialysis compared with transplantation patients [21], but previous research did not observe cognitive improvements after transplantation in attention, visual planning, mental processing speed, or motor abilities [22]. Worse attention and executive function [23] and increased risk of developing dementia have been observed in ESRD patients treated with hemodialysis compared with ESRD patients treated with peritoneal dialysis [24]. However, other investigations did not find systematic differences in cognitive performance when comparing both modalities of dialysis, in a wide variety of cognitive domains [25]. In terms of dialysis efficacy, low dialysis clearance time per body water volume (Kt/V) has been frequently associated with severe cognitive impairment [26,27]. In other cases, however, the relationship has been the opposite (with greater Kt/V associated with worse cognitive performance) [28,29]. With respect to body composition parameters, better post-hemodialysis cognitive-psychomotor performance has been observed in ESRD patients with high body mass index (BMI) [30], whereas the medical literature usually associates a higher BMI with cognitive impairment in normal populations [31], and neurological [32] and neuropsychological consequences of obesity and overweight are well known [33,34]. As to biochemical values, increased urea levels have been related to both the impairment [12] and improvement [8,20] of cognitive performance, while reports on the relationship of calcium, phosphorus, and sodium levels with neuropsychological performance have been inconsistent [6,20].
In general, studies on cognitive performance in ESRD patients treated with hemodialysis have small sample sizes, do not adequately control for sociodemographic variables related to cognitive performance (eg, age and years of education), and take little consideration into the timing of neuropsychological evaluations with respect to the hemodialysis [26,35]. The few investigations on the acute effect of hemodialysis share the same limitations [4,6]. In addition, due to the high prevalence of emotional disturbances such as anxiety and depression in ESRD patients treated with hemodialysis [36], and the relationship of these variables with cognitive performance [37,38], it is important to control for the influence of these variables on cognition.
With the above background, this case-control study aimed to evaluate cognitive function in 43 patients with ESRD before and after hemodialysis in centers located in southern Spain, including analysis of duration of hemodialysis, biochemistry findings, patient body composition, and treatment variables. Thus, the aims of this research were: (1) to compare cognitive performance, using memory, attention, and processing speed indices, between ESRD patients treated with hemodialysis and healthy participants (HPs, as a control group) matched for major sociodemographic characteristics; (2) to compare cognitive performance before and after hemodialysis; and (3) to analyze associations of cognitive performance with biochemical, treatment, and body composition variables. Our hypotheses were that: (1) cognitive performance would be lower in ESRD patients treated with hemodialysis than in HPs, when controlled for sociodemographic and emotional variables; (2) the performance would be superior after vs before hemodialysis; and (3) there would be associations between biochemical, treatment, and body composition variables and the cognitive performance indices studied.
Material and Methods
PARTICIPANTS:
The study included 43 patients (8 female, 35 male) with ESRD treated with hemodialysis, and 42 HPs (13 female, 29 male). Seven of the ESRD patients had been previously under peritoneal dialysis, and 17 were previously transplanted. ESRD was diagnosed on the basis of a glomerular filtration rate <15 mL/min/1.73 m2. The method used for hemodialysis was conventional high permeability hemodialysis. Inclusion criteria for the ESRD patients treated with hemodialysis group were: (1) hemodialysis treatment for ≥3 months before the study; (2) receipt of 3 weekly 4-hour hemodialysis sessions; (3) absence of neurological, infectious, or systemic disorders or traumatic brain injury; (4) absence of previous psychiatric diagnosis including drug abuse; and (5) absence of severe auditory and/or visual impairment. The same inclusion criteria were applied for the HP group, except for points 1 and 2. The 2 groups were similar in age, sex, and years of education (Table 1). The causes of ESRD were: glomerulonephritis (39.5%), hereditary (23.3%), vascular (11.6%), systemic (4.7%), interstitial (4.7%), diabetic (2.3%), miscellaneous (2.3%), or undefined (11.6%). All participants were native Spanish speakers.
COGNITIVE ASSESSMENT:
The instruments used to evaluate cognitive processes were:
Detailed information about these instruments and methods can be obtained elsewhere [8].
CLINICAL AND TREATMENT VARIABLES:
Medical data for the ESRD patients treated with hemodialysis group were gathered from hospital records. The records included: disease etiology, current and total time (in months) under hemodialysis, number of transplants, total time (in months) since transplantation, total time (in months) under peritoneal dialysis or hemodialysis, dialysis effectiveness (Kt/V), and hours since the last hemodialysis. Furthermore, information was gathered before the hemodialysis (or first evaluation of controls) on the most recent biochemical analysis results (hemoglobin, hematocrit, total proteins, total cholesterol, ferritin, calcium, phosphorus, sodium, urea, and creatinine in blood tests), body composition (using a Bodystat® 1500 monitoring unit), and 7 blood pressure measurements (by a 3M Tensocare B100 arm blood pressure monitor). Anxiety and depression were measured using the Spanish version [45] of the Hospital Anxiety and Depression Scale (HADS) [46], avoiding the influence of somatic symptoms. Scores in the 2 subscales were added together to obtain a global mood score.
PROCEDURE:
The patients were selected from 5 hemodialysis centers in Granada and Jaén provinces (southern Spain). The patients were individually evaluated around 56 h after their previous hemodialysis (first evaluation; a few hours before receiving the second hemodialysis session). Then, they were evaluated again at approximately 20 h after the second hemodialysis session (around 48 hours after the pre-hemodialysis evaluation for the second hemodialysis session) (Table 1). HPs were also evaluated on 2 occasions with an equal period of time between evaluations as the hemodialysis patients. Participants did not consume tobacco, food, alcohol, or caffeine during the evaluations, which were conducted in the participants’ homes after verifying that conditions were adequate for this purpose. Tests were performed in the same order by all participants, exchanging more/less difficult and verbal/non-verbal tests to avoid possible cognitive fatigue, which was also countered by allowing short 5–10 min rests between tasks. Figure 1 depicts the test administration sequence.
STATISTICAL ANALYSIS:
Group differences in cognitive performance were analyzed by multivariate analysis of variance (MANOVA), entering data from the pre-hemodialysis session (first evaluation of HPs) that included years of education, age, systolic blood pressure, and mood as covariates. A 2x(2) repeated-measures ANOVA was used to evaluate changes between the first and second evaluations (pre-post hemodialysis), with group as the between-subjects factor and the 2 assessments as repeated measures. A significant group x pre-post interaction effect associated with a greater increase from the pre- to the post- evaluations in the ESRD patients treated with hemodialysis group would indicate a hemodialysis-related improvement effect. Cohen’s d and adjusted squared theta (
Results
GROUP DIFFERENCES IN NEUROPSYCHOLOGICAL PERFORMANCE:
The MANOVA showed a main significant effect of group (F(16,64)=3.15, P=0.001, ηp2=0.44) and significant effects of the covariates age (F(16,64)=2.63, P=0.003, ηp2=0.40) and education level (F(16,64)=3.59, P≤0.001, ηp2=0.47). Table 2 lists the mean (and standard deviation) of each of the study variables and the comparison between groups. Before the hemodialysis (the first evaluation), the performance on 3 of the 4 verbal memory indices (TAVEC RLCP, TAVEC RLLP, TAVEC RIAT), all 3 sustained and selective attention indices (d2 TCA, d2 TOT, d2 CON), and 7 of the 9 processing speed indices (TMT-A C2, TMT-A C3, Stroop C1, Stroop C2, 5DT C1, 5DT C2, d2 TR) was lower in the ESRD patients treated with hemodialysis group than in the HP group. No between-group differences were observed in visual memory (ROCF copy and ROCF memory execution). Effect sizes (Cohen’s d) ranged between 0.30 (ROCF copy execution) and 0.94 (verbal memory in TAVEC RIAT) (see Figure 1).
PRE-POST DIALYSIS EFFECT:
The analysis revealed that the group factor (for global cognitive performance during both assessments) was significant for visual memory indices (ROCF copy execution:
Performance levels in visual memory (ROCF memory execution), verbal memory (TAVEC RLCP, TAVEC RLLP, TAVEC RIAT, TAVEC Discrim), sustained and selective attention (d2 TCA, d2 TOT, d2 CON), and processing speed (ROCF copy time, TMT-A C2, TMT-A C3, Stroop C1, Stroop C2, 5DT C2, d2 TR) were superior before vs after the hemodialysis (Table 3). However, the group x pre-post interaction was not significant for any study variable.
ASSOCIATIONS BETWEEN NEUROPSYCHOLOGICAL PERFORMANCE AND CLINICAL PARAMETERS IN ESRD PATIENTS TREATED WITH HEMODIALYSIS:
Discussion
Scores for verbal memory, sustained/selective attention, and processing speed were lower in ESRD patients treated with hemodialysis than in HPs, with no between-group differences in visual memory. No acute hemodialysis-specific effect on performance was observed. Several biochemistry variables were associated with performance, both negatively and positively. The finding of cognitive impairment in these functions is consistent with previous reports of disorders in attention [5,7], verbal and visual memory [26], and processing speed [5,7,26] in these patients.
In the second evaluation (ESRD patients, post-hemodialysis), superior results were obtained in visual and verbal memory, selective and sustained attention, and processing speed for both groups. However, as the interaction group x pre-post was not significant, this improvement can be explained by learning effects in the 2 groups. Thus, no acute hemodialysis-specific effect on performance was clearly observed, and our hypothesis that hemodialysis would improve neuropsychological performance was therefore rejected. In contrast, Griva et al [20] described significant improvements in attention and visual/verbal memory scores in ESRD patients treated with hemodialysis at 24 h post-hemodialysis in comparison with 2 h pre-hemodialysis, while no difference was observed in patients treated with peritoneal dialysis before and after dialysis. Schneider et al [4] observed significant improvements in processing speed and visual memory, but not in attention, at 19 h post-hemodialysis in comparison with 1 h pre-hemodialysis, while no differences in these domains were observed in HPs between a first and second evaluation. Discrepant results in the present study may have various explanations: the utilization of different evaluation tests (showing agreement only with those using TMT-A); the distinct groups used for comparison (eg, HPs in the present study vs peritoneal dialysis patients in Griva et al [20], differences in education level between cases and controls in some studies [4], or the inadequate control of learning processes between the 2 evaluations). Another possible explanation could be the duration of the kidney disease in the patients in the different studies. Compared with the patients who participated in the Griva et al [20] and Schneider et al [4] studies, our patients had a longer total duration of hemodialysis treatment (around a year longer on average). Maybe this suggests that in patients with a long history of kidney disease, constant exposure to a state of high uremia, and exposure to the invasive treatment for the vascular system that hemodialysis is, could be producing permanent changes in certain cognitive processes. Therefore, at a certain point in the diseases, hemodialysis treatment might not be able to remove excess urea at a rate sufficient to produce improvements in cognitive processes. Furthermore, maybe hemodialysis only produces improvements in cognitive performance if it is used for a short period of time. More studies should be carried out, with samples composed of patients who differ in the duration of their renal disease and hemodialysis treatment, to check this hypothesis.
Related to this last hypothesis, our results showed that a longer time period under hemodialysis was associated with reduced verbal memory (TAVEC Discrim). This is in agreement with previous reports of greater deterioration in memory [47], higher cognitive impairment [21], and dementia [24] rates, and more severe structural brain anomalies [48] in ESRD patients treated with hemodialysis vs ESRD patients treated with peritoneal dialysis. This increased impairment with longer-term hemodialysis may be attributable to a direct effect of the renal disease duration or may be related to this treatment modality. A larger number of transplants were associated with an increase in processing speed (d2 TR), consistent with previous findings of improved cognitive performance in transplanted patients vs ESRD patients treated with hemodialysis, in attention [5], processing speed [5,49,50], verbal memory [49–51], and visual memory [50,51], and a greater integrity of the white matter in brain areas associated with executive functions and memory [52]. According to the above data, brain and cognitive alterations may depend on the substitutive renal therapy modality and may be partially reversible.
With respect to body composition parameters, a higher percentage of body water was associated with a reduction in verbal memory (TAVEC Discrim), while a higher BMI and dry weight were related to increased processing speed (TMT-A C2). Dry weight was also positively associated with an improved performance in sustained and selective attention (d2 CON). These findings confirm previous observations on the relationship between nutrition [53,54] and hydration [55] status and cognitive performance. Worse processing speed scores (TMT-A) have been observed in patients with lower intradialytic weight [6]. Conversely, better performance in visual orientation, convergent thinking, and memory have been recorded in patients with higher BMI (≥23 vs <23) [30], and BMI and dry weight have been positively associated with working memory [8]. According to Giang et al [56], low-weight ESRD patients treated with hemodialysis are likely to have more comorbidities and are often malnourished, increasing the susceptibility to hemodialysis-related toxicity and the risk of cognitive impairment.
Our analysis of biochemical variables showed that total protein was negatively associated with verbal memory (TAVEC RLCP, TAVEC RIAT) and sustained and selective attention (d2 TCA, d2 CON). Increased total proteins may reflect a rise in acute-phase reactant proteins (eg, C-Reactive protein), which could be a marker of inflammation rather than protein nutrition [57]. Several studies have shown a relationship between high levels of inflammatory markers and cognitive impairment, both in the general population [58,59], and in hemodialysis [53,60] and chronic kidney disease [61] patients. Our results also showed that total cholesterol was negatively associated with verbal memory indices (TAVEC, RLCP, RLLP). Regression analysis confirmed a negative association of total cholesterol with these verbal memory variables. High total cholesterol levels have previously been associated with cognitive impairment and Alzheimer’s disease [62], and low levels were found to predict improved cognitive functions in the cognitively impaired elderly [63]. In addition, a poorer performance in memory tasks [64] and executive functions [64,65] has been observed in patients with familial hypercholesterolemia, and attention and executive function deficits have been reported in patients with type-2 diabetes mellitus and poor cholesterol control [66].
In our results, phosphorus was positively associated with verbal memory (TAVEC Discrim), sustained/selective attention (d2 TCA, d2 TOT, d2 CON), and processing speed (d2 TR), whereas a previous study found an association between cognitive impairment and high phosphorus levels in ESRD patients treated with hemodialysis [67]. It is possible that the elevated phosphorus levels in the present patients reflected their superior nutritional status and were therefore only secondarily related to improved cognitive performance. Sodium was positively associated with visual memory (ROCF copy execution); regression analysis confirmed this association, in line with previous reports of an association between hyponatremia and cognitive impairment in patients with ESRD treated with hemodialysis [67,68] or peritoneal dialysis [69] and in those with chronic hyponatremia [70] or heart disease [71]. Conversely, the correction of sodium levels has been associated with an improvement in cognitive performance in older patient groups [72].
Creatinine levels were positively associated with sustained and selective attention (d2 TCA, d2 TOT, d2 CON) and with processing speed (TMT-A C2, d2 TR), and were found to predict improved performance in sustained and selective attention (d2 TOT, d2 CON) and processing speed (d2 TR) in the regression analysis. A positive relationship was also recently observed between creatinine levels and working memory in ESRD patients treated with hemodialysis [8]. In contrast, higher creatinine levels have previously been associated with a worse cognitive performance overall and in attention [73,74] and visual [73,74] and verbal [74] memory in chronic kidney disease, including patients treated with hemodialysis [73,74]. The higher creatinine levels may again reflect the good nutritional status of the present patients, with a consequent increase in muscle mass that may be linked to a superior cognitive performance. The contribution of creatinine to performance is also likely to be mediated by other clinical and biochemical variables.
No associations were found with other biochemical variables frequently associated with cognitive performance in patients with renal disease, such as urea [8,20], protein uremic toxins [75], hemoglobin [5,8,27,76], and hematocrit [77]. In the cases of hemoglobin and hematocrit, this may be because associations are observed at levels below those observed in the present patients (>10 g/dL and 35.17%, respectively). Likewise, no association was observed with Kt/V, which has frequently been associated with cognitive performance in ESRD patients treated with hemodialysis [26,27], although other studies found no such association [56].
A major strength of the present study is the extensive battery of cognitive performance tests applied and the large number of indices evaluated. Furthermore, we also examined the acute effect of hemodialysis on cognitive execution and the effects of clinical and biochemical parameters related to ESRD and hemodialysis. In comparisons between ESRD patients treated with hemodialysis and HPs, age, educational level, and mood were controlled for and the sample size was greater than in previous studies in this area [4]. The main limitation of our study is the small sample size. However, the majority of ESRD patients treated with hemodialysis at the Nephrology Services of the Provinces of Jaén and Granada that met the inclusion criteria did participate in the study.
Conclusions
In conclusion, measures of cognitive performance, including verbal memory, sustained and selective attention, and processing speed were worse in ESRD patients treated with hemodialysis than in healthy participants, but there was no difference in visual memory. Comparison of evaluations before and after hemodialysis revealed no acute hemodialysis-specific improvement in cognitive performance. The cognitive deficits may be an indicator of permanent cognitive damage associated with the duration of kidney disease. In addition, the total time under hemodialysis showed a negative association with cognitive performance, and a history of transplantation showed a positive association. More studies with groups of patients with different duration of renal disease and different types of treatment could clarify our results. Finally, our results suggest the importance of good nutritional status and hydration in these patients, information that may be useful for patients and for the medical professionals who work with them.

Tables
Table 1. Sociodemographic, biochemical, blood pressure, body composition, and treatment characteristics data in end-stage renal disease patients treated with hemodialysis and heathy participants.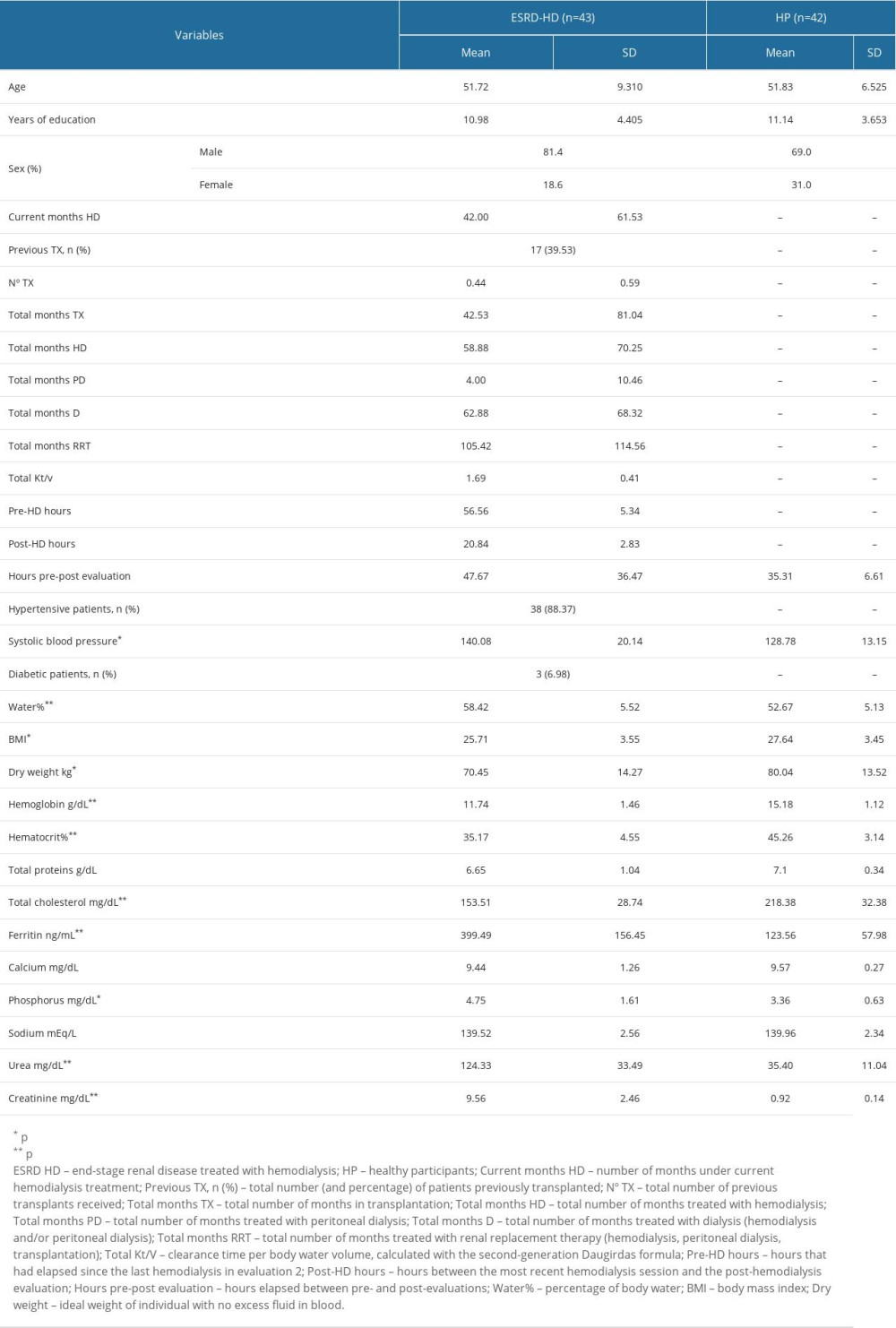 Table 2. Mean (±SD) of cognitive variables for the 2 groups during the pre-hemodialysis evaluation.
Table 2. Mean (±SD) of cognitive variables for the 2 groups during the pre-hemodialysis evaluation.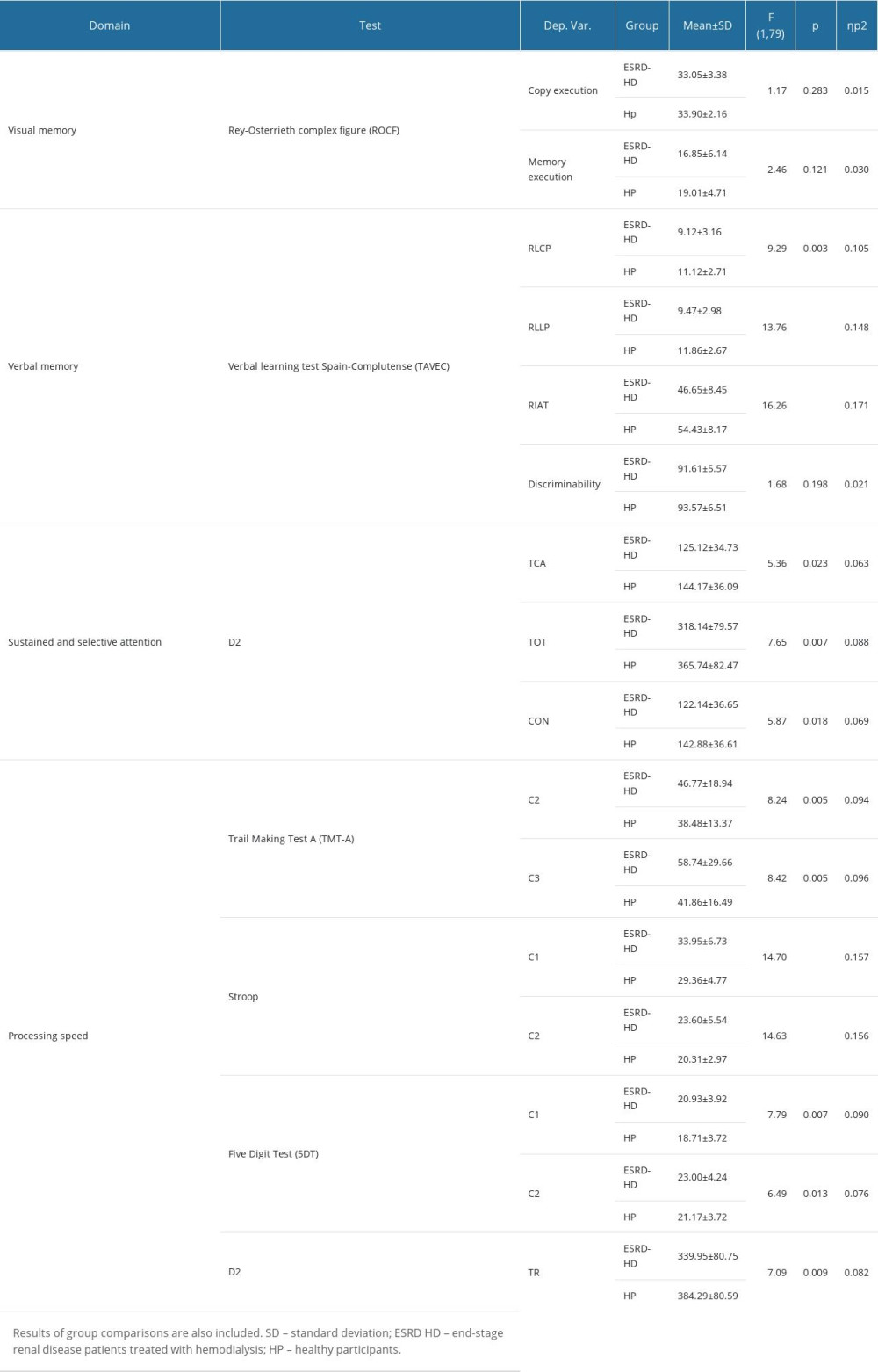 Table 3. Means (±SD) of cognitive variables during the first and second evaluations (pre- and post-hemodialysis evaluations in end-stage renal disease patients treated with hemodialysis) for which significant changes were observed. Results of within-subject analysis are also included.
Table 3. Means (±SD) of cognitive variables during the first and second evaluations (pre- and post-hemodialysis evaluations in end-stage renal disease patients treated with hemodialysis) for which significant changes were observed. Results of within-subject analysis are also included.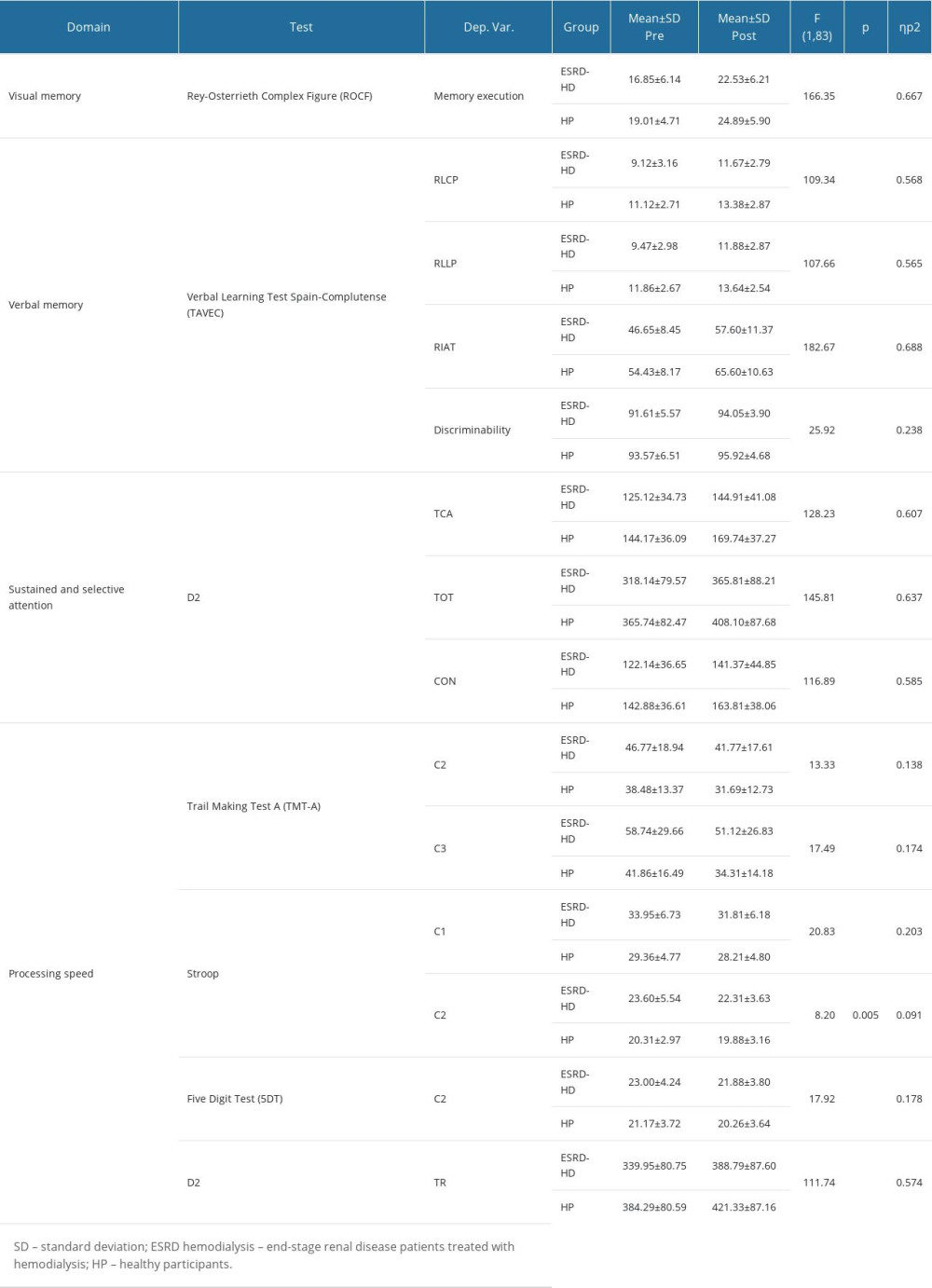
References
1. Etgen T, Chonchol M, Förstl H, Sander D, Chronic kidney disease and cognitive impairment: A systematic review and meta-analysis: Am J Nephrol, 2012; 35(5); 474-82
2. Koushik NS, McArthur SF, Baird AD, Adult chronic kidney disease: Neurocognition in chronic renal failure: Neuropsychol Rev, 2010; 20(1); 33-51
3. O’Lone E, Connors M, Masson P, Cognition in people with end-stage kidney disease treated with hemodialysis: A systematic review and meta-analysis: Am J Kidney Dis, 2016; 67(6); 925-35
4. Schneider SM, Malecki AK, Müller K, Effect of a single dialysis session on cognitive function in CKD5D patients: A prospective clinical study: Nephrol Dial Transplant, 2015; 30(9); 1551-59
5. Anwar W, Ezzat H, Mohab A, Comparative study of impact of hemodialysis and renal transplantation on cognitive functions in ESRD patients: Nefrologia, 2015; 35(6); 567-71
6. Costa AS, Tiffin-Richards FE, Holschbach B, Clinical predictors of individual cognitive fluctuations in patients undergoing hemodialysis: Am J Kidney Dis, 2014; 64(3); 434-42
7. Post JB, Morin KG, Sano M, Increased presence of cognitive impairment in hemodialysis patients in the absence of neurological events: Am J Nephrol, 2012; 35(2); 120-26
8. Sanchez-Fernandez MM, Reyes del Paso GA, Gil-Cunquero JM, Fernandez-Serrano MJ, Executive function in end-stage renal disease: Acute effects of hemodialysis and associations with clinical factors: PLoS One, 2014; 13(9); e0203424
9. Tiffin-Richards FE, Costa AS, Holschbach B, The Montreal Cognitive Assessment (MoCA) – a sensitive screening instrument for detecting cognitive impairment in chronic hemodialysis patients: PLoS One, 2014; 9(10); e106700
10. Jung S, Lee YK, Choi SR, Relationship between cognitive impairment and depression in dialysis patients: Yonsei Med J, 2013; 54(6); 1447-53
11. Odagiri G, Sugawara N, Kikuchi A, Cognitive function among hemodialysis patients in Japan: Ann Gen Psychiatry, 2011; 25; 10-20
12. Harciarek M, Williamson JB, Biedunkiewicz B, Risk factors for selective cognitive decline in dialyzed patients with end-stage renal disease: evidence from verbal fluency analysis: J Int Neuropsychol Soc, 2012; 18(1); 162-67
13. Kurella Tamura M, Unruh ML, Nissenson AR, Effect of more frequent hemodialysis on cognitive function in the frequent hemodialysis network trials: Am J Kidney Dis, 2013; 61(2); 228-37
14. Kurella Tamura M, Larive B, Unruh ML, Prevalence and correlates of cognitive impairment in hemodialysis patients: The Frequent Hemodialysis Network trials: Clin J Am Soc Nephrol, 2010; 5(8); 1429-38
15. Pereira AA, Weiner DE, Scott T, Subcortical cognitive impairment in dialysis patients: Hemodial Int, 2007; 11(3); 309-14
16. Kurella M, Mapes DL, Port FK, Chertow GM, Correlates and outcomes of dementia among dialysis patients: The Dialysis Outcomes and Practice Patterns Study: Nephrol Dial Transplant, 2006; 21(9); 2543-48
17. Griva K, Stygall J, Hankins M, Cognitive impairment and 7-year mortality in dialysis patients: Am J Kidney Dis, 2010; 56(4); 693-703
18. Drew DA, Weiner DE, Tighiouart H, Cognitive function and all-cause mortality in maintenance hemodialysis patients: Am J Kidney Dis, 2015; 65(2); 303-11
19. Sharma A, Yabes J, Al Mawed S, Impact of cognitive function change on mortality in renal transplant and end-stage renal disease patients: Am J Nephrol, 2016; 44(6); 462-72
20. Griva K, Newman SP, Harrison MJ, Acute neuropsychological changes in hemodialysis and peritoneal dialysis patients: Health Psychol, 2003; 22(6); 570-78
21. Ozcan H, Yucel A, Avşar UZ, Kidney transplantation is superior to hemodialysis and peritoneal dialysis in terms of cognitive function, anxiety, and depression symptoms in chronic kidney disease: Transplant Proc, 2015; 47(5); 1348-51
22. Griva K, Thompson D, Jayasena D, Cognitive functioning pre- to post-kidney transplantation – a prospective study: Nephrol Dial Transplant, 2006; 21(11); 3275-82
23. Neumann D, Mau W, Wienke A, Girndt M, Peritoneal dialysis is associated with better cognitive function than hemodialysis over a one-year course: Kidney Int, 2018; 93(2); 430-38
24. Wolfgram DF, Szabo A, Murray AM, Whittle J, Risk of dementia in peritoneal dialysis patients compared with hemodialysis patients: Perit Dial Int, 2015; 35(2); 189-98
25. Griva K, Newman SP, Harrison MJ, Acute neuropsychological changes in hemodialysis and peritoneal dialysis patients: Health Psychol, 2003; 22(6); 570-78
26. Murray AM, Tupper DE, Knopman DS, Cognitive impairment in hemodialysis patients is common: Neurology 25, 2006; 67(2); 216-23
27. Kalaitzidis RG, Karasavvidou D, Tatsioni A, Risk factors for cognitive dysfunction in CKD and hypertensive subjects: Int Urol Nephrol, 2013; 45(6); 1637-46
28. Giang LM, Weiner DE, Agganis BT, Cognitive function and dialysis adequacy: No clear relationship: Am J Nephrol, 2011; 33(1); 33-38
29. Kurella Tamura M, Larive B, Unruh ML, Prevalence and correlates of cognitive impairment in hemodialysis patients: the Frequent Hemodialysis Network trials: Clin J Am Soc Nephrol, 2010; 5(8); 1429-38
30. Radić J, Ljutic D, Radić M, Cognitive-psychomotor functions and nutritional status in maintenance hemodialysis patients: Are they related?: Ther Apher Dial, 2011; 15(6); 532-39
31. Malandrino N, Capristo E, Taveira TH, Cognitive function in individuals with normal weight obesity: Results from the Third National Health and Nutrition Examination Survey (NHANES III): J Alzheimer Dis, 2018; 65(1); 125-35
32. O’Brien PD, Hinder LM, Callaghan BC, Feldman EL, Neurological consequences of obesity: Lancet Neurol, 2017; 16(6); 465-77
33. Prickett C, Brennan L, Stolwyk R, Examining the relationship between obesity and cognitive function: A systematic literature review: Obes Res Clin Pract, 2015; 9(2); 93-113
34. Yang Y, Shields GS, Guo C, Liu Y, Executive function performance in obesity and overweight individuals: A meta-analysis and review: Neurosci Biobehav Rev, 2018; 84; 225-44
35. Murray AM, Pederson SL, Tupper DE, Acute variation in cognitive function in hemodialysis patients: A cohort study with repeated measures: Am J Kidney Dis, 2007; 50(2); 270-78
36. Perales-Montilla CM, Duschek S, Reyes Del Paso GA, Quality of life related to health chronic kidney disease: Predictive importance of mood and somatic symptoms: Nefrología, 2016; 36(3); 275-82
37. Darcet F, Gardier AM, Gaillard R, Cognitive dysfunction in major depressive disorder. A translational review in animal models of the disease: Pharmaceuticals (Basel), 2016; 9(1); 9
38. Hoffmann A, Ettinger U, Reyes Del Paso GA, Duschek S, Executive function and cardiac autonomic regulation in depressive disorders: Brain Cogn, 2017; 118; 108-17
39. Rey A, Test de copia de una figura compleja: TEA Ediciones, 2009
40. Benedet MJ, Alejandre MA, TAVEC: Test de Aprendizaje Verbal España Complutense: TEA Ediciones, 1998 [in Spanish]
41. Delis DC, Kramer JH, Kaplan E, Ober BA, California Verbal Learning Test: Adult version: Psychological Corporation, 1987
42. Brickenkamp R, Zillmer E, Test de Atención d2: TEA Ediciones, 2002 [in Spanish]
43. Delis D, Kaplan E, Kramer JH, Delis Kaplan executive function system: Psychological Corporation, 2001
44. Sedó M, Test de los Cinco Dígitos: Five Digit Test: TEA Ediciones, 2005 [in Spanish]
45. Caro I, Ibáñez E, La escala hospitalaria de ansiedad y depresión: Boletín de Psicología, 1992; 36; 43-69 [in Spanish]
46. Zigmond A, Snaith R, The hospital anxiety and depression scale: Psychiatrica Scandinavica, 1983; 67; 361-70
47. Sánchez-Román S, Ostrosky-Solís F, Morales-Buenrostro LE, Neurocognitive profile of an adult sample with chronic kidney disease: J Int Neuropsychol Soc, 2011; 17(1); 80-90
48. Pi HC, Xu YF, Xu R, Cognitive impairment and structural neuroimaging abnormalities among patients with chronic kidney disease: Kidney Blood Press Res, 2016; 41(6); 986-96
49. Dixon BS, VanBuren JM, Rodrigue JR, Cognitive changes associated with switching to frequent nocturnal hemodialysis or renal transplantation: BMC Nephrol, 2016; 17; 12
50. Harciarek M, Biedunkiewicz B, Lichodziejewska-Niemierko M, Cognitive performance before and after kidney transplantation: A prospective controlled study of adequately dialyzed patients with end-stage renal disease: J Int Neuropsychol Soc, 2009; 15(5); 684-94
51. Griva K, Thompson D, Jayasena D, Cognitive functioning pre- to post-kidney transplantation – a prospective study: Nephrol Dial Transplant, 2006; 21(11); 3275-82
52. Gupta A, Lepping RJ, Yu AS, Cognitive function and white matter changes associated with renal transplantation: Am J Nephrol, 2016; 43(1); 50-57
53. Rotondi S, Tartaglione L, Pasquali M, Association between cognitive impairment and malnutrition in hemodialysis patients: two sides of the same coin: Nutrients, 2023; 15(4); 813
54. Yang Y, Da J, Li Q, Long Y, The impact of malnutrition, inflammation on cognitive impairment in hemodialysis patients: A multicenter study: Kidney Blood Press Res, 2022; 47(12); 711-21
55. Shin DJ, Kim T, Jung DU, Association between dialysis adequacy and cognition in patients with peritoneal dialysis: Psychiatry Investig, 2020; 17(11); 1143-48
56. Giang LM, Weiner DE, Agganis BT, Cognitive function and dialysis adequacy: No clear relationship: Am J Nephrol, 2011; 33(1); 33-38
57. Fernández-Soto ML, González-Jiménez A, Valoración y soporte nutricional en la Enfermedad Renal Crónica: Nutr Clin Med, 2014; 8(3); 136-53 [in Spanish]
58. Heringa SM, van den Berg E, Reijmer YD, Markers of low-grade inflammation and endothelial dysfunction are related to reduced information processing speed and executive functioning in an older population – the Hoorn Study: Psychoneuroendocrinol, 2014; 40; 108-18
59. Stenfors CUD, Jonsdottir IH, Magnusson Hanson LL, Theorell T, Associations between systemic pro-inflammatory markers, cognitive function and cognitive complaints in a population-based sample of working adults: J Psychosom Res, 2017; 96; 49-59
60. Kaltsatou A, Kouidi E, Kimiskidis VK, The impact of inflammation and Autonomic Nervous System activity on cognitive impairment during a hemodialysis session: J Clin Exp Nephrol, 2016; 1; 14
61. Kurella Tamura M, Tam K, Vittighoff E, Inflammatory markers and risk for cognitive decline in chronic kidney disease: The CRIC Study: Kidney Int Rep, 2017; 2(2); 192-200
62. Toro P, Degen Ch, Pierer M, Cholesterol in mild cognitive impairment and Alzheimer’s disease in a birth cohort over 14 years: Eur Arch Psychiatry Clin Neurosci, 2014; 264(6); 485-92
63. Suzuki T, Shimada H, Makizako H, A randomized controlled trial of multicomponent exercise in older adults with mild cognitive impairment: PLoS One, 2013; 8(4); e61483
64. Zambón D, Quintana M, Mata P, Higher incidence of mild cognitive impairment in familial hypercholesterolemia: Am J Med, 2010; 123(3); 267-74
65. Ariza M, Cuenca N, Mauri M, Neuropsychological performance of young familial hypercholesterolemia patients: Eur J Intern Med, 2016; 34; e29-e31
66. Xia W, Zhang B, Yang Y, Poorly controlled cholesterol is associated with cognitive impairment in T2DM: A resting-state fMRI study: Lipids Health Dis, 2015; 14; 47
67. Shavit L, Mikeladze I, Torem C, Slotki I, Mild hyponatremia is associated with functional and cognitive decline in chronic hemodialysis patients: Clin Nephrol, 2014; 82(5); 313-19
68. Fan S, Lin L, Chen V, Effects of lower past-year serum sodium and hyponatremia on depression symptoms and cognitive impairments in patients with hemodialysis: Ther Apher Dial, 2020; 24(2); 169-77
69. Xu R, Pi HC, Xiong ZY, Hyponatremia and cognitive impairment in patients treated with peritoneal dialysis: Clin J Am Soc Nephrol, 2015; 10(10); 1806-13
70. Fujisawa H, Sugimura Y, Takagi H, Chronic hyponatremia causes neurologic and psychologic impairments: J Am Soc Nephrol, 2016; 27(3); 766-80
71. Albabtain M, Brenner MJ, Nicklas JM, Hyponatremia, cognitive function, and mobility in an outpatient heart failure population: Med Sci Monit, 2016; 22; 4978-85
72. Soiza RL, Cumming K, Clarke JM, Hyponatremia: Special considerations in older patients: J Clin Med, 2014; 3(3); 944-58
73. Elias MF, Elias PK, Seliger SL, Chronic kidney disease, creatinine and cognitive functioning: Nephrol Dial Transplant, 2009; 24(8); 2446-52
74. Owolabi LF, Abdu A, Ibrahim A, Related factors and predictors of cognitive dysfunction in chronic kidney disease on maintenance hemodialysis in Nigeria: J Neurosci Rural Pract, 2016; 7(Suppl 1); S62-67
75. Lin YT, Wu PH, Liang SS, Protein-bound uremic toxins are associated with cognitive function among patients undergoing maintenance hemodialysis: Sci Rep, 2019; 9(1); 20388
76. Nasser Mel T, Shawki S, Assessment of cognitive dysfunction in kidney disease: Saudi J Kidney Dis Transpl, 2012; 23(6); 1208-14
77. Lee SY, Lee HJ, Kim YK, Neurocognitive function and quality of life in relation to hematocrit levels in chronic hemodialysis patients: J Psychosom Res, 2004; 57(1); 5-10
Tables
Table 1. Sociodemographic, biochemical, blood pressure, body composition, and treatment characteristics data in end-stage renal disease patients treated with hemodialysis and heathy participants.Table 2. Mean (±SD) of cognitive variables for the 2 groups during the pre-hemodialysis evaluation.Table 3. Means (±SD) of cognitive variables during the first and second evaluations (pre- and post-hemodialysis evaluations in end-stage renal disease patients treated with hemodialysis) for which significant changes were observed. Results of within-subject analysis are also included.Table 1. Sociodemographic, biochemical, blood pressure, body composition, and treatment characteristics data in end-stage renal disease patients treated with hemodialysis and heathy participants.Table 2. Mean (±SD) of cognitive variables for the 2 groups during the pre-hemodialysis evaluation.Table 3. Means (±SD) of cognitive variables during the first and second evaluations (pre- and post-hemodialysis evaluations in end-stage renal disease patients treated with hemodialysis) for which significant changes were observed. Results of within-subject analysis are also included. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387