14 May 2023: Clinical Research
A Scanning Electron Microscopy Study Comparing 3 Obturation Techniques to Seal Dentin to Root Canal Bioceramic Sealer in 30 Freshly Extracted Mandibular Second Premolars
Nuha S. Alghamdi1ABEFG, Ruaa A. AlamoudiDOI: 10.12659/MSM.940599
Med Sci Monit 2023; 29:e940599






Abstract
BACKGROUND: Obturation is a crucial step in dentistry, involving the filling and sealing of a prepared root canal with sealer and core material to prevent bacterial invasion and ensure successful treatment. This study employed scanning electron microscopy to compare the effectiveness of 3 obturation techniques – single-cone technique (SCT), cold lateral compaction technique (CLCT), and continuous-wave technique (CWT) – in sealing dentin to recently introduced root canal bioceramic sealer in 30 extracted mandibular second premolars. The goal was to determine the optimal technique for minimizing gaps at the sealer-dentin interface.
MATERIAL AND METHODS: Thirty premolars were divided into 3 groups (n=10 each) based on obturation technique: SCT, CLCT, and CWT. All groups used CeraSeal bioceramic root canal sealer. Root samples were sectioned at apical, middle, and coronal thirds, and high-resolution scanning electron microscopy was performed to measure marginal/internal gaps. Data were analyzed using one-way ANOVA and Tukey range test, with P≤0.05 considered statistically significant.
RESULTS: CWT showed fewer voids at all levels, with non-significant differences within a technique. Among the techniques, SCT had the largest mean gaps at all levels [apical (5.43±0.16), middle (5.28±0.20), coronal (5.73±0.24)], while CWT had the smallest mean gaps [apical (3.02±0.19), middle (2.95±0.14), coronal (2.76±0.15)]. The differences in means between techniques were statistically significant (P≤0.05).
CONCLUSIONS: CWT obturation with CeraSeal root canal sealer produces fewer marginal gaps at the sealer-dentin interface.
Keywords: Calcibiotic Root Canal Sealer, Endodontics, Regenerative Endodontics, Root Canal Filling Materials, Root Canal Obturation, Microscopy, Electron, Scanning, Bicuspid, Dental Pulp Cavity, Dentin
Background
Endodontic treatment of deciduous or permanent natural teeth, either in unison with the patient’s current treatment requirement or as part of multidisciplinary referrals, is a common dental treatment, with the primary objective being to save the natural tooth from removal. One of the most defining clinical steps that determine the long-term success of endodontic treatment of any tooth is root canal obturation. Obturation is basically a method of filling that includes sealing of a root canal that was prepared accordingly, and the seal is obtained using a root canal sealer and core material. Hermetic seal is a term that has been synonymous for obturation goals for a long time, which in contemporary current practice has been replaced by the terms fluid-impervious and/or bacteria-tight seal [1,2]. The primary goal of canal obturation is to plug and cover the endodontic space in 3 dimensions (3D) so as to prevent regress/relapse/reinfection of microorganism within the canal [3]. The associated pain in such cases is a useful indicator of disease but takes long time to develop, which makes obturation a critical clinical step to prevent such failure. Gutta-percha (a tree, genus Palaquium in the family Sapotaceae) in conjunction with a root canal sealer (RCS) are the 2 major components of canal obturation. The gutta-percha cone, either single or multiple, essentially forms the core, while they may be adhesively or cohesively joined together and/or to the dentin surface by an RCS and/or application of chemicals/heat. Traditional techniques of heat applied to soften and bond the gutta-percha cones inadvertently affect the physical properties of gutta-percha cones while at the same time rendering RCS unstable and affecting its biocompatibility [4,5]. Gutta-percha cones (natural thermoplastic latex) cannot bond to the dentin surface or between cones, which is why endodontic sealers have to be used to enhance the connection between additional cones and the dentinal surface. In doing so, they form an attachment complex between gutta-percha cones and also seal the dentinal tubular surface along with any accessary root canal present within the canal [6,7]. Marginal and/or surface gap within an obturated canal between the inner dentinal surface and the RCS can lead to treatment failure through reinfection; therefore, close adherence of sealer to dentine is also mandatory [8]. Efficient root canal cleaning/shaping does not preclude the absence of infection within the canal, and 30% of cases have been reported to have persistent infection [9].
RCS thus serves the primary function of being a lubricant for gutta-percha that plugs vacuums (spaces) while allowing the whole complex to also fill accessory root canals that cannot be obturated conventionally using gutta-percha. To achieve an attachment between a non-binding core (gutta-percha) on 1 side and a consistently damp dentin surface, various RCS materials have evolved. Zinc oxide eugenol was the first material used, followed by resin-based (epoxy), cements (glass ionomer), silicones, and the more recent bioceramic calcium silicate-based sealers (CSBS) [10]. Bioceramic sealers are inorganic, nonmetallic, and biocompatible materials that have mechanical properties similar to dental hard tissues. Being chemically stable and noncorrosive they interact well with the organic tissue. Newer bioceramic sealers possess very high bond strength with dentin walls through the formation of hydroxyapatite crystals [11]. Progress in development of RCS brought multiple different obturation clinical techniques (e.g., single/multiple cones, chemo- and thermo-plasticized, lateral/vertical compaction, apical barrier) to produce the best possible non-leakage seal within the root canal obturation complex. Some basic techniques (e.g., lateral compaction) have been adapted (warm and cold) for use in different clinical situations. The widely-used cold lateral compaction technique (CLCT) provides a standard for comparison of other obturation techniques [12]. The technique traditionally uses a core of gutta-percha with zinc oxide eugenol RCS, which necessitates extra clinical time and clinician effort [13]. Conversely, the single-cone technique (SCT) is more convenient, requires less clinical time, and has better canal wall adaptation [14], which is based on core cones equivalent in size and taper to the corresponding instrumentation files. The continuous-wave down technique (CWDT) or CWT utilizes specific customized instruments that allow a heat carrier to soften the gutta-percha core mass. With heat carrier moving apically, the gutta-percha is forced laterally to eliminate canal irregularities. CeraSeal (Meta Biomed, Cheongju-si, Korea) is a recently developed 1-paste system bioceramic root canal sealer that contains primarily calcium silicate (tricalcium silicate-based) and zirconium oxide. The sealer claims to have no shrinkage, is bioactive (biomineralization), and has high flow and adhesive ability, thus making it a promising new RCS. Since gutta-percha is inherently hydrophobic, any sealer is likely to pull away from gutta-percha once the material sets. This shrinkage in the sealer creates marginal gaps. Therefore, marginal adaptation measurement of CeraSeal RCS for the 3 above-mentioned techniques can provide a high-quality obturation method. Therefore, the present scanning electron microscopy study aimed to compare 3 obturation techniques (SCT, CLCT, and CWT) to seal dentin to the root canal using a recently-introduced bioceramic sealer (CeraSeal) in 30 freshly extracted mandibular second premolars. We hypothesized that there will be differences between the 3 techniques. Alternatively, the null hypothesis states that there will no differences between 3 techniques when using a CeraSeal RCS.
Material and Methods
ETHICS:
The current in vitro study was conceptualized after a literature review, following which a research proposal was submitted and duly approved (approval no IRB/KKUCOD/ETH/2021-22/019) by the Committee on Research Ethics of the College of Dentistry and the affiliated university (King Khalid University, Saudi Arabia). The extracted teeth used in the study were obtained from the patients who had consented for their extraction as part of their dental treatment.
STUDY DESIGN:
This ex vivo study was conducted between the first and third quarter of the year 2022. The study design was experimental, in which intervention in the form of the canal obturation was done on natural extracted teeth followed by storage, sectioning, and evaluation by scanning electron microscopy.
SAMPLE SELECTION AND PREPARATION: Calculated sample size for the measures was based on a power analysis [power of 0.8 at significance level of 0.05 (β=0.2)]. The sample size accordingly was decided to be 10 teeth per group. Freshly extracted teeth stored (formalin-dipped) in the Department of Oral Surgery and Orthodontics were procured, from which 35 mandibular premolars with a single straight root with no evidence of occlusal/root/secondary caries were selected. The teeth were first decontaminated (5.25% sodium hypochlorite solution) for 10 minutes, then physically cleaned with water, following which they were ultrasonically cleaned (scaler) and polished (pumice). The selected teeth then were radiographed to exclude teeth with extra canals, root fractures, internal resorption, or non-negotiable root canals (tortuous/curved, calcified, unnatural anatomy). Thirty-five (30 for the study with 5 extras as replacements) mandibular second premolar (18 right and 17 left) teeth were then stored in a container filled with distilled water. A standard root length of 15 mm was considered to be optimum for the experiment requirement. Each tooth was marked 15 mm from its root apex, and the length was divided into 3 divisions of 5 mm each, as apical, middle, and coronal third sections of the tooth samples (Figure 1A). The center of each section was also marked with a V-shaped notch on each root surface at the same time as sectioning of the root specimens for scanning electron microscopy evaluation. Each sample tooth was then decoronated at a level higher than the previously planned root length (15 mm from the root apex) with a sectioning disk (diamond) (KG Sorensen, São Paulo, Brazil) [8]. Since the crown of each sample was in the same vertical plane alteration, the root-to-crown ratio was insignificant in terms of the level of the decoronation radiographically or in vitro [15].
ENDODONTIC PROCEDURE: Decoronation of samples was supervened by thorough evaluation of the cross-sectional thickness of the roots, as mentioned in previous literature [16]. This was then followed by an endodontic instrumentation procedure that involved, foremost, removal of pulp tissue using a barbed broach (Dentsply, Switzerland). The patency of each investigated canal was performed with endodontic file (# 10 k), following which canal length was determined with a similar-size file (Dentsply, Switzerland). Working length for each sample was estimated by observing the tip of the instrument at the apex with the naked eye. After withdrawing a safety distance of 1 to 2 mm from the visible apex, the probable working length was noted for each individual sample. A fixed mounting jig fastened to the working table of a preclinical laboratory was used to standardize the alignment of each tooth. Each tooth was attached to the jig with the intervening space filled with a putty-consistency elastomer (Reprosil, Dentsply/Caulk; USA). After adjusting for the most convenient axial inclination for the root of each tooth, the jig was locked in place with a tooth firmly held by the hardened putty surrounding it. This assembly also allowed each individual tooth to be removed with ease later for sectioning. For all teeth, the instrumentation of the root canals (biomechanical preparation) was performed using NiTi rotary files (ProTaper next, Dentsply-Maillefer) attached to the corresponding contra-angled Endo-Motor (Endo-Mate DT, Japan). Standardization for biomechanical root canal preparation included constant speed (300 rpm) and torque (200 gcm), access cavity preparation (endo access bur, Dentsply) (Figure 1B), irrigation (5.25% sodium hypochlorite) (Chloraxid, Poland), smear layer removal (17% ethylene diamine tetra acetic acid, EDTA) (PD, Vevey, Switzerland), rinsing (5 ml distilled water), canal desiccating (paper points – Pro Taper next size X3) (Dentsply-Maillefer), and related instructions of the manufacturer [6]. Biomechanical preparation for each canal followed the standard clinical procedure, which included instrumentation of each canal up to Pro Taper next file size X3.
SAMPLE GROUPING BASED ON OBTURATION TECHNIQUES: Differences in the experimental procedures started at this stage with an allotment of 10 samples each of 3 specific groups (Gp) based on the obturation technique [Gp 1: single-cone technique (SCT), Gp 2: cold lateral compaction technique (CLCT), Gp 3: continuous-wave technique (CWT). An exemplary completed obturation that shows the level at which the gutta-percha core was cut is presented in Figure 1C.
DATA MEASUREMENTS, EVALUATION, COLLECTION, AND ANALYSIS:
Data collection was all related to the data observed under scanning electron microscopic evaluations. The predetermined positions for sectioning that were marked before the obturation process were located on both sides and marked with a notch. Using normal water for irrigation with a minitom (Struers, Germany), each sample was sectioned at 3 places to yield 3 corresponding samples (apical, middle, and coronal third). Each section was further reduced to an observable thickness of 1 mm. Finishing of each section was done using sandpaper (fine, emery) while polishing was achieved with orthophosphoric acid (10%). Once the samples were dried, they were further dehydrated through increasing ethyl alcohol (Sigma Pool, India) concentrations (30%, 50%, 70%, 90%, 100%). Finally, all specimens were then observed under a scanning electron microscope (VEGA Easy Probe, Germany) at 3 randomly selected points to measure the marginal gaps. The SEM uses electrons rather than use of light to form high-resolution images, which follows a vertical path through the column of the microscope, thus minimizing distortion since the beams are focused. The lenses used are condenser lens made of magnets that can bend the path of electrons, which produces clear and detailed images. The gap width (maximum) considered was the maximum distance between material and the canal, which was measured accordingly (magnification 5000×). The photomicrographs for each specimen were viewed at higher magnifications (500 to 1000 times). Each image was then analyzed using software (Image I), after automatic correction for brightness and contrast, for calculating the surface area of the gaps. The marginal/internal gap area was thus calculated after fractionizing it into a percentage of the total canal area. Thus, for each root specimen, internal gaps were recorded at different levels (coronal, apical, and middle).
STATISTICAL ANALYSIS:
Internal marginal gap values for each section (apical, middle, and coronal third) in each group were recorded on an Excel sheet. The mean scores of each section were calculated from 3 values randomly chosen for each SEM photomicrograph. The standard deviation for each mean value was calculated. Following the testing of data distribution for normality, a one-way analysis of variance (ANOVA) with a post hoc multiple range test (Tukey) was used to determine the differences between the 3 studied groups. A
Results
SEM PHOTOMICROGRAPH:
The marginal gap voids for different groups as seen under a scanning electron microscope are presented in Figure 3 (Gp 1) [SCT – A (apical third), B (middle third), C (coronal third)], Figure 4 (Gp 2) [CLCT – A (apical third), B (middle third), C (coronal third)] and Figure 5 (Gp 3) [CWT – A (apical third), B (middle third), C (coronal third)]. Gaps at different levels (apical, middle, and coronal) are presented for Gp 1 (Figure 3A–3C), Gp 2 (Figure 4A–4C), and Gp 3 (Figure 5A–5C). The marginal gaps observed in samples for SCT were visible at apical, middle, and coronal thirds. The least marginal gaps were observed in samples of Gp 3 for continuous-wave technique.
DIFFERENCES IN MARGINAL ADAPTATION WITHIN EACH TECHNIQUE:
Table 1 presents the comparative differences in mean gap voids within each group at 3 observed levels. The samples in group 1 and group 2 showed smaller gap voids in the middle third (5.28±0.20 and 3.42±0.13, respectively), while samples in Gp 3 showed the smallest width in the apical third (2.76±0.15). Differences in gap voids for all groups between the 3 observed levels were found to be non-significant (P<0.05). Despite having larger gaps at 3 levels, the samples in Gp 1 were not significantly different, and despite having smaller marginal gaps in Gp 3, the differences between the 3 levels were not significant.
DIFFERENCES IN MARGINAL ADAPTATION BETWEEN THE 3 TECHNIQUES:
Table 2 presents the mean and standard deviations of gaps in the material-to-dentin interface with the 3 obturation techniques. The largest gap was found for Gp 1 at the coronal level (5.73±0.24), while the smallest gaps were found for Gp 3 at the coronal level (2.76±0.15). The samples in Gp 1 had the largest gaps at all observed levels, while the samples in Gp 3 had the smallest gaps at all levels. The differences between the 3 groups were statistically significant (P<0.05 (Table 2). At the apical portion of the samples, the smallest gaps were in Gp 3 (2.76±0.15), while the largest gaps in Gp 1 (5.43±0.16) (Figure 6).
Discussion
CERASEAL AS A BIOCERAMIC SEALER:
Bioceramic sealers are broadly branded as 2 different types: calcium silicate-based and calcium phosphate-based. The calcium silicate-based sealers are further classified as either mineral trioxide (MTA)-containing or non-MTA-containing. A tricalcium silicate (MTA)-based bioceramic root canal sealer is available commercially as a 1-paste system, containing calcium silicates, zirconium oxide, and a thickening agent. The contents are premixed to allow for direct application. Calcium silicate presents a gel of calcium aluminate and calcium silicate hydrate on contact with moisture from root canal dentin [19]. The reaction is accompanied by crystallization of calcium hydroxide, which distinguishes its biocompatibility (bioactive), allowing them to form surface hydroxyapatite as well as exerting their osteogenic effects [11]. The sealer does not shrine or discolor and has a shorter setting time of 3.5 h. The short setting time prevents washout of the sealer and allows sealer penetration to intricate shapes of canals, even after treatment [20]. In case the sealer is not sufficiently cured, physical forces tend to wash it away, which is prevented by its shorter setting time. CeraSeal cures faster than other bioceramic sealers. Its high flow is enhanced by hydraulic press dispensation and a very narrow nozzle intra-canal tip that allows placement within a narrow canal. Although the final mix is acidic (pH 12.7), because it is it nontoxic does not harm tissue. Unlike other ceramic and non-ceramic sealers, the use of zirconium oxide prevents tooth discoloration over time.
DIFFERENCES AMONG TECHNIQUES:
The results of this study show that the CWT obturation showed comparatively smaller mean marginal gaps throughout the whole extent of the root canal wall when compared with SCT and CLCT obturation. The CWT uses primarily a single Pro Taper gutta-percha cone that fits to the anatomical apical thirds. The technique is principally based on penetration of a heated tip within the gutta-percha and compressing the tip apically up to a predetermined distance. The peripheral adaptation of the sealer is potentially affected by the lateral compaction that occurs while applying the heated tip vertically. The gutta-percha is displaced laterally, which pushes the free-flowing ceramic sealer into the lateral accessory canals, as well as causing a close adaptation of the sealer to the dentin wall [21]. The effect of negative pressure in enhancing sealers’ adaptation to the dentin walls has been investigated with other obturation techniques, with promising results [8,22]. Compared to the other 2 techniques (SCT and CLCT), CWT shows greater marginal adaptation with minimum gap voids. Our results agree with the findings of Oh et al [23], who reported superior filling adaptation and increased density of filling in CWT as compared to CLCT. Void areas have also been compared between CWT and thermoplasticized (Guttacore) gutta-percha obturation. The differences between the 2 have not been found to be significant, suggesting that in relation to interface adaptation, the CWT shows superior results in different studies [24,25]. Contrary to our results, Olczak et al reported no significant differences for gutta-percha and sealer content in terms of percentage, nor in voids between CWT, CLCT, and thermoplasticized obturation [14]. CLCT, being a widely-used clinical technique, is still used for comparison with new obturation techniques/systems.
Our results show that SCT obturation produced larger marginal gap voids than CLCT and CWT obturation. Artificial irregularities within mandibular incisors root canals have been reported to be unfilled when cold gutta-percha was used [26], and these irregularities must be filled by sealers. However, sealer accumulation in gap areas increases the chances of poor marginal adaptation, contraction after setting, and sealer dissolution [27]. The SCT has been investigated with different types of sealers [28], different gutta-percha cones (bioceramic impregnated gutta-percha) [29], and different clinical techniques (warm vertical compaction) [30]. SCT has been shown to adequately fill accessory canals when used with bioceramic sealer (AH Plus), while it produced more gaps when bioceramic impregnated gutta-percha was used. Use of heat was reported to decrease the marginal gaps in SCT when used with bioceramic sealer (Bioroot RCS) [31]. The bioceramic sealer used in the present study shows that in addition to its sealing capacity, it also promotes adaptation while setting and, most importantly, is compatible with the thermal changes that occur when the heated tip is placed. These features are in agreement with the previously reported studies that investigated other bioceramic sealers (AH Plus) [32–34]. Application of heat has been reported to produce a percentage weight loss [4,35], but bioceramic sealers were reported to undergo minimal structural changes. CWT has been also reported to properly fill even difficult root canals (molar) [23]. Variations in the results between the comparative studies are attributed to various factors, especially the methods of testing and observation.
DIFFERENCES WITHIN EACH TECHNIQUE:
We found that CWT obturation produced the smallest marginal gaps within the root canal at the 3 observed levels (apical, middle, and coronal thirds). CLCT had smaller marginal gaps than the SCT but larger than CWT obturation. Different techniques of CLCT (manual, mechanical, and ultrasonic) have been investigated but were found to cause void areas within the canal [36]. These voids have been attributed to the use of a spreader that generates larger spaces than with other cones [37]. The superiority of CWT obturation in terms of better marginal adaptation and concomitantly smaller gap voids have been attributed to its ability to allow plasticization of the entire length of gutta-percha cone., which creates a mass that is homogenous and can fill minor irregularities [38]. This homogenization also decreases the sealer layer, which is less dimensionally stable than the gutta-percha core [39]. For a pulpal infection to recur and spread to the periodontal area, the quality of the obturation in the apical third of the root canal becomes critical [40]. SCT and CLCT had a larger gap width in the coronal third than in the apical third, while the CWT had larger gaps in the apical third than in the middle and coronal thirds. However, the interpretation of these results should be made with caution since the comparisons were made within groups. The larger gap voids in the apical third for the CWT obturation may be attributed to the technique used, since the heated tip is not meant to reach the apical third. When compared to other groups, the CWT had smaller marginal gaps in the apical third, which agrees with earlier studies [23,37]. Our results for CWT marginal gap width comparison among apical, middle, and coronal thirds are contrary to those obtained by Pinto et al [37], who reported low void percentage in the apical third when compared to the coronal and middle thirds. Among the 3 techniques, the CWT also showed less voids in the coronal third, which agrees with previous studies [38,41]. The presence of smaller void in the coronal third is attributed to the coronal third receiving more compaction forces directly [42]. The ability of the sealer also has to be taken into account. CeraSeal, being a bioceramic sealer, can promote new mineralized tissue regeneration or development due to its physicochemical properties [43].
Bioceramic sealers have been shown to penetrate dentinal tubules and form a hybrid layer (due to hydrophilic monomers and solvent) [11]. This hybrid layer seals external-to-internal canal communication, thus forming a complete seal. It is also quite possible that the technique may be only bringing the sealer in close contact to the dentin surface, while the sealer which is bioactive may close the gaps later through its biomineralization abilities. Other factors like porosities within the sealer, setting contraction, dissolution of sealer, and taper of the cones may play significant roles in the larger marginal gaps found using SCT obturation. In addition, bioceramic sealers have a small particle size, low contact angles, chemical bonding to dentin, significant expansion, continuous flow, surface activity, and hydrophilicity, which in combination contribute to minimizing marginal gaps at the obturation interface.
STRENGTH AND LIMITATIONS:
This study investigated the effect of 3 different obturation techniques on the marginal gap of CeraSeal bioceramic-based root canal sealer, which has been recently introduced in the Middle East and thus has been little studied. The strength of the study is the SEM evaluation of marginal gaps, which provides high-resolution detection of small voids in root canal obturation. The study is limited by the number of obturation techniques investigated, for which further studies are advised, especially those that use heat for compaction.
Conclusions
Under similar conditions used in this study, we conclude that CWT obturation produces smaller marginal gaps between a root canal and CeraSeal RCS. The study also concludes that marginal adaptation of CWT performed better than CLCT and SCT. Comparatively, in CWT, marginal adaptation was better in the coronal and middle and apical thirds, which is attributed to the limitation of the technique recommended by manufacturer. Whether the CWT tip can be modified to extend into the apical third is a matter for future study.
Figures
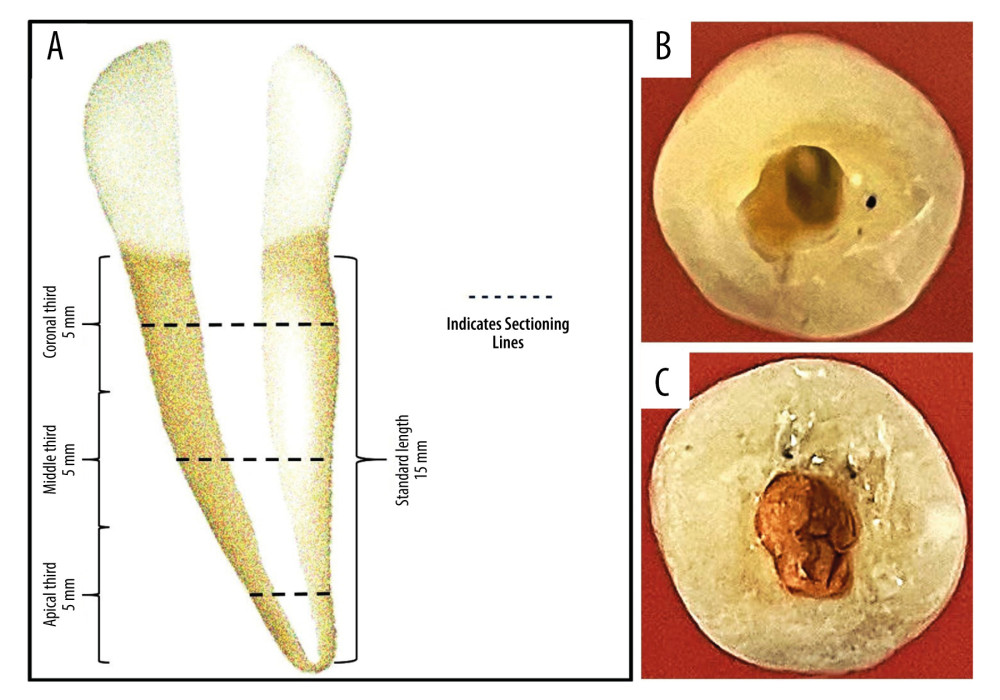 Figure 1. (A) Schematic depiction of the specimen measurements and their planned sections. (B) An exemplary specimen showing access cavity preparation. (C) An exemplary specimen showing the completed obturation. Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), Windows 11 Pro, (Microsoft corporation).
Figure 1. (A) Schematic depiction of the specimen measurements and their planned sections. (B) An exemplary specimen showing access cavity preparation. (C) An exemplary specimen showing the completed obturation. Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), Windows 11 Pro, (Microsoft corporation). 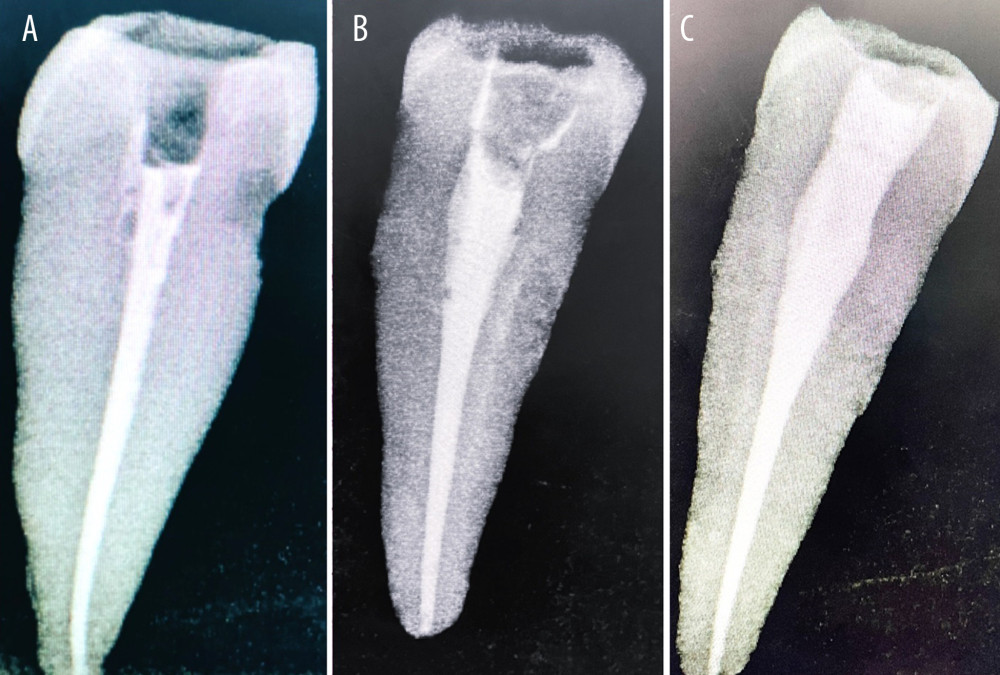 Figure 2. (A) An exemplary intra-oral periapical radiograph showing the radiographic quality of single-cone technique obturation. (B) An exemplary intra-oral periapical radiograph showing the radiographic quality of Cold Lateral Compaction Technique obturation. (C) An exemplary intra-oral periapical radiograph showing the radiographic quality of continuous-wave down technique. Photographs taken using a digital single-lens reflex (DSLR) camera (Canon EOS 700D) with 100 mm macro lens) with/without ring flash.
Figure 2. (A) An exemplary intra-oral periapical radiograph showing the radiographic quality of single-cone technique obturation. (B) An exemplary intra-oral periapical radiograph showing the radiographic quality of Cold Lateral Compaction Technique obturation. (C) An exemplary intra-oral periapical radiograph showing the radiographic quality of continuous-wave down technique. Photographs taken using a digital single-lens reflex (DSLR) camera (Canon EOS 700D) with 100 mm macro lens) with/without ring flash. 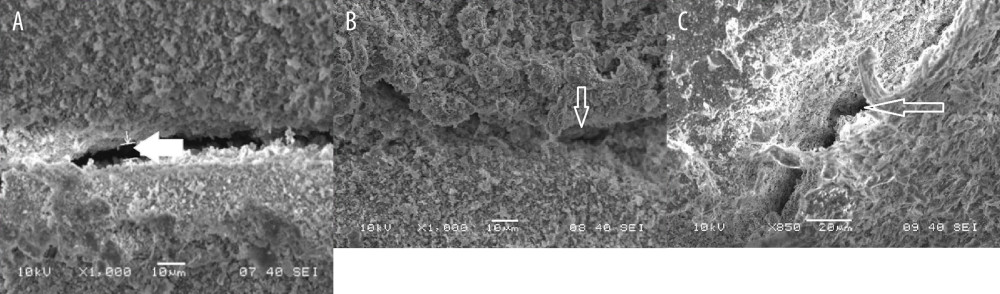 Figure 3. (A) SEM photomicrograph (5000×) showing marginal gap width at the apical third of the canal in a sample with SCT obturation. (B) SEM photomicrograph (5000×) showing marginal gap width at the middle third of the canal in a sample with SCT obturation. (C) SEM photomicrograph (5000×) showing marginal gap width at the coronal third of the canal in a sample with SCT obturation. Figure created using MS Paint, version 11.2301.22.0, Windows 11 Pro, (Microsoft Corporation).
Figure 3. (A) SEM photomicrograph (5000×) showing marginal gap width at the apical third of the canal in a sample with SCT obturation. (B) SEM photomicrograph (5000×) showing marginal gap width at the middle third of the canal in a sample with SCT obturation. (C) SEM photomicrograph (5000×) showing marginal gap width at the coronal third of the canal in a sample with SCT obturation. Figure created using MS Paint, version 11.2301.22.0, Windows 11 Pro, (Microsoft Corporation). 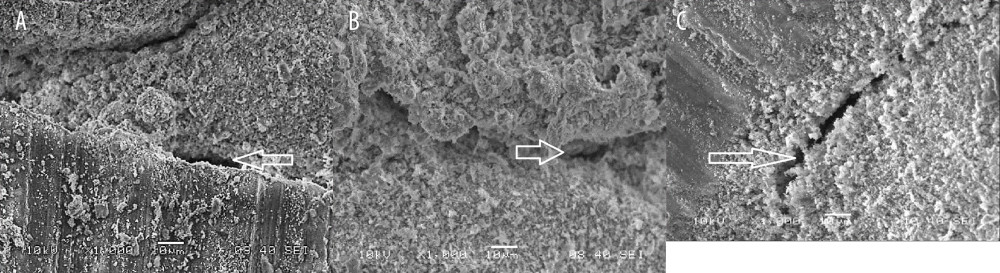 Figure 4. (A) SEM photomicrograph (5000×) showing marginal gap width at the apical third of the canal in a sample with cold lateral compaction technique obturation (CLCT). (B) SEM photomicrograph (5000×) showing marginal gap width at the middle third of the canal in a sample with cold lateral compaction technique obturation (CLCT). (C) SEM photomicrograph (5000×) showing marginal gap width at the coronal third of the canal in a sample with cold lateral compaction technique obturation (CLCT). Figure created using MS Paint, version 11.2301.22.0, Windows 11 Pro, (Microsoft Corporation).
Figure 4. (A) SEM photomicrograph (5000×) showing marginal gap width at the apical third of the canal in a sample with cold lateral compaction technique obturation (CLCT). (B) SEM photomicrograph (5000×) showing marginal gap width at the middle third of the canal in a sample with cold lateral compaction technique obturation (CLCT). (C) SEM photomicrograph (5000×) showing marginal gap width at the coronal third of the canal in a sample with cold lateral compaction technique obturation (CLCT). Figure created using MS Paint, version 11.2301.22.0, Windows 11 Pro, (Microsoft Corporation). 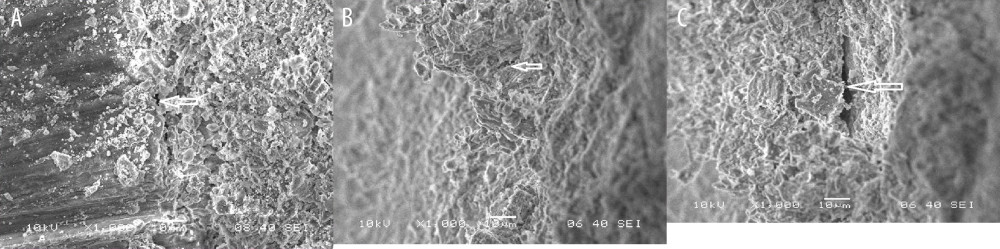 Figure 5. (A) SEM photomicrograph (5000×) showing marginal gap width at the apical third of the canal in a sample with continuous-wave technique (CWT) obturation. (B) SEM photomicrograph (5000×) showing marginal gap width at the middle third of the canal in a sample with continuous-wave technique (CWT) obturation. (C) SEM photomicrograph (5000×) showing marginal gap width at the coronal third of the canal in a sample with continuous-wave technique (CWT) obturation. Figure created using MS Paint, version 11.2301.22.0, Windows 11 Pro, (Microsoft Corporation).
Figure 5. (A) SEM photomicrograph (5000×) showing marginal gap width at the apical third of the canal in a sample with continuous-wave technique (CWT) obturation. (B) SEM photomicrograph (5000×) showing marginal gap width at the middle third of the canal in a sample with continuous-wave technique (CWT) obturation. (C) SEM photomicrograph (5000×) showing marginal gap width at the coronal third of the canal in a sample with continuous-wave technique (CWT) obturation. Figure created using MS Paint, version 11.2301.22.0, Windows 11 Pro, (Microsoft Corporation). 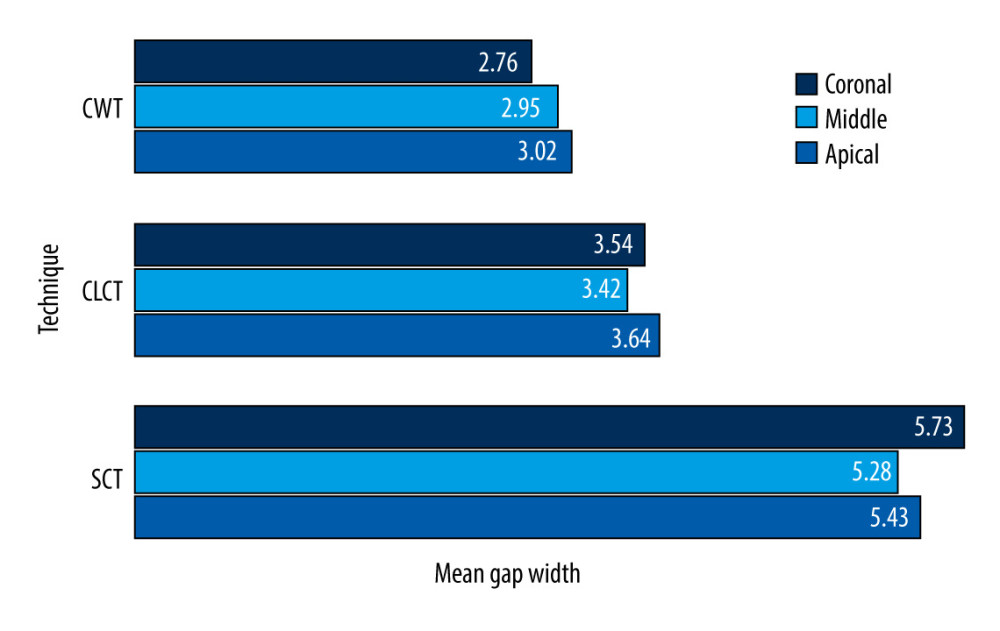 Figure 6. Graphical presentation of the differences between the 3 obturation techniques and the mean marginal gaps observed at 3 different levels. Figure created using MS Excel, version 20H2 (OS build 19042,1466), Windows 11 Pro, Microsoft Corporation).
Figure 6. Graphical presentation of the differences between the 3 obturation techniques and the mean marginal gaps observed at 3 different levels. Figure created using MS Excel, version 20H2 (OS build 19042,1466), Windows 11 Pro, Microsoft Corporation). References
1. Cohen S, Hargreaves KM: Pathways of the pulp, 2011; 352, St Louis, Mo, Elsevier Mosby
2. Polineni S, Bolla N, Mandava P, Marginal adaptation of newer root canal sealers to dentin: A SEM study: J Conserv Dent, 2016; 19(4); 360-63
3. Ingle JI, Newton CW, West JD, Obturation of the radicular space: Endodontics, 2002; 571-668, Hamilton, Ontario, BC Decker
4. Chavarria-Bolanos D, Komabayashi T, Shen I, Effects of heat on seven endodontic sealers: J Oral Sci, 2022; 64(1); 33-39
5. Mattoo KA, Garg R, Gupta A, Jain N, Toxicology and biocompatibility of dental materials: A review: Res J Pharmac Biol Chem Sci, 2012; 3(4); 1091-99
6. Kumar SA, Shivanna V, Naian MT, Shivamurthy GB, Comparative evaluation of the apical sealing ability and adaptation to dentine of three resin-based sealers: An in vitro study: J Cons Dent, 2011; 14(1); 16-20
7. Salz U, Poppe D, Sbicego S, Roulet JF, Sealing properties of a new root canal sealer: Int Endod J, 2009; 42(12); 1084-89
8. Li GH, Niu LN, Selem LC, Quality of obturation achieved by an endodontic core-carrier system with cross linked gutta-percha carrier in single-rooted canals: J Dent, 2014; 42; 1124-34
9. Waltimo T, Trope M, Haapasalo M, Ørstavik D, Clinical efficacy of treatment procedures in endodontic infection control and one year follow-up of periapical healing: J Endod, 2005; 31(12); 863-66
10. Al Shawkani HA, Mattoo K, Ali FM, Effect of two different experimental mixing ratios on selective physical, antibacterial and tissue compatibility properties of two commonly used endodontic root canal sealers – an in-vitro and in-vivo study: J Biomater Tissue Eng, 2022; 12(10); 2092-99
11. Al-Haddad A, Che Ab Aziz ZA, Bioceramic-based root canal sealers: A review: Int J Biomater, 2016; 2016; 9753210
12. Hammad M, Qualtrough A, Silikas N, Evaluation of root canal obturation: A three-dimensional in vitro study: J Endod, 2009; 35(4); 541-44
13. Lipski M, Root surface temperature rises in vitro during root canal obturation with thermoplasticized gutta-percha on a carrier or by injection: J Endod, 2004; 30(6); 441-43
14. Olczak K, Klimek L, Pawlicka H, Ex vivo area-metric analysis of root canal obturation using cold and warm gutta-percha: Adv Mater Sci, 2016; 16; 1-7
15. Sindi AS, Al Sanabani F, Al-Makramani BM, A Radiographic study of the root-to-crown ratio of natural permanent teeth in 81 Saudi adults: Med Sci Monit, 2022; 28; e936085
16. Yadav L, Mattoo KA, Kapoor A, Shuja S, Factors associated with post core correction of malpositioned teeth: International Journal of Research in Medical Sciences and Technology, 2015; 1(2); 5-7
17. Tyagi S, Mishra P, Tyagi P, Evolution of root canal sealers: An insight story: Eur J Gen Dent, 2013; 2(3); 199-218
18. Shahravan A, Haghdoost AA, Adl A, Effect of smear layer on sealing ability of canal obturation: A systematic review and meta-analysis: J Endod, 2007; 33(2); 96-105
19. Allan NA, Walton RE, Schaffer M, Setting times for endodontic sealers under clinical usage and in vitro conditions: J Endod, 2001; 27; 421-23
20. Nunes VH, Silva RG, Alfredo E, Adhesion of epiphany and AH Plus sealers to human root dentin treated with different solutions: Braz Dent J, 2008; 19; 46-50
21. Angerame D, De Biasi M, Pecci R, Analysis of single point and continuous wave of condensation root filling techniques by micro-computed tomography: Ann Ist Super Sanita, 2012; 48; 35-41
22. Munoz HR, Camacho-Cuadra K, In vivo efficacy of three different endodontic irrigation systems for irrigant delivery to working length of mesial canals of mandibular molars: J Endod, 2012; 38(4); 445-48
23. Oh S, Perinpanayagam H, Kum DJW, Evaluation of three obturation techniques in the apical third of mandibular first molar mesial root canals using micro-computed tomography: J Dent Sci, 2016; 11; 95-102
24. Celikten B, Uzuntas CF, Orhan AI, Evaluation of root canal sealer filling quality using a single-cone technique in oval shaped canals: An in vitro micro-CT study: Scanning, 2016; 38(2); 133-40
25. Guess GM, Edwards KR, Yang ML, Iqbal MK, Kim S, Analysis of continuous-wave obturation using a single-cone and hybrid technique: J Endod, 2003; 29(8); 509-12
26. Schneider SW, A comparison of canal preparations in straight and curved root canals: Oral Surg Oral Med Oral Pathol, 1971; 32(2); 271-75
27. Kikly A, Jaâfoura S, Kammoun D, Sahtout S, Sealing ability of endodontic cements: An in vitro study: Int J Dent, 2020; 2020; 5862598
28. Fernández R, Restrepo JS, Aristizábal DC, Álvarez LG, Evaluation of the filling ability of artificial lateral canals using calcium silicate-based and epoxy resin-based endodontic sealers and two gutta-percha filling techniques: Int Endod J, 2016; 49; 365-73
29. Eltair M, Pitchika V, Hickel R, Evaluation of the interface between gutta-percha and two types of sealers using scanning electron microscopy (SEM): Clin Oral Investig, 2018; 22; 1631-39
30. Kim JA, Hwang YC, Rosa V, Root canal filling quality of a premixed calcium silicate endodontic sealer applied using gutta-percha cone-mediated ultrasonic activation: J Endod, 2018; 44; 133-38
31. Atmeh AR, AlShwaimi E, The effect of heating time and temperature on epoxy resin and calcium silicate-based endodontic sealers: J Endod, 2017; 43; 2112-18
32. Macedo LM, Silva-Sousa Y, Silva SR, Influence of root canal filling techniques on sealer penetration and bond strength to dentin: Braz Dent J, 2017; 28; 380-84
33. Santos-Junior AO, Tanomaru-Filho M, Pinto JC, Effect of obturation technique using a new bioceramic sealer on the presence of voids in flattened root canals: Braz Oral Res, 2021; 35; e028
34. Qu W, Bai W, Liang YH, Gao XJ, Influence of warm vertical compaction technique on physical properties of root canal sealers: J Endod, 2016; 42(12); 1829-33
35. Shen I, Daniel J, Vo K, Ahn C, Use of micro-CT to examine effects of heat on coronal obturation: J Oral Sci, 2022; 64(3); 224-27
36. Ho ES, Chang JW, Cheung GS, Quality of root canal fillings using three gutta-percha obturation techniques: Restor Dent Endod, 2016; 41(1); 22-28
37. Pinto JC, Pivoto-João MM, Guerreiro-Tanomaru JM, Continuous wave of condensation improves the filling of curved canals: A micro-CT study: Odovtos – International Journal of Dental Sciences, 2023; 305-15
38. Keleş A, Alcin H, Kamalak A, Versiani MA, Micro-CT evaluation of root filling quality in oval-shaped canals: Int Endod J, 2014; 47(12); 1177-84
39. Lea CS, Apicella MJ, Mines P, Comparison of the obturation density of cold lateral compaction versus warm vertical compaction using the continuous wave of condensation technique: J Endod, 2005; 31(1); 37-39
40. Saunders WP, Saunders EM, Herd D, Stephens E, The use of glass ionomer as a root canal sealer – a pilot study: Int Endod J, 1992; 25(5); 238-44
41. Iglecias EF, Freire LG, de Miranda Candeiro GT, Presence of voids after continuous wave of condensation and single-cone obturation in mandibular molars: A micro-computed tomography analysis: J Endod, 2017; 43(4); 638-642
42. Zhang W, Li Z, Peng B, Assessment of a new root canal sealer’s apical sealing ability: Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2009; 107; e79-e82
43. Monticelli F, Osorio R, Mazzitelli C, Limited decalcification/diffusion of self-adhesive cements into dentin: J Dent Res, 2008; 87; 974-79
Figures
Figure 1. (A) Schematic depiction of the specimen measurements and their planned sections. (B) An exemplary specimen showing access cavity preparation. (C) An exemplary specimen showing the completed obturation. Figure created using MS PowerPoint, version 20H2 (OS build 19042,1466), Windows 11 Pro, (Microsoft corporation).Figure 2. (A) An exemplary intra-oral periapical radiograph showing the radiographic quality of single-cone technique obturation. (B) An exemplary intra-oral periapical radiograph showing the radiographic quality of Cold Lateral Compaction Technique obturation. (C) An exemplary intra-oral periapical radiograph showing the radiographic quality of continuous-wave down technique. Photographs taken using a digital single-lens reflex (DSLR) camera (Canon EOS 700D) with 100 mm macro lens) with/without ring flash.Figure 3. (A) SEM photomicrograph (5000×) showing marginal gap width at the apical third of the canal in a sample with SCT obturation. (B) SEM photomicrograph (5000×) showing marginal gap width at the middle third of the canal in a sample with SCT obturation. (C) SEM photomicrograph (5000×) showing marginal gap width at the coronal third of the canal in a sample with SCT obturation. Figure created using MS Paint, version 11.2301.22.0, Windows 11 Pro, (Microsoft Corporation).Figure 4. (A) SEM photomicrograph (5000×) showing marginal gap width at the apical third of the canal in a sample with cold lateral compaction technique obturation (CLCT). (B) SEM photomicrograph (5000×) showing marginal gap width at the middle third of the canal in a sample with cold lateral compaction technique obturation (CLCT). (C) SEM photomicrograph (5000×) showing marginal gap width at the coronal third of the canal in a sample with cold lateral compaction technique obturation (CLCT). Figure created using MS Paint, version 11.2301.22.0, Windows 11 Pro, (Microsoft Corporation).Figure 5. (A) SEM photomicrograph (5000×) showing marginal gap width at the apical third of the canal in a sample with continuous-wave technique (CWT) obturation. (B) SEM photomicrograph (5000×) showing marginal gap width at the middle third of the canal in a sample with continuous-wave technique (CWT) obturation. (C) SEM photomicrograph (5000×) showing marginal gap width at the coronal third of the canal in a sample with continuous-wave technique (CWT) obturation. Figure created using MS Paint, version 11.2301.22.0, Windows 11 Pro, (Microsoft Corporation).Figure 6. Graphical presentation of the differences between the 3 obturation techniques and the mean marginal gaps observed at 3 different levels. Figure created using MS Excel, version 20H2 (OS build 19042,1466), Windows 11 Pro, Microsoft Corporation). Tables
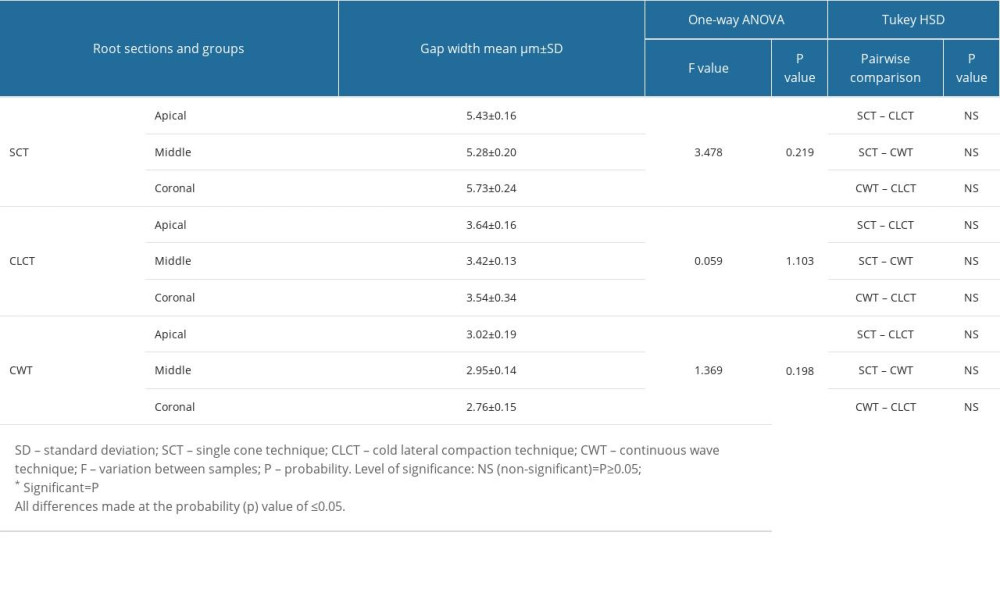 Table 1. Comparative differences in mean interval voids at different cross-sections of the root within each group.
Table 1. Comparative differences in mean interval voids at different cross-sections of the root within each group.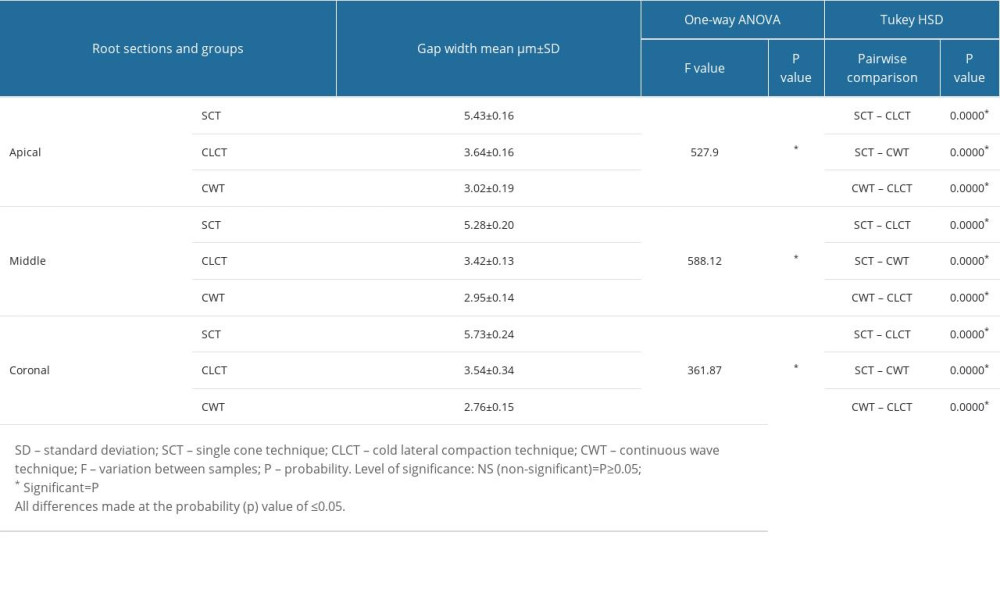 Table 2. Comparative differences in mean interval voids at different cross-sections of the root among the 3 groups.Table 1. Comparative differences in mean interval voids at different cross-sections of the root within each group.Table 2. Comparative differences in mean interval voids at different cross-sections of the root among the 3 groups.
Table 2. Comparative differences in mean interval voids at different cross-sections of the root among the 3 groups.Table 1. Comparative differences in mean interval voids at different cross-sections of the root within each group.Table 2. Comparative differences in mean interval voids at different cross-sections of the root among the 3 groups. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387