02 November 2023: Clinical Research
Effect of Dynamic Taping versus Kinesiology Taping on Pain, Foot Function, Balance, and Foot Pressure in 3 Groups of Plantar Fasciitis Patients: A Randomized Clinical Study
Dong-Ho Kim1ABCDEF, Yongwoo LeeDOI: 10.12659/MSM.941043
Med Sci Monit 2023; 29:e941043






Abstract
BACKGROUND: Biomechanical dynamic tape supports muscles, joints, and ligaments and is used in ankle and foot injuries. Kinesiology tape (KT), also known as elastic tape, is widely used in sports medicine. Plantar fasciitis, due to inflammation of the plantar fascia, is a common cause of heel pain. This study aimed to compare the effects of dynamic taping and KT on pain, function, and balance in 3 groups of patients with plantar fasciitis.
MATERIAL AND METHODS: Sixty-nine patients with plantar fasciitis were randomly assigned to the dynamic taping with physical therapy (PT) group, the KT with PT group, and the control group (23 each). All groups received conservative physical therapy. Dynamic taping and KT were performed twice a week for 4 weeks, and the taping was removed after 12 h of application. Patients’ pain, foot function, and balance were assessed using the visual analog scale (VAS), foot function index (FFI), and Y-balance test (YBT), respectively, before and immediately after the intervention.
RESULTS: In the FFI and YBT, the treatment provided to the dynamic taping with PT group with PT showed a greater effect than in the KT with PT group with PT (P<0.05), and the control group showed the lowest effect. Dynamic taping and KT with PT did not show significant differences in VAS and foot pressure, but both were more effective than the control group (P<0.05).
CONCLUSIONS: The results of this study suggest that dynamic taping with PT is the most effective method for FFI and YBT in patients with plantar fasciitis, and that dynamic taping and KT with PT are effective methods for treating pain and foot pressure.
Keywords: Athletic Tape, Fasciitis, Plantar, pain management, Physical Therapy Modalities, postural balance, Humans, Pain, Lower Extremity, Ankle
Background
Plantar fasciitis is a disease caused by degeneration of the plantar fascia of the heel, and is characterized by localized pain in the heel [1]. This is often an overuse injury primarily due to a repetitive strain causing micro-tears of the plantar fascia but can occur as a result of trauma or other multifactorial causes [2]. Plantar fasciitis is one of the most common foot diseases [3], accounting for about one-quarter of foot injuries [4], with a prevalence of 3.6~7% [5]. Plantar fasciitis occurs frequently in active groups, and people with plantar fasciitis have been found to have lower physical function, quality of life, and mental health than those without it [6].
The plantar fascia is a complex fibrous tissue that extends over the entire foot and, starting from the medial calcaneal tubercle, attaches to the phalanx to support the arch and provide stability to the foot [7]. The plantar fascia supports weight in static postures and dynamic movements, and as the arch-spring stores and releases elastic energy during walking, the length of the fascia increases and shortens throughout walking, enabling efficient use of energy [8].
Overuse, which causes micro-tears of the plantar fascia, is the main cause, but it can also be caused by various causes, such as flat foot, pes cavus, or excessive pronation and supination of the foot [9]. Among them, flat feet are a representative cause of plantar fasciitis, which occurs when the inner arch of the foot descends during weight-bearing and is accompanied by pronation of the subtalar joint during walking, causing plantar fasciitis [10].
Elongation and weakness of the plantar fascia due to flat feet cause excessive activity of intrinsic and extrinsic muscles and abnormal alignment of the foot, which can lead to a decrease in proprioception of the foot and cause plantar fasciitis and foot dysfunction. Therefore, interventions to improve this are necessary [11].
There are numerous non-surgical treatments to relieve plantar fasciitis pain, and typical treatments include rest, exercise (extension and resistance exercise), conservative physical therapy, braces, and taping [12]. Interventions for plantar fasciitis include NSAIDs for pain control, as well as deep friction massage and shoe inserts. Stretching and rehabilitation of the muscles around the feet are also useful. Surgery is the last option to be considered when conservative treatments are not successful [13]. Taping is a conservative treatment that is easy to apply and can be quickly effective [14].
Taping is divided into non-elastic taping and elastic taping, and the purpose and effect vary depending on which taping method is used. Non-elastic taping has no elasticity and is primarily used for mechanical restraint purposes. Elastic taping is largely divided into dynamic taping and kinesiology taping (KT) [15]. KT, developed by Kenso Kase, can correct ligament damage and improve proprioceptive sensation, and in particular, it can improve the disadvantages of existing rigid tapes due to the elasticity of the tape [16,17].
Dynamic taping with added elasticity was developed by Ryan Kendrick as a recent technology development [18]. Dynamic taping has the advantage of allowing participation in daily activities without restrictions, even after application, and not restricting joint movements. This is due to the nature of the material, in which the tape stretches both horizontally and vertically [19]. Because of these advantages, dynamic taping can be used not only for training in individual or team sports, but also for prevention of limb injury during games [20,21].
In a previous study by Song et al [22], dynamic taping and KT were compared for plantar flexor muscle endurance and muscle fatigue, and as a result, dynamic taping was suggested as one of the intervention methods for reducing muscle endurance and muscle fatigue. Lim et al [23] compared the effects of dynamic taping and KT on and balance and center of gravity in barefoot conditions, and the front-back and left-right shaking during balance and walking were greatly reduced by dynamic taping (
Although various types of taping are used in clinical practice, studies comparing the effect with dynamic taping have not been actively conducted. Dynamic taping and KT both rely on elasticity, but the main effect is different. KT focuses on improving circulation and stimulating proprioception, while dynamic taping focuses on the mechanical effect of muscles, helping muscles work and maximizing energy efficiency [22]. Many previous studies assessed the effect of KT and other tapings on plantar fasciitis pain, but there is insufficient research comparing the effects of dynamic taping, KT, and conservative physical therapy. Therefore, the objective of the present study was to evaluate and compare the effects of dynamic taping with PT, KT with PT, and conservative PT alone on pain, function, foot pressure, and balance in patients with plantar fasciitis over a 4-week intervention period.
Material and Methods
SUBJECTS:
This study was conducted with the approval of the Research Ethics Review Committee of Sahmyook University (approval number: SYU 2022-10-006). Additionally, this study was conducted in accordance with the Declaration of Helsinki and its subsequent amendments. Before participating in the experiment, the purpose, process, and expected effects of the study were sufficiently explained to the participants, and written consent was obtained from all participants in the experiment.
Sixty-nine patients who visited Clinic P in Seoul in 2022 and were diagnosed with plantar fasciitis participated. The inclusion criteria were local pain in the heel and sole of the foot due to plantar fasciitis, pain when taking the first steps in the morning or taking a break and walking, no deformation of the ankle joint, without cognitive impairment or communication problems, and consented to participate. The exclusion criteria were allergy to adhesives, joint inflammatory findings, received steroid injections within the last 3 months, sensory or motor paralysis, and surgery within the last 6 months [25].
The calculation of study subjects was calculated with G*power 3.1 [26]. The study’s sample size was calculated using G*power 3.1 software with an ANOVA (repeated-measures, within-between interaction). We set the effect size to 0.25, the alpha error probability (significance level) to 0.05, and the power to 0.95. Anticipating 5% potential dropouts over the 4-week study period, we increased the required sample size from 66 to a total of 69 subjects. We performed repeated-measures ANOVA with 3 groups and 2 measurements, assuming a correlation among repetitive measures of 0.5 and a nonsphericity correction epsilon of 1.
PROCEDURE:
Participants were recruited through promotional materials within the clinic. Group assignment was randomized by having participants take a paper, representing 1 of the 3 groups, from a mixed envelope during their visit.
Before the experiment, general characteristics such as gender, age, height, weight, and body mass index (BMI) were recorded. We also measured participants’ VAS for pain, FFI for foot function, YBT for balance, and foot pressure.
Dynamic taping, KT, and conservative physical therapy were applied twice a week for 4 weeks. The application of dynamic taping and KT was to be removed after maintaining the taping for 12 h, and explanations on possible skin problems and how to deal with them were fully explained. After each intervention was performed for 4 weeks, post-intervention evaluation was performed.
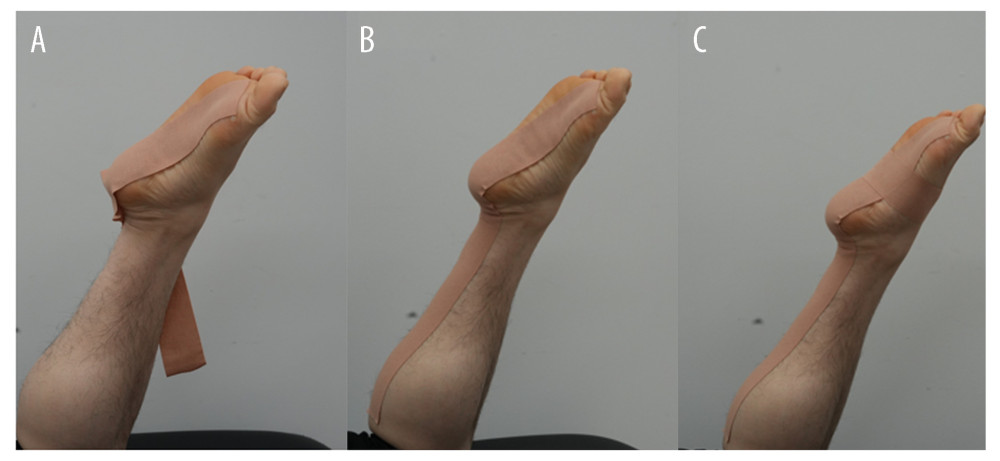
DYNAMIC TAPING: In this study, to attach the tape, the calf hair was removed with a razor and dynamic taping (Tape-Pro, TS, Inc, Gimpo, Korea) was applied. Taping was applied by placing the patient in a position where the length of the muscles was shortened by inverting and plantar flexing the ankle as much as possible while the knee was bent 90 degrees while lying face down on the bed. This is to maximize the use of shock absorption and elastic energy applied to the sole and ankle by using the elasticity, which is a characteristic of taping, by applying the body part in a close state. The application site was applied in an I-shape from the metatarsal head to the calf through the plantar fascia and Achilles tendon (to the height of the fibula head), and the taping tension was applied at about 10%. After I-shaped taping, taping was applied from the base of the 5th metatarsal to the medial arch in dorsiflexion to support the arch (Figure 1). The application of dynamic taping was directly performed by a physical therapist in the 10th year of clinical practice and proceeded according to previous studies [27]. Tape was applied twice a week for 4 weeks, and was removed after maintaining in place for more than 12 h on the same day.
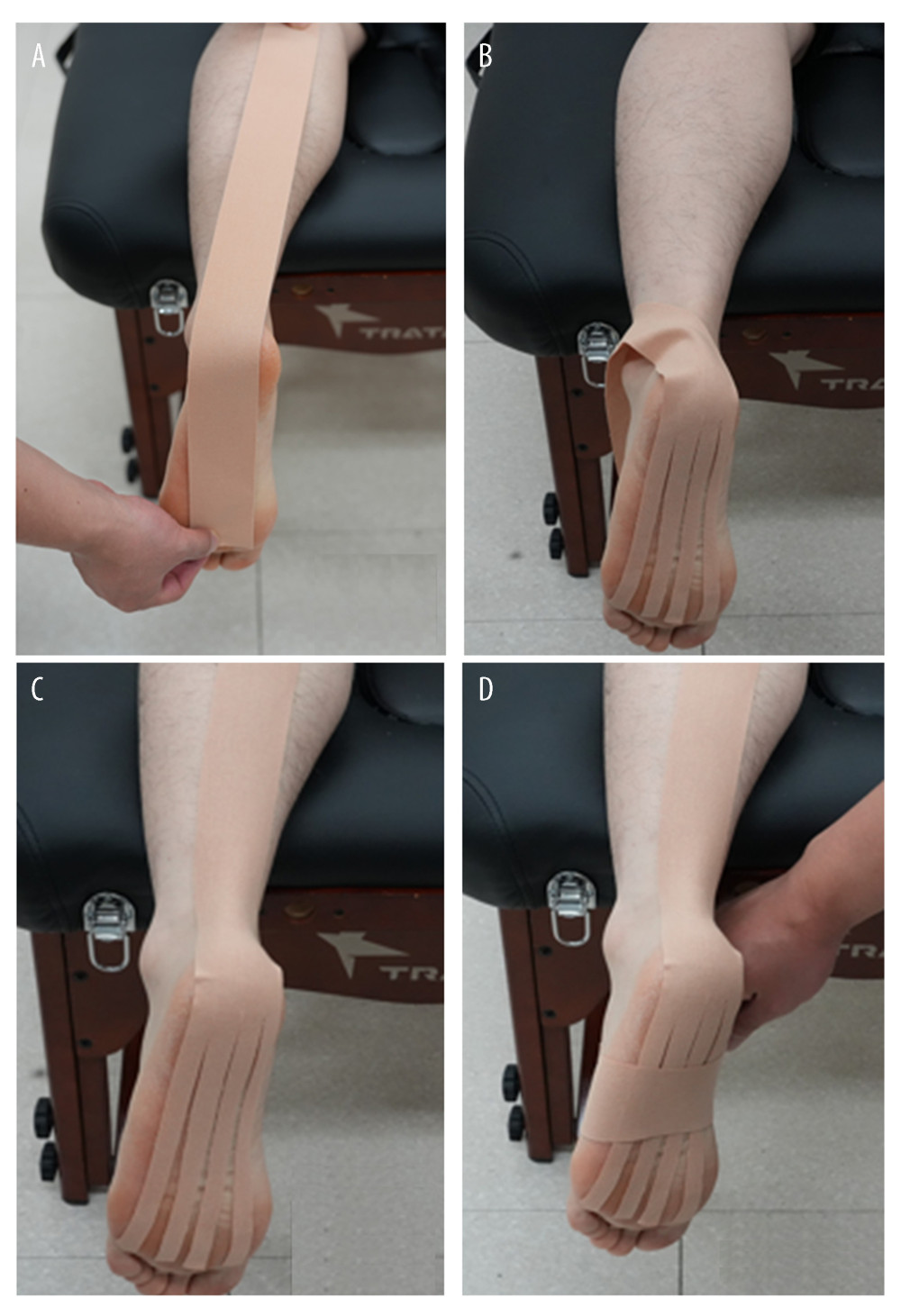
KINESIOLOGY TAPING (KT): In this study, to attach the taping, the calf hair was removed with a razor and KT (Nitto Kinesiology tape, Nitto, Osaka, Japan) was applied. The taping was applied with the patient lying face down on the bed, extending the knee, dorsiflexing the ankle to the maximum, and maximally stretching the plantar fascia and calf muscles. The application was applied in an I-shape starting from the metatarsal head and passing through the plantar fascia and Achilles tendon to the calf muscle (to the height of the fibular head). About 50% of the taping tension was applied to the Achilles tendon area, and then about 15% of the taping tension was applied to the calf muscle area. After I-shaped taping, taping was applied at 50% of the taping tension from the base of the 5th metatarsal to the medial arch in dorsiflexion to support the arch (Figure 2). The application of KT was directly performed by a physical therapist with 10 years of clinical practice, and proceeded according to previous studies [28]. Taping was applied twice a week for 4 weeks, and was removed after maintaining in place for more than 12 h on the same day.
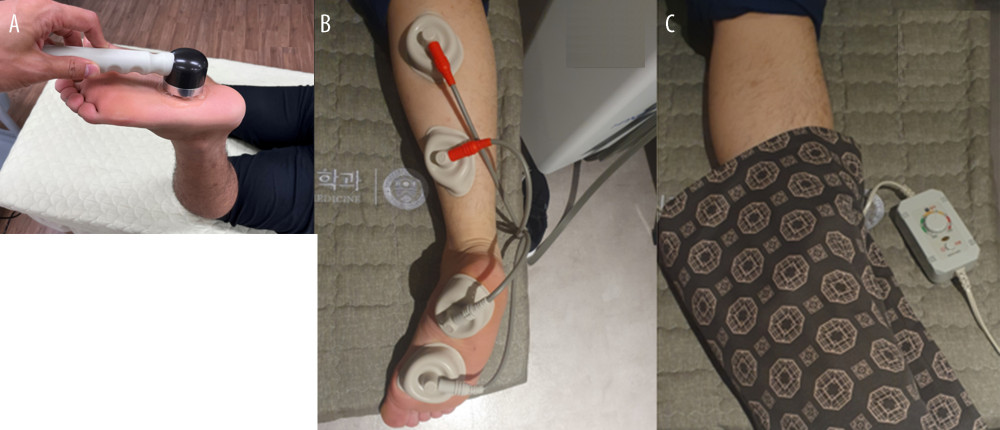
CONSERVATIVE PHYSICAL THERAPY: Conservative physical therapy was applied to the painful area twice a week for 4 weeks to relieve the patient’s pain and improve blood circulation. A second-year physical therapist applied an electric hot pack (SH-1100, Sejong Healthcare, Korea) to the painful area at 45 degrees for 15 min, and applied ultrasound treatment (HS-502, Hanil-TM, Korea) to the heel pain area at 1 MHz for 5 min. The interference wave (H-401, Hanil-TM, Korea) was applied to the calf and sole for 15 min at 4000 Hz (Figure 3).
VISUAL ANALOG SCALE OF PAIN: The VAS of pain can be used to measure pain progression, both acute and chronic, and to compare pain between patients with similar conditions [29]. The VAS was designed to mark the level of pain felt by the subject on a 100-mm-long horizontal line. The left starting point, ‘0’ at the beginning, means no pain, and the right end, 100 points, means maximum pain. The validity of the VAS was 0.76~0.84, and the reliability was 0.60~0.77 [30]. The minimum clinically important difference (MCID) of the VAS ranges from 1.8 to 5.2 points [31].
FOOT FUNCTION INDEX: The foot function index (FFI) was developed as a self-reported assessment that measures several aspects of foot function. It consists of 23 items divided into 3 subscales of pain, function, and daily life that quantify the impact of foot pathology on the patient’s pain, disability, and activity limitation [32]. Each item is scored on a scale of 1 to 10, with a maximum score of 90 for pain, a maximum of 90 for function, and a maximum of 50 for activity limitation, for a total possible score of 230. The FFI was designed to measure current conditions and changes in conditions [33]. The validity study of FFI, which was investigated through correlation with Medical Outcomes Study Short Form-36 (SF-36), showed that the FFI is a reasonable tool for checking the patient’s status [34]. The intraclass correlation coefficient (ICC) of the Korean foot function index used in this study shows excellent reliability with pain 0.90, disability 0.94, and activity limitation 0.91 [35]. The MCID of the FFI is 7 points for the total scale [36].
Y-BALANCE TEST: The Y-balance test (YBT) is one of the most commonly used assessment tools to measure dynamic balance and is used to measure leg strength, flexibility, and proprioception [37]. The YBT measures reach by extending the opposite leg as far as possible in 3 directions (forward, outside back, and inside back) while standing on 1 foot. A difference of more than 1 cm in the length of the legs of the subjects can affect the results [38]. YBT measurements were obtained as the composite reach, which was obtained by dividing the sum of the 3 reach directions by 3 times the length of the lower extremity and then multiplying by 100%. The YBT has excellent reliability, with intra-rater reliability of 0.91 and inter-rater reliability of 0.99 [38]. The minimal detectable change values of the YBT range from 5.87% to 7.84% [39].
FOOT PRESSURE: Foot pressure was measured using a Gateview analyzer device (alFOOTs, Inc., Seoul, Korea) to measure the foot pressure inside the heel of the affected side and the left-right foot pressure ratio. The size of the Gaitview device is 550×480×35 mm, the thickness is 0.15 mm, the sensor size is 0.73 cm2, there are 2304 (48×48) sensors, and the maximum pressure is 100 N/cm2 [40]. Data processing was measured using the static test mode using Gaitview software [41]. Foot pressure was measured before and after the intervention. After walking in place for 10 s, the subjects stepped onto the device barefoot and gazed straight ahead for 30 s in a comfortable standing position. It was measured 3 times and the average value was used [42]. The inter- and intra-rater reliability of the Gaitview ranged from 0.69 to 0.97 [43].
STATISTICAL ANALYSIS:
Statistical analyses in this study were carried out using IBM SPSS 19.1 software. The general characteristics of the participants were summarized by calculating the mean and standard deviation of all variables. Normality tests for age, height, weight, BMI, and leg length data were conducted using the Shapiro-Wilk test.
The homogeneity of sex across different groups was assessed using a chi-square test. The data were tabulated in a contingency table, presenting the frequency of males and females in each group (Table 1). A chi-square test was then used to check if these distributions were significantly different from each other. Differences before and after within groups were analyzed using the paired-sample t test. One-way ANOVA was used to identify significant differences between the groups in terms of the amount of change in the variables of interest. If the ANOVA showed a significant effect, Scheffe’s post hoc analysis was conducted to identify which specific groups significantly differed from each other. All tests performed in this study were 2-sided, and a P value less than 0.05 was considered statistically significant. The P value threshold of 0.05 means that if the calculated P value was less than 0.05, the null hypothesis was rejected and the result was considered to show a statistically significant difference or correlation.
Results
CHANGES OF VISUAL ANALOG SCALE:
In the VAS, the dynamic taping group significantly decreased from 83.92±8.84 points before intervention to 63.26±8.20 points after intervention (P<0.001). The KT group significantly decreased from 86.08±7.06 points before intervention to 69.13±8.56 points after intervention (P<0.001), and the conservative physical therapy group significantly decreased from 85.21±7.30 points before intervention to 75.65±8.56 points after intervention (P<0.001). The difference between the values before and after the intervention decreased by 20.21±7.75 points in the dynamic taping group, 16.95±5.78 points in the KT group, and 9.56±6.72 points in the conservative physical therapy group, showing a statistically significant difference between the 3 groups (P<0.001). In the post hoc test to compare the before and after changes between the 3 groups, there was no statistically significant difference between the dynamic taping group and the KT group (mean difference: −3.26, 95% CI: −8.28,1.76), and these 2 groups were more improved than the conservative physical therapy group (KT mean difference: 7.39, 95% CI: 2.36, 12.41; Dynamic taping mean difference: 10.65, 95% CI: 5.62, 15.67) (Table 2).
CHANGES OF FOOT FUNCTION INDEX:
In pain, a subscale of the foot function index, the dynamic taping with PT group significantly decreased from 83.10±6.20 points before intervention to 56.89±5.14 points after intervention (
In function, a subscale of the foot function index, the dynamic taping with PT group significantly decreased from 80.53±5.33 points before intervention to 51.35±5.50 points after intervention (
In the activity limitation, a subscale of the foot function index, the dynamic taping with PT group significantly decreased from 73.91±6.86 points before intervention to 44.92±6.73 points after intervention (P<0.001), and the KT with PT group significantly decreased from 72.17±6.32 points before intervention to 49.56±6.05 points after intervention (P<0.001). In addition, the conservative PT group significantly decreased from 71.88±6.18 points before intervention to 60.86±7.53 points after intervention (P<0.001). The difference between the values before and after the intervention decreased by 28.98±5.72 points in the dynamic taping with PT group, 22.60±3.17 points in the KT with PT group, and 11.01±4.07 points in the conservative PT group, showing statistically significant differences among the 3 groups (P<0.001). In the post hoc test to compare the before and after changes between the 3 groups, there were significant differences among the 3 groups (P<0.05), and the treatment in the dynamic taping with PT group was more effective than in the KT with PT group and the conservative PT group (P<0.05). The treatment in the taping group was more effective than in the conservative PT group (P<0.05) (Table 3).
CHANGES OF THE Y-BALANCE TEST:
In the YBT, the dynamic taping with PT group significantly decreased from 65.11±6.53% before intervention to 72.02±5.35% after intervention (P<0.001), and the KT with PT group significantly decreased from 61.17±6.43% before intervention to 66.15±6.62% after intervention (P<0.001). In addition, the conservative PT group significantly decreased from 62.16±7.09% before intervention to 65.03±7.15% after intervention (P<0.001). The difference between the values before and after the intervention was 6.90±1.98% in the dynamic taping with PT group, 4.98±1.86% in the KT with PT group, and 2.86±1.12% in the conservative PT group, showing statistically significant differences among the 3 groups (P<0.001). In the post hoc test to compare the before and after changes between the 3 groups, there were significant differences among the 3 groups (P<0.05), and the treatment in the dynamic taping with PT group was more effective than in the KT with PT group (mean difference: 1.19, 95% CI: 0.66, 3.17) and the conservative PT group (mean difference: 4.03, 95% CI: 2.77, 5.29). The treatment in the taping group was more effective than in the conservative PT group (KT mean difference: −2.11, 95% CI: −3.37, −0.85; Dynamic taping: −4.03, 95% CI: −5.29, −2.77) (P<0.05) (Table 4).
CHANGES OF FOOT PRESSURE:
Medial heel foot pressure in the dynamic taping with PT group significantly decreased from 166.47±6.98 Kpa before intervention to 158.23±6.88 Kpa after intervention (
The foot pressure ratio significantly decreased in the dynamic taping with PT group, from 52.87±1.66% before intervention to 50.57±1.88% after intervention (P<0.001), and in the KT with PT group it significantly decreased from 53.12±2.42% before intervention to 50.65±2.56% after intervention (P<0.01). In the conservative PT group, there was no significant difference, from 51.97±2.13% before intervention to 51.66±2.26% after intervention. The difference between the values before and after the intervention decreased to 2.30±2.45% in the dynamic taping with PT group, 2.47±3.31% in the KT with PT group, and 0.31±1.75% in the conservative PT group, showing statistically significant differences among the 3 groups (P<0.01). In the post hoc test to compare the before and after changes among the 3 groups, there was no statistically significant difference between the dynamic taping with PT group and the KT with PT group, and treatments in both taping groups were more effective than in the conservative PT group (P<0.05) (Table 5).
Discussion
This study was conducted to determine which intervention method – dynamic taping with PT, KT with PT, or conservative PT – is more effective for plantar fasciitis. We found that dynamic taping with conservative PT was most effective for foot function and balance (
In this study, the treatments in the dynamic taping with PT group and the KT with PT group were found to be significantly more effective in reducing pain than in the conservative PT group (
Since the foot performs many functional activities, it is important to evaluate both pain and function. Therefore, we used the foot function index to evaluate foot function. The results showed that there was a significant difference in the foot function index within the group (
Patients with plantar fasciitis tend to shift their center of gravity to one side due to pain, which affects their sense of balance [45]. We found a significant difference among groups in the Y-danamic balance test (
In previous studies targeting patients with plantar fasciitis and patients with flat feet, the effects of dynamic taping and kinesio taping were studied using the Y-danamic balance test [23,25]. In a previous study by Yunjin Han [25], kinesio taping was applied from the sole of the foot to the posterior tibialis muscle and compared results with the conservative PT group. Lim et al [23] compared the effects of dynamic taping and kinesio taping on patients with flat feet. In both previous studies, it was confirmed that elastic taping was more effective in improving YBT compared to the control group. These results suggest that applying dynamic taping and kinesio taping, which are types of elastic taping, to the plantar fascia and calf muscles may have a positive effect on YBT by increasing the proprioceptive feedback of the intrinsic and extrinsic muscles of the foot and assisting the biomechanical role of the muscles. It is thought that dynamic taping, which has strong elastic resistance and mechanical action, has a better effect than KT.
In the experimental results of the heel medial foot pressure and pressure ratio in the present study, there was a significant difference between the dynamic taping with PT group and the KT with PT group (
As a limitation of this study, first, the taping was intended to last for 12 h, but partial falls while the participants were dressing or taking a shower were completely uncontrollable. Second, the age of the subjects was not controlled, and the number of participants was small, so larger studies with participants of various ages are needed to produce more generalizable results. Third, the thickness of the plantar fascia and the height of the navicular bone could not be examined. Comparing the thickness of the plantar fascia and the height of the navicular bone before and after taping application is thought to be more objective and to provide good research data. Fourth, the intra-tester or inter-tester reliability of the equipment used to measure foot pressure was not measured in patients.
Conclusions
The results of this study show that dynamic taping with PT is the most effective method for FFI and YBT in patients with plantar fasciitis, and dynamic taping and KT with PT can be used as effective methods for pain and foot pressure.
Tables
Table 1. General characteristic of subjects (N=69).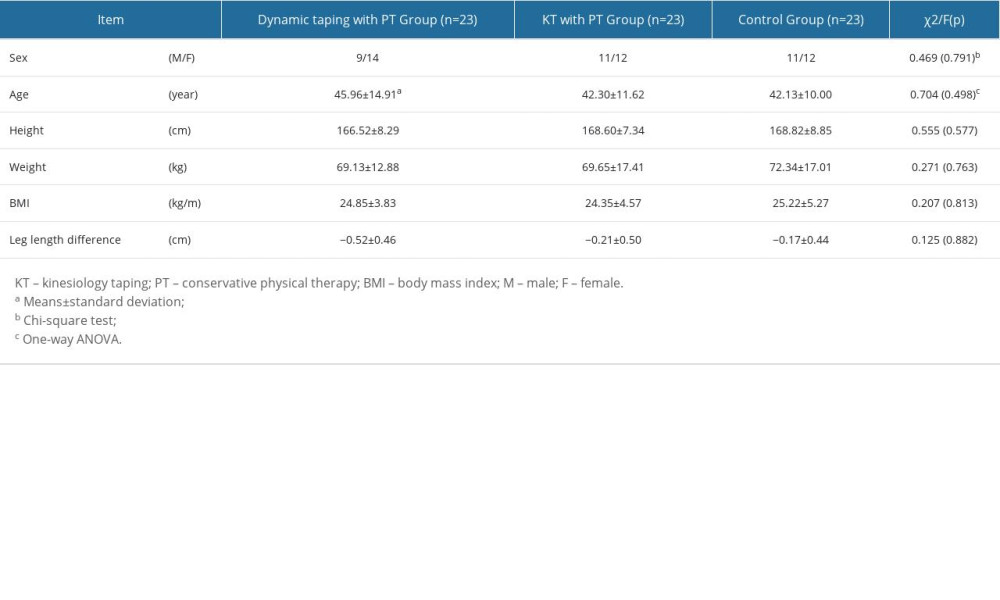 Table 2. Changes of visual analog scale according to intervention methods (N=69).
Table 2. Changes of visual analog scale according to intervention methods (N=69).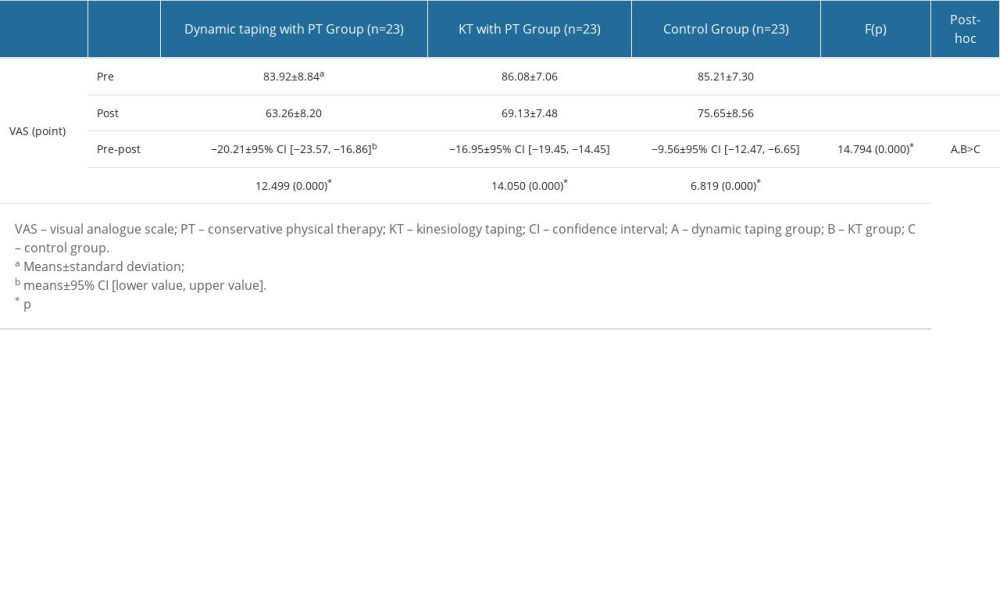 Table 3. Changes of foot function index according to intervention methods (N=69).
Table 3. Changes of foot function index according to intervention methods (N=69).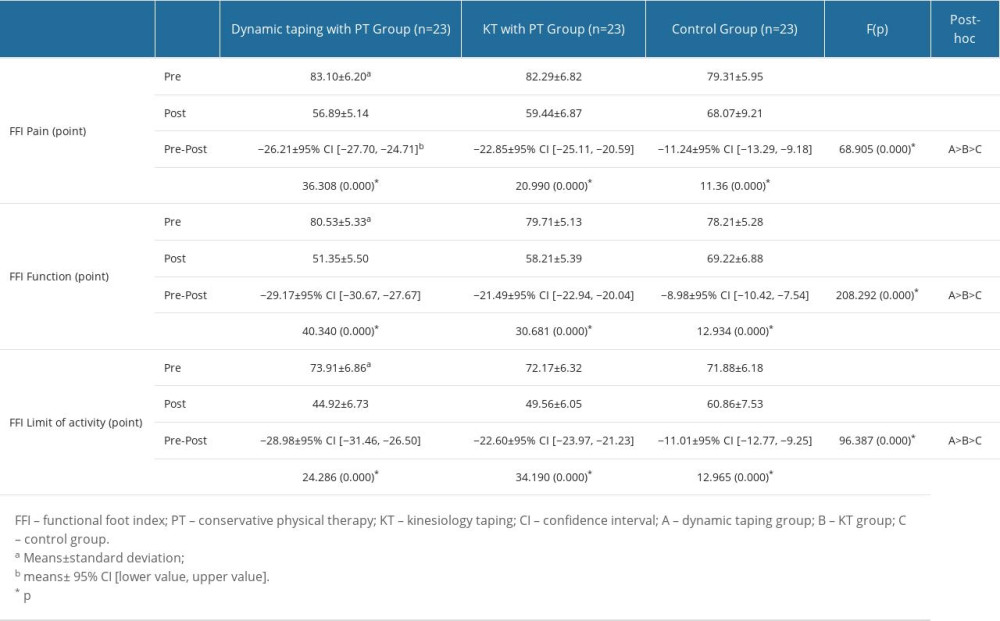 Table 4. Changes of the Y-balance test according to intervention methods (N=69).
Table 4. Changes of the Y-balance test according to intervention methods (N=69).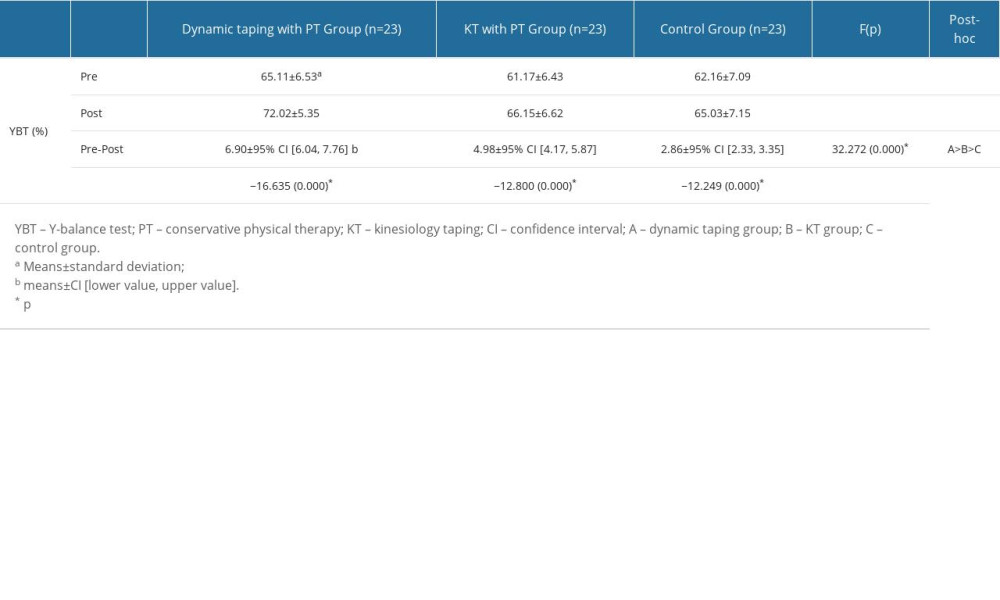 Table 5. Changes of medial heel pressure according to intervention method (N=69).
Table 5. Changes of medial heel pressure according to intervention method (N=69).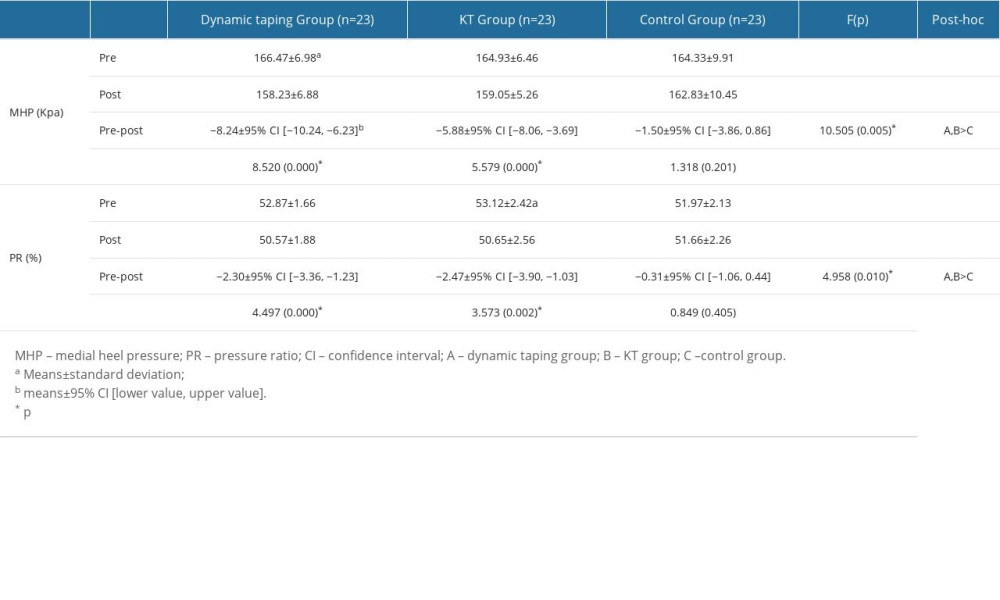
References
1. Becker BA, Childress M, Common foot problems: Over-the-counter treatments and home care: Am Fam Physician, 2018; 98; 298-303
2. Finkenstaedt T, Siriwanarangsun P, Statum S, The calcaneal crescent in patients with and without plantar fasciitis: an ankle MRI study: Am J Roentgenol, 2018; 211(5); 1075-82
3. Landorf KB, Radford JA, Keenan AM, Redmond AC, Effectiveness of low-Dye taping for the short-term management of plantar fasciitis: J Am Podiatr Med Assoc, 2005; 95; 525-30
4. Chen TL, Wong DW, Peng Y, Zhang M, Prediction on the plantar fascia strain offload upon Fascia taping and Low-Dye taping during running: J Orthop Translat, 2020; 20; 113-21
5. Rathleff MS, Mølgaard CM, Fredberg U, High-load strength training improves outcome in patients with plantar fasciitis: A randomized controlled trial with 12-month follow-up: Scand J Med Sci Sports, 2015; 25; e292-300
6. Landorf KB, Kaminski MR, Munteanu SE, Clinical measures of foot posture and ankle joint dorsiflexion do not differ in adults with and without plantar heel pain: Sci Rep, 2021; 11; 6451
7. Cheung JT, Zhang M, An KN, Effect of Achilles tendon loading on plantar fascia tension in the standing foot: Clin Biomech (Bristol, Avon), 2006; 21; 194-203
8. Welte L, Kelly LA, Kessler SE, The extensibility of the plantar fascia influences the windlass mechanism during human running: Proc Biol Sci, 2021; 288; 20202095
9. Arnold MJ, Moody AL, Common running injuries: Evaluation and management: Am Fam Physician, 2018; 97; 510-16
10. Shih YF, Chen CY, Chen WY, Lin HC, Lower extremity kinematics in children with and without flexible flatfoot: A comparative study: BMC Musculoskelet Disord, 2012; 13; 31
11. Jung H-W, Yoo W-GComparison of flatfoot on the activities of medial and lateral plantar flexor muscle during heel rising: Physical Therapy Korea, 2021; 28; 132-37 [in Korean]
12. Agrawal S, Deshpande M, Effectiveness of Mulligan’s taping for the short term management of plantar heel pain – randomised control trial: International Journal of Biomedical and Advance Research, 2015; 6; 531-36
13. Mcclinton S, Heiderscheit B, Mcpoil TP, Flynn T, Physical therapist decision-making in managing plantar heel pain: Cases from a pragmatic randomized clinical trial: Physiother Theory Pract, 2020; 36; 638-62
14. Gonnade N, Bajpayee A, Elhence A, Regenerative efficacy of therapeutic quality platelet-rich plasma injections versus phonophoresis with kinesiotaping for the treatment of chronic plantar fasciitis: A prospective randomized pilot study: Asian J Transfus Sci, 2018; 12; 105-11
15. Mcneill W, Pedersen C, Dynamic tape. Is it all about controlling load?: J Bodyw Mov Ther, 2016; 20; 179-88
16. Williams S, Whatman C, Hume PA, Sheerin K, Kinesio taping in treatment and prevention of sports injuries: A meta-analysis of the evidence for its effectiveness: Sports Med, 2012; 42; 153-64
17. Slevin ZM, Arnold GP, Wang W, Abboud RJ, Immediate effect of kinesiology tape on ankle stability: BMJ Open Sport Exerc Med, 2020; 6; e000604
18. Kodesh E, Benzoor MC, Dar G, Effect of dynamic tape on postural sway in individuals with chronic ankle instability: J Bodyw Mov Ther, 2021; 28; 62-67
19. Pawik Ł, Pawik M, Wysoczańska E, In patients with grade I and II ankle sprains, dynamic taping seems to be helpful during certain tasks, exercises and tests in selected phases of the rehabilitation process: A preliminary report: Int J Environ Res Public Health, 2022; 19; 5291
20. Halabchi F, Hassabi M, Acute ankle sprain in athletes: Clinical aspects and algorithmic approach: World J Orthop, 2020; 11; 534-58
21. Botsis AE, Schwarz NA, Harper ME: J Funct Morphol Kinesiol, 2019; 4; 19
22. Song JY, Park SH, Lee MMComparison of the effects of dynamic taping and kinesio taping on endurance and fatigue of plantar flexor: Journal of Korean Physical Therapy Science, 2022; 29; 73-86 [in Korean]
23. Lim O-B, Park S-YComparison of the effects of barefoot, kinesio tape, and dynamic tape on static and dynamic balance in subjects with asymptomatic flexible: Physical Therapy Korea, 2020; 27; 78-86 [in Korean]
24. Tezel N, Umay E, Bulut M, Cakci A, Short-term efficacy of Kinesiotaping versus extracorporeal shockwave therapy for plantar fasciitis: A randomized study: Saudi J Med Med Sci, 2020; 8; 181-87
25. Han YJThe effect of functional taping techniques when applied to the posterior tibialis on pain, foot pressure and dynamic balance in patience with plantar fasciitis (master’s thesis), 2021, Seoul, SahmYook University [in Korean]
26. Faul F, Erdfelder E, Lang A-G, Buchner A, G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences: Behav Res Methods, 2007; 39; 175-91
27. Ryan Kendrick K, Seung-Min Park, Soyeon: Dynamic taping, 2020, Seoul, PANMUNEDUCATION
28. Kase K, Wallis J, Kase T: Clinic therapeutic application of the kinesiotaing method, 2013, Kinesio
29. Delgado DA, Lambert BS, Boutris N, Validation of digital visual analog scale pain scoring with a traditional paper-based visual analog scale in adults: J Am Acad Orthop Surg Glob Res Rev, 2018; 2; e088
30. Boonstra AM, Schiphorst Preuper HR, Reliability and validity of the visual analogue scale for disability in patients with chronic musculoskeletal pain: Int J Rehabil Res, 2008; 31; 165-69
31. Sutton RM, Mcdonald EL, Shakked RJ, Determination of Minimum Clinically Important Difference (MCID) in Visual Analog Scale (VAS) pain and Foot and Ankle Ability Measure (FAAM) scores after hallux valgus surgery: Foot Ankle Int, 2019; 40; 687-93
32. Budiman-Mak E, Conrad KJ, Mazza J, Stuck RM, A review of the foot function index and the foot function index – revised: J Foot Ankle Res, 2013; 6; 5
33. Pourtier-Piotte C, Pereira B, Soubrier M, French validation of the Foot Function Index (FFI): Ann Phys Rehabil Med, 2015; 58; 276-82
34. Soohoo NF, Samimi DB, Vyas RM, Botzler T, Evaluation of the validity of the Foot Function Index in measuring outcomes in patients with foot and ankle disorders: Foot Ankle Int, 2006; 27; 38-42
35. Choo Y-K, Bae W-SPhysiotherapy approach to patients with chronic plantar fasciitis: Comparison of the effects of specific stretching exercise and high-load strengthening exercise: Journal of The Korean Society of Integrative Medicine, 2021; 9; 151-61 [in Korean]
36. Rathleff MS, Mølgaard CM, Fredberg U, High-load strength training improves outcome in patients with plantar fasciitis: A randomized controlled trial with 12-month follow-up: Scand J Med Sci Sports, 2015; 25; e292-e300
37. Powden CJ, Dodds TK, Gabriel EH, The reliability of the star excursion balance test and lower quarter y-balance test in healthy adults: a systematic review: Int J Sports Phys Ther, 2019; 14; 683-94
38. Plisky PJ, Gorman PP, Butler RJ, The reliability of an instrumented device for measuring components of the star excursion balance test: N Am J Sports Phys Ther, 2009; 4; 92-99
39. Powden CJ, Dodds TK, Gabriel EH, The reliability of the star excursion balance test and lower quarter y-balance test in healthy adults: A systematic review: Int J Sports Phys Ther, 2019; 14; 683
40. Park SThe effects of exercise type on fall-related risk factors in the elderly women: Sports Science Review, 2013; 7; 25-35 [in Korean]
41. Ji S-G, Nam G-W, Kim M-K, Cha H-KThe effect of visual feedback training using a mirror on the balance in hemiplegic patients: Journal of the Korean Society of Physical Medicine, 2011; 6; 153-63 [in Korean]
42. Yang S, 2022, Cheonan, The Graduate School of Namseoul University [in Korean]
43. Yang HKThe effects of creative dance program on balance, gait, and activities on daily living function of adults with dystonic cerebral palsy, (master’s thesis), 2019, Seoul, The Graduate School of Seoul National Univeristy [in Korean]
44. Tsai C-T, Chang W-D, Lee J-P, Effects of short-term treatment with kinesiotaping for plantar fasciitis: J Musculoskelet Pain, 2010; 18; 71-80
45. Kim JWThe effect of low-dye taping on pain, foot function index with and balance in patients with plantar fasciitis, in department of physical therapy, (master’s thesis).], 2021, Seoul, SahmYook University [in Korean]
46. Karishma K, Muhammad A, Ameer SH, Raza ZSW, Comparison of the efficacy of kinesiology taping versus therapeutic ultrasound in the management of plantar fasciitis: A randomized controlled trial: Balneo and PRM Research Journal, 2022; 13; 481-81
Figures
Tables
Table 1. General characteristic of subjects (N=69).Table 2. Changes of visual analog scale according to intervention methods (N=69).Table 3. Changes of foot function index according to intervention methods (N=69).Table 4. Changes of the Y-balance test according to intervention methods (N=69).Table 5. Changes of medial heel pressure according to intervention method (N=69).Table 1. General characteristic of subjects (N=69).Table 2. Changes of visual analog scale according to intervention methods (N=69).Table 3. Changes of foot function index according to intervention methods (N=69).Table 4. Changes of the Y-balance test according to intervention methods (N=69).Table 5. Changes of medial heel pressure according to intervention method (N=69). In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387