30 July 2024: Review Articles
Why MASLD Lags Behind MAFLD: A Critical Analysis of Diagnostic Criteria Evolution in Metabolic Dysfunction-Associated Liver Diseases
Mohamed AlboraieDOI: 10.12659/MSM.945198
Med Sci Monit 2024; 30:e945198






Abstract
ABSTRACT: Emerging in the 1800s under the label “fat in the liver” and later gaining prominence in the 1980 as non-alcoholic fatty liver disease (NAFLD), the disease predominantly attributed to metabolic dysfunction presents a formidable health issue marked by substantial morbidity and mortality. It was 2020 when a change of one letter “NAFLD” to metabolic dysfunction-associated fatty liver disease “MAFLD” linked with the change in the definition and diagnostic criteria began a new controversy around the globe. Metabolic dysfunction-associated fatty liver disease (MAFLD) criteria represent a substantial departure from previous diagnostic measures of NAFLD, and provide the first set of positive criteria for diagnosis of the disease in adults and children that emphasise the key attribute of metabolic dysfunction in the pathogenesis, and acknowledges that the disease is a continuum across the life span. In 2023, an adapted version of the diagnostic criteria of MAFLD was proposed to define a slightly modified term; metabolic dysfunction-associated steatotic liver disease (MASLD). The MASLD criteria did not provide any conceptual advantage, and emerging evidence suggests that it actually performs worse than the MAFLD criteria. This raises the intriguing question of why MASLD was unable to take advantage of being second? In this review, we will explore the possible reasons for this unique case and highlight the current evidence supporting the use of MAFLD instead of MASLD in defining metabolic dysfunction-associated fatty liver diseases.
Keywords: Diagnostic Errors, Fatty Liver, Metabolic Diseases, Terminology, Humans, Non-alcoholic fatty liver disease, Liver, Liver Diseases
Introduction
Emerging in the 1800s under the label “fat in the liver” and later gaining prominence in the 1980 as non-alcoholic fatty liver disease (NAFLD), the disease predominantly attributed to metabolic dysfunction presents a formidable health issue marked by substantial morbidity and mortality. Despite its extensive historical recognition and terminology refinement, the field continues to confront significant challenges in redefining the disease, diagnostic criteria, and enhancing therapeutic strategies [1].
In 2020, a new term “metabolic dysfunction-associated fatty liver disease” (MAFLD) was proposed, changing one letter from “NAFLD” to “MAFLD”, which was linked with the change in the definition and diagnostic criteria and began a new controversy around the globe. Looking at what additional importance the MAFLD criteria hold, it is clear that while the 2020 the MAFLD criteria signify a significant shift from the previous diagnostic approach of NAFLD, they also provide the first set of positive criteria for diagnosis of the disease in adults and children that emphasise the key role of metabolic dysfunction in the pathogenesis, and acknowledge that the disease occurs as a continuum across the life span [2–5]. Additionally, MAFLD has practical ramifications for treatment strategies and patient interactions [5]. Over the past few years “MAFLD” has become a popular term in research and practice and is widely endorsed [6], but it has also been resisted in some parts of the world, provoking division and controversy.
In 2023, an adapted version of the diagnostic criteria of MAFLD was proposed to define a slightly modified term – metabolic dysfunction-associated steatotic liver disease (MASLD) [7]. Scientific knowledge is the most solid and robust kind of knowledge that humans have because of the evolving character inherent in its own processes. Evolution of the performance of new versions of diagnostic criteria is typical in science, as subsequent criteria give the opportunity to capitalize on previous efforts. To our surprise, the MASLD criteria did not provide any conceptual advance; rather, the emerging evidence suggests that it performs worse than the MAFLD criteria. This raises the intriguing question of why MASLD did not benefit from being second.
Inability to achieve the target with a proposed definition or diagnostic criteria is a normal and critical part of the scientific process; however, admitting this inability remains largely stigmatized within the sciences. However, the analysis of the causes of this inability is crucial for further improvement. Therefore, this article endeavours to clarify the following problem: what are the factors leading to innovation inability with specific reflection on the MASLD case? We discuss 3 critical sources of the inability to innovate: a) goal missing, b) planning problems, and c) execution issues. In this review we present evidence to support the use of MAFLD rather than MASLD in defining metabolic dysfunction-associated fatty liver diseases, as the later lacks specificity and has lower performance in many diseases. We also offer our views on the best path forward.
MAFLD vs MASLD Evidence
OVER-DIAGNOSIS:
Over-diagnosis is a major issue in modern healthcare that can lead to harmful and costly outcomes. It can be caused by 2 factors: over-detection and over-definition of disease. Over-detection happens when medical professionals detect abnormalities that will not cause any harm to the patient or progress too slowly to cause symptoms or harm during the patient’s lifetime [12]. Over-definition is caused by lowering the threshold for a risk factor or expanding disease definitions to include patients with mild symptoms. These patients are usually at lower risk than those diagnosed under earlier definitions. Over-diagnosis can lead to over-treatment, which offers little to no benefit and can have significant physical, psychological, social, and financial consequences (Figure 2). For instance, there is an increase in early forms of cancer or smaller abdominal aortic aneurysm diagnosis, without a reduction in advanced disease or death, which can be a sign of over-diagnosis through over-detection [13,14]. In regions with limited resources and high prevalence of fatty liver disease, it may be difficult to apply the MASLD criteria.
LOWER PERFORMANCE:
The effectiveness of MASLD was compared to the existing criteria for MAFLD. Recent data strongly indicate that MAFLD is highly effective in identifying subjects at high risk for metabolic dysfunction, as well as hepatic and extra-hepatic outcomes [15–21]. This change in name and criteria to MASLD causes confusion without increasing utility.
LOW PERFORMANCE IN PEDIATRIC POPULATIONS:
The definition of MASLD has been called into question, particularly in the context of children and adolescents [17]. However, the MAFLD definition provides a comprehensive framework for understanding pediatric fatty liver disease. The definition includes 3 types: Type 1, which is fatty liver associated with a systemic disorder; Type 2, which is MAFLD; and Type 3, which is fatty liver without an underlying defect (but one that may become apparent over time).
This classification is of utmost importance to prevent misclassification and to avoid unnecessary testing, which can cause physical, psychological, and economic harm to patients. In contrast, the MASLD concept does not account for these aspects. Moreover, the MAFLD definition includes age-specific criteria for children and adolescents, whereas the MASLD criteria do not. Therefore, it is essential to consider changes in body composition that contribute to the differential risk of metabolic dysfunction.
Furthermore, some of the obesity and metabolic factor cut-offs used in MASLD are factually incorrect, such as body mass index (BMI). These inaccuracies make it unsurprising that a recent study demonstrated the superiority of the MAFLD definition over the MASLD definition in pediatrics [17].
INABILITY TO CONSIDER A GLOBAL PERSPECTIVE:
For any new proposal to be adopted naturally without forcing it requires taking into consideration a global perspective. The MASLD definition falls short in this aspect. Staring from proposing changing MAFLD to MASLD, discarding the fact that for all non-Latin languages that are spoken by more than 5 billion people globally, there is no distinction between the 2 words. Another striking example is the proposed MetALD term to describe the coexistence of MASLD with excessive alcohol consumption above an arbitrary threshold. Therefore, apart from being flawed concept, it again reflects the self-centric approach of the MASLD proposal that ignores the global status. What about the coexistence of MASLD with other diseases such as hepatitis C and B, or autoimmune hepatitis, which it is more prevalent in other parts of the world [22]? Unfortunately, the MASLD definition did not take this into consideration.
POTENTIAL CAUSES OF MASLD’S INABILITY TO BETTER DEFINE FATTY LIVER ATTRIBUTED TO METABOLIC DYSFUNCTION:
These findings raise the intriguing question of why the MASLD definition did not benefit from being proposed after MAFLD and could not provide any conceptual advance. Below, we analyze some of the potential key reasons for this.
Goal Missing
The main objective of the consensus process proposed in the MASLD definition was to resist the original proposal to adopt MAFLD, as pointed out by multiple recent articles [23,24]. This likely deviated the effort from providing a real conceptual advance.
Planning Problems
The MASLD concept is the birth of a consensus process that is formulated as a questionnaire of personal views rather than evidence. However, expert opinion is not a surrogate for evidence-based data. Science is not about consensus; it is about the truth [25]. An example of applying the Delphi-method to a transplant-related question incorrectly recommended high-dose chemotherapy and an auto-transplant for some women with high-risk breast cancer [26]. Subsequent randomized trials showed this approach was ineffective [27]. Consistently, in a recent analysis of over 100 consensus statements, the rigor of statement development was found to be one-third lower than that of evidence-based recommendations [28].
Execution Issues
The consensus of expert opinion is heavily influenced by the selection of participating experts and their perspectives, as well as the way the questionnaire is formulated. Unfortunately, the MASLD process has been criticized for selecting experts who favor one viewpoint over another, leading to a poor representation of most real-world physicians and active academics. Additionally, the questionnaire used in this process was not validated or transparent. However, without quality evidence, expert opinions may have little impact.
Conclusions
The above evidence suggests that, in retrospect, the process needed to “restate its objectives, seek out its rationale.” Going forward, there is an urgent need for a true consensus process that allows for the development of evidence-based guideline statements. This process should involve a systematic review of the evidence, with equal contribution from all regions of the world, patients, research, and clinical panellists. This is the only way to ensure that the outcomes will be widely adopted. It is important to note that identifying an objective-level consensus is only possible when gathering quantifiable data. In some qualitative Delphi studies, the judgement on consensus may be rather subjective on the part of the researcher, potentially leading to bias. We should learn from the problems associated with the concept of MASLD and use evidence to guide us. There is an urgent need for an appropriate consensus process.
Figures
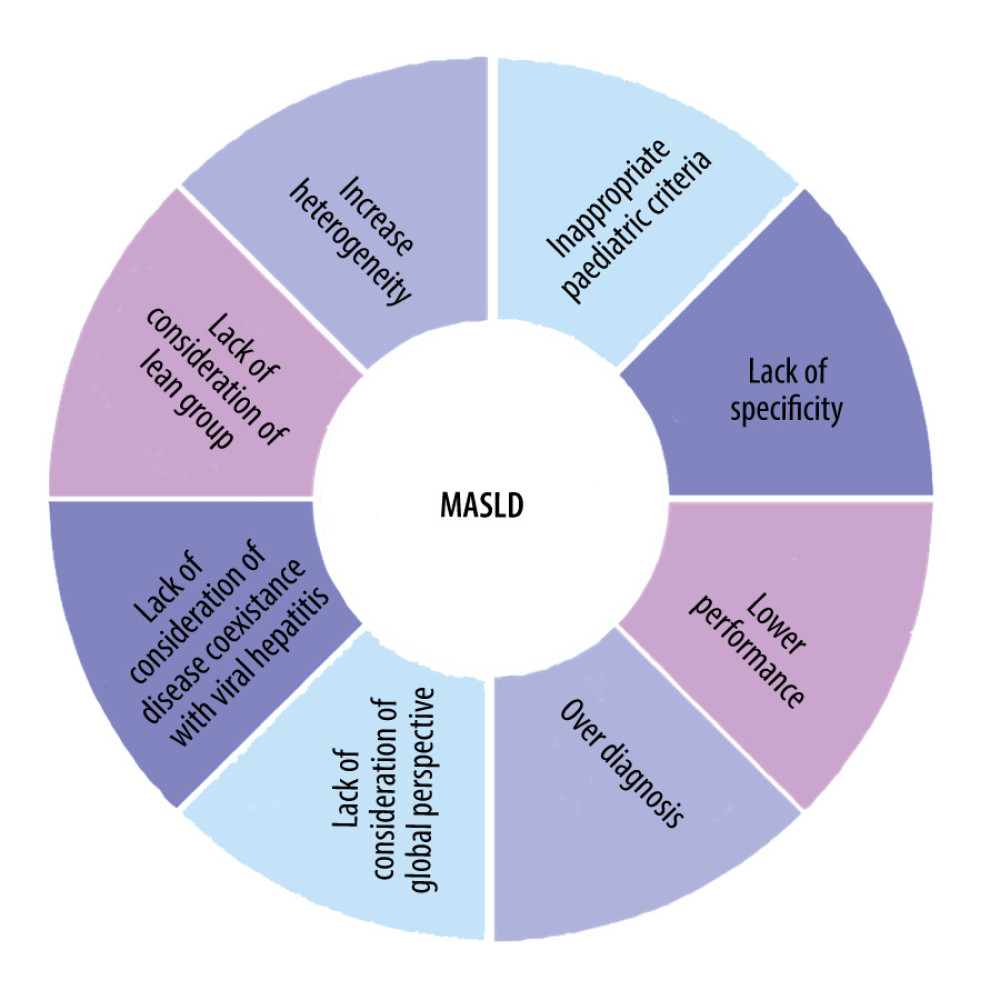 Figure 1. Limitations of the Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) definition.
Figure 1. Limitations of the Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) definition.  Figure 2. The negative consequences (unnecessary care, psychological stress, and financial burden) of over-diagnosis when applying the Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) definition on population and professional levels that ultimately cause more harm than benefit.
Figure 2. The negative consequences (unnecessary care, psychological stress, and financial burden) of over-diagnosis when applying the Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) definition on population and professional levels that ultimately cause more harm than benefit. References
1. Eslam M, El-Serag HB, Francque S, Metabolic (dysfunction)-associated fatty liver disease in individuals of normal weight: Nat Rev Gastroenterol Hepatol, 2022; 19(10); 638-51
2. Eslam M, Alkhouri N, Vajro P, Defining paediatric metabolic (dysfunction)-associated fatty liver disease: An international expert consensus statement: Lancet Gastroenterol Hepatol, 2021; 6(10); 864-73
3. Mohammed E, Jacob G, Two years on, a perspective on MAFLD: eGastroenterology, 2023; 1(2); e100019
4. Eslam M, Newsome PN, Sarin SK, A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement: J Hepatol, 2020; 73(1); 202-9
5. Alharthi J, Gastaldelli A, Cua IH, Ghazinian H, Eslam M, Metabolic dysfunction-associated fatty liver disease: A year in review: Curr Opin Gastroenterol, 2022; 38(3); 251-60
6. Mendez-Sanchez N, Bugianesi E, Gish RG, Global multi-stakeholder endorsement of the MAFLD definition: Lancet Gastroenterol Hepatol, 2022; 7(5); 388-90
7. Rinella ME, Lazarus JV, Ratziu V, A multisociety Delphi consensus statement on new fatty liver disease nomenclature: Hepatology, 2023; 78(6); 1966-86
8. Semmler G, Balcar L, Wernly S, Insulin resistance and central obesity determine hepatic steatosis and explain cardiovascular risk in steatotic liver disease: Front Endocrinol (Lausanne), 2023; 14; 1244405
9. Ciardullo S, Carbone M, Invernizzi P, Perseghin G, Exploring the landscape of steatotic liver disease in the general US population: Liver Int, 2023; 43(11); 2425-33
10. Choudhary NS, Dhampalwar S, Saraf N, Soin AS, Metabolic dysfunction-associated steatotic liver disease: Where does non-alcoholic fatty liver disease in liver transplant recipients fit in this new definition?: J Hepatol Feb, 2024; 80(2); e77-e79
11. Anirvan P, Khatua CR, Panigrahi MK, Singh SP, Definition of metabolic dysfunction: Shifting goalposts: J Clin Exp Hepatol, 2024; 14(2); 101301
12. Brodersen J, Schwartz LM, Heneghan C, Overdiagnosis: What it is and what it isn’t: BMJ Evid Based Med, 2018; 23(1); 1-3
13. Esserman L, Shieh Y, Thompson I, Rethinking screening for breast cancer and prostate cancer: JAMA, 2009; 302(15); 1685-92
14. Johansson M, Hansson A, Brodersen J, Estimating overdiagnosis in screening for abdominal aortic aneurysm: could a change in smoking habits and lowered aortic diameter tip the balance of screening towards harm?: BMJ, 2015; 350; h825
15. Ramirez-Mejia MM, Jimenez-Gutierrez C, Eslam M, Breaking new ground: MASLD vs. MAFLD-which holds the key for risk stratification?: Hepatol Int, 2024; 18(1); 168-78
16. Ramírez-Mejía MM, Eslam M, Méndez-Sánchez N, The MAFLD and MASLD conundrum: Is it reinvention of the wheel?: J Hepatol, 2024; 81(1); e22-e23
17. Pan Z, Eslam Mpanel of collaborators, The MASLD criteria overlook a number of adolescent patients with severe steatosis: J Hepatol, 2024 [Online ahead of print]
18. Zhao Q, Deng Y, Comparison of mortality outcomes in individuals with MASLD and/or MAFLD: J Hepatol, 2024; 80(2); e62-e64
19. Pan Z, Al-Busafi SA, Abdulla M, MAFLD identifies patients with significant hepatic fibrosis better than MASLD: Hepatol Int, 2024; 18(3); 964-72
20. Pan Z, Derbala M, AlNaamani K, MAFLD criteria are better than MASLD criteria at predicting the risk of chronic kidney disease: Ann Hepatol, 2024; 29(5); 101512
21. Pan Z, Shiha G, Esmat G, MAFLD predicts cardiovascular disease risk better than MASLD: Liver Int, 2024; 44(7); 1567-74
22. Fouad Y, Sanai F, Alboraie M, Zheng MH, What the new definition of MASLD left behind: Dual etiology with viral hepatitis: Clin Gastroenterol Hepatol, 2023 [Online ahead of print]
23. Fouad Y, Alboraie M, El-Shabrawi M, Zheng MH, Letter to the Editor: How F to S turned the premature to be mature?: Hepatology, 2024; 79(6); E157-E58
24. Emanuele E, Minoretti P, Letter to the Editor: NAFLD, MAFLD or MASLD? Cut the Gordian knot with “Ludwig disease”: Hepatology, 2024; 79(1); E4
25. Fouad Y, Elwakil R, Elsahhar M, The NAFLD-MAFLD debate: Eminence vs evidence: Liver Int, 2021; 41(2); 255-60
26. Gale RP, Park RE, Dubois R, Delphi-panel analysis of appropriateness of high-dose chemotherapy and blood cell or bone marrow autotransplants in women with breast cancer: Clin Transplant, 2000; 14(1); 32-41
27. Tallman MS, Gray R, Robert NJ, Conventional adjuvant chemotherapy with or without high-dose chemotherapy and autologous stem-cell transplantation in high-risk breast cancer: N Engl J Med, 2003; 349(1); 17-26
28. Jacobs C, Graham ID, Makarski J, Clinical practice guidelines and consensus statements in oncology – an assessment of their methodological quality: PLoS One, 2014; 9(10); e110469
Figures
Figure 1. Limitations of the Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) definition.Figure 2. The negative consequences (unnecessary care, psychological stress, and financial burden) of over-diagnosis when applying the Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) definition on population and professional levels that ultimately cause more harm than benefit. In Press
Clinical Research
Comparative Effectiveness of a Nurse-Led Care Model vs Usual Care in Rheumatoid Arthritis: A Longitudinal C...Med Sci Monit In Press; DOI: 10.12659/MSM.953211
Clinical Research
Impact of Treatment Modality on Pain, Sexual Function, and Psychological Well-Being in Patients With Bartho...Med Sci Monit In Press; DOI: 10.12659/MSM.952422
Clinical Research
Association Between Radiographic Knee Osteoarthritis, Pre-Fracture Mobility, and Hip Fracture Patterns in O...Med Sci Monit In Press; DOI: 10.12659/MSM.952678
Clinical Research
Association Between Total Cholesterol–to–High-Density Lipoprotein Ratio and Gestational Hypertension: A Cas...Med Sci Monit In Press; DOI: 10.12659/MSM.952395
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,084
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,757,530
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,116
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,768
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387