03 December 2024: Clinical Research
Machine Learning Models for Predicting 24-Hour Intraocular Pressure Changes: A Comparative Study
Chen Ranran ACDEG 1,2, Lei Jinming ACD 3, Liao Yujie BC 1,2, Jin Yiping BC 1,2, Wang Xue CD 4, Li Hong BD 1, Bi Yanlong ACF 5*, Zhu Haohao ABFG 1,2
DOI: 10.12659/MSM.945483
Med Sci Monit 2024; 30:e945483






Abstract
BACKGROUND: Predicting 24-hour intraocular pressure (IOP) fluctuations is crucial for enhancing glaucoma management. Traditional methods of measuring 24-hour IOP fluctuations are complex and present certain limitations. The present study leverages machine learning techniques to forecast 24-hour IOP fluctuations based on daytime IOP measurements.
MATERIAL AND METHODS: A binary method was used to classify 24-hour IOP fluctuations as either >8 mmHg or £8 mmHg. Data were collected from 24-hour IOP monitoring, including 22 different features. Feature selection involved the chi-square test and point-biserial correlation, leading to the establishment of 4 subsets with significance levels of P<1, P<0.1, P<0.05, and P<0.025. Five binary classification machine learning algorithms were used to construct the model. Model performance was assessed by comparing accuracy, specificity, 10-fold cross-validation, precision, sensitivity, F1 score, area under the curve (AUC), and Area Under the Precision-Recall Curve (AUCPR). The model with the highest performance was selected, and feature importance was assessed using Shapley additive explanations.
RESULTS: In the subset of features where P<0.05, all models performed better than those in the other subsets, with XGBoost standing out the most. The XGBoost algorithm achieved an accuracy of 0.886, a specificity of 0.972, a 10-fold cross-validation of 0.872, a precision of 0.857, a sensitivity of 0.585, and an F1 score of 0.696. Additionally, it obtained an AUC of 0.890 and an AUCPR of 0.794.
CONCLUSIONS: Our study illustrates the predictive capabilities of machine learning algorithms in forecasting 24-hour IOP fluctuations. The exceptional performance of the XGBoost algorithm in predicting IOP fluctuations underscores its significance for future research and clinical applications.
Keywords: Glaucoma, Pressure, Algorithms, Tonometry, Ocular, Humans, Intraocular Pressure, machine learning, Male, Female, Middle Aged, adult, Area Under Curve, Circadian Rhythm
Introduction
Glaucoma, a chronic neuropathic condition, is clinically characterized by distinct indicators, including an asymmetric (>0.2) cup-to-disc ratio (C/D ratio), rim thinning, notching, excavation, and retinal nerve fiber layer defects, alongside progressive visual field alterations and consistent abnormal test findings [1]. In the management of glaucoma, intraocular pressure (IOP) stands as the sole modifiable risk factor [2]. It is now well-established that IOP is not constant but varies significantly throughout the day [3,4].
Although IOP fluctuation is believed to potentially impact glaucoma progression, the exact role of IOP fluctuation remains debated [4–10]. For instance, Asrani et al demonstrated that significant diurnal IOP fluctuations are an independent risk factor for glaucoma progression, even within the normal range of office-based IOP readings [4]. Similarly, Collaer and colleagues found a significant relationship between visual field deterioration and the range and peak of IOP in normal-tension glaucoma patients based on sequential office measurements within a single day [11]. However, some studies have failed to establish that either diurnal or long-term IOP fluctuations, as measured in clinical practice, are independent risk factors for glaucoma progression [12]. These discrepancies may arise from variations in study design and methods of data analysis [12].
In China, the diagnostic criteria for primary open-angle glaucoma (POAG) include: (1) IOP >25 mmHg on 3 separate occasions within 1 day; (2) 24-hour IOP fluctuation >8 mmHg; (3) typical glaucoma changes in the visual field; and (4) typical glaucoma changes in the optic disc [13]. Additionally, a 24-hour IOP fluctuation exceeding 8 mmHg is currently considered abnormal and may necessitate medication adjustment [14]. Given the ongoing debate about the impact of IOP fluctuations on glaucoma, predicting 24-hour IOP fluctuations remains of significant clinical importance for aiding diagnosis and assessing disease progression.
Traditional 24-hour IOP monitoring necessitates hospitalization, involving intermittent measurements at specified intervals. However, this approach disrupts patients’ sleep due to nighttime pressure assessments, placing additional burdens on healthcare providers and patients alike. Contact lens sensors offer a promising solution for continuous IOP monitoring, characterized by superior patient tolerance and non-invasiveness [15,16]. However, potential cost implications remain.
Artificial Intelligence (AI), a subset of computer science, strives to create systems capable of tasks typically requiring human intelligence, such as processing information, making predictions, and adapting to changing scenarios. Machine learning, a prominent AI subset, empowers computers to learn and enhance their performance on specific tasks through data analysis, all without explicit programming. Machine learning algorithms, including support vector machines (SVM), random forest, and extreme gradient boosting (XGBoost), excel at recognizing patterns, classifying data, and making predictions.
Therefore, we propose developing a 24-hour IOP fluctuation prediction model. Based on the Chinese guidelines that classify 24-hour IOP fluctuation exceeding 8 mmHg as requiring intervention [14], we plan to use a binary classification approach to predict 24-hour IOP fluctuation, categorizing it as ≤8 mmHg or >8 mmHg. This model aims to provide support for the diagnosis and treatment evaluation of glaucoma.
Material and Methods
DATA SOURCE:
This study adheres to the ethical principles set forth in the Helsinki Declaration, and has received approval from the Ethics Committee of Shanghai Fifth People’s Hospital, affiliated with Fudan University (Ethics Approval No. 083). Due to the retrospective nature of the study, the requirement for informed consent was waived.
Inclusion criteria were as follows: age between 18 and 85 years, both male and female, and diagnosis of glaucoma or suspected glaucoma. Regarding the definition of glaucoma, patients were included if they met the diagnostic criteria for primary angle-closure glaucoma (PACG) or if they were diagnosed with or suspected of having POAG, as specified in the American Academy of Ophthalmology (AAO) Preferred Practice Pattern Guidelines, which include: Primary Angle Closure Preferred Practice Pattern Guidelines [17], Primary Open-Angle Glaucoma Suspect Preferred Practice Pattern Guidelines [18], and Primary Open-Angle Glaucoma Preferred Practice Pattern Guidelines [19]. We therefore diagnosed patients into 3 categories according to the AAO diagnostic criteria: suspected glaucoma, PACG, or POAG. Exclusion criteria were as follows: completion of 24-hour IOP monitoring in only a single eye; a history of ophthalmic surgery; other types of glaucoma; concurrent corneal diseases; or non-ophthalmologic conditions, including completed neurosurgical procedures.
All patients in this study were admitted for ophthalmologic reasons, falling into the following categories: (1) patients with suspected glaucoma who required 24-hour IOP monitoring for further diagnosis; (2) glaucoma patients with well-controlled daytime IOP, but who showed progression in visual field or retinal nerve fiber layer during follow-up; (3) patients already diagnosed with glaucoma and using anti-glaucoma eye drops, who needed 24-hour IOP monitoring to assess the effectiveness of their IOP control.
This retrospective investigation involved the enrollment of 478 patients (956 eyes) who underwent 24-hour IOP monitoring at our institution between January 1, 2014, and July 31, 2023. Various parameters, including blood pressure and 24-hour IOP values, were collected for analysis.
In our study, 24-hour IOP monitoring was conducted under inpatient conditions. Measurements began at 10: 00 AM on the first day and were taken every 2 hours until 8: 00 AM the following day. The specific measurement times were as follows: 10: 00 AM, 12: 00 PM (noon), 2: 00 PM, 4: 00 PM, 6: 00 PM, 8: 00 PM, 10: 00 PM, 12: 00 AM (midnight), 2: 00 AM, 4: 00 AM, 6: 00 AM, and 8: 00 AM. The monitoring started at 10: 00 AM to allow for the collection of a full 24-hour cycle of IOP data within a standard clinical schedule, ensuring that all daytime and nighttime periods were covered effectively. This start time aligns with typical clinical practice and maximizes the efficiency of the monitoring process within the constraints of a hospital setting.
In clinical practice and research, several IOP-derived parameters are commonly used to summarize IOP variation, including mean IOP (the average of IOP over multiple visits), peak IOP (the highest IOP reading during follow-up), and IOP fluctuation (the standard deviation [SD] or range of IOP over time). In our study, 24-hour IOP fluctuation was defined as the difference between the minimum and maximum IOP values within 24 hours. We chose this method because it captures the maximum range of IOP variation within that timeframe. This approach is utilized in clinical research to assess IOP fluctuations and may provide insights into the potential impact of these fluctuations on glaucoma progression [4,13,14].
Non-contact tonometry (CT-80A, JAPAN) was employed for IOP measurement, with patients in a seated position. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were recorded using a brachial mercury sphygmomanometer (GB3053-1993) on the upper left arm after the subjects had been seated for a minimum of 3 minutes. Parameters such as height, weight, and blood pressure were expertly measured and recorded by nursing staff at 10: 00 AM after patient admission.
For the duration of the study, blood pressure measurements were consistently obtained at 10: 00 AM during the patients’ hospitalization periods. Specifically, the mean ocular perfusion pressure (MOPP) was computed using the recorded blood pressure value at 10: 00 AM and simultaneous IOP measurement. Corneal thickness was accurately measured using equipment from TOPCON CORPORATION (Tokyo, Japan). IOP and central corneal thickness (CCT) measurements were conducted by experienced physicians, with IOP measured thrice at each timepoint, and the average value of these 3 measurements used for analysis.
In this retrospective study, we analyzed the medication regimens used by the glaucoma patients. In the monotherapy group, patients were given 1 drop of 0.005% latanoprost or 0.0015% tafluprost once daily in the evening. In the dual therapy group, patients were given 1 drop of 0.005% latanoprost or 0.0015% tafluprost once daily in the evening, along with 2% carteolol or 1% brinzolamide eye drops, which were given twice daily. The triple therapy group included: (1) 1 drop of 0.005% latanoprost or 0.0015% tafluprost daily in the evening, combined with 2% carteolol and 1% brinzolamide, both given twice daily; (2) 1 drop of 0.005% latanoprost or 0.0015% tafluprost daily in the evening, combined with 1% brinzolamide and 0.5% dorzolamide-timolol (fixed combination). The quadruple therapy group included: (1) 1 drop of 0.005% latanoprost or 0.0015% tafluprost daily in the evening, combined with 2% carteolol, 1% brinzolamide (both given twice daily), and 0.2% brimonidine tartrate, which was given twice daily; (2) 1 drop of 0.005% latanoprost or 0.0015% tafluprost daily in the evening, combined with 1% brinzolamide and 0.5% dorzolamide-timolol fixed combination, and 0.2% brimonidine tartrate, which was given twice daily. This study primarily focused on evaluating IOP changes across different drug combinations, without further subclassification of patients
The 0.005% latanoprost (Xalatan®, Pfizer Manufacturing Belgium NV) and 0.0015% tafluprost (Tapros®, Santen Pharmaceutical Co., Ltd. Shiga Plant) are classified as prostaglandin analogs; 2% carteolol (Mikelan®, Otsuka Pharmaceuticals Co., Ltd. China) is a β-adrenoceptor antagonist; 0.2% brimonidine tartrate (ALLERGAN®, Allergan Pharmaceuticals Ireland) is an α-adrenergic agonist; and 1% brinzolamide (AZOPT®, Alcon Labs, Cairo, Egypt) is a carbonic anhydrase inhibitor.
FEATURE DESCRIPTION:
Through a literature review, we identified common and distinct risk factors for PACG, POAG, and suspected glaucoma. Common risk factors across these conditions include older age [20–22], IOP [23,24], lower ocular perfusion pressure (OPP) [25,26], myopia [27–30], thinner central cornea [21,24,31], and a larger C/D ratio [24,31]. Specifically, PACG is more prevalent in female patients [20,32]. Additionally, literature suggests that body mass index (BMI) [33,34], metabolic status and obesity (MSO) [35,36], and the slope of the diurnal curve [37] may also be risk factors for glaucoma.
We planned to select the following features: age, sex, MSO, CCT, C/D ratio, blood pressure and OPP at 10: 00 AM, the number and duration of anti-glaucoma eye drops used, myopic refractive error, IOP slope, and IOP values from 10: 00 AM to 4: 00 PM. Data from different categories were extracted from the original records, resulting in a dataset comprising 22 features. Our objective was to analyze the correlation between these selected features and 24-hour IOP fluctuations, and to identify relevant features to construct and validate a predictive model for 24-hour IOP fluctuations. Since features such as MSO, blood pressure, OPP, and IOP slope involve formula calculations or require further explanation, we provide supplementary details on these features in the following sections.
BMI:
BMI was calculated as weight in kilograms divided by height in meters squared (BMI=weight [kg]/height2 [m2]). Obesity has been reported to be an independent risk factor for elevated IOP and has been shown to have a positive correlation with elevated IOP in many studies [33,34].
METABOLIC STATUS AND OBESITY:
Jung et al identified a nuanced relationship between obesity, metabolic health, and IOP [32]. They categorized subjects into 4 groups based on MSO criteria [35,36] to explore the link between these factors and IOP. These groups were: metabolically healthy normal weight (MHNW), metabolically healthy obesity (MHO), metabolically unhealthy normal weight (MUNW), and metabolically unhealthy obesity (MUO).
THE SLOPE OF THE DIURNAL CURVE:
Camilo et al found that IOP at 8: 00 AM and pressure concavity are the most effective predictors of IOP >21 mmHg at 6: 00 AM [37]. The slope of the diurnal curve at 10: 00 AM (S10am) was defined as the difference between IOP at 12: 00 PM (IOP12pm) and IOP at 10: 00 AM (IOP10am) divided by 2, as there was a 2-hour interval between the measurements. This definition is represented by the following equation: S10am=(IOP12pm-IOP10am)/2. A negative S10am indicated that the IOP decreased from 10: 00 AM to 12: 00 PM, while a positive S10am indicated the opposite. Greater fluctuations in IOP may be related to the slope of daytime IOP.
Based on this principle, we calculated S10am, the slope of the diurnal curve at 12: 00 PM (S12pm), and the slope of the diurnal curve at 2: 00 PM (S2pm). By applying machine learning to these parameters, we aimed to help in the prediction of fluctuations in 24-hour IOP.
BLOOD PRESSURE AND OPP:
OPP, representing the pressure available for ocular blood supply, plays a crucial role in ocular health [38]. OPP can be subcategorized into MOPP, systolic ocular perfusion pressure (SOPP), and diastolic ocular perfusion pressure (DOPP). Mean arterial pressure (MAP) was calculated as DBP+1/3 (SBP-DBP). MOPP was defined as 2⁄3(MAP-IOP), SOPP as SBP-IOP, and DOPP as DBP-IOP. The relationship between blood pressure, OPP, and open-angle glaucoma (OAG) is multifaceted. Low DBP, reduced MOPP, and decreased DOPP are independent risk factors for OAG in ethnic Malays [39]. Bowe et al found that nocturnal blood pressure dips exceeding 10% are linked to visual field deterioration in OAG patients [40]. A longitudinal study of 85 normal-tension glaucoma patients (32% hypertensive) found nighttime blood pressure dips predict visual field deterioration [41]. Low diastolic, systolic, and mean perfusion pressures, low DBP, and high systolic and mean arterial blood pressure are associated with higher OAG prevalence in Latinos [42].
STATISTICAL ANALYSIS:
In our study, a binary classification method was employed to delineate 24-hour IOP fluctuations, with fluctuations exceeding 8 mmHg categorized as 1, and those at or below 8 mmHg categorized as 0. Parameters such as metabolic health status, sex, and the number of anti-glaucoma drugs used were presented discretely and expressed in numerical and proportional formats. The chi-square test was utilized to explore the associations among these variables. Furthermore, continuous variables such as IOP values at different time points, CCT, C/D ratio, age, and blood pressure were summarized using mean values and standard deviations.
Data preprocessing and visualization were conducted using Python 3.11. Statistical analyses were also performed using Python 3.11. The following libraries and their versions were used:
1) CORRELATION ANALYSIS:
Chi-squared test of independence and point-biserial correlation coefficient were conducted using the scipy library, version 1.11.4.
2) MACHINE LEARNING ALGORITHMS:
Logistic regression (LR), SVM, K-nearest neighbors (KNN), and Naive Bayes algorithms were implemented using the scikit-learn library, version 1.2.2.
XGBoost was implemented using the XGBoost library, version 2.0.3.
3) FIGURE GENERATION:
Receiver operating characteristic (ROC) curves, precision-recall curves, SHapley Additive exPlanations (SHAP) plots, and violin plots were generated using Python (Software used for figure creation: Spyder IDE, Version 5.4.3, Anaconda, Inc.).
Bar plots were created using WPS Office (Software used for figure creation: WPS Office, Version 6.9.0, Kingsoft Office Software Corporation).
FEATURE SELECTION:
The objective of our study was to predict whether 24-hour IOP fluctuations will exceed 8 mmHg; therefore, a binary classification algorithm was selected. IOP fluctuations greater than 8 mmHg were labeled as 1, while those equal to or less than 8 mmHg were labeled as 0. To prevent overfitting and enhance model performance, feature selection was conducted to identify the most suitable subset from 22 potential features. Correlation analysis between various features and IOP fluctuations exceeding 8 mmHg over a 24-hour period was performed. Based on the results of the correlation analysis, different α values (α=1, 0.1, 0.05, and 0.025) were chosen, and the training set was divided into 4 subsets, each corresponding to a specific α value. Five different algorithms were employed to train models on each subset, followed by model validation. Ultimately, the optimal α value was determined based on the performance of the models during validation, as illustrated in Figure 1.
DATA PREPROCESSING: FILLING IN THE MISSING ITEMS:
Missing values in CCT were handled using mean imputation. Mean imputation is a straightforward and practical method for dealing with missing data, where missing values are replaced with the average value of the feature. This approach ensures data completeness without introducing additional bias. It is applicable to various types of features and datasets, providing better support for machine learning model training and prediction. It contributes to improving data integrity, model performance and stability, and data availability.
DATA NORMALIZATION:
Standardization was applied to ensure uniformity in feature scales, facilitating algorithm optimization for enhanced convergence and model performance. Several parameters, including metabolic health status (categorized as metabolically healthy or obese) and sex, were encoded into numerical values. This encoding simplifies data processing for algorithms, eliminating the need for additional conversion or preprocessing steps. For instance, sex was encoded as 1 for male and 0 for female. Within the metabolic health status category, we assigned the following labels: MHNW as 1, MHO as 2, MUNW as 3, and MUO as 4.
MODEL CONSTRUCTION:
To ensure the objectivity and reliability of the research results and to avoid potential biases or correlations affecting the experimental outcomes, we employed a random split method to divide individuals in the dataset into a training group (80% of the data) and a testing group (20% of the data). The dataset was partitioned into 2 subsets: 80% for training and 20% for validation to assess accuracy. Our study employed 5 machine learning algorithms: SVM, LR, XGBoost, KNN, and Naive Bayes. Among these algorithms, XGBoost demonstrated superior performance, thus warranting a brief introduction to this method.
The algorithm is summarized by the following pseudocode:
Python was the programming language employed in this study, with the XGBoost library being used for the implementation of the random forest model.
MODEL EVALUATION:
In our research, the model validation process encompasses both feature-selection validation and final model validation. The prediction model for 24-hour IOP fluctuations in our study employs 5 different methods. The complete flow of our prediction model, utilizing these 5 methods, is illustrated in Figure 2.
VALIDATION OF FEATURE SELECTION:
To validate our chosen feature-selection approach, we adopted a stepwise validation methodology to determine the optimal
Initially, a model is constructed using all available features (
Subsequently, features exhibiting stronger correlations with the target variable are selected, starting from relatively higher
The
The optimal
1) ACCURACY:
This metric represents the ratio of correctly predicted samples to the total sample size. While straightforward, it may be misleading when dealing with imbalanced classes.
2) SPECIFICITY:
This measures the proportion of actual negative samples correctly predicted as negatives. High specificity indicates the model’s effectiveness in avoiding false-positive classifications.
3) 10-FOLD CROSS-VALIDATION:
Cross-validation divides the dataset into 10 subsets for training and evaluation, helping estimate the model’s generalization performance and mitigating overfitting.
4) PRECISION:
Precision focuses on the accuracy of positive predictions. A higher precision implies that positive predictions are less likely to be false positives.
5) SENSITIVITY:
Sensitivity, also known as the true positive rate (TPR), is defined as TPR=TP/(TP+FN), where TP represents the number of true positives and FN represents the number of false negatives. This metric evaluates the model’s ability to correctly identify true positive cases.
6) F1-SCORE:
The F1-score is a combined metric calculated as F1-score=2×(Precision×Recall)/(Precision+Recall). It balances precision and recall, providing a comprehensive assessment of model performance.
7) ROC CURVE:
The ROC curve is a common metric for evaluating prediction accuracy. The AUC quantifies overall model performance, with higher values indicating better discrimination between classes.
8) PRECISION-RECALL CURVE:
The Precision-Recall curve is another common metric for evaluating classifier performance. In this curve, precision represents the proportion of samples classified as positive that are truly positive, while recall represents the proportion of truly positive samples that are correctly classified as positive. Typically, Precision-Recall curves plot precision and recall at different thresholds on the same chart, and adjusting the threshold yields different Precision-Recall points. The AUC of the Precision-Recall curve quantifies the overall performance of the curve, with higher values indicating a better balance between the predictive accuracy and recall of the positive class.
Collectively, these metrics offer insights into different facets of a classification model’s performance. In practical applications, the choice of metrics can be tailored to specific requirements, ensuring a more effective evaluation of the model’s efficacy.
SHAP:
SHAP is a method for interpreting machine learning model outputs by quantifying the contribution of each feature to the prediction. In our study, we employed SHAP to analyze the feature importance for a 24-hour IOP fluctuation prediction model.
Results
Table 1 provides a summary of the demographic characteristics of the Training+Testing Set and Testing Set. We compiled electronic medical records from 956 eyes, corresponding to 478 patients. To ensure effective model development in our machine learning process, we randomly divided the data into training and testing sets based on individuals, with 80% allocated for training and 20% for testing. Additionally, as part of our data preprocessing, we conducted imputation for 92 missing corneal thickness data points. In this report, daytime IOP refers to the measurements taken between 10: 00 AM and 4: 00 PM.
Figure 3 displays the distribution of IOP at different time points over a 24-hour period. Overall, the IOP values exhibit significant variation throughout the day, reaching peaks particularly at 2: 00 AM and 4: 00 AM, while being relatively lower at 10: 00 PM and midnight. From 10: 00 AM to 8: 00 PM, the IOP distribution is relatively stable, showing minimal fluctuations. The violin plot clearly indicates that IOP is higher during the night (especially in the early morning hours) and lower in the evening and around midnight.
A heatmap illustrating the correlations between various features and 24-hour IOP fluctuations is presented in Figure 4. The color intensity denotes the strength of these correlations, with deeper blue hues representing stronger positive correlations and deeper yellow hues representing stronger negative correlations. Statistically significant correlations are indicated as follows: * for (0.05<
The ROC curves and AUC results for predicting 24-hour IOP fluctuations using 5 different machine learning algorithms across 4 feature-selection criteria (
The PR curves and AUCPR results for predicting 24-hour IOP fluctuations using 5 machine learning algorithms across 4 feature-selection criteria (
The accuracy of 5 machine learning algorithms across 4 feature-selection criteria (
Figures 5–7 demonstrate that the XGBoost algorithm performed the best, showing the highest AUC, AUCPR, and accuracy under the
The performance evaluation results of the 5 different algorithms for predicting 24-hour IOP fluctuations under feature selection with
The SHAP values for the model predicting 24-hour IOP fluctuations are illustrated in Figure 8. Among the features, age (Feature 4) was the most influential factor, demonstrating the highest SHAP value and contributing significantly to the model’s predictions. This was followed by IOP12pm (Feature 9) and MAP10am (Feature 12), which also play critical roles in the model’s performance. Additional significant contributors included IOP10am (Feature 8), CCT (Feature 6), and myopic refractive error (Feature 5). In contrast, treatment-related factors such as the number of anti-glaucoma drugs used (Feature 1) and the duration of anti-glaucoma drug use (Feature 2), as well as sex (Feature 3), had relatively minor impacts on the model.
We selected 2 patients for analysis: one with 24-hour IOP fluctuations greater than 8 mmHg (with daytime IOP fluctuations ≤8 mmHg), and the other with 24-hour IOP fluctuations ≤8 mmHg. SHAP force plots, which provide individualized explanations for the predicted 24-hour IOP fluctuations based on test set patient samples, are presented in Figure 9A, 9B. In these plots, the blue bars on the right represent features that contribute to lower IOP fluctuation predictions, while the red bars on the left correspond to features that contribute to higher IOP fluctuation predictions.
For Patient A, with 24-hour IOP fluctuations greater than 8 mmHg (and daytime IOP fluctuations ≤8 mmHg), factors such as elevated MAP10am, increased IOP4pm, and a higher myopic refractive error significantly contributed to the increased IOP fluctuations (Figure 9A). Additionally, patient sex and the number of anti-glaucoma drugs used were also influential (Figure 9A). For Patient B, who exhibited 24-hour IOP fluctuations ≤8 mmHg, high CCT and DBP10am were the primary drivers of the IOP fluctuations, while contributions from age as well as lower IOP10am and IOP12pm help to mitigate the fluctuations (Figure 9B).
Discussion
Conventional IOP measurements taken during working hours may offer an incomplete representation of a patient’s IOP profile, making it challenging for clinicians to establish precise IOP target values. Our analysis of 24-hour IOP data, shown in Figure 3, reveals higher IOP levels primarily between midnight and 8: 00 AM, with lower levels observed at other times. These findings align with the findings of previous studies on 24-hour IOP profiles [3,4,43]. This observation necessitates a deeper exploration, since relying solely on daytime IOP measurements may not adequately capture the nuances of a patient’s 24-hour IOP profile. Based on these considerations, we have a concept: while 24-hour IOP monitoring poses challenges, obtaining daytime IOP measurements is relatively feasible. Therefore, our study aims to develop a predictive model using machine learning algorithms.
The relationship between IOP fluctuations and glaucoma progression remains a subject of debate, potentially due to variations in study populations and methodologies. However, existing research indicates that 24-hour IOP fluctuations can be a significant factor in glaucoma progression. In China, diurnal IOP fluctuations exceeding 8 mmHg are typically considered indicative of abnormal IOP, warranting medication and close monitoring. Consequently, we opted to develop a predictive model for 24-hour IOP fluctuations using a binary classification algorithm. Our research results show that approximately 30% of eyes in our database experience 24-hour IOP fluctuations exceeding 8 mmHg, indicating a higher risk of glaucoma progression in this subgroup. Patients with abnormal IOP fluctuations may require closer monitoring and tailored treatment plans to mitigate the risk of glaucoma progression.
To address potential model overfitting, we conducted feature selection by reviewing existing literature and leveraging commonly available data types in standard healthcare environments. Subsequently, we refined these features based on the outcomes of correlation analysis. This feature-selection process is intended to help reduce the risk of model overfitting, improve model interpretability, lower computational complexity, and mitigate the impact of data noise.
Our study indicated that MOPP10am is negatively correlated with IOP fluctuations (
A study by Yuning Zhang et al demonstrated a positive correlation between male sex and IOP variation [48]. This sex difference may be related to sex hormones, which play a significant role in the pathogenesis of POAG [49–51]. Several studies have shown that hormone replacement therapy can reduce the risk of POAG. However, female sex is a risk factor for PACG [50,51]. These findings suggest that risk factors may differ between the sexes for different types of glaucoma. Our research indicates that male patients are more likely to experience IOP fluctuations greater than 8 mmHg over 24 hours. Further studies with larger sample sizes are needed to explore the relationship between sex and 24-hour IOP fluctuations.
The relationship between age and IOP remains controversial. While many studies have found a positive association between older age and higher IOP levels [20–24], other research presents different perspectives. For instance, some studies [52,53], such as those by Yang et al, have indicated that younger age, male sex, and thicker CCT are associated with higher IOP in patients with POAG [52]. In contrast, in patients with ocular hypertension, only a thicker CCT is correlated with higher IOP [52]. Our findings reveal a negative correlation between age and 24-hour IOP fluctuations, and a positive correlation between the number of medications and IOP fluctuations. These observations appear to conflict with some existing literature [20–24,54,55]. We speculate that these discrepancies may be related to the characteristics of our study population. Our study encompassed 3 categories of patients for 24-hour IOP monitoring: those aiding in glaucoma diagnosis, those receiving treatment with ongoing disease progression, and those assessed for the efficacy of IOP-lowering medications. The inclusion of these distinct patient groups may introduce bias into our results.
Younger patients, who may have lower rates of glaucoma diagnosis or have not yet commenced IOP-lowering treatment, may exhibit greater IOP fluctuations. Conversely, older patients, who are more likely to have a confirmed diagnosis and be on long-term medication, may demonstrate less fluctuation. Additionally, patients on a higher number of medications often have poorly controlled IOP, leading to increased 24-hour IOP variability.
The aim of our correlation analysis was to identify factors potentially affecting 24-hour IOP fluctuations to inform predictive modeling. The current analysis does not represent an exhaustive investigation. Future studies should incorporate more detailed subgroup analyses based on factors such as age and medication regimen, and include control groups to facilitate a more comprehensive examination of these relationships.
To ensure data integrity, the dataset was divided by individuals, not by eyes. Specifically, 80% of the participants were randomly assigned to the training set, while the remaining 20% were allocated to the testing set. This approach was implemented to prevent data overlap between the training and testing phases, thus ensuring the reliability and validity of the model evaluation.
For feature selection, we evaluated algorithms using features at
In our study, SHAP values were employed to identify factors influencing 24-hour IOP fluctuations and to enhance model interpretability (Figure 8). The results indicate that age is the most significant predictor of IOP fluctuations. Additionally, IOP12pm and MAP10am are important factors, highlighting the influence of time-specific measurements and systemic factors. CCT and myopic refractive error also play key roles in understanding individual IOP variations. Treatment-related factors, including the number of anti-glaucoma medications, duration of treatment with medication, and sex, have relatively minor impacts on the model’s predictions. This suggests that, while these factors are relevant, their effect on IOP fluctuations is less pronounced compared with physiological and anatomical factors.
SHAP force plots provide a detailed visualization of these findings (Figure 9). For Patient A, who experienced 24-hour IOP fluctuations exceeding 8 mmHg (with daytime IOP fluctuations ≤8 mmHg), elevated MAP10am, increased IOP later in the day, and higher myopic refractive error were major contributors. This suggests that changes in SBP and time-of-day variations in IOP are significant drivers of overall IOP fluctuation. The effects of patient sex and medication use point to a complex interaction among these variables. In contrast, in Patient B, with 24-hour IOP fluctuations ≤8 mmHg, higher CCT and DBP10am were associated with reduced fluctuations. Lower IOP at 10: 00 AM and 12: 00 PM also contributed to this stability, indicating their role in minimizing IOP fluctuations.
Overall, our results emphasize the multifactorial nature of IOP fluctuation, where age, time-specific IOP measurements, and anatomical features are all prominent factors. While treatment-related factors and sex have a lesser impact, they should still be considered in a comprehensive approach to IOP management. Future research should explore these relationships across diverse patient populations to validate and refine these findings, thereby enhancing the precision and effectiveness of IOP fluctuation management in clinical practice.
Our study is subject to several limitations. Firstly, the patient selection for 24-hour IOP monitoring was based on clinical needs, focusing on individuals with suspected glaucoma, POAG, or PACG, which may introduce selection bias and limit the generalizability of the model. The dataset primarily included patients with ocular diseases and lacked data from healthy individuals.
Secondly, while Goldmann applanation tonometry is a standard method for measuring IOP [56,57], it underscores the need for improved methodologies, particularly for nocturnal IOP measurements, to better guide clinical management. In our study, IOP measurements were taken while the patient was seated at night. Previous research suggests that IOP values may be higher when measured in the supine position at night, highlighting the potential variability introduced by different postures [58].
Additionally, our model used the number and duration of medications as features without differentiating specific medication regimens. Future research should incorporate detailed medication information to enhance the model’s accuracy.
Lastly, the model performed binary classification based on guidelines for 24-hour IOP fluctuations in China rather than predicting specific fluctuation values. Further validation and refinement are necessary to assess its applicability across different populations.
Conclusions
We have developed a predictive model for 24-hour IOP fluctuations using machine learning algorithms. By integrating key patient parameters collected during clinical visits and IOP measurements taken at specific time points (10: 00 AM, 12: 00 PM, 2: 00 PM, and 4: 00 PM), our model aims to predict whether IOP fluctuations exceed 8 mmHg over a 24-hour period. This approach is intended to offer a novel method for monitoring IOP and could potentially contribute to improved diagnosis and management of glaucoma.
Figures
 Figure 1. Flow of the feature-selection method.
Figure 1. Flow of the feature-selection method.  Figure 2. Flow of the prediction model. ROC, receiver operating characteristic.
Figure 2. Flow of the prediction model. ROC, receiver operating characteristic. 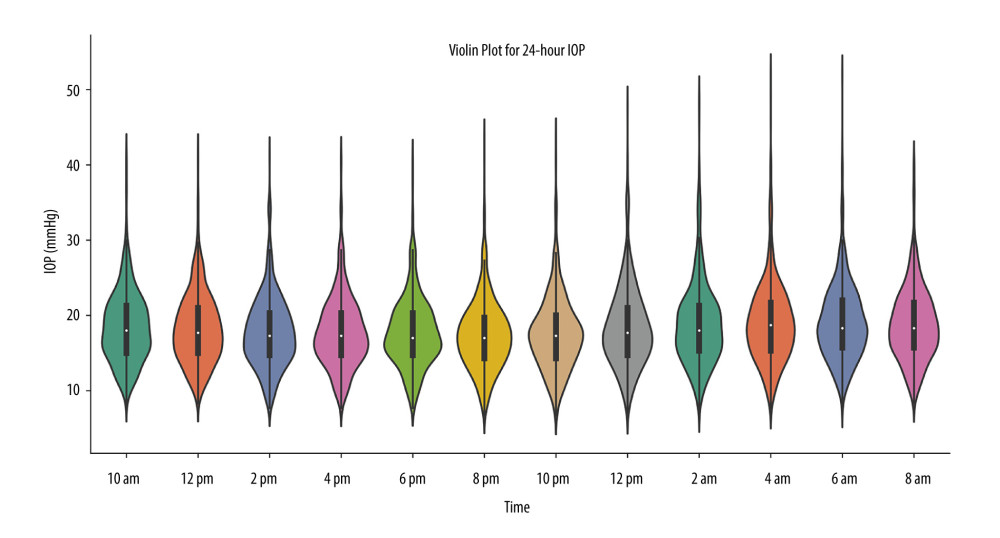 Figure 3. Profiles of 24-hour IOP. IOP, intraocular pressure.
Figure 3. Profiles of 24-hour IOP. IOP, intraocular pressure.  Figure 4. Heatmap of correlations between various features and 24-hour IOP fluctuations. IOP – intraocular pressure; MSO – metabolic status and obesity; C/D ratio – cup-to-disc ratio; RE – refractive error; CCT – central corneal thickness; SBP10am – systolic blood pressure at 10: 00 AM; DBP10am – diastolic blood pressure at 10: 00 AM; BMI – body mass index; IOP10am – intraocular pressure at 10: 00 AM; IOP12pm – intraocular pressure at 12: 00 PM; IOP2pm – intraocular pressure at 2: 00 PM; IOP4pm – intraocular pressure at 4: 00 PM; MAP10am – mean arterial pressure at 10: 00AM; SOPP10am – systolic ocular perfusion pressure at 10: 00 AM; DOPP10am – diastolic ocular perfusion pressure at 10: 00 AM; MOPP10am – mean ocular perfusion pressure at 10: 00 AM; S10am – the slope of the diurnal curve at 10: 00 AM; S12pm – the slope of the diurnal curve at 12: 00 PM; S2pm – the slope of the diurnal curve at 2: 00 PM.
Figure 4. Heatmap of correlations between various features and 24-hour IOP fluctuations. IOP – intraocular pressure; MSO – metabolic status and obesity; C/D ratio – cup-to-disc ratio; RE – refractive error; CCT – central corneal thickness; SBP10am – systolic blood pressure at 10: 00 AM; DBP10am – diastolic blood pressure at 10: 00 AM; BMI – body mass index; IOP10am – intraocular pressure at 10: 00 AM; IOP12pm – intraocular pressure at 12: 00 PM; IOP2pm – intraocular pressure at 2: 00 PM; IOP4pm – intraocular pressure at 4: 00 PM; MAP10am – mean arterial pressure at 10: 00AM; SOPP10am – systolic ocular perfusion pressure at 10: 00 AM; DOPP10am – diastolic ocular perfusion pressure at 10: 00 AM; MOPP10am – mean ocular perfusion pressure at 10: 00 AM; S10am – the slope of the diurnal curve at 10: 00 AM; S12pm – the slope of the diurnal curve at 12: 00 PM; S2pm – the slope of the diurnal curve at 2: 00 PM.  Figure 5. ROC curves and AUC for predicting 24-hour IOP fluctuations. (A) The 5 algorithms, P<1; (B) The 5 algorithms, P<0.1; (C) The 5 algorithms, P<0.05; (D) The 5 algorithms, P<0.025. ROC – receiver operating characteristic; AUC – area under the curve; IOP – intraocular pressure; SVM – support vector machines; LR – Logistic Regression; XGBoost – Extreme Gradient Boosting; KNN – K-Nearest Neighbors; Naive Bayes – Naive Bayes Classifier.
Figure 5. ROC curves and AUC for predicting 24-hour IOP fluctuations. (A) The 5 algorithms, P<1; (B) The 5 algorithms, P<0.1; (C) The 5 algorithms, P<0.05; (D) The 5 algorithms, P<0.025. ROC – receiver operating characteristic; AUC – area under the curve; IOP – intraocular pressure; SVM – support vector machines; LR – Logistic Regression; XGBoost – Extreme Gradient Boosting; KNN – K-Nearest Neighbors; Naive Bayes – Naive Bayes Classifier.  Figure 6. Precision-Recall curves and AUCPR results for predicting 24-hour IOP fluctuations. (A) The 5 algorithms, P<1; (B) The 5 algorithms, P<0.1; (C) The 5 algorithms, P<0.05; (D) The 5 algorithms, P<0.025. IOP, intraocular pressure; SVM – support vector machines; LR – Logistic Regression; XGBoost – Extreme Gradient Boosting; KNN – K-Nearest Neighbors; Naive Bayes – Naive Bayes Classifier.
Figure 6. Precision-Recall curves and AUCPR results for predicting 24-hour IOP fluctuations. (A) The 5 algorithms, P<1; (B) The 5 algorithms, P<0.1; (C) The 5 algorithms, P<0.05; (D) The 5 algorithms, P<0.025. IOP, intraocular pressure; SVM – support vector machines; LR – Logistic Regression; XGBoost – Extreme Gradient Boosting; KNN – K-Nearest Neighbors; Naive Bayes – Naive Bayes Classifier.  Figure 7. Accuracy of the 5 algorithms across different feature-selection criteria. SVM – support vector machines; LR – Logistic Regression; XGBoost – Extreme Gradient Boosting; KNN – K-Nearest Neighbors; Naive Bayes – Naive Bayes Classifier.
Figure 7. Accuracy of the 5 algorithms across different feature-selection criteria. SVM – support vector machines; LR – Logistic Regression; XGBoost – Extreme Gradient Boosting; KNN – K-Nearest Neighbors; Naive Bayes – Naive Bayes Classifier.  Figure 8. SHAP value analysis for 24-hour IOP fluctuation prediction models. IOP – intraocular pressure; IOP12pm – intraocular pressure at 12: 00 PM; MAP10am – mean arterial pressure at 10: 00AM; IOP10am – intraocular pressure at 10: 00 AM; CCT – central corneal thickness; RE – refractive error; MOPP10am – mean ocular perfusion pressure at 10: 00 AM; IOP4pm – intraocular pressure at 4: 00 PM; IOP2pm – intraocular pressure at 2: 00 PM; DBP10am – diastolic blood pressure at 10: 00 AM.
Figure 8. SHAP value analysis for 24-hour IOP fluctuation prediction models. IOP – intraocular pressure; IOP12pm – intraocular pressure at 12: 00 PM; MAP10am – mean arterial pressure at 10: 00AM; IOP10am – intraocular pressure at 10: 00 AM; CCT – central corneal thickness; RE – refractive error; MOPP10am – mean ocular perfusion pressure at 10: 00 AM; IOP4pm – intraocular pressure at 4: 00 PM; IOP2pm – intraocular pressure at 2: 00 PM; DBP10am – diastolic blood pressure at 10: 00 AM.  Figure 9. The SHAP force plot interpretations for individual prediction results. (A) A case with 24-hour IOP fluctuations exceeding 8 mmHg (with daytime IOP fluctuations ≤8 mmHg); (B) a case with 24-hour IOP fluctuations ≤8 mmHg. IOP – intraocular pressure; DBP10am – diastolic blood pressure at 10: 00 AM; CCT – central corneal thickness; RE, refractive error; IOP4pm – intraocular pressure at 4: 00 PM; MAP10am – mean arterial pressure at 10: 00AM; IOP10am – intraocular pressure at 10: 00 AM; IOP12pm – intraocular pressure at 12: 00 PM and IOP4pm – intraocular pressure at 4: 00 PM.
Figure 9. The SHAP force plot interpretations for individual prediction results. (A) A case with 24-hour IOP fluctuations exceeding 8 mmHg (with daytime IOP fluctuations ≤8 mmHg); (B) a case with 24-hour IOP fluctuations ≤8 mmHg. IOP – intraocular pressure; DBP10am – diastolic blood pressure at 10: 00 AM; CCT – central corneal thickness; RE, refractive error; IOP4pm – intraocular pressure at 4: 00 PM; MAP10am – mean arterial pressure at 10: 00AM; IOP10am – intraocular pressure at 10: 00 AM; IOP12pm – intraocular pressure at 12: 00 PM and IOP4pm – intraocular pressure at 4: 00 PM. 

References
1. Weinreb RN, Khaw PT, Primary open-angle glaucoma: Lancet, 2004; 363; 1711-20
2. Leske MC, Heijl A, Hyman L, Predictors of long-term progression in the early manifest glaucoma trial: Ophthalmology, 2007; 114(11); 1965-72
3. Choi J, Kim KH, Jeong J, Circadian fluctuation of mean ocular perfusion pressure is a consistent risk factor for normal-tension glaucoma: Invest Ophthalmol Vis Sci, 2007; 48; 104-11
4. Asrani S, Zeimer R, Wilensky J, Large diurnal fluctuations in intraocular pressure are an independent risk factor in patients with glaucoma: J Glaucoma, 2000; 9(2); 134-42
5. Bengtsson B, Leske MC, Hyman L, Fluctuation of intraocular pressure and glaucoma progression in the early manifest glaucoma trial: Ophthalmology, 2007; 114(2); 205-9
6. Musch DC, Gillespie BW, Niziol LM, Intraocular pressure control and long-term visual field loss in the collaborative initial glaucoma treatment study: Ophthalmology, 2011; 118(9); 1766-73
7. Lee PP, Walt JW, Rosenblatt LC, Association between intraocular pressure variation and glaucoma progression: Data from a United States chart review: Am J Ophthalmol, 2007; 144(6); 901-7
8. Caprioli J, Coleman AL, Intraocular pressure fluctuation a risk factor for visual field progression at low intraocular pressures in the advanced glaucoma intervention study: Ophthalmology, 2008; 115(7); 1123-29e3
9. Nouri-Mahdavi K, Hoffman D, Coleman AL, Predictive factors for glaucomatous visual field progression in the Advanced Glaucoma Intervention Study: Ophthalmology, 2004; 111(9); 1627-35
10. Gardiner SK, Fortune B, Wang L, Intraocular pressure magnitude and variability as predictors of rates of structural change in non-human primate experimental glaucoma: Exp Eye Res, 2012; 103; 1-8
11. Collaer N, Zeyen T, Caprioli J, Sequential office pressure measurements in the management of glaucoma: J Glaucoma, 2005; 14(3); 196-200
12. Kim JH, Caprioli J, Intraocular pressure fluctuation: Is it important?: J Ophthalmic Vis Res, 2018; 13(2); 170-74
13. Zhang MZ, Zhi FF, Liu XR, Zheng CA comparison study of pulsitile ocular blood flow in normal eyes and primary open angle glaucoma: Zhonghua Yan Ke Za Zhi, 2004; 40(4); 250-53 [in Chinese]
14. Li MY: Glaucoma Studies [M], 2004; 120, Beijing, People’s Medical Publishing House
15. Chen X, Wu XD, Lin XQ, Outcome, influence factor and development of CLS measurement in continuous IOP monitoring: A narrative review: Cont Lens Anterior Eye, 2021; 44(4); 101376
16. Steven Y, Rahul NK, Milan S, Efficacy and safety of suprachoroidal CLS-TA for macular edema secondary to noninfectious uveitis: Phase 3 randomized trial: Ophthalmology, 2020; 127(7); 948-55
17. Prum BE, Lim MC, Mansberger SL, Primary open-angle glaucoma suspect preferred practice pattern (PPP) guidelines: Ophthalmology, 2016; 123(1); 112-51
18. Prum BE, Herndon LW, Moroi SE, Primary angle-closure preferred practice pattern (PPP) guidelines: Ophthalmology, 2016; 123(1); 1-P40
19. Prum BE, Rosenberg LF, Gedde SJ, Primary open-angle glaucoma preferred practice pattern (PPP) guidelines: Ophthalmology, 2016; 123(1); 41-111
20. Seah SK, Foster PJ, Chew PT, Incidence of acute primary angle-closure glaucoma in Singapore. An island-wide survey: Arch Ophthalmol, 1997; 115; 1436-40
21. Gordon MO, Beiser JA, Brandt JD, The Ocular Hypertension Treatment Study: Baseline factors that predict the onset of primary open-angle glaucoma: Arch Ophthalmol, 2002; 120; 714-20 discussion 829–30
22. Le A, Mukesh BN, McCarty CA, Taylor HR, Risk factors associated with the incidence of open-angle glaucoma: The visual impairment project: Invest Ophthalmol Vis Sci, 2003; 44; 3783-89
23. Dielemans I, Vingerling JR, Wolfs RC, The prevalence of primary open-angle glaucoma in a population-based study in The Netherlands: The Rotterdam Study: Ophthalmology, 1994; 101; 1851-55
24. Kass MA, Heuer DK, Higginbotham EJ, The Ocular Hypertension Treatment Study: A randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma: Arch Ophthalmol, 2002; 120; 701-713 discussion 829–30
25. Leske MC, Wu SY, Hennis ABESs Study Group, Risk factors for incident open-angle glaucoma: The Barbados Eye Studies: Ophthalmology, 2008; 115; 85-93
26. Tielsch JM, Katz J, Sommer A, Hypertension, perfusion pressure, and primary open-angle glaucoma. A population-based assessment: Arch Ophthalmol, 1995; 113; 216-21
27. Leske MC, Connell AM, Wu SY, Risk factors for open-angle glaucoma. The Barbados Eye Study: Arch Ophthalmol, 1995; 113; 918-24
28. Mitchell P, Hourihan F, Sandbach J, Wang JJ, The relationship between glaucoma and myopia: The Blue Mountains Eye Study: Ophthalmology, 1999; 106; 2010-2015
29. Grodum K, Heijl A, Bengtsson B, Refractive error and glaucoma: Acta Ophthalmol Scand, 2001; 79; 560-66
30. Xu L, Wang Y, Wang S, Jonas JB, High myopia and glaucoma susceptibility the Beijing Eye Study: Ophthalmology, 2007; 114; 216-20
31. Brandt JD, Beiser JA, Kass MA, Gordon MO, Central corneal thickness in the Ocular Hypertension Treatment Study (OHTS): Ophthalmology, 2001; 108; 1779-88
32. Wolfs RC, Grobbee DE, Hofman A, de Jong PT, Risk of acute angle-closure glaucoma after diagnostic mydriasis in nonselected subjects: The Rotterdam Study: Invest Ophthalmol Vis Sci, 1997; 38; 2683-87
33. Reddy A, Halenda K, Cromer P, The association of intraocular pressure with obesity and cardiometabolic risk in a young farmworker population: J Glaucoma, 2021; 30(1); 24-31
34. Jung Y, Kim GN, Oh EB, Metabolic health, obesity, and intraocular pressure: J Clin Med, 2023; 12(5); 2066
35. World Health Organization, Regional Office for the Western Pacific: The Asia-Pacific perspective: Redefining obesity and its treatment, 2000, Sydney, Australia, Health communications Australia
36. Alberti KG, Eckel RH, Grundy SM, Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity: Circulation, 2009; 120; 1640-45
37. Camilo BR, Sebastião C, Veloso AW, Use of machine learning to predict the risk of early morning intraocular pressure peaks in glaucoma patients and suspects: Arq Bras Oftalmol, 2021; 84(6); 569-75
38. Costa VP, Harris A, Anderson D, Ocular perfusion pressure in glaucoma: Acta Ophthalmol, 2014; 92(4); e252-66
39. Zheng Y, Wong TY, Mitchell P, Distribution of ocular perfusion pressure and its relationship with open-angle glaucoma: The Singapore Malay eye study: Invest Ophthalmol Vis Sci, 2010; 51(7); 3399-404
40. Bowe A, Grünig M, Schubert J, Circadian variation in arterial blood pressure and glaucomatous optic neuropathy – a systematic review and meta-analysis: Am J Hypertens, 2015; 28; 1077-82
41. Charlson ME, de Moraes CG, Link A, Nocturnal systemic hypotension increases the risk of glaucoma progression: Ophthalmology, 2014; 121; 2004-12
42. Memarzadeh F, Mei YL, Chung J, Blood pressure, perfusion pressure, and open-angle glaucoma: The Los Angeles Latino Eye Study: Invest Ophthalmol Vis Sci, 2010; 51(6); 2872-77
43. Quaranta L, Katsanos A, Russo A, 24-hour intraocular pressure and ocular perfusion pressure in glaucoma: Surv Ophthalmol, 2013; 58(1); 26-41
44. Medeiros FA, Sample PA, Zangwill LM, Corneal thickness as a risk factor for visual field loss in patients with preperimetric glaucomatous optic neuropathy: Am J Ophthalmol, 2003; 136; 805-13
45. Dueker DK, Singh K, Lin SC, Corneal thickness measurement in the management of primary open-angle glaucoma: A report by the American Academy of Ophthalmology: Ophthalmology, 2007; 114; 1779-87
46. Congdon NG, Broman AT, Bandeen-Roche K, Central corneal thickness and corneal hysteresis associated with glaucoma damage: Am J Ophthalmol, 2006; 141; 868-75
47. Kim JW, Chen PP, Central corneal pachymetry and visual field progression in patients with open-angle glaucoma: Ophthalmology, 2004; 111; 2126-32
48. Zhang YN, Wei YF, Lee CHC, Continuous 24-hour intraocular pressure monitoring in normal Chinese adults using a novel contact lens sensor system: Br J Ophthalmol, 2024 [Online ahead of print]
49. Russo R, Cavaliere F, Watanabe C, Beta-estradiol prevents retinal ganglion cell loss induced by acute rise of intraocular pressure in rat: Prog Brain Res, 2008; 173; 583-90
50. Pasquale LR, Rosner BA, Hankinson SE, Kang JH, Attributes of female reproductive aging and their relation to primary open-angle glaucoma: A prospective study: J Glaucoma, 2007; 16; 598-605
51. Newman-Casey PA, Talwar N, Nan B, The potential association between postmenopausal hormone use and primary open-angle glaucoma: JAMA Ophthalmol, 2014; 132; 298-303
52. Yang YF, Zhang XY, Chen ZD, Intraocular pressure and diurnal fluctuation of open-angle glaucoma and ocular hypertension: A baseline report from the LiGHT China trial cohort: Br J Ophthalmol, 2023; 107(6); 823-27
53. Yang YF, Jiang YZ, Huang ST, Laser in glaucoma and ocular hypertension trial (LIGHT) in China – a randomized controlled trial: Design and baseline characteristics: Am J Ophthalmo, 2021; 230; 143-50
54. Varma R, Hwang LJ, Grunden JW, Bean GW, Using diurnal intraocular pressure fluctuation to assess the efficacy of fixed-combination latanoprost/timolol versus latanoprost or timolol monotherapy: Br J Ophthalmol, 2010; 94(1); 80-84
55. Özyol E, Özyol P, The efficacy of a latanoprost/timolol fixed combination versus latanoprost and timolol gel-forming solution unfixed combination on daytime intraocular pressure: J Glaucoma, 2016; 25(2); 135-39
56. Goldmann H, Schmidt T, Applanation tonometry: Ophthalmologica, 1957; 134; 221-42
57. Ehlers N, Bramsen T, Sperling S, Applanation tonometry and central corneal thickness: Acta Ophthalmol (Copenh), 1975; 53; 34-43
58. Weber AK, Price J, Pressure differential of intraocular pressure measured between supine and sitting position: Ann Ophthalmol, 1981; 13(3); 323-26
Figures
Figure 1. Flow of the feature-selection method.Figure 2. Flow of the prediction model. ROC, receiver operating characteristic.Figure 3. Profiles of 24-hour IOP. IOP, intraocular pressure.Figure 4. Heatmap of correlations between various features and 24-hour IOP fluctuations. IOP – intraocular pressure; MSO – metabolic status and obesity; C/D ratio – cup-to-disc ratio; RE – refractive error; CCT – central corneal thickness; SBP10am – systolic blood pressure at 10: 00 AM; DBP10am – diastolic blood pressure at 10: 00 AM; BMI – body mass index; IOP10am – intraocular pressure at 10: 00 AM; IOP12pm – intraocular pressure at 12: 00 PM; IOP2pm – intraocular pressure at 2: 00 PM; IOP4pm – intraocular pressure at 4: 00 PM; MAP10am – mean arterial pressure at 10: 00AM; SOPP10am – systolic ocular perfusion pressure at 10: 00 AM; DOPP10am – diastolic ocular perfusion pressure at 10: 00 AM; MOPP10am – mean ocular perfusion pressure at 10: 00 AM; S10am – the slope of the diurnal curve at 10: 00 AM; S12pm – the slope of the diurnal curve at 12: 00 PM; S2pm – the slope of the diurnal curve at 2: 00 PM.Figure 5. ROC curves and AUC for predicting 24-hour IOP fluctuations. (A) The 5 algorithms, P<1; (B) The 5 algorithms, P<0.1; (C) The 5 algorithms, P<0.05; (D) The 5 algorithms, P<0.025. ROC – receiver operating characteristic; AUC – area under the curve; IOP – intraocular pressure; SVM – support vector machines; LR – Logistic Regression; XGBoost – Extreme Gradient Boosting; KNN – K-Nearest Neighbors; Naive Bayes – Naive Bayes Classifier.Figure 6. Precision-Recall curves and AUCPR results for predicting 24-hour IOP fluctuations. (A) The 5 algorithms, P<1; (B) The 5 algorithms, P<0.1; (C) The 5 algorithms, P<0.05; (D) The 5 algorithms, P<0.025. IOP, intraocular pressure; SVM – support vector machines; LR – Logistic Regression; XGBoost – Extreme Gradient Boosting; KNN – K-Nearest Neighbors; Naive Bayes – Naive Bayes Classifier.Figure 7. Accuracy of the 5 algorithms across different feature-selection criteria. SVM – support vector machines; LR – Logistic Regression; XGBoost – Extreme Gradient Boosting; KNN – K-Nearest Neighbors; Naive Bayes – Naive Bayes Classifier.Figure 8. SHAP value analysis for 24-hour IOP fluctuation prediction models. IOP – intraocular pressure; IOP12pm – intraocular pressure at 12: 00 PM; MAP10am – mean arterial pressure at 10: 00AM; IOP10am – intraocular pressure at 10: 00 AM; CCT – central corneal thickness; RE – refractive error; MOPP10am – mean ocular perfusion pressure at 10: 00 AM; IOP4pm – intraocular pressure at 4: 00 PM; IOP2pm – intraocular pressure at 2: 00 PM; DBP10am – diastolic blood pressure at 10: 00 AM.Figure 9. The SHAP force plot interpretations for individual prediction results. (A) A case with 24-hour IOP fluctuations exceeding 8 mmHg (with daytime IOP fluctuations ≤8 mmHg); (B) a case with 24-hour IOP fluctuations ≤8 mmHg. IOP – intraocular pressure; DBP10am – diastolic blood pressure at 10: 00 AM; CCT – central corneal thickness; RE, refractive error; IOP4pm – intraocular pressure at 4: 00 PM; MAP10am – mean arterial pressure at 10: 00AM; IOP10am – intraocular pressure at 10: 00 AM; IOP12pm – intraocular pressure at 12: 00 PM and IOP4pm – intraocular pressure at 4: 00 PM. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387