04 March 2025: Clinical Research
Gastrointestinal System Endoscopy and Pathological Findings in Non-Dialysis Chronic Kidney Disease: A Single-Center Study
Mehmet Usta DOI: 10.12659/MSM.946516
Med Sci Monit 2025; 31:e946516






Abstract
BACKGROUND: Different gastrointestinal complications can occur due to moderate and severe kidney function loss in chronic kidney disease (CKD). This study examined the endoscopic and pathological findings in CKD patients with renal failure who were not receiving dialysis treatment and renal transplantation.
MATERIAL AND METHODS: A total of 60 pre-dialysis CKD patients who underwent upper-gastrointestinal endoscopy due to dyspeptic concerns were included. Endoscopic and pathological findings were compared with those of 68 non-uremic patients with similar concerns. Dyspeptic symptoms included upper-abdominal discomfort, nausea, vomiting, anorexia, indigestion, and regurgitation. Serum creatinine levels ≥1.5 mg/dL and eGFR stages 3a-4 (KDIGO guidelines) were used to define CKD.
RESULTS: This study found no significant difference in gastroesophageal reflux frequency between the groups. However, antral gastritis, erythematous gastritis, active chronic gastritis, and non-ulcerative lesions were significantly more frequent in CKD patients (P<0.001). Conversely, erosive pangastritis was more prevalent in the non-CKD group. Helicobacter pylori (HP) frequency was significantly lower in CKD patients (23.5%) compared to the non-CKD group (59.1%, P<0.001). Intestinal metaplasia, atrophy, and metaplastic gastritis rates were similar in both groups. Multivariate analysis identified gastritis and serum calcium as independent factors affecting HP positivity.
CONCLUSIONS: In CKD patients, uremic toxins, impaired circulation, and hypergastrinemia likely contribute to mucosal damage and increased the risk of gastrointestinal complications. Early detection and management of these lesions in pre-dialysis CKD patients are crucial, especially for kidney transplant candidates. Endoscopic evaluation and appropriate treatment can help reduce potential complications associated with immunosuppressive therapy and can improve patient outcomes.
Keywords: Dialysis, Endoscopes, Gastrointestinal, Kidney Failure, Chronic, gastritis, Helicobacter pylori, Dyspepsia, Pathology, Clinical, Humans, Male, Female, Middle Aged, Renal Insufficiency, Chronic, Endoscopy, Gastrointestinal, Aged, adult, Renal Dialysis, Helicobacter Infections
Introduction
Complications can occur due to decreased kidney function in patients with chronic kidney disease (CKD) [1]. Gastrointestinal problems are one of them. In patients with CKD, hypergastrinemia due to uremic toxins is associated with decreased gastrointestinal motility, hypo- and hypersecretion of stomach acid, polypharmacy, and the risk of gastrointestinal disturbances due to
In this study, we assessed endoscopic and pathological findings in patients with severe CKD who underwent upper-gastrointestinal system endoscopy due to dyspepsia.
Material and Methods
STATISTICAL ANALYSIS:
We used the Shapiro-Wilk test to assess the normal distribution of continuous variables. We present descriptive statistics for group comparisons, including mean±standard deviation or median (minimum: maximum) values. We made comparisons of numerical variables in both groups using the Mann-Whitney U test and the independent paired-sample
Results
A total of 128 patients were included in the study. The mean age in the CKD group was similar to that the non-CKD group (median age was 59) [59.5±11.5 (25–79) vs. 53.6±13.2 (29–86) years] (
Endoscopic findings are given in Table 2. The 2 groups had similar rates of non-ulcerous and ulcerous lesions, such as gastroesophageal reflux, antral erosive gastritis, duodenitis and fundus polyp. The CKD group had significantly higher rates of antral gastritis, erythematous gastritis, erosive pangastritis, active chronic gastritis, and esophageal varicose veins, whereas the non-CKD group had significantly higher rates of esophagitis LA and bulbitis (Figure 1). Pyloric diverticulum was not detected in either group.
Histopathological findings obtained from biopsy samples are shown in Table 3 and Figures 2–4. The groups had similar rates of intestinal metaplasia and oedema-congestion, atrophic metaplastic gastritis, fundic and hyperplastic polyps, and chronic gastritis. The incidence of inflammation in the CKD group was significantly higher than in the non-CKD group (48.3% vs 20.6%,
Multivariate logistic regression analysis determined independent risk factors affecting the development of endoscopic gastritis, duodenitis, pathological chronic gastritis, and HP. The logistic regression models obtained in the last stage of the analysis were found to be significant, and the data set was found to be compatible with the models. The variables included in the regression analysis models were determined for each dependent variable. For the presence of endoscopic gastritis: pathological chronic gastritis, HP positivity, hypertension, triglyceride, LDL and HDL cholesterol (Model χ2=11.5,
Discussion
Upper-gastrointestinal system disorders are common in CKD patients due to high ammonium levels, systemic and local circulatory disorders, frequent drug use, and hypergastrinemia [5]. However, in most patients, symptom severity does not correlate with severity of gastroduodenal lesions as assessed by endoscopy, and most patients have mild symptoms [6]. In our previous study of patients receiving hemodialysis (HD) or peritoneal dialysis (PD) maintenance therapy for end-stage renal disease, most did not have any significant upper-gastrointestinal symptoms despite the high rate of gastritis in HD (63.6%) and PD (61.3%) patients [7]. In the current study, antral gastritis, erythematous gastritis, erosive pangastritis, and active chronic gastritis were found to be significantly higher in our non-dialysis uremic patients with Stage 3b and Stage 4 CKD, while the rates of esophageal varicose veins, esophagitis, and bulbitis were higher in the non-uremic control group. Lower albumin, total cholesterol, and LDL and HDL levels are seen in addition to anemia in many patients, often due to infection, inflammation, nutritional deficiency, or erythropoietin deficiency.
In different studies conducted in chronic HD patients, erosive esophagitis 30.2%, gastroesophageal reflux 10%, esophagitis 5.8%, exanthematous pangastritis 57.3%, diffuse antral erythema 27.8%, gastric erosion 5.8%, gastric antral erosion 22.8%, gastric intestinal metaplasia 8.3%, gastritis and duodenitis 42%, duodenal erosion 18–32%, peptic ulcer 7.3%, gastric ulcer 7–14%, duodenal ulcer 7.3–18%, angiodysplasia 4.4%, and gastric polyp were observed at rates of 1.5% [5,8–11]. In our previous study of dialysis patients, we found gastroesophageal reflux in 41.5%, chronic gastritis in 75.5%, non-specific gastritis in 24.5%, intestinal metaplasia in 17%, atrophy in 15.1%, HP in 28.3%, and hyperplastic polyp in 3.8% [7]. Gastric dysplasia was not detected in either of our studies. While rates of antral gastritis, erythematous gastritis, erosive pangastritis, active chronic gastritis, and esophageal varicose veins were detected at lower rates in the CKD group, esophagitis and bulbitis rates were significantly higher in the non-CKD-group.
The frequency of ulcerous lesions was similar in both groups. The frequency of ulcerative lesions in the general population is 10–20% [12]. A retrospective study of dialysis patients found 31.8% had peptic ulcers, and age, low albumin, high GGT, peritoneal dialysis, and diabetes were reported as risk factors [13]. In the present study, intestinal metaplasia was detected in 8.3%, edema-congestion in 10%, inflammation in 48.3%, HP in 23.5%, atrophy metaplastic gastritis in 3.3%, fundus polyp in 3.3%, hyperplastic polyp in 6.7%, and chronic gastritis in 43.3%. The rates in the control group were 14.7% for intestinal metaplasia, 2.9% for edema-congestion, 20.6% for inflammation, 59.1% for HP, 2.9% for fundus polyp, 2.9% for hyperplastic polyp, and 41.2% for chronic gastritis. Inflammation was significantly higher in the CKD group than in the control group. However, although this rate in dialysis patients is reported to be as high as 75.5% in the literature, the frequency of chronic gastritis that we found to be higher in the CKD group in our study did not reach statistical significance [7].
HP was more common in the control group than in the CKD group (59.1% vs 23.5%). While the prevalence of HP is 24–32% in the general population, it was found to be 28.3% in dialysis patients [7,12]. In the present study, the rate of chronic gastritis was 41.2% in the non-uremic patient group with high HP and 43.3% in the CKD group. In a previous study of hemodialysis patients, the prevalence of
The rates of esophagitis (13.2%) and duodenitis (18.9%) in chronic dialysis patients in our previous study were close to the rates in the current study (13.3%) [7]. In the non-uremic patient group, the rate of esophagitis was higher (53.7%). In studies conducted in HD patients, gastroesophageal reflux was found in 10%, 15% in our patients, and 6% in the control group [5,9,10], while pangastritis was high in HD patients (57.3%), and this rate was lower in our patients (13.3%). Pangastritis is very common in HD patients. While antral erosive gastritis was found in 27.8% of HD patients, this rate was lower (6.7%) in our non-dialysis CKD patients. Antral gastritis, erythematous gastritis, erosive pangastritis, active chronic gastritis, and inflammation were significantly higher in our non-dialysis CKD patients than in the control group. Many drugs used for complications such as high serum urea level, inflammation, stress, mineral bone disorder, anemia, and hypertension in patients with CKD may be effective in this condition, together with uremic toxins [13,15].
A recent study found that gastrointestinal symptoms and signs were common in patients with CKD. Some symptoms and diseases also varied according to whether the renal replacement was peritoneal or hemodialysis type. The prevalence of esophagitis and gastritis diagnosed by symptomatic evaluation varied depending on the type of dialysis and whether it occurred in the pre-dialysis period. Although our study differed from this one in that it included endoscopic diagnostic classification of symptomatic pre-dialysis patients compared to non-uremic patients, the significant difference in the frequency of esophagitis and gastritis histologic subtypes between the groups is compatible with the above study [16].
In our study, no statistically significant independent relationships were detected between hemoglobin, urea, and total cholesterol and the presence of duodenitis, chronic gastritis, and HP in multivariate logistic regression analysis. Our previous study of dialysis patients showed the independent effect of HP and total cholesterol [7].
Conclusions
In uremic patients, risk factors like urea-related toxins, impairment of local and systemic circulations, and hypergastrinemia cause damage to the gastric mucosa. In addition, in chronic uremic patients with cardiovascular damage, anemia and mineral bone disease are frequently seen. These complications and the medications administered to treat them can adversely affect the upper-gastrointestinal system. In the general population, chronic gastritis, inflammation, and gastric and duodenal ulcers are seen frequently. These diseases generally cause symptoms such as vomiting, anorexia, abdominal pain, heartburn, and bleeding. Although most chronic uremic patients have these lesions, they remain asymptomatic.
Even though most chronic uremic patients have these lesions since they remain asymptomatic so, their diagnosis and treatment are often delayed; therefore, the lesions that arise in the gastrointestinal system among pre-dialysis uremic patients should be treated early, bearing in mind that they are potential candidates for kidney transplantation. Adverse effects on the gastrointestinal system of the drugs used, especially in uremic patients, should be minimized.
Figures
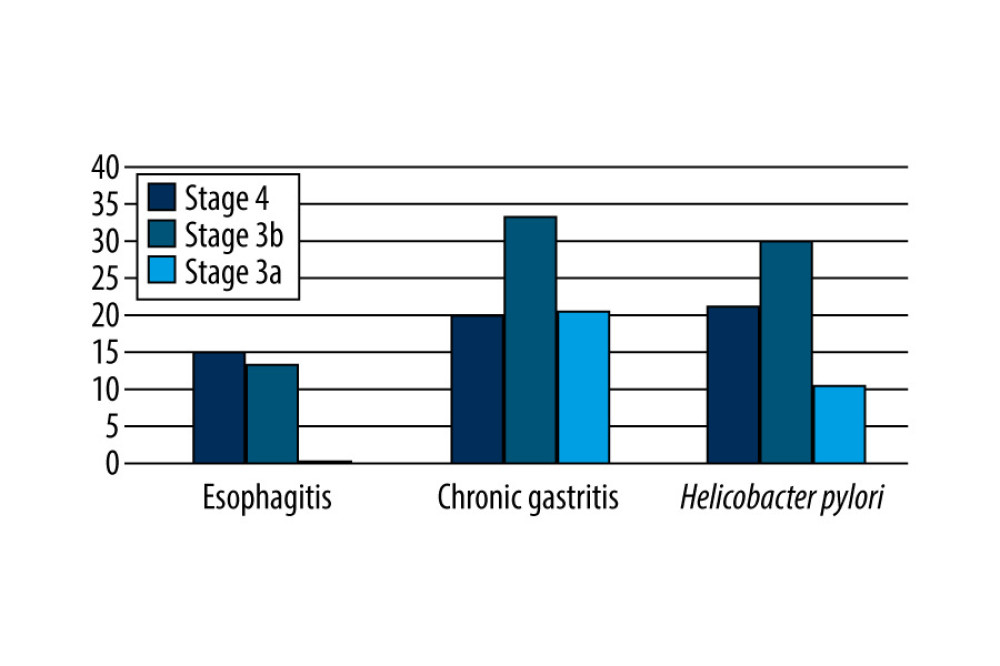 Figure 1. Esophagitis, chronic gastritis, and H. pylori rates determined according to the stages of chronic kidney disease.
Figure 1. Esophagitis, chronic gastritis, and H. pylori rates determined according to the stages of chronic kidney disease.  Figure 2. Stomach pathology stained with hematoxylin-eosin (H&E), Chronic gastritis; Marked inflammatory cell infiltration in the lamina propria. Possible glandular changes and lymphoid cell clusters.
Figure 2. Stomach pathology stained with hematoxylin-eosin (H&E), Chronic gastritis; Marked inflammatory cell infiltration in the lamina propria. Possible glandular changes and lymphoid cell clusters.  Figure 3. Stomach pathology stained with hematoxylin-eosin (H&E). Chronic active gastritis is usually seen in patients with Helicobacter pylori infection. Lymphocytic inflammation and neutrophilic epithelium infiltration.
Figure 3. Stomach pathology stained with hematoxylin-eosin (H&E). Chronic active gastritis is usually seen in patients with Helicobacter pylori infection. Lymphocytic inflammation and neutrophilic epithelium infiltration.  Figure 4. Stomach pathology stained with hematoxylin-eosin (H&E). Erythematous gastritis, mucosal structure, glandular structures on the upper left. In the lamina propria, clusters of red erythrocytes are evident on the left side.
Figure 4. Stomach pathology stained with hematoxylin-eosin (H&E). Erythematous gastritis, mucosal structure, glandular structures on the upper left. In the lamina propria, clusters of red erythrocytes are evident on the left side. Tables
Table 1. Comparison of laboratory parameters of both groups. Table 2. Comparison of endoscopic findings of both groups.
Table 2. Comparison of endoscopic findings of both groups. Table 3. Comparison of pathological findings in groups.
Table 3. Comparison of pathological findings in groups. Table 4. Multivariable logistic regression analysis of independent risk factors affecting the development of endoscopic gastritis and duodenitis and pathological chronic gastritis and HP positivity.
Table 4. Multivariable logistic regression analysis of independent risk factors affecting the development of endoscopic gastritis and duodenitis and pathological chronic gastritis and HP positivity.
References
1. , KDIGO 2012 Clinic practice guideline for the evaluation and management of chronic kidney disease: Kidney Int Suppl, 2013; 3; 136
2. Strid H, Simrén M, Johansson AC, The prevalence of gastrointestinal symptoms in patients with chronic renal failure is increased and associated with impaired psychological general well-being: Nephrol Dial Transplant, 2002; 17(8); 1434-39
3. Leja M, Grinberga-Derica I, Bilgilier C, Steininger C: Helicobacter, 2019; 24(Suppl 1); e12635
4. Zhou F, Zhong X, Chen J: Diabetes Res Clin Pract, 2015; 110(3); 328-34
5. Wijarnpreecha K, Thongprayoon C, Nissaisorakarn P: World J Gastroenterol, 2017; 23(8); 1497-506
6. Sotoudehmanesh R, Ali Asgari A, Ansari R, Nouraie M, Endoscopic findings in end-stage renal disease: Endoscopy, 2003; 35(6); 502-5
7. Usta M, Ersoy A, Ayar Y, Comparison of endoscopic and pathological findings of the upper gastrointestinal tract in transplant candidate patients undergoing hemodialysis or peritoneal dialysis treatment: A review of literature: BMC Nephrol, 2020; 21(1); 444
9. Bunchorntavakul C, Atsawarungruangkit A: J Med Assoc Thai, 2014; 97(Suppl 11); S62-68
10. Homse Netto JP, Pinheiro JPS, Ferrari ML, Upper gastrointestinal alterations in kidney transplant candidates: J Bras Nefrol, 2018; 40(3); 266-72
11. Karari EM, Lule GN, McLigeyo SO, Amayo EO: East Afr Med J, 2000; 77(8); 406-9
12. Moriyama T, Matsumoto T, Hirakawa K: J Gastroenterol, 2010; 45(5); 515-22
13. Kim M, Kim CS, Bae EH, Risk factors for peptic ulcer disease in patients with end-stage renal disease receiving dialysis: Kidney Res Clin Pract, 2019; 38(1); 81-89
14. Huang C, Chen Q, Jiang J: Ren Fail, 2012; 34(4); 420-24
15. Zhang X, Bansal N, Go AS, Hsu CY, Gastrointestinal symptoms, inflammation and hypoalbuminemia in chronic kidney disease patients: A cross-sectional study: BMC Nephrol, 2015; 16; 211
16. Karahan D, Şahin İ, Comparison of gastrointestinal symptoms and findings in renal replacement therapy modalities: BMC Nephrol, 2022; 23(1); 261
Figures
Figure 1. Esophagitis, chronic gastritis, and H. pylori rates determined according to the stages of chronic kidney disease.Figure 2. Stomach pathology stained with hematoxylin-eosin (H&E), Chronic gastritis; Marked inflammatory cell infiltration in the lamina propria. Possible glandular changes and lymphoid cell clusters.Figure 3. Stomach pathology stained with hematoxylin-eosin (H&E). Chronic active gastritis is usually seen in patients with Helicobacter pylori infection. Lymphocytic inflammation and neutrophilic epithelium infiltration.Figure 4. Stomach pathology stained with hematoxylin-eosin (H&E). Erythematous gastritis, mucosal structure, glandular structures on the upper left. In the lamina propria, clusters of red erythrocytes are evident on the left side. Tables
Table 1. Comparison of laboratory parameters of both groups.Table 2. Comparison of endoscopic findings of both groups.Table 3. Comparison of pathological findings in groups.Table 4. Multivariable logistic regression analysis of independent risk factors affecting the development of endoscopic gastritis and duodenitis and pathological chronic gastritis and HP positivity.Table 1. Comparison of laboratory parameters of both groups.Table 2. Comparison of endoscopic findings of both groups.Table 3. Comparison of pathological findings in groups.Table 4. Multivariable logistic regression analysis of independent risk factors affecting the development of endoscopic gastritis and duodenitis and pathological chronic gastritis and HP positivity. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387