12 July 2025: Clinical Research
Association Between Central Obesity and Membranous Nephropathy
Daoyuan Lv BCDEFG 1,2, Laping Chu BCDF 1,2, Yuan Du BCDF 1,2, Hongwei Jiang BCD 1,2, Xilian Zhou BCD 1,2, Yafen Yu AG 1,2*
DOI: 10.12659/MSM.947570
Med Sci Monit 2025; 31:e947570






Abstract
BACKGROUND: The global prevalence of central obesity has increased dramatically. However, the impact of central obesity on membranous nephropathy (MN) remains elusive. This retrospective cross-sectional study investigated the association between central obesity and MN.
MATERIAL AND METHODS: The study enrolled 255 biopsy-proven MN patients. Central obesity was evaluated with waist-to-hip ratio (WHR). The clinical/pathological phenotypes of MN patients were evaluated via urinary/blood biochemistry and renal pathology examinations. Clinical/pathological phenotypes were compared between patients with and without central obesity. Correlations between the WHR and clinical/pathological phenotypes were explored. The risks of central obesity for massive proteinuria and severe podocyte injury were investigated.
RESULTS: Patients with central obesity were more likely to have more severe nephrotic syndrome and podocyte injury, as indicated by increased 24 h urine protein (24 h-UPro), total cholesterol (T-CHOL), triglyceride (TG), high-density lipoprotein (HDL), and low-density lipoprotein (LDL) levels; increased average podocyte foot process width; and decreased serum total protein (TP) and albumin (ALB) levels. They also tended to have poorer renal function and more severe glomerular immunoglobulin and complement deposition and sclerosis. Central obesity was also positively correlated with 24 h-UPro, T-CHOL, TG, HDL, LDL, and the podocyte foot process width, and was negatively correlated with TP and ALB. Central obesity is also a risk factor for massive proteinuria and severe podocyte injury.
CONCLUSIONS: Central obesity can have adverse effects on MN.
Keywords: Obesity, Nephrology, nephrotic syndrome, Podocytes, Humans, Glomerulonephritis, Membranous, Male, Female, Middle Aged, adult, Cross-Sectional Studies, Retrospective Studies, Obesity, Abdominal, Proteinuria, Risk Factors, Waist-Hip Ratio, kidney
Introduction
Membranous nephropathy (MN) is an autoimmune glomerular disease that is a leading cause of nephrotic syndrome and end-stage renal disease [1]. MN is characterized by extensive alterations in podocyte structure and function caused by subepithelial immune complex deposition and complement activation. Due to the recent discovery of a series of novel antigens, understanding of the pathophysiology of MN has substantially advanced [2]. However, the factors that initiate and exacerbate MN remain largely unknown.
Central obesity is characterized by the accumulation of ectopic fat in the abdomen, which can be effectively measured via the waist-to-hip ratio (WHR) [3]. The global prevalence of central obesity has increased dramatically in recent decades due to physical inactivity and unhealthy diet [4,5]. Emerging evidence suggests that obesity-related lipotoxicity can exacerbate podocyte injury through mitochondrial oxidative stress, inflammatory response, and cytoskeletal remodeling, and central obesity significantly increases the risk of the onset and progression of chronic kidney disease (CKD) [6–10]. However, the specific impact of central obesity – a stronger predictor of metabolic risk than general obesity – on MN progression remains controversial. A critical knowledge gap exists regarding whether visceral adiposity directly aggravates immune-mediated podocytopathy or merely reflects systemic metabolic disturbances. This cross-sectional study systematically investigated the epidemiological and clinicopathological correlates of central obesity in MN, beginning with establishing its prevalence in biopsy-confirmed MN patients, proceeding to compare clinical profiles and histological injury patterns between centrally obese and non-obese subgroups, and ultimately determining the effect of central obesity on critical features of MN, including massive proteinuria and severe podocyte injury.
Material and Methods
STUDY DESIGN AND POPULATION:
This was a retrospective, cross-sectional, observational study. The sample size calculation was performed with Cochran’s formula. The prevalence of central obesity in MN was hypothesized to range from 5% to 25% (informed by a reported prevalence of 16.79% in Chinese adults) [4], and the parameters included a 95% confidence level and a 5% margin of error. The estimated sample size ranged from 73 to 289 cases. We enrolled hospital inpatients aged 18–75 years who were diagnosed with primary MN according to renal biopsy prior to glucocorticoids or immunosuppressive therapies in the Department of Nephrology of the Affiliated Hospital of Jiangnan University between January 2010 and December 2023. Exclusion criteria were: secondary MN (n=57), diabetes (n=45), estimated glomerular filtration rate (eGFR) <30 min−1 per 1.73 m2 (n=28), and incomplete data (n=24). A total of 255 MN patients were enrolled for the final analysis, which was close to the estimated sample size. All patients were educated to limit sodium intake and avoid nephrotoxic medications immediately upon diagnosis. This study was approved by the Medical Ethics Committee of the Affiliated Hospital of Jiangnan University (LS2023087).
CLINICAL DATA AND LABORATORY TESTS:
Data on demographic characteristics, including sex and age, were collected at the time of hospitalization. The WHR was measured by trained nurses and calculated by dividing the narrowest point of the waist by the widest point of the hips with a tape measure. Blood pressure was measured with a mercury sphygmomanometer according to the Korotkoff method, and the mean arterial pressure (MAP) was calculated. We collected 24-h urine samples in clean plastic containers, and 24-h urine protein (24 h-UPro) levels were tested via the biuret colorimetric method. Blood was collected from the peripheral vein of patients after they fasted for at least 8 h, and the serum was separated in a refrigerated centrifuge. The serum total protein (TP), albumin (ALB), total cholesterol (T-CHOL), triglyceride (TG), high-density lipoprotein (HDL), low-density lipoprotein (LDL), serum creatinine (SCr), and blood urea nitrogen (BUN) levels were determined via an automatic biochemical analyzer (7180, Hitachi, Ltd., Tokyo, Japan). The eGFR was calculated by using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation [11].
PATHOLOGY:
Renal biopsy was conducted by using a Tru-Cut grooved cutting needle under the guidance of ultrasonography. The fresh renal cortical tissues were separated for pathological and immunopathological examinations. Immunofluorescence was used to stain the tissues for immunoglobulin G (IgG), immunoglobulin A (IgA), immunoglobulin M (IgM), complement C3, and complement C1q, and the intensity of immunofluorescence was classified into 5 grades: 0-negative; 1-trace; 2-mild staining; 3-moderate staining; and 4-strong staining. Tissues were subjected to Masson trichrome staining and periodic acid silver methenamine (PASM)-Masson staining for light microscopy, and the rate of glomerular sclerosis was calculated. Tissues were stained with uranyl acetate and lead citrate for transmission electron microscopy (TEM), and the average foot process width of podocytes was calculated according to the following formula: (π/4) × (∑ glomerular basement membrane length/∑ number of foot processes). All the above pathological examinations were performed by 2 independent renal pathologists.
DEFINITIONS:
Central obesity was defined as a WHR ≥0.9 for men and a WHR ≥0.85 for women. A high normal MAP was defined as a MAP ≥95 mmHg. Massive proteinuria was defined as a 24-h-UPro >3.5 g, and hypoproteinemia was defined as a TP <60 g/L. Hypoalbuminemia was defined as an ALB <30 g/L. Hypercholesteremia was defined as a T-CHOL >6 mmol/L, and hypertriglyceridemia was defined as a TG >1.7 mmol/L. Elevated HDL was defined as HDL >2.07 mmol/L, and elevated LDL was defined as LDL >3.4 mmol/L. Decreased eGFR was defined as eGFR <90 min−1 per 1.73 m2. The presence of glomerular sclerosis was defined as ≥1 sclerotized glomeruli, and severe podocyte injury was defined as severe foot process fusion with an average foot process width >2200 nm.
STATISTICAL ANALYSIS:
Statistical analyses were performed using SPSS 20.0 software (IBM Corporation, Armonk, USA). Measurement data are expressed as the mean and standard deviation, and Student’s or Satterthwaite
Results
MN PATIENTS WITH CENTRAL OBESITY EXHIBIT A MORE SEVERE NEPHROTIC SYNDROME AND PATHOLOGICAL INJURY TO THE KIDNEY:
Among the 255 MN patients enrolled; 54 were diagnosed with central obesity according to the WHR, indicating a 21.18% prevalence of central obesity in MN patients. As shown in Table 1, no statistically significant differences were found in sex or age between central obesity and non-central obesity patients, suggesting consistency in baseline characteristics between the 2 groups. Patients with central obesity manifested more severe nephrotic syndrome, as reflected by higher 24-h-UPro, T-CHOL, TG, HDL, and LDL levels and lower TP and ALB levels than those without central obesity. Renal function tended to be poorer in patients with central obesity, as reflected by the tendency toward higher SCr and BUN levels and lower eGFR. However, these differences were not significant. Additionally, a higher MAP, a potential aggravator of MN, was also observed in the central obesity group. As shown in Table 2, the average podocyte foot process width of patients with central obesity was significantly greater than that of patients without central obesity, suggesting more severe podocyte injury. No significant differences in glomerular IgG, IgA, IgM, C1q, or C3 deposition or glomerular sclerosis were observed between the groups. However, tendencies toward more severe immunoglobulin and complement depositions and sclerosis in the glomeruli were found according to the sample data, and these findings correspond to more severe podocyte injury in the central obesity group. As shown in Table 3, WHR was positively correlated with MAP, 24-h-UPro, T-CHOL, TG, HDL, LDL, and podocyte foot process width and negatively correlated with TP and ALB. These results indicate that MN patients with central obesity tend to have more severe nephrotic syndrome and pathological injury to the kidney.
CENTRAL OBESITY IS A RISK FACTOR FOR MASSIVE PROTEINURIA AND SEVERE PODOCYTE INJURY IN MN PATIENTS:
As massive proteinuria and podocyte injury are prominent features of the clinical and pathological phenotypes of MN, the associations of central obesity with massive proteinuria and severe podocyte injury in MN patients were investigated. As shown in Table 4, both the univariate, adjusted models (models 1, 2) that included potential confounders and multivariable logistic regression models that included all clinical and pathological phenotypes (model 3) all validated that central obesity is a risk factor for massive proteinuria, although central obesity was insufficiently indicated as a risk factor in the stepwise regression analysis. Similarly, central obesity was also a risk factor for severe podocyte injury, as reflected by the univariate, adjusted (models 4 and 5) and multivariable (model 6) logistic regression models. According to the stepwise regression analysis, central obesity remained a risk factor [OR=2.783 (1.329, 5.831)] for severe podocyte injury. The associations between central obesity and other factors relevant to nephrotic syndrome and pathological injuries were also explored via univariate logistic regression models, and we found that central obesity was a risk factor for hypoalbuminemia [OR=2.010 (1.028, 3.928)], hypercholesteremia [OR=2.474 (1.283, 4.770)], hypertriglyceridemia [OR=2.171 (1.138, 4.144)], elevated HDL [OR=5.312 (2.463, 11.457)], and elevated LDL [OR=3.252 (1.666, 6.348)], but was not a risk factor for decreased eGFR [OR=1.530 (0.831, 2.818)] or glomerular sclerosis [OR=1.406 (0.758, 2.608)]. Collectively, these results demonstrate that central obesity is a risk factor for massive proteinuria and severe podocyte injury in MN patients.
Discussion
The current study illustrates that MN patients with central obesity exhibit more severe nephrotic syndrome and podocyte injury, and central obesity is an important risk factor for massive proteinuria and severe podocyte injury in MN patients. Obesity is a chronic metabolic disease characterized by excessive accumulation of fat or adipose tissue in the body [12]. Accumulating evidence has shown that body fat distribution described by the WHR can better predict a series of adverse outcomes than total adiposity as described by BMI [3]. Several mechanisms may account for the unfavorable effects of central obesity on renal injury in MN patients. First, podocytes are vulnerable to ectopic lipid accumulation caused by central obesity, which is defined as lipotoxicity. Lipotoxicity is characterized by mitochondrial oxidative stress, endosomal dyshomeostasis, actin cytoskeleton remodeling, insulin resistance, and an inflammatory response that can result in podocyte hypertrophy, detachment, and death [9,10]. Second, central obesity can activate the renin-angiotensin-aldosterone system (RAAS), and the RAAS increases nicotinamide adenine dinucleotide phosphate oxidase/reactive oxygen species. This increase causes effacement and abnormalities in the slit diaphragm of podocytes and subsequent albuminuria [13]. In addition, angiotensin II, a major RAAS effector, can also directly damage podocytes by promoting metabolic aberrations, cytoskeletal remodeling, and apoptosis [14–16]. Third, central obesity can induce inflammation and oxidative stress, which are partially mediated by cytokines, including tumor necrosis factor-α and interleukin-6, which are secreted from adipose tissue, and not only inflammation and oxidative stress per se but also tumor necrosis factor-α and interleukin-6 can lead to podocyte injury in MN patients [17–20]. Furthermore, sympathetic nervous system activation, renal hemodynamic impairment, and insulin resistance, which are driven by central obesity, can all potentially disturb podocyte homeostasis [21]. Similar to our findings, Shah et al [22] reported that obesity was associated with reduced proteinuria remission in nephrotic syndrome, suggesting a shared pathogenic role of adiposity in glomerular injury across proteinuric diseases.
In MN, immunological conflict results in pathophysiological disturbance of the podocyte, followed by immune complex deposition and complement activation [2]. Loss of immune tolerance, genetic factors, and environmental factors are all potential etiopathogeneses for such an immunologic disorder [2]. No significant associations between central obesity and immune complex deposition or complement activation in the glomeruli were detected in our study. The effect of central obesity on autoimmune processes in MN remains unclear, and the dysregulated adipokines released from adipose tissue may be potential intermediaries between obesity and immune system functions, resulting in disorders of immune tolerance and subsequent autoimmune responses [23]. These findings might explain the tendencies toward more severe glomerular immunoglobulin and complement deposition in patients with central obesity, as indicated by the sample data.
We found that the prevalence of central obesity in individuals with MN was 21.18%, which is higher than the 16.79% prevalence in Chinese adults and lower than the 41.5% in adults worldwide [4,5]. These discrepancies may be attributed to differences in ethnicities, measurement standards and health conditions among the cohorts included in various investigations. The prevalence of central obesity in CKD stage 3–5 patients is 49%, and such high rates may be related to the more severe lipid metabolism disorders in advanced CKD patients than in MN patients [24]. Larger epidemiological studies are needed to investigate the prevalence of central obesity in MN patients.
The study has several limitations. First, the single-center design may restrict the generalizability of findings across diverse populations. Second, the cross-sectional nature precludes causal inference between adiposity measures and MN outcomes. Third, the lack of adipokine profiling limits elucidation of underlying mechanistic pathways. Prospective cohort studies are needed to evaluate whether lifestyle intervention-induced WHR reduction confers clinical benefits in MN management.
Conclusions
MN patients complicated with central obesity exhibited more severe nephrotic syndrome and podocyte injury. Central obesity is a risk factor for massive proteinuria and severe podocyte injury in MN patients. These findings highlight the adverse impact of abdominal adiposity on MN progression and underscore the clinical significance of weight management in nephrotic syndrome care.
Tables
Table 1. Clinical phenotypes of the enrolled patients.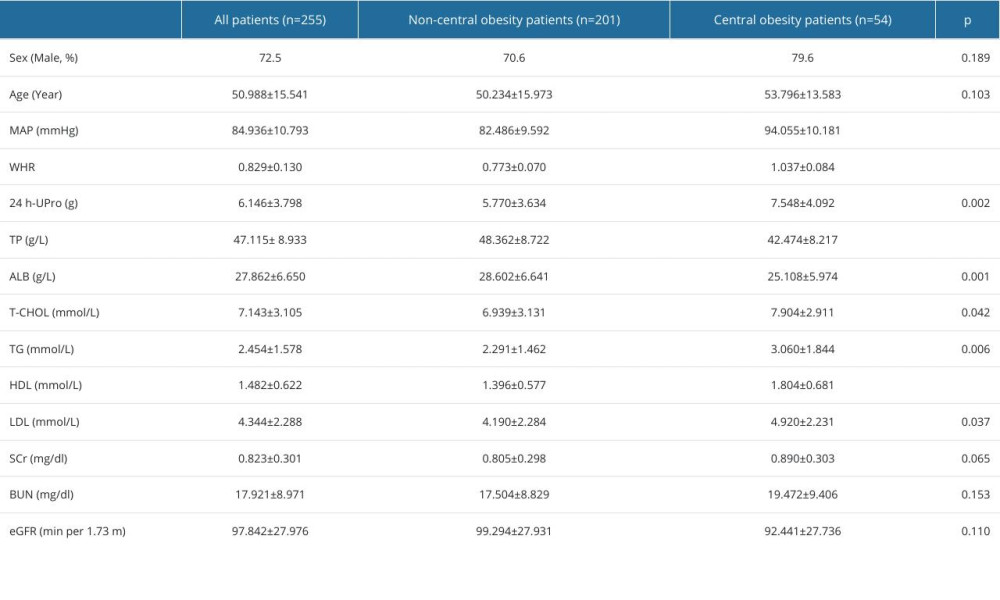 Table 2. Pathological phenotypes of the enrolled patients.
Table 2. Pathological phenotypes of the enrolled patients. Table 3. Correlation between WHR and clinical/pathological phenotypes of the enrolled patients.
Table 3. Correlation between WHR and clinical/pathological phenotypes of the enrolled patients.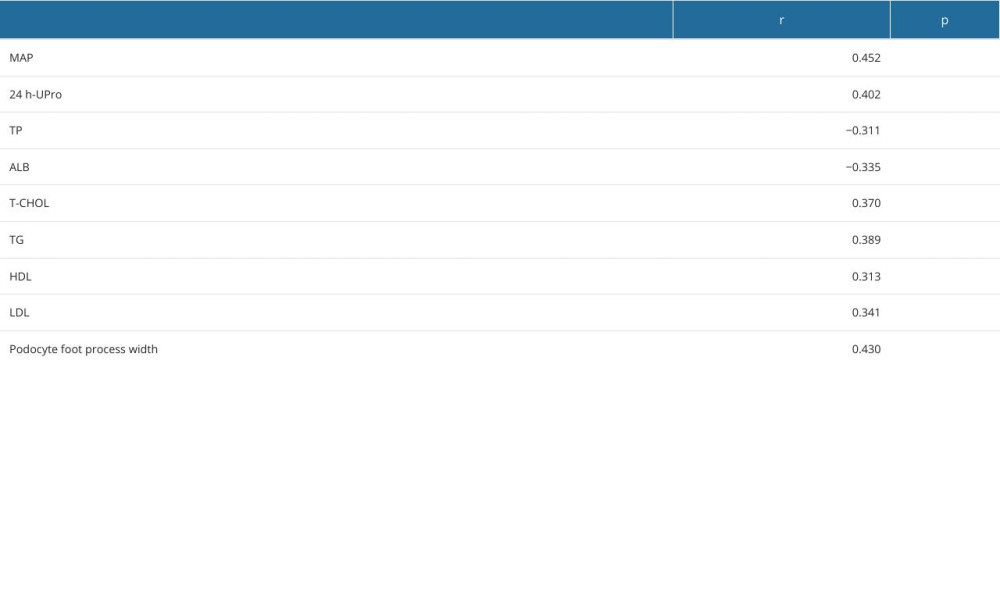 Table 4. Logistic regression analysis of the associations of central obesity with massive proteinuria and severe podocyte injury in MN patients.
Table 4. Logistic regression analysis of the associations of central obesity with massive proteinuria and severe podocyte injury in MN patients.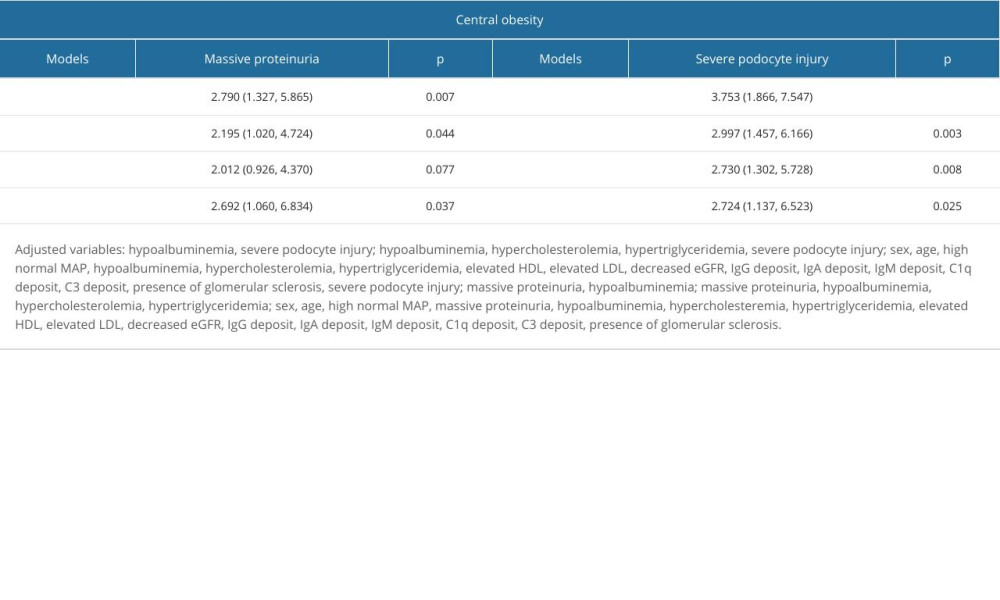
References
1. Downie ML, Gupta S, Tekman MC, Identification of a locus on the X chromosome linked to familial membranous nephropathy: Kidney Int Rep, 2021; 6(6); 1669-76
2. Hoxha E, Reinhard L, Stahl RAK, Membranous nephropathy: New pathogenic mechanisms and their clinical implications: Nat Rev Nephrol, 2022; 18(7); 466-78
3. Zhang Y, Chen GC, Sotres-Alvarez D, General or central obesity and mortality among US Hispanic and Latino adults: JAMA Network Open, 2024; 7(1); e2351070
4. Zhou L, Cao D, Si Y, Income-related inequities of adult obesity and central obesity in China: Evidence from the China Health and Nutrition Survey 1997–2011: BMJ Open, 2020; 10(10); e034288
5. Wong MCS, Huang J, Wang J, Global, regional and time-trend prevalence of central obesity: A systematic review and meta-analysis of 13.2 million subjects: Eur J Epidemiol, 2020; 35(7); 673-83
6. Shen FC, Chiu YW, Kuo MC, U-shaped association between waist-to-hip ratio and all-cause mortality in stage 3–5 chronic kidney disease patients with body mass index paradox: J Pers Med, 2021; 11(12); 1355
7. Garofalo C, Borrelli S, Minutolo R, A systematic review and meta-analysis suggests obesity predicts onset of chronic kidney disease in the general population: Kidney Int, 2017; 91(5); 1224-35
8. Bellizzi V, Annunziata G, Albanese A, Approaches to patients with obesity and CKD: focus on nutrition and surgery: Clin Kidney J, 2024; 17(Suppl 2); 51-64
9. Sun Y, Cui S, Hou Y, Yi F, The updates of podocyte lipid metabolism in proteinuric kidney disease: Kidney Dis (Basel), 2021; 7(6); 438-51
10. Hasegawa S, Nangaku M, Takenaka Y, Organelle communication maintains mitochondrial and endosomal homeostasis during podocyte lipotoxicity: JCI Insight, 2024; 9(18); e182534
11. Levey AS, Stevens LA, Schmid CH, A new equation to estimate glomerular filtration rate: Ann Intern Med, 2009; 150(9); 604-12
12. Zhang Z, Wang J, Lin Y, Nutritional activities of luteolin in obesity and associated metabolic diseases: An eye on adipose tissues: Crit Rev Food Sci Nutr, 2024; 64(12); 4016-30
13. Sowers JR, Metabolic risk factors and renal disease: Kidney Int, 2007; 71(8); 719-20
14. Ha TS, Seong SB, Ha DS, Kim SJ, Upregulation of NADH/NADPH oxidase 4 by angiotensin II induces podocyte apoptosis: Kidney Res Clin Pract, 2023; 42(2); 202-15
15. Luo Z, Chen Z, Zhu Z, Angiotensin II induces podocyte metabolic reprogramming from glycolysis to glycerol-3-phosphate biosynthesis: Cell Signal, 2022; 99; 110443
16. Ma Y, Yang Q, Zhong Z, Role of c-Abl and nephrin in podocyte cytoskeletal remodeling induced by angiotensin II: Cell Death Dis, 2018; 9(2); 185
17. Scurt FG, Ganz MJ, Herzog C, Association of metabolic syndrome and chronic kidney disease: Obes Rev, 2024; 25(1); e13649
18. Zhao Q, Dai H, Jiang H, Activation of the IL-6/STAT3 pathway contributes to the pathogenesis of membranous nephropathy and is a target for Mahuang Fuzi and Shenzhuo Decoction (MFSD) to repair podocyte damage: Biomed Pharmacother, 2024; 174; 116583
19. Liu B, Lu R, Li H, Zhen-wu-tang ameliorates membranous nephropathy rats through inhibiting NF-κB pathway and NLRP3 inflammasome: Phytomedicine, 2019; 59; 152913
20. Luo Z, Chen Z, Hu J, Ding G, Interplay of lipid metabolism and inflammation in podocyte injury: Metabolism, 2024; 150; 155718
21. Al-Chalabi S, Syed AA, Kalra PA, Sinha S, Mechanistic links between central obesity and cardiorenal metabolic diseases: Cardiorenal Med, 2024; 14(1); 12-22
22. Shah PP, Brady TM, Meyers KEC, Association of obesity with cardiovascular risk factors and kidney disease outcomes in primary proteinuric glomerulopathies: Nephron, 2021; 145(3); 245-55
23. Carbone F, La Rocca C, De Candia P, Metabolic control of immune tolerance in health and autoimmunity: Semin Immunol, 2016; 28(5); 491-504
24. Ge M, Fontanesi F, Merscher S, Fornoni A, The vicious cycle of renal lipotoxicity and mitochondrial dysfunction: Front Physiol, 2020; 11; 732
Tables
Table 1. Clinical phenotypes of the enrolled patients.Table 2. Pathological phenotypes of the enrolled patients.Table 3. Correlation between WHR and clinical/pathological phenotypes of the enrolled patients.Table 4. Logistic regression analysis of the associations of central obesity with massive proteinuria and severe podocyte injury in MN patients. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387