10 July 2025: Clinical Research
Incremental Prognostic Value of Right and Left Atrial Volume Indices for Predicting Cardiovascular Outcomes in Atrial Fibrillation: A Cohort Study
Ferit Böyük DOI: 10.12659/MSM.948798
Med Sci Monit 2025; 31:e948798






Abstract
BACKGROUND: Atrial fibrillation (AF) is a common arrhythmia associated with high morbidity and mortality. While the left atrial volume index (LAVI) is a known prognostic marker, the right atrial volume index (RAVI) in this setting remains less well defined. This study aimed to investigate the incremental prognostic value of the RAVI alongside the LAVI in predicting adverse cardiovascular outcomes in patients with AF, a common arrhythmia associated with increased morbidity and mortality.
MATERIAL AND METHODS: A retrospective cohort study was conducted involving 421 patients with non-valvular AF. Patients were classified based on the occurrence of adverse events, including hospitalization for heart failure, stroke, and all-cause mortality. Echocardiographic assessments of LAVI and RAVI were performed according to international guidelines.
RESULTS: Among the 421 patients, 180 (43%) experienced adverse events. Enlargement of both LAVI and RAVI was significantly associated with death, stroke, and heart failure (P<0.001). In multivariate analysis adjusted for age and sex, LAVI and RAVI were independent predictors of adverse outcomes. The presence of either LAVI or RAVI enlargement was associated with increased mortality (HR=1.96, 95% CI: 1.17-3.31), while the combined enlargement of both indices further increased the risk (HR=4.38, 95% CI: 2.71-7.08). Similar patterns were observed for stroke and heart failure, where the combination of both enlarged indices significantly amplified risk.
CONCLUSIONS: RAVI adds significant incremental prognostic value to LAVI in patients with AF. Combined assessment of both atrial volume indices enhances risk stratification for heart failure, stroke, and mortality, supporting more personalized treatment approaches in clinical practice.
Keywords: Atrial Fibrillation, Echocardiography, Echocardiography, Doppler, Cardiac Volume, Humans, Male, Female, Prognosis, Heart Atria, Aged, Retrospective Studies, Middle Aged, Cohort Studies, Heart Failure, Risk Factors, Stroke
Introduction
Atrial fibrillation (AF), the most common sustained arrhythmia worldwide, is strongly associated with adverse cardiovascular outcomes. Left atrial (LA) enlargement, frequently observed in AF, is a well-established prognostic marker linked to increased risk of stroke, heart failure, and mortality [1–3].
Although LAVI has been widely recognized as a prognostic marker, emerging evidence suggests that RAVI may also carry prognostic value, particularly in patients with systolic and diastolic heart failure, as well as pulmonary hypertension [4–6]. In AF, right atrial (RA) enlargement is commonly observed and has been linked to clinical symptoms and adverse hemodynamic consequences [7]. However, the prognostic significance of RA enlargement in patients with AF remains less defined. Few studies have examined the independent and incremental contribution of RAVI in this population [8,9].
This study aims to evaluate whether RAVI provides incremental prognostic value beyond LAVI in predicting adverse cardiovascular outcomes in patients with AF. We hypothesized that combined assessment of LA and RA volumes may offer a more comprehensive view of atrial remodeling and improve risk stratification for stroke, heart failure, and mortality. These insights could support more personalized treatment strategies and enhance patient outcomes.
Material and Methods
STUDY DESIGN AND POPULATION:
This retrospective cohort study aimed to investigate the relationship between RAVI and clinical outcomes in patients diagnosed with AF and to identify potential risk factors associated with adverse outcomes in this patient population. Approval for the study was obtained from the University of Hong Kong’s Institutional Review Board (IRB No: UW 21-224). The study population included adult patients diagnosed with non-valvular AF between January 2008 and December 2020. As shown in the flowchart (Figure 1), of the initial cohort patients, those with valvular AF were excluded, as were patients who lacked echocardiography records for LAVI or RAVI. Patients who did not have sufficient follow-up data or whose outcomes were unrelated to cardiovascular disease were also excluded. Patients with missing echocardiographic or follow-up data were excluded from the final analysis. No data imputation techniques were applied. It resulted in a final cohort of patients with both LAVI and RAVI measurements available, from which only those who experienced at least 1 outcome of interest were included in the analysis.
DATA COLLECTION AND ECHOCARDIOGRAPHIC ASSESSMENT:
Relevant clinical history and all variables were extracted from electronic medical records. LAVI was calculated from LA volume measurements taken from standard apical four-chamber views at end-systole, just before the mitral valve (MV) opening, and was indexed to body surface area (BSA) in square meters. RAVI was similarly calculated from RA volume measurements obtained from standard apical four-chamber views at end-systole, just before the tricuspid valve (TV) opening, and indexed to BSA.
Baseline characteristics were collected to assess their potential influence on outcomes. These baseline variables included age, sex, body mass index (BMI, kg/m2), BSA, medication use (eg, anticoagulants, digoxin, ACE inhibitors, ARBs, calcium channel blockers, diuretics, and beta-blockers), and comorbid conditions such as hypertension, diabetes mellitus, hyperlipidemia, and smoking status. Additional baseline echocardiographic parameters included left ventricular ejection fraction (LVEF), left ventricular end-systolic dimension (LVESD), left ventricular end-diastolic dimension (LVEDD), tricuspid valve regurgitant systolic peak velocity (TVmax), RAVI, and LAVI.
Experienced echocardiographers performed comprehensive transthoracic echocardiograms using commercially available ultrasound machines (General Electric Vivid E9 and E95, General Electric Healthcare; Philips IE 33 and EPIQ, Philips). The measurements adhered to the American Society of Echocardiography guidelines and the European Association of Cardiovascular Imaging. RAVI was determined using the Simpson method from apical four-chamber views, while LAVI was calculated using the biplane disk summation method from both four-chamber and two-chamber views. The LA volumes excluded the pulmonary vein ostia and the left atrial appendage. Two independent researchers blinded to the patient’s clinical outcomes performed all measurements.
STUDY PARTICIPANTS:
The final analysis included 421 AF patients admitted to the hospital between January 2008 and December 2020. Patients were stratified into 2 groups based on clinical outcomes: those without adverse outcomes (n=241) and those with at least 1 adverse outcome (n=180). Adverse outcomes were defined as stroke, heart failure, or death during the follow-up period.
OUTCOME MEASURES:
Follow-up data were collected from the centralized inter-hospital patient management system in Hong Kong. The mean follow-up duration was 8.1±2.9 years. The primary outcome was a composite endpoint, including hospitalizations due to heart failure, incidence of stroke, and all-cause mortality, whichever came first. Hospitalization for heart failure was defined as a clinical syndrome necessitating a minimum of 1 overnight hospital stay and the presence of at least 2 of the following signs or symptoms: paroxysmal nocturnal dyspnea, orthopnea, elevated jugular venous pressure, pulmonary rales, third heart sound, cardiomegaly on chest X-ray, or pulmonary edema on lung imaging.
STATISTICAL ANALYSIS:
Analysis was conducted using MEDCALCv.20.022 and SPSS-v25 software. The study divided patients into 2 groups based on outcomes: “Patients with Outcome” and “Patients without Outcome”. The “Patients with Outcome” group included individuals who experienced the composite event. The normality of the data distribution was assessed using the Shapiro-Wilk test. Since the continuous data did not follow a normal distribution, the Mann-Whitney U test was used to compare groups. Categorical variables were compared using the chi-square test. Receiver operating characteristic (ROC) analysis was conducted to determine cut-off values for the variables. The Youden J index was used to identify optimal cut-off points and risk factors through univariate chi-square tests. Variables that showed significance in the univariate analysis were further examined using multivariable logistic regression analysis to identify independent risk factors, with corresponding OR values reported. Survival analysis was performed using the Kaplan-Meier method to estimate survival probabilities, and differences in survival times between groups were assessed using the log-rank test. Cox proportional hazards regression was used to investigate risk factors affecting survival times, with hazard ratios (HR) provided for each variable. Multivariable Cox regression models were adjusted for potential confounding variables, including age, sex, and clinical comorbidities. Based on the RAVI and LAVI cut-off values, patients were further classified into 3 subgroups: “Group 1” (1) if both RAVI and LAVI were below their respective cut-offs, “Group 2” (2) if either RAVI or LAVI exceeded the cut-off, and “Group 3” (3) if both values surpassed the cut-offs.
Results
DEMOGRAPHIC AND CLINICAL CHARACTERISTICS:
Patients with AF who experienced adverse outcomes were older compared to those without outcomes (78 vs 67 years; p<0.001), with similar sex distribution between groups (
ROC FOR PREDICTING OUTCOMES:
In analyzing the cut-off values for predicting outcomes (Table 1), LAVI showed strong predictive power, with an AUC of 0.762 (95% CI: 0.718–0.802, P<0.001). The optimal cut-off for LAVI, a cut-off of >51.88 ml/m2 achieved a sensitivity of 64.44% and specificity of 82.57%. RAVI also emerged as a notable predictor with an AUC of 0.682 (95% CI: 0.635–0.726, P<0.001) and a cut-off value of >41.67 ml/m2, providing a sensitivity of 52.78% and specificity of 83.4%. The left ventricular end-diastolic volume (LVEDV) and left ventricular ejection fraction (LVEF) parameters were significant but demonstrated lower predictive performance, with AUCs of 0.572 and 0.623, respectively. Parameters such as left ventricular end-systolic volume (LVESV) and left atrial volume indices/right atrial volume indices (LAVI/RAVI) ratio did not demonstrate predictive value.
LOGISTIC REGRESSION ANALYSIS:
In the univariable analysis, age over 74 years was a strong predictor of adverse outcomes, with an OR of 6.58 (95% CI: 4.27–10.15,
In the univariable analysis, other significant predictors of adverse outcomes included LVEDV >79 ml (OR: 2.20, 95% CI: 1.43–3.38, P<0.001) and RAVI >41.67 ml/m2 (OR: 5.62, 95% CI: 3.59–8.79, P<0.001). In the multivariable analysis, significant predictors included LAVI >51.88 ml/m2 (OR: 3.05, 95% CI: 1.67–5.54, P<0.001), LVEF ≤60% (OR: 2.24, 95% CI: 1.26–3.97, P=0.006), and RAVI >41.67 ml/m2 (OR: 2.95, 95% CI: 1.61–5.41, P<0.001). Variables such as smoking, sex, and the remaining echocardiographic parameters did not retain significance in the multivariable model (Table 2).
SURVIVAL ANALYSIS:
The study analyzed survival times for death, stroke, and heart failure based on LAVI and RAVI. Patients in Group 1, without elevated bi-atrial indices, showed the best survival for all outcomes, while those in Group 3, with both elevated indices, had the worst prognosis. For death (Figure 2), the mean survival was 9.23±0.15 years for Group 1, 8.29±0.29 years for Group 2, and 6.43±0.36 years for Group 3 (P<0.001, Table 3). Regarding stroke (Figure 3), the mean survival time was 10.31±0.26 years for Group 1, 10.57±0.51 years for Group 2, and 9.78±0.53 years for Group 3 (P<0.001). Pairwise comparisons revealed significant differences between Group 1 vs Group 2 (p=0.006), Group 1 vs Group 3 (P<0.001), and Group 2 vs Group 3 (P=0.038). For heart failure (Figure 4), the mean survival time was 9.31±0.14 years for Group 1, 7.84±0.32 years for Group 2, and 6.72±0.44 years for Group 3 (P<0.001). Significant differences were observed in pairwise comparisons among all groups, with Group 1 vs Group 2 (P<0.001), Group 1 vs Group 3 (P<0.001), and Group 2 vs Group 3 (P=0.001).
MULTIVARIABLE ANALYSIS:
Multivariable analysis for death (Table 3) demonstrated that an elevated atrial index (either LAVI or RAVI) was associated with a significantly higher risk of death, with a hazard ratio (HR) of 2.43 (95% CI: 1.46–4.08, P=0.001). The risk was even higher for patients with elevation of both LAVI and RAVI, with an HR of 6.07 (95% CI: 3.85–9.58, P<0.001). When age and sex were included in the model, the risk of death for patients with 1 elevated index decreased slightly but remained significant, with an HR of 1.96 (95% CI: 1.17–3.31, P =0.011). The risk for those with both elevated indices was lower than the model, excluding age and sex, with an HR of 4.38 (95% CI: 2.71–7.08, P<0.001).
While excluding age and sex, multivariable analysis for stroke (Table 3) demonstrated that elevation of either atrial index was associated with an HR of 3.14 (95% CI: 1.43–6.88, P=0.004). The risk was higher for patients with both elevated indices, with an HR of 5.74 (95% CI: 2.75–12, P<0.001). With age and sex included, the HR for stroke in the elevation of either 1 index was 2.56 (95% CI: 1.17–5.63, P=0.019), and for those with elevation of both indices, HR was 3.91 (95% CI: 1.82–8.41, P<0.001). Age remained a predictor, with an HR of 1.06 per year increase (95% CI: 1.03–1.09, P<0.001), while sex was not significant (HR: 0.77, 95% CI: 0.44–1.37, P=0.382).
In the analysis of heart failure (Table 3), excluding age and sex, having 1 elevated atrial index resulted in an HR of 4.00 (95% CI: 2.25–7.13, P<0.001), while having both elevated indices resulted in a substantially higher risk with an HR of 8.20 (95% CI: 4.79–14.06, P<0.001). When age and sex were added to the model, the risk for 1 elevated index was an HR of 3.46 (95% CI: 1.93–6.21, P<0.001), and for both elevated indices, the HR was 6.29 (95% CI: 3.58–11, P<0.001). Age remained a significant factor with an HR of 1.03 per year increase (95% CI: 1.01–1.05, P=0.002). However, sex did not affect the outcome (HR: 1.06, 95% CI: 0.71–1.59, P=0.774).
Discussion
CLINICAL IMPLICATIONS:
This study underscores the prognostic significance of incorporating both LA and RA volumes in the clinical management of patients with non-valvular AF. By assessing both atrial volumes, our findings suggest that a more comprehensive approach to risk stratification can be achieved, ultimately enhancing clinical decision-making. Given the reproducibility and ease of measurement of RAVI, its inclusion alongside LAVI holds substantial promise for improving prognostic accuracy in predicting adverse cardiovascular outcomes, including stroke, heart failure, and mortality.
Our results indicate that concurrent enlargement of both LA and RA volumes is associated with a heightened risk of adverse clinical events. In such cases, more intensive medical management and closer clinical monitoring may be warranted to mitigate the risk of poor outcomes. Incorporating both LAVI and RAVI into routine clinical assessments could allow for more precise identification of high-risk patients, enabling targeted therapeutic interventions.
Furthermore, our findings can be integrated into existing risk models to enhance predictive accuracy. By adding both LAVI and RAVI to these models, clinicians could refine the identification of high-risk individuals, leading to more personalized treatment strategies. These enhanced models would not only offer individualized care but also facilitate the proactive management of potential complications in patients with non-valvular AF.
Future studies are warranted to prospectively validate the prognostic utility of RAVI in larger and more diverse AF populations. In particular, integrating RAVI into existing clinical risk stratification tools such as the CHA2DS2-VA score may enhance their predictive accuracy. Such incorporation could improve the identification of high-risk individuals and support more personalized, evidence-based treatment strategies.
LIMITATIONS:
This study has several limitations that should be acknowledged. The retrospective design inherently limits the ability to infer causality between atrial volume indices and clinical outcomes. Additionally, the single-center nature of the study, along with the relatively modest sample size, may limit the generalizability of the findings to broader patient populations. Although multiple potential confounders were controlled for, the influence of unmeasured variables remains a limitation, and the potential for model overfitting cannot be excluded. These factors should be considered when interpreting the conclusions of the study.
Conclusions
Our study demonstrates that the combined assessment of bi-atrial volumes provides incremental prognostic value in predicting adverse cardiovascular outcomes in patients with AF. By incorporating both LAVI and RAVI into clinical risk models, healthcare providers can achieve more accurate risk stratification, which can ultimately lead to more personalized and effective management strategies. These findings underscore the potential for more informed clinical decision-making and improved patient outcomes. Future prospective studies with larger cohorts are needed to validate and expand upon these findings, particularly with regard to integrating bi-atrial volume indices into broader risk models for AF-related complications.
Figures
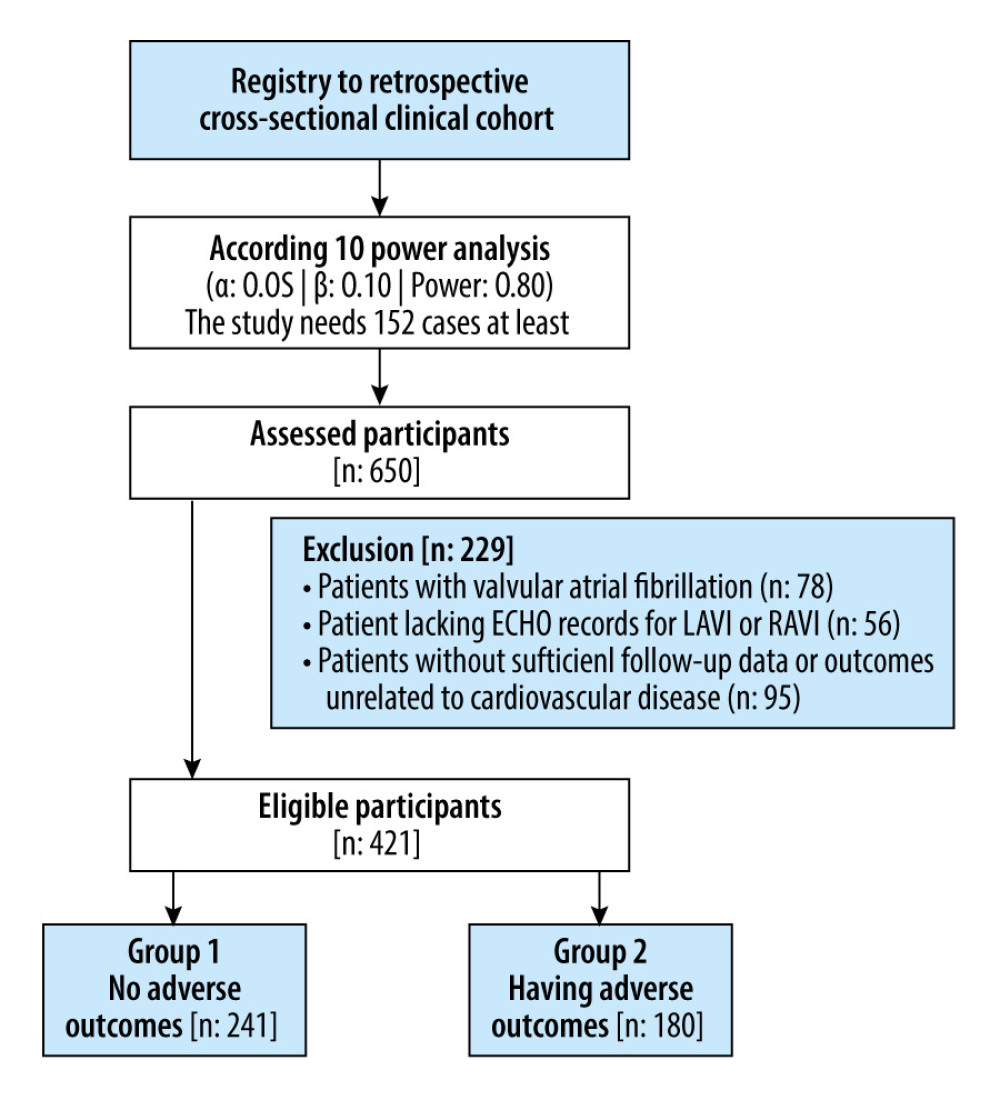 Figure 1. Patient selection flowchart.
Figure 1. Patient selection flowchart. 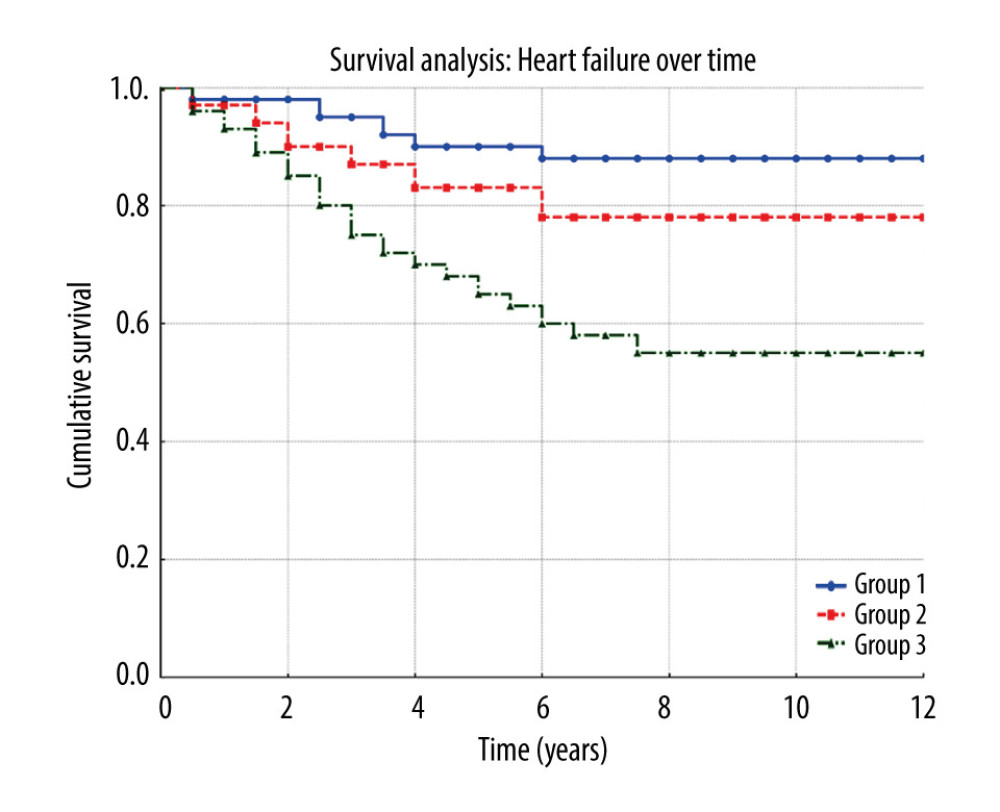 Figure 2. Heart failure survival over time. Kaplan-Meier plot shows cumulative survival probabilities for patients grouped by LAVI and RAVI status: no difference between the 2 groups (Group 1), 1 atrial enlargement (Group 2), and both atrial enlargement (Group 3).
Figure 2. Heart failure survival over time. Kaplan-Meier plot shows cumulative survival probabilities for patients grouped by LAVI and RAVI status: no difference between the 2 groups (Group 1), 1 atrial enlargement (Group 2), and both atrial enlargement (Group 3). 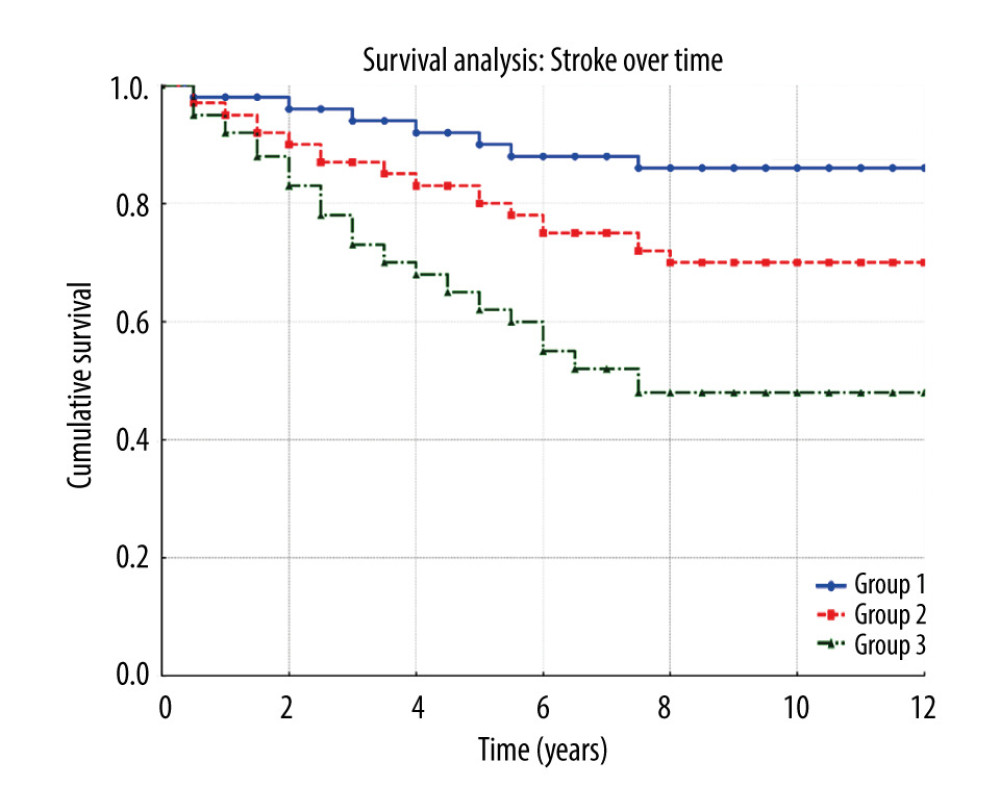 Figure 3. Stroke survival over time. Kaplan-Meier plot displays survival probabilities for patients based on LAVI and RAVI status: no difference between 2 groups (Group 1), 1 atrial enlargement (Group 2), and both atrial enlargement (Group 3).
Figure 3. Stroke survival over time. Kaplan-Meier plot displays survival probabilities for patients based on LAVI and RAVI status: no difference between 2 groups (Group 1), 1 atrial enlargement (Group 2), and both atrial enlargement (Group 3). 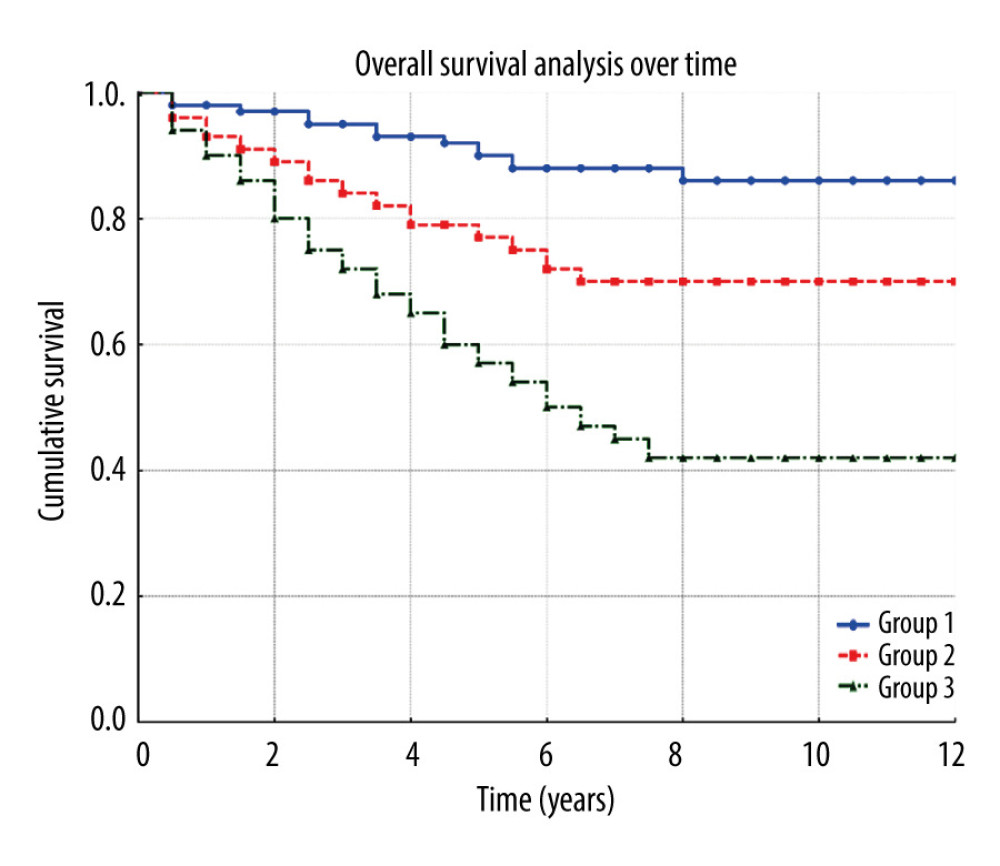 Figure 4. Overall survival over time. Kaplan-Meier plot presents survival probabilities over time for patients categorized by LAVI and RAVI status: no difference between the 2 groups (Group 1), 1 atrial enlargement (Group 2), and both atrial enlargement (Group 3).
Figure 4. Overall survival over time. Kaplan-Meier plot presents survival probabilities over time for patients categorized by LAVI and RAVI status: no difference between the 2 groups (Group 1), 1 atrial enlargement (Group 2), and both atrial enlargement (Group 3). References
1. Anter E, Jessup M, Callans DJ, Atrial fibrillation and heart failure: Treatment considerations for a dual epidemic: Circulation, 2009; 119(18); 2516-25
2. Benjamin E, D’Agostino R, Belanger A, Left atrial size and the risk of stroke and death: The Framingham Heart Study: ACC Current Journal Review, 1996; 1(5); 54
3. Zhang S, Zuo P, Obesity-hyperlipidemia, hypertension, and left atrial enlargement during stroke in young adults: Neurologist, 2023; 28(6); 386-90
4. Mantziari L, Kamperidis V, Ventoulis I, Increased right atrial volume index predicts low Duke activity status index in patients with chronic heart failure: Hellenic J Cardiol, 2013; 54(1); 32-38
5. Kizer JR, Bella JN, Palmieri V, Left atrial diameter as an independent predictor of first clinical cardiovascular events in middle-aged and elderly adults: The Strong Heart Study (SHS): American heart journal, 2006; 151(2); 412-18
6. Cioffi G, de Simone G, Mureddu G, Right atrial size and function in patients with pulmonary hypertension associated with disorders of respiratory system or hypoxemia: Eur J Echocardiogr, 2007; 8(5); 322-31
7. Ko K-Y, Jang J-H, Choi S-H, Impact of right atrial enlargement on clinical outcome in patients with atrial fibrillation: Front Cardiovasc Med, 2022; 9; 989012
8. Ebtia M, Murphy D, Gin K, Best method for right atrial volume assessment by two-dimensional echocardiography: validation with magnetic resonance imaging: Echocardiography, 2015; 32(5); 734-39
9. Akutsu Y, Kaneko K, Kodama Y, Association between left and right atrial remodeling with atrial fibrillation recurrence after pulmonary vein catheter ablation in patients with paroxysmal atrial fibrillation: A pilot study: Circ Cardiovasc Imaging, 2011; 4(5); 524-31
10. Kuperstein R, Blechman I, Zekry SB, Reverse remodeling and the mechanism of mitral regurgitation improvement in patients with dilated cardiomyopathy: Cardiol J, 2015; 22(4); 391-96
11. Xiang H, Xue Y, Chen Z, The association between left ventricular hypertrophy and the occurrence and prognosis of atrial fibrillation: A meta-analysis: Front Cardiovasc Med, 2021; 8; 639993
12. Hoit BD, Left atrial size and function: Role in prognosis: J Am Coll Cardiol, 2014; 63(6); 493-505
13. Lang RM, Badano LP, Mor-Avi V, Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging: Eur Heart J Cardiovasc Imaging, 2015; 16(3); 233-71
14. Pathak R, Lau DH, Mahajan R, Sanders P, Structural and functional remodeling of the left atrium: clinical and therapeutic implications for atrial fibrillation: J Atr Fibrillation, 2013; 6(4); 986
15. Xu X, Zhou Q, Ren C, Evaluation of patients with angiographically-confirmed coronary artery disease to investigate the association between epicardial fat thickness and atrial fibrillation: Med Sci Monit, 2022; 28; e936446
16. Luong C, Thompson DJ, Bennett M, Right atrial volume is superior to left atrial volume for prediction of atrial fibrillation recurrence after direct current cardioversion: Can J Cardiol, 2015; 31(1); 29-35
17. Gosselink AM, Crijns HJ, Hamer HP, Changes in left and right atrial size after cardioversion of atrial fibrillation: role of mitral valve disease: J Am Coll Cardiol, 1993; 22(6); 1666-72
18. Moon J, Hong YJ, Shim J, Right atrial anatomical remodeling affects early outcomes of nonvalvular atrial fibrillation after radiofrequency ablation: Circ J, 2012; 76(4); 860-67
19. Sallach JA, Tang WW, Borowski AG, Right atrial volume index in chronic systolic heart failure and prognosis: JACC Cardiovasc Imaging, 2009; 2(5); 527-34
20. Heidenreich PA, Bozkurt B, Aguilar D, 2022 AHA/ACC/HFSA guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines: J Am Coll Cardiol, 2022; 79(17); e263-e421
21. Letnes JM, Eriksen-Volnes T, Nes B, Variability of echocardiographic measures of left ventricular diastolic function. The HUNT study: Echocardiography, 2021; 38(6); 901-8
Figures
Figure 1. Patient selection flowchart.Figure 2. Heart failure survival over time. Kaplan-Meier plot shows cumulative survival probabilities for patients grouped by LAVI and RAVI status: no difference between the 2 groups (Group 1), 1 atrial enlargement (Group 2), and both atrial enlargement (Group 3).Figure 3. Stroke survival over time. Kaplan-Meier plot displays survival probabilities for patients based on LAVI and RAVI status: no difference between 2 groups (Group 1), 1 atrial enlargement (Group 2), and both atrial enlargement (Group 3).Figure 4. Overall survival over time. Kaplan-Meier plot presents survival probabilities over time for patients categorized by LAVI and RAVI status: no difference between the 2 groups (Group 1), 1 atrial enlargement (Group 2), and both atrial enlargement (Group 3). Tables
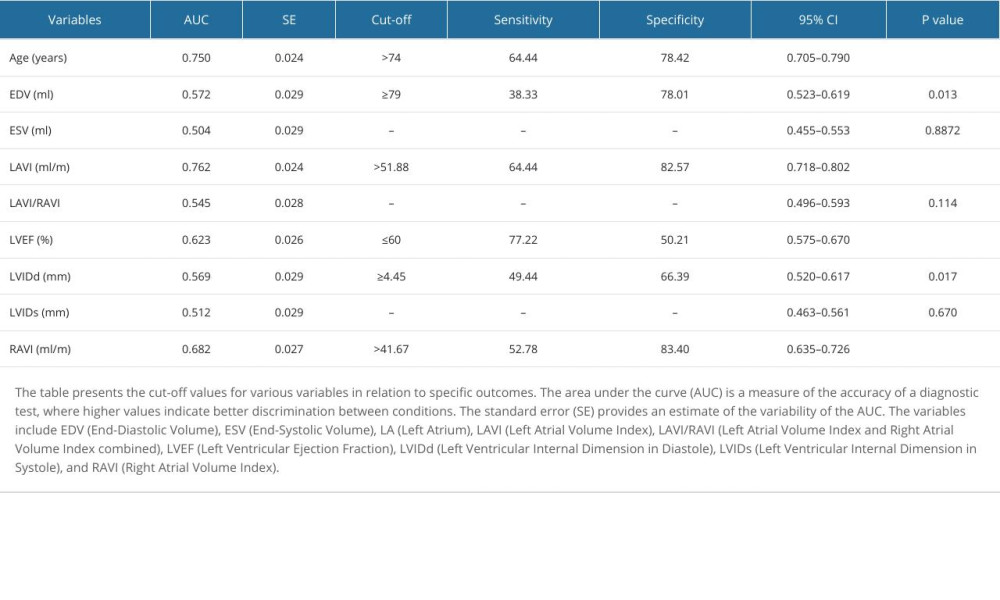 Table 1. Cut-off values according to specific outcomes.
Table 1. Cut-off values according to specific outcomes.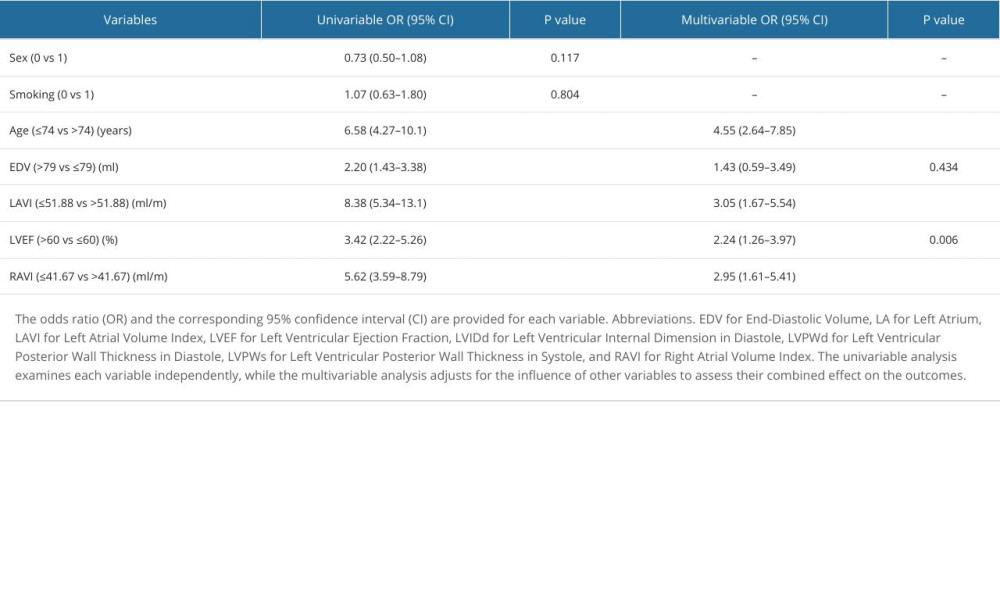 Table 2. Univariable and multivariable logistic regression analysis for predicting outcomes.
Table 2. Univariable and multivariable logistic regression analysis for predicting outcomes.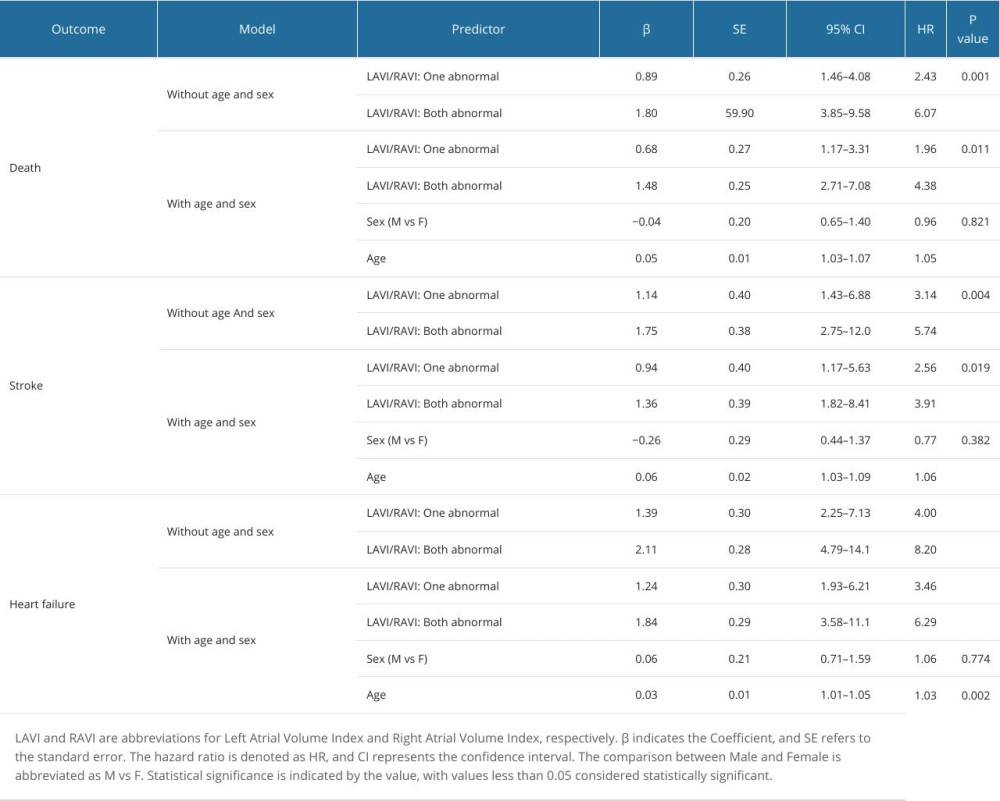 Table 3. Cox analysis for death, stroke, and heart failure.Table 1. Cut-off values according to specific outcomes.Table 2. Univariable and multivariable logistic regression analysis for predicting outcomes.Table 3. Cox analysis for death, stroke, and heart failure.
Table 3. Cox analysis for death, stroke, and heart failure.Table 1. Cut-off values according to specific outcomes.Table 2. Univariable and multivariable logistic regression analysis for predicting outcomes.Table 3. Cox analysis for death, stroke, and heart failure. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387