17 December 2020: Review Articles
Current Status of Diagnostic Testing for SARS-CoV-2 Infection and Future Developments: A Review
Jing Gao12ABCEF, Lei Quan1AEF*DOI: 10.12659/MSM.928552
Med Sci Monit 2020; 26:e928552






Abstract
ABSTRACT: The coronavirus disease 2019 (COVID-19) caused by a novel coronavirus, SARS-CoV-2, has infected more than 50.6 million individuals and caused over 1.2 million deaths globally, raising a major health concern. To date, no specific antiviral treatment or vaccine for COVID-19 has been approved by the Food and Drug Administration (FDA). Highly sensitive and specific laboratory diagnostics are therefore critical for controlling the rapidly evolving COVID-19 pandemic and optimizing clinical care, infection control, and public health interventions. The FDA has issued emergency use authorization (EUA) for hundreds of COVID-19 diagnostic tests of different classes. Whereas nucleic acid testing (NAT) such as RT-PCR remains the criterion standard for COVID-19 diagnosis, serological antibody and antigen tests are increasingly being developed. Tests based on the novel RNA sensing techniques (e.g., SHERLOCK, DETECTR, and Toehold Switch) are promising due to their relatively low cost, high accuracy, and rapid detection time. Diagnostic testing results for SARS-CoV-2 should be interpreted with caution, since they depend heavily on factors such as viral load, virus replication, the source and timing of sample collection, sample extraction, and characteristics of various testing methods. This review aims to present the current status of common diagnostic testing for SARS-CoV-2 infection, review the current regulatory requirements, and identify future directions in the development of improved diagnostics that are more accurate, accessible, and rapid.
Keywords: clustered regularly interspaced short palindromic repeats, COVID-19, Early Diagnosis, Molecular Diagnostic Techniques, COVID-19, COVID-19 Testing, COVID-19 Vaccines, Clinical Laboratory Techniques, Diagnostic Techniques and Procedures, Diagnostic Tests, Routine, Pandemics, SARS-CoV-2, Viral Load, Virus Replication
Background
Initially identified in Wuhan, a Chinese city of over 10 million population, severe acute respiratory syndrome coronavirus 2 (SARS-COV-2) spread rapidly throughout the country and internationally since late 2019, causing the global coronavirus disease 2019 (COVID-19) pandemic [1,2]. As of 10 November 2020, there have been over 50.6 million confirmed cases of COVID-19 globally across more than 200 countries, including 1,261,075 deaths, mostly caused by severe pneumonia [3,4]. To date, no specific antiviral treatment or vaccine for SARS-COV-2 has been approved by the FDA. The infection’s extent, clinical penetrance, and dynamics underlying the rapid spread of SARS-COV-2 have not been fully understood, either. Under such circumstance, access to accurate and timely laboratory testing has been one of the keys to controlling the spread of the disease and protect lives, as suggested by the World Health Organization (WHO) [5]. Here, we summarize the recent major advances in the diagnostic tests of COVID-19 and revolutionary techniques under development that may be important for the detection of SARS-COV-2 and other emerging novel pathogens in the future.
Policies and Criteria for Diagnostic Testing
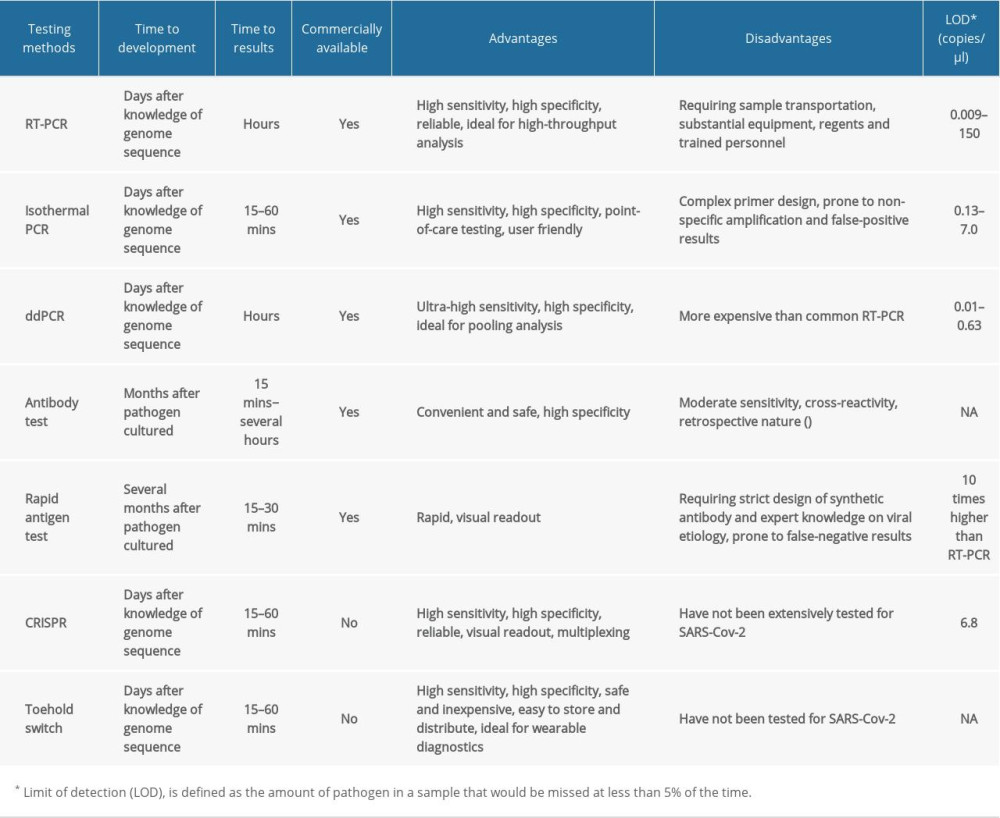
Many governments decide who should be tested based on contact history with infected persons and clinical symptoms such as fever, respiratory symptoms, smell and taste disorders, and difficulty breathing [6]. Diagnostic testing was initially regulated in the United States at the early stage of the COVID-19 outbreak. In March 2020, however, restrictive testing criteria was removed by the Centers for Disease Control and Prevention (CDC) to encourage the clinicians to determine whether to conduct a test according to specific situations [7]. Also in March 2020, the Food and Drug Administration (FDA) released a guidance document that enacted several unprecedented policies concerning COVID-19 diagnosis to counteract the potential public health threat posed by SARS-CoV-2. These policies allowed clinical laboratory improvement amendments (CLIA)-certified laboratories and other SARS-CoV-2 diagnostic test developers to use validated SARS-CoV-2 diagnostic tests clinically with only notification to the FDA [8]. To date, the FDA has also issued emergency use authorization (EUA), a mechanism by which the FDA fast-tracks diagnostic and therapeutic medical devices to respond to public health emergencies, for 182 molecular diagnostic tests, 35 high-complexity molecular-based laboratory developed tests, 55 serology/antibody assays, and 6 antigen diagnostic tests to overcome the widespread shortages of COVID-19 diagnostic tests throughout the United States [9]. Characteristics of the common types of molecular and serological tests are briefly summarized in Table 1 and described in more detail below.
SARS-CoV-2 Nucleic Acid Testing (NAT)
Currently, reverse transcription-polymerase chain reaction (RT-PCR)-based nucleic acid testing (NAT), due to its high specificity, is still the criterion standard for diagnosis of SARS-CoV-2 infection. At the early stage of the outbreak, the SARS-COV-2 virus was isolated and sequenced by the Chinese CDC. Subsequently, full genomic information of the virus was submitted to the WHO and deposited at GISAID [1,10]. RT-PCR-based molecular diagnostic tools were developed accordingly using specific primers and probes to target the viral genes of envelope (E), RNA-dependent RNA polymerase (RdRP), and nucleocapsid protein (N) in a stepwise manner in Europe, or to target the open reading frame (ORF1a and ORF1b) and N genes as recommended by the Chinese CDC [11, 12]. In the United States, 2 regions of the SARS-CoV-2 N gene and the control human RNase P gene were initially amplified in the CDC diagnostic test, but presented certain technical issues [13].
Although RT-PCR tests have facilitated the diagnosis of numerous COVID-19 patients, false-negative results remain an issue, as for similar tests for other pathogens [5,14]. In a standard procedure, clinical samples are collected as nasopharyngeal swabs (NPS) and oropharyngeal swabs (OPS) in a sterile and sealed container with viral transport medium or isotonic saline for viral detection. Recent reports, however, have demonstrated dynamic shedding of SARS-COV-2, which may contribute to the false-negative problem [15]. Viral loads appear higher at the early stage of SARS-COV-2 infection and were more detectable in the nose than in the throat. Also, respiratory tract samples such as bronchoalveolar lavage (BAL) and endotracheal aspirate present even higher viral loads [16,17]. The positive rates of RT-PCR for the detection of SARS-CoV-2 are 73% and 63% for NPS from severely and mildly symptomatic patients, respectively, in the first 14 days after disease onset, 85% and 78% for sputum samples, and 54% and 53% for OPS [18]. Therefore, the results of RT-PCR are influenced by factors such as the viral load, virus replication, and the source and timing of sample collection in relation to the disease onset, and needs to be cautiously interpreted. Multiple follow-up tests are necessary for the suspected cases with negative RT-PCR results, and many clinicians have suggested chest CT scans as an additional diagnostic tool, with its high sensitivity at certain stages after viral infection [19].
Test protocols for RT-PCR require laboratory facilities with substantial equipment, regents, and personnel trained for nuclear-acid manipulation. As recommended by the WHO, the handling of SARS-COV-2 biospecimens should be conducted in at least a biosafety level 2 (BSL2) laboratory [5,20]. Therefore, molecular diagnosis of SARS-COV-2 infection is often carried out in central or regional laboratories. Despite the extensive collaboration between various institutions in academia, industry, and healthcare, the turnaround time for testing results often exceed 48 h, which may be further delayed by the daily testing capacity of a laboratory [21]. This was an obvious issue previously in Wuhan, China when facing the rocketing numbers of cases, and is currently posing problems in other parts of the world. Recently, several studies have explored the potential use of pooling strategies to improve testing throughput, or to develop tests that utilize isothermal amplification and do not require a RNA extraction step, and showed encouraging results [22,23]. High detection rates of SARS-COV-2 have been reported in saliva samples, possibly due to the expression of angiotensin-converting enzyme II (ACE2) as a receptor for the virus in salivary glands [24]. Although the sensitivity of saliva as a diagnostic specimen is slightly lower than that of NPS, saliva testing may offer a useful alternative for first-line screening, especially in poor-resource settings lacking personal protective equipment and swabs. It is also feasible for patients to collect saliva samples by themselves, which could potentially reduce risk to healthcare workers and simplify testing procedures [25].
More recently, several studies have utilized the droplet digital PCR (ddPCR) technique to detect SARS-COV-2 with ultra-high sensitivity [26]. Compared with the traditional real-time PCR, ddPCR enables absolute quantification and removes potential amplification bias by partitioning each sample into more than 20,000 water-oil emulsion droplets and conducting PCR amplification in each individual droplet. Impressively, the dd-PCR-based method has been able to detect positive SARS-COV-2 infection among approximately 30% of clinical samples that tested negative for RT-PCR, exhibiting a limit of detection (LOD) as low as 10−2 copies per microliter of input. Since false-negative test results are collectively caused by low viral load in samples and the high LOD of diagnostic testing, the ddPCR method provides a powerful alternative to RT-PCR, especially when confirming suspected negative patients [27,28].
Serology Testing for SARS-CoV-2 Antibodies
Extensive research is being carried out globally to complement RT-PCR tests and reduce diagnostic time of COVID-19 through serological antibody detection. This method detects IgM, IgG, or total antibodies against the N and spike (S) proteins, which are 2 major immunogens of SARS-CoV-2, using enzyme-linked immunosorbent assay (ELISA), immunochromatographic assay, and proteomic microarray techniques [29–31]. Again, the sensitivity of serological tests depends heavily on the sampling time from disease onset. The cumulative seroprevalence of IgM and IgG are about 44% and 56% on day 7 after disease onset, respectively, but this percentage rapidly reaches over 95% on day 20 for IgM and day 16 for IgG. The levels of IgM start to decline 28 days after disease onset, whereas IgG can remain at high levels for at least 7 more weeks [32]. Of importance, although the highest seropositive rates were observed for IgG, both IgM and IgG should be measured, since individuals with IgM or IgG positivity alone have been reported [32].
Rapid and near-patient antibody test kits are under development to deliver diagnostic results in 15 min from a few drops of finger-prick blood [31]. Despite the advantage of faster screening of infected individuals in various contexts, serological antibody tests are not suitable for diagnosing the acute phase of COVID-19, since they are negative during the first week of illness. The serological method should only be used for contact tracing, detection of prior infection and immunity, retrospective assessment of the extent of outbreaks, and screening or diagnosis of asymptomatic patients, as recommended by the U.S. CDC [33]. It is also critical that serologic tests for SARS-CoV-2 antibodies not cross-react with other coronaviruses to avoid limitation by poor specificity [21].
Antigen Testing for SARS-CoV-2
Rapid antigen diagnostic tests have recently been developed for SARS-CoV-2 detection. To date, the FDA has given EUA for 6 tests in this category. On August 26, 2020, an EUA for the first antigen test that does not require an instrument was issued to Abbott Diagnostics Scarborough for the BinaxNOW COVID-19 Ag Card [9]. Such tests are designed to detect viral proteins in nasal swabs in as few as 15 minutes and provide highly specific results that can be read directly from a testing card [34]. However, false-negative results remain as an issue due to their even lower sensitivity compared with molecular diagnostic tests. A recent study has demonstrated that although rapid antigen tests could detect SARS-CoV-2 infection among 11.1% to 45.7% of clinical samples tested positive by RT-PCR, their limits of detection (LOD) are approximately 10,000 times higher, and thus should only be used jointly with RT-PCR [35].
Novel RNA Sensing Techniques
RNA is the ideal molecule to mediate highly specific nucleic acid recognition through base pair complementarity, a phenomenon commonly evidenced by biological processes such as the RNA interference or RNA modification [36]. Evolving insights into such properties of RNA and its analogous molecule have also revolutionized the field of molecular diagnostics by providing rapid and accurate sensing techniques for nuclear acids of emerging novel pathogens, including SARS-COV-2.
Clustered regularly interspaced short palindromic repeats (CRISPR)-Cas was described a decade ago as a bacterial adaptive defense system, in which the acquisition of short DNA pieces into the prokaryotic chromosome guides immunity against foreign DNA, such as in phages, plasmids, or transposons [37]. Recent studies report that when certain CRISPR-Cas proteins cleave double-stranded DNA in a sequence-specific manner, they also induce robust and nonspecific trans-cleavage of single-stranded nucleic acids; specifically, collateral cleavage [38].
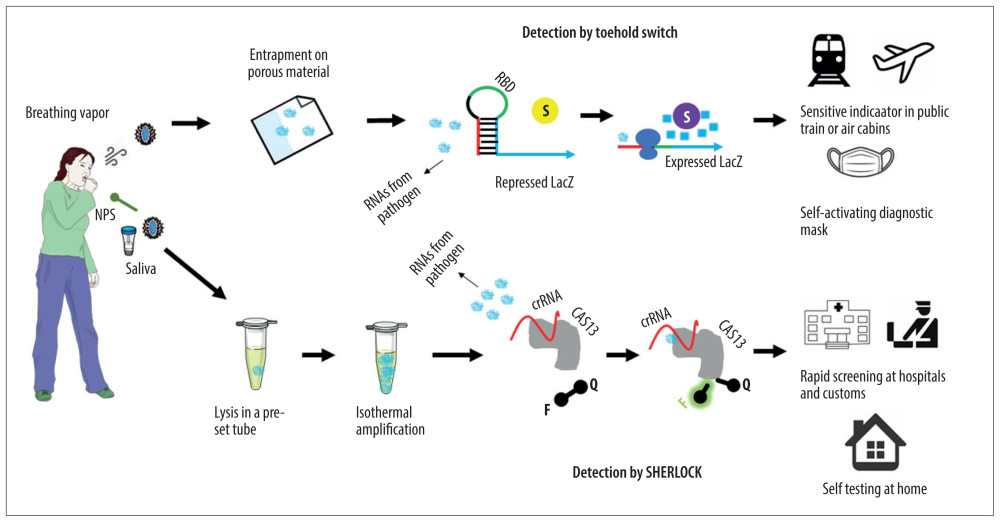
On a specific high-sensitivity enzymatic reporter unlocking (SHERLOCK) platform developed by Zhang and colleagues, two target regions were amplified from the S and ORF1ab genes of the SARS-CoV-2 genome using a commercially available recombinase polymerase amplification (RPA) kit and specific amplification primers [39]. A special member of the CRISPR-associated (Cas) proteins, Cas13, is harnessed to recognize the viral molecules of COVID-19 under the guidance of a pre-designed guide CRISPR RNA (crRNA), which in turn activates trans-cleavage of reporter-coupled single-strand nucleic acids by Cas13 to generate fluorescent signals or readable colorimetric signals on a lateral flow strip (Figure 1). With guide crRNA sequences specifically selected to minimize off-targets to related genomes of other human respiratory viruses, the platform is able to consistently detect SARS-CoV-2 target sequences in a range of 20–200 aM and return test results in less than an hour. Although the SHERLOCK platform exhibited excellent sensitivity and specificity in the detection of Zika virus and Dengue virus from human samples, clinical verification has not yet been undertaken for SARS-CoV-2 [40]. However, on a similar CRISPR-Cas12-based DNA endonuclease-targeted CRISPR trans-reporter (DETECTR) platform, 78 patients with COVID-19 or other viral respiratory infections have been tested, providing an encouraging result of 95% positive predictive agreement and 100% negative predictive agreement [41].
Utilizing the highly sensitive molecular sensors coupled to the cell-free synthetic biology network, wearable diagnostics such as a COVID-19 diagnostic face mask are under development by Collins and colleagues [42]. In this system, the secondary structure of a pre-designed riboregulator-like sequence, namely Toehold Switch, represses the expression of a downstream reporter gene [43]. The structure is unwound upon binding of a cognate RNA from the target pathogen in a sequence-specific manner, leading to the exposure of the ribosome-binding domain (RBD) in the construct and induction of a reporter gene such as LacZ, which in turn cleaves the yellow color substrate chlorophenol red-b-D-glucopyranoside to produce a purple color visible to the naked eyes [43] (Figure 1). This is achieved on the paper, cloth, or other porous substrates that have been pre-blotted with cell-free gene expression systems and can restore the fundamental transcription and translation properties simply by rehydration [44]. The system is sterile and abiotic, inexpensive, and easy to store and distribute. Importantly, the sensors can be developed in 1 day after the genetic sequence of a target pathogen is known, which makes them more favorable for the detection of emerging novel pathogens than antibody tests that generally take months to develop [44]. Again, the system has showed excellent accuracy in the detection of Ebola and Zika virus, but has not been tested clinically for SARS-CoV-2.
Conclusions
Hard lessons have been learned from the COVID-19 pandemic, and even tougher challenges from emerging and re-emerging pathogens will appear in the future. Rapid, accurate, and accessible diagnostics are needed for the early detection of pathogens in their preclinical and asymptomatic (but likely still contagious) stages and the follow-up until their disappearance. Besides helping to answer critical questions such as the infection’s extent, clinical penetrance, and dynamics, this would allow us to optimize clinical care, infection control, and public health intervention to limit the disease spread. RT-PCR remains the criterion standard and most commonly used diagnostic testing for SARS-CoV-2 infection. DdPCR is especially useful to detect low levels of virus and could help to avoid false-negative results. Serological antibody testing and rapid antigen testing are being increasing developed. However, both the retrospective nature of antibody tests and the low sensitivity of rapid antigen tests may limit their application. RNA sensing techniques have also been developed or are under development for the detection of SARS-CoV-2. So far, they have exhibited impressively low cost, high accuracy, and rapid detection. Testing results should be interpreted with caution since they depend heavily on the biological site, timing, quality of samples, and characteristics of various testing methods. Moreover, the correlation between viral RNA load and infectivity awaits proven.
References
1. Wang C, Horby PW, Hayden FG, Gao GF, A novel coronavirus outbreak of global health concern: Lancet, 2020; 395(10223); 470-73
2. Remuzzi A, Remuzzi G, COVID-19 and Italy: What next?: Lancet, 2020; 395(10231); 1225-28
3. Zhu N, Zhang D, Wang W, A Novel Coronavirus from Patients with Pneumonia in China, 2019: N Engl J Med, 2020; 382(8); 727-33
4. World Health Organization: WHO Coronavirus Disease (COVID-19) Dashboard, 2020a https://covid19.who.int
5. World Health Organization: Laboratory testing for coronavirus disease 2019 (COVID-19) in suspected human cases: interim guidance March 2, 2020; 2020 https://apps.who.int/iris/handle/10665/331329
6. Huang C, Wang Y, Li X, Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China: Lancet, 2020; 395(10223); 497-506
7. Centers for Disease Control and Prevention: Evaluating and testing persons for coronavirus disease 2019 (COVID-19), 2020 https://www.cdc.gov/coronavirus/2019-nCoV/hcp/clinical-criteria.html
8. U.S. Food and Drug Administration: Policy for coronavirus disease-2019 tests during the public health emergency (revised), 2020 https://www.fda.gov/media/135659/download
9. U.S. Food and Drug Administration, 2020 https://www.fda.gov/medical-devices/coronavirus-disease-2019-covid-19-emergency-use-authorizations-medical-devices/vitro-diagnostics-euas
10. Shu Y, McCauley J, GISAID: Global initiative on sharing all influenza data – from vision to reality: Euro Surveill, 2017; 22(13); 30494
11. Corman VM, Landt O, Kaiser M, Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR: Euro Surveill, 2020; 25(3); 2000045
12. Li Q, Guan X, Wu P, Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia: N Engl J Med, 2020; 382(13); 1199-207
13. Centers for Disease Control and Prevention: CDC 2019-novel coronavirus (2019-nCoV) real-time RT-PCR diagnostic panel, 2020 https://www.fda.gov/media/134922/download
14. U.S. Food and Drug Administration: Use of laboratory methods for SARS diagnosis, 2020 https://www.who.int/csr/sars/labmethods/en/
15. Wang W, Xu Y, Gao R, Detection of SARS-CoV-2 in different types of clinical specimens: JAMA, 2020; 323(18); 1843-44
16. Zhang W, Du R-GH, Li B, Molecular and serological investigation of 2019-nCoV infected patients: Implication of multiple shedding routes: Emerg Microbes Infect, 2020; 9(1); 386-89
17. Zou L, Ruan F, Huang M, SARS-CoV-2 viral load in upper respiratory specimens of infected patients: N Engl J Med, 2020; 382(12); 1177-79
18. Yang Y, Yang M, Shan C, Evaluating the accuracy of different respiratory specimens in the laboratory diagnosis and monitoring the viral shedding of 2019-nCoV infections: medRxiv, 2020; 2020 20021493
19. Fang Y, Zhang H, Xie J, Sensitivity of Chest CT for COVID-19: Comparison to RT-PCR: Radiology, 2020; 296(2); E115-17
20. World Health Organization: Assessment tool for laboratories implementing SARS-CoV-2 testing: interim guidance October 2, 2020; 2020 https://apps.who.int/iris/handle/10665/335843
21. Beeching NJ, Fletcher TE, Beadsworth MBJ, Covid-19: Testing times: BMJ, 2020; 369; m1403
22. Ben-Ami R, Seidel M, Sido T, Large-scale implementation of pooled RNA extraction and RT-PCR for SARS-CoV-2 detection: Clin Microbiol Infect, 2020; 26(9); 1248-53
23. Fukumoto T, Iwasaki S, Fujisawa S, Efficacy of a novel SARS-CoV-2 detection kit without RNA extraction and purification: Int J Infect Dis, 2020; 98; 16-17
24. Shamsoddin E, Saliva: A diagnostic option and a transmission route for 2019-nCoV: Evid Based Dent, 2020; 21(2); 68-70
25. Nagura-Ikeda M, Imai K, Tabata S, Clinical evaluation of self-collected saliva by RT-qPCR, direct RT-qPCR, RT-LAMP, and a rapid antigen test to diagnose COVID-19: J Clin Microbiol, 2020; 58(9); e01428-20
26. MacKay MJ, Hooker AC, Afshinnekoo E, The COVID-19 XPRIZE and the need for scalable, fast, and widespread testing: Nat Biotechnol, 2020; 38(9); 1021-24
27. Dang Y, Liu N, Feng Y, Comparison of qualitative and quantitative analyses of COVID-19 clinical samples: Clin Chim Acta, 2020; 510; 613-16
28. Suo T, Liu X, Feng J, ddPCR: A more accurate tool for SARS-CoV-2 detection in low viral load specimens: Emerg Microbes Infect, 2020; 9(1); 1259-68
29. Wolfel R, Corman VM, Guggemos W, Virological assessment of hospitalized patients with COVID-2019: Nature, 2020; 581(7809); 465-69
30. Zhao J, Yuan Q, Wang H, Antibody responses to SARS-CoV-2 in patients of novel coronavirus disease 2019: Clin Infect Dis, 2020; 71(16); 2027-34
31. Li Z, Yi Y, Luo X, Development and clinical application of a rapid IgM-IgG combined antibody test for SARS-CoV-2 infection diagnosis: J Med Virol, 2020 [Online ahead of print]
32. Xu X, Sun J, Nie S, Seroprevalence of immunoglobulin M and G antibodies against SARS-CoV-2 in China: Nat Med, 2020; 26(8); 1193-95
33. Centers for Disease Control and Prevention: Overview of testing for SARS-CoV-2 (COVID-19), 2020 https://www.cdc.gov/coronavirus/2019-ncov/hcp/testing-overview.html
34. U.S. Food and Drug Administration: COVID-19 Update: FDA authorizes first diagnostic test where results can be read directly from testing card, 2020 https://www.fda.gov/news-events/press-announcements/covid-19-update-fda-authorizes-first-diagnostic-test-where-results-can-be-read-directly-testing-card
35. Mak GC, Cheng PK, Lau SS, Evaluation of rapid antigen test for detection of SARS-CoV-2 virus: J Clin Virol, 2020; 129; 104500
36. Morris KV, Mattick JS, The rise of regulatory RNA: Nat Rev Genet, 2014; 15(6); 423-37
37. Barrangou R, Fremaux C, Deveau H, CRISPR provides acquired resistance against viruses in prokaryotes: Science, 2007; 315(5819); 1709-12
38. Chertow DS, Next-generation diagnostics with CRISPR: Science, 2018; 360(6387); 381-82
39. Zhang F: A protocol for detection of COVID-19 using CRISPR diagnostics, 2020 https://www.broadinstitute.org/files/publications/special/COVID-19%20detection%20(updated).pdf
40. Myhrvold C, Frejie CA, Gootenborg JS, Field-deployable viral diagnostics using CRISPR-Cas13: Science, 2018; 360(6387); 444-48
41. Broughton JP, Deng X, Yu G, CRISPR-Cas12-based detection of SARS-CoV-2: Nat Biotechnol, 2020; 38(7); 870-74
42. Boettner B: The Wyss Institute’s response to COVID-19: Beating back the coronavirus, 2020 https://wyss.harvard.edu/news/news-the-wyss-institutes-response-to-covid-19-beating-back-the-coronavirus/
43. Green AA, Silver PA, Collins JJ, Yin P: Cell, 2014; 159(4); 925-39
44. Pardee K, Green AA, Ferrante T, Paper-based synthetic gene networks: Cell, 2014; 159(4); 940-54
In Press
Clinical Research
Comparative Effectiveness of a Nurse-Led Care Model vs Usual Care in Rheumatoid Arthritis: A Longitudinal C...Med Sci Monit In Press; DOI: 10.12659/MSM.953211
Clinical Research
Impact of Treatment Modality on Pain, Sexual Function, and Psychological Well-Being in Patients With Bartho...Med Sci Monit In Press; DOI: 10.12659/MSM.952422
Clinical Research
Association Between Radiographic Knee Osteoarthritis, Pre-Fracture Mobility, and Hip Fracture Patterns in O...Med Sci Monit In Press; DOI: 10.12659/MSM.952678
Clinical Research
Association Between Total Cholesterol–to–High-Density Lipoprotein Ratio and Gestational Hypertension: A Cas...Med Sci Monit In Press; DOI: 10.12659/MSM.952395
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,084
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,757,530
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,116
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,768
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387