17 January 2022: Clinical Research
Epidemiology of Birth Defects in Eastern China and the Associated Risk Factors
Qiao-Qiao Wang1BEG*, Cha-Ying He2AC, Jin Mei3ADF, Yi-Lin Xu4BCDOI: 10.12659/MSM.933782
Med Sci Monit 2022; 28:e933782






Abstract
BACKGROUND: This study aimed to survey the overall situation of birth defects (BDs) among citizens of Hangzhou, China, and the risk factors of different BD types.
MATERIAL AND METHODS: We collected the data of 4349 perinatal infants with BDs in Hangzhou. The potentially associated risk factors of BDs were recorded and logistic regression analysis was used to predict the high incidence of BDs.
RESULTS: Among all perinatal infants with BDs, there were 4105 (94.3%) single births, 225 (5.2%) twin births, and 10 (0.2%) multiple births. In clinical outcomes, there were 2477 (57.0%) live births, 1806 (41.5%) dead fetuses, and 11 (0.3%) stillbirths. Down syndrome ranked first, accounting for 30.7% of the total births, followed by cleft lip and polydactyly. Low family income, nulliparity, high parity, high education level, and taking contraceptives in early pregnancy were found to be risk factors of Down syndrome. Low parity, low education level, and pesticide exposure were found to be risk factors of cleft lip. For polydactyly, young age of the mother and a parity above 0 were identified as risk factors.
CONCLUSIONS: Different risks factors can influence BD development and potentially help to predict specific BD types, such as demographic features and harmful exposure in early pregnancy.
Keywords: Fetal Alcohol Spectrum Disorders, Gaucher Disease, Perinatal Lethal, Jaundice, Neonatal, Teratogenesis, Adult, China, Cleft Lip, Congenital Abnormalities, Contraceptive Agents, Down Syndrome, Educational Status, Female, Humans, Incidence, Infant, Newborn, Male, Maternal Age, Parity, Pesticides, Poverty, Pregnancy, Risk Factors
Background
The term birth defect (BD) refers to abnormalities in body structure, function, or metabolism that occur before delivery [1–3]. The causes of BDs are complex and multifactorial and include environmental and genetic factors, such as chromosome aberrations or gene mutations. Currently, BDs are still a major public health problem affecting children’s health. In China, the prevalence of BDs ranges from 0.715% to 19.184%, and the annual number of new BDs is approximately 900 000 cases [3–5]. Recently, emphasis has been placed on BDs in Eastern China. However, there have been extremely limited epidemiological investigations of BDs in this region. Also, the genetic and environmental risk factors of teratogenicity (toward each BD type) are not fully understood. Hangzhou is one of the most economically developed cities in China. An epidemiological survey of Hangzhou citizens can be helpful to understand the overall situation of BDs in Eastern China and can assist in inferring the common risk factors of different types of BDs. This study aimed to provide a reference for revealing the influencing factors of BDs and preventive interventions.
Material and Methods
STUDY POPULATION:
Perinatal babies (from 28 weeks of gestation to 7 days after delivery) with BDs in all available medical institutions in Hangzhou were enrolled from 2009 to 2013, including live births, mid-term induced abortions, fetal death (the fetus died in the uterus after 20 weeks of gestation), stillbirth (the fetus died in the process of delivery), and death within 7 days after delivery. All medical institutions in Hangzhou offering midwifery services used the nationally unified Medical Institutions’ Birth Defects Registration Card to record data in the Hangzhou Maternal and Child Health Network. To ensure that the data were true and accurate, this project adopted a 3-level quality management system. First, all recording personnel were professionally trained, and the recorded information was checked by 2 staff members. Second, each district/county care institution reviewed the statements and reported them after confirmation. Finally, the Hangzhou Maternity and Child Health Hospital conducted verification of all the reported cards annually. After confirming that the original data were correct, 2 data-input staff managed the Epidata database and conducted a consistency check. For all infants with BDs, the diagnostic methods included prenatal ultrasound diagnosis, postnatal clinical diagnosis, autopsy, and chromosome examination, as appropriate. The key demographic characteristics of the mother and family were recorded, including the age and education level of the mother, gravidity, parity, family monthly income per capita, and residential environment. The potential BD-associated factors were documented, including taking medications in early pregnancy (especially contraceptives), illness in early pregnancy (especially fever), and exposure to harmful substances in early pregnancy (radiation and pesticide exposure).
STATISTICAL ANALYSIS:
The datasets were extracted from Epidata and analyzed using SPSS. Categorical data were described by percentages, and continuous variables were expressed as mean±standard deviation (SD). Logistic regression analysis was used for the prediction of several high-incidence BDs. A
Results
CLINICAL CHARACTERISTICS OF INFANTS WITH BDS AND THE PREGNANT WOMEN:
In total, 4349 perinatal infants with BDs were included, with an average gestational age of 232.05±49.66 days. As shown in Table 1, there were 4105 (94.3%) single births, 225 (5.2%) twin births, and 10 (0.2%) multiple births. Among these infants, 2271 (52.2%) were male and 1795 (41.3%) were female; however, the sex of 6.5% of infants was unknown. In clinical outcomes, there were 2477 (57.0%) live births, 1806 (41.5%) dead fetuses, and 11 (0.3%) stillbirths. These rates are similar to those of several BD investigations in China and western countries [6–9]. Moreover, 55 (1.3%) infants with BDs died within 7 days after delivery.
The demographic features of the pregnant women are presented in Table 2. The average age was 28.61±4.70 years, and 54.82% had a high-school education or below. About half of these women had a monthly income between 1000 and 4000 yuan, and 63.27% were from urban areas. Approximately 80% of the women had been previously pregnant or had given birth.
BD TYPES AND PROPORTIONS:
Of the BDs among the 4349 perinatal infants, Down syndrome was most common, accounting for 30.7% of the total BDs, followed by cleft lip and polydactyly. Other common BDs included hypospadias, encephalocele, congenital hydrocephalus, cleft palate, small ears (or no ears), syndactyly, conjoined twins, congenital diaphragmatic hernia, and congenital hydrocephalus. The frequencies and proportions of all observed BDs are presented in Table 3.
CORRELATION BETWEEN IMPORTANT DEMOGRAPHIC CHARACTERISTICS, RISK FACTORS IN EARLY PREGNANCY, AND BDS:
As expected, the incidence of BDs was found to be associated with some demographic characteristics and risk factors in early pregnancy. The detected strong correlations (R, between 2 variables, P<0.01) are presented in Tables 4 and 5. Notably, conjoined twins was positively correlated with mother’s age; Down syndrome was negatively correlated with gravidity; and parity showed a positive relationship with encephalocele, small ears (or no ears), Down syndrome, and esophageal atresia but had a negative correlation with cleft spine, congenital diaphragmatic hernia, cleft palate, umbilical bulge, cleft lip, gastroschisis, conjoined twins, and bladder exstrophy. Moreover, a higher education level was related to a low incidence of anencephaly, encephalocele, and esophageal atresia but a high incidence of Down syndrome. In addition, regarding fetal sex, female fetuses were more likely to have the following BDs: anencephaly, cleft spine, congenital diaphragmatic hernia, umbilical bulge, and gastroschisis.
In early pregnancy, women who had fever were more likely to have babies with syndactyly; pesticide exposure was correlated with umbilical bulge and cleft lip; and radiation exposure in early pregnancy was correlated with BDs such as anencephaly and bladder exstrophy.
REGRESSION ANALYSIS OF THE RISK FACTORS ASSOCIATED WITH COMMON BDS:
Next, logistic regression analysis was performed to clarify the influence of potential risk factors. The 3 most common BDs were Down syndrome, cleft lip, and polydactyly. The potential risk factors were analyzed using the forward logistic regression method to discover the risk factors associated with above BDs. The regression analysis results of Down syndrome are shown in Table 6: low family income, only 1 gravidity, high parity, high education level, and taking contraceptives in early pregnancy were found to be risk factors of Down syndrome. The logistic regression analysis of cleft lip is shown in Table 7: low parity, low education level, and pesticide exposure were identified as risk factors of cleft lip. For polydactyly, young age of the pregnant woman and a parity above 0 were the only 2 risk factors (Table 8). Taken together, the most important risks factors that may strongly influence the outcome of BDs included age of the pregnant women, gravidity, parity, education level, and harmful factors (fever, contraceptives, pesticide exposure, and radiation exposure) in early pregnancy.
Discussion
The main findings of this study are as follows. Down syndrome was the most common BD, accounting for more than 30% of all types of BDs, followed by cleft lip, polydactyly, hypospadias, and others. These results are consistent with the order of BD incidence in Jiangsu and Zhejiang. Also, different risks factors influence BD development, in particular, age of the pregnant woman, gravidity, parity, family monthly income, education level, fever in early pregnancy, taking contraceptives in early pregnancy, and exposure to pesticide or radiation.
Our study is among the surveys with the largest sample sizes in clinical BD research. Although most of our findings can be supported by previous studies, these well-known studies in BDs include no more than 1000 cases, even in developing countries [10,11]. For example, Down syndrome is the most common BD group and a significant contributor to neonatal and infant death. In China, the overall incidence of Down syndrome was 0.2%, and serum free beta-human chorionic gonadotrophin (β-hCG) and pregnancy-associated protein-A concentrations can be useful indicators [12]. However, to date, the present study is the first study with a large sample showing that family income and the mother’s education level are associated with Down syndrome in babies. Related studies have just surveyed the academic attainments of the children with Down syndrome [13]. Also, the link between contraceptive usage and Down syndrome has seldom been investigated. In fact, previous studies have shown no indication of any relationship between oral contraceptive use and Down syndrome [14,15]. We confirmed, for the first time in China, that the use of contraceptives in early pregnancy may increase the incidence of Down syndrome, and this interesting finding is worth researching in animal experiments to identify the underlying mechanisms. In the present study, cleft lip was most often found in first-born children, as shown by our correlation analysis and logistic regression analysis. This has not been reported in similar research. Known risk factors of cleft lip and palate include a family history of clefts, lack of folic acid, consanguineous marriage, paternal smoking, and malnutrition [16–18]. In the present study, we found that maternal pesticide exposure was a significant risk factor of cleft lip, which is consistent with another multiethnic study in Xinjiang, China [19]. This effect was also noticed in Mexico in 2013 [20]; however, there is still little solid evidence to date. Another high-incidence BD is polydactyly. Known risk factors of polydactyly in offspring include occupational exposure to chemicals in a textile factory during pregnancy, active and passive maternal smoking during pregnancy, and PM10 exposure [21–23]. In the present study, we found no correlation between exposure to harmful substances (as the above studies showed) during pregnancy and polydactyly; however, we were the first researchers to find that parity above 0 was more likely to lead to polydactyly, which was not likely due to older maternal age. As shown in Table 8, mother’s age seemed to be a protective factor (Exp B=0.959), implying that the influence was slight, although statistically significant. The logistic regression analysis, as shown in Table 8, eliminated confounding factors, and when the influencing factor of age with parity was excluded, it appeared that polydactyly was mainly caused by repeated deliveries but not an older mother’s age. The detailed mechanisms involved, however, are not yet clear; therefore, this conclusion requires more supportive evidence. Higher parity is also an important risk factor for encephalocele, small ears (or no ears), Down syndrome, and esophageal atresia. The adverse outcomes of a higher parity are closely related to genetic environmental factors, maternal age, lifestyle, pre-pregnancy and pregnancy behaviors, and previous medical or surgical treatments [23]. A high parity implies that more internal and external environmental factors exist in the mother, which may be related to the high proportion of chromosomal abnormalities in the women. Regarding miscarriage, it has been confirmed that miscarriage history is associated with gastroschisis, omphalocele, talipes, spina bifida, and hypospadias [24]. Birth cohort studies revealed that autoimmune diseases can influence time-to-pregnancy, pregnancy loss, and live birth rate [25]; miscarriage history is associated with bacterial vaginosis (eg, septic abortion [26]), which can induce huge toxicity to the fetus [27]. Additionally, some potentially hazardous surgeries (eg, dilatation and curettage) can increase the risk of a medically managed miscarriage or induced abortion [28], and this damage to the uterus can last until the subsequent pregnancy. Collectively, it is reasonable that a higher parity can be associated with many BD risks. However, we also found that parity was negatively correlated with conditions such as cleft spine, congenital diaphragmatic hernia, and cleft lip. This is understandable because primiparity/nulliparity is a known risk factor for several BDs, including limb deficiencies, congenital diaphragmatic hernia, gastroschisis, and omphalocele [29,30].
There are some limitations in this study. First, we have not assessed the risk factors of neonatal deaths in these babies with BDs. However, BDs are significantly associated with neonatal death. They are also associated with death 7 days after birth, and death up to 1 year [31]. We also observed a large number of fatal cases, including fetal deaths, stillbirths, and deaths within 7 days of birth. It is worth investigating which types of BDs have higher risks for mortality in future studies. Another limitation of the study is that we chose only the most important risk factors, which had a wide range of roles toward different BDs; however, a more accurate regression model should be used to assess a variety of potential factors, including additional demographic information, different dimensions of the perinatal status, and other maternity histories, and target each specific type of BD. In our universal prediction model, the power and usefulness were not optimal, because many key features were not included.
Conclusions
Down syndrome was the most common BD found in this study, accounting for more than 30% of all BD types, followed by cleft lip, polydactyly, hypospadias, and others. Different risks factors can influence BD development, in particular, age of the pregnant women, gravidity, parity, family monthly income, education level, fever in early pregnancy, taking contraceptives in early pregnancy, and exposure to pesticides or radiation.
Tables
Table 1. Clinical characteristics of enrolled infants.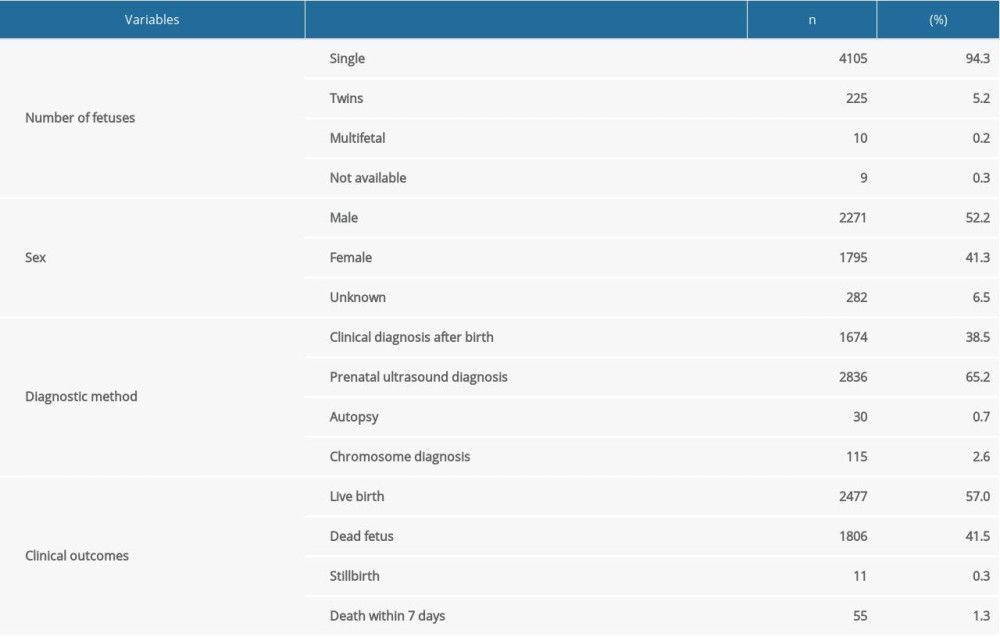 Table 2. General characteristics of enrolled pregnant women.
Table 2. General characteristics of enrolled pregnant women.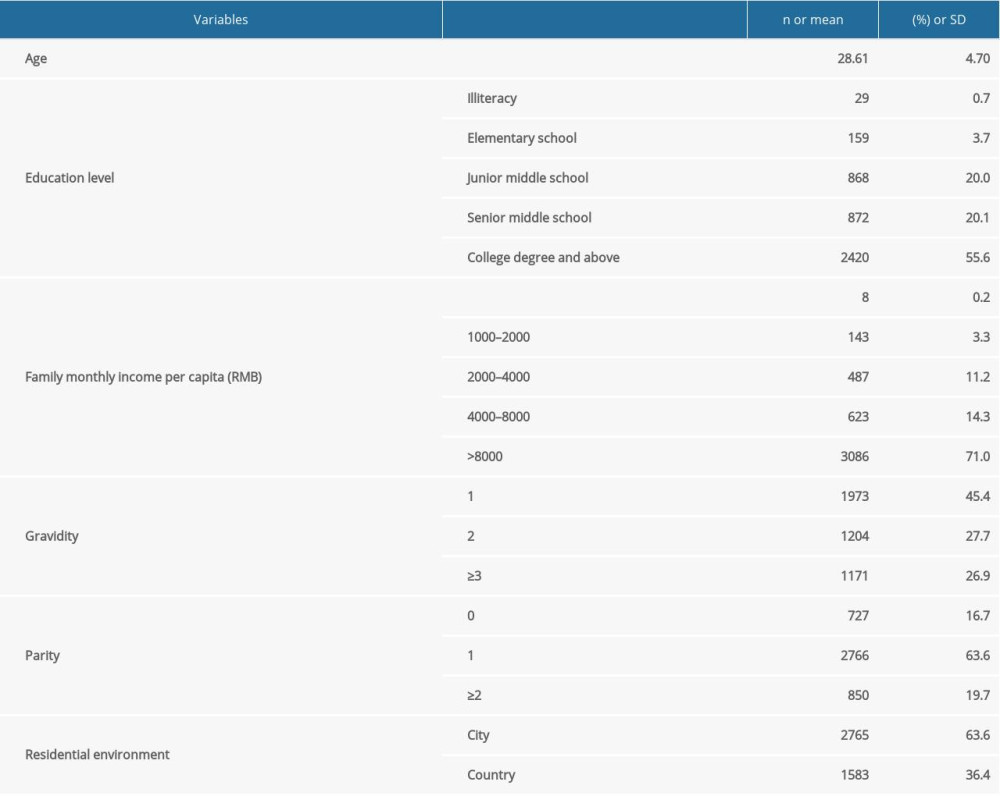 Table 3. Birth defect types and proportions.
Table 3. Birth defect types and proportions.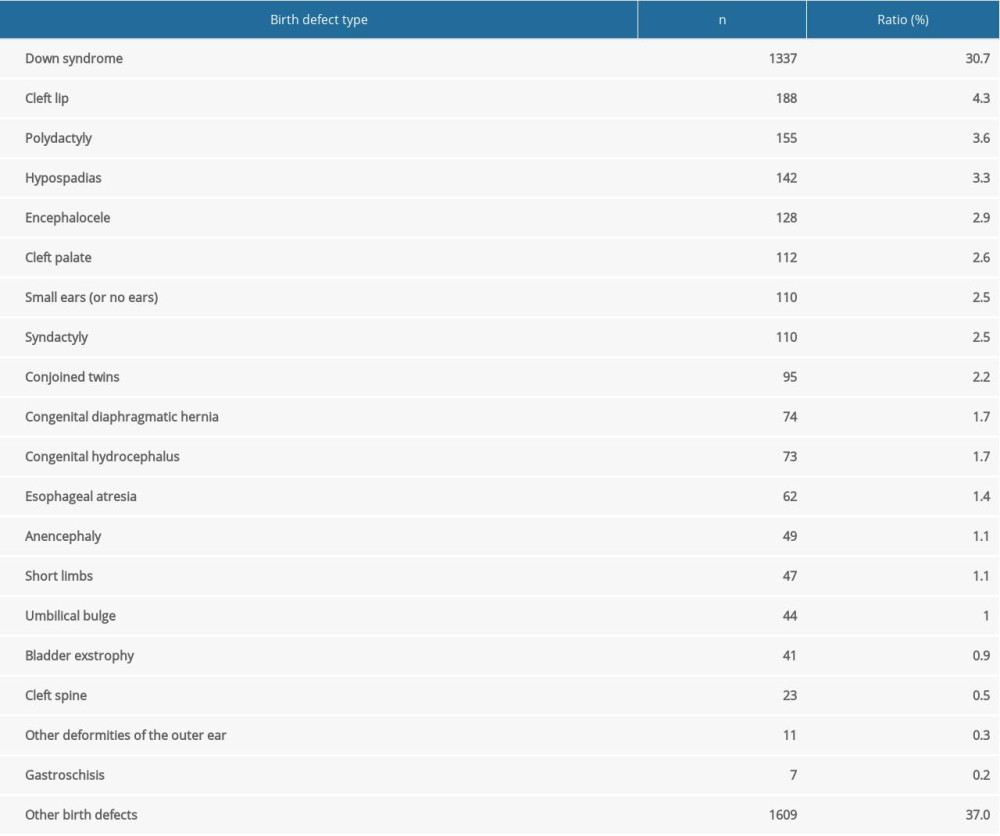 Table 4. Correlation between important demographic characteristics and birth defects (P<0.01).
Table 4. Correlation between important demographic characteristics and birth defects (P<0.01). Table 5. Correlation between risk factors in early pregnancy and birth defects (P<0.01).
Table 5. Correlation between risk factors in early pregnancy and birth defects (P<0.01).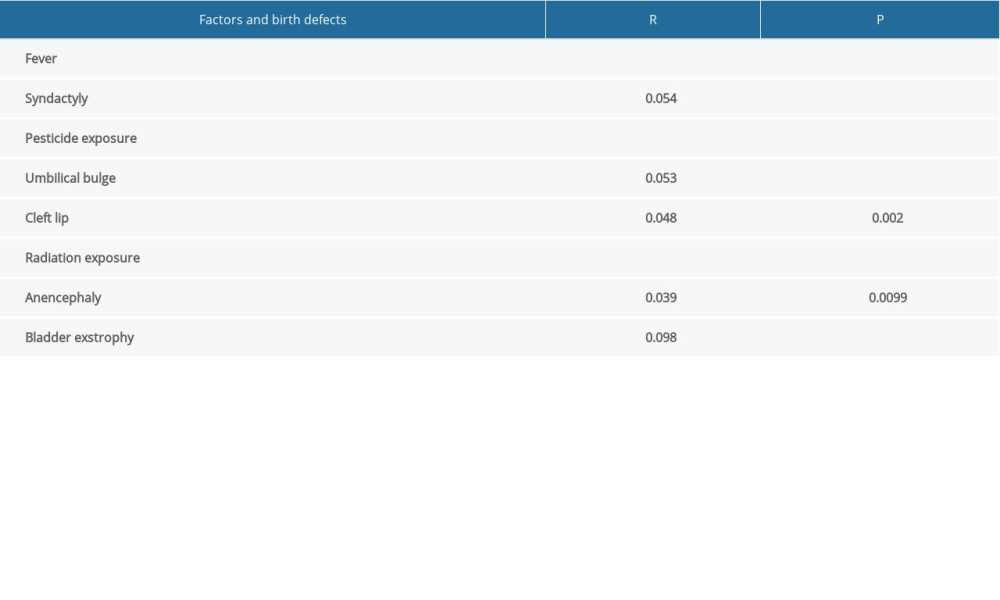 Table 6. Logistic regression analysis of Down syndrome.
Table 6. Logistic regression analysis of Down syndrome.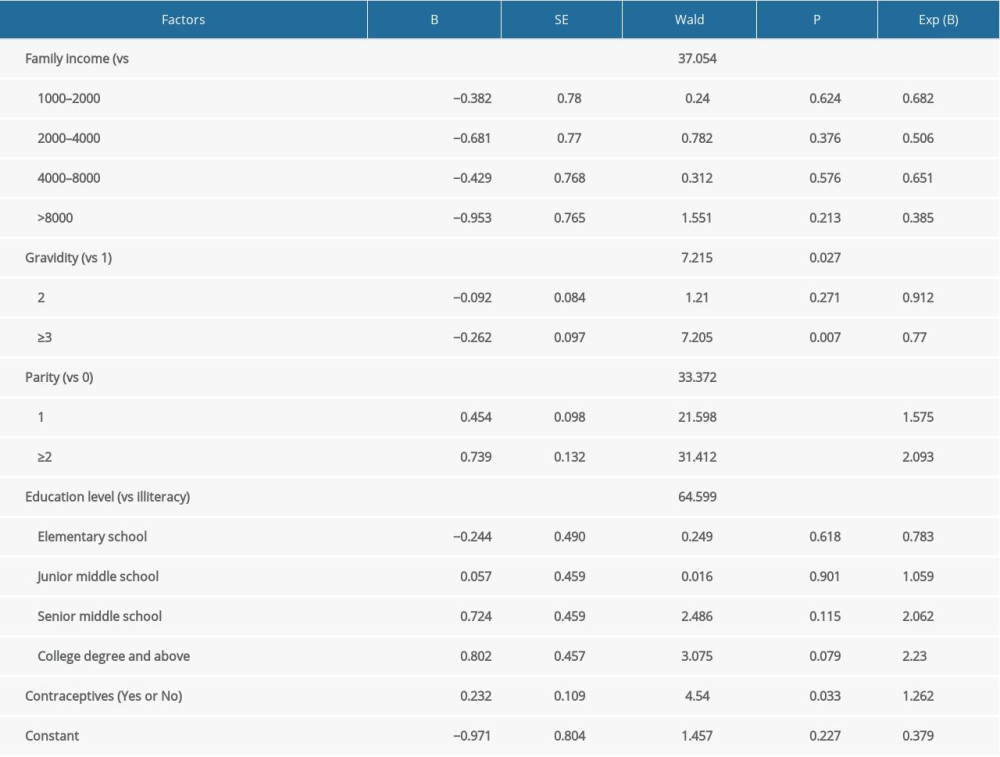 Table 7. Logistic regression analysis of cleft lip.
Table 7. Logistic regression analysis of cleft lip.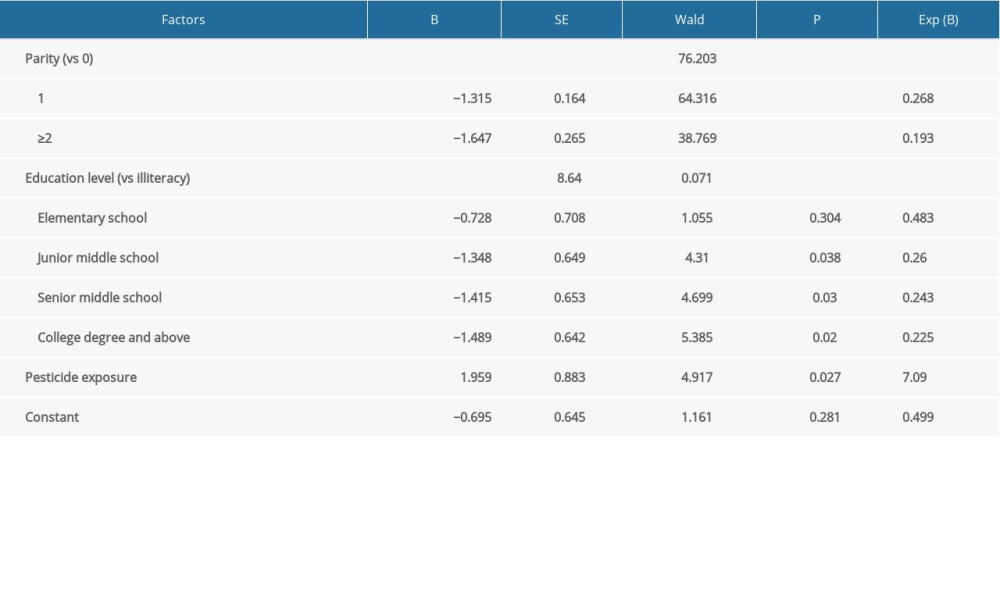 Table 8. Logistic regression analysis of polydactyly.
Table 8. Logistic regression analysis of polydactyly.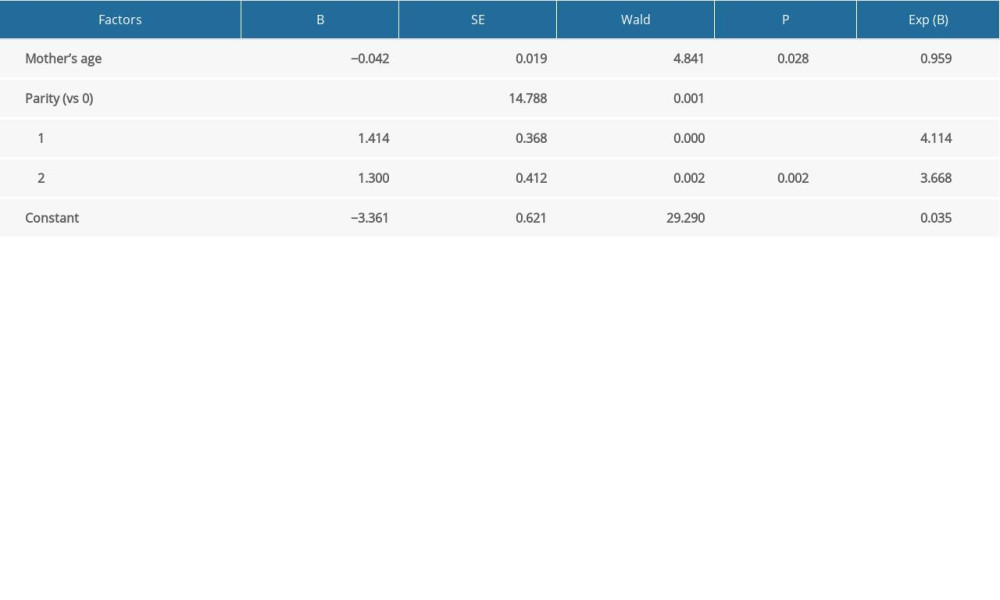
References
1. Benjamin RH, Yu X, Navarro Sanchez ML, Co-occurring defect analysis: A platform for analyzing birth defect co-occurrence in registries: Birth Defects Res, 2019; 111(18); 1356-64
2. Elias D, Campaña H, Poletta F, A graph theory approach to analyze birth defect associations: PLoS One, 2020; 15(5); e0233529
3. Zhou Y, Mao X, Zhou H, Epidemiology of birth defects based on a birth defect surveillance system in Southern Jiangsu, China, 2014–2018: J Matern Fetal Neonatal Med, 2020 [Online ahead of print]
4. Xie D, Yang T, Liu Z, Epidemiology of birth defects based on a birth defect surveillance system from 2005 to 2014 in Hunan Province, China: PLoS One, 2016; 11; e0147280
5. Chen J, Huang X, Wang B, Epidemiology of birth defects based on surveillance data from 2011–2015 in Guangxi, China: Comparison across five major ethnic groups: BMC Public Health, 2018; 18(1); 1008
6. Dong BQ, Chen BY, Liang QYStudy on the characteristics of major birth defects in 1.69 million cases of fetus in Guangxi Zhuang Autonomous Region: Zhonghua Liu Xing Bing Xue Za Zhi, 2019; 40(12); 1554-59 [in Chinese]
7. Svensson E, Ehrenstein V, Nørgaard M, Estimating the proportion of all observed birth defects occurring in pregnancies terminated by a second-trimester abortion: Epidemiology, 2014; 25(6); 866-71
8. Deng K, Qiu J, Dai L, Perinatal mortality in pregnancies with omphalocele: Data from the Chinese national birth defects monitoring network, 1996–2006: BMC Pediatr, 2014; 14; 160
9. Zhang Y, Riehle-Colarusso T, Correa A, Observed prevalence of congenital heart defects from a surveillance study in China: J Ultrasound Med, 2011; 30(7); 989-95
10. Mat Bah MN, Sapian MH, Jamil MT, Survival and associated risk factors for mortality among infants with critical congenital heart disease in a developing country: Pediatr Cardiol, 2018; 39(7); 1389-96
11. Demianczyk AC, Behere SP, Thacker D, Social risk factors impact hospital readmission and outpatient appointment adherence for children with congenital heart disease: J Pediatr, 2019; 205; 35-40e1
12. Miao ZY, Liu X, Shi TK, First trimester, second trimester, and integrated screening for Down’s syndrome in China: J Med Screen, 2012; 19(2); 68-71
13. Turner S, Alborz A, Academic attainments of children with Down’s syndrome: A longitudinal study: Br J Educ Psychol, 2003; 73(Pt 4); 563-83
14. Ericson A, Källén B, Lindsten J, Lack of correlation between contraceptive pills and Down’s syndrome: Acta Obstet Gynecol Scand, 1983; 62(5); 511-14
15. Janerich DT, Flink EM, Keogh MD, Down’s syndrome and oral contraceptive usage: Br J Obstet Gynaecol, 1976; 83(8); 617-20
16. Escher PJ, Zavala H, Lee D, Malnutrition as a risk factor in cleft lip and palate surgery: Laryngoscope, 2021; 131(6); E2060-65
17. Jamilian A, Sarkarat F, Jafari M, Family history and risk factors for cleft lip and palate patients and their associated anomalies: Stomatologija, 2017; 19(3); 78-83
18. Hong Y, Xu X, Lian F, Environmental risk factors for nonsyndromic cleft lip and/or cleft palate in Xinjiang Province, China: A multiethnic study: Cleft Palate Craniofac J, 2021; 58(4); 489-96
19. Ibarra-Lopez JJ, Duarte P, Antonio-Vejar V, Maternal C677T MTHFR polymorphism and environmental factors are associated with cleft lip and palate in a Mexican population: J Investig Med, 2013; 61(6); 1030-35
20. Shi J, Lv ZT, Lei Y, Maternal occupational exposure to chemicals in the textile factory during pregnancy is associated with a higher risk of polydactyly in the offspring: J Matern Fetal Neonatal Med, 2019 [Online ahead of print]
21. Shi J, Tian Y, Lei Y;Active and passive maternal smoking during pregnancy and risk of having a child with polydactyly: A case-control study: Zhonghua Liu Xing Bing Xue Za Zhi, 2018; 39(11); 1482-85 [in Chinese]
22. Zhang JY, Gong TT, Huang YH, Association between maternal exposure to PM10 and polydactyly and syndactyly: A population-based case-control study in Liaoning province, China: Environ Res, 2020; 187; 109643
23. Zhou SS, Ge X, Xu YQPrevious medical or surgical abortions and subsequent risk of preterm birth: A birth cohort study: Zhonghua Liu Xing Bing Xue Za Zhi, 2016; 37(11); 1536-40 [in Chinese]
24. Campaña H, Rittler M, Gili JA, Association between a maternal history of miscarriages and birth defects: Birth Defects Res, 2017; 109(4); 254-61
25. Plowden TC, Connell MT, Hill MJ, Family history of autoimmune disease in relation to time-to-pregnancy, pregnancy loss, and live birth rate: J Transl Autoimmun, 2020; 3; 100059
26. Takahashi Y, Iwagaki S, Itoh M, Cohort study of the incidence of spontaneous preterm birth and septic abortion referred by pathological examination in Gifu prefecture in Japan: Early Hum Dev, 2017; 104; 33-37
27. Gioan M, Fenollar F, Loundou A, Development of a nomogram for individual preterm birth risk evaluation: J Gynecol Obstet Hum Reprod, 2018; 47(10); 545-48
28. Lemmers M, Verschoor MA, Hooker AB, Dilatation and curettage increases the risk of subsequent preterm birth: A systematic review and meta-analysis: Hum Reprod, 2016; 31(1); 34-45
29. Syvänen J, Raitio A, Nietosvaara Y, Risk factors and prevalence of limb deficiencies associated with amniotic band sequence: A population-based case-control study: J Pediatr Orthop, 2021; 41(1); e94-e97
30. Duong HT, Hoyt AT, Carmichael SL, Is maternal parity an independent risk factor for birth defects?: Birth Defects Res A Clin Mol Teratol, 2012; 94(4); 230-36
31. Steurer MA, Peyvandi S, Baer RJ, Impaired fetal environment and gestational age: What is driving mortality in neonates with critical congenital heart disease?: J Am Heart Assoc, 2019; 8(22); e013194
Tables
Table 1. Clinical characteristics of enrolled infants.Table 2. General characteristics of enrolled pregnant women.Table 3. Birth defect types and proportions.Table 4. Correlation between important demographic characteristics and birth defects (P<0.01).Table 5. Correlation between risk factors in early pregnancy and birth defects (P<0.01).Table 6. Logistic regression analysis of Down syndrome.Table 7. Logistic regression analysis of cleft lip.Table 8. Logistic regression analysis of polydactyly. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387