08 March 2022: Review Articles
Adie’s Pupil: A Diagnostic Challenge for the Physician
Sui-yi XuDOI: 10.12659/MSM.934657
Med Sci Monit 2022; 28:e934657






Abstract
ABSTRACT: Adie’s pupil, also called tonic pupil, is mainly seen in young women. Most patients have unilateral eye involvement. The pupil of the affected side is significantly larger than that on the healthy side. The direct and indirect light reflection from the pupil on the affected side disappears. The pupil on the affected side is sensitive to low concentrations of pilocarpine. The pathogeneses of Adie’s pupil are complex, some of which are insidious and lack corresponding specific diseases. Through a literature review, we found that Adie’s pupil is mainly associated with infectious diseases, most commonly syphilis, followed by immune diseases and paraneoplastic syndromes. The ophthalmological symptoms and pupil abnormalities can disappear after active treatment of the primary disease. Pilocarpine can be used to treat ophthalmologic symptoms, such as blurred vision, for which patients might visit an ophthalmologist or neurologist. It is essential for clinicians to improve their understanding of the disease to avoid misdiagnosis. Differential diagnosis between Adie’s pupil, oculomotor nerve palsy, anticholinergic drug overdose, Argyll-Robertson pupil, and congenital mydriasis need to be identified by the physician. Here, the clinical manifestations, pathogenesis, relationship between Adie’s pupil and diseases, and differential diagnosis of Adie’s pupil are reviewed.
Keywords: Pilocarpine, Pupil Disorders, Vision Disorders, Adie Syndrome, Diagnosis, Differential, Humans, Physicians, Pupil, Tonic Pupil
Background
The size of the pupil is adjusted by the pupillary sphincter and dilator. The contraction of the pupillary sphincter muscle when innervated by the parasympathetic nerve fibers shrinks the pupil. However, the contraction of the pupillary dilator muscle when innervated by the sympathetic nerve fibers dilates the pupil [1]. There are 2 types of pupil reflection. The first is the light reflex, which causes bilateral pupils to shrink when 1 pupil is illuminated; the second is the accommodative reflex, also known as the near reflex, which is manifested by the bilateral pupil constriction when staring at a nearby object [2].
Adie’s pupil, also called tonic pupil, was first reported by the British neurologist William John Adie in 1931 [3]. It manifests as unilateral or bilateral pupil dilation, direct and indirect loss or weakening of light reflection, abnormal adjustment reflex, and pupil contraction disorder. Adie’s pupil is predominantly seen in young women, with an age of onset of 20 to 40 years. Patients usually observe that 1 pupil is larger than the other when looking in the mirror. Unilateral involvement is observed in 80% of patients [4]. Adie’s pupil usually exists in isolation, but it should be noted that it can be associated with other symptoms or can be part of other symptoms. When it is accompanied by weakening or disappearance of deep reflexes, it is known as Adie syndrome or Holmes-Adie syndrome [5]. When Adie’s pupil is accompanied by weakened or absent deep reflexes and segmental anhidrosis, it is known as Ross syndrome [6]. The complexity of the pathogenesis often leads to difficulty in identifying Adie’s pupil and possible related diseases by ophthalmologists and neurologists.
Survey Methodology
In this review, we used PubMed, Scopus, Web of Science, and Google Scholar to collect case reports of Adie’s pupil from 2010 to 2020 (Table 1) [7–42]. In the reports found, women accounted for 62.5% (25/40), and men accounted for 37.5% (15/40) of cases. The main symptoms of patients were blurred vision (65%, 26/40), photophobia (15%, 6/40), diplopia (12.5%, 5/40), and pain behind the eyeball (5%, 2/40). Some patients experienced no ophthalmologic symptoms (30%, 12/40).
Clinical Manifestations of Adie’s Pupil
The characteristics of Adie’s pupil can be summarized as follows: the affected pupil is significantly larger than the normal pupil; the direct and indirect reflection of light from the affected pupil disappears; and the affected pupil is sensitive to low concentrations of pilocarpine (Figure 1).
Pathogenesis of Adie’s Pupil
Adie’s pupil is usually secondary to eye diseases, including infections, tumors, autoimmune diseases, and trauma; however, it can also be associated with systemic diseases with autonomic dysfunction. It is generally considered a peripheral neuropathy caused by damage to the ciliary ganglion and its parasympathetic postganglionic fibers [3]. The ciliary ganglion contains fibers that innervate the ciliary muscle (responsible for adjusting the lens) and the pupillary sphincter. The number of fibers that innervate the ciliary muscle far exceed those that innervate the pupillary sphincter. Thus, when the ciliary ganglion is damaged, the fibers innervating the ciliary muscles have a greater chance of survival. This causes the fibers that originally innervated the ciliary muscles to innervate the pupillary sphincter [40]. Compared with normal pupil fiber regeneration, this abnormal regeneration leads to pupillary contraction and abnormal accommodation.
Relationship Between Adie’s Pupil and Diseases
Through the literature review, we found that Adie’s pupils are mainly associated with infectious diseases, most commonly syphilis, followed by immune diseases and paraneoplastic syndromes (Table 1). On encountering Adie’s pupils, the first disease that needs to be ruled out is syphilis, followed by other diseases, such as Vogt-Koyanagi-Harada syndrome and Sjogren syndrome, and other infections, autoimmune diseases, and paraneoplastic syndromes (Figure 2). The ophthalmologic symptoms and pupil abnormalities can disappear after treatment of the primary disease. A diagnosis of idiopathic Adie’s pupil can be considered after exclusion of all possible primary diseases. Pilocarpine can be used to treat ophthalmologic symptoms, such as blurred vision [40].
Differential Diagnosis of Adie’s Pupil
OCULOMOTOR NERVE PALSY:
In addition to the dilated pupils and loss of light reflection, there are other clinical manifestations, such as ptosis and restricted eye movements. Brain magnetic resonance imaging can reveal damage to the oculomotor nerve nucleus and fibers [43], and the pilocarpine test is usually negative [44].
DRUG OVERDOSE:
Atropine is an anticholinergic drug that can lead to a series of anticholinergic symptoms after excessive intake, including dilated pupils, hallucinations, agitation, tachycardia, delirium, and fever [45]. In addition, Datura, a traditional Chinese medicine, can also cause the above symptoms when ingested in large quantities [46].
ARGYLL-ROBERTSON PUPIL:
It is generally thought to be related to neurosyphilis. Patients usually present with bilateral miosis, loss of direct and indirect light reflection, and presence of accommodation and convergence reflexes. The affected pupil dilates after atropine instillation [47].
CONGENITAL MYDRIASIS:
Mydriasis and associated loss of light reflex are congenital, and both pupils can be affected. It is more common in women, and the pathogenesis is unclear. A combination of medical history and negative pilocarpine test can assist in identification of congenital mydriasis [48].
Conclusions
Adie’s pupil demonstrates sex predilection, having a greater incidence in women than men. Blurred vision is the main clinical manifestation of this disease. However, some patients have no ophthalmologic symptoms. The characteristics of Adie’s pupil can be summarized as follows: the affected pupil is significantly larger than the normal pupil; the direct and indirect reflection of light from the affected pupil disappears; and the affected pupil is sensitive to low concentrations of pilocarpine.
Adie’s pupil is mainly associated with infectious diseases, most commonly syphilis, followed by immune diseases and paraneoplastic syndromes. After active treatment of the primary disease, the ophthalmologic symptoms and pupil abnormalities can disappear. Pilocarpine can be used to treat ophthalmic symptoms, such as blurred vision. Differential diagnosis between Adie’s pupil, oculomotor nerve palsy, anticholinergic drug overdose, Argyll-Robertson pupil, and congenital mydriasis need to be identified by the physician. Therefore, when evaluating patients with manifestations similar to Adie’s pupil, physicians should first identify the diseases mentioned above. Low concentrations of pilocarpine, detailed history, and physical examination can be helpful. The primary disease spectrum behind Adie’s pupil should be actively screened.
Figures
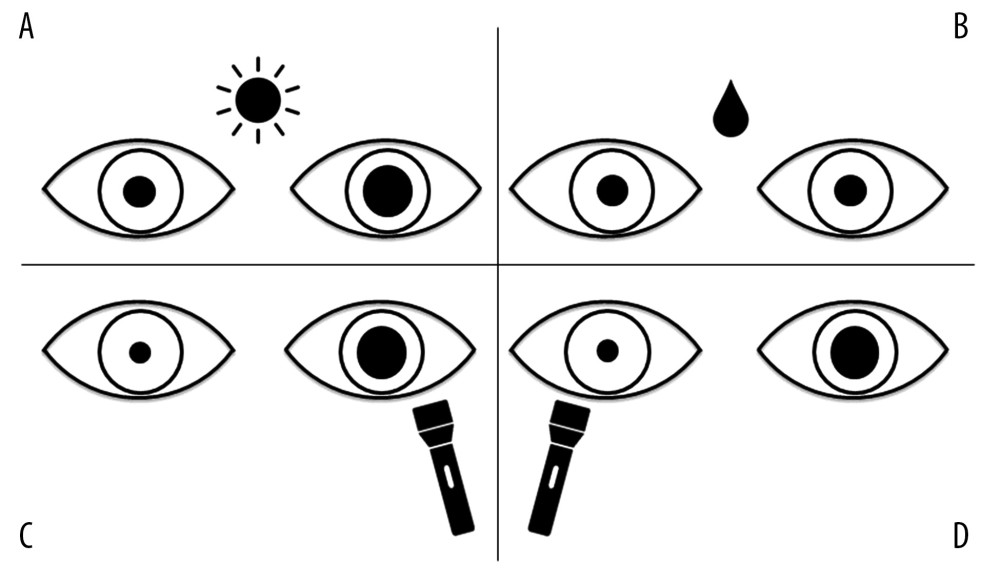 Figure 1. The characteristics of Adie’s pupils. (A) Under natural light, the pupil on the left is significantly larger than the pupil on the right. (B) After 0.125% pilocarpine is applied in both eyes, the left pupil shows obvious contraction; however, the right pupil remains unchanged. (C) On exposure of the left pupil to a flashlight, it remains unchanged, while the right pupil contracts significantly; that is, the direct reflection of light from the left pupil is absent, and the indirect reflection from the right pupil exists. (D) On exposure of the right pupil to the flashlight, it contracts significantly, while the left pupil does not change; that is, direct reflection of light from the right pupil exists, and indirect reflection from the left pupil is absent. The sun symbol represents natural light; the water drop symbol represents the use of pilocarpine applied in the eyes; the flashlight symbol represents the light reflection from the pupil.
Figure 1. The characteristics of Adie’s pupils. (A) Under natural light, the pupil on the left is significantly larger than the pupil on the right. (B) After 0.125% pilocarpine is applied in both eyes, the left pupil shows obvious contraction; however, the right pupil remains unchanged. (C) On exposure of the left pupil to a flashlight, it remains unchanged, while the right pupil contracts significantly; that is, the direct reflection of light from the left pupil is absent, and the indirect reflection from the right pupil exists. (D) On exposure of the right pupil to the flashlight, it contracts significantly, while the left pupil does not change; that is, direct reflection of light from the right pupil exists, and indirect reflection from the left pupil is absent. The sun symbol represents natural light; the water drop symbol represents the use of pilocarpine applied in the eyes; the flashlight symbol represents the light reflection from the pupil. 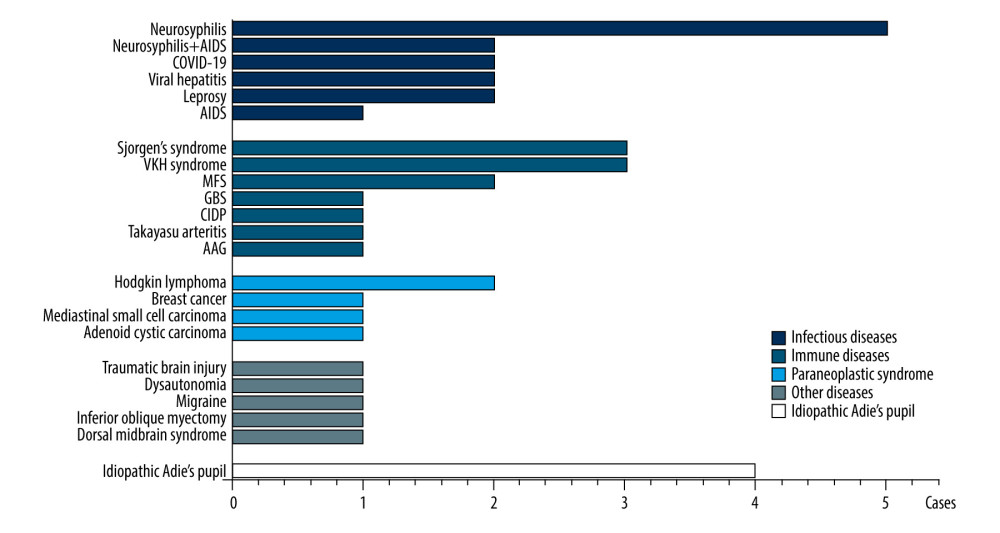 Figure 2. The disease spectrum of Adie’s pupil. AAG – autoimmune autonomic ganglionopathy; AIDS – acquired immunodeficiency syndrome; CIDP – chronic inflammatory demyelinating polyneuropathy; COVID-19 – coronavirus disease 2019; GBS – Guillain-Barre syndrome; IVIg – intravenous immunoglobulin; IVMP – intravenous methylprednisolone; MFS – Miller Fisher syndrome; VKH syndrome – Vogt-Koyanagi-Harada syndrome.
Figure 2. The disease spectrum of Adie’s pupil. AAG – autoimmune autonomic ganglionopathy; AIDS – acquired immunodeficiency syndrome; CIDP – chronic inflammatory demyelinating polyneuropathy; COVID-19 – coronavirus disease 2019; GBS – Guillain-Barre syndrome; IVIg – intravenous immunoglobulin; IVMP – intravenous methylprednisolone; MFS – Miller Fisher syndrome; VKH syndrome – Vogt-Koyanagi-Harada syndrome. 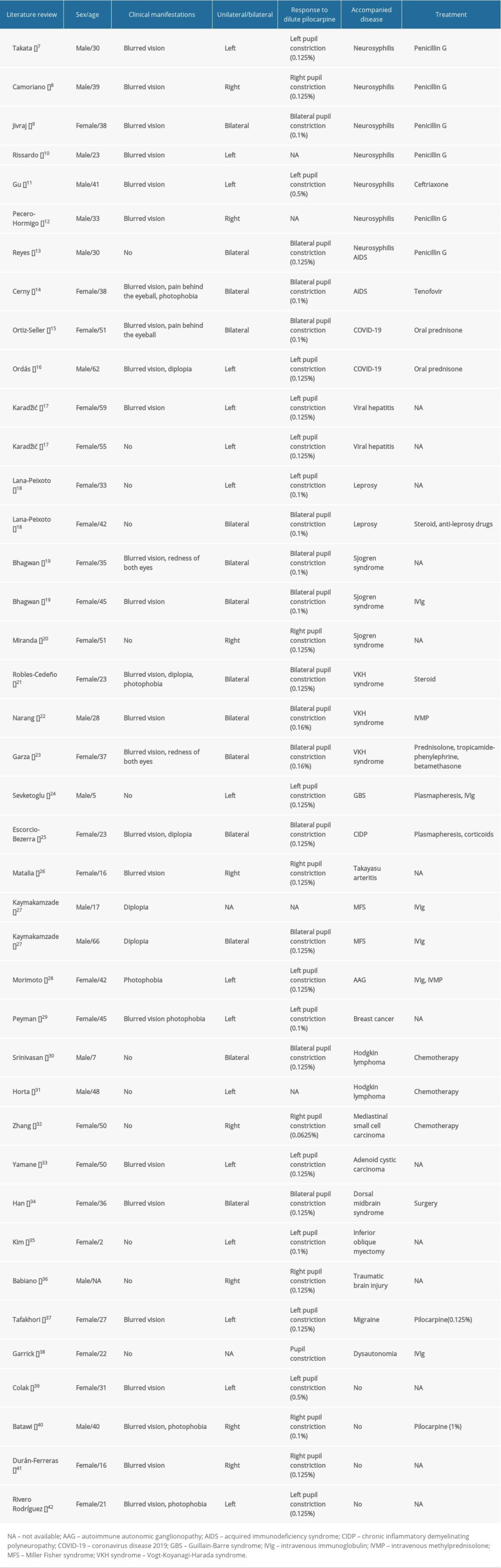
References
1. Bouffard MA, The pupil: Continuum (Minneap Minn), 2019; 25(5); 1194-214
2. Mathot S, Pupillometry: Psychology, physiology, and function: J Cogn, 2018; 1(1); 16
3. Adie WJ, Argyll robertson pupils true and false: Br Med J, 1931; 2(3681); 136-38
4. Adie WJ, Complete and incomplete forms of the benign disorder characterised by tonic pupils and absent tendon reflexes: Br J Ophthalmol, 1932; 16(8); 449-61
5. Bramwell E, The Holmes-Adie syndrome: A benign clinical entity which simulates syphilis of the nervous system: Edinb Med J, 1936; 43(6); T83-92
6. Hagemann G, Bartke T, Images in clinical medicine. Adie’s pupil in the Ross syndrome: N Engl J Med, 2006; 355(6); e5
7. Takata T, Kamada M, Ikeda K, Unilateral mydriatic tonic pupil as an early isolated symptom of neurosyphilis: J Neurol Sci, 2014; 344(1–2); 219-20
8. Camoriano GD, Kassab J, Suchak A, Gimbel HV, Neurosyphilis masquerading as an acute Adie’s tonic pupil: Report of a case: Case Rep Ophthalmol, 2011; 2(2); 205-10
9. Jivraj I, Johnson M, A rare presentation of neurosyphilis mimicking a unilateral Adie’s tonic pupil: Semin Ophthalmol, 2014; 29(4); 189-91
10. Rissardo JP, Caprara ALF, Silveira JOF, Generalized convulsive status epilepticus secondary to Jarisch-Herxheimer reaction in neurosyphilis: A case report and literature review: Neurologist, 2019; 24(1); 29-32
11. Gu X, Guan Z, Chai Z, Zhou P, Unilateral mydriasis as the primary sign of neurosyphilis: Infection, 2014; 42(1); 215-17
12. Pecero-Hormigo MDC, Gonzalez-Tena C, Gaspar-Garcia E, Lopez-Lara LN, Tonic pupil and dermal injuries, Is it just what it seems?: Enferm Infecc Microbiol Clin, 2019; 37(4); 274-75
13. Reyes AJ, Ramcharan K, Aboh S, Giddings SL, Dilated tonic pupils with tabes dorsalis in neurosyphilis as first manifestation of HIV/AIDS: A video report: BMJ Case Rep, 2018; 2018 bcr-2017-223727
14. Cerny R, Rozsypal H, Kozner P, Machala L, Bilateral Holmes-Adie syndrome as an early manifestation of the HIV neuropathy: Neurol Sci, 2010; 31(5); 661-63
15. Ortiz-Seller A, Martinez Costa L, Hernandez-Pons A, Ophthalmic and neuro-ophthalmic manifestations of coronavirus disease 2019 (COVID-19): Ocul Immunol Inflamm, 2020; 28(8); 1285-89
16. Ordas CM, Villacieros-Alvarez J, Pastor-Vivas AI, Corrales-Benitez A, Concurrent tonic pupil and trochlear nerve palsy in COVID-19: J Neurovirol, 2020; 26(6); 970-72
17. Karadzic J, Jakovic N, Kovacevic I, Unilateral Adie’s tonic pupil and viral hepatitis – report of two cases: Srp Arh Celok Lek, 2015; 143(7–8); 451-54
18. Lana-Peixoto MA, Campos WR, Reis PA, Tonic pupil in leprosy: Arq Bras Oftalmol, 2014; 77(6); 395-96
19. Bhagwan S, Bhagwan B, Moodley A, Bilateral tonic pupils as the initial manifestation of Sjogren’s syndrome: Neuroophthalmology, 2015; 39(5); 248-52
20. Miranda Bacallado Y, Gonzalez Hernandez A, Tandon Cardenes LA, Curutchet Mesner LTonic pupil as an initial manifestation of Sjogren’s syndrome: Med Clin (Barc), 2016; 146(11); 515-16 [in Spanish]
21. Robles-Cedeno R, Fures JF, Molins A, A Moroccan patient with Vogt-Koyanagi-Harada syndrome and bilateral Adie’s pupils: Neurol Sci, 2014; 35(3); 483-85
22. Narang S, Sood S, Malik A, Probable Vogt-Koyanagi-Harada’s syndrome associated with tonic pupils: Nepal J Ophthalmol, 2010; 2(2); 154-56
23. Garza Leon M, Herrera-Jimenez IP, Gonzalez-Madrigal PM, Complete Vogt-Koyanagi-Harada disease and Holmes-Adie syndrome: Case report: Ocul Immunol Inflamm, 2014; 22(4); 336-40
24. Sevketoglu E, Tatli B, Tugcu B, An unusual cause of fulminant Guillain-Barre syndrome: Angel’s trumpet: Pediatr Neurol, 2010; 43(5); 368-70
25. Escorcio-Bezerra ML, Manzano GM, Bichuetti DB, Tonic pupils: an unusual autonomic involvement in chronic inflammatory demyelinating polyneuropathy (CIDP): Neurol Sci, 2019; 40(8); 1725-27
26. Matalia J, Kasturi N, Anaspure HD, Shetty BK, Tonic pupil, anterior ischemic optic neuropathy in a teenager with Takayasu arteritis: Can J Ophthalmol, 2013; 48(6); e159-63
27. Kaymakamzade B, Selcuk F, Koysuren A, Pupillary involvement in Miller Fisher syndrome: Neuroophthalmology, 2013; 37(3); 111-15
28. Morimoto N, Takahashi S, Inaba T, A case of seropositive autoimmune autonomic ganglionopathy with diffuse esophageal spasm: J Clin Neurosci, 2017; 39; 90-92
29. Peyman A, Kabiri M, Peyman M, Tonic pupil, a paraneoplastic neuro-ophtalmological disease associated with occult breast cancer: Breast J, 2015; 21(5); 543-44
30. Srinivasan A, Satish G, Scott JX, Two uncommon paraneoplastic neurological syndromes in a child with Hodgkin lymphoma: J Pediatr Hematol Oncol, 2016; 38(6); 473-75
31. Horta E, McKeon A, Lennon VA, Benarroch EE, Reversible paraneoplastic tonic pupil with PCA-Tr IgG and Hodgkin lymphoma: Neurology, 2012; 78(20); 1620-22
32. Zhang L, Luo S, Jin H, Anti-Hu antibody-associated Adie’s pupil and paraneoplastic sensorimotor polyneuropathy caused by primary mediastinal small cell carcinoma: Front Neurol, 2019; 10; 1236
33. Yamane ML, Perez EL, Moonis G, Odel J, Tonic pupil caused by adenoid cystic carcinoma versus postradiation changes to the ciliary ganglion: BMJ Case Rep, 2020; 13(7); e232755
34. Han SW, Ryu JH, Baik JS, Early dorsal midbrain syndrome mimicking an Adie’s tonic pupil: J Clin Neurol, 2010; 6(1); 38-40
35. Kim WJ, Kim MM, Permanent tonic pupil following inferior oblique myectomy: J AAPOS, 2015; 19(2); 193-94
36. Babiano Fernandez MAAdie’s pupil: Aten Primaria, 2020; 52(2); 129-30 [in Spanish]
37. Tafakhori A, Aghamollaii V, Modabbernia A, Pourmahmoodian H, Adie’s pupil during migraine attack: Case report and review of literature: Acta Neurol Belg, 2011; 111(1); 66-68
38. Garrick AO, Jones D, Bowel obstruction and urinary retention in a 22-year-old: Beware the tonic pupil: Surgeon, 2010; 8(3); 172-73
39. Colak S, Erdogan MO, Senel A, A rare case in the Emergency Department: Holmes-Adie syndrome: Turk J Emerg Med, 2015; 15(1); 40-42
40. Batawi H, Micieli JA, Adie’s tonic pupil presenting with unilateral photophobia successfully treated with dilute pilocarpine: BMJ Case Rep, 2020; 13(1); e233136
41. Duran-Ferreras E, Idigoras-Hurtado A, Caballero-Granado JAdie’s pupil: Med Clin (Barc), 2012; 138(15); e29 [in Spanish]
42. Rivero Rodriguez D, Scherle Matamoros C, Pernas Sanchez Y, Adie pupil. Pilocarpine test: Med Clin (Barc), 2018; 151(4); 170
43. Raza HK, Chen H, Chansysouphanthong T, Cui G, The aetiologies of the unilateral oculomotor nerve palsy: A review of the literature: Somatosens Mot Res, 2018; 35(3–4); 229-39
44. Trechot F, Tonnelet R, Conart JB, Mydriasis revealing vascular and osteodural compression of the oculomotor nerve: An observational study on five cases: J Fr Ophtalmol, 2016; 39(6); 491-97
45. McLendon K, Preuss CV, Atropine: StatPearls, 2021, Treasure Island (FL), StatPearls, StatPearls Publishing LLC
46. Chung WM, Chian YY, Azmir A, Datura fruit poisoning: Med J Malaysia, 2018; 73(6); 453-54
47. Dichter SL, Shubert GS, Argyll Robertson pupil: StatPearls, 2021, Treasure Island (FL), StatPearls, StatPearls Publishing LLC
48. Atik S, Koc F, Kaplan YC, Yurtseven SG, Congenital mydriasis: Diagnostic challenge in a case with accompanying neurologic symptoms: Neuroophthalmology, 2014; 38(3); 153-55
Figures
Figure 1. The characteristics of Adie’s pupils. (A) Under natural light, the pupil on the left is significantly larger than the pupil on the right. (B) After 0.125% pilocarpine is applied in both eyes, the left pupil shows obvious contraction; however, the right pupil remains unchanged. (C) On exposure of the left pupil to a flashlight, it remains unchanged, while the right pupil contracts significantly; that is, the direct reflection of light from the left pupil is absent, and the indirect reflection from the right pupil exists. (D) On exposure of the right pupil to the flashlight, it contracts significantly, while the left pupil does not change; that is, direct reflection of light from the right pupil exists, and indirect reflection from the left pupil is absent. The sun symbol represents natural light; the water drop symbol represents the use of pilocarpine applied in the eyes; the flashlight symbol represents the light reflection from the pupil.Figure 2. The disease spectrum of Adie’s pupil. AAG – autoimmune autonomic ganglionopathy; AIDS – acquired immunodeficiency syndrome; CIDP – chronic inflammatory demyelinating polyneuropathy; COVID-19 – coronavirus disease 2019; GBS – Guillain-Barre syndrome; IVIg – intravenous immunoglobulin; IVMP – intravenous methylprednisolone; MFS – Miller Fisher syndrome; VKH syndrome – Vogt-Koyanagi-Harada syndrome. In Press
Clinical Research
Establishment of a Novel Approach for Drug Abuse Monitoring and Its Application in Medical InstitutionsMed Sci Monit In Press; DOI: 10.12659/MSM.952054
Database Analysis
Epidemiology of Incidence and Mortality Due to Head and Neck Cancer in Poland in 2000 to 2022Med Sci Monit In Press; DOI: 10.12659/MSM.952477
Clinical Research
Comparison of Outcomes From Sequential Endoscopic Therapy in 60 Patients With Cirrhosis and Esophagogastric...Med Sci Monit In Press; DOI: 10.12659/MSM.952290
Clinical Research
Impact of a Staged Enteral Nutrition Nursing Pathway Based on Dynamic Assessment of Tolerance and Aspiratio...Med Sci Monit In Press; DOI: 10.12659/MSM.953263
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,688
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,764,843
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,422
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,979
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387