05 September 2022: Clinical Research
Interaction of High-Sugar Diet and History of Stroke with Risk of Cognitive Decline in Older Adults
Qian Xu1AEFG, Sicong Zhang2BCD, Yanqing Gu1C, Ping Wang1D, Qian Zhang1B, Chunlei Shan234AEG*DOI: 10.12659/MSM.937572
Med Sci Monit 2022; 28:e937572






Abstract
BACKGROUND: Cognitive decline has become a public health concern as it causes adverse economic and socio-psychological outcomes. Studies have assessed the effects of history of stroke or high-sugar diet on cognitive decline of older adults, but whether there was interaction between high-sugar diet and history of stroke in affecting cognitive decline was still unclear. The present study explored the interaction between high-sugar diet and history of stroke in affecting the risk of cognitive decline in older adults.
MATERIAL AND METHODS: This cross-sectional study included 2710 subjects. Univariate analysis was applied to explore the associations of high-sugar diet or history of stroke in affecting cognitive decline. The relative excess risk of interaction (RERI), synergy index (SI), and attributable proportion of interaction (API) were used to assess the interaction of high-sugar diet and history of stroke in risk of cognitive decline.
RESULTS: An increased risk of cognitive decline was observed in people with history of stroke [odds ratio (OR)=1.826, 95% confidence interval (CI): 1.124-2.968] and high-sugar diet (OR=1.509, 95% CI: 1.109-2.052). The confidence intervals of interaction indicators RERI=1.257 (95% CI: 0.188-2.326) and API=0.386 (95% CI: 0.135-0.638) did not contain 0 and were both >0; the confidence interval of SI=2.261 (95% CI: 1.063-4.809) did not contain 1 and were >1.
CONCLUSIONS: A high-sugar diet and history of stroke interacted synergically in association with cognitive decline in older adults, which might provide a reference for management of cognition in older adults.
Keywords: Cognition, Frail Elderly, Stroke, sugars, Aged, Cross-Sectional Studies, Diet, Humans
Background
As one of the vital elements of health status, cognitive function is an essential determinant of independence, daily living ability, and quality of life, especially in older adults [1]. Brain aging may increase the risk of behavioral dysfunction and cognitive decline, which is a common geriatric syndrome in older adults, with an increased prevalence in Chinese adults aged ≥60 years [2]. Cognitive decline has become a public health concern as it brings adverse economic and socio-psychological outcomes [3,4]. Cognitive decline decreases the quality of life and the ability to perform instrumental activities of daily living, which is thought to be the precursor symptom of dementia [5,6]. Therefore, cognitive decline in older adults is of great importance.
Cognitive decline is a major medical outcome after stroke, and patients who have had stroke have increased risk of cognitive decline compared to those without stroke [7]. Levine et al found that cognitive decline can occur immediately or sometime later after stroke [8]. Previous studies demonstrated that 38% of stroke survivors had cognitive impairment 1 year after stroke, and dementia occurred in about 10% of stroke survivors in the first year after stroke and in one-third within 3 years of initial stroke [9,10]. Previously, several studies revealed that excessive sugar consumption may lead to impaired memory and increased risk of dementia [11]. Ye et al found that higher sugar intake was associated with lower cognitive performance among middle-aged and older people [12]. A meta-analysis showed that high sugar intake was negatively correlated to overall memory, executive function, and psychomotor speed, and was positively associated with neurological disorders in older people [13]. Increasing evidence shows that excessive sugar consumption can increase the risk of stroke [14]. Some other studies indicated that excessive sugar intake is associated with elevated risk of stroke and dementia [15,16]. These findings suggest an association between dietary sugar and stroke. Studies have found the effects of history of stroke and high-sugar diet on cognitive performance in older adults, but whether there was an interaction between high-sugar diet and history of stroke in cognitive decline was still unclear.
The present study explored the roles of history of stroke and high-sugar diet, as well as the interaction between high-sugar diet and history of stroke, on the risk of cognitive decline in older adults based on the data from National Health and Nutrition Examination Survey (NHANES). Our results may offer a reference for sugar intake in patients with a history of stroke in the management of their cognitive performance.
Material and Methods
STUDY DESIGN AND POPULATION:
In this cross-sectional study, the data of 2937 older adults were extracted from NHANES 2-year cycles (2011–2012 and 2013–2014) as the 2 cycles specifically inquired about cognition [17]. NHANES is conducted by the US Centers for Disease Control and Prevention (CDC), which performs ongoing 2-year-cycle cross-sectional surveys involving more than 5000 participants each year from 15 different locations in US counties based on a complex, multi-stage probability sampling design [17]. NHANES examines the health and nutritional status of the non-institutional population in the US. The survey obtained approval from the Research Ethics Review Board at the National Center for Health Statistics. After excluding people without data on cognition, history of stroke, and high-sugar diet, 2710 subjects were included – 1032 had cognitive decline and 1678 had no cognitive decline. NHANES was approved by the NCHS Research Ethics Review Board (ERB) [Approval number: 2011–2012 (Protocol #2011–17) and 2012–2014 (Continuation of Protocol #2011–17)] (https://www.cdc.gov/nchs/nhanes/irba98.htm). As there were no samples from our own hospital, the study was exempted from ethics review by the Institutional Review Board of Shanghai Second Rehabilitation Hospital.
DATA COLLECTION:
The data analyzed in this study included age (years), gender, the amount of added sugars consumed (normal or high level), race (Mexican American, Non-Hispanic White, Non-Hispanic Black, or other race), body mass index (BMI, kg/m2), marital status (married, widowed/divorced, unmarried or cohabitation), education (less than high school, high school, or more than high school), family annual income ($), sleep disorder, sleep duration (h), smoker, drinker, vigorous work activity (vigorous-intensity activities, moderate-intensity activities or others), vigorous recreational activities (vigorous-intensity activities, moderate-intensity activities or others), depression, hypertension, diabetes, congestive heart failure (CHF; yes or no), coronary heart disease (CHD; yes or no), heart disease (yes or no), total cholesterol (TC; Mgd/L), high-density lipoprotein (HDL; Mgd/L), glycosylated hemoglobin (GHb;%), and history of stroke (yes or no).
DEFINITION OF VARIABLES:
Vigorous work activity indicated the time spent doing different types of physical activity in a typical week, the time spent doing work such as paid or unpaid work, studying or training, household chores, and yard work. Vigorous-intensity activities referred to activities that require hard physical effort and cause large increases in breathing or heart rate, and moderate-intensity activities referred to activities that require moderate physical effort and cause small increases in breathing or heart rate. Vigorous recreational activities included sports, fitness, and recreational activities. Vigorous-intensity sports, fitness, or recreational activities referred to activities that cause large increases in breathing or heart rate, like running or basketball, for at least 10 min continuously.
“Added sugars” was defined as sugars added to foods as an ingredient during preparation, processing, or at the table. Added sugars do not include naturally occurring sugars (eg, lactose in milk and fructose in fruits). The amount of added sugars=added sugars (teaspoon/day)×4.2 (g/teaspoon)×3.87(kcal/g)/kcal (kcal/day)×100 (%). The amount of added sugars was dichotomized and stratified, and added sugars higher than the 75th quantile (weighted) was defined as high added sugars.
The word learning and recall modules from the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) was applied for assessing the immediate and delayed learning ability of new language information (memory subdomain). The CERAD test includes 3 consecutive learning trials and 1 delayed recall. Participants were asked to recall words after learning the test. The score was 0–10 points, with 1 point for each correct answer. The CERAD score was the sum of the 4 tests [18]. The DSST was applied to evaluate the sustained attention and working memory. Participants should match the numbers in 133 boxes to the corresponding symbols within 120 s The score was 133 points and each of correct match scored 1 point [19]. The Animal Fluency test was employed for testing absolute language fluency. Participants should name as many animals as possible within a minute, and each answer was scored 1 point [20]. Cognitive decline was defined based on the 25th percentile of the combined scores of the CERAD, the DSST, and Animal Fluency test, and the lowest quartile was set as the cut-off point. As age has a significant effect on cognitive performance, the score was further categorized based on age (60 years to <70 years, 70 years to <80 years, and ≥80 years). For each cognitive test, scores lower than the lowest quartile in each age group were defined as cognitive decline.
THE ADDITIVE INTERACTION MODEL:
The relative excess risk of interaction (RERI), attributable proportion of interaction (API), and synergy index (SI) were indexes assessing the interaction between a high-sugar diet and history of stroke in affecting the risk of cognitive decline according to the additive model. RERI=R11−R10−R01+1: represents the difference between the sum of the combined effects of the 2 factors and the sum of the separate effects, which reveals the risk degree of interaction in comparison with all other factors except the 2 factors. API=RERI/R11: represents the proportion of total effects attributed to interaction. SI=R11 (R10×R01): the meaning is the same as RERI. When 0 was involved in the confidence intervals (CIs) of RERI and API and 1 was included in the CIs of SI indicates that no interaction was found.
STATISTICAL ANALYSIS:
Mean±standard error (SE) was applied for displaying the measurement data with normal distribution and comparisons in groups were subjected to independent sample
Results
COMPARISONS OF THE CHARACTERISTICS BETWEEN PEOPLE WITH AND WITHOUT COGNITIVE DECLINE:
This study extracted the data of 2937 older adults. We excluded those without data on cognitive decline (n=695), and those with history of stroke (n=5) and added sugars (n=222). Finally, 2710 subjects were enrolled and grouped into a cognitive decline group (n=1032) and a non-cognitive decline group (1678) (Figure 1). The average age was 69.10 years. The proportions of alcohol consumption (36.74% vs 23.72%), depression (13.35% vs 5.13%), hypertension (65.55% vs 56.64%), and heart failure (10.45% vs 5.79%) in the cognitive decline group were higher than the non-cognitive decline group (all P<0.05) (Table 1). Figure 2 shows the distributions of people with high or normal added sugar in the cognitive decline group and non-cognitive decline group, as well as people with or without history of stroke in the cognitive decline group and non-cognitive decline group.
THE ASSOCIATIONS OF HISTORY OF STROKE OR THE AMOUNT OF ADDED SUGAR WITH COGNITIVE DECLINE:
The associations between a history of stroke or high-sugar diet with cognitive decline are displayed in Table 2. The crude model revealed that a history of stroke or high-sugar diet might be related to increased risk of cognitive decline. After adjustment for age, gender, diabetes, and GHb, we found that history of stroke (OR=2.151, 95% CI: 1.428–3.240) or high-sugar diet (OR=1.864, 95% CI: 1.418–2.451) were associated with increased risk of cognitive decline. The increased risk of cognitive decline was observed in people with history of stroke (OR=1.826, 95% CI: 1.124–2.968) and high added sugar (OR=1.509, 95% CI: 1.109–2.052) in the adjusted model for age, gender, diabetes, GHb, BMI, race, marital status, education, family income, drinking, vigorous work activity, vigorous recreational activities, depression disorder, hypertension, congestive heart failure, heart disease, TC, and HDL.
INTERACTION BETWEEN HISTORY OF STROKE AND HIGH-SUGAR DIET IN DETERMINING THE RISK OF COGNITIVE DECLINE:
The additive interaction terms of a history of stroke and high added sugar included normal amount of added sugars and no history of stroke, normal amount of added sugars and a history of stroke, large amount of added sugars and no history of stroke, and large amount of added sugar and a history of stroke. The sample size of each interaction term was presented in Table 3. After adjusting for age, gender, diabetes, and GHb, people with normal amount of added sugar and a history of stroke had a 1.749-fold higher risk of cognitive decline (OR=1.749, 95% CI: 1.217–2.516). large amount of added sugar and no history of stroke was associated a 1.691-fold higher risk of cognitive decline (OR=1.691, 95% CI: 1.264–2.264). Large amount of added sugar and a history of stroke was linked with a 5.326-fold higher risk of cognitive decline (OR=5.326, 95% CI: 2.236–12.685). In the adjusted model for age, gender, diabetes, GHb, BMI, race, marital status, education, family income, drinking, vigorous work activity, vigorous recreational activities, depression disorder, hypertension, congestive heart failure, heart disease, TC, and HDL, compared with people with normal amount of added sugar and no history of stroke, people with normal amount of added sugar and history of stroke (OR=1.598, 95% CI: 1.010–2.529), large amount of added sugar and no history of stroke (OR=1.399, 95% CI: 1.005–1.946), as well as people with large amount of added sugar and history of stroke (OR=3.254, 95% CI: 1.098–9.641) were linked had higher risk of cognitive decline.
The confidence intervals of interaction indicators RERI=1.257 (95% CI: 0.188–2.326) and API=0.386 (95% CI: 0.135–0.638) did not contain 0 and were both >0; the confidence interval of SI=2.261 (95% CI: 1.063–4.809) did not contain 1 and were >1. This suggested that there was synergistic interaction between consuming a large amount of added sugar and a history of stroke in affecting cognitive decline after adjusting for confounders. The API was 0.386, indicating that 38.6% of people with cognitive decline was attributed to consuming a large amount of added sugar and a history of stroke (Table 4). The visualization results of the ORs of interaction terms in Model 1, Model 2, and Model 3 are shown in Figure 3A–3C.
Subgroup analysis concerning differences in education level revealed that no significant association was found in amount of added sugar and history of stroke with cognitive decline in people with less than high school education level (P>0.05). In people with high school education level, large amount of added sugar and history of stroke was associated with increased risk of cognitive decline (OR=26.199, 95% CI: 2.169–346.516). In people with more than high school education level, history of stroke was linked with increased risk of cognitive decline (OR=2.233, 95% CI: 1.159–4.299). The interaction of large amount of added sugar and history of stroke on the risk of cognitive decline in people with different education levels was no statistically different (P>0.05) (Supplementary Table 1).
Discussion
This study collected the data of 2710 people from NHANES to evaluate the interaction between high-sugar diet and history of stroke in affecting cognitive decline of older adults. The results found that the risk of cognitive decline in older adults might be increased in people with a large amount of added sugar or a history of stroke. High intake of added sugar and history of stroke had a synergistic interaction in affecting risk of cognitive decline. Our results suggest that people with history of stroke should limit their dietary intake of sugar.
Refined sugar is a main part of the modern human diet and interest in studying the effects of sugar consumption on cognitive performance has been increasing in recent years [21,22]. In our study, high intake of added sugar was associated with increased risk of cognitive decline, as supported by previous studies. Yeomans found that high dietary intake of sugar had adverse effects on the human cognition [23]. Chong et al recruited 1209 subjects aged ≥60 years through multi-stage random sampling in Malaysia to evaluate the association between habitual sugar intake and cognitive impairment, which found excessive sugar consumption was linked with poor cognitive function among older adults [24]. These results suggested that controlling sugar intake in older adults could help prevent cognitive decline. Several studies have indicated that glycemic status is associated with cognitive decline in older adults, and higher glycated hemoglobin (A1c) values can cause a higher risk of cognitive impairment and an accelerated rate of cognitive decline [25,26]. This may be the potential mechanism underlying the association between high-sugar diet and cognitive decline in older adults. A recent meta-analysis of 9 longitudinal hospital-based cohorts found that patients with a history of stroke experienced significantly faster cognitive decline than those without stroke history [27]. Hreha et al reported that cognitive decline can occur immediately or sometimes after stroke, and the prevalence of cognitive decline was higher in stroke survivors than those without a stroke history [28]. These studies support the findings of our study, which showed that compared to people without a history of stroke, the risk of cognitive decline was higher in those with a history of stroke.
Another interesting finding in our study was that high-sugar diet and history of stroke had a synergistic effect on cognitive decline. A prospective cohort study found that sugar in beverages increased the risk of dementia by 1.80-fold, and stroke by 1.11-fold [29]. It was reported that prediabetes was associated with post-stroke cognitive impairment in patients with stroke [30]. These findings suggest an interaction between high-sugar diet and history of stroke in affecting cognitive decline. A possible mechanism may be that a high-sugar diet affects hippocampal-dependent forms of cognitive performance through neuro-inflammation and increasing the expression of pro-inflammatory cytokines, such as interleukin-1β, tumor necrosis factor-α (TNF-α), and the marker of glial cell activation [glial fibrillary acidic protein (GFAP)] [13, 31]. A high-sugar diet might reduce the long-term potentiation in hippocampal pyramidal neurons and affect neuroplasticity [32,33]. In people with a history of stroke, a high-sugar diet might aggravate the pro-inflammatory processes and neuroplasticity in the brain, leading to increased ischemic damage [34]. The findings of our study emphasize the importance of controlling the dietary intake of refined sugar in stroke patients.
In previous studies, education and income were reported to impact cognitive performance in people aged ≥50 years [35]. A systematic review indicated that individuals had cognitive impairment during the first episode of depression and those with multiple episodes showed more severe cognitive impairment [36]. Physical activities were also found to be linked with higher cognitive performance, especially in attention and memory [37]. Age and gender were frequently identified as factors associated with cognitive decline [38]. Cognitive dysfunction might be an emerging complication of diabetes mellitus [39]. These studies suggested that these factors might be confounding variables affecting the results of our study. In the current study, we adjusted confounding variables in 2 models, one adjusted for age, gender, diabetes and GHb, and another adjusted for age, gender, diabetes, GHb, BMI, race, marital status, education, family income, drinking, vigorous work activity, vigorous recreational activities, depression disorder, hypertension, congestive heart failure, heart disease, TC, and HDL, to obtain more reliable results. Considering the association of education with cognitive decline, subgroup analysis was performed in patients with different levels of education. High dietary intake of sugar and history of stroke were associated with increased risk of cognitive decline in people with high school education, and history of stroke was linked with increased risk of cognitive decline in people with more than high school education.
Given the increasing global impact of cognitive decline, early interventions and treatments are required in the management of older adults, especially those with a history of stroke. Our study identified a synergistic interaction between high dietary intake of sugar and history of stroke in affecting cognitive decline in older adults, which might provide a reference for dietary sugar intake in older adults. This suggests that older adults with a history of stroke should control their dietary sugar intake. There were several limitations of the present study. First, some variables such as social support and rehabilitation after stroke, which might affect cognitive decline in older adults, were not included due to limitations of the NHANES database. Second, this was a cross-sectional study, so we could only assess the association of high dietary intake of sugar or history of stroke with cognitive decline of older adults, and a cause-effect association could not be deduced. The results of the current study require validation in prospective studies.
Conclusions
The interaction between high dietary intake of sugar and history of stroke in affecting cognitive decline of older adults was evaluated based on the data of 2710 people from the NHANES database. The data revealed that the risk of cognitive decline in older adults is higher in people with high dietary intake of sugar or history of stroke. High dietary intake of sugar and history of stroke had a synergistic effect on cognitive decline. The findings of our study might help deepen understanding of the association of high-sugar diet and history of stroke with cognitive decline in older adults.
Figures
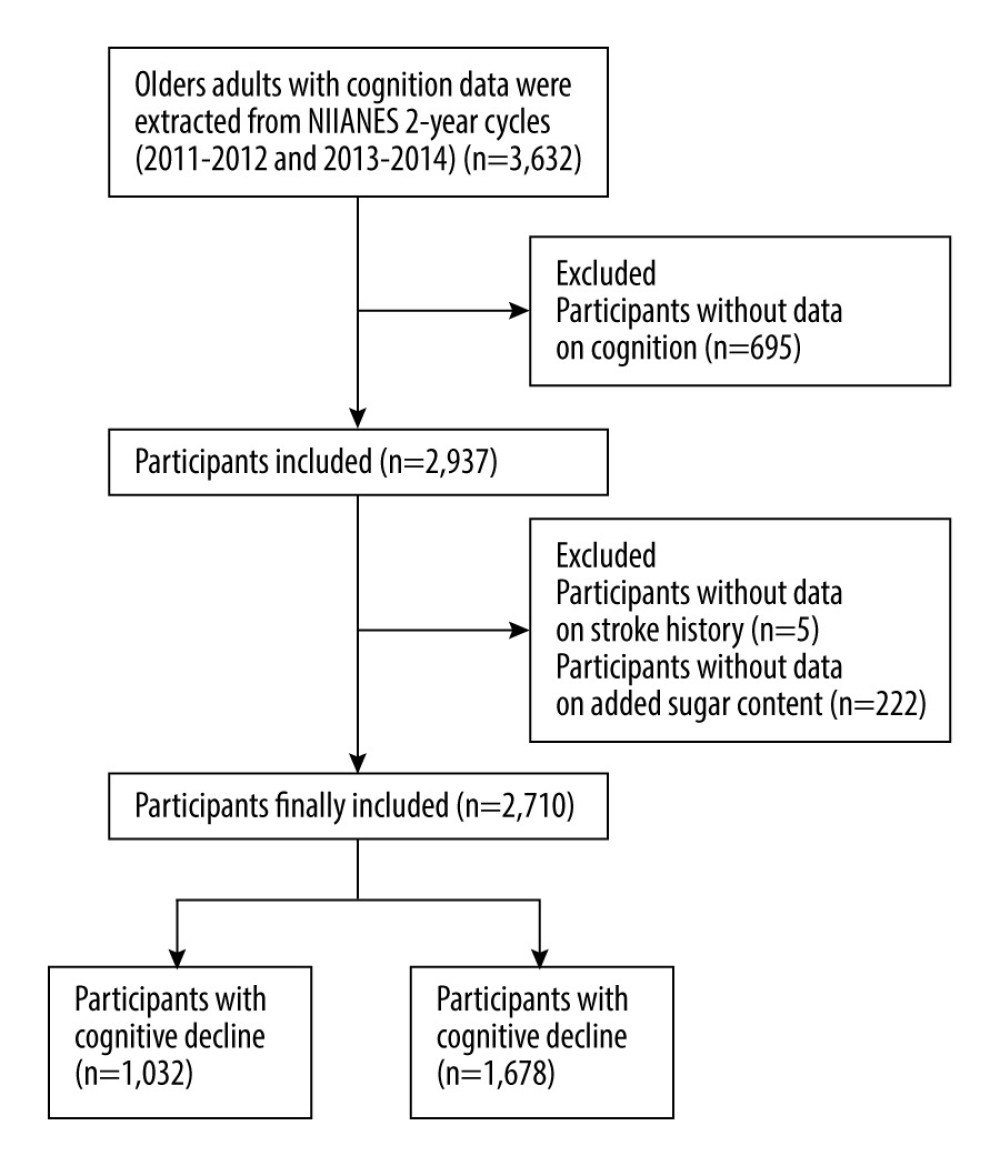 Figure 1. The screen process of the participants. The figure was plotted via GraphPad Prism 8 (GraphPad Software, San Diego, California, USA).
Figure 1. The screen process of the participants. The figure was plotted via GraphPad Prism 8 (GraphPad Software, San Diego, California, USA). 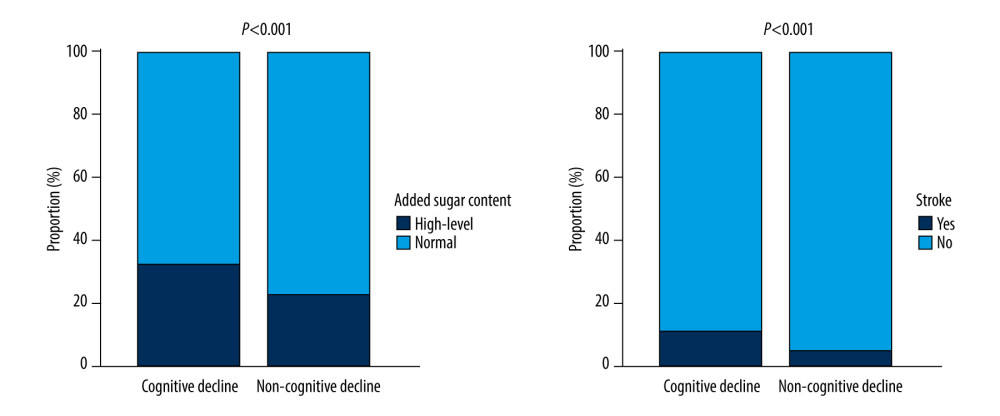 Figure 2. The proportions of people in the cognitive decline group with high or normal consumption of added sugar as well people with or without history of stroke. The figure was plotted via GraphPad Prism 8 (GraphPad Software, San Diego, California, USA).
Figure 2. The proportions of people in the cognitive decline group with high or normal consumption of added sugar as well people with or without history of stroke. The figure was plotted via GraphPad Prism 8 (GraphPad Software, San Diego, California, USA). 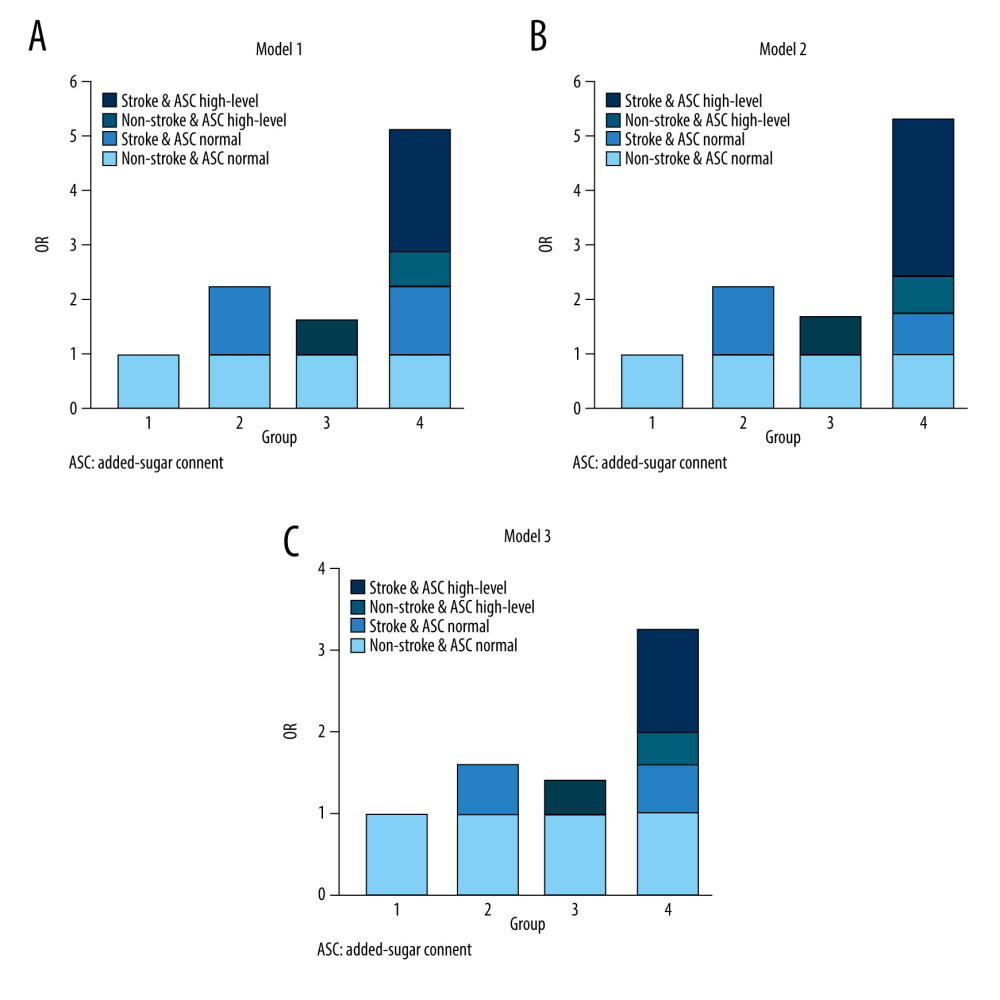 Figure 3. The OR values of interaction between amount of added sugar consumed and history of stroke in affecting cognitive decline of older adults in Model 1 (A), Model 2 (B), and Model 3 (C). The figure was plotted via GraphPad Prism 8 (GraphPad Software, San Diego, California, USA).
Figure 3. The OR values of interaction between amount of added sugar consumed and history of stroke in affecting cognitive decline of older adults in Model 1 (A), Model 2 (B), and Model 3 (C). The figure was plotted via GraphPad Prism 8 (GraphPad Software, San Diego, California, USA). Tables
Table 1. The characteristics of participants with and without cognitive decline.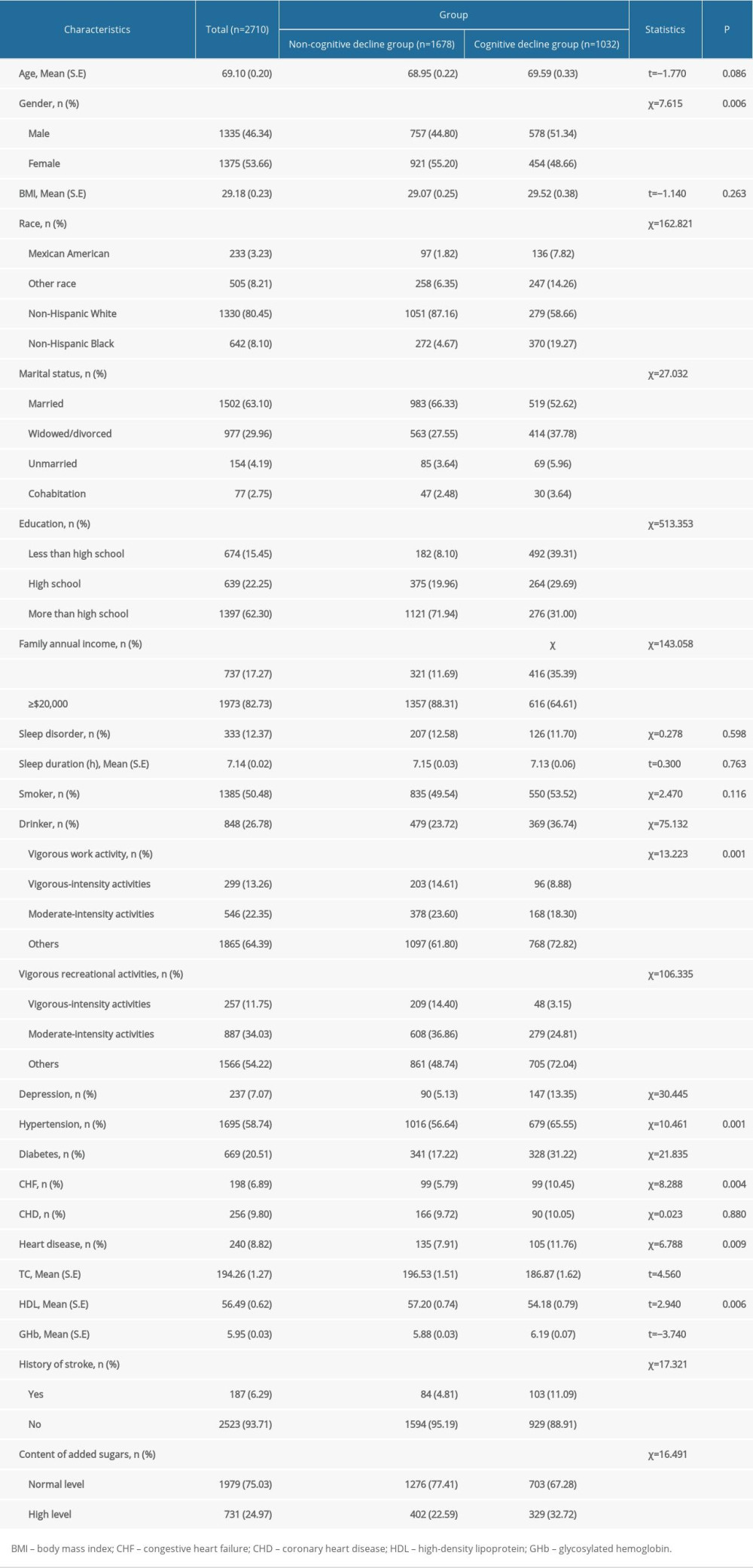 Table 2. The associations of history of stroke or high-sugar diet with cognitive decline.
Table 2. The associations of history of stroke or high-sugar diet with cognitive decline.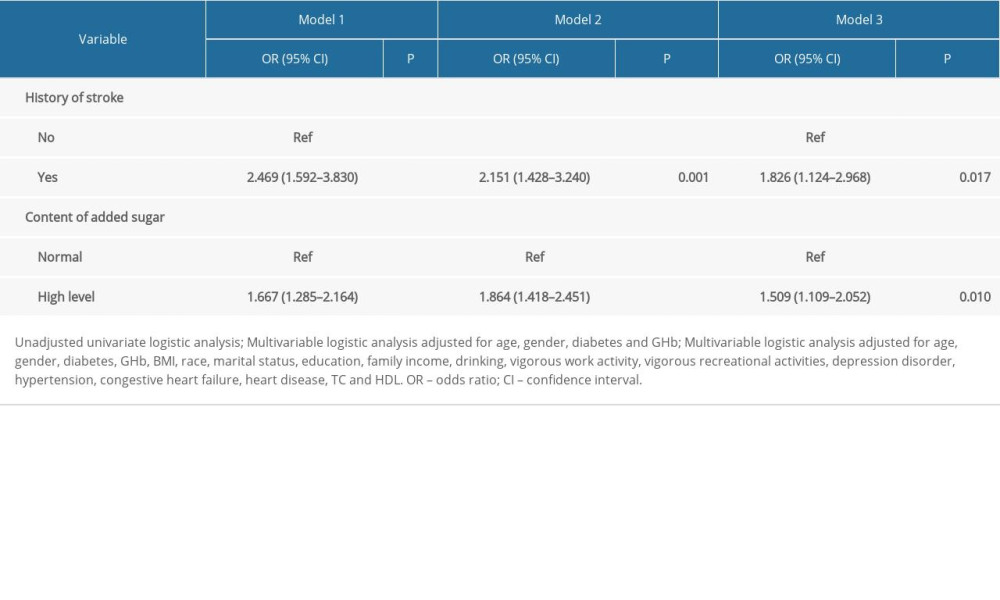 Table 3. The sample size of each interaction term.
Table 3. The sample size of each interaction term.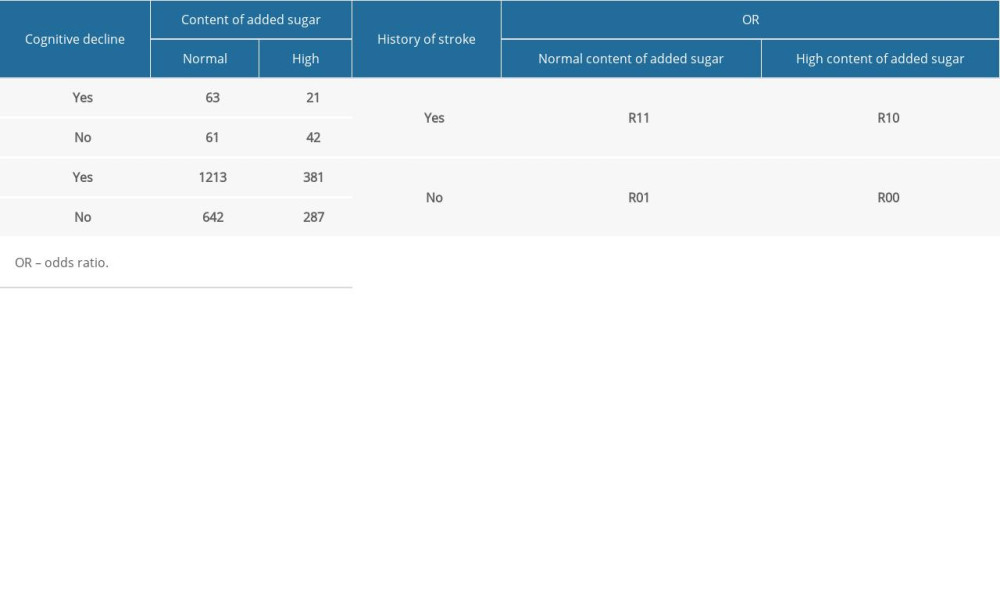 Table 4. Interaction between a history of stroke and high-sugar diet on cognitive decline.
Table 4. Interaction between a history of stroke and high-sugar diet on cognitive decline.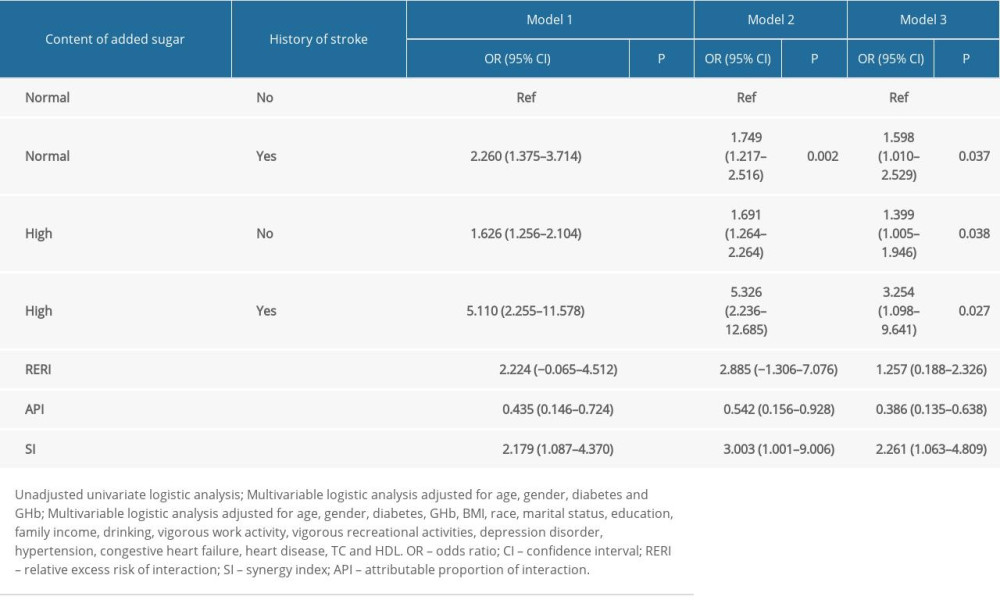 Supplementary Table 1. Interaction between a history of stroke and high-sugar diet in affecting cognitive decline in people with different education levels.
Supplementary Table 1. Interaction between a history of stroke and high-sugar diet in affecting cognitive decline in people with different education levels.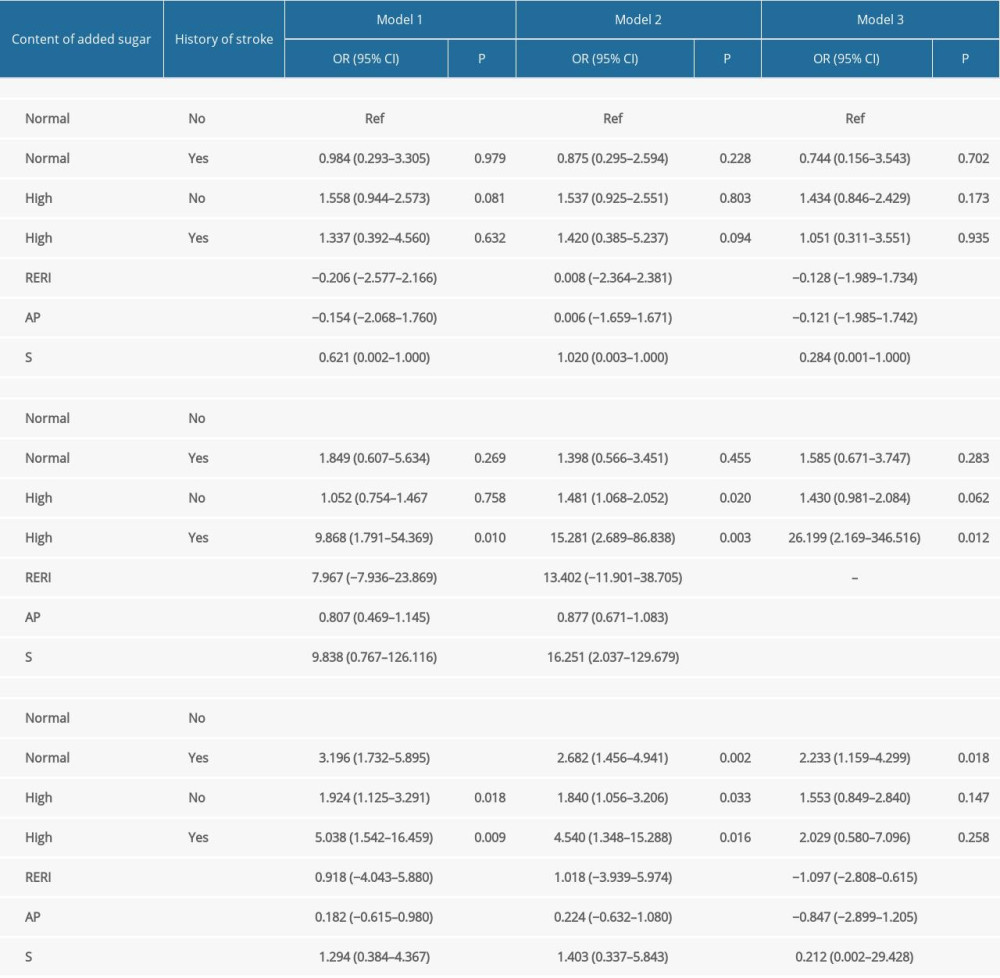
References
1. Yang L, Cheng J, Wang H, Place of residence and cognitive function in older adults in China: The mediating role of social participation: Int J Environ Res Public Health, 2021; 19(1); 13
2. Xue J, Li J, Liang J, Chen S, The prevalence of mild cognitive impairment in China: A systematic review: Aging Dis, 2018; 9; 706-15
3. Huang G, Ren G, Interaction between ω-6 fatty acids intake and blood cadmium on the risk of low cognitive performance in older adults from National Health and Nutrition Examination Survey (NHANES) 2011–2014: BMC Geriatr, 2022; 22(1); 292
4. Han K, Jia W, Wang S, Synergistic impact of body mass index and cognitive function on all-cause mortality in older adults: A nationwide longitudinal study: Front Endocrinol, 2021; 12; 620261
5. Zhang W, Liu S, Sun F, Dong X, Neighborhood social cohesion and cognitive function in U.S. Chinese older adults-findings from the PINE study: Aging Ment Health, 2019; 23; 1113-21
6. Lee J, Sung J, Choi M, The factors associated with subjective cognitive decline and cognitive function among older adults: J Adv Nurs, 2020; 76; 555-65
7. Hbid Y, Fahey M, Wolfe CDA, Risk prediction of cognitive decline after stroke: J Stroke Cerebrovasc Dis, 2021; 30; 105849
8. Levine DA, Galecki AT, Langa KM, Trajectory of cognitive decline after incident stroke: JAMA, 2015; 314(1); 41-51
9. Sexton E, McLoughlin A, Williams DJ, Systematic review and meta-analysis of the prevalence of cognitive impairment no dementia in the first year post-stroke: Eur Stroke J, 2019; 4; 160-71
10. Jeffares I, Rohde D, Doyle F, The impact of stroke, cognitive function and post-stroke cognitive impairment (PSCI) on healthcare utilisation in Ireland: A cross-sectional nationally representative study: BMC Health Serv Res, 2022; 22; 414
11. Crichton GE, Elias MF, Torres RV, Sugar-sweetened soft drinks are associated with poorer cognitive function in individuals with type 2 diabetes: The Maine-Syracuse Longitudinal Study: Br J Nutr, 2016; 115; 1397-405
12. Ye X, Gao X, Scott T, Tucker KL, Habitual sugar intake and cognitive function among middle-aged and older Puerto Ricans without diabetes: Br J Nutr, 2011; 106; 1423-32
13. Abbott KN, Arnott CK, Westbrook RF, Tran DMD, The effect of high fat, high sugar, and combined high fat-high sugar diets on spatial learning and memory in rodents: A meta-analysis: Neurosci Biobehav Rev, 2019; 107; 399-421
14. Wang Y, Zhao R, Wang B, The dose-response associations of sugar-sweetened beverage intake with the risk of stroke, depression, cancer, and cause-specific mortality: A systematic review and meta-analysis of prospective studies: Nutrients, 2022; 14(4); 777
15. Wersching H, Gardener H, Sacco RL, Sugar-sweetened and artificially sweetened beverages in relation to stroke and dementia: Are soft drinks hard on the brain?: Stroke, 2017; 48(5); 1129-31
16. Pase MP, Himali JJ, Beiser AS, Sugar- and artificially sweetened beverages and the risks of incident stroke and dementia: A prospective cohort study: Stroke, 2017; 48(5); 1139-46
17. (NCHS) NCfHS https://www.cdc.gov/nchs/nhanes/about_nhanes
18. Xu H, Wang S, Gao F, Li C, Vitamin B(6), B(9), and B(12) intakes and cognitive performance in elders: National Health and Nutrition Examination Survey, 2011–2014: Neuropsychiatr Dis Treat, 2022; 18; 537-53
19. Liu S, Chen X, MedDiet adherence score for the association between inflammatory markers and cognitive performance in the elderly: A study of the NHANES 2011–2014: BMC Geriatr, 2022; 22(1); 511
20. Koning R, Eltchaninoff H, Commeau P, Stent placement compared with balloon angioplasty for small coronary arteries: In-hospital and 6-month clinical and angiographic results: Circulation, 2001; 104(14); 1604-8
21. Mizera J, Kazek G, Niedzielska-Andres E, Pomierny-Chamiolo L, Maternal high-sugar diet results in NMDA receptors abnormalities and cognitive impairment in rat offspring: FASEB J, 2021; 35; e21547
22. Hartmann H, Pauli LK, Janssen LK, Preliminary evidence for an association between intake of high-fat high-sugar diet, variations in peripheral dopamine precursor availability and dopamine-dependent cognition in humans: J Neuroendocrinol, 2020; 32; e12917
23. Yeomans MR, Adverse effects of consuming high fat-sugar diets on cognition: implications for understanding obesity: Proc Nutr Soc, 2017; 76; 455-65
24. Chong CP, Shahar S, Haron H, Din NC, Habitual sugar intake and cognitive impairment among multi-ethnic Malaysian older adults: Clin Interv Aging, 2019; 14; 1331-42
25. Mansur RB, Lee Y, Zhou AJ, Determinants of cognitive function in individuals with type 2 diabetes mellitus: A meta-analysis: Ann Clin Psychiatry, 2018; 30; 38-50
26. Zheng F, Yan L, Yang Z, HbA(1c), diabetes and cognitive decline: The English Longitudinal Study of Ageing: Diabetologia, 2018; 61; 839-48
27. Lo JW, Crawford JD, Desmond DW, Long-term cognitive decline after stroke: An individual participant data meta-analysis: Stroke, 2022; 53; 1318-27
28. Hreha KP, Downer B, Ehrlich JR, Association between vision impairment and cognitive decline in older adults with stroke: Health and Retirement Study: Aging Clin Exp Res, 2021; 33; 2605-10
29. Miao H, Chen K, Yan X, Chen F, Sugar in beverage and the risk of incident dementia, Alzheimer’s disease and stroke: A prospective cohort study: J Prev Alzheimer’s Dis, 2021; 8; 188-93
30. Wang Q, Zhao K, Cai Y, Prediabetes is associated with post-stroke cognitive impairment in ischaemic stroke patients: Brain Res, 2018; 1687; 137-43
31. Che H, Zhou M, Zhang T, Comparative study of the effects of phosphatidylcholine rich in DHA and EPA on Alzheimer’s disease and the possible mechanisms in CHO-APP/PS1 cells and SAMP8 mice: Food Funct, 2018; 9; 643-54
32. Morin JP, Rodríguez-Durán LF, Guzmán-Ramos K, Palatable hyper-caloric foods impact on neuronal plasticity: Front Behav Neurosci, 2017; 11; 19
33. Spinelli M, Fusco S, Mainardi M, Brain insulin resistance impairs hippocampal synaptic plasticity and memory by increasing GluA1 palmitoylation through FoxO3a: Nat Commun, 2017; 8; 2009
34. Shukla V, Shakya AK, Perez-Pinzon MA, Dave KR, Cerebral ischemic damage in diabetes: An inflammatory perspective: J Neuroinflammation, 2017; 14; 21
35. Rodriguez FS, Hofbauer LM, Röhr S, The role of education and income for cognitive functioning in old age: A cross-country comparison: Int J Geriat Psychiatry, 2021; 36(12); 1908-21
36. Varghese S, Frey BN, Schneider MA, Functional and cognitive impairment in the first episode of depression: A systematic review: Acta Psychiatr Scand, 2022; 145(2); 156-85
37. Lee SY, Pang BWJ, Lau LK, Cross-sectional associations of housework with cognitive, physical and sensorimotor functions in younger and older community-dwelling adults: The Yishun Study: BMJ Open, 2021; 11(11); e052557
38. Hu X, Gu S, Zhen X, Trends in cognitive function among chinese elderly from 1998 to 2018: An age-period-cohort analysis: Front Public Health, 2021; 9; 753671
39. Pignalosa FC, Desiderio A, Mirra P, Diabetes and cognitive impairment: A role for glucotoxicity and dopaminergic dysfunction: Int J Mol Sci, 2021; 22(22); 12366
Figures
Figure 1. The screen process of the participants. The figure was plotted via GraphPad Prism 8 (GraphPad Software, San Diego, California, USA).Figure 2. The proportions of people in the cognitive decline group with high or normal consumption of added sugar as well people with or without history of stroke. The figure was plotted via GraphPad Prism 8 (GraphPad Software, San Diego, California, USA).Figure 3. The OR values of interaction between amount of added sugar consumed and history of stroke in affecting cognitive decline of older adults in Model 1 (A), Model 2 (B), and Model 3 (C). The figure was plotted via GraphPad Prism 8 (GraphPad Software, San Diego, California, USA). Tables
Table 1. The characteristics of participants with and without cognitive decline.Table 2. The associations of history of stroke or high-sugar diet with cognitive decline.Table 3. The sample size of each interaction term.Table 4. Interaction between a history of stroke and high-sugar diet on cognitive decline.Table 1. The characteristics of participants with and without cognitive decline.Table 2. The associations of history of stroke or high-sugar diet with cognitive decline.Table 3. The sample size of each interaction term.Table 4. Interaction between a history of stroke and high-sugar diet on cognitive decline.Supplementary Table 1. Interaction between a history of stroke and high-sugar diet in affecting cognitive decline in people with different education levels. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387