19 September 2022: Clinical Research
Circulating Methylated DNA Analyses to Predict Recurrence Risk and Adjuvant Chemotherapy Benefit in Stage II to III Colorectal Cancer
Zhen Yuan12ABCDEF, Shuyuan Wang12ABCDEF, Kemin NiDOI: 10.12659/MSM.937757
Med Sci Monit 2022; 28:e937757






Abstract
BACKGROUND: We aimed to evaluate the ability of circulating cell-free methylated SETP9 DNA (mSEPT9) to identify recurrence and to determine its clinical utility in adjuvant chemotherapy (ACT) regimen decisions.
MATERIAL AND METHODS: This study enrolled 426 patients with stage II-III CRC who received radical resection between January 8, 2018, and November 30, 2020. The median follow-up duration was 15.8 months (range, 8.1-43.4 months). The primary endpoint was recurrence-free survival (RFS). A propensity score matching model was used to minimize potential confounding covariates and to confirm our findings.
RESULTS: In stage II-III CRC patients, postoperative (within 1 month after surgery) mSEPT9 positivity was significantly correlated with worse RFS (HR=6.21, P<0.001), and it remained the strongest independent predictor in multivariate Cox regression analysis (HR=5.83, P<0.001), which was significantly superior to CEA, CA19-9, and CA242. During disease surveillance, mSEPT9 positivity preceded radiographic recurrence by a median of 5.0 months. The postoperative mSEPT9-positive patients benefited more from CAPEOX compared to FOLFOX (HR=3.97, P=0.017), while for mSEPT9-negative patients, CAPEOX and FOLFOX resulted in similar RFS (HR=1.70, P=0.322). Furthermore, 3 months of CAPEOX was more effective than 3 and 6 months of FOLFOX (HR=4.40, P=0.065; HR=1.56, P=0.073, respectively).
CONCLUSIONS: Our results revealed that mSEPT9 detection after radical resection could identify minimal residual disease (MRD) and could predict a high risk of recurrence in patients with stage II-III CRC. Furthermore, we show pioneering work that mSEPT9 detection could be used to guide the selection of an adjuvant chemotherapy regimen to improve RFS.
Keywords: Colorectal Neoplasms, Neoadjuvant Therapy, Prognosis, SEPTIN9 Protein, Human, Biomarkers, Tumor, CA-19-9 Antigen, Cell-Free Nucleic Acids, Chemotherapy, Adjuvant, DNA, Humans, Septins
Background
Colorectal cancer (CRC) is the third leading cause of cancer death [1]. The 5-year survival rate of CRC with all stages is 64%, but with the presence of distant metastasis, it drops to 14% [2]. Surgical radical resection remains the primary treatment choice for nonmetastatic colorectal cancer [3]. It is highly significant that routine postoperative surveillance with regular clinical assessments and radiologic imaging is recommended. Despite this, a large proportion of recurrence events are detected late, and distant relapse is the major cause of mortality [4].
A potential source for early recurrence and metastasis is the existence of postoperative minimal residual disease (MRD), which is difficult to detect by traditional radiological imaging and serum tumor biomarkers [5]. The ability of imaging modalities to identify MRD is still far from optimal due to their limited resolution [6,7]. The serum tumor biomarkers currently used for surveillance, such as carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9), and carbohydrate antigen 242 (CA242), have limited sensitivity and specificity [7,8]. Thus, it is essential to identify reliable indicators to detect MRD, serving as a harbinger for recurrence or metastasis before becoming clinically evident.
Aberrant DNA methylation has been well characterized in tumor progression and widely described in cancer patients [9–11]. A variety of methylated DNA have been identified as biomarkers for cancer diagnosis and prognostic prediction [12–14]. Among these epigenetic biomarkers, methylated
Our primary aim was to evaluate the role of postoperative mSEPT9 in recurrence risk prediction and ACT regimen selection for patients with stage II–III CRC. Furthermore, we aimed to explore the value of continuous surveillance of mSEPT9 in CRC prognosis prediction.
Material and Methods
STUDY DESIGN AND PARTICIPANTS:
This retrospective study was based on a database of 687 patients who underwent surgical treatment at Tianjin Union Medical Center in China between January 8, 2018, and November 30, 2020. A total of 261 patients were excluded from subsequent analysis due to loss to follow-up (n=70), diagnosis with non-CRC (n=31), nonprimary CRC (n=5), neoadjuvant therapy before surgery (n=61), no radical resection (n=15), insufficient imaging for recurrence (n=6), and stage 0 (n=4), stage I (n=46), or stage IV (n=23) CRC (Figure 1). Thus, a total of 426 evaluable patients who presented with histologically confirmed primary CRC were enrolled in the present study, and all of them subsequently underwent radical resection with or without ACT. The regimen and duration delivered were determined at the discretion of clinicians and patients and included single-agent (5-FU/capecitabine), FOLFOX (fluorouracil, leucovorin, and oxaliplatin), CAPEOX (capecitabine and oxaliplatin), and FOLFIRI (irinotecan, fluorouracil, and leucovorin). If patients received more than 1 treatment regimen, the regimen with the longest duration was included in the analysis. All patients had previously consented for their data to be used in this study. The study was approved by the Ethics Committee and was conducted in accordance with the Declaration of Helsinki.
The test results of mSEPT9, CEA, CA19-9, and CA242 levels in plasma before surgery (preoperative), within 1 month after surgery (postoperative), and at various time points during disease surveillance were collected for analysis. Longitudinal mSEPT9 positivity was defined as random mSEPT9 positivity during surveillance. All patients received treatment and follow-up according to the guidelines of the National Comprehensive Cancer Network and Chinese Society of Clinical Oncology. RFS was measured from the date of surgery to the verified first radiographic recurrence (including local recurrence and distant metastasis) or the date of death caused by CRC. Patients provided oral and written informed consent before blood collection.
PLASMA METHYLATED SEPT9 QUANTIFICATION:
A 10-ml peripheral blood sample was collected in a 10-ml K2EDTA anticoagulant tube, and a 3.5-ml plasma sample was collected from it upon centrifugation for the SEPT9 assay (BioChain [Beijing] Science and Technology, Inc., Beijing, PR China). Briefly, the SEPT9 gene methylation assay (PCR fluorescence probe method) was composed of 2 steps. First, total cell-free DNA was extracted from 3.5-mL plasma samples using a plasma processing kit manufactured by BioChain (Beijing) Science and Technology, Inc. and then incubated with bisulfite, leaving unmethylated cytosine converted to uracil, whereas methylated cytosines were not. In the second step, double PCR amplification was performed on bisulfite-converted DNA. PCR blocking oligonucleotides and probes could distinguish between methylated and unmethylated sequences, leading to preferential amplification of methylated DNA sequences. The methylated SEPT9-specific fluorescent probes could specifically detect the methylated sequence. PCR was performed in a 60.0-μL reaction system. The sequences of the primers, blockers, and probes for SEPT9 detection used in methylation-specific PCR amplification were as follows:
Positive (methylated SEPT9 DNA) and negative controls (SEPT9 DNA) were run in parallel with samples each time as quality controls. β-actin was used as an internal reference to evaluate the plasma DNA quality and the validity of PCR amplification. The sequences of the primers and probes for β-actin detection used in PCR amplification were as follows:
The PCR was programmed as follows: 94°C for 20 min; 45 cycles at 62°C for 5 s, 55.5°C for 35 s, and 93°C for 30 s; and cooling at 40°C for 5 s. According to the instructions, mSETP9 positive was defined as cycle threshold (Ct) value ≤41, while mSETP9 negative was defined as Ct value >41 or not detected (ND). For those not detected samples, Ct values were set as 45 (the maximal number of PCR cycles run in the mSEPT9 assay).
SERUM CEA, CA19-9, AND CA242 QUANTIFICATION:
Serum CEA and CA19-9 were measured by the electrochemiluminescence immunoassay (ECLI) on a Cobas E601 immunoassay analyzer (Roche Diagnostics, GmbH, Mannheim, Germany). Serum
CA242 was measured by CanAg CA242 enzyme immunometric assay (ELISA) kit (CanAg Diagnostics AB, Gothenburg, Sweden). The positive value was defined by widely accepted cutoffs (CEA: 5 ng/mL, CA19-9: 37 U/mL, CA242: 20 U/mL).
STATISTICAL ANALYSIS:
The chi-square test or Fisher’s exact test was used to compare categorical variables between the mSEPT9-positive and mSEPT9-negative subgroups, while the Wilcoxon rank test was used to compare continuous parameters. Kaplan-Meier estimates were performed to calculate the survival rate with the log-rank test to compare the differences. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated using Cox proportional hazards regression models. Receiver operating characteristic (ROC) curves and the area under the curve (AUC) were used to assess the predictive performance of mSEPT9, CEA, CA19-9, and CA242.
The propensity score model (PSM) was performed to match the potential bias of confounding covariates between subgroups (Supplementary Table 1). Logistic regression was run first to calculate propensity scores, and then clinicopathological factors, including age, sex, histology, differentiation, pT stage, pN stage, and localization, were used to match controls for the cases. A 1: 1 nearest neighbor matching algorithm with a 0.02 caliper width added without replacement was performed in preoperative mSEPT9-positive and -negative matching, CAPEOX and FOLFOX matching, and other subgroups if appropriate. In addition, 1: n nearest neighbor caliper matching without replacement was performed in postoperative mSEPT9-positive and -negative matching, and longitudinal mSEPT9-positive and -negative matching. All analyses were performed using SPSS 26.0 and R 4.1.2. Two-sided P values <0.05 were considered to be statistically significant.
Results
CLINICOPATHOLOGICAL CHARACTERISTICS AND MSEPT9:
A total of 426 patients with histologically confirmed stage II–III CRC who received radical resection were enrolled in the present study. The baseline characteristics based on the status of preoperative mSEPT9, postoperative mSEPT9 (within 1 month after surgery) and longitudinal mSEPT9 (within 12 months after surgery) are presented in Table 1.
Overall, the median age of the patients was 62 years (range, 23–83 years), and 253/426 (59.4%) were male. The proportions of patients with stage II and III disease were 180/426 (42.3%) and 246/426 (57.7%), respectively. With a median follow-up of 15.8 months (range, 8.1–43.4 months), 10 patients died from the progression of CRC, and 50/426 (11.7%) patients were observed to have recurrence. Local recurrence and distant metastasis cases were 9/50 (12.0%) and 41/50 (82.0%), respectively.
Preoperative mSEPT9 was evaluable in 348/426 (81.7%) patients, while postoperative mSEPT9 detected within 1 month after resection was evaluable in 339/426 (79.6%) patients. The preoperative and postoperative mSEPT9-positive rates were 173/348 (49.7%) and 60/339 (17.7%), respectively.
ASSOCIATION BETWEEN MSEPT9 AND RFS:
Preoperative mSEPT9 had no association with RFS (HR=1.26, 95% CI=0.68–2.33, P=0.465) (Figure 2A), whereas postoperative mSEPT9 positivity was significantly associated with worse RFS (HR=6.08, 95% CI=3.27–11.31, P<0.001) (Figure 2B).
Furthermore, we evaluated the dynamic change in postoperative mSEPT9. Patients with persistent negativity for 12 months after surgery had a superior RFS, while patients with a conversion from mSEPT9 negativity to positivity had a worse RFS (HR=3.12, 95% CI=1.37–7.08, P<0.01, Supplementary Figure 1A). Patients with persistent positivity had the worst RFS, even compared to the group that changed from negative to positive (HR=6.70, 95% CI=2.72–16.50, P<0.001, Supplementary Figure 1A).
POTENTIAL UTILITY OF MSEPT9 IN GUIDING ACT SELECTION:
The majority of patients (403/426, 94.6%) received adjuvant chemotherapy, and the proportion of patients receiving the different chemotherapy regimens was as follows: 161/426 (37.8%) received FOLFOX, 177/426 (41.5%) received CAPEOX, and 36/426 (8.5%) received FOLFIRI; a single-agent capecitabine was administered to 26/426 (6.1%) patients; and 26/426 (6.1%) did not receive any adjuvant therapy. A total of 148/426 (34.7%) patients received at least 3 months of adjuvant chemotherapy, and 253/426 (59.2%) patients completed a full course (6 months) of treatment (Table 1). Although guidelines have already provided detailed recommendations for selecting treatment regimens, including drugs and cycles, the optimal regimens among the first-line recommendations remain to be determined.
We further explored whether postoperative mSEPT9 was correlated with RFS when the patients were stratified by 2 first-line therapies, FOLFOX and CAPEOX. There was no significant difference in RFS of the mSEPT9-negative subgroup (P=0.325, Figure 2C), whereas in the postoperative mSEPT9-positive subgroup, patients who received CAPEOX had a markedly better RFS than those who received FOLFOX (HR=4.43, 95% CI=1.27–15.38, P < 0.05, Figure 2D), indicating that the difference in efficacy between regimens was correlated with mSEPT9.
For postoperative mSEPT9-positive patients, a surprising trend was observed in which 3 months of CAPEOX was more effective than 3 and 6 months of FOLFOX (3 months, HR=4.40, 95% CI=0.90–21.37, P=0.065; 6 months, HR=1.56, 95% CI=0.92–2.62, P=0.073) (Supplementary Figure 1B), but this difference was not statistically significant, probably owing to the limited number of patients. No significant difference between 3 and 6 months was found for either FOLFOX (HR=1.25, 95% CI=0.28–2.19, P=0.660) or CAPEOX (HR=1.20, 95% CI=0.07–9.18, P=0.878) (Supplementary Figure 1B).
SERUM CEA, CA19-9, CA242, AND RECURRENCE:
The elevation rates of preoperative CEA, CA19-9, and CA242 levels were 181/404 (44.8%), 67/403 (16.6%), and 26/405 (6.4%), respectively, and postoperative rates were 44/353 (12.5%), 21/341 (6.2%), and 29/264 (11.0%), respectively. The Kaplan-Meier curves of preoperative and postoperative CEA, CA19-9, and CA242 are shown in Supplementary Figure 2A–2F, none of which showed a significant difference in RFS between the elevated group and the nonelevated group (all P>0.05).
For patients with recurrence, the mSEPT9-positive rates in elevated postoperative CEA, CA19-9, and CA242 were 5/6 (83.3%), 4/4 (100.0%), and 4/5 (80.0%), respectively. However, as shown in Supplementary Table 2, for recurrence patients with postoperative mSEPT9 positivity, the elevation rates of CEA, CA19-9, and CA242 were just 5/19 (26.3%), 4/19 (21.1%), and 4/18 (22.2%), respectively. Furthermore, postoperative mSEPT9 positivity remained strongly associated with worse RFS even for patients with nonelevated CEA (HR=7.05, 95% CI=3.26–15.25, P<0.001, Supplementary Figure 3A), CA19-9 (HR=6.24, 95% CI=2.97–13.13, P<0.001, Supplementary Figure 3B) and CA242 (HR=6.51, 95% CI=2.95–14.36, P<0.001, Supplementary Figure 3C).
Furthermore, among patients who had recurrence, the postoperative mSEPT9-positive rate was maintained at 40% to 60% during surveillance, which was higher than the levels of CEA, CA19-9, and CA242 (Figure 3A), and it increased before clinical relapse, suggesting that mSEPT9 could better reflect the existence of MRD. In contrast, for patients without recurrence, the mSEPT9-positive rate remained below 20% within 12 months after surgery (Figure 3B).
In ROC curve analysis (Figure 3C), mSEPT9 also showed the best ability to monitor recurrence (AUC=0.821, 95% CI=0.752–0.890), outperforming CEA (AUC=0.501, 95% CI=0.408–0.594), CA19-9 (AUC=0.573, 95% CI=0.488–0.659), and CA242 (AUC=0.531, 95% CI=0.430–0.632).
L2 Longitudinal mSEPT9 Performed Better in Predicting Recurrence and Guiding ACT Selection
Next, we explored whether longitudinal mSEPT9 analysis performed better as a monitoring biomarker. As mentioned above, longitudinal mSEPT9 positivity was defined as random mSEPT9 positivity occurring during surveillance. Of 50 patients with recurrence, 72.0% had longitudinal mSEPT9 positivity, while only 52.5% had postoperative mSEPT9 positivity.
The longitudinal mSEPT9-positive group had a worse RFS than the longitudinal mSEPT9-negative group (HR=8.55, 95% CI=4.61–15.85, P<0.001, Figure 4A), which was more significant than that in the postoperative mSEPT9 analysis. Among the longitudinal positive mSEPT9 patients, those treated with CAPEOX showed better RFS than those treated with FOLFOX (HR=2.98, 95% CI=1.32–6.74, P<0.01, Figure 4B). However, there was no difference in RFS between regimens under longitudinal negative mSEPT9 conditions (P>0.05, Figure 4C).
In addition, the longitudinal mSEPT9-positivity rate was 36/50 (72.0%) for patients with recurrence. In 33 of these 36 patients (91.7%), mSEPT9 was detected early ahead of the radiological evidence. The median lead time from positive mSEPT9 detection to radiological relapse was 5.0 months (Wilcoxon signed-rank test, Z=4.721, P<0.001; Figure 4D). Moreover, of 376 patients without recurrence, 302 (80.3%) patients had a longitudinal negative mSEPT9.
Additional analyses for longitudinal CEA, CA19-9, and CA242 are shown in Supplementary Figure 2G–2I, none of which was associated with RFS (all P>0.05).
FURTHER VERIFICATION BY PROPENSITY SCORE MATCHING:
The PSM was performed to reduce the potential bias of confounding covariates between each subgroup. Baseline characteristics according to the status of preoperative, postoperative, and longitudinal mSEPT9 after matching are presented in Supplementary Table 1, and those according to CAPEOX/FOLFOX before and after matching are presented in Supplementary Table 3. No significant difference was observed between any 2 groups after matching. The absolute values of standardized differences were all <10%, implying that matched variables were well balanced between the 2 groups. All analyses were performed again after matching, and the results were even more significant than before.
For recurrence detection, there remained no association between preoperative mSEPT9 and RFS after matching (P>0.05, Figure 5A), while postoperative mSEPT9 positivity was significantly associated with worse RFS (HR=6.78, 95% CI=3.33–13.97, P<0.001, Figure 5B), and longitudinal mSEPT9 performed even better in relapse prediction (HR=7.22, 95% CI=3.57–14.62, P<0.001, Figure 5C).
Regarding the role of mSEPT9 in guiding chemotherapy, CAPEOX still had a better RFS than FOLFOX after matching in patients who were postoperatively mSEPT9-positive (HR=7.74, 95% CI=0.95–63.01, P<0.05, Figure 5D), as well as in patients who were longitudinally mSEPT9-positive (HR=3.64, 95% CI=1.17–11.32, P<0.05, Supplementary Figure 4A). No analysis was performed for PSM in patients who received different durations of therapy because of the limited number of cases.
In addition, postoperative mSEPT9 positivity remained associated with better survival when serum protein biomarkers were not elevated, including CEA (HR=7.63, 95% CI=3.08–18.93, P<0.001, Supplementary Figure 4B), CA19-9 (HR=6.05, 95% CI=2.53–14.44, P<0.001, Supplementary Figure 4C), and CA242 (HR=7.52, 95% CI=2.85–19.84, P<0.001, Supplementary Figure 4D).
Discussion
Plasma mSEPT9 detection has emerged as a promising method in CRC screening, diagnosis, and prognosis prediction [23,24]. In this study, we examined the prognostic value of postoperative mSEPT9 in CRC patients and compared it to that of the traditional tumor biomarkers CEA, CA19-9, and CA242. mSEPT9 showed a much better ability to predict recurrence than the 3 tumor biomarkers, with an AUC value of 0.821. Moreover, we continuously monitored mSEPT9 status for 12 months for the first time and defined it as longitudinal mSEPT9. The results showed that longitudinal mSEPT9 performed best in recurrence monitoring for patients with CRC and even preceded radiological recurrence by a median of 5 months. Furthermore, this study performed pioneering work to reveal the role of mSEPT9 status in ACT selection for CRC patients, in which patients with positive mSEPT9 could benefit more from the CAPEOX regimen than the FOLFOX regimen.
The positivity rate of mSEPT9 was 49.7% before the operation and dramatically declined to 17.7% within 1 month after the operation, which is similar to that reported previously [25]. This conversion of mSEPT9 reflects the tumor burden in real time [13,26], since as a kind of ccfDNA, the half-life of mSEPT9 is approximately 2 h [27]. Therefore, the potential role of mSEPT9 in CRC diagnosis has been extensively investigated and gradually introduced into CRC screening programs [19,22]. Regarding the prognostic value of mSEPT9, several recent studies have reported that positive postoperative mSEPT9 was correlated with a worse RFS, and a similar finding also emerged from our study. A study revealed that patients with positive postoperative mSEPT9 had significantly worse cancer-specific survival (CSS) than those with negative mSEPT9, and the correlation was affected by mismatch repair (MMR) status and specific genotype mutation [20]. Huang et al [22] demonstrated that mSEPT9 is a prognostic predictor for stage II–III CRC patients and that its expression is associated with vascular invasion, vascular invasion, and other clinical parameters. Nevertheless, few studies have continuously monitored the status of mSEPT9 and evaluated the prognostic value of longitudinal mSEPT9 in CRC patients. Our analysis demonstrated that longitudinal mSEPT9 has a better ability to identify recurrence than postoperative mSEPT9, in which 72.0% patients who had a recurrence had longitudinal mSEPT9 positivity, and 91.7% mSEPT9 positivity was detected early ahead of the radiological evidence with a median lead time of 5 months.
Serum biomarkers, such as CEA, CA19-9, and CA242, have been widely used clinically for postoperative surveillance in CRC [28–32]. However, the sensitivity and specificity of any single one of them is not sufficient to make it a reliable indicator in CRC monitoring. In our study, the specificity (80.1%) and sensitivity (74.0%) of mSEPT9 for detecting recurrence were remarkably higher than those of any single serum marker, which was similar to that reported by Sun et al, and they also found that mSEPT9 combined with CEA showed a stronger predictive ability [20]. Another recent study revealed that the positive detection rate of the combination of mSEPT9 with CECT was higher than that of single CECT and the combination of tumor markers with CECT [18].
In this study, we mainly focused on the potential value of mSEPT9 in the selection of chemotherapy regimens. Although guidelines have already made recommendations in the selection of chemotherapy regimens for patients with different stages of CRC, when several options exist for first-line treatment, such as FOLFOX and CAPEOX for stage II–III CRC [33–35], choosing the most reasonable regimen for patients remains a challenge due to limited evidence in prognosis studies. Our results revealed that patients with stage II–III CRC who received CAPEOX had a better RFS than those who received FOLFOX, especially those with postoperatively positive mSEPT9. However, the advantage of CAPEOX disappeared in patients with postoperatively negative mSEPT9. When considering the duration of chemotherapy, 3 months of CAPEOX even had a better RFS than 3 months of FOLFOX, which was consistent with several previous studies [36,37].
This could be partly explained by the different frequencies of fluoropyrimidine administration. Patients treated with FOLFOX received fluorouracil administered via intravenous infusion every 2 weeks, while those treated with CAPEOX received capecitabine administered via the oral route twice daily. The latter mode could maintain a stable blood drug concentration and be more effective in terms of MRD clearance than the former [38]. Given the ability of mSEPT9 to detect MRD and the outstanding ability of CAPEOX to remove MRD, CAPEOX would be better than FOLFOX in patients with positive mSEPT9. Correspondingly, patients with negative mSEPT9 had lower MRD levels and risk of recurrence; thus, there was no significant difference between these 2 regimens [39].
Moreover, although FOLFOX and CAPEOX are the first-line ACT regimens, 8.5% of patients were administered second-line FOLFIRI in this study because of the adverse reactions of FOLFOX and CAPEOX, including nausea, vomiting, diarrhea, and hematological toxicities. Meanwhile, stage II patients without high-risk factors who received ACT accounted for 15.5% of all participants due to the comprehensive consideration from clinicians and the willingness of patients, although that was not recommended in the latest guidelines [3].
This study had some limitations. First, the retrospective nature of this study is still a notable weakness, although PSM was used to reduce bias. Second, with the situations mentioned above and with the aim of ensuring the homogeneity of the population, patients with rectal cancer in our study only received adjuvant therapy, whereas the modern approach to these patients is neoadjuvant therapy. Third, the number of patients was relatively low, and not all patients had mSEPT9 detected before and after surgery and during surveillance; thus, some patients had recurrence but no positive mSEPT9, possibly due to a lack of periodic detection during surveillance.
Conclusions
This study revealed that mSEPT9 detection could identify MRD and dynamically predict the risk of recurrence in resected stage II–III CRC patients. Furthermore, we showed pioneering work that mSEPT9-positive patients could benefit more from CAPEOX than FOLFOX. Thus, postoperative mSEPT9-defined MRD status could be used to guide chemotherapy regimens to improve survival.
Figures
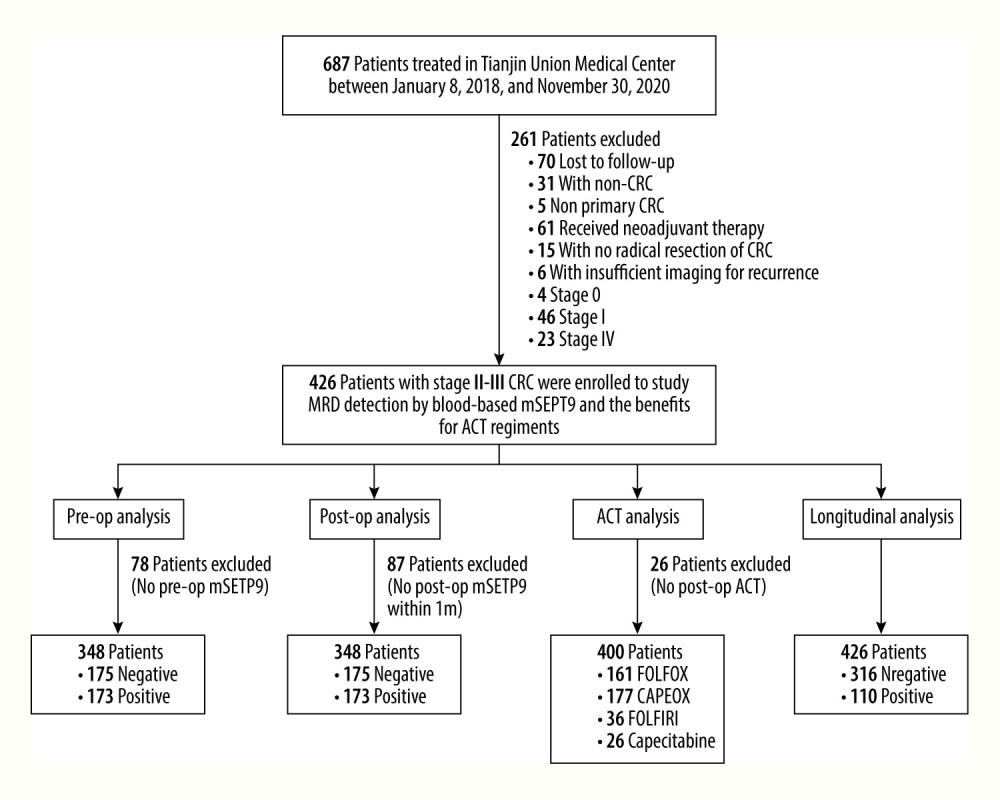 Figure 1. Flowchart depicting the process of patient inclusion. CRC – colorectal cancer; ACT – adjuvant chemotherapy; MRD – minimal residual disease; op – operative. PowerPoint (Microsoft Inc., Redmond, WA, USA) was used for Figure creation.
Figure 1. Flowchart depicting the process of patient inclusion. CRC – colorectal cancer; ACT – adjuvant chemotherapy; MRD – minimal residual disease; op – operative. PowerPoint (Microsoft Inc., Redmond, WA, USA) was used for Figure creation. 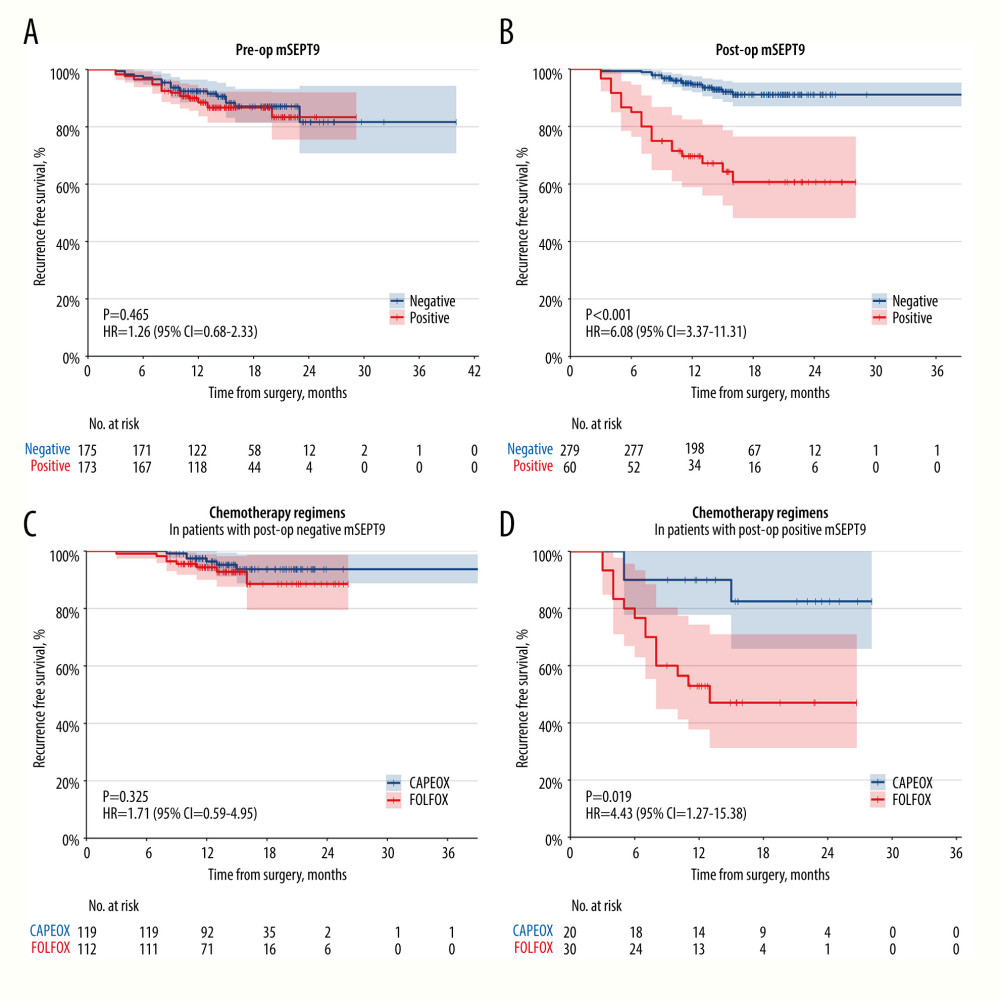 Figure 2. Recurrence-free survival stratified by preoperative mSEPT9 (A) and postoperative mSEPT9 (B). Recurrence-free survival stratified by chemotherapy regimens (FOLFOX/CAPEOX) in patients with postoperative negative mSEPT9 (C) and in those with postoperative positive mSEPT9 (D). R software 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) was used for Figure creation.
Figure 2. Recurrence-free survival stratified by preoperative mSEPT9 (A) and postoperative mSEPT9 (B). Recurrence-free survival stratified by chemotherapy regimens (FOLFOX/CAPEOX) in patients with postoperative negative mSEPT9 (C) and in those with postoperative positive mSEPT9 (D). R software 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) was used for Figure creation. 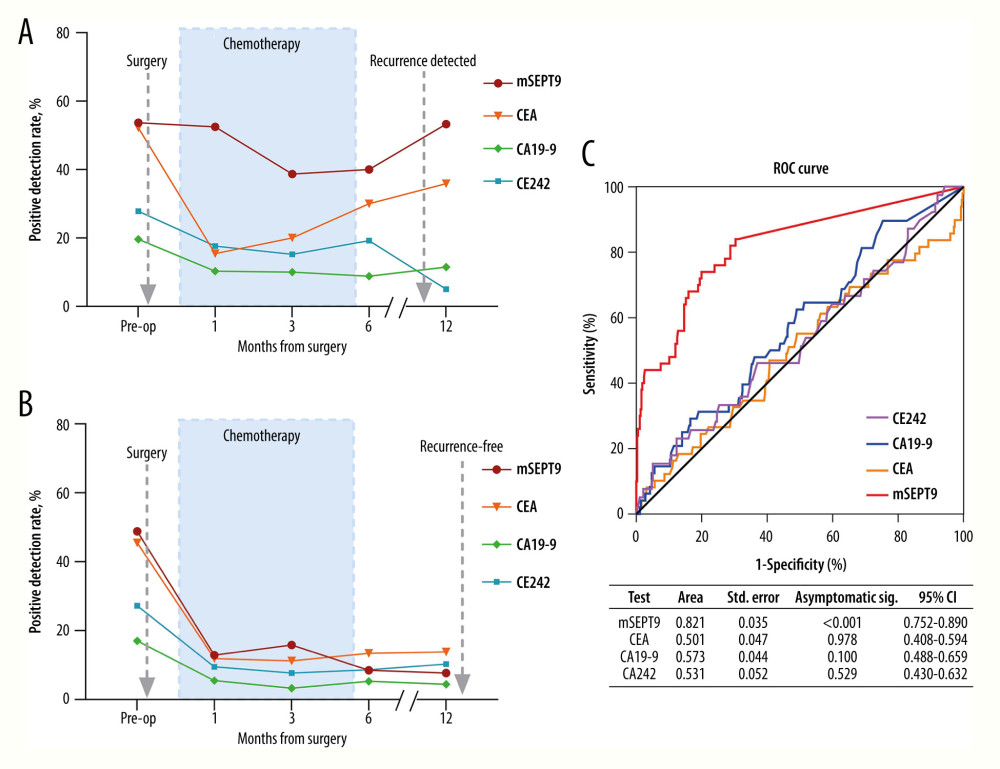 Figure 3. Positive detection rate of mSEPT9, CEA, CA19-9, and CA242 for patients who received adjuvant chemotherapy and subsequently suffered a radiologic recurrence (A) or remained radiological recurrence-free (B) during their surveillance. (C) The ROC curve for mSEPT9, CEA, CA19-9 and CA242. ROC, receiver operating characteristic. SPSS 26.0 (SPSS, Inc., Chicago, Illinois, USA) and PowerPoint 2018 (Microsoft, Inc., Redmond, WA, USA) were used for Figure creation.
Figure 3. Positive detection rate of mSEPT9, CEA, CA19-9, and CA242 for patients who received adjuvant chemotherapy and subsequently suffered a radiologic recurrence (A) or remained radiological recurrence-free (B) during their surveillance. (C) The ROC curve for mSEPT9, CEA, CA19-9 and CA242. ROC, receiver operating characteristic. SPSS 26.0 (SPSS, Inc., Chicago, Illinois, USA) and PowerPoint 2018 (Microsoft, Inc., Redmond, WA, USA) were used for Figure creation. 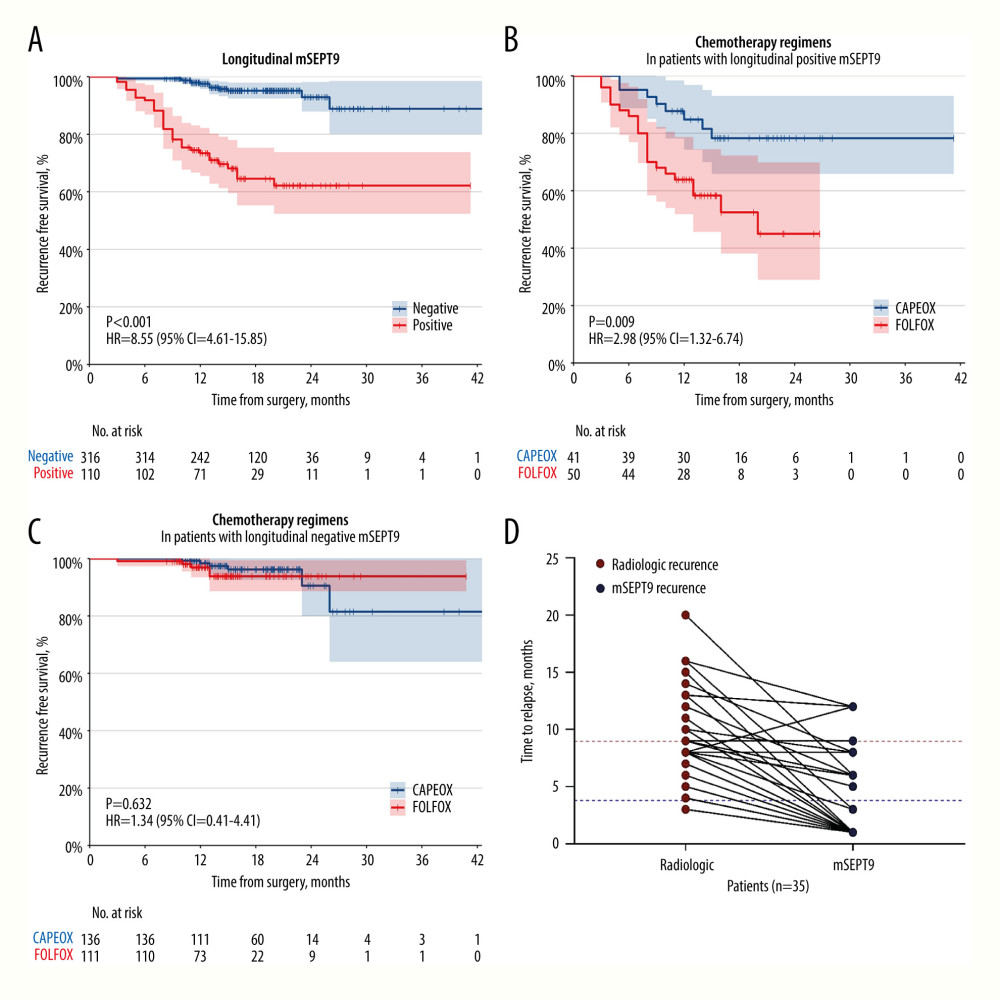 Figure 4. Recurrence-free survival stratified by longitudinal mSEPT9 (A) and further stratified by chemotherapy regimens (FOLFOX/CAPEOX) in patients with longitudinal positive mSEPT9 (B) and in those with longitudinal negative mSEPT9 (C). (D) Comparison of time to recurrence detected by mSEPT9 and radiology (p<0.001). R software 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) was used for Figure creation.
Figure 4. Recurrence-free survival stratified by longitudinal mSEPT9 (A) and further stratified by chemotherapy regimens (FOLFOX/CAPEOX) in patients with longitudinal positive mSEPT9 (B) and in those with longitudinal negative mSEPT9 (C). (D) Comparison of time to recurrence detected by mSEPT9 and radiology (p<0.001). R software 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) was used for Figure creation. 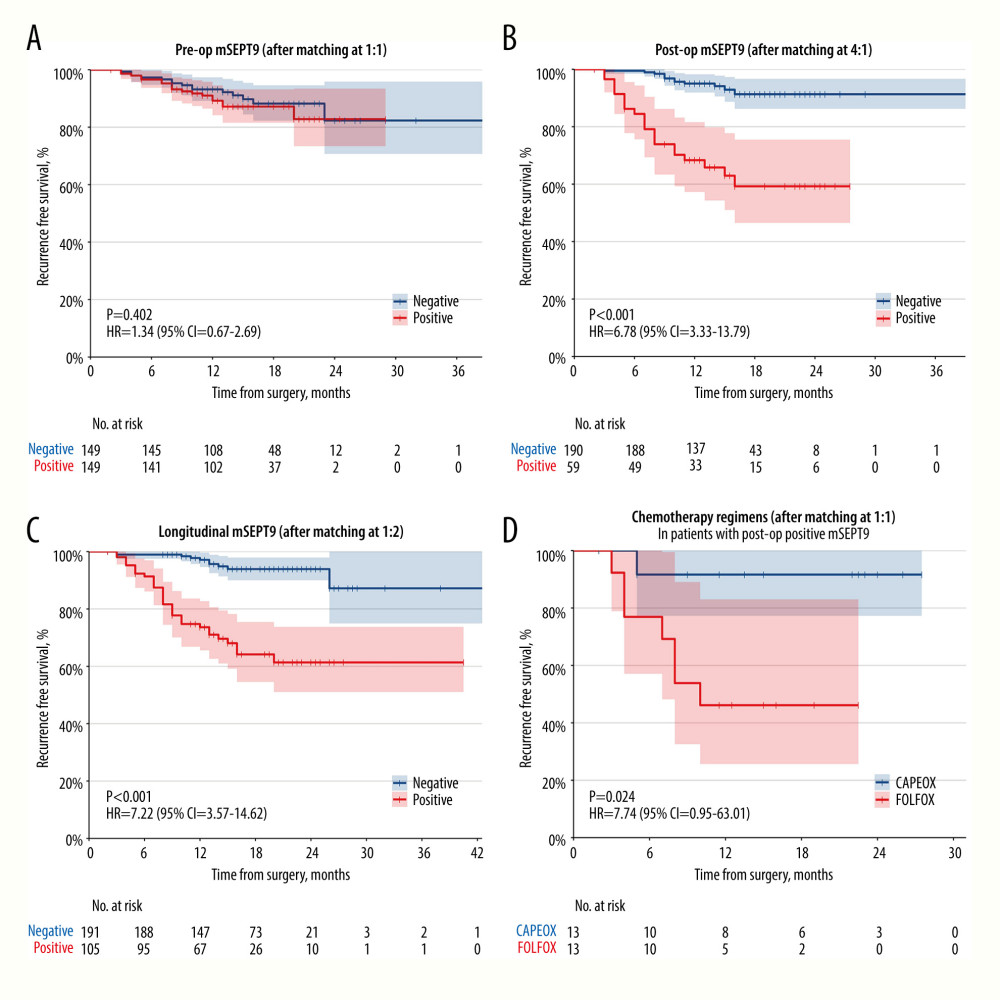 Figure 5. Recurrence-free survival stratified by preoperative (A), postoperative (B) and longitudinal mSEPT9 (C) after propensity matching. (D) Recurrence-free survival stratified by chemotherapy regimen (FOLFOX/CAPEOX) in patients with postoperative positive mSEPT9 after propensity matching. R software 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) was used for Figure creation.
Figure 5. Recurrence-free survival stratified by preoperative (A), postoperative (B) and longitudinal mSEPT9 (C) after propensity matching. (D) Recurrence-free survival stratified by chemotherapy regimen (FOLFOX/CAPEOX) in patients with postoperative positive mSEPT9 after propensity matching. R software 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) was used for Figure creation. Tables
Table 1. Baseline characteristics of patients with stage II–III colorectal cancer.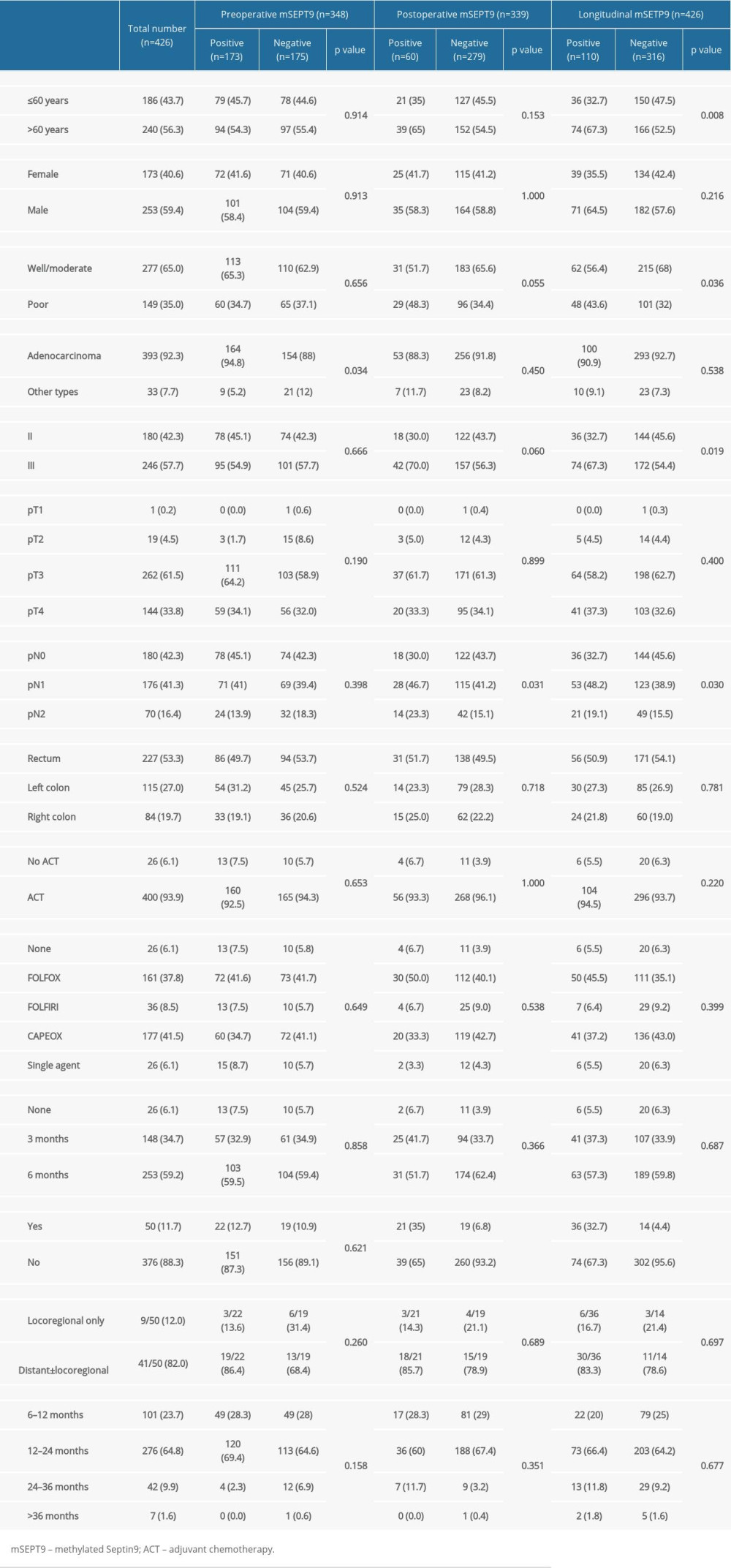 Supplementary Table 1. Baseline characteristics of patients with stage II–III CRC after propensity matching.
Supplementary Table 1. Baseline characteristics of patients with stage II–III CRC after propensity matching.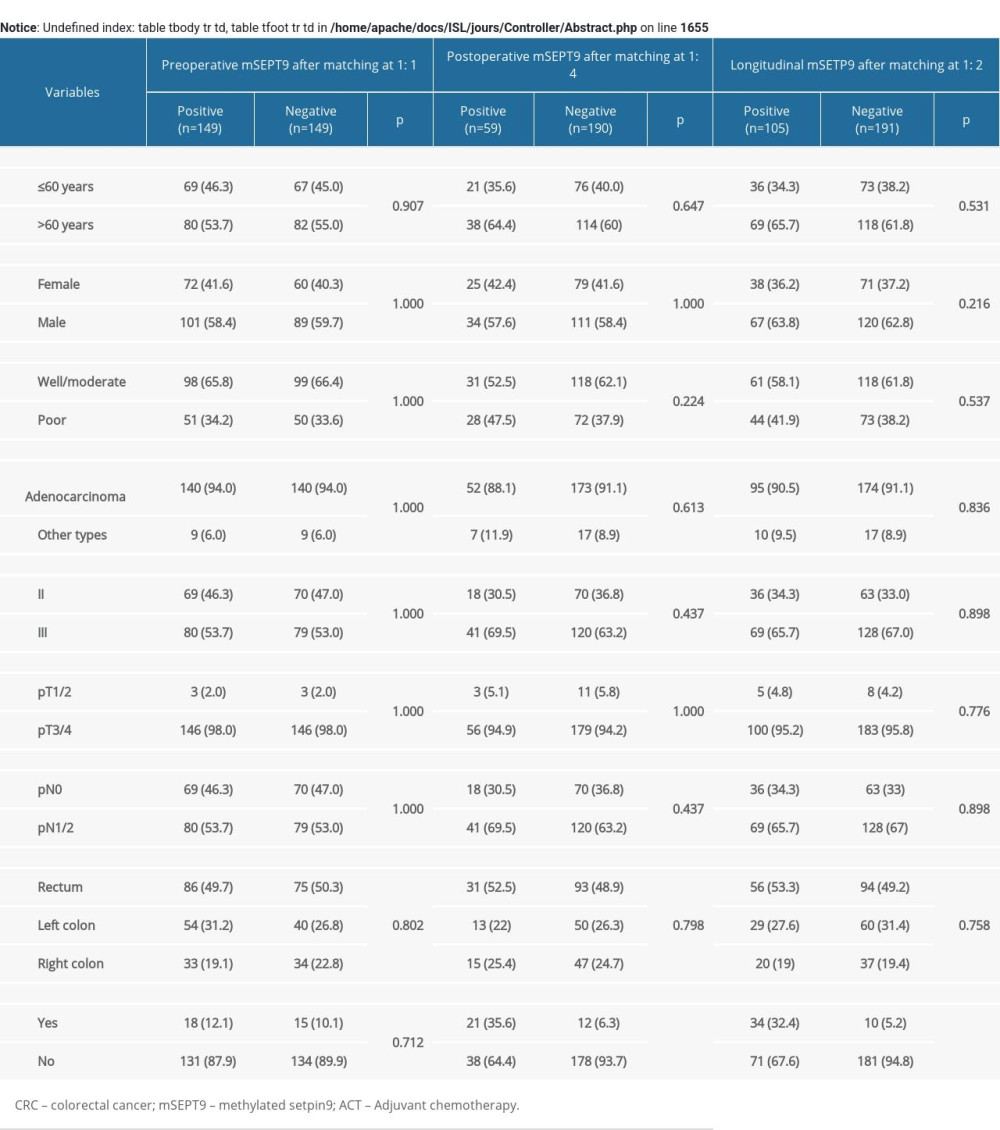 Supplementary Table 2. Relationship between postoperative mSETP9, CEA, CA19-9, and CA242 levels and recurrence status.
Supplementary Table 2. Relationship between postoperative mSETP9, CEA, CA19-9, and CA242 levels and recurrence status. Supplementary Table 3. Baseline characteristics of the patients who received CAPEOX and FOLFOX before and after propensity matching.
Supplementary Table 3. Baseline characteristics of the patients who received CAPEOX and FOLFOX before and after propensity matching.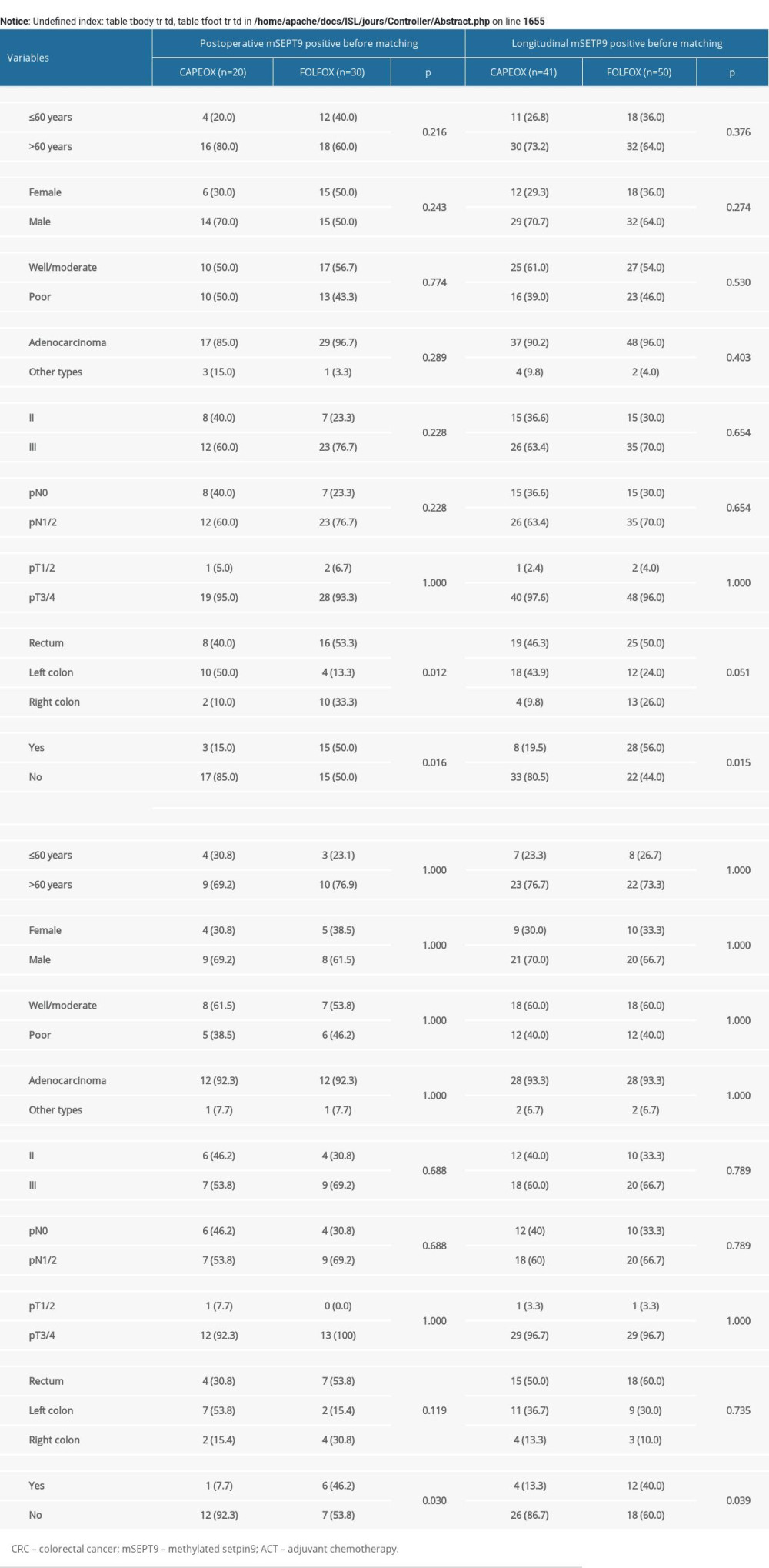
References
1. Sung H, Ferlay J, Siegel RL, Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries: Cancer J Clin, 2021; 71(3); 209-49
2. Siegel RL, Miller KD, Jemal A, Cancer statistics, 2020: Cancer J Clin, 2020; 70(1); 7-30
3. Benson AB, Venook AP, Al-Hawary MM, Colon cancer, version 2.2021, NCCN Clinical Practice Guidelines in Oncology: J Natl Compr Canc Netw, 2021; 19(3); 329-59
4. Snyder RA, Hu CY, Cuddy A, Association between intensity of posttreatment surveillance testing and detection of recurrence in patients with colorectal cancer: JAMA, 2018; 319(20); 2104-15
5. Dasari A, Morris VK, Allegra CJ, ctDNA applications and integration in colorectal cancer: An NCI Colon and Rectal-Anal Task Forces whitepaper: Nat Rev Clin Oncol, 2020; 17(12); 757-70
6. Mainenti PP, Romano F, Pizzuti L, Non-invasive diagnostic imaging of colorectal liver metastases: World J Radiol, 2015; 7(7); 157-69
7. Chao M, Gibbs P, Caution is required before recommending routine carcinoembryonic antigen and imaging follow-up for patients with early-stage colon cancer: J Clin Oncol, 2009; 27(36); e279-80 author reply e281
8. Young GP, Pedersen SK, Mansfield S, A cross-sectional study comparing a blood test for methylated BCAT1 and IKZF1 tumor-derived DNA with CEA for detection of recurrent colorectal cancer: Cancer Med, 2016; 5(10); 2763-72
9. Ebert MP, Mooney SH, Tonnes-Priddy L, Hypermethylation of the TPEF/HPP1 gene in primary and metastatic colorectal cancers: Neoplasia, 2005; 7(8); 771-78
10. Toyota M, Shen L, Ohe-Toyota M, Aberrant methylation of the Cyclooxygenase 2 CpG island in colorectal tumors: Cancer Res, 2000; 60(15); 4044-48
11. Toyooka S, Toyooka KO, Harada K, Aberrant methylation of the CDH13 (H-cadherin) promoter region in colorectal cancers and adenomas: Cancer Res, 2002; 62(12); 3382-86
12. Leung WK, To KF, Man EP, Quantitative detection of promoter hypermethylation in multiple genes in the serum of patients with colorectal cancer: Am J Gastroenterol, 2005; 100(10); 2274-79
13. Barault L, Amatu A, Siravegna G, Discovery of methylated circulating DNA biomarkers for comprehensive non-invasive monitoring of treatment response in metastatic colorectal cancer: Gut, 2018; 67(11); 1995-2005
14. Coppedè F, Epigenetic biomarkers of colorectal cancer: Focus on DNA methylation: Cancer Lett, 2014; 342(2); 238-47
15. Semaan A, van Ellen A, Meller S, SEPT9 and SHOX2 DNA methylation status and its utility in the diagnosis of colonic adenomas and colorectal adenocarcinomas: Clin Epigenetics, 2016; 8; 100
16. Thierry AR, Mouliere F, Gongora C, Origin and quantification of circulating DNA in mice with human colorectal cancer xenografts: Nucleic Acids Res, 2010; 38(18); 6159-75
17. Mouliere F, El Messaoudi S, Pang D, Multi-marker analysis of circulating cell-free DNA toward personalized medicine for colorectal cancer: Mol Oncol, 2014; 8(5); 927-41
18. Sun J, Fei F, Zhang M, The role of (m)SEPT9 in screening, diagnosis, and recurrence monitoring of colorectal cancer: BMC Cancer, 2019; 19(1); 450
19. Lu P, Zhu X, Song Y, Methylated Septin 9 as a promising biomarker in the diagnosis and recurrence monitoring of colorectal cancer: Dis Markers, 2022; 2022; 7087885
20. Sun J, Xu J, Sun C, Screening and prognostic value of methylated Septin9 and its association with clinicopathological and molecular characteristics in colorectal cancer: Front Mol Biosci, 2021; 8; 568818
21. Ma ZY, Law WL, Ng EKO, Methylated Septin 9 and carcinoembryonic antigen for serological diagnosis and monitoring of patients with colorectal cancer after surgery: Sci Rep, 2019; 9(1); 10326
22. Huang M, He J, Lai W, Methylated septin 9 gene is an important prognostic marker in stage II and stage III colorectal cancer for evaluating local recurrence or distant metastasis after surgery: BMC Gastroenterol, 2022; 22(1); 87
23. Warren JD, Xiong W, Bunker AM, Septin 9 methylated DNA is a sensitive and specific blood test for colorectal cancer: BMC Med, 2011; 9; 133
24. Church TR, Wandell M, Lofton-Day C, Prospective evaluation of methylated SEPT9 in plasma for detection of asymptomatic colorectal cancer: Gut, 2014; 63(2); 317-25
25. Bergheim J, Semaan A, Gevensleben H, Potential of quantitative SEPT9 and SHOX2 methylation in plasmatic circulating cell-free DNA as auxiliary staging parameter in colorectal cancer: A prospective observational cohort study: Br J Cancer, 2018; 118(9); 1217-28
26. Reinert T, Schøler LV, Thomsen R, Analysis of circulating tumour DNA to monitor disease burden following colorectal cancer surgery: Gut, 2016; 65(4); 625-34
27. Diehl F, Schmidt K, Choti MA, Circulating mutant DNA to assess tumor dynamics: Nat Med, 2008; 14(9); 985-90
28. Acharya A, Markar SR, Matar M, Use of tumor markers in gastrointestinal cancers: Surgeon perceptions and cost-benefit trade-off analysis: Ann Surg Oncol, 2017; 24(5); 1165-73
29. Gao Y, Wang J, Zhou Y, Evaluation of serum CEA, CA19-9, CA72-4, CA125 and ferritin as diagnostic markers and factors of clinical parameters for colorectal cancer: Sci Rep, 2018; 8(1); 2732
30. Carpelan-Holmström M, Louhimo J, CEA, CA 242, CA 19-9, CA 72-4 and hCGbeta in the diagnosis of recurrent colorectal cancer: Tumour Biol, 2004; 25(5–6); 228-34
31. Wang WS, Lin JK, Chiou TJ, CA19-9 as the most significant prognostic indicator of metastatic colorectal cancer: Hepatogastroenterology, 2002; 49(43); 160-64
32. Yang XQ, Chen C, Peng CW, Carbohydrate antigen 242 highly consists with carbohydrate antigen 19-9 in diagnosis and prognosis of colorectal cancer: study on 185 cases: Med Oncol, 2012; 29(2); 1030-36
33. André T, Boni C, Navarro M, Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the MOSAIC trial: J Clin Oncol, 2009; 27(19); 3109-16
34. Yothers G, O’Connell MJ, Allegra CJ, Oxaliplatin as adjuvant therapy for colon cancer: Updated results of NSABP C-07 trial, including survival and subset analyses: J Clin Oncol, 2011; 29(28); 3768-74
35. Haller DG, Tabernero J, Maroun J, Capecitabine plus oxaliplatin compared with fluorouracil and folinic acid as adjuvant therapy for stage III colon cancer: J Clin Oncol, 2011; 29(11); 1465-71
36. Yoshino T, Yamanaka T, Oki E, Efficacy and long-term peripheral sensory neuropathy of 3 vs 6 months of oxaliplatin-based adjuvant chemotherapy for colon cancer: The ACHIEVE phase 3 randomized clinical trial: JAMA Oncol, 2019; 5(11); 1574-81
37. Grothey A, Sobrero AF, Shields AF, Duration of adjuvant chemotherapy for stage III colon cancer: N Engl J Med, 2018; 378(13); 1177-88
38. Chau I, Norman AR, Cunningham D, A randomised comparison between 6 months of bolus fluorouracil/leucovorin and 12 weeks of protracted venous infusion fluorouracil as adjuvant treatment in colorectal cancer: Ann Oncol, 2005; 16(4); 549-57
39. Twelves C, Wong A, Nowacki MP, Capecitabine as adjuvant treatment for stage III colon cancer: N Engl J Med, 2005; 352(26); 2696-704
40. Tóth K, Wasserkort R, Sipos F, Detection of methylated septin 9 in tissue and plasma of colorectal patients with neoplasia and the relationship to the amount of circulating cell-free DNA: PLoS One, 2014; 9(12); e115415
41. Payne SR, From discovery to the clinic: the novel DNA methylation biomarker (m)SEPT9 for the detection of colorectal cancer in blood: Epigenomics, 2010; 2(4); 575-85
42. Sanz-Pamplona R, Cordero D, Berenguer A, Gene expression differences between colon and rectum tumors: Clin Cancer Res, 2011; 17(23); 7303-12
43. Johnson DA, Barclay RL, Mergener K, Plasma Septin9 versus fecal immunochemical testing for colorectal cancer screening: a prospective multicenter study: PLoS One, 2014; 9(6); e98238
Figures
Figure 1. Flowchart depicting the process of patient inclusion. CRC – colorectal cancer; ACT – adjuvant chemotherapy; MRD – minimal residual disease; op – operative. PowerPoint (Microsoft Inc., Redmond, WA, USA) was used for Figure creation.Figure 2. Recurrence-free survival stratified by preoperative mSEPT9 (A) and postoperative mSEPT9 (B). Recurrence-free survival stratified by chemotherapy regimens (FOLFOX/CAPEOX) in patients with postoperative negative mSEPT9 (C) and in those with postoperative positive mSEPT9 (D). R software 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) was used for Figure creation.Figure 3. Positive detection rate of mSEPT9, CEA, CA19-9, and CA242 for patients who received adjuvant chemotherapy and subsequently suffered a radiologic recurrence (A) or remained radiological recurrence-free (B) during their surveillance. (C) The ROC curve for mSEPT9, CEA, CA19-9 and CA242. ROC, receiver operating characteristic. SPSS 26.0 (SPSS, Inc., Chicago, Illinois, USA) and PowerPoint 2018 (Microsoft, Inc., Redmond, WA, USA) were used for Figure creation.Figure 4. Recurrence-free survival stratified by longitudinal mSEPT9 (A) and further stratified by chemotherapy regimens (FOLFOX/CAPEOX) in patients with longitudinal positive mSEPT9 (B) and in those with longitudinal negative mSEPT9 (C). (D) Comparison of time to recurrence detected by mSEPT9 and radiology (p<0.001). R software 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) was used for Figure creation.Figure 5. Recurrence-free survival stratified by preoperative (A), postoperative (B) and longitudinal mSEPT9 (C) after propensity matching. (D) Recurrence-free survival stratified by chemotherapy regimen (FOLFOX/CAPEOX) in patients with postoperative positive mSEPT9 after propensity matching. R software 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) was used for Figure creation. Tables
Table 1. Baseline characteristics of patients with stage II–III colorectal cancer.Table 1. Baseline characteristics of patients with stage II–III colorectal cancer.Supplementary Table 1. Baseline characteristics of patients with stage II–III CRC after propensity matching.Supplementary Table 2. Relationship between postoperative mSETP9, CEA, CA19-9, and CA242 levels and recurrence status.Supplementary Table 3. Baseline characteristics of the patients who received CAPEOX and FOLFOX before and after propensity matching. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387