12 January 2023: Clinical Research
Static and Dynamic Plantar Pressure Distribution in 94 Patients with Different Stages of Unilateral Knee Osteoarthritis Using the Footscan Platform System: An Observational Study
Yong-jin He1BCDE, Xiao-long Zheng1BDE, Deng-feng Wang1DEF, Zuo-zhou Mu1BCD, Gui-yu Li2BC, Zhen-zhen Fang2BC, Wang FeiDOI: 10.12659/MSM.938485
Med Sci Monit 2023; 29:e938485






Abstract
BACKGROUND: Plantar pressure analysis is widely used in the study of knee osteoarthritis (KOA). The present study aimed to investigate the static and dynamic plantar pressure distribution in patients with different stages of unilateral KOA using the Footscan® platform system.
MATERIAL AND METHODS: We recruited 94 patients aged 61.75±7.23 years old with different stages of unilateral KOA for static and dynamic analysis using the Footscan® platform system. The static pressure (%) of the left, right, anterior, posterior, and the pelvic rotation (°) was assessed. The peak pressure (PP, kPa) was investigated in 10 areas of the foot: medial heel (MH), lateral heel (LH), midfoot (MF), first to fifth metatarsals (M1-M5), hallux (T1), and toes 2-5 (T2-5). The correlation between KOA stages and plantar pressure distributions was investigated.
RESULTS: The results revealed that static pressure on the unaffected side and pelvic rotation were positively correlated with KOA stages. In addition, there was a positive correlation between KOA stages and PP of M5, MF, and LH zones on the affected side and PP of M2, M3, and M4 zones on the unaffected side, and a negative correlation between KOA stages and PP of T1 and T2-5 zones on the affected side.
CONCLUSIONS: With the progression of KOA, static plantar pressure tends to distributed on the unaffected side, and the dynamic plantar pressure tends to be distributed laterally on both feet. The plantar pressure distributions in unilateral KOA patients are abnormal and are closely related to the severity of KOA.
Keywords: Foot, Knee, Osteoarthritis, Pressure, Humans, Middle Aged, Aged, Osteoarthritis, Knee, Gait, Heel
Background
Knee osteoarthritis (KOA) is a common degenerative disease, and the global prevalence of symptomatic KOA is reported to be approximately 13% in women and 10% in men aged 60 and older [1]. KOA causes destruction of articular cartilage and the entire surrounding joint structures. The goal of treatment is to alleviate symptoms of the disease and slow its progression if possible, using physiotherapy, pharmacotherapy, orthopedic aids, and, finally, surgery [2]. Restoration of the neutral mechanical alignment in KOA patients has traditionally been considered an important factor influencing loading distribution [3]. In humans, the feet are the only part of the body that contact the ground directly during standing and walking, and foot loading patterns provide sensory information [4]. The Footscan® platform system has been validated as a reliable tool for determining loading distributions and alterations on the lower extremity and their reflection on the foot sole [5], which has been increasingly used for plantar pressure analysis [6,7].
Numerous previous studies have reported that there are characteristic changes in plantar pressure distribution in patients with KOA, mainly manifested by more lateral plantar pressure distribution and balance disturbances [8,9]. However, previous studies mainly analyzed the difference in plantar loading between KOA patients and the normal population [8,9], and did not investigate the effect of KOA severity on plantar pressure distributions. If a relationship between KOA severity and plantar pressure distribution is established, closer attention to loading of the foot may ultimately provide important insights into the pathogenesis of disease progression at the knee.
Given the increased risk of falls and eventual fall rates in people with KOA [3], it is important to establish the extent of balance impairment in different stages of KOA. We hypothesized that plantar pressure distribution in patients with different stages KOA was different, and the severity of KOA may influence the balance function of these patients. Therefore, the present single-center study of patients with different stages of unilateral KOA aimed to evaluate the use of static and dynamic analysis of plantar pressure distribution using the Footscan® platform system, and to investigate the relationship between plantar pressure distribution and KOA stages.
Material and Methods
ETHICS STATEMENT:
This cross-sectional study was conducted between March 2018 and April 2021 in the Orthopedics Department of Xijing Hospital. The study protocol was approved by our institutional review board (CR20180032); it adhered to the principles outlined in the Declaration of Helsinki, all participants were informed of the procedures before they consented to participate, and all participants signed an informed consent statement.
SUBJECTS:
Patients who were previously diagnosed with unilateral KOA and radiographically confirmed by a knee expert in our institution were included in the study. The inclusion criteria were as follows: (a) age between 50 and 70 years; (b) did not receive drug or physical therapy in the past week; (c) no history of surgery involving both lower extremities. The exclusion criteria were as follows: (a) neuromuscular disorders affecting the lower extremities, such as cerebral palsy; (b) underlying diseases limiting activities of daily living, such as coronary heart disease and lumbar spinal stenosis; (c) other deformities such as tarsal coalition and vertical talus.
KOA severity was defined according to the Kellgren-Lawrence (KL) grade [3] (Figure 1) combined with clinical symptoms: (a) early-stage: mild to moderate pain with activity, no obvious deformity, acceptable joint motion, KL grade 0/I; (b) mid-stage: activity limitation due to severe pain, presence of deformities and joint instability, KL grade II/III; (c) end-stage: unable to move without aid due to severe pain, obvious deformity, limited joint motion, KL grade IV.
SAMPLE SIZE ESTIMATION:
A pilot study was conducted to estimate the sample size. The power was set as 0.8, and alpha was set as 0.05/3. The final sample size calculated using PASS 11.0 software (NCSS, LLC, USA) was 25 of each group.
INSTRUMENTATION:
Dynamic foot pressure data were collected using the Footscan® platform system (RSscan International, Belgium) [5], which consists of a data processing box and a 2.00×0.40×0.02 m force plate, with 40 960 resistive sensors distributed in a 256×64 matrix. The minimum measurement area was 0.25 cm2 with the sampling frequency of 125 Hz and pressure collection interval of 0–200 N/cm2.
PLANTAR PRESSURE ANALYSIS:
The plantar pressure analysis consisted of 2 tests: a static test and a dynamic test. Each test was completed 3 times successively, and the data were averaged for further analysis.
STATIC TEST: Before tests, patients were asked to assume a relaxed standing posture, facing the instrument. Then, they were instructed to step onto the force plate barefoot and keep their head straight, eyes closed, and arms along their body for at least 20 s [7] while the static plantar pressure parameters measurement was performed.
DYNAMIC TEST: Before tests, all patients completed a 10-min acclimatization walking trial along the force plate, barefoot, without any aid, at their comfortable walking pace while looking forward. Based on the walking trials, each patient determined a suitable starting position to ensure that 3 steps were taken prior to force plate contact [6], then they were instructed to perform dynamic tests while the dynamic pressure parameters were recorded. For each trial, only 2 representative and reliable steps of each side were selected for further analysis.
DATA COLLECTION:
The static plantar pressure parameters were automatically measured using Scientific Footscan Software (RSscan International) [5], including percentages of anterior pressure, posterior pressure, left pressure, and right pressure, which were reported as percentages of the total foot pressure, and the pelvic rotation (°) (Figure 2).
For the dynamic plantar pressure parameters, the software automatically divides the foot into 10 masked zones: hallux (T1), toes 2–5 (T2–5), first to fifth metatarsals (M1, M2, M3, M4, and M5), midfoot (MF), medial heel (MH), and lateral heel (LH) (Figure 3). Only the most clinically relevant parameter, peak pressure (PP, kPa), was selected for evaluation. Eventually, 10 parameters were assessed: PP of 10 masked zones.
STATISTICAL ANALYSIS:
Statistical analysis was performed using SPSS version 24.0 software (SPSS, Inc., IL, USA). The data were explored for outliers and distribution. Normally distributed data are presented as mean±standard deviation.
Results
THE DEMOGRAPHIC INFORMATION OF SUBJECTS:
From March 2018 to April 2021, 106 consecutive patients satisfying the inclusion criteria were recruited into this research. Among those patients, 4 refused to participate in the tests, another 5 could not walk without aid, and another 3 could not generate enough planter pressure data. Eventually, 94 patients participated and completed the experiment successfully, and their test data were selected for further analysis. According to the patients’ KOA severity, they were divided into 3 groups: 30 in the early-stage group, 37 in the mid-stage group, and 27 in the end-stage group. Among the 3 groups, there were no significant differences in age, height, weight, BMI, foot length, foot width, affected side, or gender (P>0.05), and there were significant differences in pain severity (P<0.001) (Table 1).
DIFFERENCES IN STATIC PLANTAR PRESSURE DISTRIBUTION OF EACH GROUP:
The analysis of static plantar pressure distribution showed significant differences in left pressure, right pressure, and pelvic rotation among the 3 groups (P<0.05). The subsequent pairwise comparisons showed significant differences in left pressure and right pressure between patients of the early-stage and end-stage groups(P<0.001). For the pelvic rotation, there were significant differences between patients of the early-stage and end-stage groups (P<0.001), as well as between the mid-stage and end-stage groups (P<0.001). See Table 2 for detailed data.
CORRELATION BETWEEN THE CLINICAL STAGE OF KOA AND THE STATIC PLANTAR PRESSURE DISTRIBUTION:
The Spearman rank correlation analysis showed that patients’ clinical stage was positively correlated with the static pressure on the unaffected side (left affected, r=0.875, P<0.001; right affected, r=0.557, P<0.001, respectively), and was negatively correlated with the static pressure on the affected side (left affected, r=−0.875, P<0.001; right affected, r=−0.557, P<0.001, respectively). In addition, there was a positive correlation between clinical stage and pelvic rotation (left affected, r=0.369, P=0.015; right affected, r=0.378, P=0.010, respectively). See Table 3 for detailed data.
DIFFERENCES BETWEEN THE DYNAMIC PLANTAR PRESSURE DISTRIBUTION OF EACH GROUP:
The result of dynamic plantar pressure distribution showed that, for the affected side, there were significant differences in the PP of T1, T2–5, M5, MF, and LH zones (P<0.05). for the unaffected side, the significant differences in the PP appeared in M2, M3, and M4 zones (P<0.05). The subsequently pairwise comparisons’ results are shown in Table 4.
CORRELATION BETWEEN THE CLINICAL STAGE OF KOA AND THE DYNAMIC PLANTAR PRESSURE DISTRIBUTION:
The Spearman rank correlation analysis showed that, for the affected side, the patients’ clinical stage was positively correlated with the PP of M5 and LH zone (r=0.289, P=0.011; r=0.265, P=0.013, respectively), and negatively correlated with the PP of T1 and T2–5 zone (r=−0.221, P=0.040; r=−0.338, P=0.002, respectively). For the unaffected side, there were positive correlations between the clinical stage and the PP in M2, M3, and M4 zones (r=0.218, P=0.038; r=0.435, P<0.001; r=0.309, P=0.004, respectively). See Table 5 for details.
ORDINAL MULTINOMIAL LOGISTIC REGRESSION:
Ordinal multivariate logistic regression was used to analyze the independent influencing factors of clinical stage of knee osteoarthritis. The clinical stage was set as the dependent variable, and setting the PP in T1, T2–5, M5, MF, LH zone on the affected side and PP in M2, M3, M4 zone on the unaffected side as covariates, the results showed that the PP in T2–5 and LH zone on the affected side and the PP in M3 zone on the unaffected side were independent influencing factors of the clinical stage of knee osteoarthritis (β=−0.386, 0.187, 0.673, respectively,
Discussion
The present study examined the associations of KOA severity with static and dynamic plantar pressure among patients with unilateral KOA, and demonstrated that the plantar pressure distributions varied in different stages of KOA. Furthermore, the current study also revealed that the plantar pressure distributions were significantly correlated with KOA severity, which could provide useful information on the postural sways and balance status of KOA patients.
Static plantar pressure analysis is widely used in the study of patients’ balance function [10]. Previous studies have reported abnormal balance function in patients with KOA, which is characterized as a great amount of swing on the center of gravity in the left and right directions during one-leg stance and impaired postural control [8,9,11]. In the present study, the static plantar pressure of unilateral KOA patients tended to be distributed on the unaffected side, which is caused by a compensatory behavior of trunk lateral flexion to alleviate pain on the knee [5,12], manifested as pelvic rotation and reduction of weight bearing on the affected side. The present study also demonstrated that balance deficits were further exacerbated as KOA progresses, indicating that people with end-stage KOA have a higher risk of falls.
Numerous previous studies have investigated dynamic plantar pressure distribution in KOA patients. Panyarachun et al [13] noted that the foot load of KOA patients tends to be laterally distributed. Zhang et al [8] investigated the plantar pressure distribution of KOA and found that the varus of the knee joint leads to an increase in PP in the M5 and LH zones. The current findings are consistent with the above studies. It is worth noting that the present study also found that the PP in the T1 and T2–5 zones gradually decreased with the progression of KOA. Previous studies have shown that the toe-off period of the affected side in KOA patients is longer than that of the unaffected side [14]. According to the pathological process of KOA, due to changes in lower-limb alignment and muscle strength, before the toe-off period, the process of knee flexion to knee extension is prolonged, and in some severe cases, the knee joint even does not allow full extension [15], which greatly reduces the strength to push off the ground. As compensation, KOA patients tend to use the metatarsal heads to contact and push off rather than the toes. Therefore, during the toe-off period, the muscles that control the toes’ plantar flexion stop functioning in advance, resulting in toe dorsiflexion and metatarsal heads loading, thereby reducing the PP in the T1 and T2–5 zones.
Abnormal plantar pressure distribution was also found in the unaffected foot of unilateral KOA patients. In normal adults, the load of M1 zone is twice that of the M2–4 zone [5], while in present study, the PP in M2–4 zone increased significantly with KOA progression, which indicates that the plantar pressure distribution of the unaffected side also tends to be laterally distributed. Since the lateral longitudinal arch is more conducive to maintaining stability [10,16], the loading is shifted to the lateral side to redistribute the center of gravity and maintain balance. Over time, compensatory varus also occurs in the unaffected ankle joint, and even affects the unaffected knee joint [17]. Therefore, the abnormal distribution of plantar pressure on the unaffected side of patients with unilateral KOA also deserves attention, especially in patients with end-stage KOA.
In the present study, an ordinal multinomial logistic regression analysis was conducted, and the results showed that the PP in T2–5 and LH zone on the affected side and the PP in M3 zone on the unaffected side were independent influencing factors of the clinical stage of knee osteoarthritis. Although this initial cross-sectional study was not designed to identify a potential marker of KOA, it raises the possibility that plantar pressure parameters might serve as markers and may ultimately be useful as outcome measures. We believe that plantar pressure analysis can be used as a monitoring tool in rehabilitation programs, which has the advantage of being easy to administer and more objective and sensitive. The rehabilitation programs targeting these abnormal plantar pressure distributions could be beneficial for restoring balance function in individuals with KOA.
The study has certain limitations. First, we did not include patients with bilateral KOA, due to the differences between unilateral and bilateral KOA [18], so the results of the present study cannot be universally applied to patients with bilateral KOA, and the distribution of plantar pressure in bilateral KOA remains to be further investigated. Second, the present study only analyzed PP in different zones, and other commonly used clinical parameters such as contact area, contact time, and pressure-time integral were not analyzed. These parameters may provide more reference for clinical diagnosis and treatment, and further research is needed on this aspect. Last but not the least, the present study aimed to investigate the influence of KOA severity on plantar pressure distributions, and verify whether the plantar pressure analysis can detect these differences. Although the results are positive, further studies are needed before applying our findings in clinical practice.
Conclusions
For static plantar pressure distribution, the clinical stages are positively correlated with pressure on the unaffected side and pelvic rotation. For the dynamic plantar pressure distribution, the clinical stages were positively correlated with PP of M5, MF, and LH zones on the affected side and PP of M2–4 zones on the unaffected side, and were negatively correlated with PP of T1 and T2–5 zone. Moreover, the PP of T2–5 and LH zones on the affected side and PP of M3 zone on the unaffected side could be independent influencing factors of KOA stages. These findings suggest that with the progression of KOA, the static plantar pressure tends to be distributed on the unaffected side, and the dynamic plantar pressure tends to be distributed laterally on both feet. The plantar pressure distributions of both feet in unilateral KOA patients are abnormal and closely related to the severity of KOA.
Figures
 Figure 1. Upright position X-ray of patients with different Kellgren-Lawrence grades of knee osteoarthrosis.(A) Grade I, slight narrowing of knee joint space with suspicious osteophyte formation, and the patient was defined as early-stage; (B) Grade II, moderate narrowing of knee joint space with small osteophyte formation, and the patient was defined as mid-stage; (C) Grade III, obvious narrowing of knee joint space with moderate osteophyte formation, and the patient was defined as mid-stage; (D) Grade IV, severe narrowing of the knee joint space and massive osteophyte formation, and the patient was defined as end-stage.
Figure 1. Upright position X-ray of patients with different Kellgren-Lawrence grades of knee osteoarthrosis.(A) Grade I, slight narrowing of knee joint space with suspicious osteophyte formation, and the patient was defined as early-stage; (B) Grade II, moderate narrowing of knee joint space with small osteophyte formation, and the patient was defined as mid-stage; (C) Grade III, obvious narrowing of knee joint space with moderate osteophyte formation, and the patient was defined as mid-stage; (D) Grade IV, severe narrowing of the knee joint space and massive osteophyte formation, and the patient was defined as end-stage.  Figure 2. Schematic diagram of static plantar pressure analysis.The parameters include anterior pressure, posterior pressure, left pressure, right pressure, and pelvic rotation.
Figure 2. Schematic diagram of static plantar pressure analysis.The parameters include anterior pressure, posterior pressure, left pressure, right pressure, and pelvic rotation. 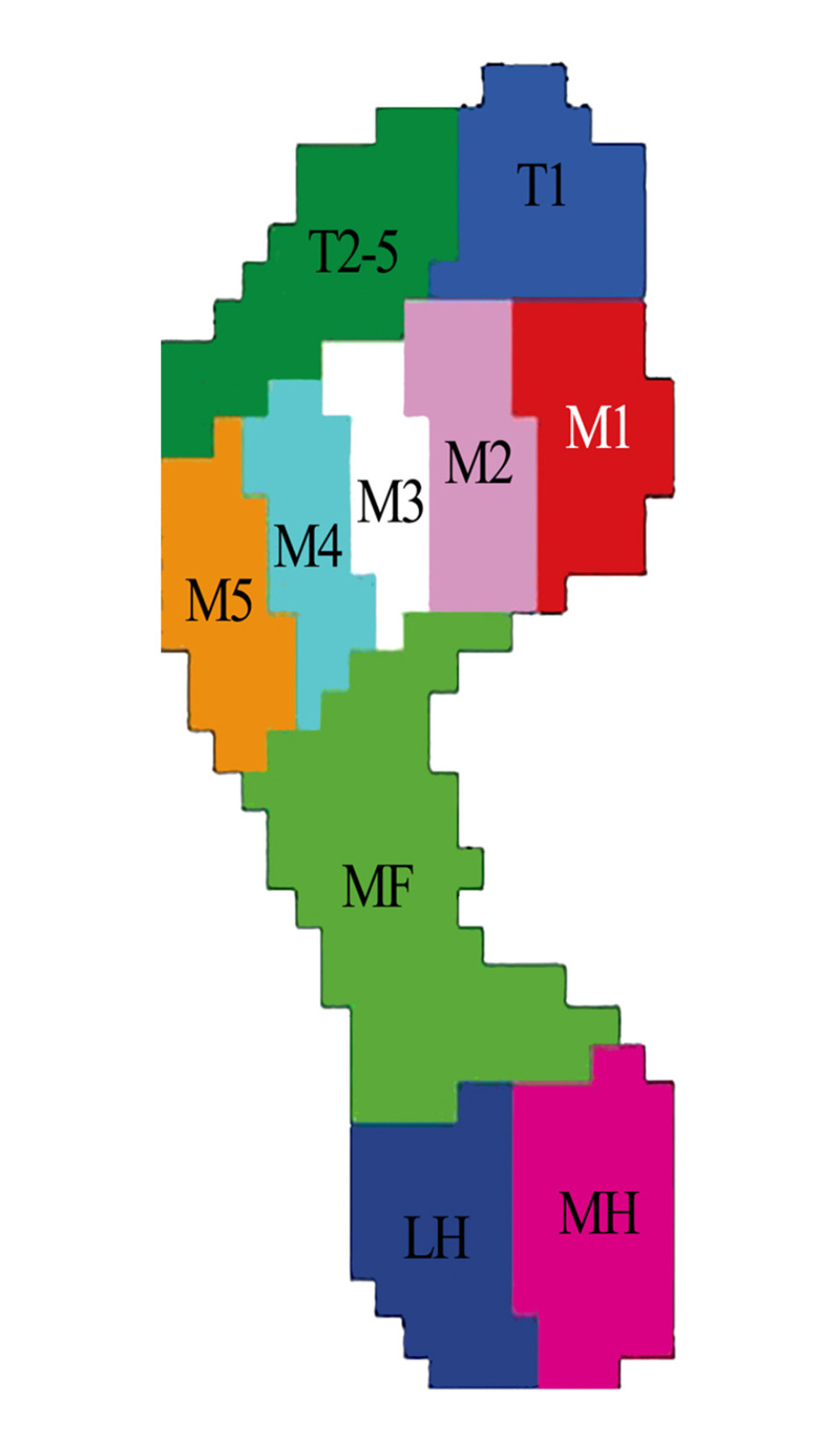 Figure 3. Schematic diagram of dynamic plantar pressure masked zones.The 10 masked zones include: hallux (T1), toes 2–5 (T2–5), first to fifth metatarsals (M1, M2, M3, M4, and M5), midfoot (MF), medial heel (MH), and lateral heel (LH).
Figure 3. Schematic diagram of dynamic plantar pressure masked zones.The 10 masked zones include: hallux (T1), toes 2–5 (T2–5), first to fifth metatarsals (M1, M2, M3, M4, and M5), midfoot (MF), medial heel (MH), and lateral heel (LH). Tables
Table 1. Demographic data for each group.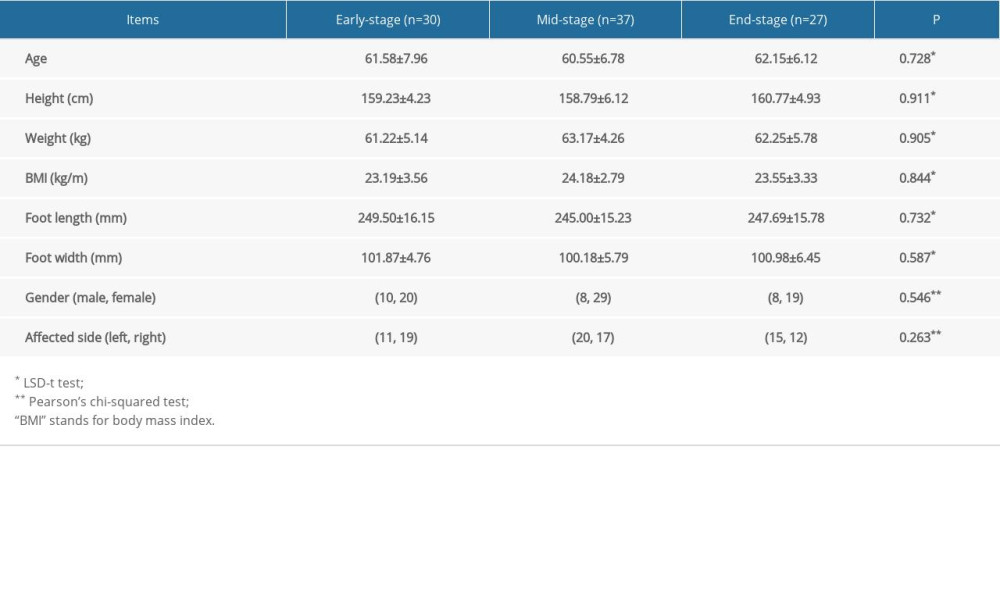 Table 2. Differences between the static plantar pressure distribution of each group.
Table 2. Differences between the static plantar pressure distribution of each group.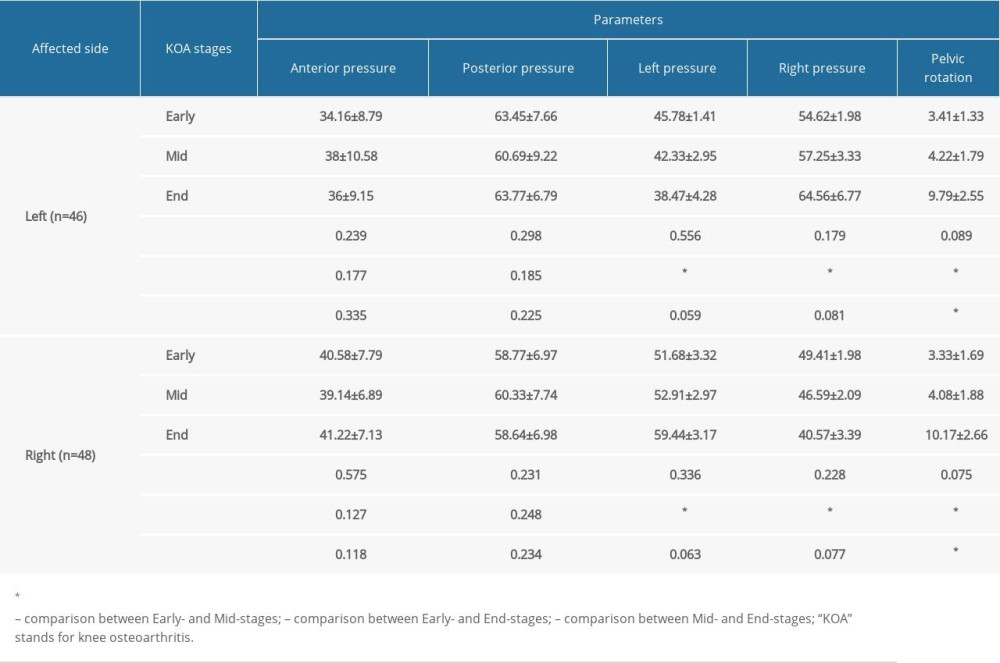 Table 3. Correlation between the clinical stage of KOA and the static plantar pressure distribution.
Table 3. Correlation between the clinical stage of KOA and the static plantar pressure distribution.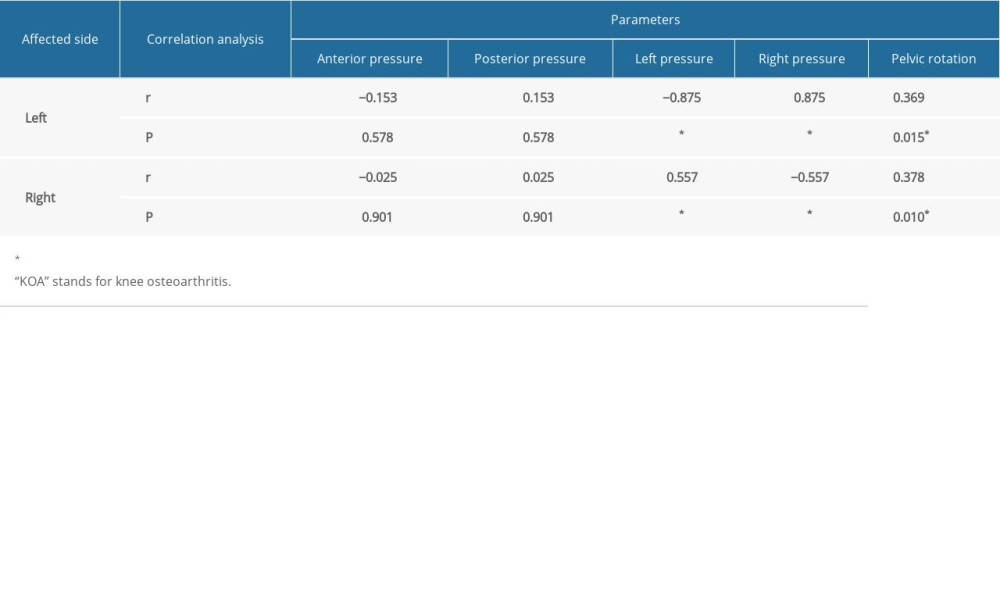 Table 4. Differences between the dynamic plantar pressure distribution of each group.
Table 4. Differences between the dynamic plantar pressure distribution of each group. Table 5. Correlation between the clinical stage of KOA and the dynamic plantar pressure distribution.
Table 5. Correlation between the clinical stage of KOA and the dynamic plantar pressure distribution.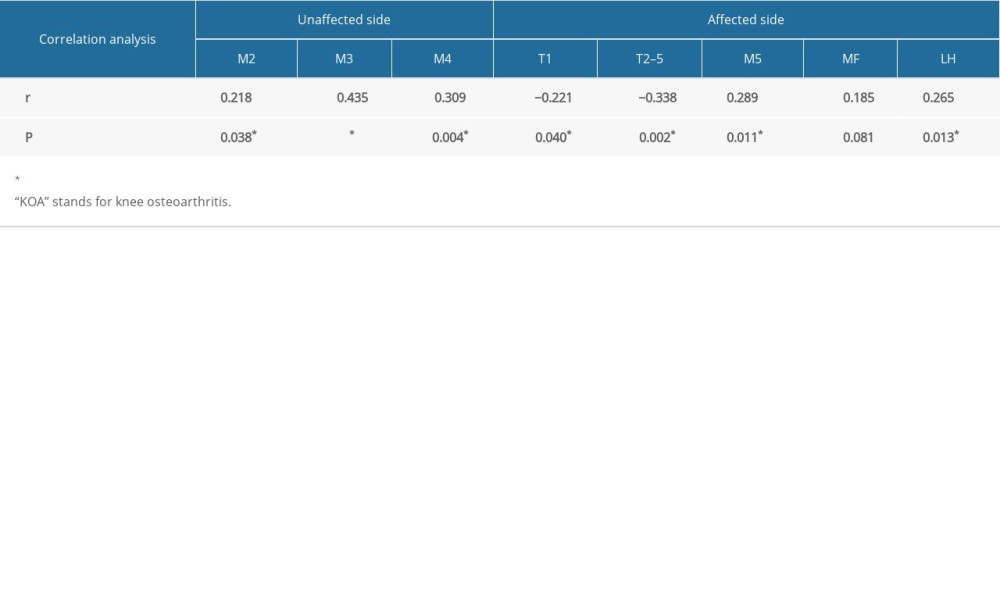
References
1. Hunter DJ, Bierma-Zeinstra S, Osteoarthritis: Lancet, 2019; 393(10182); 1745-59
2. Michael JW, Schlüter-Brust KU, Eysel P, The epidemiology, etiology, diagnosis, and treatment of osteoarthritis of the knee: Dtsch Arztebl Int, 2010; 107(9); 152-62
3. Jang S, Lee K, Ju JH, Recent updates of diagnosis, pathophysiology, and treatment on osteoarthritis of the knee: Int J Mol Sci, 2021; 22(5); 2619
4. Jasiewicz B, Klimiec E, Młotek M, Quantitative analysis of foot plantar pressure during walking: Med Sci Monit, 2019; 25; 4916-22
5. Xu C, Wen XX, Huang LY: J Foot Ankle Res, 2017; 10; 30
6. Xu C, Wei J, Yan YB, Pedobarographic analysis following ponseti treatment for unilateral neglected congenital clubfoot: Sci Rep, 2018; 8(1); 6270
7. Fryzowicz A, Murawa M, Kabaciński J, Reference values of spatiotemporal parameters, joint angles, ground reaction forces, and plantar pressure distribution during normal gait in young women: Acta Bioeng Biomech, 2018; 20(1); 49-57
8. Zhang Z, Wang L, Hu K, Liu Y, Characteristics of plantar loads during walking in patients with knee osteoarthritis: Med Sci Monit, 2017; 23; 5714-19
9. Lidtke RH, Muehleman C, Kwasny M, Block JA, Foot center of pressure and medial knee osteoarthritis: J Am Podiatr Med Assoc, 2010; 100(3); 178-84
10. Yu B, Xie Q, Xu J, Impairments and compensations of static balance and plantar load distribution in patients with chronic stroke: An observational study: J Manipulative Physiol Ther, 2021; 44(9); 734-42
11. Akimoto T, Kawamura K, Wada T, Gait cycle time variability in patients with knee osteoarthritis and its possible associating factors: J Phys Ther Sci, 2022; 34(2); 140-45
12. Vassão PG, Silva BA, de Souza MC, Level of pain, muscle strength and posture: Effects of PBM on an exercise program in women with knee osteoarthritis – a randomized controlled trial: Lasers Med Sci, 2020; 35(9); 1967-74
13. Panyarachun P, Angthong C, Jindasakchai P, Abnormal foot pressure in older adults with knee osteoarthritis: A systematic review: Eur Rev Med Pharmacol Sci, 2022; 26(17); 6236-41
14. Kaufman KR, Hughes C, Morrey BF, Gait characteristics of patients with knee osteoarthritis: Chin J Clin Med, 2014; 34(7); 907-15
15. Wang Y, Zhang K, Zeng J, Coordination of lower limbs in patients with knee osteoarthritis during walking: Gait Posture, 2021; 83; 160-66
16. Fukano M, Fukubayashi T, Motion characteristics of the medial and lateral longitudinal arch during landing: Eur J Appl Physiol, 2009; 105(3); 387-92
17. DeMik DE, Marinier MC, Gulbrandsen TR, Does isolated unilateral hip or knee osteoarthritis lead to adverse changes in extremity composition?: Iowa Orthop J, 2022; 42(1); 163-67
18. Creaby MW, Bennell KL, Hunt MA, Gait differs between unilateral and bilateral knee osteoarthritis: Arch Phys Med Rehabil, 2012; 93(5); 822-27
Figures
Figure 1. Upright position X-ray of patients with different Kellgren-Lawrence grades of knee osteoarthrosis.(A) Grade I, slight narrowing of knee joint space with suspicious osteophyte formation, and the patient was defined as early-stage; (B) Grade II, moderate narrowing of knee joint space with small osteophyte formation, and the patient was defined as mid-stage; (C) Grade III, obvious narrowing of knee joint space with moderate osteophyte formation, and the patient was defined as mid-stage; (D) Grade IV, severe narrowing of the knee joint space and massive osteophyte formation, and the patient was defined as end-stage.Figure 2. Schematic diagram of static plantar pressure analysis.The parameters include anterior pressure, posterior pressure, left pressure, right pressure, and pelvic rotation.Figure 3. Schematic diagram of dynamic plantar pressure masked zones.The 10 masked zones include: hallux (T1), toes 2–5 (T2–5), first to fifth metatarsals (M1, M2, M3, M4, and M5), midfoot (MF), medial heel (MH), and lateral heel (LH). Tables
Table 1. Demographic data for each group.Table 2. Differences between the static plantar pressure distribution of each group.Table 3. Correlation between the clinical stage of KOA and the static plantar pressure distribution.Table 4. Differences between the dynamic plantar pressure distribution of each group.Table 5. Correlation between the clinical stage of KOA and the dynamic plantar pressure distribution.Table 1. Demographic data for each group.Table 2. Differences between the static plantar pressure distribution of each group.Table 3. Correlation between the clinical stage of KOA and the static plantar pressure distribution.Table 4. Differences between the dynamic plantar pressure distribution of each group.Table 5. Correlation between the clinical stage of KOA and the dynamic plantar pressure distribution. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387