02 June 2023: Clinical Research
Differences in Outcomes Between Human Epidermal Growth Factor Receptor 2 (HER2)-Positive Metastatic Breast Cancer Patients in Upper Middle-Income versus High-Income Countries: A Retrospective Study from 4 Oncology Centers
Dragana Miletić1ADEF*, Marija Kraljević1ADEF, Emir Sokolović2CDE, Majana Soče3B, Marijana Milović-Kovačević4B, Simonida Bobić4B, Timur Cerić2ABDE, Stjepko Pleština3A, Semir Bešlija2AE, Inga Marijanović15ADEDOI: 10.12659/MSM.940356
Med Sci Monit 2023; 29:e940356






Abstract
BACKGROUND: Therapeutic options for human epidermal growth factor 2 (HER2)-positive metastatic breast cancer (mBC) are developing rapidly. This study aimed to determine the differences in the survival outcomes of patients with HER2-positive mBC in relation to access to anti-HER therapy at 3 oncology centers in upper-middle-income countries (UMICs) and 1 oncology center in a high-income country (HIC).
MATERIAL AND METHODS: We retrospectively identified 42 patients from Croatia (HIC), 71 patients from Serbia (UMIC), and 57 from Bosnia and Herzegovina (UMIC) diagnosed with HER2-positive mBC who were treated between January 2015 and December 2020. The pathohistological features of the tumors were obtained from the pathological findings, which were made according to standard procedures for each center. Patients were treated depending on the availability of therapy, which differed for centers in different countries. We evaluated disease-free survival, progression-free survival, and overall survival (OS) based on the availability of first- and second-line anti-HER2 therapy in UMICs vs HIC.
RESULTS: OS in first-line therapy was better in patients treated with dual HER2 blockade than in patients treated without dual HER2 blockade, P<0.001. OS in second-line therapy was significantly better in patients treated with trastuzumab emtansine than in patients treated with other reported regimens, P=0.004.
CONCLUSIONS: Results of our study showed superior survival among patients who were treated with dual first-line HER2 therapy as well as second-line trastuzumab emtansine therapy than in those patients in other centers where these drugs were not available. Raising awareness about this could help improve the situation.
Keywords: Breast Neoplasms, Receptor, erbB-2, Neoplasm Metastasis, Antineoplastic Agents, Survival, Costs and Cost Analysis, Humans, Female, Ado-Trastuzumab Emtansine, Retrospective Studies, Trastuzumab, Developed Countries, Antibodies, Monoclonal, Humanized, Antineoplastic Combined Chemotherapy Protocols
Background
Low- and middle-income nations have greater breast cancer mortality rates than high-income nations; therefore, there has been an international movement to increase the capacity for breast cancer care in the past 10 years [1]. According to estimates, 2.3 million new cases of female breast cancer would be diagnosed globally in 2020, accounting for 11.7% of all cancer cases, 1 in 4 cancer diagnoses, and 1 in 6 cancer deaths [2]. Breast cancer ranks first for mortality in 110 nations and first for incidence in 159 of 185 countries [2]. Transitional countries have higher incidence rates than do developing countries (55.9 and 29.7 per 100 000, respectively) [2]. The cancer burden in Europe, which accounts for a sizable portion of the global burden, is a significant area of concern [3]. Breast cancer is the most frequently diagnosed cancer in women across all of Europe and the leading cause of cancer death in women in most nations [3].
Breast tumors that are human epidermal growth factor receptor 2 (HER2)-positive account for 15% to 20% of all cases of breast cancer [4].
The National Comprehensive Cancer Network Task Force concluded that the clinical decision-making for the treatment of breast cancer in both adjuvant and metastatic contexts requires precise assignment of the HER2 status of invasive breast cancer [5]. At least one-third of patients with HER2-positive breast cancer already have regional or distant metastatic disease or develop it later [6].
The preferred therapy for HER2-positive metastatic breast cancer (mBC) is systemic anti-HER2 therapy combined with chemotherapy. Dual therapy (trastuzumab-pertuzumab) in addition to chemotherapy is the criterion standard for the first-line treatment of HER2-positive mBC. Trastuzumab emtansine (T-DM1) is the recommended therapy for HER2-positive mBC in second-line treatment [7].
Nonetheless, in certain patients with hormone receptor-positive HER2-positive breast cancer, chemo-free anti-HER2 therapies could also be considered. Many novel anti-HER2 medicines are becoming accessible in the third-line context and beyond, including tucatinib, fam-trastuzumab deruxtecan-nxki (DS-8201a), neratinib, and margetuximab-cmkb [8].
Advanced HER2-positive breast cancer has been treated with HER2-directed monoclonal antibodies, small molecule tyrosine kinase inhibitors (TKIs), and antibody drug conjugates [9–12]. Continued HER2 suppression after progression with HER2-directed therapy is recommended [6].
Patients with mBC have an increasing number of well-known options for therapy and condition monitoring, but little is known about how different types of care are delivered [13]. Access to healthcare facilities is restricted in low- and middle-income nations, and most patients do not even have access to dual anti-HER2 medication [14].
The world’s economies are divided into 4 income groups by the World Bank: low, lower-middle, upper-middle, and high income. Currently, the World Bank identifies Bosnia and Herzegovina (BiH) and Serbia as upper-middle-income countries (UMICs) and Croatia as a high-income country (HIC) [15]. The availability of drugs for each individual oncology clinical center varies by country and is the same for each individual center in a given country.
Targeted therapies for HER2-positive mBC in BiH are available through the Solidarity Fund, a branch of the federal government in charge of allocating expensive drugs. Trastuzumab has been available on the list of the Solidarity Fund since January 2004, and pertuzumab since 2017. Trastuzumab is available for all patients with an indication for treatment, and there is no waiting list, while there is a waiting list for pertuzumab, and it is not available for all patients with HER2-positive mBC. Currently, there is still no available T-DM1 drug treatment, although we are witnessing the development of anti-HER2 therapy and the introduction of trastuzumab deruxtecan in the second line of mBC treatment [16].
The situation is similar in Serbia, where trastuzumab has been available since 2006, pertuzumab since 2019, and T-DM1 is not available for the treatment of patients with HER2-positive mBC [17].
In Croatia, an HIC, there is availability of all mentioned therapies through the Croatian Institute for Health Insurance. In the first decade of the 2000s, trastuzumab entered the list of medicines of the Institute for the treatment of HER2-positive mBC, pertuzumab in 2015, and T-DM1 in 2016 [18].
Several studies conducted between 2000 and 2015 reported that almost 15% of patients in the United States, up to 54% in Europe, and almost 50% in China did not receive trastuzumab or any other anti-HER2 therapy to treat mBC. Difficulties in anti-HER2 therapy access are complex and include worries about drug funding and the high cost of patient care that has been observed worldwide [19].
According to our literature review, few studies have been conducted to describe outcomes of patients with HER2-positive mBC regarding access to therapy among different countries and there is lack of evidence in this area. These were mostly studies that compared the outcomes with the results of previous clinical studies [20] or that assessed what the outcome would be according the availability of anti-HER therapy [21].To the best of our knowledge, no previous published research has evaluated outcomes of patients with HER2-positive mBC regarding access to therapy for this disease in different income countries. Data on the differences of the availability and type of therapy as well as data of survival for HER2-positive mBC for the countries of BiH and Serbia as UMICs and Croatia as an HIC are limited.
Therefore, we aimed to determine the differences in the survival outcomes of patients with HER2-positive mBC in relation to access to anti-HER therapy at 3 oncology centers in UMICs and 1 oncology center in an HIC.
Material and Methods
ETHICS STATEMENT:
Ethics approval was obtained from the Institutional Ethics Committee (number 293/23). This study was performed following institutional guidelines, and all procedures followed were in accordance with the Helsinki Declaration of 1975 in its most recent version.
PATIENTS:
We retrospectively identified 170 patients diagnosed with HER-2 positive mBC who were treated between January 2015 and December 2020 in 4 oncology centers. Three oncology centers were from UMICs: Department of Oncology, University Hospital Mostar (BiH); Oncology clinic, Clinical Center University of Sarajevo (BiH); and Department for Radiation Oncology and Diagnostics, Institute of Oncology and Radiology of Serbia (Serbia). One oncology center was from an HIC: Department of Oncology, University Hospital Centre Zagreb (Croatia). There were a total of 42 patients from Croatia, 71 patients from Serbia, and 57 patients from BiH.
The following information was gathered about the patients: sex, age, family positivity of breast cancer, menopausal status, method of histopathological analysis, histological type, comorbidities, histopathological features (estrogen and progesterone status, HER2 status, Ki-67 index, e-cadherin), metastatic location, number of metastatic sites, disease-free survival (DFS), Eastern Cooperative Oncology Group (ECOG) status, first-line and second-line progression-free survival (PFS), overall-survival (OS), and toxicities. The pathohistological features of the tumor were obtained from the pathological findings, which were made according to standard procedures for each center. The testing for HER2 status was conducted according to the Guidelines of the American Society of Clinical Oncology/College of American Pathologists from 2013 and then from 2018 [22,23]. Patients were treated depending on the availability of therapy, which differed for centers in different countries. The hospital case records provided clinical information about patients who were identified via the hospital registry. Information about patients in BiH treated with trastuzumab and pertuzumab were obtained from Health Insurance and Reinsurance Institute of the FBiH (Solidarity Fund).
All patients with breast cancer included in the study were ≥18 years old and diagnosed with HER2-positive mBC.
ASSESMENT OF PATIENT OUTCOMES:
We evaluated DFS, PFS, OS, and toxicity due to the availability of anti-HER2 therapy (first and second line) in UMICs vs HIC.
The OS was calculated by accounting for the time from the date of surgery or biopsy to the date of death or the most recent follow-up. PFS was determined by taking into account the period from the date of first-line or second-line therapy to the date of progression, or the most recent follow-up, and DFS was calculated from the date of surgery or biopsy to the date of distant metastasis.
STATISTICAL ANALYSIS:
IBM SPSS Statistics v. 23.0 was used for statistical analysis. We defined descriptive measures, including absolute values and percentages.
Frequencies of nominal categorical variables were compared using the chi-square test. Post hoc chi-square testing was performed to analyze adjusted residuals and to identify cells with statistically significant z-scores in cross tabulation.
One-way analysis of variance was used to compare the values of continuous parametric variables between multiple groups of patients, The Kruskal-Wallis test was used to compare the values of continuous non-parametric variables between multiple groups of patients. The Mann-Whitney test was used to compare the values of a continuous variables between 2 groups of patients. Size of influence (r) of the difference in the values of the continuous variable between 2 groups was determined according to Cohen’s criterion.
The Kaplan-Meier method with log-rank (Mantel-Cox) test was used to evaluate the differences of survival between certain groups. Cox regression hazard analysis (univariate and multivariate) was performed to evaluate the influence of several factors on the overall survival of patients. Variables with statistically significant results in the univariate analysis were included in the multivariate Cox regression hazard analysis.
Results
BASELINE CHARACTERISTICS OF PATIENTS:
The baseline characteristics of the patients are presented in Table 1. There were 170 patients, with a mean age of 55.64±12.05 years in Zagreb, 59.17±9.75 years in Belgrade, 58.69±10.56 years in Sarajevo, and 57.86±10.13 years in Mostar. Histological tumor type, tumor hormone receptor status (estrogene and progesterone), and Ki-67 value are also described for each center separately.
Table 2 shows the location of metastases, number of metastatic sites, and ECOG performance status of the patients.
TYPE OF FIRST- AND SECOND-LINE THERAPY AND RESPONSE TO THERAPY:
Tables 3 and 4 summarize the type of first-line and second-line treatment in each center.
Types of first-line treatments were taxane-based chemotherapy + dual HER2 blockade; chemotherapy-only; chemotherapy + trastuzumab; hormonal therapy; hormonal therapy + dual HER2 blockade; hormonal therapy + trastuzumab; trastuzumab; taxanes-based chemotherapy + dual HER2 blockade + hormonal therapy; and chemotherapy + dual HER2 blockade + hormonal therapy. The types of second-line treatments were T-DM1; chemotherapy-only; chemotherapy + trastuzumab; hormonal therapy; hormonal therapy + dual HER2 blockade; hormonal therapy + trastuzumab; hormonal therapy + TKI; chemotherapy + dual HER2 blockade; and trastuzumab.
Figures 1 and 2 show the patient responses to these first-line and second-line therapies.
TIME FROM DIAGNOSIS TO TREATMENT INITIATION:
The Kruskal-Wallis test revealed a statistically significant difference in time from diagnosis to initiation of treatment among clinical centers (Belgrade, n=71; Mostar, n=28; Sarajevo, n=29; Zagreb, n=42), χ2 (3, n=170)=38.9,
The log rank (Mantel-Cox) test did not reveal a statistically significant difference in OS and PFS between patients who waited less than 2 months from diagnosis to start treatment and those who did (P=0.39; P=0.95, respectively; Figures 3, 4).
TOXICITY OF THE TREATMENTS:
In the first-line treatment, 77 (45.3%) of treated patients (N=170) reported adverse effects to treatment.
Hematological toxicity was identified in 52 (30.6%) patients, cardiotoxicity in 12 (7.1%) patients, allergic reactions in 7 (4.1%) patients, and other types of adverse effects in 37 (21.8%) patients. Toxicity was the cause of treatment discontinuation in 21 (12.4%) patients and the cause of dose reduction in 26 (15.3%) patients.
Second-line treatment was prescribed in 118 patients. In the second-line treatment, 38 (32.2%) of treated patients (N=118) reported adverse effects from treatment. Hematological toxicity was identified in 24 (20.3%) patients, cardiotoxicity in 6 (5.1%) patients, allergic reactions in 3 (2.5%) patients, and other types of adverse effects in 12 (10.2%) patients. Toxicity was the cause of treatment discontinuation in 12 (10.2%) patients and the cause of dose reduction in 10 (8.47%) patients.
SURVIVAL ANALYSIS:
In the studied sample of patients (N=170), the median (range) first-line PFS was 12 (2–51) months. Median (range) second-line PFS was 5 (0–29) months, and median (range) OS was 34 (13–76) months.
The log rank (Mantel-Cox) test revealed a statistically significant difference in OS between patients treated in different oncology clinics (χ2=36.34, P<0.001). Median OS for patients treated in Zagreb was not reached, patients in Sarajevo had median OS (95% CI) of 36 (27.8–44.2) months, patients in Belgrade 33 (25.7–40.3) months, and patients in Mostar 28 (16.0–39.9) months (Figure 5).
First-line treatment PFS was significantly different between patients treated in different centers (χ2=38.5 P<0.001). Median first-line PFS (95% CI) for patients treated in Zagreb was 36 (28.4–43.5) months. Patients in Sarajevo had first-line PFS of 12 (9.9–14.1) months, patients in Belgrade 8 (2.2–13.8) months, and patients in Mostar 22 (14.3–29.7) months (Figure 6).
Second-line treatment PFS was not significantly different between patients treated in different centers (χ2=5.5; P=0.138; Figure 7). Patients who had visceral metastases had significantly worse OS (χ2=25.09, P<0.001), with median (95% CI) of 30 (25.1–34.9) months, than patients who did not had visceral metastases, with median of 65 (49.6–80.4) months (Figure 8).
Survival was not significantly different between patients divided in 2 groups based on the hormone-receptor positivity of the tumor and the presence of comorbidities, bone metastases, and central nervous system metastases.
COX REGRESSION HAZARD ANALYSIS:
Cox regression hazard analysis was performed to evaluate the influence of several factors on the OS of patients included in our study.
Baseline characteristics of the study population from Table 1, variables from Table 2, and certain treatments were evaluated for possible influence on OS.
Cox regression hazard analysis showed that age at the time of diagnosis, menopausal status, first-line dual anti-HER2 treatment, and treatment with T-DM1 in the second-line had a statistically significant influence on OS (Table 5).
Variables with statistically significant results in the univariate analysis were included in the multivariate Cox regression hazard analysis. T-DM1 in the second-line treatment was shown to be the only independent marker of OS in our study,
Kaplan-Meier analysis showed a statistically significant difference in the OS between patients treated without dual HER2 blockade in the first-line of treatment, with a median survival (95% CI) of 35 (29.8–40.2) months, vs patients treated with dual HER2 blockade (median survival was not reached), P<0.001 (Figure 9).
Moreover, survival was significantly better in patients treated with T-DM1 in the second-line treatment (median survival was not reached) than in patients treated with other regimens reported in Table 4 (median survival [95% CI] of 35 [28.5–41.5] months, P=0.004; Figure 10).
Discussion
In our study, the analysis showed a better first-line OS in patients treated with dual HER2 blockade than in patients treated without dual HER2 blockade. Moreover, OS was significantly better in patients treated with T-DM1 as second-line therapy than in patients treated with other reported regimens.
Our results confirmed the results of previous studies. Therapeutic options for HER2-positive mBC have improved during the last 10 years. For individuals with metastatic disease, trastuzumab was licensed in the United States in 1998 and in the European Union a few years later. Studies have shown the benefit of adding trastuzumab to chemotherapy in the treatment of HER2-positive mBC [24] and as a single agent in mBC that has progressed after chemotherapy [25]. Monoclonal HER2-targeting antibodies (trastuzumab and pertuzumab) plus taxane is the standard of care for initial therapy in patients with HER2-positive mBC, based on the phase 3 CLEOPATRA trial. According to the study, in patients with HER2-positive mBC, the addition of pertuzumab to trastuzumab and docetaxel, as compared with the addition of placebo, significantly improved the median OS to 56.5 months and extended the results of earlier analyses that demonstrated the effectiviness of this combination therapy [26]. Preferred second-line therapy (at the time of this study) was the antibody-drug conjugate T-DM1, based on EMILIA and and TH3RESA trials. Treatment with T-DM1 significantly improved PFS (median survival, 9.6 months, vs 6.4 months with lapatinib plus capecitabine) [27]. Moreover T-DM1 significantly improved OS compared with treatment of the doctor’s choice in patients who had progressed to 2 or more HER2-directed regimens [28].
In addition to our results confirming the results of earlier studies, it is important to emphasize that this study showed that the outcomes were highly dependent on the availability of therapy, which differed in UMICs and HICs. Also, some earlier studies warned about the importance of the availability and access to anti-HER2 therapy for HER2-positive mBC, which differs among many countries in the world. As expected, results of outcomes are significantly impacted by the limited availability and access to anti-HER2 drugs [20,21,29].
Today, trastuzumab deruxtecan is the new standard of care in second-line HER2-positive mBC therapy due to the development of new-generation antibody-drug conjugates [30]. Results from the DESTINY-Breast-03 trial showed the superiority of trastuzumab deruxtecan (T-DXd) over T-DM1 in second-line mBC therapy [31].
Even in 2023, there are waiting lists for pertuzumab in the UMICs in our study, and T-DM1 is not even on those lists; therefore, anti-HER2 therapy is not available to the general population in these countries, and the results of our study show how the unavailability of targeted anti-HER2 therapy in UMICs results in statistically significantly worse treatment outcomes.
According to a technical report by the World Health Organization, countries with lower national incomes had lower availability of cancer medicines, or availability only with higher out-of-pocket patient payments, especially for higher-cost medicines, including targeted therapies [32]. The results of the present study proved the importance of ensuring patients’ timely and equal access to drugs that have proven safety and efficacy.
Although our data showed no difference in survival between patients who received therapy within 2 months and those after 2 months, it is essential to emphasize that in less developed and medium-developed countries, there are waiting lists for many drugs [16], which contributes to the fact that drugs are approved later and that treatment is started later, which all contributes to a worse treatment effect and survival [33].
To assess the generalizability of clinical trial results across a broad patient population and among individuals who would not have met the inclusion criteria for a clinical trial, real-world evidence is crucial [34]. The results of a real-world study from China showed that patients in resource-limited regions were less likely to receive trastuzumab-based therapy, and patients in resource-abundant regions (gross domestic product per capita >$15 000 or trastuzumab included in Medicare) were more likely to receive trastuzumab than those in resource-limited regions during their early stage (37.3% vs 13.0%) and metastatic stage (87.5% vs 42.3%) [35].
According to findings from a global survey, up to two-thirds of patients in low middle-income countries with early HER2-overexpressing breast cancer were not receiving the advised adjuvant HER2-directed therapy, mostly because the test was not readily available and the cost of treatment was prohibitive [36].
Real-world evidence also reveals important information about the toxicity of the applied therapy, because the therapies are used in patients with numerous comorbidities, which are not normally represented in randomized clinical studies [37]. In the present study, in the first-line treatment, 45.3% of treated patients reported adverse effects of the treatment. It is also very imporant to emphasize the effects of adverse events on treatment discontinuation and dose reduction, which could have an impact on response and survival. Many real-world patients receive systemic therapy and may benefit even if they don’t meet the standard eligibility requirements for clinical studies. The proportion of real-world patients in clinical trials will improve, and the results’ generalizability will rise when the inclusion criteria become widened [38]. Due to strict exclusion criteria, a substantial percentage of real-world patients are not eligible to take part in clinical trials, although many continue to receive therapy in everyday practice. It is necessary to enlarge the cancer clinical trials’ eligibility requirements [39].
This study had limitations, including its retrospective design, limited patient population, sparse and under reporting data in low- and middle-income nations, which may have an impact on the findings.
Conclusions
As the results of our study showed superiority in survival among those patients who were treated with dual HER2 therapy in the first line as well as T-DM1 in the second line than in those patients in other centers where these drugs were not available, we can conclude that these outcomes may help to improve anti-HER2 therapy for HER2-positive mBC, particularly in low- and middle-income regions with limited access to these potentially effective, but still expensive, targeted drugs.
Dual anti-HER2 therapy in combination with chemotherapy in first-line therapy and with T-DM1 in second-line therapy was linked with improved survival outcomes compared to patients treated without anti-HER2 therapy in this real-world group of patients with HER2-positive mBC and alerts us about the importance of equalizing care for all oncology patients.
We anticipate that the findings of our study will have an impact on how best to treat the aforementioned patient group in UMICs. We must map the future and create workable methods to address potential solutions to the problem of medication access. Concerted efforts should be made to ensure that future survival benefits are promising. It is difficult yet necessary to establish healthcare priorities and a clear plan for budget distribution.
Figures
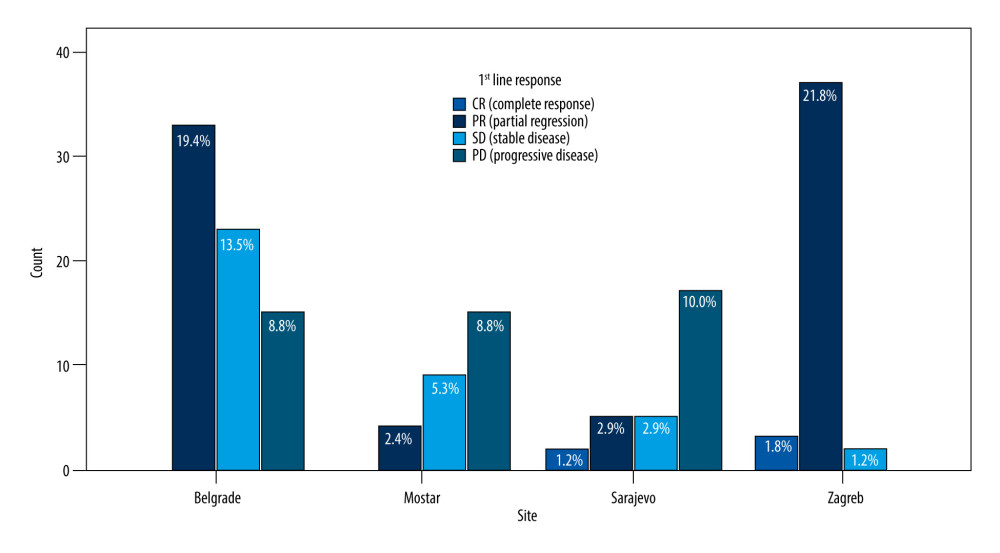 Figure 1. Responses to first-line therapy in patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.
Figure 1. Responses to first-line therapy in patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries. 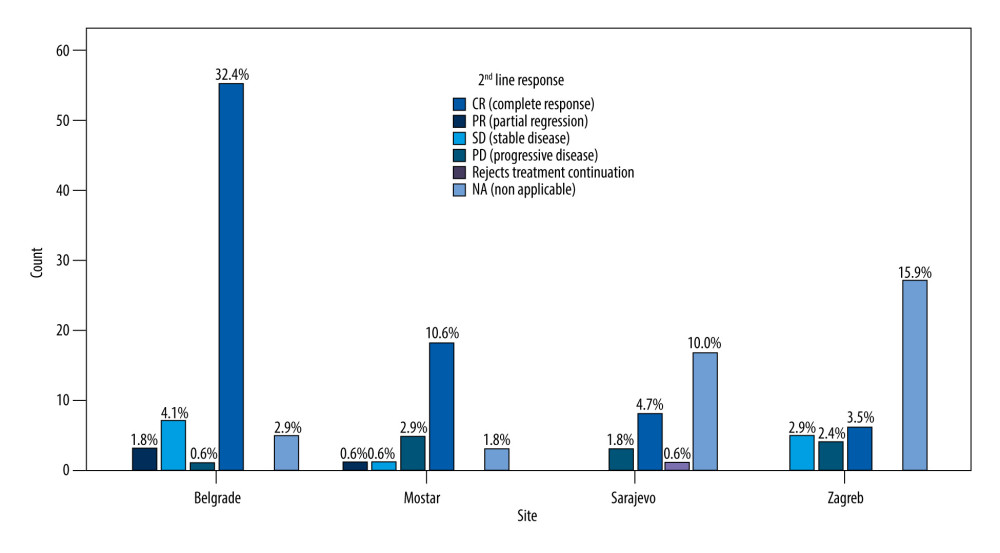 Figure 2. Responses to second-line therapy in patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.
Figure 2. Responses to second-line therapy in patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries. 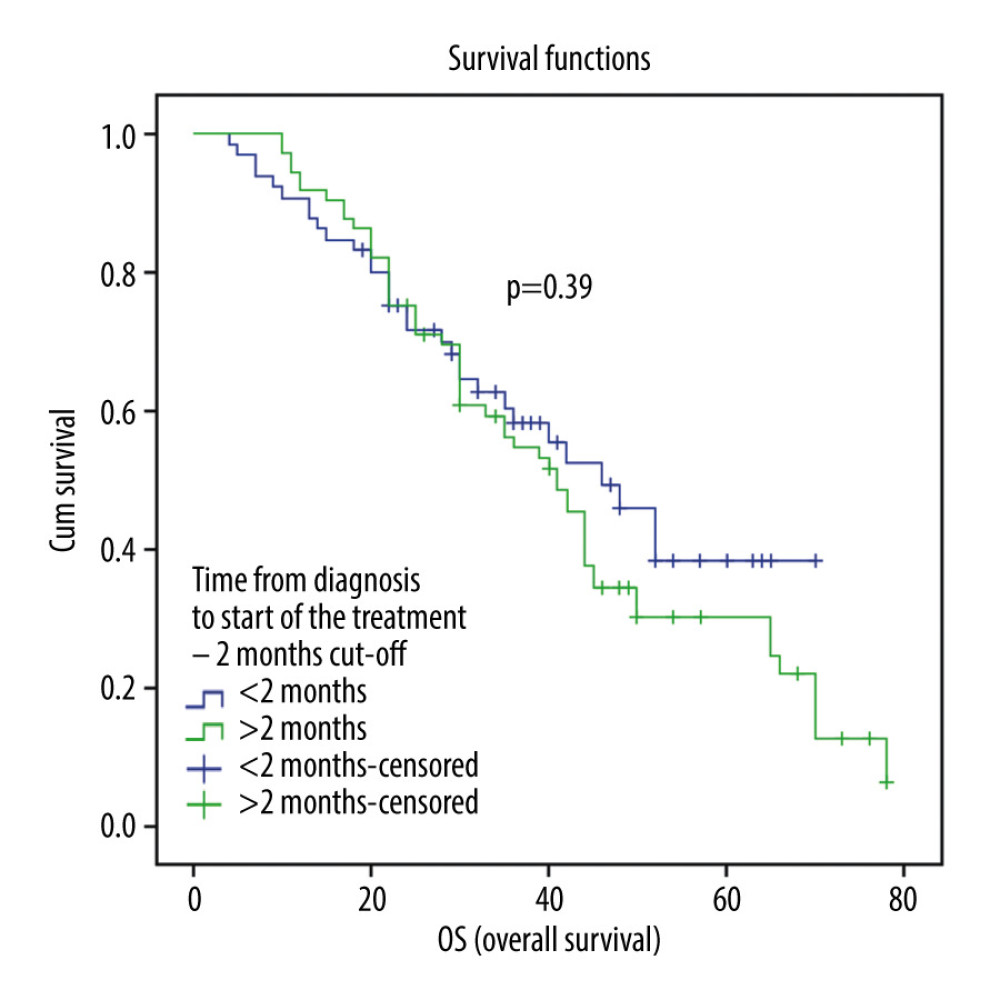 Figure 3. Overall survival (OS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to time from diagnosis to start of the treatment, with 2-month cutoff.
Figure 3. Overall survival (OS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to time from diagnosis to start of the treatment, with 2-month cutoff. 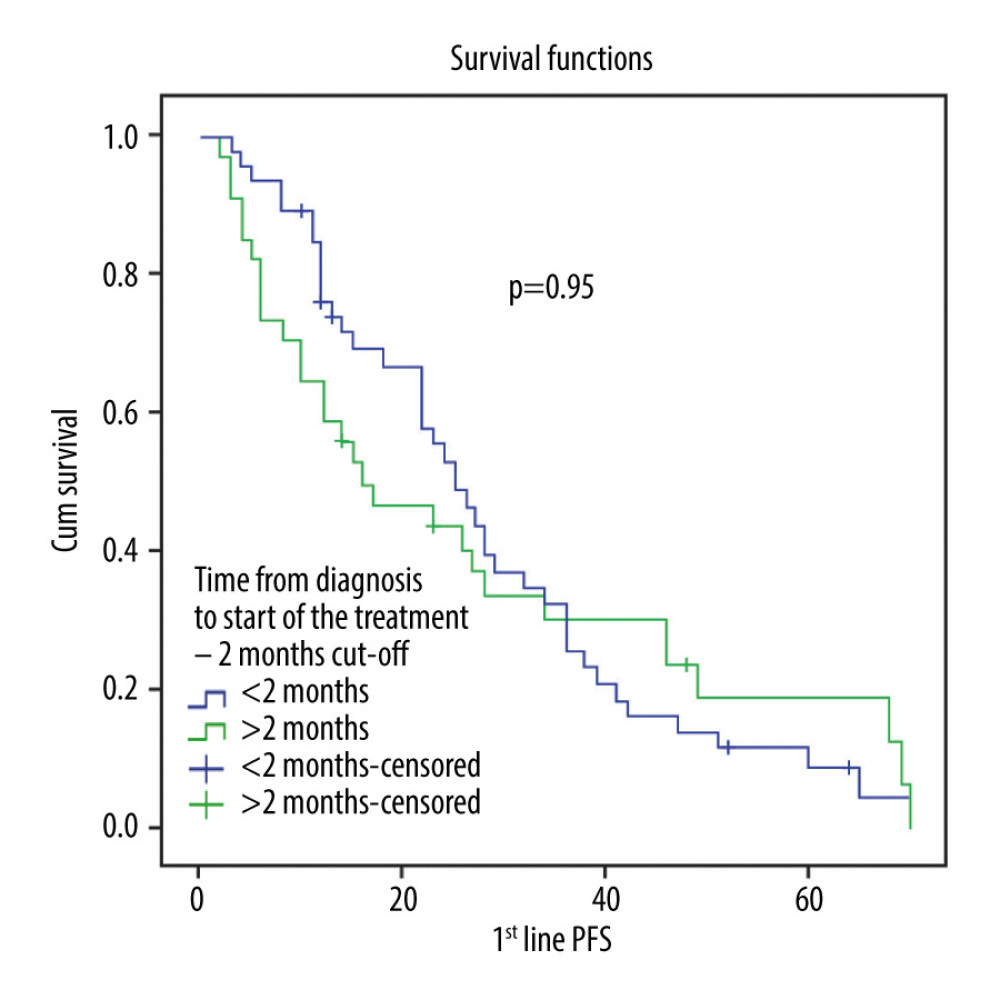 Figure 4. First-line progression free survival (PFS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to time from diagnosis to start of the treatment, with 2-month cutoff.
Figure 4. First-line progression free survival (PFS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to time from diagnosis to start of the treatment, with 2-month cutoff. 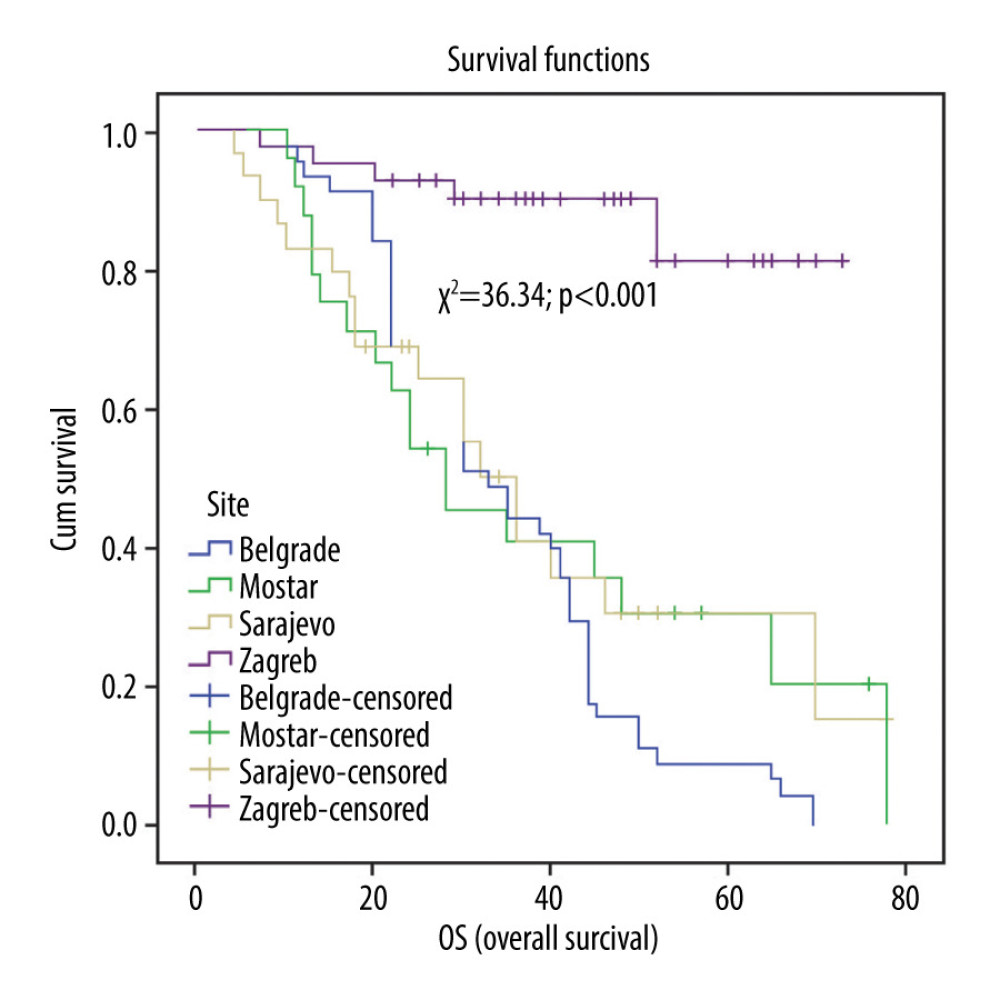 Figure 5. Overall survival (OS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to the different oncology clinics.
Figure 5. Overall survival (OS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to the different oncology clinics. 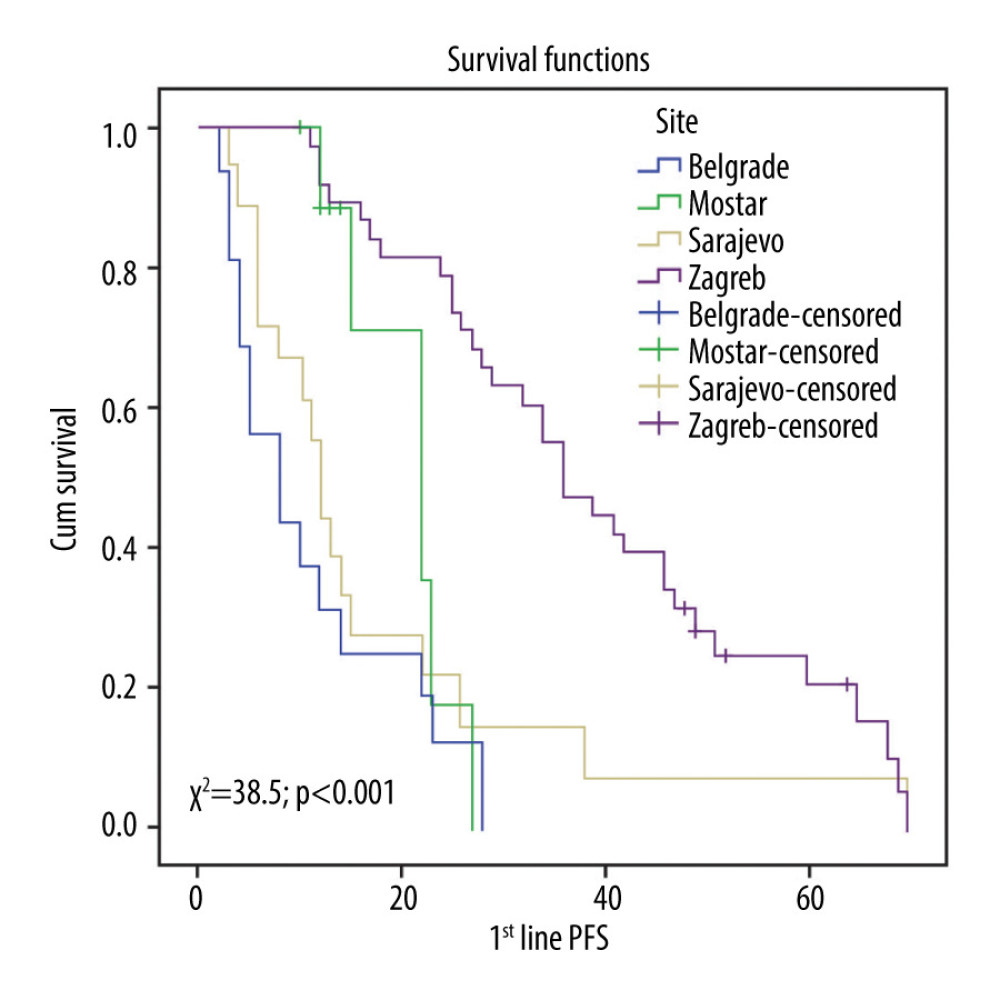 Figure 6. First-line progression-free survival (PFS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to the different oncology clinics.
Figure 6. First-line progression-free survival (PFS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to the different oncology clinics. 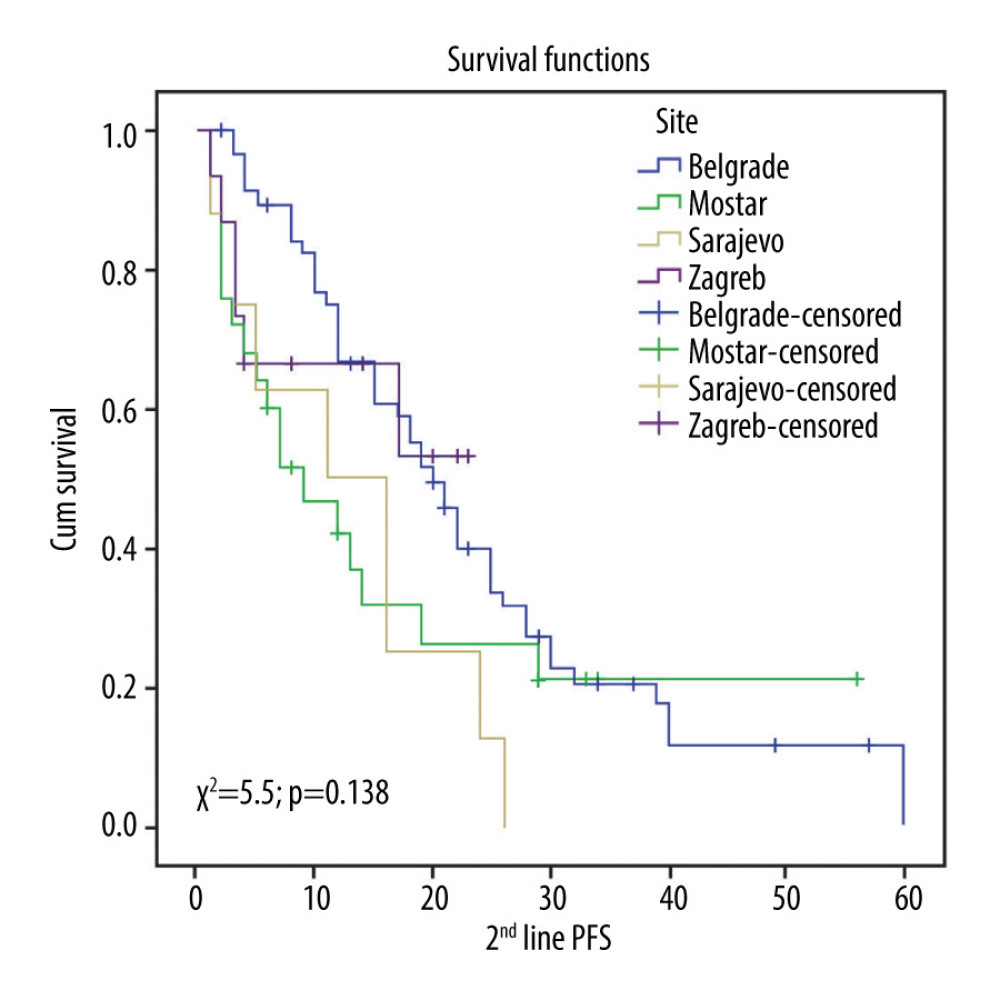 Figure 7. Second-line progression-free survival (PFS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to the different oncology clinics.
Figure 7. Second-line progression-free survival (PFS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to the different oncology clinics. 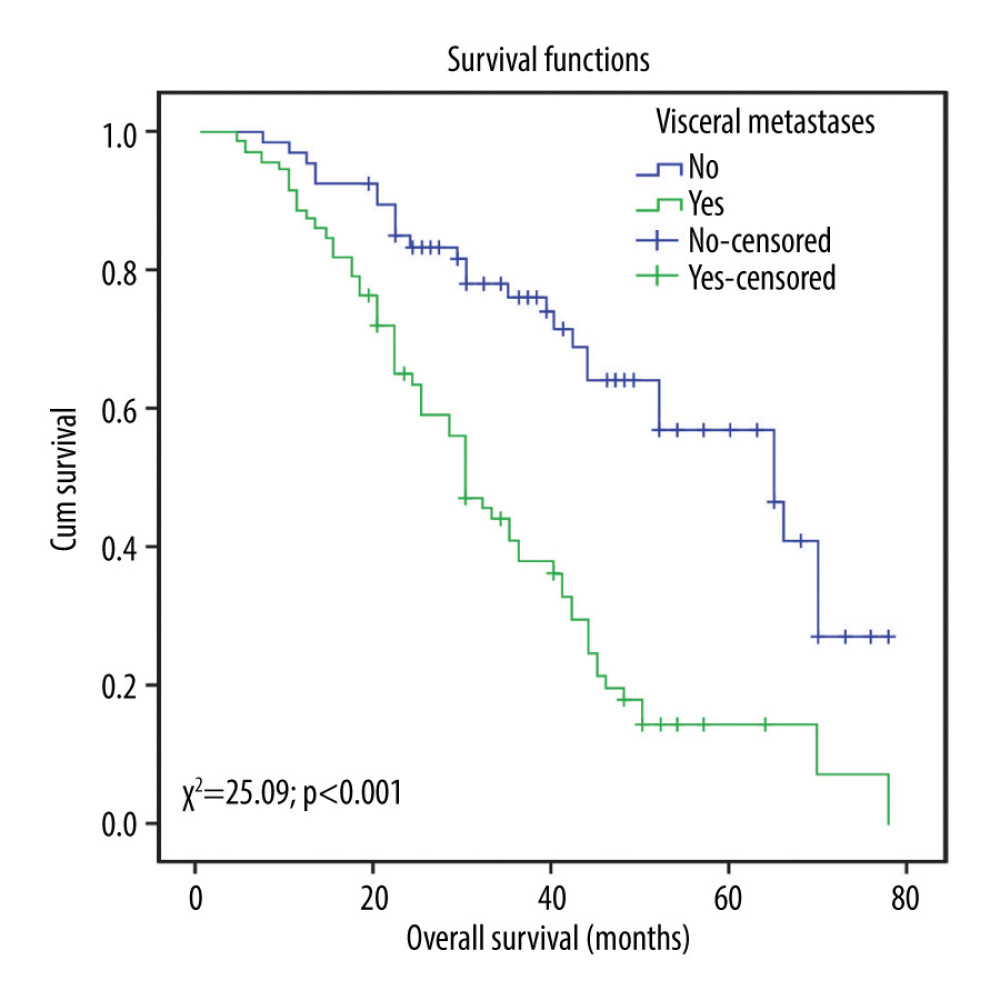 Figure 8. Overall survival (OS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to the presence of visceral metastases.
Figure 8. Overall survival (OS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to the presence of visceral metastases. 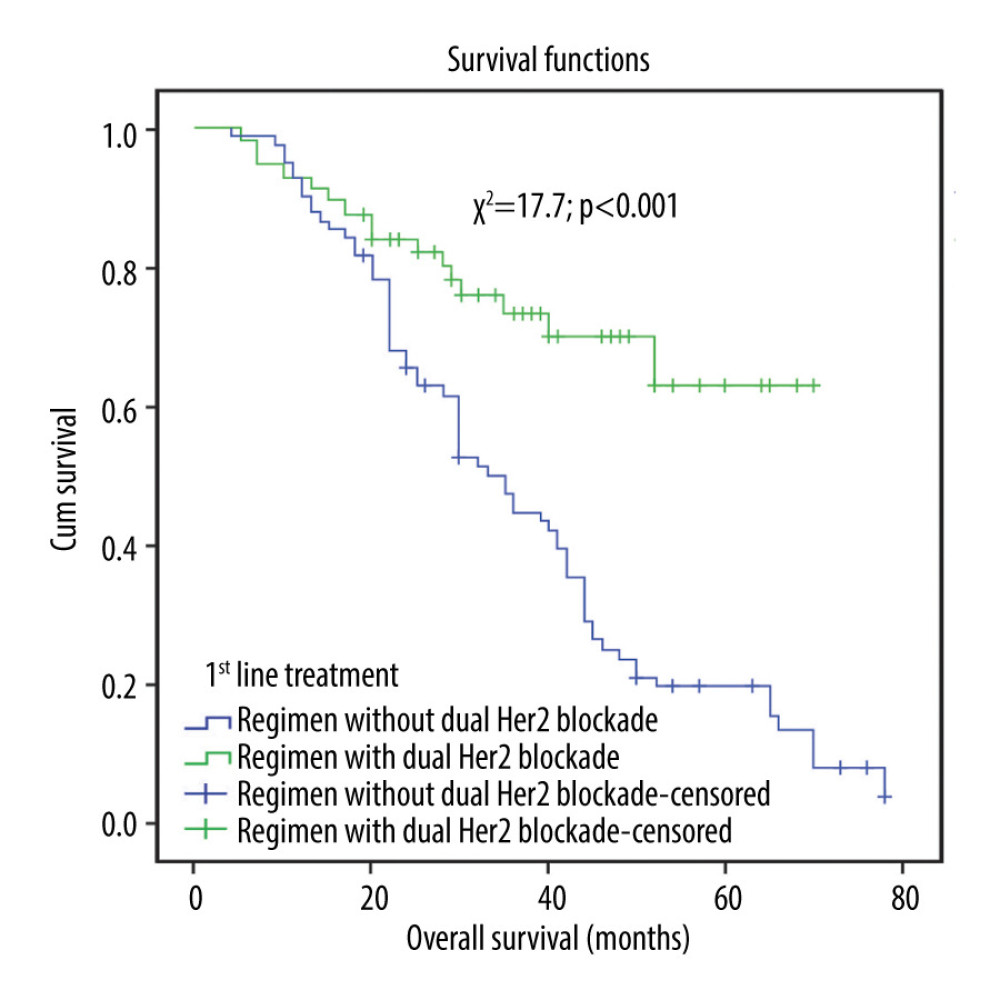 Figure 9. Overall survival (OS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to first-line treatment (regimen without dual HER2 blockade vs regimen with dual HER2 blockade).
Figure 9. Overall survival (OS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to first-line treatment (regimen without dual HER2 blockade vs regimen with dual HER2 blockade). 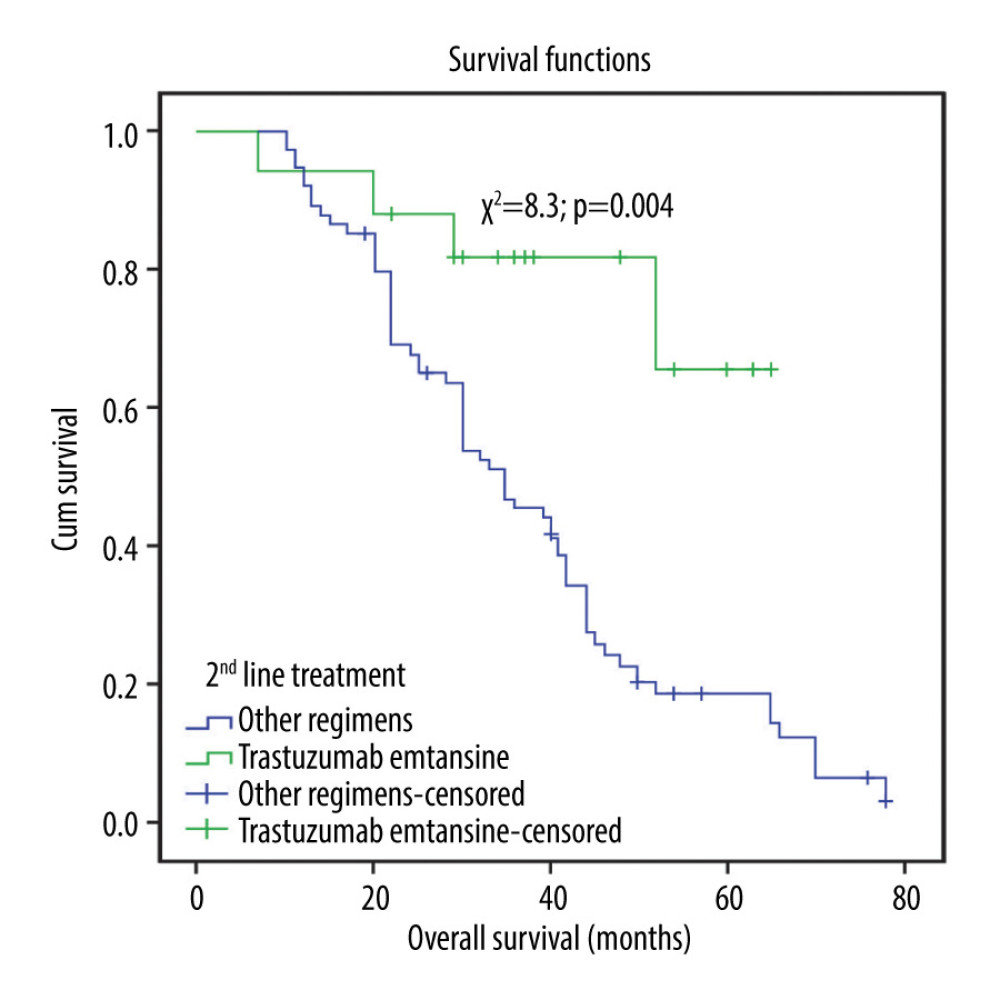 Figure 10. Overall survival (OS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to second-line treatment (regimen with trastuzumab emtansine vs other regimens).
Figure 10. Overall survival (OS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to second-line treatment (regimen with trastuzumab emtansine vs other regimens). Tables
Table 1. Baseline characteristics of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.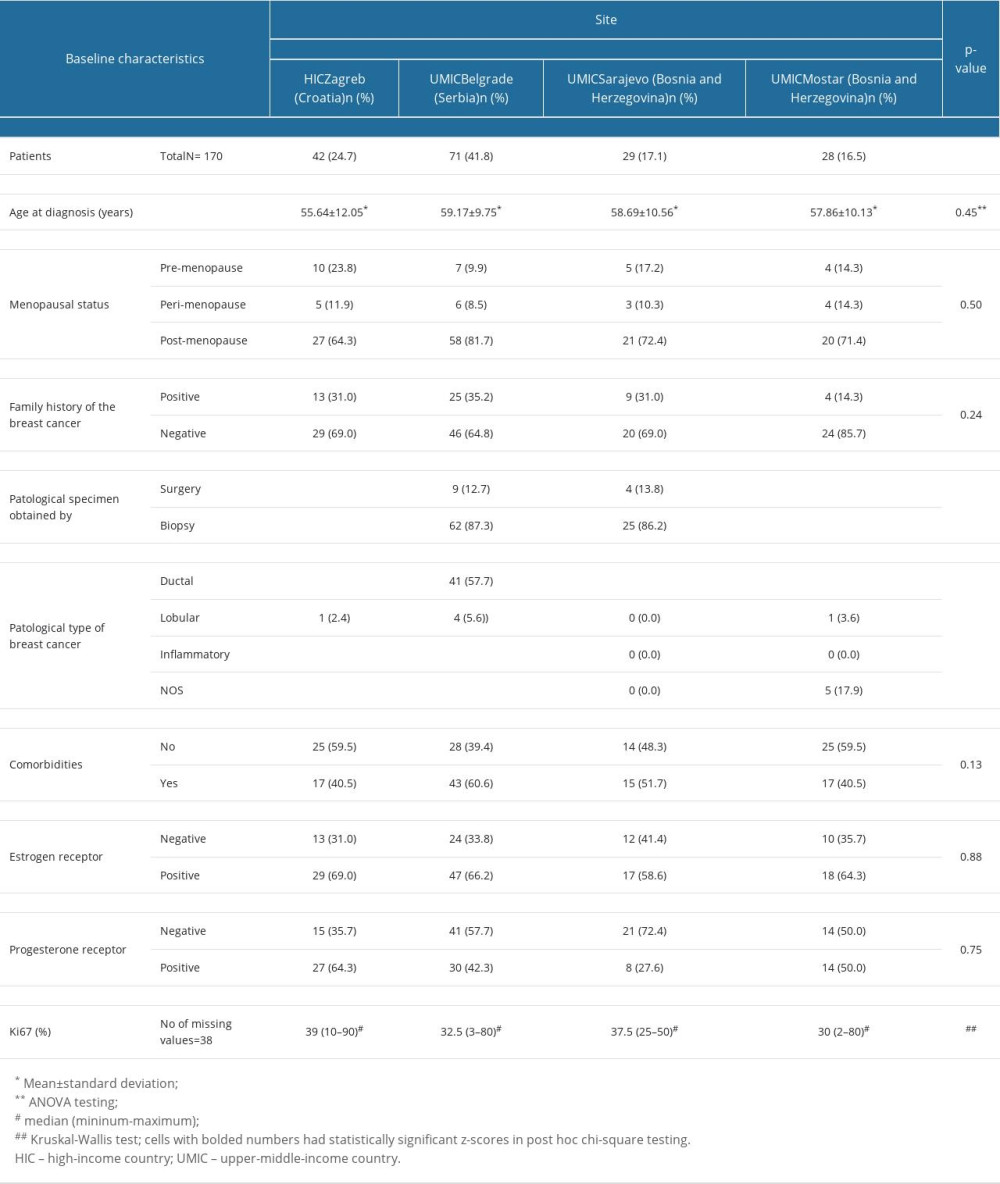 Table 2. Location of metastases and number of metastatic sites, and ECOG performance status of the patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.
Table 2. Location of metastases and number of metastatic sites, and ECOG performance status of the patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.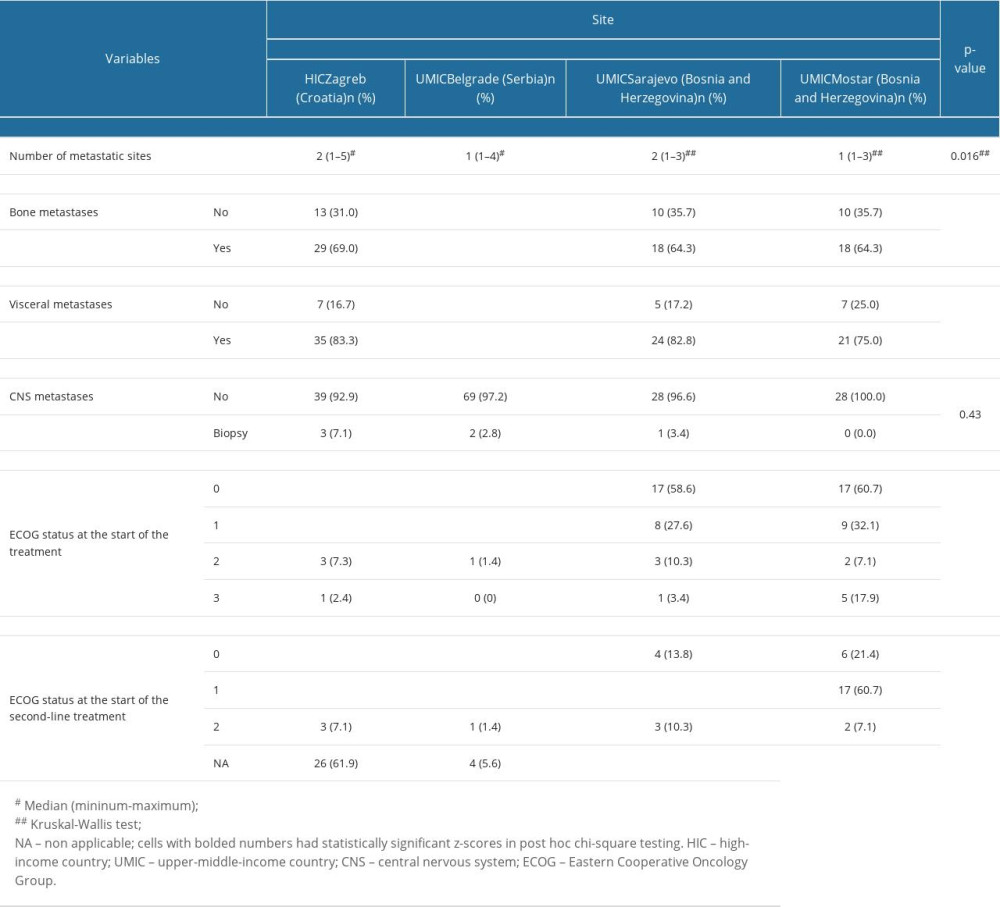 Table 3. First-line treatment of the patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.
Table 3. First-line treatment of the patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.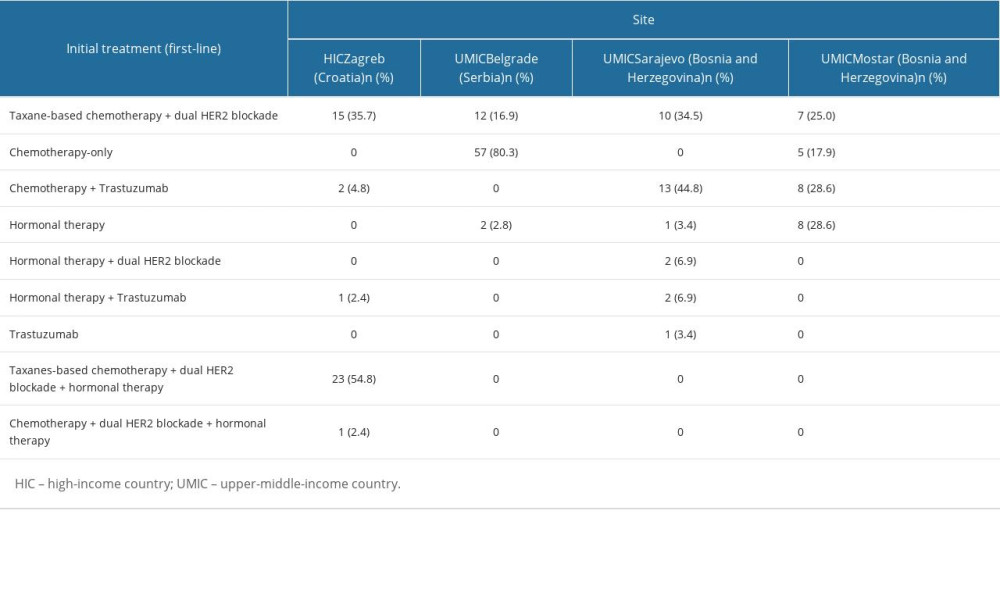 Table 4. Second-line treatment of the patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.
Table 4. Second-line treatment of the patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.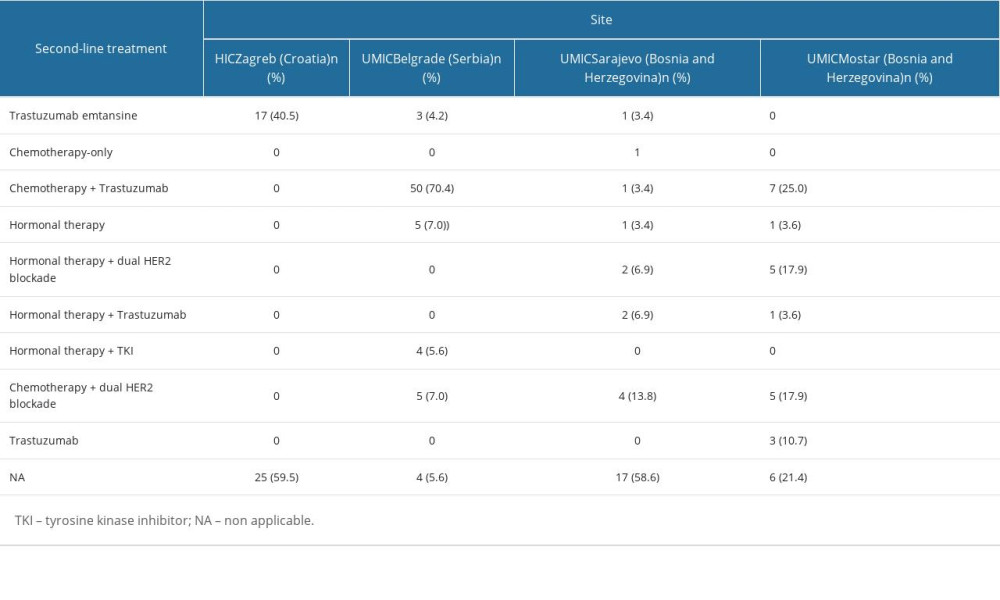 Table 5. Univariate Cox regression hazard analysis of the overall survival (OS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.
Table 5. Univariate Cox regression hazard analysis of the overall survival (OS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.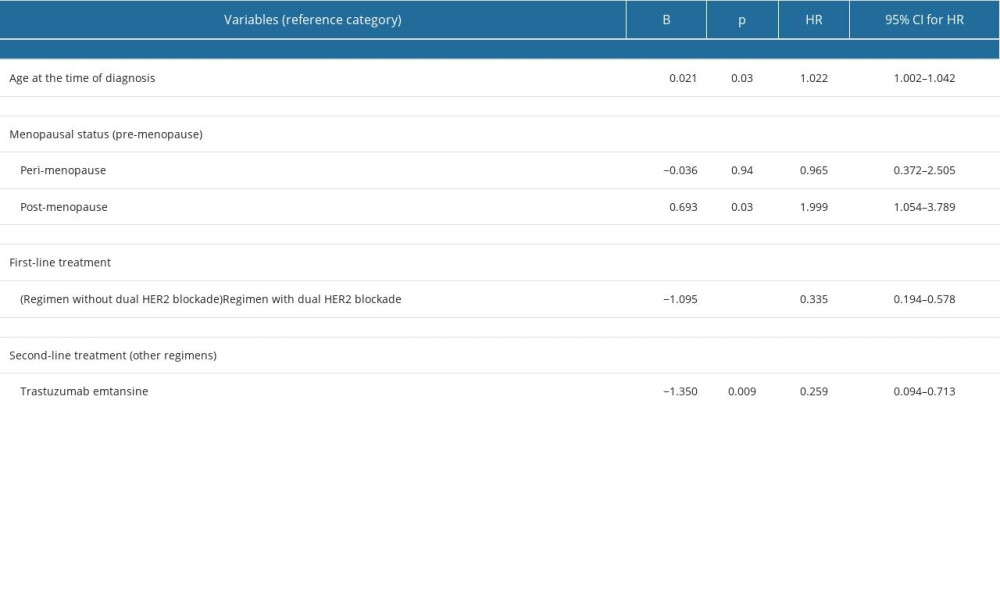
References
1. Erfani P, Bhangdia K, Mugunga JC, Cost of breast cancer care in low- and middle-income countries: A scoping review protocol: JBI Evid Synth, 2021; 19(10); 2813-28
2. Sung H, Ferlay J, Siegel RL, Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries: Cancer J Clin, 2021; 71(3); 209-49
3. Dyba T, Randi G, Bray F, The European cancer burden in 2020: Incidence and mortality estimates for 40 countries and 25 major cancers: Eur J Cancer, 2021; 157; 308-47
4. Exman P, Tolaney SM, HER2-positive metastatic breast cancer: A comprehensive review: Clin Adv Hematol Oncol, 2021; 19(1); 40-50
5. Carlson RW, Moench SJ, Hammond ME, HER2 testing in breast cancer: NCCN Task Force report and recommendations: J Natl Compr Canc Netw, 2006; 4(Suppl 3); S1-S24
6. Simmons C, Rayson D, Joy AA, Current and future landscape of targeted therapy in HER2-positive advanced breast cancer: Redrawing the lines: Ther Adv Med Oncol, 2022; 14; 17588359211066677
7. Bešlija S, Gojković Z, Cerić T, 2020 consensus guideline for optimal approach to the diagnosis and treatment of HER2-positive breast cancer in Bosnia and Herzegovina: Bosn J Basic Med Sci, 2021; 21(2); 120-35
8. Martínez-Sáez O, Prat A, Current and future management of HER2-positive metastatic breast cancer: JCO Oncol Pract, 2021; 17(10); 594-604
9. Slamon DJ, Leyland-Jones B, Shak S, Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2: N Engl J Med, 2001; 344(11); 783-92
10. Cameron D, Casey M, Oliva C, Lapatinib plus capecitabine in women with HER-2-positive advanced breast cancer: final survival analysis of a phase III randomized trial: Oncologist, 2010; 15(9); 924-34
11. Verma S, Miles D, Gianni LEMILIA Study Group, Trastuzumab emtansine for HER2-positive advanced breast cancer: N Engl J Med, 2012; 367(19); 1783-91
12. Barroso-Sousa R, Tolaney SM, Clinical development of new antibody–drug conjugates in breast cancer: To infinity and beyond: Biodrugs, 2021; 35; 159-74
13. Caswell-Jin JL, Callahan A, Purington N, Treatment and monitoring variability in US metastatic breast cancer care: JCO Clin Cancer Inform, 2021; 5; 600-14
14. Soares LR, Rosa VDL, Freitas-Junior R, Anti-HER2 therapy for metastatic breast cancer in low- and middle-income countries: Bridging the gap between clinical trials and real life: Breast Cancer Res Treat, 2020; 181(3); 693-94
15. The World bank: World Bank Blogs Available from: https://blogs.worldbank.org/
16. Kurtovic-Kozaric A, Vranic S, Kurtovic S, Lack of access to targeted cancer treatment modalities in the developing world in the era of precision medicine: Real-life lessons from Bosnia: J Glob Oncol, 2018; 4; 1-5
17. National Health Insurance Administration Available from: http://www.eng.rfzo.rs/
18. Croatian Health Insurance Fund Available from: https://hzzo.hr/en
19. Blackwell K, Gligorov J, Jacobs I, Twelves C, The global need for a trastuzumab biosimilar for patients with HER2-positive breast cancer: Clin Breast Cancer, 2018; 18; 95-113
20. Gong IY, Yan AT, Earle CC, Comparison of outcomes in a population-based cohort of metastatic breast cancer patients receiving anti-HER2 therapy with clinical trial outcomes: Breast Cancer Res Treat, 2020; 181(1); 155-65
21. Debiasi M, Reinert T, Kaliks R, Estimation of premature deaths from lack of access to anti-HER2 therapy for advanced breast cancer in the Brazilian Public Health System: J Glob Oncol, 2016; 3(3); 201-7
22. Wolff AC, Hammond EH, Hicks DG, Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Update: J Clin Oncol, 2013; 21; 3997-4013
23. Wolff AC, Hammond MEH, Schwartz JN, ASCO/CAP HER2 testing in breast cancer update: Arch Pathol Lab Med, 2018; 142; 1370-74
24. Slamon D, Leyland-Jones B, Shak S, Addition of Herceptin (humanized anti HER-2antibody) to first line chemotherapy for HER2 overexpressing metastatic breast cancer markedly increases anticancer activity: A randomized, multi national controlled Phase III trial: Proc Am Soc Clin Oncol, 1998; 17; 377
25. Cobleigh MA, Vogel CL, Tripathy D, Efficacy and safety of Herceptin (humanized anti-HER2 antibody) as a single agent in 222 women with HER2 overexpression who relapsed following chemotherapy for metastatic breast cancer: Proc Am Soc Clin Oncol, 1998; 17; 376
26. Swain SM, Baselga J, Kim SB, Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer: N Engl J Med, 2015; 372; 724-34
27. Verma S, Miles D, Gianni L, Trastuzumab emtansine for HER2-positive advanced breast cancer: N Engl J Med, 2012; 367; 1783-91
28. Krop IE, Kim SB, Martin AG, Trastuzumab emtansine versus treatment of physicia’s choice in patients with previously treated HER2-positive metastatic breast cancer (TH3RESA): Final overall survival results from a randomised open-label phase 3 trial: Lancet Oncol, 2017; 18(6); 743-54
29. Barrios CH, Reinert T, Werutsky G, Access to high-cost drugs for advanced breast cancer in Latin America, particularly trastuzumab: Ecancermedicalscience, 2019; 13; 898
30. Vega Cano KS, Marmolejo Castañeda DH, Escrivá-de-Romaní S, Saura C, Systemic therapy for HER2-positive metastatic breast cancer: Current and future trends: Cancers (Basel), 2022; 15(1); 51
31. Cortés J, Kim SB, Chung WP, Trastuzumab deruxtecan versus trastuzumab emtansine for breast cancer: N Engl J Med, 2022; 386; 1143-54
32. World Health Organization: Technical report: Pricing of cancer medicines and its impacts: A comprehensive technical report for the world health assembly resolution 70.12: Operative Paragraph 2,9 on Pricing approaches and their impacts on availability and affordability of medicines, 2018, Geneva, World Health Organization
33. Gallagher CM, More K, Kamath T, Delay in initiation of adjuvant trastuzumab therapy leads to decreased overall survival and relapse-free survival in patients with HER2-positive non-metastatic breast cancer: Breast Cancer Res Treat, 2016; 157(1); 145-56
34. DeMichele A, Cristofanilli M, Brufsky A, Comparative effectiveness of first-line palbociclib plus letrozole versus letrozole alone for HR+/HER2− metastatic breast cancer in US real-world clinical practice: Breast Cancer Res, 2021; 23(1); 37
35. Li J, Wang S, Wang Y, Disparities of trastuzumab use in resource-limited or resource-abundant regions and its survival benefit on HER2 positive breast cancer: A real-world study from China: Oncologist, 2017; 22(11); 1333-38
36. Chavarri-Guerra Y, St Louis J, Bukowski A, Real world patterns of care in HER2-overexpressing breast cancer: Results of a survey of TEACH clinical trial investigators in 2011: Breast, 2017; 31; 197-201
37. Gyawali B, Parsad S, Feinberg BA, Nabhan C, Real-world evidence and randomized studies in the precision oncology era: The right balance: JCO Precis Oncol, 2017; 1; 1-5
38. Batra A, Kong S, Cheung WY, Eligibility of real-world patients with metastatic breast cancer for clinical trials: Breast, 2020; 54; 171-78
39. Karim S, Xu Y, Kong S, Generalisability of common oncology clinical trial eligibility criteria in the real world: Clin Oncol (R Coll Radiol), 2019; 31(9); e160-e66
Figures
Figure 1. Responses to first-line therapy in patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.Figure 2. Responses to second-line therapy in patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.Figure 3. Overall survival (OS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to time from diagnosis to start of the treatment, with 2-month cutoff.Figure 4. First-line progression free survival (PFS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to time from diagnosis to start of the treatment, with 2-month cutoff.Figure 5. Overall survival (OS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to the different oncology clinics.Figure 6. First-line progression-free survival (PFS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to the different oncology clinics.Figure 7. Second-line progression-free survival (PFS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to the different oncology clinics.Figure 8. Overall survival (OS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to the presence of visceral metastases.Figure 9. Overall survival (OS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to first-line treatment (regimen without dual HER2 blockade vs regimen with dual HER2 blockade).Figure 10. Overall survival (OS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries according to second-line treatment (regimen with trastuzumab emtansine vs other regimens). Tables
Table 1. Baseline characteristics of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.Table 2. Location of metastases and number of metastatic sites, and ECOG performance status of the patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.Table 3. First-line treatment of the patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.Table 4. Second-line treatment of the patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.Table 5. Univariate Cox regression hazard analysis of the overall survival (OS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.Table 1. Baseline characteristics of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.Table 2. Location of metastases and number of metastatic sites, and ECOG performance status of the patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.Table 3. First-line treatment of the patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.Table 4. Second-line treatment of the patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries.Table 5. Univariate Cox regression hazard analysis of the overall survival (OS) of patients with metastatic HER2-positive breast cancer in 4 oncology centers in high-income and upper-middle-income countries. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387