26 November 2024: Clinical Research
Sarcopenia’s Role in Neoadjuvant Chemotherapy Outcomes for Locally Advanced Breast Cancer: A Retrospective Analysis
Mustafa Karaca1ACDEF, Mustafa Serkan Alemdar2BDF, Özge Deniz Karaca3ABEF, Yıldız Kılar4BD, Gökhan Köker3BEF, Hasan Sözel5CDE, Mustafa Yıldız2DEF, Gülhan Özçelik Köker1DEF, Mustafa Özgür Arici DOI: 10.12659/MSM.945240
Med Sci Monit 2024; 30:e945240






Abstract
BACKGROUND: Sarcopenia, characterized by loss of skeletal muscle mass and function, is linked to poor outcomes in cancer patients. In breast cancer, sarcopenia has been associated with reduced treatment tolerance and survival. However, its impact on patients with locally advanced breast cancer receiving neoadjuvant chemotherapy is understudied. This study aimed to assess sarcopenia’s impact on outcomes in 226 women with advanced breast cancer, pre- and post-chemotherapy.
MATERIAL AND METHODS: This retrospective cohort study included 226 patients with stage II-III breast cancer who received neoadjuvant chemotherapy (NAC) between 2015 and 2021. Sarcopenia was assessed using psoas muscle area (PMA) from pre- and post-NAC computed tomography scans, with a 25th percentile cut-off (415.4 mm²). Pathological response was evaluated using the Miller-Payne grading system, and survival outcomes were analyzed using Kaplan-Meier curves. Statistical significance was set at P<0.05.
RESULTS: The mean PMA decreased significantly after NAC (502.8 mm2 to 454.3 mm², P<0.001). Pre-NAC, sarcopenia was present in 24.8% of patients. This increased to 40.7% after NAC. Sarcopenia was more prevalent in obese patients (P<0.001), but no significant association was found between sarcopenia and pathological complete response (pCR) or survival outcomes. Although pre- and post-NAC sarcopenia did not affect recurrence or mortality, non-sarcopenic patients were more likely to achieve pCR (P=0.012). Hematologic toxicity was higher in sarcopenic patients with comorbidities (P<0.05).
CONCLUSIONS: Sarcopenia significantly increases after NAC but does not independently impact pathological response, recurrence, or survival in locally advanced breast cancer. Obesity and comorbid conditions are key factors influencing sarcopenia, highlighting the need for comprehensive management to mitigate treatment-related sarcopenia.
Keywords: Breast Neoplasms, Neoadjuvant Therapy, sarcopenia, Humans, Female, Retrospective Studies, Middle Aged, Aged, adult, Treatment Outcome, Kaplan-Meier Estimate, Psoas Muscles, Chemotherapy, Adjuvant, Neoplasm Staging
Introduction
Breast cancer continues to be the most common type of malignancy among women, accounting for 15% of cancer deaths [1,2]. The enhanced focus on early diagnosis and the development of more efficacious therapies has led to a reduction in the mortality associated with breast cancer, but quality of life can be adversely affected [3]. Over time, quality of life has become an important outcome measure in clinical research and survival studies for breast cancer, due to advancements in diagnosis and treatment of the disease [4].
Sarcopenia, originally defined by Rosenberg in 1989 as “muscle loss”, involves a reduction in skeletal muscle mass [5]. Since this primitive initial definition, sarcopenia has evolved beyond mere muscle loss. Today, sarcopenia is recognized as a geriatric syndrome characterized by muscle insufficiency; it presents as decreased muscle mass, function, and performance [6]. The European Working Group on Sarcopenia in Older People 2 (EWGSOP2) defines sarcopenia as a “progressive and generalized skeletal muscle disorder associated with increased likelihood of adverse outcomes including falls, fractures, physical disability, and death” [5,7]. Decreased muscle strength, low muscle quality, and reduced physical performance are accepted diagnostic criteria by EWGSOP2, and sarcopenia is considered severe when all 3 criteria are met [7].
While sarcopenia plays a significant role in the progression of chronic illness, symptoms like physical inactivity and loss of appetite can in turn exacerbate sarcopenia [8]. Patients with sarcopenia have lower tolerance to cancer treatments; they are more susceptible to complications such as infections, chemotherapy toxicity, and perioperative problems, all of which complicate cancer treatment [7,9]. There are 4 main reasons for sarcopenia during chemotherapy: (I) reduced intake of vitamin D, omega-3 fatty acids, and protein due to impaired food intake; (II) decreased physical activity due to fatigue; (III) the direct effect of chemotherapy or targeted agents on muscle; (IV) malabsorption due to mucositis or treatment-related pancreatic insufficiency [10].
Some studies have shown that pre-treatment sarcopenia predicts chemotherapy toxicity, reduced treatment response, increased disability, poor anti-tumor response, and lower survival rates [11]. Sarcopenia is linked to increased dose-limiting toxicities in patients undergoing chemotherapy for breast cancer [12]. Early-stage breast cancer patients on adjuvant chemotherapy have a high risk of sarcopenia [13]. The relationship between breast cancer and sarcopenia has been studied in early-stage and metastatic breast cancer [14]; however, it has not been sufficiently investigated in locally advanced breast cancer patients receiving neoadjuvant therapy. The limited data in the literature are based on studies with relatively small sample sizes [15,16]. Therefore, the present retrospective study, which included 226 women with locally advanced breast cancer, aimed to evaluate the association between sarcopenia, measured by right and left psoas muscle area (PMA), and outcomes before and after neoadjuvant chemotherapy (NAC).
Material and Methods
ETHICAL STATEMENT:
This retrospective cohort study was conducted according to the standards of the Helsinki Declaration and approval was obtained from the Health Sciences University Antalya Training and Research Hospital’s clinical research ethics committee on 29.09.2022, with decision number 18/15.
STUDY DESIGN:
This retrospective cohort study included patients diagnosed with invasive breast cancer who received NAC at the Health Sciences University Antalya Training and Research Hospital between 2015 and 2021.
PATIENT SELECTION:
Patients with histologically confirmed stage II or III breast cancer, who underwent surgery after NAC and had complete follow-up data, were included. Early-stage or metastatic breast cancer cases and those with incomplete data were excluded. Demographic, clinicopathologic, and laboratory data were collected from archival files and the hospital database. Postoperative pathology reports were reviewed to document the pathologic response to NAC.
MEASUREMENTS:
For sarcopenia assessment, PMA measurements were obtained from routine computed tomography scans, as shown in Figure 1. The mean PMA was calculated by averaging the right and left psoas areas, and the 25th percentile (415.4 mm2) was used as the cut-off for sarcopenia, in accordance with previous studies [17–19]]. Tumor subtypes were categorized into human epidermal growth factor 2 (HER2)-positive, triple-negative, luminal A, and luminal B, based on immunohistochemical markers. Body mass index (BMI) was used to classify patients as overweight (BMI 25–29.9) or obese (BMI ≥30). Neoadjuvant chemotherapy regimens were in accordance with international guidelines, with anthracycline-cyclophosphamide followed by paclitaxel or docetaxel as the most common, and trastuzumab/pertuzumab added for HER2-positive cases.
Pathological complete response (pCR) was defined as the absence of invasive cancer in the breast and lymph nodes (ypT0/Tis ypN0). Response was graded using the Miller-Payne (MP) system [20]. Disease-free survival (DFS) was calculated from surgery to relapse, metastasis, or death, while overall survival (OS) was measured from diagnosis to death from any cause.
STATISTICAL ANALYSIS:
In our study, patients’right and left PMA values were measured before and after NAC. The pre-chemotherapy right and left measurements were summed and divided by 2 to obtain the average PMA value. The 25th percentile of this value was found to be 415.4 mm2, which was taken as the cut-off point. Sarcopenia presence before and after NAC was assessed based on the average of the right and left values, with individuals falling below the cut-off considered sarcopenic, while others were classified as normal. Statistical analyses were performed using the SPSS 29.0 software package. A
Results
DEMOGRAPHIC AND CLINICAL CHARACTERISTICS:
The study included 226 female patients with a mean age of 50.0±11.5 years. Of these, 55.8% were postmenopausal, and 72.6% were either overweight or obese. A total of 32.7% of patients had at least one comorbid condition, with hypertension being the most common (22.1%), followed by diabetes (13.3%). Most patients were clinical stage II (58.8%) and had clinical N1 status (67.3%). Luminal B was the most prevalent subtype of breast cancer, with 64.6% being HER2 negative. The pathologic characteristics of the patients are summarized in Table 1.
NEOADJUVANT CHEMOTHERAPY RESPONSE:
The response to NAC revealed that 58.8% of patients did not achieve a pCR, and 41.1% were classified as MP-5 according to the MP grading system. During a median follow-up of 37.2 months, 8.8% of patients experienced disease recurrence, and 3.5% (8 patients) died (Table 2).
SARCOPENIA PREVALENCE:
The mean pre-NAC PMA was 502.8±118.0 mm2, decreasing to 454.3±115.1 mm2 post-NAC. Pre-NAC sarcopenia was present in 24.8% of patients, increasing to 40.7% after NAC. A total of 45 patients who were non-sarcopenic before NAC developed sarcopenia after undergoing NAC, while 9 patients with pre-NAC sarcopenia were no longer sarcopenic after receiving NAC. This increase in sarcopenic patients was statistically significant (P<0.001). The details are presented in Table 3.
ASSOCIATION WITH OBESITY:
Obesity was significantly associated with sarcopenia. Before NAC, 55.3% of non-sarcopenic patients were obese, and among the patients who were sarcopenic before receiving NAC, 100% were obese (
PATHOLOGICAL CHARACTERISTICS:
No significant correlation was found between pre-NAC sarcopenia and the patients’ pathological characteristics. However, estrogen receptor positivity was observed in 75.4% of patients without sarcopenia and 62% of sarcopenic patients (P=0.031). Similarly, progesterone receptor positivity was higher in non-sarcopenic patients (62.7%) compared with sarcopenic patients (47.8%) (P=0.027). No significant associations were found between post-NAC sarcopenia and other pathological characteristics (Table 4).
IMPACT ON TREATMENT RESPONSE:
Pre-NAC sarcopenia did not influence the pathological response to treatment. Furthermore, no correlation was identified between sarcopenia and recurrence or mortality. Post-NAC sarcopenia was not associated with pCR, pathologic response, recurrence, or mortality (Table 5). In comparisons between pre- and post-NAC sarcopenia, no significant differences were observed in terms of pCR, recurrence, or mortality. Among patients without pre-NAC sarcopenia, 58.4% did not achieve pCR, and all patients without post-NAC sarcopenia also had a non-pCR response (P=0.012) (Table 6).
There were no significant differences in hematologic adverse effects between sarcopenic and non-sarcopenic patients, but patients with at least one comorbid condition showed significant differences in hematologic adverse effects (Table 7).
SURVIVAL ANALYSIS:
Survival analyses showed no statistical differences in DFS or OS between pre- and post-NAC sarcopenic and non-sarcopenic patients. The mean DFS for patients with pre-NAC sarcopenia was 6.27 years (95% CI 5.4–6.9), compared with 7.2 years (95% CI 6.7–7.7) for patients who developed sarcopenia post-NAC (P=0.111). The mean OS was 6.9 years (95% CI 6.3–7.5) for patients with pre-NAC sarcopenia and 7.1 years (95% CI 6.3–7.9) for those with post-NAC sarcopenia (P=0.547) (Figures 2, 3).
Discussion
The present study aimed to evaluate the impact of sarcopenia on treatment outcomes, pathological response, and survival in patients with locally advanced breast cancer undergoing NAC. Our findings suggest that sarcopenia, particularly post-treatment sarcopenia, is significantly associated with obesity but does not directly affect pathological response, recurrence, or OS.
Sarcopenia is associated with increased chemotherapy toxicity, heightened post-surgical complications, and reduced survival rates in oncological treatment regimens [21]. Sarcopenia is common in patients with breast cancer [22] and is associated with increased chemotherapy toxicity [23,24], earlier tumor progression [25], and a rise in overall mortality [26]. Therefore, sarcopenia should be assessed before starting cancer treatment in all patients to optimize treatment efficacy and tolerance and minimize adverse effects. While there is growing interest in the effects of sarcopenia on breast cancer, current literature primarily focuses on survival analyses, with limited studies examining the relationship between NAC and sarcopenia, particularly its impact on treatment toxicity. Our study aims to illuminate an underexplored area by examining the effects of sarcopenia on treatment response, toxicity, and survival in breast cancer patients receiving NAC.
In line with the literature, significant differences were found between median pre-NAC PMA values and post-NAC PMA values. Our study did not find a statistical relationship between pre-NAC and post-NAC sarcopenia and pCR, which is the most important indicator of response to NAC. However, we found that sarcopenia was statistically significantly higher in patients with a BMI of 30 or above both before and after NAC, and this situation became more pronounced in the post-NAC period. Another finding was that DFS and OS were not affected by the sarcopenic state.
The mean age of the 226 patients studied in our research aligns with existing literature [27–29], though our postmenopausal patient ratio was higher than reported rates. Direct comparison with the literature was not feasible due to different cut-off values in BMI classification. Similar to other studies evaluating neoadjuvant treatment [15,27–29], the use of anthracycline- and taxane-based regimens was prominent in our study.
Consistent with previous studies [30,31], a significant difference was found between the median pre- and post-NAC PMA values in our study. The increased number of sarcopenic patients following NAC underscores the importance of proper nutritional support during chemotherapy. Moreover, an increased incidence of post-NAC sarcopenia has been observed in patients with a BMI over 30 in line with a study by Iwase et al [15]. Consistent with previous studies [27,32], no significant relationship was found between sarcopenia and breast cancer subtypes or clinical stages.
Achieving a pCR following NAC is known as a proven prognostic factor. The few studies in the literature investigating the relationship between body composition changes or sarcopenia and obtaining pCR following NAC have conflicting results. In older studies evaluating only BMI, a high BMI was inversely correlated with pCR [16,33], while a meta-analysis of 8 major studies found no association between obesity and NAC response [34]. Despite conflicting results in studies using skeletal muscle area or muscle index measurements instead of BMI [27–29], our study did not show a significant association between pCR and pre- and post-NAC sarcopenia.
In our subgroup analyses, none of the 9 patients who improved from pre-NAC sarcopenia to post-NAC non-sarcopenia achieved pCR, showing statistical significance when compared with 125 patients who were non-sarcopenic both before and after NAC. Of the 56 patients with pre-NAC sarcopenia, those who improved post-NAC (9 patients) were statistically less responsive to NAC compared with the remaining 47 with persistent sarcopenia. This suggests a lower tendency of patients with resolved sarcopenia post-NAC to achieve pCR, indicating the need for larger, prospective studies.
The relationship between sarcopenia and chemotherapy toxicity represents a significant research area in the management of side effect profiles of oncological treatments, with growing evidence on the effects of sarcopenia [35]. The potential modulatory effect of sarcopenia on chemotherapy-induced toxicity, particularly in the context of NAC, was a primary research question of the present study. In the relevant literature, Prado et al’s study on metastatic patients undergoing capecitabine treatment found that severe toxicity incidents were twice as common in patients diagnosed with sarcopenia vs those without sarcopenia [25]. In patients without sarcopenia, this rate was only 20%. Similarly, another study on breast cancer patients undergoing adjuvant therapy found that individuals with higher lean body mass experienced less toxicity from epirubicin [25], further clarifying the relationship between sarcopenia and treatment adverse effects. Although limited in number, current studies specific to neoadjuvant treatment indicate a relationship between alterations in body composition and increased toxicity risk [24,36]. Although the hematologic adverse effects in our study were not in line with the literature, the aforementioned studies used different body composition measurement methods as well as different cut-off values. More importantly, significantly higher rates of hematologic toxicity were found in patients with at least one comorbidity, both pre- and post-NAC, who were sarcopenic. This is a standout finding in the current literature evaluating the sarcopenia-chemotherapy toxicity relationship, and represents a notable distinction between the present study and previous studies. These data emphasize the need to better understand the role of sarcopenia in treatment planning and side effect management strategies, particularly in breast cancer patients receiving NAC. These findings also indicate the potential of incorporating individual body composition into oncological treatment protocols to reduce adverse effects and improve treatment adherence.
The final evaluation in our study focused on survival. Studies in the literature have reported that sarcopenia may be a prognostic factor for survival in various types of cancer [24,26,37]. However, one study also indicated that it may not be a negative prognostic factor in patients with muscle-invasive bladder cancer [38]. In the study by Iwase et al, which assessed patients with locally advanced breast cancer undergoing NAC, no relationship was found between BMI or body composition measurements and OS [15]. In their study involving patients receiving NAC, Omarini et al also found that BMI or body composition parameters did not significantly affect OS and DFS [29]. Consistent with these 2 studies, our study also did not find a statistically significant relationship between survival parameters and sarcopenia.
A limitation of our study is the lack of a control group, which could have provided a more robust comparison of sarcopenia’s impact in a broader population. Furthermore, while we used PMA as a surrogate for sarcopenia, a more comprehensive volumetric analysis could provide deeper insights into muscle mass changes. Nonetheless, the use of PMA is validated as a reliable method for assessing sarcopenia in oncology, particularly in resource-constrained settings where volumetric measurements may not be feasible.
Conclusions
In conclusion, the present study highlights the complex relationship between sarcopenia, obesity, and treatment outcomes in breast cancer patients undergoing NAC. While sarcopenia increases significantly following NAC, it does not appear to affect pathological response or survival outcomes. Future research should focus on understanding the interplay between sarcopenia, obesity, and other comorbid conditions to better predict which patients may benefit from targeted interventions aimed at preserving muscle mass during cancer treatment.
Figures
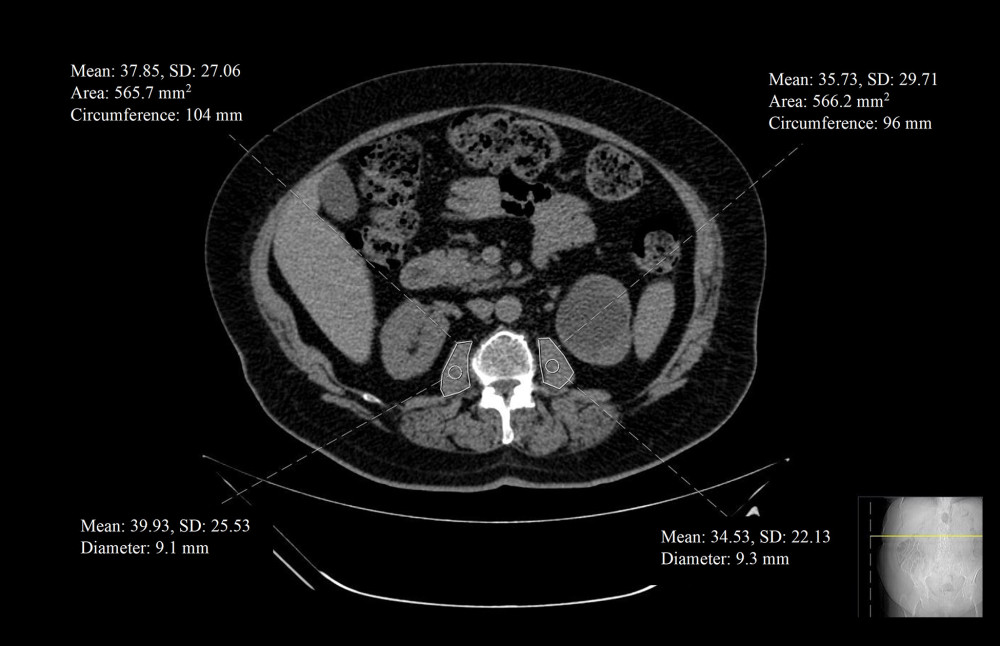 Figure 1. A single radiologist measured the cross-sectional transverse areas of the bilateral psoas muscles by manual tracing on the CT images at the middle level of the third lumbar vertebra using a software program (Sectra Workstation IDS7 Version: 25.2.15.7682 #2014 Sectra AB). The PMI, in mm2/m2 is calculated by normalizing the psoas muscle area for height in meters squared. CT – computed tomography; PMI – psoas muscle index.
Figure 1. A single radiologist measured the cross-sectional transverse areas of the bilateral psoas muscles by manual tracing on the CT images at the middle level of the third lumbar vertebra using a software program (Sectra Workstation IDS7 Version: 25.2.15.7682 #2014 Sectra AB). The PMI, in mm2/m2 is calculated by normalizing the psoas muscle area for height in meters squared. CT – computed tomography; PMI – psoas muscle index. 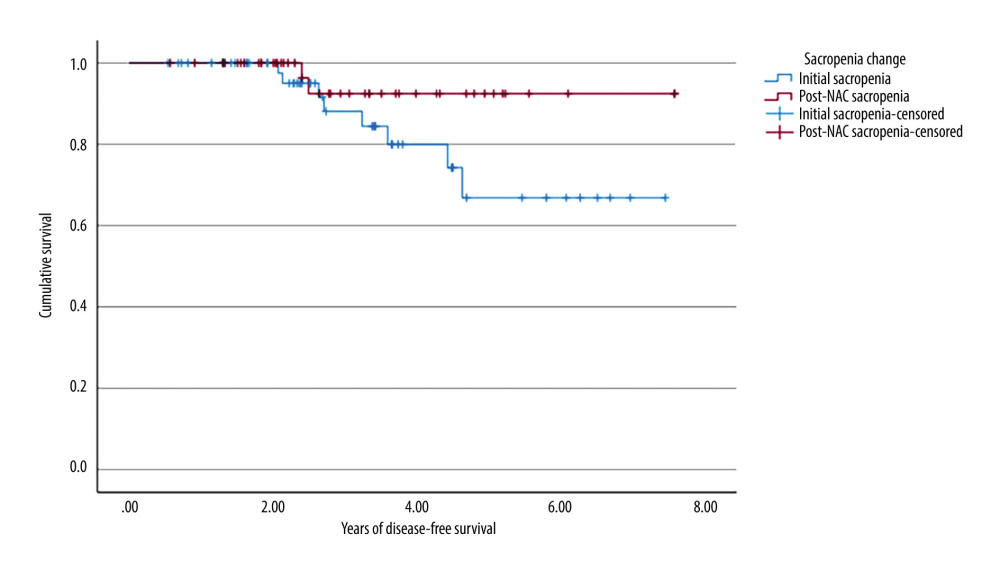 Figure 2. Kaplan-Meier survival curve for disease-free survival according to sarcopenia change status. No statistical difference was found between patients with pre-NAC sarcopenia and post-NAC sarcopenia. We used the SPSS 29.0 software package (IBM Corp., Armonk, NY) to draw this figure. NAC – neoadjuvant chemotherapy.
Figure 2. Kaplan-Meier survival curve for disease-free survival according to sarcopenia change status. No statistical difference was found between patients with pre-NAC sarcopenia and post-NAC sarcopenia. We used the SPSS 29.0 software package (IBM Corp., Armonk, NY) to draw this figure. NAC – neoadjuvant chemotherapy. 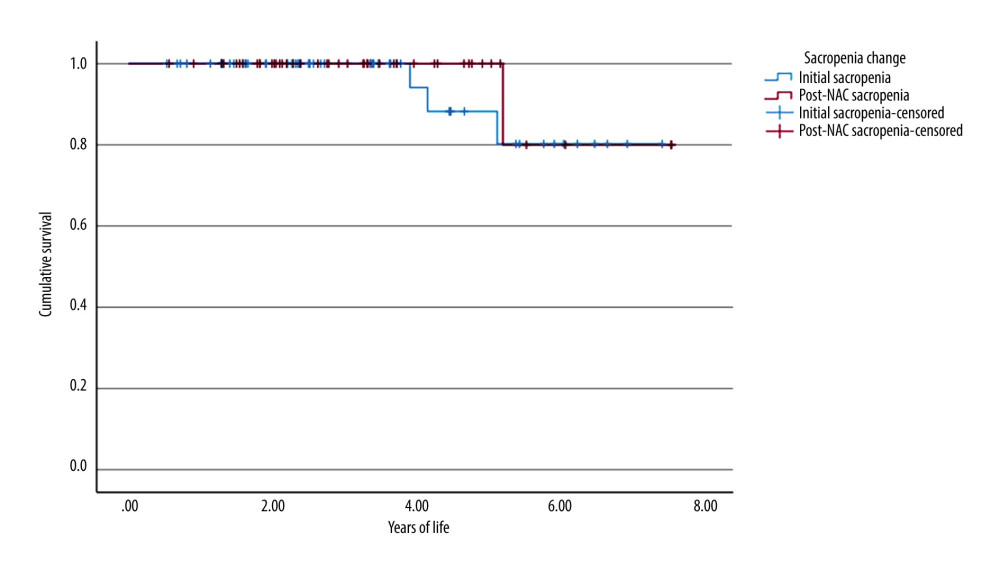 Figure 3. Kaplan-Meier survival curve for OS for disease-free survival according to sarcopenia change status. No statistical difference was found between patients with pre-NAC sarcopenia and post-NAC sarcopenia. We used the SPSS 29.0 software package (IBM Corp., Armonk, NY) to draw this figure. OS – overall survival; NAC – neoadjuvant chemotherapy.
Figure 3. Kaplan-Meier survival curve for OS for disease-free survival according to sarcopenia change status. No statistical difference was found between patients with pre-NAC sarcopenia and post-NAC sarcopenia. We used the SPSS 29.0 software package (IBM Corp., Armonk, NY) to draw this figure. OS – overall survival; NAC – neoadjuvant chemotherapy. Tables
Table 1. Pathologic characteristics of the patients. Table 2. Treatment response, recurrence/progression and final status of the patients.
Table 2. Treatment response, recurrence/progression and final status of the patients.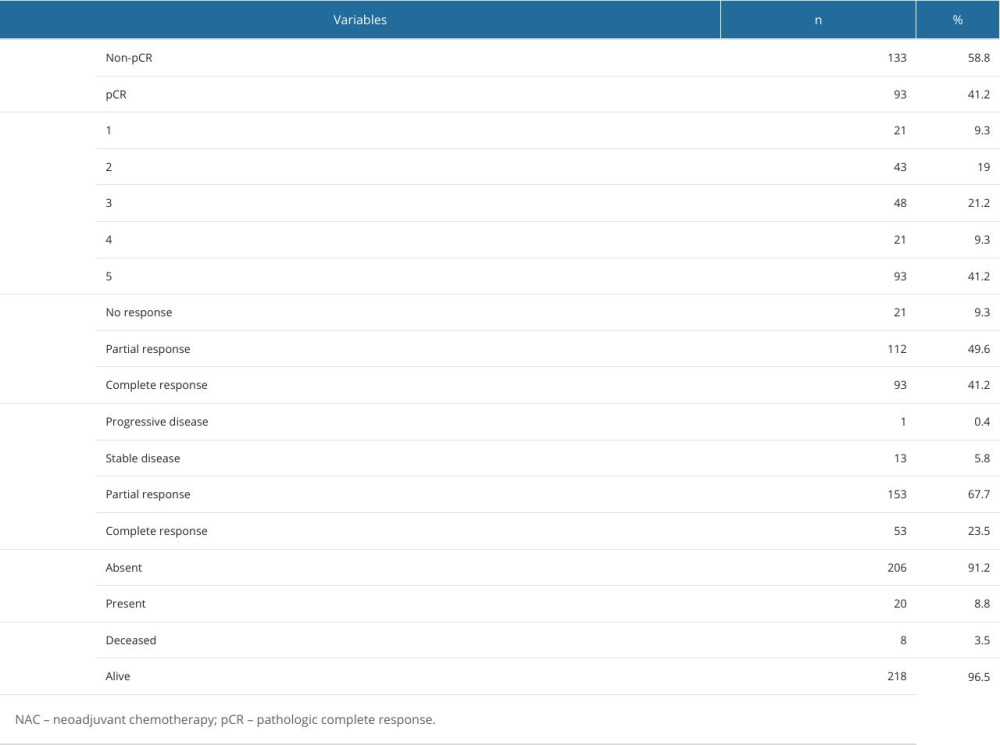 Table 3. Comparison of clinical characteristics by sarcopenia status.
Table 3. Comparison of clinical characteristics by sarcopenia status. Table 4. Comparison of treatment responses and recurrence by pre-treatment sarcopenia status.
Table 4. Comparison of treatment responses and recurrence by pre-treatment sarcopenia status.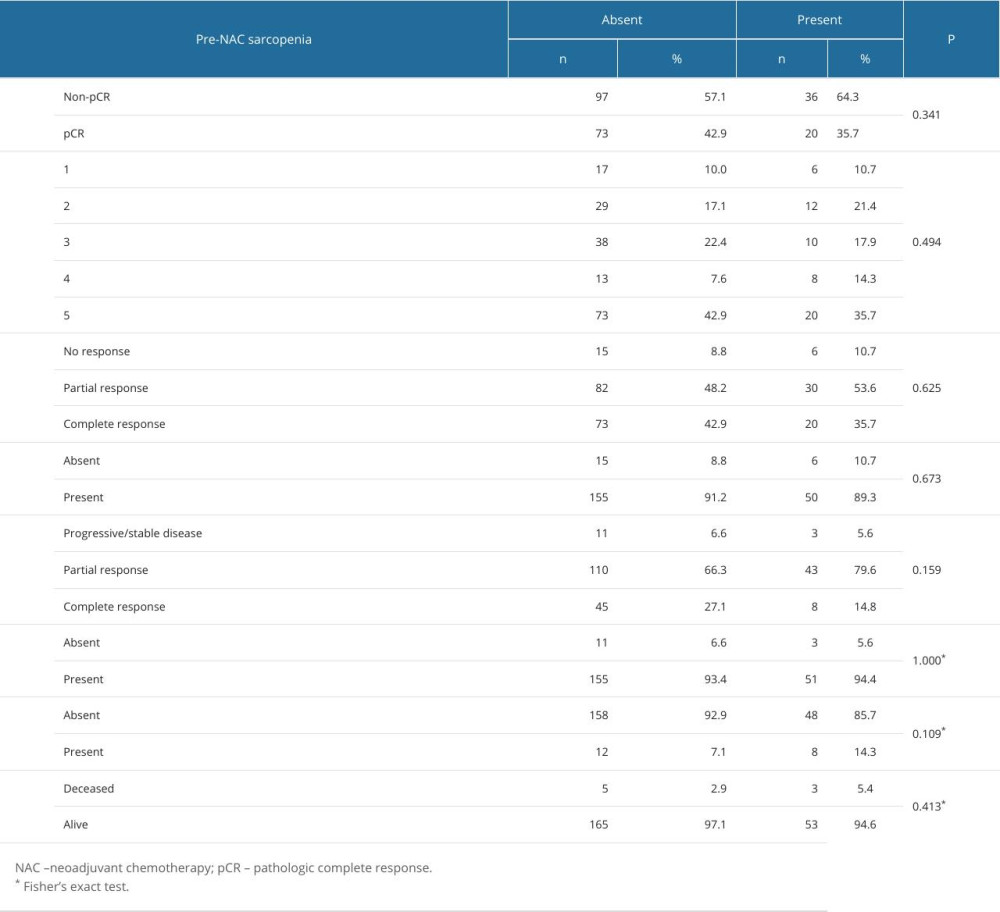 Table 5. Comparison of treatment responses and recurrence by post-treatment sarcopenia status.
Table 5. Comparison of treatment responses and recurrence by post-treatment sarcopenia status.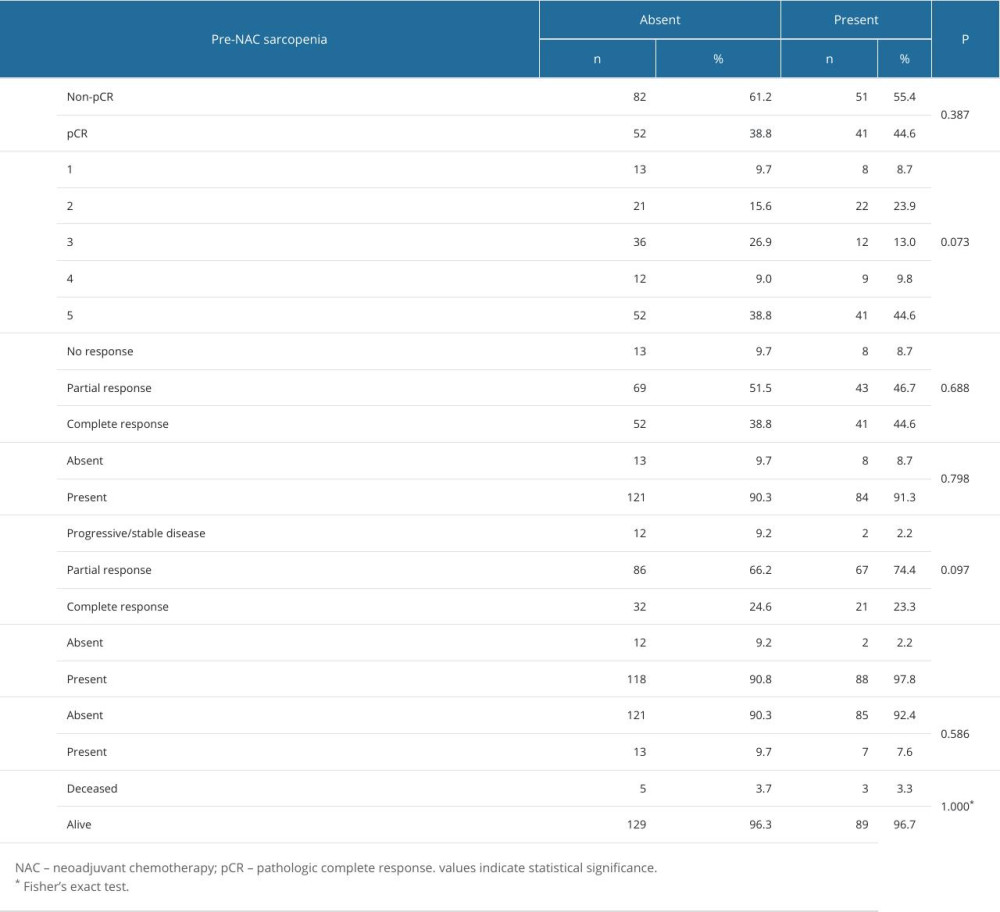 Table 6. Comparison of treatment responses in non-sarcopenic patients.
Table 6. Comparison of treatment responses in non-sarcopenic patients. Table 7. Comparison of adverse effects in patients with comorbidities based on pre- and post-treatment sarcopenia status.
Table 7. Comparison of adverse effects in patients with comorbidities based on pre- and post-treatment sarcopenia status.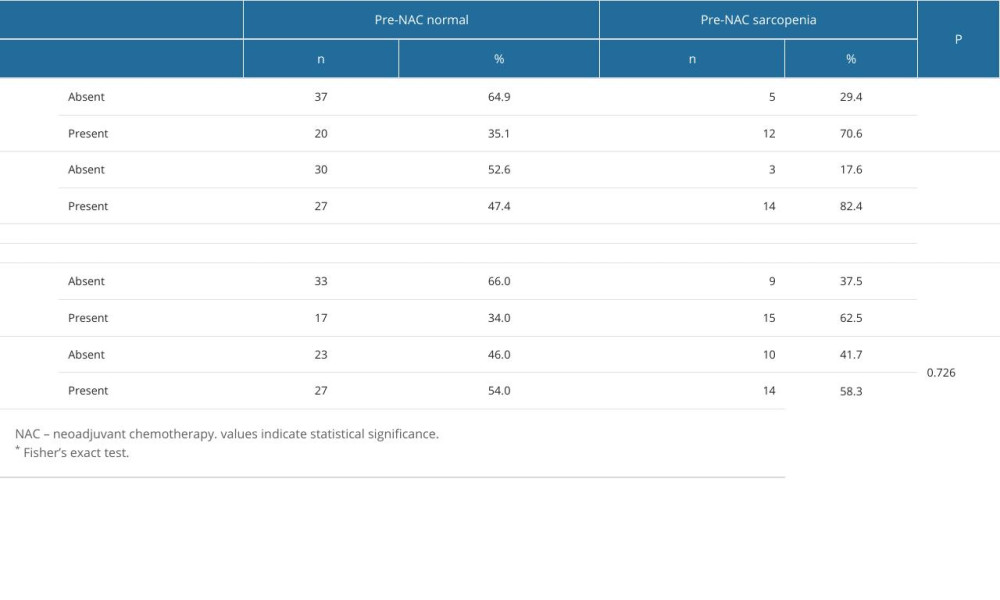
References
1. De Rose F, Meduri B, De Santis MC, Rethinking breast cancer follow-up based on individual risk and recurrence management: Cancer Treat Rev, 2022; 109; 102434
2. Ataollahi MR, Sharifi J, Paknahad MR, Paknahad A, Breast cancer and associated factors: A review: J Med Life, 2015; 8(Spec Iss 4); 6-11
3. Yedjou CG, Sims JN, Miele L, Health and racial disparity in breast cancer: Adv Exp Med Biol, 2019; 1152; 31-49
4. Mokhtari-Hessari P, Montazeri A, Health-related quality of life in breast cancer patients: Review of reviews from 2008 to 2018: Health Qual Life Outcomes, 2020; 18(1); 338
5. Rosenberg IH, Summary comments: Am J Clin Nutr, 1989; 50(5); 1231-33
6. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People: Age Ageing, 2010; 39(4); 412-23
7. Cruz-Jentoft AJ, Bahat G, Bauer J, Sarcopenia: Revised European consensus on definition and diagnosis: Age Ageing, 2019; 48(1); 16-31
8. Rom O, Kaisari S, Aizenbud D, Reznick AZ, Lifestyle and sarcopenia – etiology, prevention, and treatment: Rambam Maimonides Med J, 2012; 3(4); e0024
9. Pamoukdjian F, Bouillet T, Lévy V, Prevalence and predictive value of pre-therapeutic sarcopenia in cancer patients: A systematic review: Clin Nutr, 2018; 37(4); 1101-13
10. Dhanapal R, Saraswathi T, Govind RN, Cancer cachexia: J Oral Maxillofac Pathol, 2011; 15(3); 257-60
11. Davis MP, Panikkar R, Sarcopenia associated with chemotherapy and targeted agents for cancer therapy: Ann Palliat Med, 2019; 8(1); 86-101
12. Ardeljan AD, Hurezeanu R, Sarcopenia: StatPearls [Internet], 2024, Treasure Island (FL), StatPearls Publishing Available from:https://www.ncbi.nlm.nih.gov/books/NBK560813/
13. Adams SC, Segal RJ, McKenzie DC, Impact of resistance and aerobic exercise on sarcopenia and dynapenia in breast cancer patients receiving adjuvant chemotherapy: A multicenter randomized controlled trial: Breast Cancer Res Treat, 2016; 158(3); 497-507
14. Roberto M, Barchiesi G, Resuli B, Sarcopenia in breast cancer patients: A systematic review and meta-analysis: Cancers, 2024; 16(3); 596
15. Iwase T, Parikh A, Dibaj SS, The prognostic impact of body composition for locally advanced breast cancer patients who received neoadjuvant chemotherapy: Cancers, 2021; 13(4); 608
16. Del Fabbro E, Parsons H, Warneke CL, The relationship between body composition and response to neoadjuvant chemotherapy in women with operable breast cancer: Oncologist, 2012; 17(10); 1240-45
17. Amini N, Spolverato G, Gupta R, Impact total psoas volume on short- and long-term outcomes in patients undergoing curative resection for pancreatic adenocarcinoma: A new tool to assess sarcopenia: J Gastrointest Surg, 2015; 19(9); 1593-602
18. Okamura H, Kimura N, Tanno K, The impact of preoperative sarcopenia, defined based on psoas muscle area, on long-term outcomes of heart valve surgery: J Thorac Cardiovasc Surg, 2019; 157(3); 1071-1079e3
19. Lim MH, Lee CH, Ju MH, Je HG, Impact of sarcopenia on outcomes of minimally invasive cardiac surgery: Semin Thorac Cardiovasc Surg, 2023; 35(1); 77-85
20. Ogston KN, Miller ID, Payne S, A new histological grading system to assess response of breast cancers to primary chemotherapy: Prognostic significance and survival: Breast, 2003; 12(5); 320-27
21. Kazemi-Bajestani SMR, Mazurak VC, Baracos V, Computed tomography-defined muscle and fat wasting are associated with cancer clinical outcomes: Semin Cell Dev Biol, 2016; 54; 2-10
22. Rossi F, Valdora F, Bignotti B, Evaluation of body computed tomography-determined sarcopenia in breast cancer patients and clinical outcomes: A systematic review: Cancer Treat Res Commun, 2019; 21; 100154
23. Mazzuca F, Onesti CE, Roberto M, Lean body mass wasting and toxicity in early breast cancer patients receiving anthracyclines: Oncotarget, 2018; 9(39); 25714-22
24. Shachar SS, Deal AM, Weinberg M, Skeletal muscle measures as predictors of toxicity, hospitalization, and survival in patients with metastatic breast cancer receiving taxane-based chemotherapy: Clin Cancer Res, 2017; 23(3); 658-65
25. Prado CMM, Baracos VE, McCargar LJ, Sarcopenia as a determinant of chemotherapy toxicity and time to tumor progression in metastatic breast cancer patients receiving capecitabine treatment: Clin Cancer Res, 2009; 15(8); 2920-26
26. Caan BJ, Cespedes Feliciano EM, Prado CM, Association of muscle and adiposity measured by computed tomography with survival in patients with nonmetastatic breast cancer: JAMA Oncol, 2018; 4(6); 798-804
27. Amitani M, Oba T, Kiyosawa N, Skeletal muscle loss during neoadjuvant chemotherapy predicts poor prognosis in patients with breast cancer: BMC Cancer, 2022; 22(1); 327
28. Lee BM, Cho Y, Kim JW, Association between skeletal muscle loss and the response to neoadjuvant chemotherapy for breast cancer: Cancers, 2021; 13(8); 1806
29. Omarini C, Palumbo P, Pecchi A, Predictive role of body composition parameters in operable breast cancer patients treated with neoadjuvant chemotherapy: Cancer Manag Res, 2019; 11; 9563-69
30. Jang MK, Park S, Park C, Does neoadjuvant chemotherapy regimen affect sarcopenia status in patients with breast cancer?: Breast, 2022; 66; 1-7
31. Rossi F, Lambertini M, Brunetti N, Muscle mass loss in breast cancer patients of reproductive age (≤45 years) undergoing neoadjuvant chemotherapy: Radiol Med, 2023; 128(1); 49-57
32. Kizildag Yirgin I, Has D, Arslan G, Comparison between body composition parameters and response to neoadjuvant chemotherapy by using pre-treatment PET CT in locally advanced breast cancer: Eur J Radiol Open, 2020; 7; 100286
33. Litton JK, Gonzalez-Angulo AM, Warneke CL, Relationship between obesity and pathologic response to neoadjuvant chemotherapy among women with operable breast cancer: J Clin Oncol, 2008; 26(25); 4072-77
34. Fontanella C, Lederer B, Gade S, Impact of body mass index on neoadjuvant treatment outcome: A pooled analysis of eight prospective neoadjuvant breast cancer trials: Breast Cancer Res Treat, 2015; 150(1); 127-39
35. Antoun S, Borget I, Lanoy E, Impact of sarcopenia on the prognosis and treatment toxicities in patients diagnosed with cancer: Curr Opin Support Palliat Care, 2013; 7(4); 383-89
36. Jang MK, Park S, Park C, Hematologic toxicities, sarcopenia, and body composition change in breast cancer patients undergoing neoadjuvant chemotherapy: Support Care Cancer, 2023; 31(7); 419
37. Rier HN, Jager A, Sleijfer S, Low muscle attenuation is a prognostic factor for survival in metastatic breast cancer patients treated with first line palliative chemotherapy: Breast, 2017; 31; 9-15
38. Ferini G, Cacciola A, Parisi S, Curative radiotherapy in elderly patients with muscle invasive bladder cancer: The prognostic role of sarcopenia: In Vivo, 2021; 35(1); 571-78
Figures
Figure 1. A single radiologist measured the cross-sectional transverse areas of the bilateral psoas muscles by manual tracing on the CT images at the middle level of the third lumbar vertebra using a software program (Sectra Workstation IDS7 Version: 25.2.15.7682 #2014 Sectra AB). The PMI, in mm2/m2 is calculated by normalizing the psoas muscle area for height in meters squared. CT – computed tomography; PMI – psoas muscle index.Figure 2. Kaplan-Meier survival curve for disease-free survival according to sarcopenia change status. No statistical difference was found between patients with pre-NAC sarcopenia and post-NAC sarcopenia. We used the SPSS 29.0 software package (IBM Corp., Armonk, NY) to draw this figure. NAC – neoadjuvant chemotherapy.Figure 3. Kaplan-Meier survival curve for OS for disease-free survival according to sarcopenia change status. No statistical difference was found between patients with pre-NAC sarcopenia and post-NAC sarcopenia. We used the SPSS 29.0 software package (IBM Corp., Armonk, NY) to draw this figure. OS – overall survival; NAC – neoadjuvant chemotherapy. Tables
Table 1. Pathologic characteristics of the patients.Table 2. Treatment response, recurrence/progression and final status of the patients.Table 3. Comparison of clinical characteristics by sarcopenia status.Table 4. Comparison of treatment responses and recurrence by pre-treatment sarcopenia status.Table 5. Comparison of treatment responses and recurrence by post-treatment sarcopenia status.Table 6. Comparison of treatment responses in non-sarcopenic patients.Table 7. Comparison of adverse effects in patients with comorbidities based on pre- and post-treatment sarcopenia status.Table 1. Pathologic characteristics of the patients.Table 2. Treatment response, recurrence/progression and final status of the patients.Table 3. Comparison of clinical characteristics by sarcopenia status.Table 4. Comparison of treatment responses and recurrence by pre-treatment sarcopenia status.Table 5. Comparison of treatment responses and recurrence by post-treatment sarcopenia status.Table 6. Comparison of treatment responses in non-sarcopenic patients.Table 7. Comparison of adverse effects in patients with comorbidities based on pre- and post-treatment sarcopenia status. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387