05 April 2025: Clinical Research
Hemoglobin-Albumin-Lymphocyte-Platelet Index and Risk of In-Hospital Mortality in 793 Adult Patients Hospitalized for Acute Exacerbations of Chronic Obstructive Pulmonary Disease
Makbule Ozlem Akbay DOI: 10.12659/MSM.947098
Med Sci Monit 2025; 31:e947098






Abstract
BACKGROUND: Chronic obstructive pulmonary disease (COPD) is a progressive inflammatory condition of the airways, recognized as a leading cause of morbidity and mortality worldwide. Acute exacerbations of COPD (AECOPD) significantly worsen clinical outcomes and often result in hospitalization, which is linked to increased mortality and a substantial socioeconomic burden. This study aimed to evaluate the role of the hemoglobin-albumin-lymphocyte-platelet (HALP) index in predicting the risk of in-hospital mortality in adult patients hospitalized for AECOPD.
MATERIAL AND METHODS: A total of 793 patients (mean±SD age: 71.5±10.2 years, range 23.8-98.4 years, 69.1% males) hospitalized with AECOPD were included in this retrospective cohort study. Data on patient demographics, comorbidities, laboratory findings on the day of hospital admission, intensive care unit (ICU) stay (on initial admission or over the course of hospitalization), and in-hospital mortality rates were recorded. The factors predicting in-hospital mortality risk were analyzed via multivariate logistic regression analysis. Receiver operating characteristic (ROC) curve analysis was performed to determine the performance of HALP score in identifying patients at risk of in-hospital mortality.
RESULTS: Multivariate logistic regression analysis revealed a significant association of lower HALP scores (OR 0.758, 95% CI: 0.586 to 0.980, P=0.034) with increased risk of in-hospital mortality. ROC curve analysis revealed the HALP score to identify patients at risk of in-hospital mortality at a cut-off value of <16.84 (area under curve [AUC]: 0.678, 95% CI: 0.615-0.742, P<0.001) with a sensitivity of 69.1%, specificity of 60.4%, and a NPV of 96.3%.
CONCLUSIONS: Our findings indicate that the HALP score (at a cut-off value of <16.84) can identify AECOPD patients at high risk of in-hospital mortality, emphasizing its potential use as a simple immune–nutritional prognostic biomarker in assisting accurate prognostic assessment and timely adjustment of treatment options in at-risk patients.
Keywords: Acute Disease, biomarkers, Hospitalization, Mortality, Pulmonary Disease, Chronic Obstructive, Humans, Male, Female, Aged, Hospital Mortality, Middle Aged, Aged, 80 and over, Lymphocytes, Retrospective Studies, adult, Hemoglobins, Blood Platelets, ROC Curve, Risk Factors, Serum Albumin, Prognosis, young adult
Introduction
Chronic obstructive pulmonary disease (COPD), a slowly progressing chronic airway inflammatory disease, is associated with an age-dependent rise in incidence and is the third most common cause of morbidity and mortality, and has the highest case fatality rates among chronic respiratory diseases worldwide [1–3].
Acute exacerbations of COPD (AECOPD) refer to acute worsening of respiratory symptoms (ie, dyspnea, cough, or sputum) beyond day-to-day variability that necessitates additional therapy [1,3,4].
AECOPD are the key drivers of adverse clinical outcomes (ie, worsening of clinical symptoms, decline in lung function, and worsening comorbidities) and consequent hospitalization in patients with COPD, while hospitalization for AECOPD is independently associated with an increased mortality risk and a significant socioeconomic burden [1,4–7]. Hence, the global prevalence and impact of COPD on healthcare systems and patient quality of life underlines the critical need for better predictive tools to manage AECOPD effectively [1,2,6,7].
Given the critical role of accurate individual mortality risk assessment during exacerbation, identifying clinically meaningful biomarkers for this purpose has become the subject of interest in the setting of AECOPD [7–11]. However, finding an effective biomarker has been challenging due to the heterogeneity of exacerbations [7,12,13]. Some severity scoring systems have been developed to assist with predicting the adverse outcomes for AECOPD, but a global marker that objectively identifies at-risk patients is still lacking [5,7,12–14].
In addition to the increased airway and systemic inflammatory responses, COPD progression is also associated with widespread nutritional problems due to factors such as advanced airflow limitation, tissue hypoxia, systemic inflammatory response, and oxidative stress [10,15,16].
Although inflammatory markers based on blood cell levels, such as the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR), have been used to predict the prognosis of patients with COPD, these markers cannot reflect the nutritional status of patients [10,11,16–18].
The hemoglobin-albumin-lymphocyte-platelet (HALP) score is a novel index derived from the combination of parameters related to nutritional status (hemoglobin and albumin levels), and those related to inflammatory response (lymphocyte and platelet counts) [19–22]; therefore, it has the unique advantage of reflecting both inflammatory and nutritional status of patients based on laboratory parameters routinely used in everyday practice [19–22].
The HALP score has been demonstrated to predict several clinical outcomes and mortality in a variety of diseases, such as cancers, cardiac disease, and acute ischemic stroke [19–24]. However, the relationship between the HALP score and hospitalization outcomes in AECOPD patients remains poorly investigated, particularly in terms of the predictive ability of HALP score in identifying patients at high risk of in-hospital mortality [10]. Therefore, this study aimed to explore the ability of on-admission HALP scores, in addition to other clinical and laboratory parameters, in predicting in-hospital mortality risk in 793 adult patients hospitalized for AECOPD.
Material and Methods
ETHICS CONSIDERATIONS:
This study was conducted in accordance with the ethical principles stated in the “Declaration of Helsinki” and was approved by our Institutional Ethics Committee (Date of Approval: 13.06.2024 Protocol no: 2024–5). The requirement for informed consent was waived by the committee due to the retrospective nature of the study and minimal risk to subjects.
STUDY POPULATION:
A total of 793 patients hospitalized with AECOPD were included in this retrospective cohort study conducted at a tertiary-care chest disease clinic between January 2022 and December 2023. Hospitalization due to AECOPD and presence of at least 1 pulmonary function test result indicative of COPD in hospital records were the inclusion criteria. Patients with incomplete hospital records, lack of data on 0-h complete blood count analysis and albumin levels, and chronic diseases likely to affect the HALP score (ie, hematologic malignancy or other malignancies and dialysis-requiring chronic kidney disease) were excluded.
ASSESSMENTS:
Data on patient demographics (age, sex), comorbidities, and laboratory findings on the day of hospital admission, as well as the intensive care unit (ICU) stay (on initial admission or over the course of hospitalization) and in-hospital mortality rates were retrieved from hospital records. The HALP score was calculated using the formula: HALP score = [hemoglobin (g/dL) × albumin (g/L) × lymphocytes (103/μL)/platelets (103/μL)] [19]. The factors predicting in-hospital mortality risk were analyzed via univariate and multivariate logistic regression analyses. HALP scores were analyzed with respect to survival outcome and ICU stay. Receiver operating characteristic (ROC) curve analysis was performed to assess the performance of HALP score in identifying patients at risk of in-hospital mortality.
STATISTICAL ANALYSIS:
Statistical analysis was performed using IBM SPSS Statistics for Windows, version 27.0 (IBM Corp., Armonk, NY). The Shapiro-Wilks test and Kolmogorov-Smirnov method were used to investigate normally distributed data. The chi-square (χ2) test was used for comparison of categorical data. The Mann-Whitney U test was used for non-normally distributed data and the independent sample
Results
PATIENT DEMOGRAPHICS, COMORBIDITIES, ICU STAY, AND IN-HOSPITAL MORTALITY:
The mean±SD age of the patients was 71.5±10.2 (range, 23.8–98.4) and 69.1% of 753 patients were male. Respiratory failure (60.9%) and pneumonia (59.5%) were the leading comorbidities (Table 1). Overall, 189 (23.8%) patients required ICU stay, while in-hospital mortality occurred in 55 (5.9%) patients (Table 1).
Laboratory findings on the day of hospital admission are summarized in Table 2. The median (min-max) HALP score on hospital admission was 19.7 (range, 1.8–183.3).
PATIENT DEMOGRAPHICS, COMORBIDITIES, AND LABORATORY FINDINGS ON THE DAY OF HOSPITAL ADMISSION ACCORDING TO IN-HOSPITAL MORTALITY:
Compared with those who survived hospitalization, those with in-hospital mortality were significantly older (76.9±9.8 vs 71.1±10.1 years, P<0.001) and were at more likely to have comorbid respiratory failure (87.3% vs 58.9%, P<0.001), chronic heart failure+atrial fibrillation (50.9% vs 31.6%, P=0.003), atherosclerotic cardiovascular disease (49.1% vs 27.5, P=0.001), and diabetes mellitus (40.0% vs 26.8%, P=0.035) (Table 3).
Compared to those who survived hospitalization, patients with in-hospital mortality had significantly higher WBC (P=0.005) and neutrophil (P<0.001) counts, and significantly higher values for NLR (P<0.001), PLR (P=0.006), CRP (P<0.001), and urea (P<0.001) (Table 4).
Hemoglobin (P<0.001) and hematocrit (P=0.001) levels, lymphocyte count (P=0.001), and serum albumin levels (P<0.001) were significantly lower in patients with in-hospital mortality compared to those who survived hospitalization (Table 4).
ASSOCIATION BETWEEN HALP SCORE, ICU STAY, AND IN-HOSPITAL MORTALITY:
ICU stay was significantly more common in patients with in-hospital mortality than in those who survived hospitalization (94.5% vs 18.6%, P<0.001) (Table 3).
HALP scores were significantly lower in patients with in-hospital mortality compared to those who survived hospitalization (15.0±9.3 vs 25.8±20.5, P<0.001) (Table 4).
HALP scores were also significantly lower in patients with ICU stay than in those without ICU stay (19.7±20.4 vs 26.7±19.8,
UNIVARIATE AND MULTIVARIATE LOGISTIC REGRESSION ANALYSES FOR IN-HOSPITAL MORTALITY RISK FACTORS:
In the univariate analysis, older age (OR 1.062, P<0.001), comorbid presence of chronic heart failure + atrial fibrillation (OR 2.248, P=0.004), respiratory failure (OR 4.776, P<0.001), diabetes mellitus (OR 1.818, P=0.038) or atherosclerotic cardiovascular disease (OR 2.541, P=0.001), and higher values for WBC (OR 1.082, P=0.004), neutrophil (OR 1.144, P<0.001), NLR (OR 1.042, P=0.001), CRP (OR 1.011, P<0.001), and urea (OR 1.016, P<0.001), and lower values for RBC (OR 0.508, P=0.001), hemoglobin (OR 0.924, P=0.001), hematocrit (OR 0.737, P<0.001), lymphocyte (OR 0.489, P=0.001), albumin (OR 0.878, P<0.001) and HALP score (OR 0.576, P<0.001) on hospital admission were found to be associated with increased risk of in-hospital mortality (Table 5).
Among the variables found to be significantly associated with in-hospital mortality risk in the univariate analysis, multivariate logistic regression analysis confirmed the significant association of older age (OR 1.040, 95% CI: 1.007 to 1.073, P=0.016), comorbid respiratory failure (OR 4.716, 95% CI: 2.033 to 10.941, P<0.001), atherosclerotic cardiovascular disease (OR 2.545, 95% CI: 1.388 to 4.668, P=0.003), higher neutrophil counts (OR 1.126, 95% CI: 1.049 to 1.208, P=0.001), lower albumin levels (OR 0.894, 95% CI: 0.840 to 0.953, P=0.001), and lower HALP scores (OR 0.758, 95% CI: 0.586 to 0.980, P=0.034) with increased risk of in-hospital mortality (Table 5).
ROC ANALYSIS FOR THE PERFORMANCE OF HALP SCORE IN IDENTIFYING PATIENTS AT RISK OF IN-HOSPITAL MORTALITY:
ROC analysis revealed that HALP score identified patients at risk of in-hospital mortality at a cut-off value of <16.84 (AUC: 0.678, 95% CI: 0.615–0.742, P<0.001) with a sensitivity of 69.1%, specificity of 60.4%, and a negative predictive value (NPV) of 96.3% (Figure 1).
Discussion
Our retrospective cohort study of hospitalized patients with AECOPD revealed that 23.8% were admitted to the ICU and the in-hospital mortality rate was 5.9%. Lower HALP scores on hospital admission appeared to be associated with longer ICU stays and in-hospital mortality, while ICU stay alone was associated with increased risk of in-hospital mortality. Lower HALP scores were also found to be a significant determinant of in-hospital mortality risk in the multivariate analysis, while the ROC analysis revealed that HALP score at a cut-off value of <16.84 (AUC: 0.678) could identify patients at risk of in-hospital mortality, with a sensitivity of 69.1%, specificity of 60.4%, and NPV of 96.3%.
In a systematic review of 321 studies across different countries in 65 945 patients with AECOPD, the pooled in-hospital mortality rate was 6.2% (highest for Turkey, at 11.8%), while the pooled 30-, 90- and 365-day post-discharge mortality rates were 1.8% (1.5% for Turkey), 5.5% (11.3% for Turkey), and 10.9% (21.0% for Turkey), respectively, with considerable variability across studies and countries [25]. The in-hospital mortality rates in our cohort (5.9%) compared to Turkey-specific data (11.8%, n=1421) in the above-mentioned meta-analysis also emphasizes the potential variability in short-term prognosis of hospitalized AECOPD patients among various centers across Turkey.
The association between ICU admission and mortality in our cohort supports the higher in-hospital mortality rates in ICU-admitted patients with AECOPD hospitalization [8,25–27]. In meta-analysis of 37 studies in 189 772 AECOPD patients, mortality risk was reported to be 3.6% for short-term mortality, 31.0% for long-term (up to 2 years after discharge) mortality, and 29.0% for ICU-admitted patients [26].
Systemic inflammatory response (ie, lymphocyte and platelet counts) and nutritional status (ie, hemoglobin and albumin levels) are considered critical for the prognosis and survival of patients with AECOPD [10,28–30]. Our patients with in-hospital mortality compared to those who survived hospitalization had significantly higher WBC and neutrophil counts, higher NLR, PLR, and CRP levels, and lower lymphocyte counts and albumin levels on admission, while among these blood parameters only neutrophil counts and albumin levels remained significantly associated with mortality in multivariate analysis.
Similarly, the association of lower albumin levels with increased risk of in-hospital mortality in AECOPD patients has been consistently reported [10,14,31,32]. In a previous study with 319 AECOPD patients, in-hospital mortality was 7.2%, while higher neutrophil counts and BUN/albumin ratio ≥0.249 were independent risk factors for in-hospital mortality [14]. Nonetheless, some studies reported that NLR, PLR, and CRP levels were associated with increased in-hospital mortality risk, while NLR (cut-off value >6.90 or >6.24) is reported to be a valuable and accurate marker, with a high predicative ability in the prognosis of in-hospital mortality in AECOPD patients [11,17].
Notably, the complementary utilization of inflammation-associated biomarkers (ie, simultaneously elevated CRP, neutrophils, fibrinogen, and total WBC count) is considered a better approach for predicting the diagnosis and prognosis of AECOPD than the search for a single blood biomarker [7,33–37].
Identification of HALP score, a composite index of an inflammation (lymphocyte and platelet counts) and nutrition (hemoglobin and albumin levels) status, as an independent determinant of increased in-hospital mortality risk in our cohort seems notable in this regard, emphasizing that HALP score is a valuable prognostic biomarker that can be easily and inexpensively applied in respiratory clinical practice to assess the risk of in-hospital mortality in patients with AECOPD [7,10,38]. Similarly, in a previous study with 1533 AECOPD patients, the ICU mortality rate was 8.0%, while a low HALP score (hazard ratio [HR] 1.69) was associated with an increased ICU mortality risk, suggesting that the HALP score may be a novel prognostic predictor in patients with AECOPD [10]. Also, in bronchiectasis patients, the exacerbation period (compared to the stable period) was reported to be associated with significantly lower HALP scores, while HALP score was also correlated negatively with the infectious (leukocytes, neutrophils, and CRP) parameters and positively correlated with the pulmonary functional parameters [38]. In this regard, on-admission HALP scores seem to be a simple and convenient tool in predicting in-hospital mortality risk among patients with AECOPD, as a readily accessible measure of systemic inflammation and nutritional status, which requires only a complete blood count and albumin value [10,19].
Identification of older age as an independent determinant of in-hospital mortality risk in our patients supports the previous reports showing that older age is a significant predictor of mortality from AECOPD [8,25,26,39–42]. Indeed, older age is considered a common prognostic factor for short-term and long-term mortality in hospitalized AECOPD patients as well as for increased risk of mortality in those with ICU admission [26]. Age-specific in-hospital mortality predictors such as hemoglobin and comorbidity index have also been assessed in respiratory-related hospitalizations [43].
We found no significant sex association with in-hospital mortality risk in our study, in which females comprised 30.9% of the study cohort. This seems notable given the controversy regarding the association of male sex with in-hospital mortality in the literature, and the emphasis on the changing COPD epidemiology with increased prevalence (up to 40%) and mortality among females [25,26].
In our cohort, comorbid respiratory failure, chronic heart failure+atrial fibrillation, atherosclerotic cardiovascular disease, and diabetes mellitus were significantly more common in patients with in-hospital mortality than in those who survived hospitalization, while comorbid respiratory failure and atherosclerotic cardiovascular disease remained as significant predictors of in-hospital mortality risk in multivariate analysis. Hypertension, pneumonia, bronchiectasis-tuberculosis sequela, and chronic kidney disease were also among the comorbidities in our AECOPD patients, but they had no significant association with in-hospital mortality risk.
Likewise, in a previous study with 17 207 AECOPD patients, the in-hospital mortality rate was 13.7%, which was associated with older age, and comorbid diseases, including bacterial or viral pneumonia, aspiration pneumonia, interstitial pneumonitis, pulmonary embolism, respiratory failure, lung cancer, heart failure, cerebrovascular diseases, liver cirrhosis, and chronic renal failure [40]. Other studies also reported that extrapulmonary comorbidities such as heart failure, cerebrovascular diseases, liver diseases, and renal diseases were independent predictors of mortality in patients with AECOPD [26,44].
Hence, our findings emphasize the functional and pathophysiological adverse impact of the coexistence of COPD and pulmonary (respiratory failure in particular) and extrapulmonary comorbidities (atherosclerotic cardiovascular disease in particular) in terms of increased frequency of emergency hospitalizations and higher mortality [26,40,45].
Although concomitant pneumonia is considered a common event associated with higher mortality in hospitalized patients with AECOPD [46–48], pneumonia (present in 59.5% of patients) was not found to associated with in-hospital mortality risk in our cohort. Likewise, in a large-cohort study of AECOPD hospitalizations, concomitant pneumonia was not associated with an increased risk of in-hospital mortality, and the authors suggested the low rate of disease and a more prominent role of other comorbidities as the possible reasons [39].
Certain limitations of this study should be considered. The retrospective, single-center design is the main limitation in terms of generalizability of our findings and obtaining robust statistical results in mortality-based subgroup analyses. Other limitations include the lack of data on other outcomes of interest such as nutritional status and the use of single-point laboratory measurement rather than exploring the dynamic changes in HALP score during hospitalization. Nevertheless, our study is the first to reveal the relationship between HALP score and in-hospital mortality of patients with AECOPD through multivariate and ROC analyses.
Conclusions
Our findings in this retrospective cohort study of hospitalized patients with AECOPD indicate the ability of HALP score (at a cut-off value of <16.84) to identify patients at high risk of in-hospital mortality. Accordingly, HALP score seems to be a novel, simple immune–nutritional prognostic biomarker in patients hospitalized with AECOPD, assisting with accurate prognostic assessment and timely adjustment of treatment options in at-risk patients. Nonetheless, the clinical relevance of HALP score and the impact of dynamically changing HALP scores should be further investigated in larger prospective observational studies in the setting of AECOPD hospitalizations.
Data Availability
The detailed participant data are available from the corresponding author upon reasonable request.

Tables
Table 1. Patient demographics, comorbidities, ICU stay and in-hospital mortality.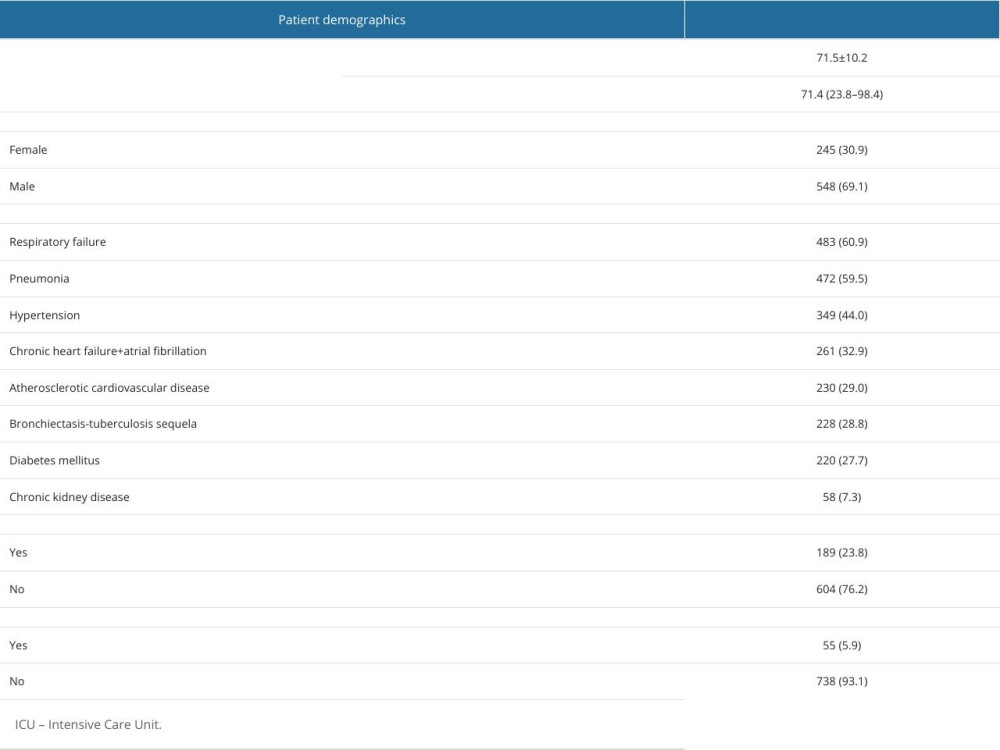 Table 2. Laboratory findings on the day of hospital admission.
Table 2. Laboratory findings on the day of hospital admission. Table 3. Patient demographics, comorbidities, and ICU stay according to in-hospital mortality.
Table 3. Patient demographics, comorbidities, and ICU stay according to in-hospital mortality. Table 4. Laboratory findings on the day of hospital admission according to in-hospital mortality.
Table 4. Laboratory findings on the day of hospital admission according to in-hospital mortality. Table 5. Univariate and multivariate logistic regression analyses for in-hospital mortality risk.
Table 5. Univariate and multivariate logistic regression analyses for in-hospital mortality risk.
References
1. Global Initiative for Chronic Obstructive Lung Disease, Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease: 2024 Report, 2024 Available from: https://goldcopd.org/2024-gold-report/
2. Agarwal AK, Raja A, Brown BD, Chronic obstructive pulmonary disease: StatPearls [Internet] Aug 7, 2023, Treasure Island (FL), StatPearls Publishing
3. Ritchie AI, Wedzicha JA, Definition, causes, pathogenesis, and consequences of chronic obstructive pulmonary disease exacerbations: Clin Chest Med, 2020; 41(3); 421-38
4. Wedzicha JA, Seemungal TA, COPD exacerbations: defining their cause and prevention: Lancet, 2007; 370(9589); 786-96
5. MacLeod M, Papi A, Contoli M, Chronic obstructive pulmonary disease exacerbation fundamentals: diagnosis, treatment, prevention and disease impact: Respirology, 2021; 26(6); 532-51
6. Lima FV, Yen TY, Patel JK, Trends in in-hospital outcomes among adults hospitalized with exacerbation of chronic obstructive pulmonary disease: COPD, 2015; 12(6); 636-42
7. Mathioudakis AG, Janssens W, Sivapalan P, Acute exacerbations of chronic obstructive pulmonary disease: In search of diagnostic biomarkers and treatable traits: Thorax, 2020; 75(6); 520-27
8. Ji Z, Li X, Lei S, A pooled analysis of the risk prediction models for mortality in acute exacerbation of chronic obstructive pulmonary disease: Clin Respir J, 2023; 17(8); 707-18
9. Chen S, Shi Y, Hu B, A prediction model for in-hospital mortality of acute exacerbations of chronic obstructive pulmonary disease patients based on red cell distribution width-to-platelet ratio: Int J Chron Obstruct Pulmon Dis, 2023; 18; 2079-91
10. Han H, Hu S, Du J, Predictive value of the hemoglobin-albumin-lymphocyte-platelet (HALP) index for ICU mortality in patients with acute exacerbations of chronic obstructive pulmonary disease (AECOPD): Intern Emerg Med, 2023; 18(1); 85-96
11. Yao C, Liu X, Tang Z, Prognostic role of neutrophil-lymphocyte ratio and platelet-lymphocyte ratio for hospital mortality in patients with AECOPD: Int J Chron Obstruct Pulmon Dis, 2017; 12; 2285-90
12. Lacoma A, Prat C, Andreo F, Biomarkers in the management of COPD: Eur Respir Rev, 2009; 18(112); 96-104
13. Patel ARC, Hurst JR, Wedzicha JA, The potential value of biomarkers in diagnosis and staging of COPD and exacerbations: Semin Respir Crit Care Med, 2010; 31(3); 267-75
14. Zeng Z, Ke X, Gong S, Blood urea nitrogen to serum albumin ratio: A good predictor of in-hospital and 90-day all-cause mortality in patients with acute exacerbations of chronic obstructive pulmonary disease: BMC Pulm Med, 2022; 22(1); 476
15. Mekal D, Czerw A, Deptala A, Dietary behaviour and nutrition in patients with COPD treated with long-term oxygen therapy: Int J Environ Res Public Health, 2021; 18(23); 12739
16. Girón R, Matesanz C, García-Río F, Nutritional state during COPD exacerbation: Clinical and prognostic implications: Ann NutrMetab, 2009; 54(1); 52-58
17. Emami Ardestani M, Alavi-Naeini N, Evaluation of the relationship of neutrophil-to lymphocyte ratio and platelet-to-lymphocyte ratio with in-hospital mortality in patients with acute exacerbation of chronic obstructive pulmonary disease: Clin Respir J, 2021; 15(4); 382-88
18. Raad S, Smith C, Allen K, Nutrition status and chronic obstructive pulmonary disease: Can we move beyond the body mass index?: Nutr Clin Prac, 2019; 34(3); 330-39
19. Chen XL, Xue L, Wang W, Prognostic significance of the combination of preoperative hemoglobin, albumin, lymphocyte and platelet in patients with gastric carcinoma: A retrospective cohort study: Oncotarget, 2015; 6(38); 41370-82
20. Güç ZG, Alacacıoğlu A, Kalender ME, HALP score and GNRI: Simple and easily accessible indexes for predicting prognosis in advanced stage NSCLC patients. The İzmir oncology group (IZOG) study: Front Nutr, 2022; 9; 905292
21. Tian M, Li Y, Wang X, The hemoglobin, albumin, lymphocyte, and platelet (HALP) score is associated with poor outcome of acute ischemic stroke: Front Neurol, 2021; 11; 610318
22. Pan H, Lin S, Association of hemoglobin, albumin, lymphocyte, and platelet score with risk of cerebrovascular, cardiovascular, and all-cause mortality in the general population: results from the NHANES 1999–2018: Front Endocrinol (Lausanne), 2023; 14; 1173399
23. Guo Y, Shi D, Zhang J, The Hemoglobin, albumin, lymphocyte, and platelet (HALP) score is a novel significant prognostic factor for patients with metastatic prostate cancer undergoing cytoreductive radical prostatectomy: J Cancer, 2019; 10(1); 81-91
24. Liu L, Gong B, Wang W, Association between haemoglobin, albumin, lymphocytes, and platelets and mortality in patients with heart failure: ESC Heart Fail, 2024; 11(2); 1051-60
25. Waeijen-Smit K, Crutsen M, Keene S, Global mortality and readmission rates following COPD exacerbation-related hospitalisation: A meta-analysis of 65 945 individual patients: ERJ Open Res, 2024; 10(1); 00838-2023
26. Singanayagam A, Schembri S, Chalmers JD, Predictors of mortality in hospitalized adults with acute exacerbation of chronic obstructive pulmonary disease: Ann am Thorac Soc, 2013; 10(2); 81-89
27. Ergan B, Ergun R, Impact of anemia on short-term survival in severe COPD exacerbations: A cohort study: Int J Chron Obstruct Pulmon Dis, 2016; 11; 1775-83
28. Park SC, Kim YS, Kang YA, Hemoglobin and mortality in patients with COPD: A nationwide population-based cohort study: Int J Chron ObstrPulm Dis, 2018; 13; 1599-605
29. Shi X, Shen Y, Yang J, The relationship of the geriatric nutritional risk index to mortality and length of stay in elderly patients with acute respiratory failure: A retrospective cohort study: Heart Lung, 2021; 50(6); 898-905
30. Chen L, Chen L, Zheng H, Emergency admission parameters for predicting in-hospital mortality in patients with acute exacerbations of chronic obstructive pulmonary disease with hypercapnic respiratory failure: BMC Pulm Med, 2021; 21(1); 258
31. Asiimwe AC, Brims FJ, Andrews NP, Routine laboratory tests can predict in-hospital mortality in acute exacerbations of COPD: Lung, 2011; 189(3); 225-32
32. Chen D, Jiang L, Li J, Interaction of acute respiratory failure and acute kidney injury on in-hospital mortality of patients with acute exacerbation COPD: Int J Chron ObstrPulm Dis, 2021; 16; 3309-16
33. Cai C, Zeng W, Wang H, Neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and monocyte-to-lymphocyte ratio (MLR) as biomarkers in diagnosis evaluation of acute exacerbation of chronic obstructive pulmonary disease: A retrospective, observational study: Int J Chron Obstruct Pulmon Dis, 2024; 19; 933-43
34. Keene JD, Jacobson S, Kechris K, Biomarkers predictive of exacerbations in the SPIROMICS and COPDGene cohorts: Am J Respir Crit Care Med, 2017; 195(4); 473-81
35. Donaldson GC, Wedzicha JA, Prediction of chronic obstructive pulmonary disease exacerbation frequency. Clinical parameters are still better than biomarkers: Am J Respir Crit Care Med, 2017; 195(4); 415-16
36. Noell G, Cosío BG, Faner R, Multi-level differential network analysis of COPD exacerbations: Eur Respir J, 2017; 50(3); 1700075
37. Thomsen M, Ingebrigtsen TS, Marott JL, Inflammatory biomarkers and exacerbations in chronic obstructive pulmonary disease: JAMA, 2013; 309(22); 2353-61
38. Çolak M, Çoban H, Sarioğlu N, Could the HALP score serve as a biomarker of bronchiectasis exacerbation?: TuberkToraks, 2024; 72(1); 9-15
39. Montagnani A, Mathieu G, Pomero F, Hospitalization and mortality for acute exacerbation of chronic obstructive pulmonary disease (COPD): An Italian population-based study: Eur Rev Med Pharmacol Sci, 2020; 24(12); 6899-907
40. Hasegawa W, Yamauchi Y, Yasunaga H, Factors affecting mortality following emergency admission for chronic obstructive pulmonary disease: BMC Pulm Med, 2014; 14; 151
41. Dong F, Ren X, Huang K, Development and validation of risk prediction model for in-hospital mortality among patients hospitalized with acute exacerbation chronic obstructive pulmonary disease between 2015 and 2019: Front Med (Lausanne), 2021; 8; 630870
42. Esteban C, Castro-Acosta A, Alvarez-Martínez CJ, Predictors of one-year mortality after hospitalization for an exacerbation of COPD: BMC Pulm Med, 2018; 18(1); 18
43. Chongthanadon B, Thirawattanasoot N, Ruangsomboon O, Clinical factors associated with in-hospital mortality in elderly versus non-elderly pneumonia patients in the emergency department: BMC Pulm Med, 2023; 23(1); 330
44. Almagro P, Cabrera FJ, Diez J, Comorbidities and short-term prognosis in patients hospitalized for acute exacerbation of COPD: The EPOC enServicios de medicina interna (ESMI) study: Chest, 2012; 142(5); 1126-33
45. Cavailles A, Brinchault-Rabin G, Dixmier A, Comorbidities of COPD: Eur Resp Rev, 2013; 22(130); 454-75
46. Stefan MS, Shieh MS, Pekow PS, Trends in mechanical ventilation among patients hospitalized with acute exacerbations of COPD in the United States, 2001 to 2011: Chest, 2015; 147(4); 959-68
47. Søgaard M, Madsen M, Løkke A, Incidence and outcomes of patients hospitalized with COPD exacerbation with and without pneumonia: Int J Chron Obstruct Pulmon Dis, 2016; 11; 455-65
48. Chalmers JD, Singanayagam A, Akram AR, Severity assessment tools for predicting mortality in hospitalised patients with community-acquired pneumonia. Systematic review and meta-analysis: Thorax, 2010; 65(10); 878-83
Tables
Table 1. Patient demographics, comorbidities, ICU stay and in-hospital mortality.Table 2. Laboratory findings on the day of hospital admission.Table 3. Patient demographics, comorbidities, and ICU stay according to in-hospital mortality.Table 4. Laboratory findings on the day of hospital admission according to in-hospital mortality.Table 5. Univariate and multivariate logistic regression analyses for in-hospital mortality risk.Table 1. Patient demographics, comorbidities, ICU stay and in-hospital mortality.Table 2. Laboratory findings on the day of hospital admission.Table 3. Patient demographics, comorbidities, and ICU stay according to in-hospital mortality.Table 4. Laboratory findings on the day of hospital admission according to in-hospital mortality.Table 5. Univariate and multivariate logistic regression analyses for in-hospital mortality risk. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387