11 July 2025: Clinical Research
Audiological and Middle Ear Outcomes in Ukrainian Soldiers with Traumatic Tympanic Membrane Perforation
Roman Barylyak DOI: 10.12659/MSM.948326
Med Sci Monit 2025; 31:e948326






Abstract
BACKGROUND: Blast injury of the ear due to explosive force can result in perforation of the tympanic membrane and damage to the middle ear structures. This study evaluated the middle ear and audiological outcomes in 70 men with persistent traumatic tympanic membrane perforation fighting the war in Ukraine.
MATERIAL AND METHODS: Participants underwent basic audiological assessment (otoscopy and pure-tone audiometry) and surgery between 2023 and 2024.
RESULTS: Perforation of 2 quadrants compared to 1 quadrant was associated with greater hearing loss (p=0.004) and larger air-bone gap (p<0.001). Lesioning of 2 quadrants was also associated with more middle ear lesions (p=0.033). Surgery improved hearing compared to preoperative data (p<0.001). Postoperatively, we noted the shift in air conduction threshold level compared to bone conduction threshold level (ie, closure of the air-bone gap) (p<0.001).
CONCLUSIONS: Tympanic membrane perforations primarily occur in 2 quadrants, leading to more significant hearing loss and a larger air-bone gap (ABG), with a statistically significant difference. No significant difference in ABG was found between the anterior and posterior quadrants. The risk of epidermal complications in the eardrum cavity is quite high, even with small to medium-sized perforations. Surgical intervention was found to improve middle ear conditions and enhance hearing outcomes.
Keywords: Blast Injuries, Hearing Loss, Tympanic Membrane Perforation, Tympanoplasty, Cholesteatoma, Humans, Male, Military Personnel, Ear, Middle, adult, Ukraine, Audiometry, Pure-Tone, Tympanic Membrane, young adult, Bone Conduction, Treatment Outcome
Introduction
Compared to the past, modern armed conflict differs in terms of form, scale, and complexity [1], and there has been a significant increase in the number of injuries caused by explosives [2,3]. During the U.S. Civil War, only 9% of injuries were due to explosives, with the other 91% due to gunshot. Subsequently, the proportion of gunshot injuries to explosive injuries has decreased, with the latter now predominating. For American soldiers, it has been estimated that in World War I the ratio was 65/35 (gunshot/explosive), in World War II it was 27/73, in Korea 31/69, Vietnam 35/65, and in Iraq and Afghanistan 19/81 [3]. Another study among U.S. servicemen, in which injuries were analyzed by dividing them into blast, gunshot, and other non-combat injuries, blast injuries were 64% in World War II, 54% in the Korean War, and 68% in Iraq [2]. During 2006–2010, 72% of U.S. military compensations were for hearing damage [4]. From Iraq, 31% of veterans were diagnosed with post-explosion ear damage [5]. In 2013, about 551 000 U.S. soldiers suffered blast injuries to the ear from operations in Iraq and Afghanistan [6,7].
The current war in Ukraine is being fought with a relatively large number of explosive devices. The main means of destruction are artillery, guided aircraft bombs, precision-guided aerial and ground drones carrying explosive charges, and missiles. Anti-personnel and anti-tank mines, as well as anti-tank guided missile systems, are most often used for short-range attacks [8]. According to available sources, the Russian army fires up to 60 000 artillery shells per day [9,10], and its airforce drops up to 3000 guided aerial bombs of varying power each month [11].
There are 4 types of blast injuries [12–15]:
Primary blast injuries most often occur to air-filled organs such as the ears and lungs, but can also involve abdominal organs, the parenchyma of the brain, and the eyes. The ears are particularly sensitive to explosions, and injuries to them manifest as hearing loss, tinnitus, dizziness, or bleeding [16]. Common injuries are damage to the ossicular chain, cochlear damage, and perforation of the eardrum (the most common injury to the middle ear) [13,17]. Horrocks (2001) found tympanic membrane rupture in 74% of people diagnosed as having primary blast injury [18]. A generally accepted procedure is to observe the healing of ear injuries for 3–6 months [19]. The physical examination should include direct visualization of the tympanic membrane (otoscopy) and a general assessment of vestibular function and hearing tests [17]. Fortunately, most traumatic tympanic membrane perforations heal spontaneously, in which case the membrane returns to its original function [20]. Spontaneous healing occurs most intensely in the first 3 months after injury and lasts up to 6 months and even up to a year [19–22]. Small perforations are more likely to close completely [23,24]. However, if healing stops, perhaps due to tissue loss, secondary infection, or the formation of pathological lesions, surgical reconstruction of the middle ear is necessary [20,25–29].
The effect of a shock wave of up to 160 dB is likely to cause serious damage to the ear [30,31]. The degree of injury depends on factors such as the speed, intensity, or duration of the pressure pulse [25]. Ear trauma can result in conductive, sensorineural, or mixed hearing loss, indicated in the results of pure-tone audiometry [32].
The most common cause of conductive-type hearing loss is damage to the tympanic membrane. The damage can range from a minor vascular defect, small linear ruptures, to wrapping of membrane fragments into the tympanic cavity; more seriously, there can be large perforations outwards or almost total perforations involving displacement and fracture of the ossicles [30,33]. Mixed or sensorineural hearing losses indicate damage to the inner ear [25,30,31]. Mixed hearing loss occurs in most patients after an explosion, although an audiometric study of U.S. Army veterans found that the majority of those with a hearing loss had sensorineural hearing loss [34].
The size of a tympanic membrane perforation is given in millimeters (mm) or as a percentage of the perforation area to the area of tympanic membrane. In a comparative study of the treatment of post-traumatic tympanic membrane perforation, a criterion based on perforation size was made, such that a small perforation was <3 mm, a medium perforation 3–5 mm, and large perforation >5 mm [35]. The same ranking of perforation sizes was also presented by Jafarov et al [36]. For patients who fail to achieve satisfactory outcomes from tympanoplasty, a final option is the use a hearing implant [37–39].
Therefore, this study evaluated the middle ear and audiological outcomes in 70 men with persistent traumatic tympanic membrane perforation fighting the war in Ukraine.
Material and Methods
ETHICS:
This retrospective study was approved by the Bioethics Committee of the Institute of Physiology and Pathology of Hearing, Warsaw (IFPS: KB/8/2024). All patients voluntarily consented to the processing of personal data under the condition of its protection according to the Law of Ukraine “On Personal Data Protection.” Collected data was anonymized and stored in a dedicated database In Excel.
INCLUSION AND EXCLUSION CRITERIA:
The inclusion criterion was post-explosive ear damage with persistent perforations not exceeding 5 mm (extending up to half the diameter of the eardrum). Exclusion criteria were perforations resulting from chronic inflammatory lesions of the ear or after previous tympanoplasty surgeries, as well as conditions following shrapnel trauma to the temporal bone.
STUDY GROUP:
A retrospective analysis of 70 patients who had persistent post-traumatic ear injury caused by blasts in warfare was performed from July 2024 to March 2025. Patients were aged 19–59 years (M=37.2; SD=10.2). All had perforations remaining after some spontaneous healing had taken place and the lesions had not been operated on before. Details of the sociodemographic and clinical characteristics of the patients are shown in Table 1.
AUDIOLOGICAL EVALUATION:
Otoscopy and pure-tone audiometry (PTA) were used for audiological evaluation. PTA was performed to determine air and bone conduction thresholds. All participants underwent hearing evaluation before and after surgery, but as we present in the following sections of the article, we only analyzed data gathered by us, not from external medical centers, to exclude variability. We obtained 59 preoperative (out of 70 participants) and 19 postoperative tests of pure-tone audiometry. We excluded 2 patients with preoperative deafness from the comparison of hearing test results. After the treatment and convalescence, patients returned to their military units and duties.
SURGICAL TECHNIQUE:
Assessment of perforation size was performed intraoperatively using ear dissectors with an arm length reaching from 2 to 5 mm. Surgeries were carried out under general anesthesia, with a cut made on the posterior wall of the external auditory canal with a Rosen knife. In some patients, it was necessary to extend the bony walls of the ear canal using a diamond cutter. In such cases, the cut was extended to the lower and anterior walls. After lifting the skin and tympanic membrane, it was possible to assess the condition of the middle ear and remove any lesions encountered in the tympanic cavity. Removal of lesions from the middle ear was often associated with an increase in the size of the perforation, especially in cases involving wrapped fragments of the tympanic membrane. These fragments were excised along with part of the edge of the perforation. The next step was to separate the tympanic membrane from the handle of the malleus. If necessary, reconstruction of the ossicles was conducted. Next, a piece of perichondrium was taken from a scrap of the ear. The perichondrium graft was placed under the tympanic membrane ring on the malleus handle under the remnants of the tympanic membrane. The surgical technique involved at least 3 points of support for the eardrum graft: on the handle of the malleus; on the bony walls (posterior, inferior, and sometimes anterior); and under the eardrum ring. A pressure dressing was left in the ear canal for up to 10 days. All surgeries were performed by the same surgeon (the first author).
STATISTICAL ANALYSIS:
Statistical analysis was performed using IBM SPSS Statistics (v. 25) and Jamovi Software (v. 2.6.44). Descriptive statistics were used to indicate the means (M) and standard deviation (SD). The Shapiro-Wilk test was used to assess the normality of the data, followed by a
Results
RELATIONSHIP BETWEEN THE SIZE OF THE PERFORATION AND PURE-TONE AUDIOMETRY RESULTS:
The size of the tympanic membrane perforation was measured during an intraoperative evaluation. According to the previously mentioned classification [35], perforations were small (<3 mm) in 4 patients (6%) and medium (3–5 mm) in 66 patients (94%). In our analysis (Kruskal-Wallis test) of the effect of the peroration size on hearing results, we discarded subjects who had a 2-mm perforation due to the smaller number of subjects compared to the other perforations. We analyzed the results in relation to ABG (n=56); a difference of 1 mm was not statistically significant (3 mm vs 4 mm – P=0.158 and 4 mm vs 5 mm – P=0.072). For an air-bone gap difference of 2 mm (3 mm vs 5 mm), the result was statistically significant (P=0.002).
RELATIONSHIP BETWEEN PREOPERATIVE PURE-TONE AUDIOMETRY RESULTS AND CHANGE IN AVERAGE THRESHOLD AND AIR-BONE GAP VALUES AFTER OTOSURGERY:
Table 2 shows the mean hearing thresholds and standard deviations for 59 subjects. To assess whether the surgery influenced hearing, a group of 19 subjects was separated and statistically analyzed via the paired-sample t test or Wilcoxon test, depending on the normality of the data. The results were statistically significant. For air conduction, the mean hearing threshold before surgery was worse than after surgery. We noted the shift in air conduction (AC) threshold level compared to bone conduction (BC) threshold level (the closure of the air-bone gap – ABG). As with bone conduction, we noted a change, but we do not see it as clinically significant because the difference was quite small (1.5 dB) and may have been due to the subjective nature of the pure-tone audiometry.
RELATIONSHIP BETWEEN THE NUMBER OF PERFORATED QUADRANTS (1 OR 2 QUADRANTS) AND PURE-TONE AUDIOMETRY RESULTS:
Most patients (42 [60%]) had perforations occurring in 2 quadrants. In the remaining 28 patients (40%), perforations were present in just 1 quadrant.
As illustrated in Table 3, perforation of 2 quadrants compared to 1 quadrant was associated with worse air conduction and larger ABG (n=59); with 2 quadrants, the mean AC was 39.1 dB and the mean ABG was 21.2; while with 1 quadrant, the mean AC was 29.0 dB and the mean ABG was 13.7 dB. The differences were statistically significant, with P=0.004 and P<0.001, respectively (n=59).
RELATIONSHIP BETWEEN THE LOCATION OF THE TYMPANIC MEMBRANE PERFORATION AND AIR-BONE GAP:
Table 4 presents a comparison of values of air-bone gaps in relation to site of perforation. Our study showed that the difference in ABG between anterior (anteroinferior and anterosuperior quadrant) and posterior (posteroinferior and posterosuperior quadrant) perforations were not statistically significant.
PATHOLOGICAL LESIONS: DIVISION INTO GROUPS, LOCATION, QUADRANTS, AND RESULTS OF PURE-TONE AUDIOMETRY:
Tympanic membrane perforations were present in all patients, and in 28 (40%) of them occurred in isolation, that is, without any other additional lesion. This was called the uncomplicated group (UG). However, 42 patients (60%) had additional lesions detected intraoperatively, and these were classified into 2 additional groups. One contained squamous epithelium lesions of the middle ear, and was called the SELG group. It included cystic epidermal lesions (cholesteatoma), epidermal layering, ingrowth from the tympanic membrane onto the walls of the tympanic cavity and ossicles, and wrapping of fragments of the tympanic membrane into the tympanic cavity. This SELG group consisted of 31 people – 22 with cholesteatoma and ingrown epidermis, and 9 without epidermal complications, but with the eardrum fused to the ossicles or walls of the eardrum cavity (which poses a risk of developing cholesteatoma complications in the future). The second group (11 patients) had advanced adhesions of connective tissue and ossicular chain lesions associated with poor conduction, and was called the fibrotic adhesions and ossicle lesions group (FAaOLG).
There were 42 patients (SELG and FAaOLG group) who had lesions and perforations. We detected unorganized epidermal masses or epidermis growing into the tympanic cavity in 17 cases (41%), cystic epidermal lesions (cholesteatoma) in 10 cases (24%), wrapping of the edges of the tympanic membrane into the tympanic cavity in 24 cases (57%), advanced adhesions of connective tissue in 28 cases (67%), and damage to the ossicular chain in 10 cases (24%).
In 13 patients (31%), the above lesions occurred in isolation. However, 17 others (41%) had 2 lesions, and 8 (19%) had 3 lesions. The presence of 4 or 5 lesions occurred in only 2 people (5%). Details of the location of the lesions are listed in Table 5.
Table 6 shows the location of tympanic membrane perforations, which occurred singly (1 quadrant) or in 2 quadrants. Tympanic membrane damage associated with middle ear epidermal lesions occurred in 31 patients, in whom 51 lesions were detected, including 16 (31%) in ears with tympanic membrane perforation in 1 quadrant and 35 (69%) in 2 quadrants.
In ears with identified lesions, perforation was most common in the lower quadrants of AI + PI (cholesteatoma, 6 of 10; ingrown epidermis, 7 of 17; ingrown eardrum edges, 11 of 24; advanced adhesions, 10 of 28). Examples of complications are illustrated in the Figures 1 and 2.
Perforation of the tympanic membrane in ears without additional lesions (n=28) was most common in the anterior and inferior quadrants, occupying the 2 quadrants AS + AI (10 times), followed by AI + PI (7 times). For 1 quadrant, the sum of anterior quadrants was higher (n=7; AS, 3 subjects; AI, 4 subjects) than the sum of posterior quadrants (n=4; PS, 0 subjects; PI, 4 subjects).
Among the 31 patients who had epidermal lesions (SELG), there were 12 (39%) who had epidermal complications not combined with “benign” lesions, of whom 4 (33%) had 1 complication, 7 (58%) had 2 types of complications, and 1 (8%) had all types – cholesteatoma, ingrown epidermis, and wrapping of the edges of the tympanic membrane. The remaining 19 individuals (61%) had connective tissue changes and ossicular defects as well as these complications. Among these 19, 11 (58%) had 1 epidermal complication, 5 (26%) had 2 complications, and 3 (16%) had all 3 complications. FAaOLG consisted of advanced adhesions changes, which appeared in 8 people (73%), 1 person (9%) had ossicular defects, and 2 people (18%) had adhesion lesions as well as ossicular defects.
Fragments of the tympanic membrane most often wrapped around the malleus (21 of 24 cases), and cholesteatoma and ingrown epidermis most often formed around the malleus handle (7 of 10 and 12 of 17, respectively). Figure 2 shows the post-explosive perforation of the tympanic membrane on the first day after injury.
In the SELG group, the average threshold for bone conduction was 21.4 dB, for air conduction it was 39.5 dB, and the mean ABG was 18.1 dB. In the FAaOLG group, these values were 13.4 dB for bone conduction, 33.0 dB for air conduction, and 19.6 for ABG. In the UG group, the values were 13.2 dB for bone conduction, 31.4 dB for air conduction, and 18.2 dB for ABG.
Among the 10 patients diagnosed with ossicular defects, advanced connective tissue lesions (possibly after bleeding into the middle ear cavity) were found in 8 subjects (80%). Epidermal complications were observed in 6 subjects (60%), including 4 subjects (67%) with 1 at-risk lesion each (2 with epidermal changes in the tympanic cavity and 2 with an ingrown tympanic membrane) and 2 (33%) with all 3 epidural complications.
Occurrence of more complications was associated with damage of 2 quadrants, which was statistically significant (
RECONSTRUCTION DETAILS:
The eardrum was reconstructed in 67 patients. In 3 (4%), mobility improved as soon as the ossicular chain was reconstructed. Two types of ossicular reconstruction were performed. In 2 patients with incus dislocation and disconnection with the stapes, ossicular chain reconstruction was performed. A prosthesis was made from the patient’s own ossicle, using the interposition method of the incus, which was prepared and placed on the stapes under the malleus handle. In 1 patient, malleus and incus mobilization was performed in the attic through the gently widened attic wall. The immobilization was probably caused by displacement of the ossicles, ligament tears, and bleeding around them. In 3 patients (4%), the middle ear was inflamed, so the tympanic cavity and ossicles were cleared of inflammation without reconstruction. In 32 ears (46%), we performed intraoperative dilatation of the bony part of the ear canal (canaloplasty) to control the anterior and inferior quadrants of the tympanic membrane. One patient developed a re-perforation following middle ear inflammation in the postoperative period.
Discussion
LIMITATIONS OF THE STUDY:
One of the limitations of the present study is that we could not assess potential confounding factors like pre-existing hearing loss or determine the force of the explosion that led to the rupture of the eardrum. Information about the circumstances of the injury is sensitive. Preoperative HRCT (high-resolution computed tomography) or MRI (magnetic resonance imaging) examinations to evaluate the condition of the tympanic and mastoid cavities were performed according to the surgeon’s decision, so their results were not evaluated in this paper. Also, the results of pathological examination of the removed tissues are not included in our analyses.
Conclusions
Injuries to the middle ear caused by explosions from military operations are frequent and require careful evaluation and observation. Tympanic membrane perforations (the most common combat injury to the middle ear) mostly appear in 2 quadrants, which leads to greater hearing loss and bigger air-bone gap. The difference in ABG was statistically significant when comparing the results of pure-tone audiometry with perforations in 1 quadrant (anterior or posterior) versus 2 quadrants. In contrast, there was no difference in ABG in the anterior and posterior quadrants. Persistent perforations of the tympanic membrane might be accompanied by several pathological lesions, among which the most important are the so-called epidermal complications for the middle ear, which include unorganized epidermal masses or epidermis growing into the tympanic cavity, cystic epidermal lesions (cholesteatoma), and wrapping of the edges of the tympanic membrane into the tympanic cavity. Occurrence of more complications was associated with damage of 2 quadrants. The incidence of complications from blast injuries during warfare may be higher than reported. If complications are suspected, early surgical intervention is recommended. Surgical intervention improves the condition of the middle ear and enhances hearing outcomes, including improved air conduction and closure of the air-bone gap.
Figures
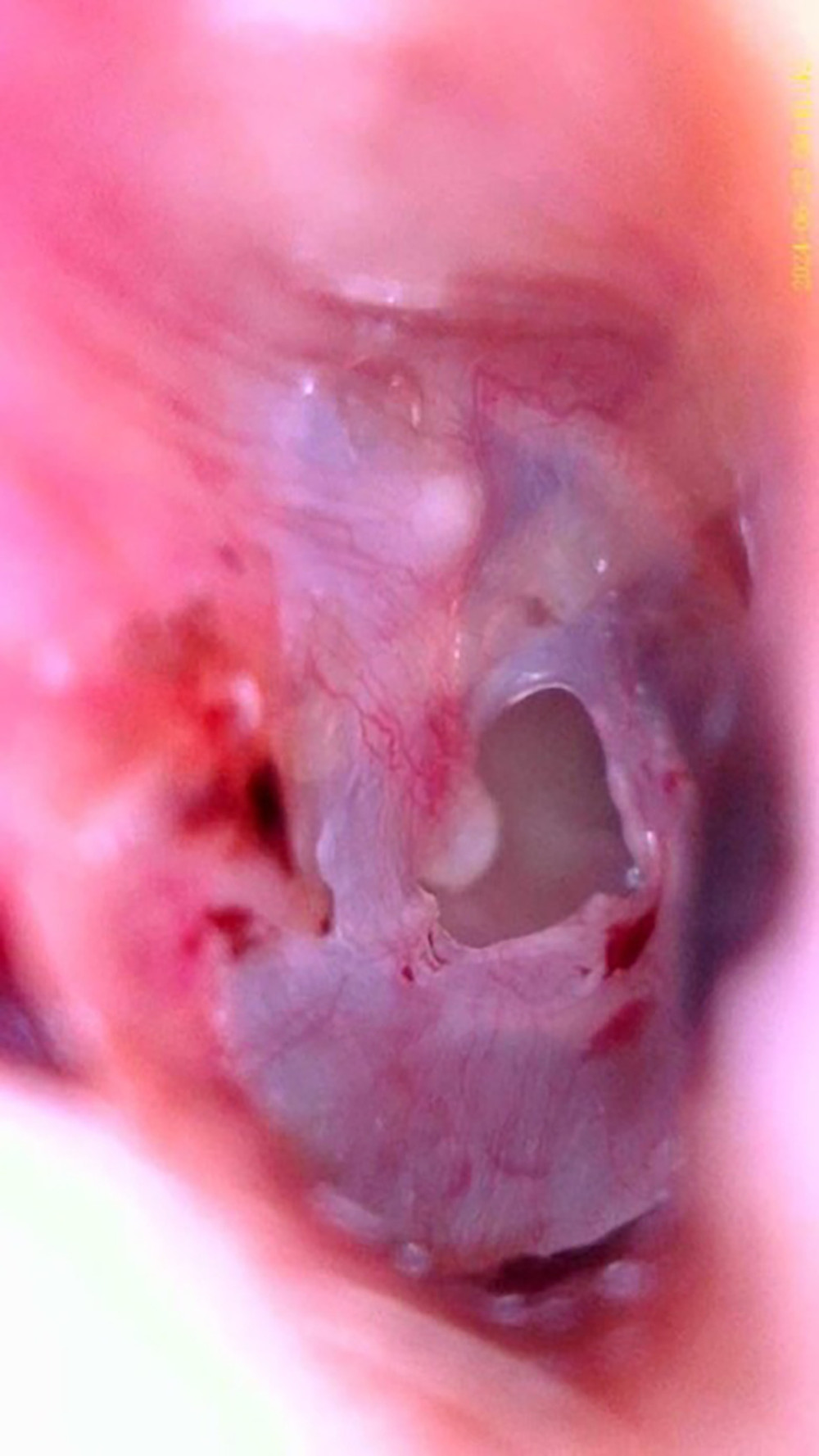 Figure 1. A typical C-shaped central perforation of the tympanic membrane, similar to a “kidney bean” shape but ripped fragment of the tip of the malleus handle wrapped in the tympanic membrane, including on the inner side. A cholesteatoma formed in the area of the auricle. The lower edge of the perforation is smooth, thickened, with possible downward wrapping of membrane fragments.
Figure 1. A typical C-shaped central perforation of the tympanic membrane, similar to a “kidney bean” shape but ripped fragment of the tip of the malleus handle wrapped in the tympanic membrane, including on the inner side. A cholesteatoma formed in the area of the auricle. The lower edge of the perforation is smooth, thickened, with possible downward wrapping of membrane fragments. 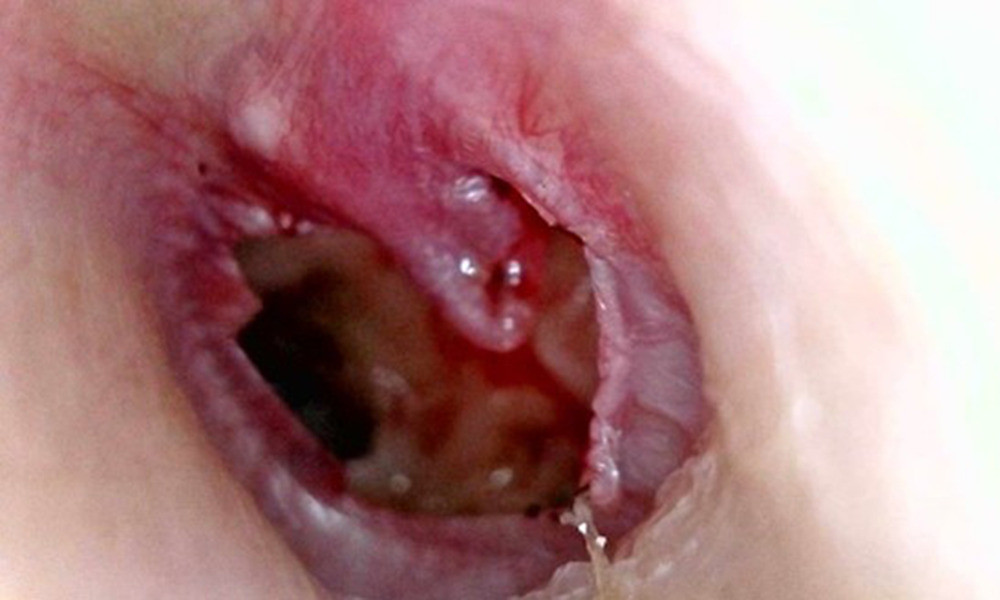 Figure 2. Post-explosive perforation of the tympanic membrane on the first day after injury. Perforation involves all quadrants. The remaining tympanic membrane was hemorrhaged. Fragments of tympanic membrane are wrapped around the handle of the malleus.
Figure 2. Post-explosive perforation of the tympanic membrane on the first day after injury. Perforation involves all quadrants. The remaining tympanic membrane was hemorrhaged. Fragments of tympanic membrane are wrapped around the handle of the malleus. Tables
Table 1. Sociodemographic and clinical data of the patients*.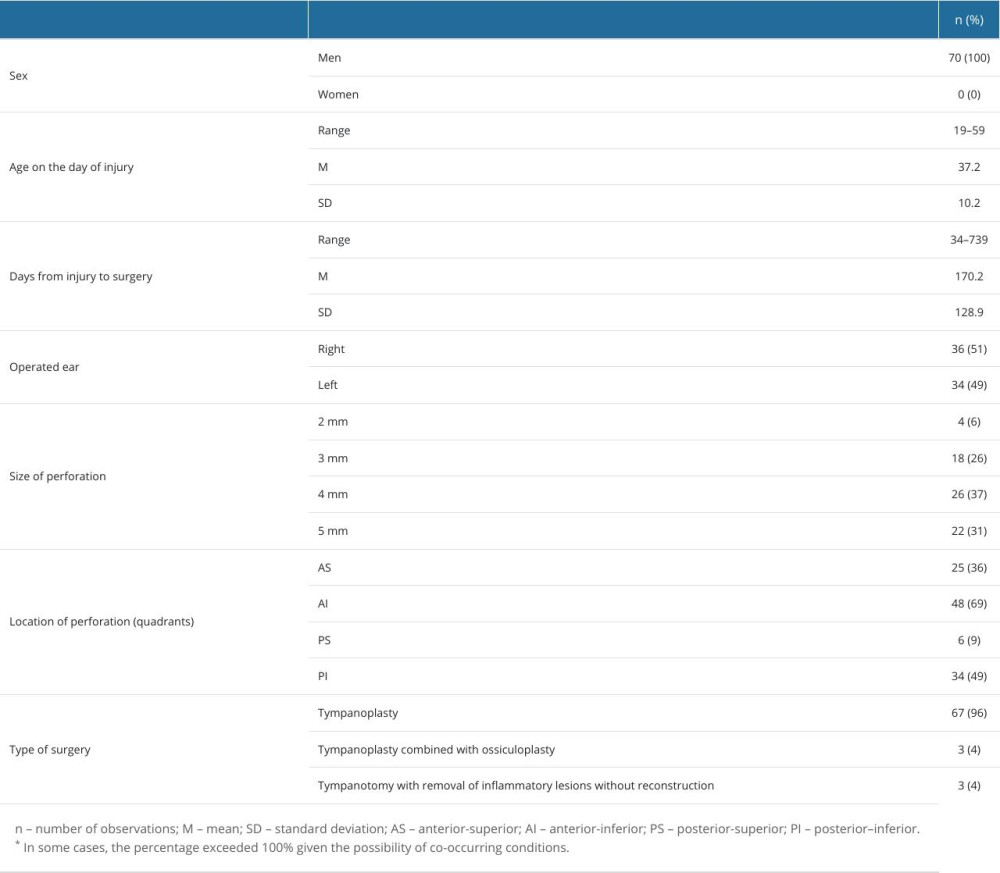 Table 2. Pre- and postoperative mean pure-tone audiometry hearing results.
Table 2. Pre- and postoperative mean pure-tone audiometry hearing results.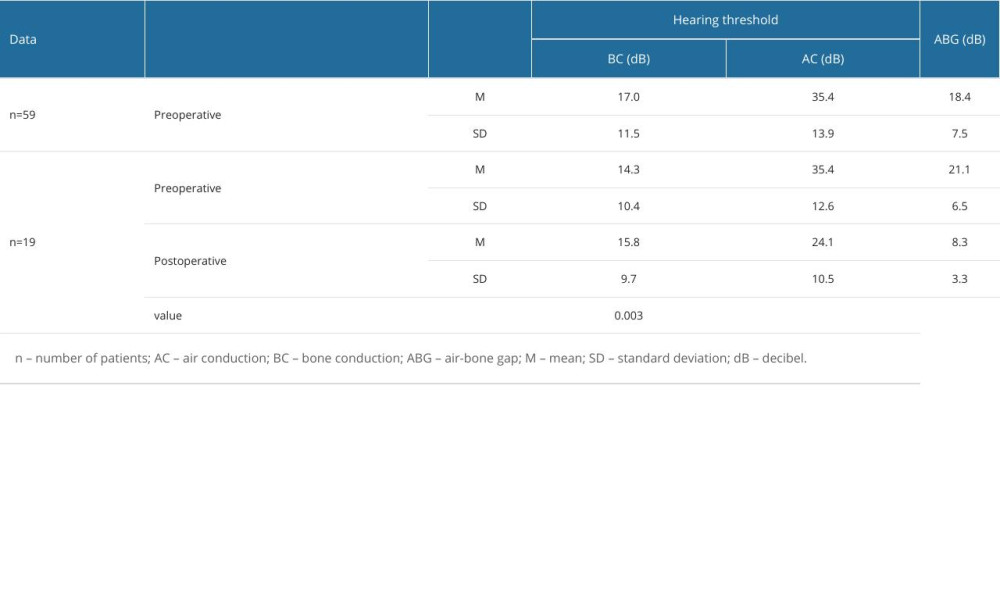 Table 3. Results of pure-tone audiometry in relation to perforation of the tympanic membrane in 1 vs 2 quadrants.
Table 3. Results of pure-tone audiometry in relation to perforation of the tympanic membrane in 1 vs 2 quadrants.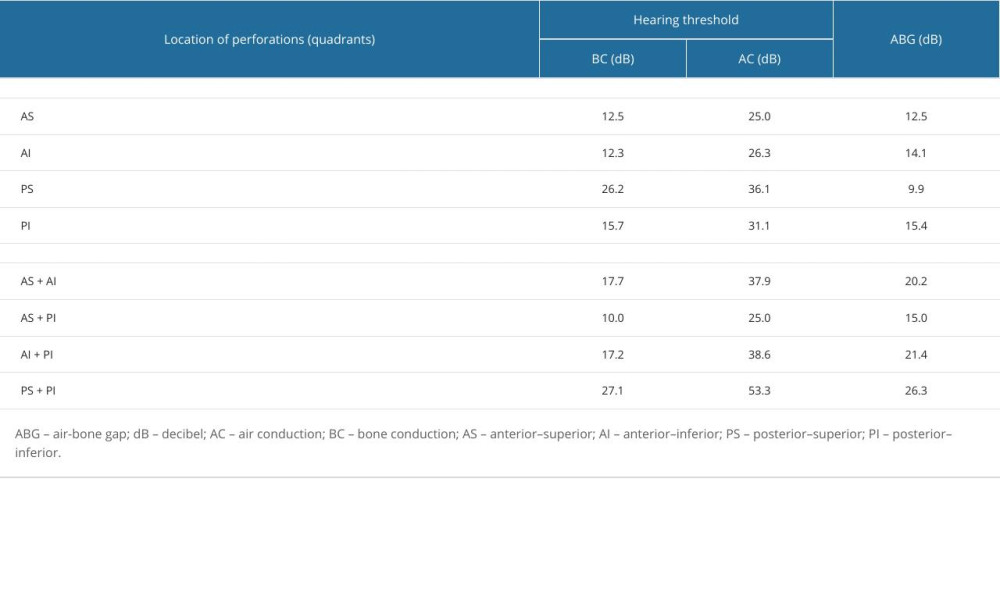 Table 4. Comparison of the site of the tympanic membrane perforation – air-bone gap values.
Table 4. Comparison of the site of the tympanic membrane perforation – air-bone gap values.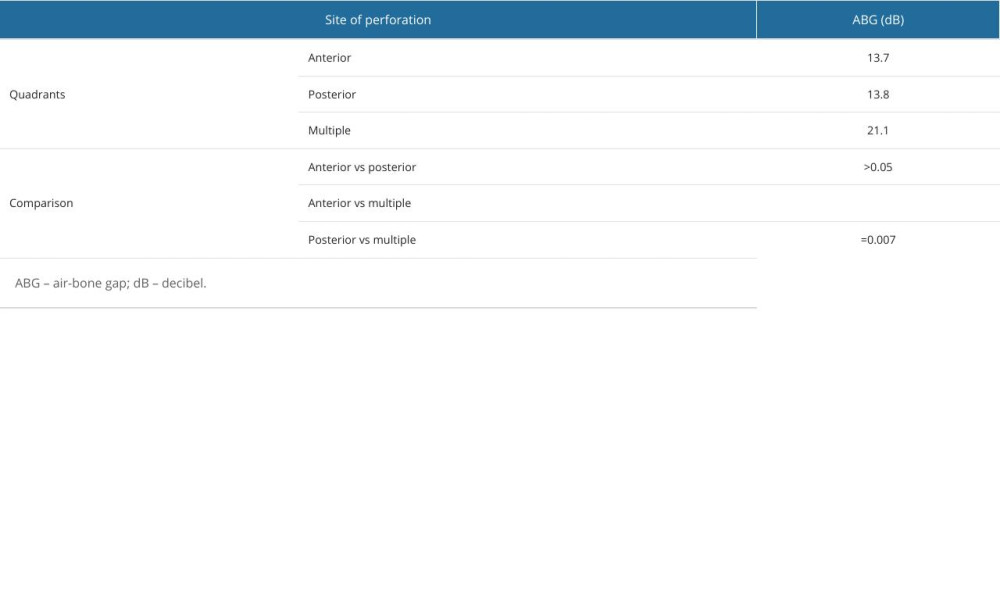 Table 5. Location of pathological lesions (in relation to middle ear structures)*.
Table 5. Location of pathological lesions (in relation to middle ear structures)*.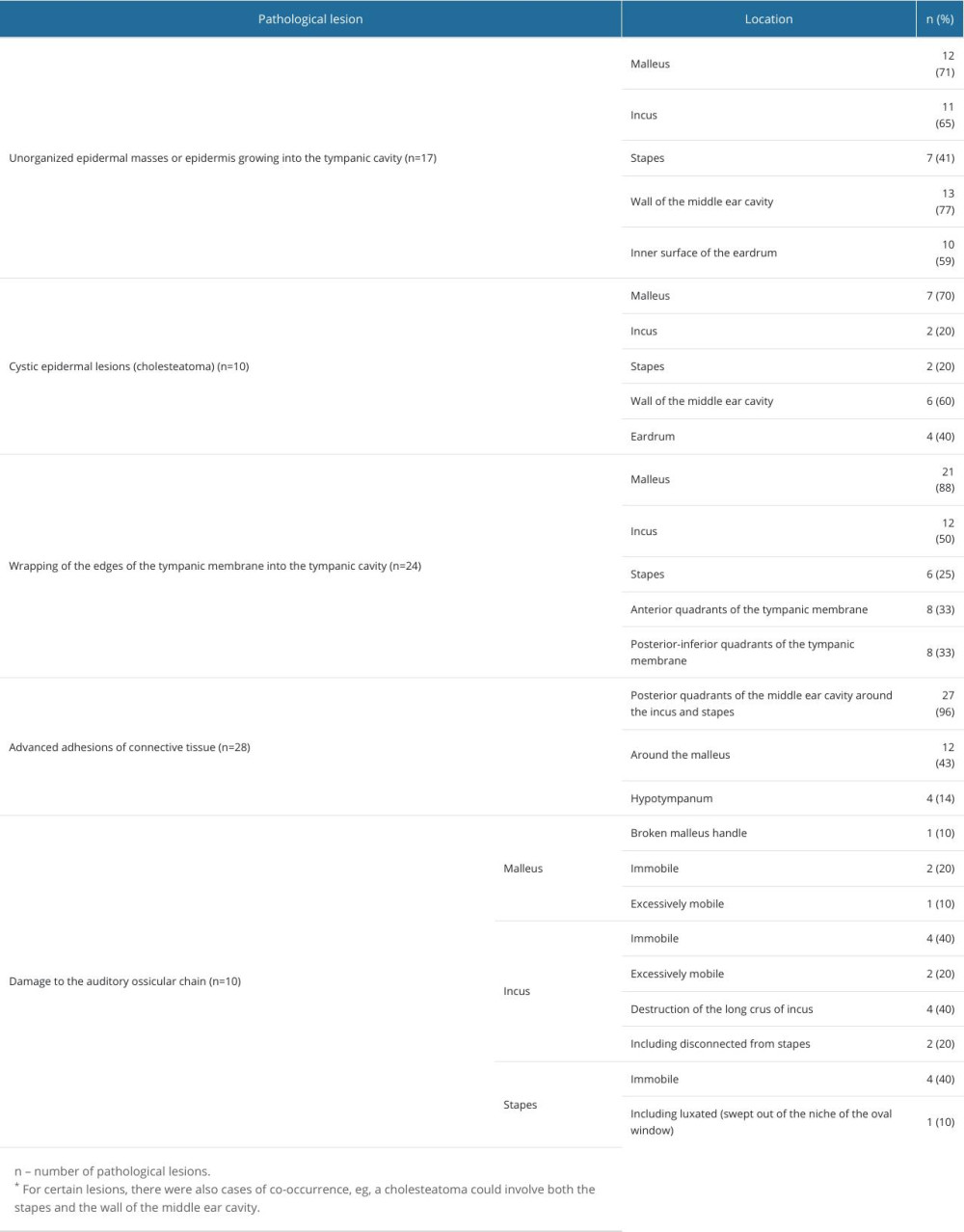 Table 6. Location of pathological lesions (in relation to quadrants).
Table 6. Location of pathological lesions (in relation to quadrants).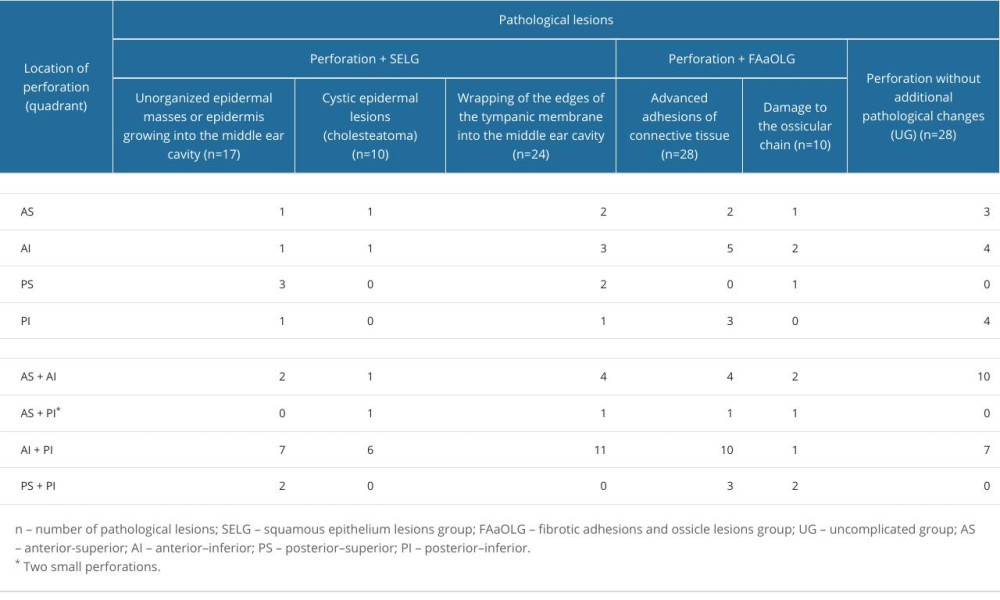
References
1. Balcerzyk D, Konflikt społeczny a konflikt zbrojny-formy jego przeciwdziałania: Zeszyty Naukowe/Wyźsza Szkoła Oficerska Wojsk Lądowych im gen T Kościuszki, 2012(1); 207-15 [in Polish]
2. Chandler CDW, Blast-related ear injury in current U.S. military operations: The ASHA Leader, 2006; 11(9); 8-29
3. Owens BD, Kragh JF, Wenke JC, Combat wounds in operation Iraqi Freedom and operation Enduring Freedom: J Trauma, 2008; 64(2); 295-99
4. Veterans Benefits Administration, Annual Benefits Report Fiscal Year 2010: VA.gov | Veterans Affairs, 2010 https://www.benefits.va.gov/REPORTS/abr/docs/2010_abr.pdf
5. Dougherty AL, MacGregor AJ, Han PP, Blast-related ear injuries among U.S. military personnel: J Rehabil Res Dev, 2013; 50(6); 893-904
6. , Veterans Benefits Administration Annual Benefits Report Fiscal Year 2013: VA.gov | Veterans Affairs, 2013 https://www.benefits.va.gov/REPORTS/abr/docs/2013_abr.pdf
7. Esquivel CR, Parker M, Curtis K, Aural blast injury/acoustic trauma and hearing loss: Mil Med, 2018; 183; 78-82
8. Holovach YO, Explosives and their compositions in the Russian-Ukrainian war: Bulletin of Kharkiv National University of Internal Affairs, 2004; 107(4); 137-50
9. Świętochowski N, Field Artillery in the defensive war of Ukraine 2022–2023. Part II. Methods of task implementation: Scientific Journal of the Military University of Land Forces, 2024; 211(1); 57-76
10. Barylyak R, Horoliuk D, Chervan I, Skarzynski PH, Treatment of ear trauma within the Ukrainian military: Organisational requirements and implementation of a three-stage regimen: BMJ Mil Health, 2024 [Online ahead of print]
11. : Росіяни щодня скидають понад 100 КАБів на позиції ЗСУ May 26, 2024, UAZMI [in Ukrainian]https://uazmi.org/news/post/a13e05a1be1bc0d12e1243c1cb7dae39
12. Kuczyńska B, Kukfisz S, Mechanizmy urazów powybuchowych wśród ofiar terrorystycznych ataków bombowych: Materiały Wysokoenergetyczne, 2011; T.3; 136-43 [in Polish]
13. Qureshi T, Awan MS, Hassan N, Effects of bomb blast injury on the ears: The Aga Khan University Hospital experience: J Pak Med Assoc, 2017; 67(9); 1313-17
14. Moloney J, Welch M, Cardinal A, Applied pathophysiology of blast injuries: Journal of High Threat and Austere Medicine, 2019; 1(1); 1-15
15. Bukowski J, Nowadly CD, Schauer SG, High risk and low prevalence diseases: Blast injuries: Am J Emerg Med, 2023; 70; 46-56
16. Jorolemon MR, Lopez RA, Krywko DM, Blast injuries: StatPearls, 2024, StatPearls Publishing http://www.ncbi.nlm.nih.gov/books/NBK430914/
17. Dolhi N, Weimer AD, Tympanic membrane perforation: StatPearls [Internet], 2025, Treasure Island (FL), StatPearls Publishing
18. Horrocks CL, Blast injuries: Biophysics, pathophysiology and management principles: J R Army Med Corps, 2001; 147(1); 28-40
19. Kerr AG, Byrne JE, Surgery of violence. IV. Blast injuries of the ear: Br Med J, 1975; 1(5957); 559-61
20. Wolf M, Kronenberg J, Ben-Shoshan J, Roth Y, Blast injury of the ear: Mil Med, 1991; 156(12); 651-53
21. Singer M: Otologic blast injuries. Dissertations, theses, and capstone projects Published online May 1, 2018
22. Kronenberg J, Ben-Shoshan J, Wolf M, Perforated tympanic membrane after blast injury: Am J Otol, 1993; 14(1); 92-94
23. Pahor AL, The ENT problems following the Birmingham bombings: J Laryngol Otol, 1981; 95(4); 399-406
24. Ritenour AE, Wickley A, Ritenour JS, Tympanic membrane perforation and hearing loss from blast overpressure in Operation Enduring Freedom and Operation Iraqi Freedom wounded: J Trauma, 2008; 64(2 Suppl); S174-78 discussion S178
25. Shah A, Ayala M, Capra G, Otologic assessment of blast and nonblast injury in returning Middle East-deployed service members: Laryngoscope, 2014; 124(1); 272-77
26. Sprem N, Branica S, Dawidowsky K, Tympanoplasty after war blast lesions of the eardrum: Retrospective study: Croat Med J, 2001; 42(6); 642-45
27. Keller M, Sload R, Wilson J, Tympanoplasty following blast injury: Otolaryngol Head Neck Surg, 2017; 157(6); 1025-33
28. Song SA, Sridhara SK, Littlefield PD, Tympanoplasty outcomes for blast-induced perforations from Iraq and Afghanistan: Otolaryngol Head Neck Surg, 2017; 156(2); 353-59
29. Plichta L, Dabkowska A, Wawszczyk-Frohlich S, Titanium prostheses for treating posttraumatic ossicular chain disruption: J Int Adv Otol, 2022; 18(5); 411-14
30. Garth RJ, Blast injury of the auditory system: A review of the mechanisms and pathology: J Laryngol Otol, 1994; 108(11); 925-29
31. Cho SI, Gao SS, Xia A, Mechanisms of hearing loss after blast injury to the ear: PLoS One, 2013; 8(7); e67618
32. Barylyak R, Kołodziejak A, Czaplicka E, Problemy otologiczne spowodowane eksplozją – przegląd piśmiennictwa: Nowa Audiofonologia, 2024; 13(4); 20-26 [in Polish]
33. Cave KM, Cornish EM, Chandler DW, Blast injury of the ear: Clinical update from the global war on terror: Mil Med, 2007; 172(7); 726-30
34. Oleksiak M, Smith BM, St Andre JR, Audiological issues and hearing loss among Veterans with mild traumatic brain injury: J Rehabil Res Dev, 2012; 49(7); 995-1004
35. Gao T, Li X, Hu J, Management of traumatic tympanic membrane perforation: A comparative study: Ther Clin Risk Manag, 2017; 13; 927-31
36. Jafarov S, İNan S, Büyüklü AF, Durukan E, Effect of small tympanic membrane perforations on hearing: KBB ve BBC Dergisi, 2019; 27(1); 22-26
37. Greenberg SL, Shipp D, Lin VY, Cochlear implantation in patients with bilateral severe sensorineural hearing loss after major blunt head trauma: Otol Neurotol, 2011; 32(1); 48-54
38. Cywka KB, Skarzynski PH, Krol B, Evaluation of the Bonebridge BCI 602 active bone conductive implant in adults: efficacy and stability of audiological, surgical, and functional outcomes: Eur Arch Otorhinolaryngol, 2022; 279(7); 3525-34
39. Ciorba A, Skarżyński PH, Gocmenler H, Hatzopoulos S, Advances in pediatric and adult cochlear implant and middle ear prostheses: J Clin Med, 2021; 10(14); 3152
40. : Інтерв’ю Президента України Володимира Зеленського німецькому телеканалу January 29, 2024, ARD [in Ukrainian]https://www.youtube.com/watch?v=NnH75tFS96o
41. Kennedy KL, Singh AK, Middle ear cholesteatoma: StatPearls, 2024, StatPearls Publishing http://www.ncbi.nlm.nih.gov/books/NBK448108/
42. Kuo CL, Etiopathogenesis of acquired cholesteatoma: Prominent theories and recent advances in biomolecular research: Laryngoscope, 2015; 125(1); 234-40
43. Okpala N, Management of blast ear injuries in mass casualty environments: Mil Med, 2011; 176(11); 1306-10
44. Yu Y, Huang J, Tang X, Exposure to blast shock waves via the ear canal induces deficits in vestibular afferent function in rats: J Otol, 2020; 15(3); 77-85
45. Bien AG, Jiang S, Gan RZ, Real-time measurement of stapes motion and intracochlear pressure during blast exposure: Hear Res, 2023; 429; 108702
46. Jensen JH, Bonding P, Experimental pressure induced rupture of the tympanic membrane in man: Acta Otolaryngol, 1993; 113(1); 62-67
47. Nafis AAM, Hossan MdA, Islam MdA, Mamun AA, Correlation of hearing loss with the site and size of tympanic membrane perforation: SAS J Surg, 2022; 8(10); 641-48
48. Aneesa M, Siraj S, Ali A, Correlation of tympanic membrane perforations with hearing loss: International Journal of Otorhinolaryngology and Head and Neck Surgery, 2019; 5(5); 1213-16
49. Sood AS, Pal P, Kumar A, Tympanic membrane perforation: Correlation of hearing loss with its site and size: International Journal of Otorhinolaryngology and Head and Neck Surgery, 2018; 4(2); 397-402
50. Rafique M, Farrukh MS, Shaikh AA, Assessment of hearing loss in tympanic membrane perforation at tertiary care hospitals: Journal of Liaquat University of Medical and Health Sciences, 2014; 13(01); 32-36
51. Mehta RP, Rosowski JJ, Voss SE, Determinants of hearing loss in perforations of the tympanic membrane: Otol Neurotol, 2006; 27(2); 136-43
Figures
Figure 1. A typical C-shaped central perforation of the tympanic membrane, similar to a “kidney bean” shape but ripped fragment of the tip of the malleus handle wrapped in the tympanic membrane, including on the inner side. A cholesteatoma formed in the area of the auricle. The lower edge of the perforation is smooth, thickened, with possible downward wrapping of membrane fragments.Figure 2. Post-explosive perforation of the tympanic membrane on the first day after injury. Perforation involves all quadrants. The remaining tympanic membrane was hemorrhaged. Fragments of tympanic membrane are wrapped around the handle of the malleus. Tables
Table 1. Sociodemographic and clinical data of the patients*.Table 2. Pre- and postoperative mean pure-tone audiometry hearing results.Table 3. Results of pure-tone audiometry in relation to perforation of the tympanic membrane in 1 vs 2 quadrants.Table 4. Comparison of the site of the tympanic membrane perforation – air-bone gap values.Table 5. Location of pathological lesions (in relation to middle ear structures)*.Table 6. Location of pathological lesions (in relation to quadrants).Table 1. Sociodemographic and clinical data of the patients*.Table 2. Pre- and postoperative mean pure-tone audiometry hearing results.Table 3. Results of pure-tone audiometry in relation to perforation of the tympanic membrane in 1 vs 2 quadrants.Table 4. Comparison of the site of the tympanic membrane perforation – air-bone gap values.Table 5. Location of pathological lesions (in relation to middle ear structures)*.Table 6. Location of pathological lesions (in relation to quadrants). In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387