29 April 2023: Database Analysis
Clinical Course of 53 Previously Vaccinated Patients Admitted to the National Hospital in Warsaw, Poland with COVID-19 Between November 2021 and March 2022
Artur Zaczyński1AB, Michał Hampel1AB, Paweł Piątkiewicz2AB*, Jacek Nasiłowski3AB, Sławomir Butkiewicz2AB, Urszula Religioni4DEF, Agnieszka Barańska5CD, Maria MalmDOI: 10.12659/MSM.939841
Med Sci Monit 2023; 29:e939841






Abstract
BACKGROUND: Current vaccines against SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) and vaccine booster programs aim to reduce hospitalizations due to severe COVID-19 (coronavirus disease 2019). It is now accepted that vaccination does not completely prevent infection and that breakthrough COVID-19 does occur. This study included 53 vaccinated patients who were hospitalized at a single center in Poland with breakthrough COVID-19 and aimed to evaluate the factors associated with their clinical course.
MATERIAL AND METHODS: This study covered the period 26 November 2021 to 11 March 2022. All patients had been vaccinated against COVID-19 with one of the following 4 vaccines: the mRNA-1273 (Moderna) mRNA vaccine (Spikevax); the BNT162b2 (Pfizer-BioNTech) mRNA vaccine (nucleoside-modified) (Comirnaty); the Ad26.COV2.S (Janssen/J0ohnson & Johnson) recombinant vaccine (Jcovden); and the AZD1222 (ChAdOx1) (Oxford/AstraZeneca) recombinant vaccine (Vaxzevria).
RESULTS: The course of COVID-19 in vaccinated patients was relatively similar. The patients vaccinated more than 24 weeks earlier rarely needed a stay in the Intensive Care Unit (ICU) (P=0.021), and the occurrence of deaths was significantly lower in this group (P=0.046). Women remained in hospital considerably longer than men (P=0.011). Age and comorbidities did not affect the course of this infection.
CONCLUSIONS: Despite the many advantages of the COVID-19 vaccination, our observations indicate a potential risk of infection after vaccination. The assessment of the course of COVID-19 in vaccinated patients gives the possibility to compare different vaccines and indicate factors that can reduce immunity.
Keywords: COVID-19 Vaccines, Hospital Mortality, Vaccination, Male, Humans, Female, Poland, Ad26COVS1, BNT162 Vaccine, ChAdOx1 nCoV-19, COVID-19, SARS-CoV-2, Hospitalization, Hospitals
Background
Since the first case was diagnosed in China, COVID-19 has rapidly spread throughout the world [1]. COVID-19 is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Since the onset of the epidemic, more than 582 million confirmed cases of COVID-19 and 6.41 million deaths have been reported globally (as of 5 August 2022) [2].
As of 5 August 2022, more than 6.08 million people in Poland have been infected with COVID-19, and 117 000 have died [3]. Subsequent SARS-CoV-2 variants that appear in populations raise many clinical concerns [4]. For this reason, the development of a safe and effective vaccine against COVID-19 aroused great global interest and hopes for public health protection [5]. The World Health Organisation (WHO) considers vaccines against COVID-19 as the most effective method to fight this disease [6]. The WHO has approved 9 vaccines against COVID-19: 2 RNA, Moderna (mRNA-1273) and Pfizer/BioNTech (BNT162b2); 3 non-replicating viral vectors, Janssen (Johnson & Johnson) (Ad26.COV2.S), Oxford/AstraZeneca (AZD1222), and Serum Institute of India Covishield (Oxford/AstraZeneca formulation); 2 protein subunits (NVX-CoV2373 and NovaVax); and inactivated virus techniques, Sinopharm (Beijing) BBIBP-CorV (Vero Cells) and Sinovac (CoronaVac) [7]. The vaccines against COVID-19 available in Poland are: the mRNA-1273 (Moderna) mRNA vaccine (Spikevax); the BNT162b2 (Pfizer-BioNTech) mRNA vaccine (nucleoside-modified) (Comirnaty); the Ad26.COV2.S (Janssen/Johnson & Johnson) recombinant vaccine (Jcovden); the AZD1222 (ChAdOx1) (Oxford/AstraZeneca) recombinant vaccine (Vaxzevria), and since 1 March 2022, Nuvaxovid (Novavax) [8]. Apart from the Janssen vaccine, in the basic dosage scheme all the vaccines required 2 doses administered at different time intervals (depending on the vaccine). Since autumn 2021, the third dose of the vaccine against COVID-19 has been authorized in Poland for people vaccinated at least 6 months earlier. Currently, the second booster dose (the fourth in the entire vaccination scheme) is available for people over 60 years of age, and people over 12 years of age with immune disorders who received all basic vaccines and the first booster dose against COVID-19 [9].
Data from randomized clinical studies and observational studies conducted in real time prove that COVID-19 vaccines currently approved for use are safe and effective in preventing serious consequences, hospitalization, and deaths caused by COVID-19 [10]. To achieve herd immunity, at least 60–70% of the population would have to get vaccinated [11,12]. In Poland, 59.4% of the population have been fully vaccinated (2 doses, as of 5 August 2022) [13].
The effectiveness of the vaccines in different groups of patients was assessed by teams all over the world. This data shows a high level of short-term protection of the vaccines against COVID-19 [14]. In the longer term, the results are not evident and indicate, for example, waning vaccine effectiveness several months after vaccination, namely in those aged 65 years or over [10,15], which can be associated with the variability of the virus and the different prevention policies in particular countries [16,17].
Considering the above, the basic objective of this study was to determine the course of COVID-19 in patients vaccinated with one of the vaccines available in Poland, to assess the influence of the type of vaccine on the severity of COVID-19, and to assess the impact of sex, age, and comorbidities. Therefore, this study included 53 vaccinated patients who were hospitalized at a single center in Poland with breakthrough COVID-19 and aimed to evaluate the factors associated with their clinical course.
Material and Methods
SETTING AND METHODS:
Data were collected at the National Hospital in Warsaw (Poland) in the period between 26 November 2021 and 11 March 2022 using the Clininet system (
The National Hospital was a temporary hospital arranged at the National Stadium in October 2020 by the Central Clinical Hospital of the Ministry of Interior and Administration to treat patients infected with COVID-19.
MATERIAL:
Our study included all 53 patients hospitalized due to COVID-19 at that time and fully vaccinated with any vaccine approved in Poland. Each patient had a positive RT-PCR test for SARS-CoV-2 conducted in the hospital. At that time, only the alpha variant of the coronavirus was present and detected in Poland. We defined full vaccination as an administration of at least 2 doses of the Pfizer, Moderna, or AstraZeneca vaccines, or 1 dose of the Jenssen vaccine. The analysis included the test results of all patients present in the hospital at that time, and thus the selection of patients was based on availability.
STATISTICAL ANALYSIS:
Statistical analysis was performed with the StatSoft, Inc. (2014) statistic software package, STATISTICA (data analysis software system Cracow, Poland), version 12.0,
Results
CHARACTERISTICS OF THE STUDY GROUP:
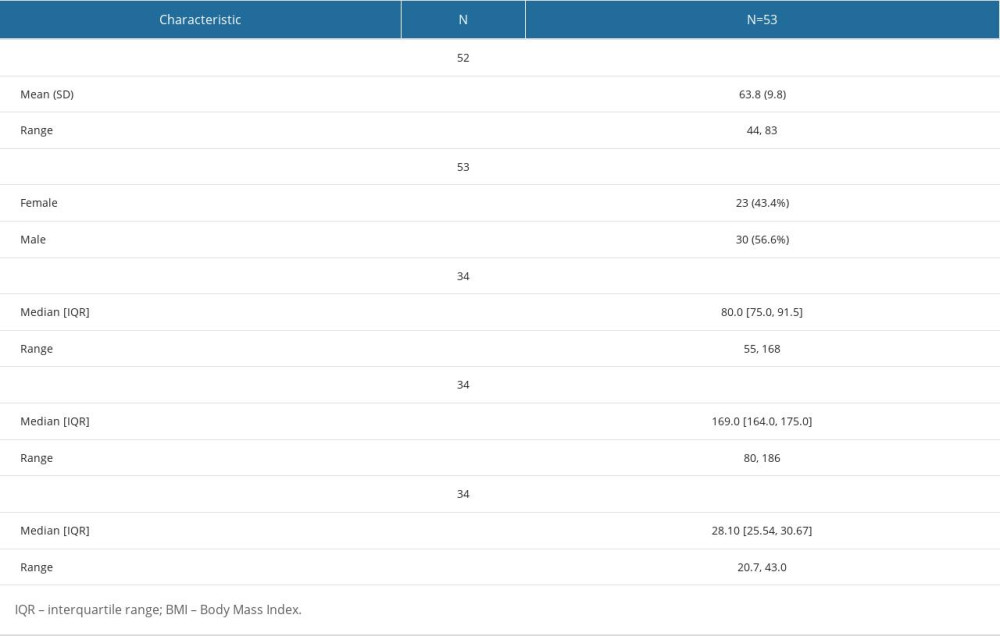
The analysis comprised 53 patients. The mean age of the patients was 63.8±9.8 years; the youngest was 44, and the oldest was 83 years old. The percentage of men was slightly higher than women (56.6% vs 43.4%, respectively). BMI of the patients ranged from 20.7 to 43, and half of the patients had BMI of 28.10 or higher. Demographic characteristics of the patients are presented in Table 1.
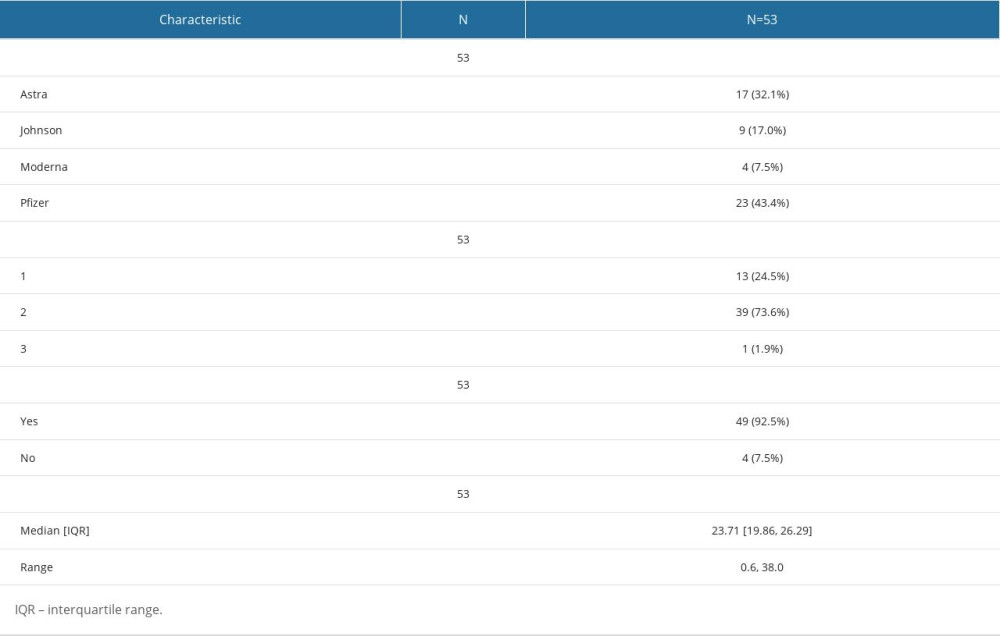
All the patients were vaccinated against COVID-19 caused by SARS-CoV-2, of which 43.4% were vaccinated with the Pfizer vaccine, 32.1% with AstraZeneca, 17.0% with Moderna, and 7.5% with Johnson. The vast majority of the patients received 2 doses (73.6%), 1 dose (24.5%), and 1 patient had 3 doses; 92.5% of the patients were fully vaccinated (received at least 1 dose of the Johnson vaccine or at least 2 doses of the AstraZeneca, Moderna, or Pfizer vaccine). The period between the last dose of the vaccine and diagnosis of infection was 0.6–38 weeks, and was at least 23.71 weeks in half of the patients (Table 2).
There were practically no addictions among the patients. Their comorbidities included hypertension (62.3%), diabetes (28.2%), hypothyroidism (18.9%), atherosclerosis (17%), autoimmune diseases (17%), cancer (13.2%), and asthma/COPD (5.7%).
Hospitalization of the patients infected with COVID-19 lasted from 1 to 33 days, and half of the patients were hospitalized for 11.5 days or longer. Nearly one-fifth of the patients (18.9%) had to stay in the ICU for 8.5±4.0 days on average, and 17% of the hospitalized patients died.
Regarding data on the vital signs and condition of the patients infected with COVID-19 on admission, the average heart rate was 87.7±14.7 beats per minute, the average systolic blood pressure was 135.4±21.3 mmHg, and the average diastolic blood pressure was 80.7±13.3 mmHg. The third quartile for temperature was 37.70°C, which indicates that the vast majority of the patients did not have a high temperature on admission. During O2 supplementation, half of the patients had an oxygen saturation of 94% or lower, and an oxygen partial pressure of 44.95 mmHg or lower.
On admission, one-third of the COVID-19 patients received oxygen therapy in the form of a nasal canula (34%), and more than one-fourth used a non-rebreather mask (28.3%). Simple oxygen masks and NIV (non-invasive ventilation) were used less frequently (9.4% and 1.9%, respectively), and one-fourth of the patients were not given oxygen therapy upon admission. Computed tomography revealed lung involvement ranging from 0% to 80%, with at least 30% in half of the patients.
During hospitalization, 62.3% of the patients experienced worsening of their condition and required a more invasive form of oxygen therapy, and 7.5% of the patients improved; 30.2% of the patients did not require a change in oxygen therapy. During hospitalization, 13.2% of the COVID-19 patients did not require oxygen therapy, which was significantly less compared to 26.4% on admission. Nasal cannulas (20.8% vs 34%) and non-rebreather masks (24.5% vs 28.3%) were less frequently used, and simple oxygen masks (13.2% vs 9.4%), high-flow oxygen therapy (7.5% compared to 0%), NIV (9.4% vs 1.9%), and respiratory therapy (11.3% vs 0%) were more frequent.
Regarding medications administered during hospitalization, the vast majority of the COVID-19 patients were given Dexaven/Demezon (81.1%) and heparin (94.3%), while Olumiant (11.3%) and Remdesivir (11.3%) were less common.
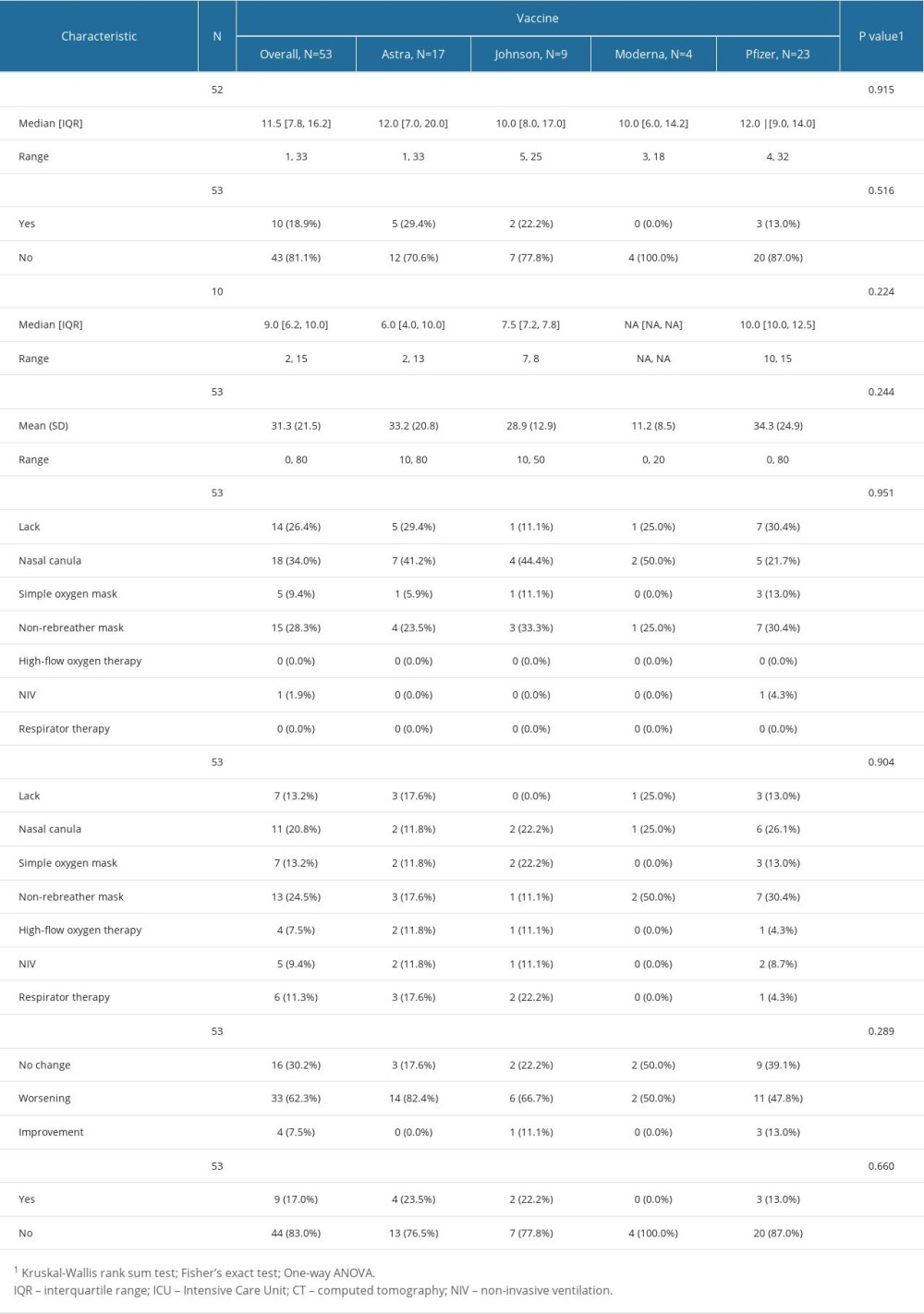
SEVERITY OF INFECTION VS TYPE OF VACCINE:
No significant influence of the type of vaccine on the severity of the infection was shown (Table 3). Patients who had been administered the Pfizer vaccine stayed slightly longer in the ICU, and the lowest percentage of lung involvement was recorded in the patients vaccinated with the Moderna vaccine. It was also noted that the patients who had been given the Moderna vaccine were more likely to experience respiratory deterioration and require changing the intensity of oxygen therapy. These outcomes were not statistically significant. The logistic regression analysis revealed that the patients vaccinated with the Pfizer vaccine were significantly less likely to experience respiratory deterioration than those who had received the AstraZeneca vaccine (OR=0.196; 95% CI: 0.0375–0.799; P=0.032).
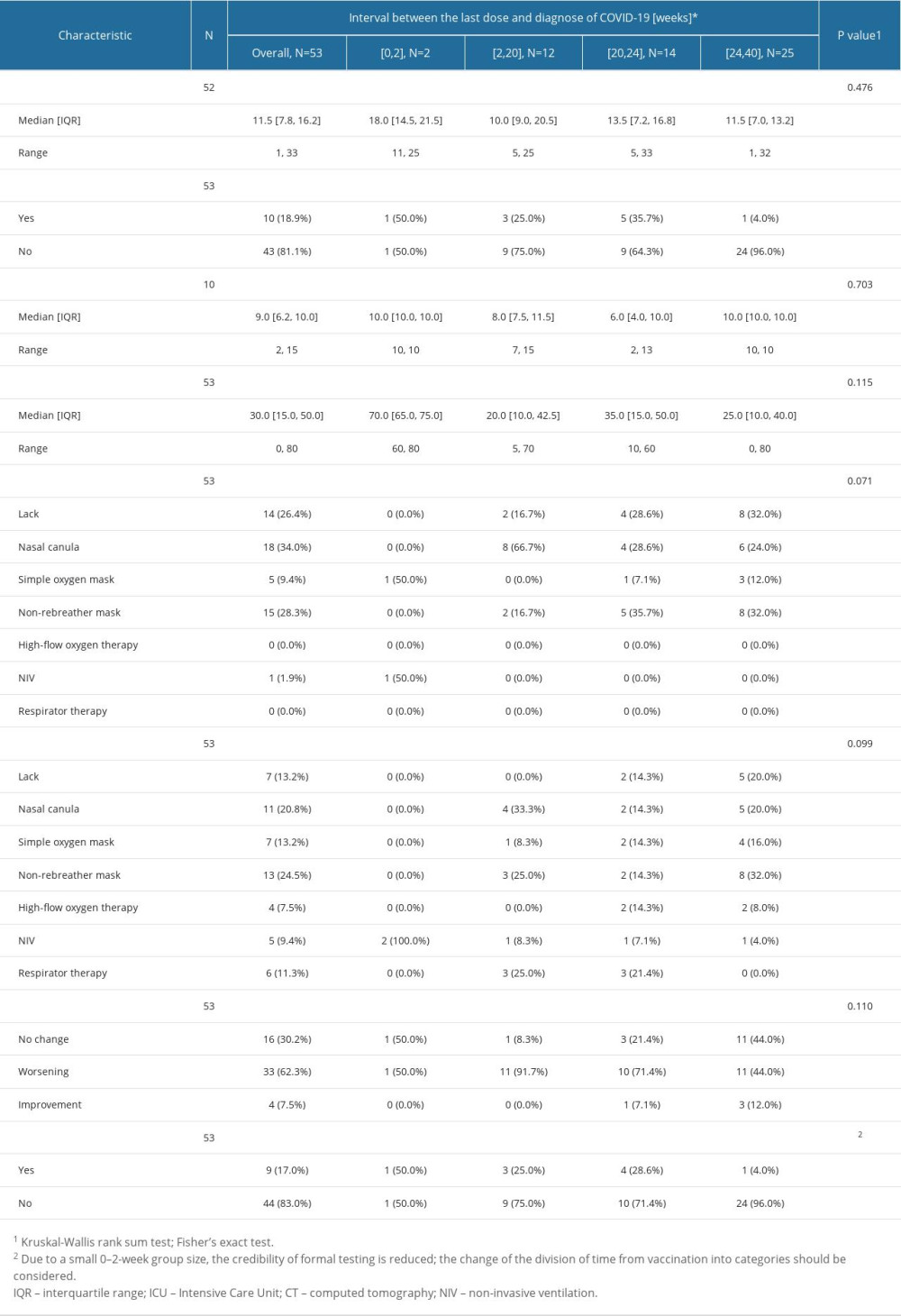
EFFECT OF TIME BETWEEN VACCINATION AND DIAGNOSIS OF INFECTION:
Patients vaccinated more than 24 weeks earlier were by far the least likely to require a stay in the ICU (P=0.021), and deaths were also significantly less frequent in this group (P=0.046). Respiratory deterioration and the resulting need to increase the intensity of oxygen therapy were most often observed in patients who had been vaccinated between 2 and 20 weeks earlier, but the result of the Fisher’s exact test was not statistically significant (P=0.110). The impact of time on the severity of the infection is presented in Table 4.
EFFECT OF AGE, SEX, AND COMORBIDITIES ON COURSE OF COVID-19:
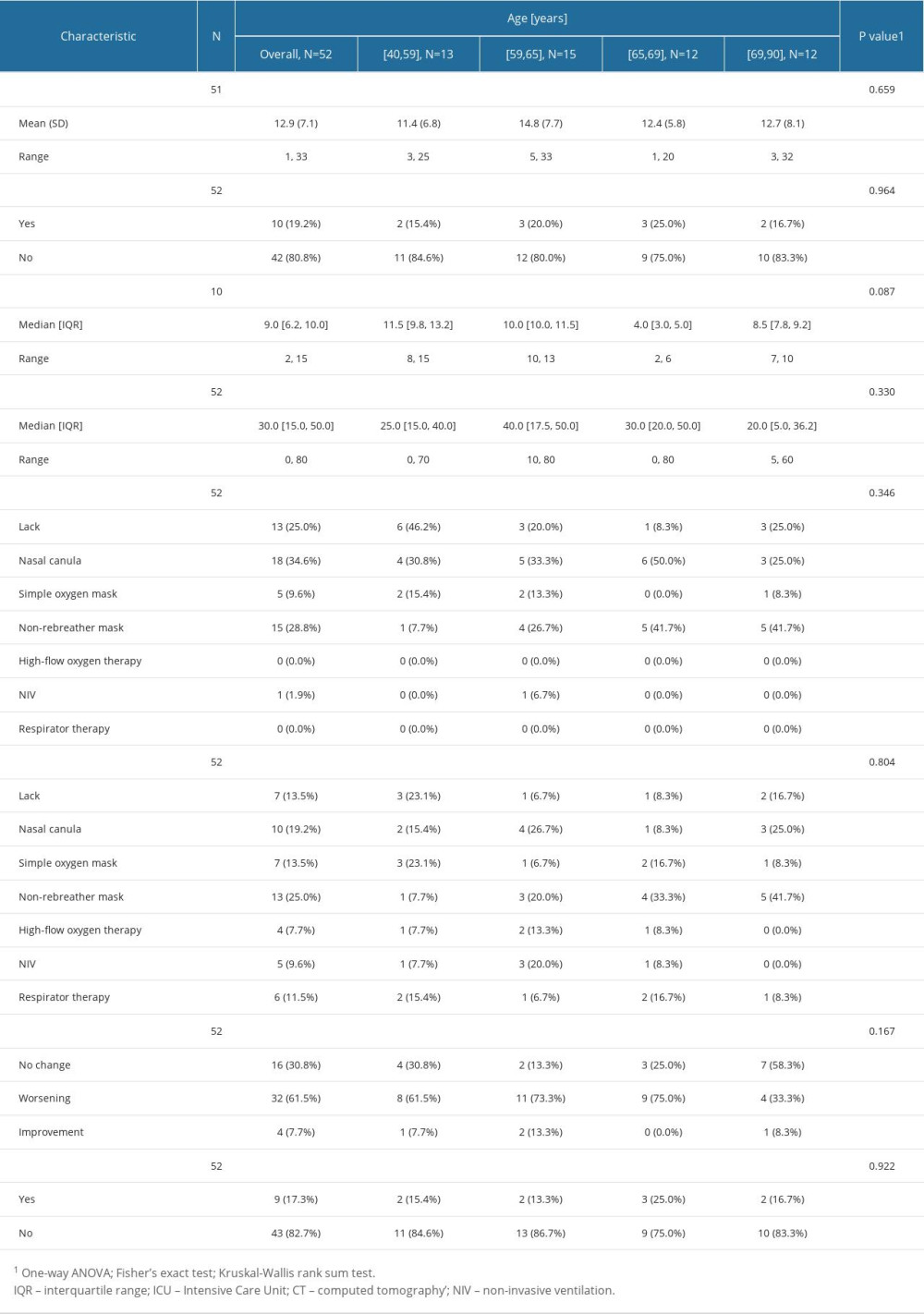
No significant influence of age on the severity of COVID-19 was found (Table 5). The length of a stay in the ICU was slightly shorter in patients aged 65–69, and the change of oxygen therapy due to respiratory deterioration was the least frequent in the patients aged more than 69, who were more likely to have no changes in oxygen therapy compared to others. The differences were not statistically significant.
Statistical analysis showed that women remained in hospital considerably longer than the men (
Practically no significant influence of comorbidities on the severity of COVID-19 was recorded. Patients with hypertension were significantly more likely to need a non-rebreather mask during oxygen therapy (42.4% vs 5%), yet the simple oxygen mask (3% compared to 20%) and nasal canula (27.3% vs 45%) were considerably less frequently used (
Discussion
This study, including 53 patients hospitalized in the National Hospital in Warsaw, Poland, shows that the various vaccines against COVID-19 have a similar influence on the course of this disease. Slight differences were observed in the length of a stay in the ICU (slightly longer in the case of the Pfizer vaccine), the degree of lung involvement (lowest in patients vaccinated with the Moderna vaccine), and respiratory function (lowest risk of respiratory deterioration in the patients who received the Pfizer vaccine).
The time from vaccination had a significant impact on ICU stay and risk of death, which were least frequent in patients vaccinated at least 24 weeks before becoming infected. It was also observed that women had a longer hospitalization. This effect was very slight in the case of age, and was not noted in terms of comorbidities.
Current studies directly indicate that the advantages of COVID-19 vaccines outweigh the risk, despite rare serious adverse effects [18,19]. Not only do vaccinations influence the frequency of infection, but also deaths and severity of infection [7,16]. Fiolet et al [18] found a similar efficacy of vaccines; the efficacy of the mRNA vaccine against hospitalization and death was 87–94%. Ghazy et al report that inactivated COVID-19 vaccine (CoronaVac) is safe in the case of hospitalization (87.5%) and death (86.3%). Similar results were observed in elderly people, which confirms similar efficacy of vaccines [7].
Studies conducted to date have not produced unequivocal evidence [5,14,19–22], and their authors indicate many determinants that influence the final outcomes of vaccinations. Although all the vaccines against COVID-19 were highly effective against the original strain, these effects are currently different due to the consequences of the variants of the virus [18].
Studies indicate reduced effectiveness of the vaccines in relation to hospitalization due to COVID-19 variants, and link this effect to an increase in the prevalence of Delta variant infections. Rosenberg et al found that the COVID-19 vaccines were highly effective against hospitalization (VE > 90%) in fully vaccinated patients, even in the period with an increased occurrence of the Delta variant [10], while non-vaccinated persons were more often hospitalized at that time. These differences have also been noted in other studies [23].
Studies also revealed reduced immunity over time since vaccination. For example, a study carried out in the United States indicated that 3 months after vaccination, the greatest decreases in the effectiveness of the vaccines were observed among patients vaccinated with the Pfizer BNT162b2 vaccine. The effectiveness of vaccines against hospitalization due to COVID-19 remains high. The lowest effectiveness against hospitalization was observed among people over age 65 and those vaccinated with the Janssen Ad26.COV2.S vaccine. Higher effectiveness against COVID-19 was observed in recently vaccinated people, particularly in the case of the Moderna mRNA-1273 vaccine [17].
Other studies confirm that a severe course of COVID-19 after vaccination occurs mainly in elderly populations, especially among people living in long-term care facilities [24,25]. Andrews et al also reported that reduced effectiveness of vaccines seems to be more likely among extremely clinically vulnerable elderly people [26]. In turn, the study by Wang et al showed an increased risk of infection in vaccinated cancer patients, especially those undergoing active cancer care, which was associated with a significant risk of hospitalization and mortality [27]. The formulation may also be important, with some studies indicating that a more severe course was reported in those who had received the Pfizer BNT162b2 vaccine [24,25]. Another study shows reduced effectiveness of the Moderna vaccine against the Delta [28] variant, similar to other studies [29].
An English study confirmed that protection against hospitalization and death due to COVID-19 remains at a high level for at least 20 weeks after receiving the second dose (the analysis comprised Pfizer and AstraZeneca vaccines) [21], but a decreased protection against infection was observed after 6 months. The effect of time is unclear. Some studies reported minimally decreased effectiveness of the vaccines over time, while others showed significant changes (protection reduction by >25%) [18,30]. A study by Andrews et al provided evidence of waning post-vaccination protection against symptomatic infection, but with protection against hospitalization and death remaining at a high level for at least 20 weeks after the second dose [14].
Summing up, the COVID-19 pandemic has changed since the development of the vaccines, which has been reflected in the severe courses and deaths, especially in patients over the age of 60 [31].
The analysis of studies indicates that reduced effectiveness of the vaccines over time has 3 potential explanations: it reflects lower effectiveness of a vaccine against a new variant, is a sign of real immunodeficiency due to a loss of immune protection, and bias of the studies [18,29].
The US Centers for Disease Control and Prevention indicate that real-world effectiveness of vaccines can be influenced by several factors, including host population factors (eg, those who were not included in clinical studies), viral factors (eg, variants), and program/political factors (eg, adhering to dosage schemes or storage/handling of the vaccines) [32].
The effectiveness of booster doses of the vaccines against COVID-19 has been emphasized. For example, a study by Bard et al showed that a booster dose increased the effectiveness of vaccines compared to people who received only the first series [33].
Like all studies, this also has some limitations. First, it comprised a relatively small group of patients hospitalized in a single facility. In addition, we assessed patients in a very short time interval. At the planning stage of the study, we did not take into account the interval between the vaccine and the disease, which may also have affected the results. Currently, the administration of the fourth dose of the vaccines to patients may also impact the outcomes.
Conclusions
The vaccines are an effective tool for preventing a severe course, hospitalization, and death due to COVID-19. Despite using the vaccines, COVID-19 remains a considerable challenge for public health worldwide, with a potential risk of infection after vaccination. Our study, conducted on a group of several dozen patients hospitalized in a National Hospital in Poland showed a relationship between the interval since the last vaccination and the course of the disease. However, there were no significant relationships between the course of infection severity and comorbidities. Although our study shows a relatively similar course of COVID-19 in vaccinated persons, the variability of the virus variants and waning immunity can influence the severity of the course of this disease and the risk of death. Thus, monitoring the effectiveness of the vaccinations is essential in understanding the scale and source of the variability of their effectiveness. Identification of groups at risk of waning immunity is of great importance. These activities will impact the effectiveness of the vaccination coverage level, the change of public health policy, and recommendations regarding vaccinations.
References
1. Sultana J, Mazzaglia G, Luxi N, Potential effects of vaccinations on the prevention of COVID-19: Rationale, clinical evidence, risks, and public health considerations: Expert RevVaccines, 2020; 19; 919-36
2. : Daily new confirmed COVID-19 deaths per million people [cited 2022 May 22]. Available fromhttps://ourworldindata.org/explorers/coronavirus-data-explorer
3. : COVID-19 Data repository by the center for systems science and engineering (CSSE) at Johns Hopkins University [cited 2022 May 22]. Available from: https://github.com/CSSEGISandData/COVID-19
4. Forman R, Shah S, Jeurissen P, COVID-19 vaccine challenges: What have we learned so far and what remains to be done?: Health Policy, 2021; 125; 553-67
5. Hacisuleyman E, Hale C, Saito Y, Vaccine breakthrough infections with SARS-CoV-2 variants: N Engl J Med, 2021; 384(23); 2212-18
6. WHO: Coronavirus disease (COVID-19): Vaccines [cited 2022 Jul 14]. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/coronavirus-disease-(covid-19)-vaccines?adgroupsurvey={adgroupsurvey}&gclid=Cj0KCQjw_7KXBhCoARIsAPdPTfjiPTXEMz0EGBPPNCsDLXyivNhxV95HkUWbZn2m9MbpQ2wdDONvJjMaAljREALw_wcB
7. Ghazy RM, Ashmawy R, Hamdy NA, Efficacy and effectiveness of SARS-CoV-2 vaccines: A systematic review and meta-analysis: Vaccines (Basel), 2022; 10; 350
8. Szczepienia PZH [cited 2023 Feb 23]. Available from: [in Polish]https://szczepienia.pzh.gov.pl/wszystko-o-szczepieniach/lista-dostepnych-szczepionek/
9. Szczepienia PZH [cited 2023 Feb 23]. Available from: [in Polish]https://szczepienia.pzh.gov.pl/faq/kto-moze-zaszczepic-sie-czwarta-dawka-szczepionki-przeciw-covid-19/
10. Rosenberg ES, Holtgrave DR, Dorabawila V, A New COVID-19 cases and hospitalizations among adults, by vaccination status – New York, May 3–July 25, 2021: MMWR Morb Mortal Wkly Rep, 2021; 70; 1150-55
11. McDermott A, Core concept: Herd immunity is an important-and often misunderstood-public health phenomenon: Proc Natl Acad Sci USA May 25, 2021; 118(21); e2107692118
12. Kadkhoda K, Herd Immunity to COVID-19: Am J Clin Pathol, 2021; 155(4); 471-72
13. Our World in Data: Covid vaccinations [cited 2022 Jun 2]. Available from: https://ourworldindata.org/covid-vaccinations
14. Andrews N, Tessier E, Stowe J, Duration of protection against mild and severe disease by COVID-19 vaccines: N Engl J Med, 2022; 386; 340-50
15. Scobie HM, Johnson AG, Suthar AB, Monitoring incidence of COVID-19 cases, hospitalizations, and deaths, by vaccination status – 13 U.S. Jurisdictions, April 4–July 17, 2021: MMWR Morb Mortal Wkly Rep, 2021; 70; 1284-90
16. Rosenberg ES, Dorabawila V, Easton D, COVID-19 vaccine effectiveness in New York State: N Engl J Med, 2022; 386; 116-27
17. Pouwel KB, Pritchard E, Matthews PC, Effect of delta variant on viral burden and vaccine effectiveness against new SARS-CoV-2 infections in the UK: Nat Med, 2021; 27; 2127-35
18. Fiolet T, Kherabi Y, MacDonald CJ, Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review: Clin Microbiol Infect, 2022; 28; 202-21
19. Suleyman G, Fadel R, Brar I, Risk factors associated with hospitalization and death in COVID-19 breakthrough infections: Open Forum Infect Dis, 2022; 9(5); ofac116
20. Pritchard E, Matthews PC, Stoesser N, Impact of vaccination on new SARS-CoV-2 infections in the United Kingdom: Nat Med, 2021; 27; 1370-78
21. Lopez Bernal J, Andrews N, Gower C, Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on covid-19 related symptoms, hospital admissions, and mortality in older adults in England: Test negative case-control study: BMJ, 2021; 373; n1088
22. El-Shabasy RM, Nayel MA, Taher MM, Three waves changes, new variant strains, and vaccination effect against COVID-19 pandemic: Int J Biol Macromol, 2022; 204; 161-68
23. Lopez Bernal J, Andrews N, Gower C, Effectiveness of COVID-19 vaccines against the B.1.617.2 (Delta) variant: N Engl J Med, 2021; 385; 585-94
24. Grannis SJ, Rowley EA, Ong TC, Interim estimates of COVID-19 vaccine effectiveness against COVID-19-associated emergency department or urgent care clinic encounters and hospitalizations among adults during SARS-CoV-2 B.1.617.2 (Delta) variant predominance – nine states, June–August 2021: MMWR Morb Mortal Wkly Rep, 2021; 70; 1291-93
25. Nanduri S, Pilishvili T, Derado G, Effectiveness of Pfizer-BioNTech and Moderna vaccines in preventing SARS-CoV-2 infection among nursing home residents before and during widespread circulation of the SARS-CoV-2 B.1.617.2 (Delta) variant – National Healthcare Safety Network, March 1–August 1, 2021: MMWR Morb Mortal Wkly Rep, 2021; 70; 1163-66
26. Nanduri S, Pilishvili T, Derado G, Effectiveness of Pfizer-BioNTech and Moderna vaccines in preventing SARS-CoV-2 infection among nursing home residents before and during widespread circulation of the SARS-CoV-2 B.1.617.2 (Delta) variant-National Healthcare Safety Network, March 1-August 1, 2021: MMWR Morb Mortal Wkly Rep, 2021; 70; 1163-66
27. Wang W, Kaelber DC, Xu R, Berger NA, Breakthrough SARS-CoV-2 infections, hospitalizations, and mortality in vaccinated patients with cancer in the US between December 2020 and November 2021: JAMA Oncol, 2022; 8(7); 1027-34
28. Bruxvoort KJ, Sy LS, Qian L, Effectiveness of mRNA-1273 against delta, mu, and other emerging variants of SARS-CoV-2: Test negative case-control study: BMJ, 2021; 375; e068848
29. Chung H, He S, Nasreen S, Effectiveness of BNT162b2 and mRNA-1273 covid-19 vaccines against symptomatic SARS-CoV-2 infection and severe COVID-19 outcomes in Ontario, Canada: Test negative design study: BMJ, 2021; 374; n1943
30. Feikin DR, Higdon MM, Abu-Raddad LJ, Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: Results of a systematic review and meta-regression: Lancet, 2022; 399; 924-44
31. De-Leon H, Calderon-Margalit R, Pederiva F, First indication of the effect of COVID-19 vaccinations on the course of the COVID-19 outbreak in Israel: medRxiv, 2021; 2021; 21250630
32. Centers for Disease Control and Prevention: COVID-19 Vaccine effectiveness research [cited 2022 Jul 30]. Available from: https://www.cdc.gov/vaccines/covid-19/effectiveness-research/protocols.html
33. Barda N, Dagan N, Cohen C, Effectiveness of a third dose of the BNT162b2 mRNA COVID-19 vaccine for preventing severe outcomes in Israel: An observational study: Lancet, 2021; 398; 2093-100
In Press
Clinical Research
Institutional and Regional Variations in Access to Clinical Trials and Next-Generation Sequencing in Turkis...Med Sci Monit In Press; DOI: 10.12659/MSM.951027
Clinical Research
Low-Intensity Blood Flow-Restricted Multi-Joint Exercise Improves Muscle Function in Patients With Patellof...Med Sci Monit In Press; DOI: 10.12659/MSM.950516
Review article
Musculoskeletal Ultrasound and MRI in the Evaluation of Chemotherapy-Induced Peripheral Neuropathy: A ReviewMed Sci Monit In Press; DOI: 10.12659/MSM.951283
Clinical Research
Sensory Processing, Dissociation, and Affective Symptoms in Misophonia: A Cross-Sectional Study of 35 AdultsMed Sci Monit In Press; DOI: 10.12659/MSM.950938
Most Viewed Current Articles
17 Jan 2024 : Review article 10,187,196
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,708,487
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,341,643
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 706,524
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387