07 January 2021: Clinical Research
Comparison of CellSearch and Circulating Tumor Cells (CTC)-Biopsy Systems in Detecting Peripheral Blood Circulating Tumor Cells in Patients with Gastric Cancer
Dawei Ning1BCEF, Kai Cui2BC, Min Liu2D, Yang Ou3BCEF, Zhendan Wang4B, Benkui Zou5B, Yangyang Shen6B, Xinyang Lu7B, Sheng Li8AG*, Pang Li9ABDOI: 10.12659/MSM.926565
Med Sci Monit 2021; 27:e926565






Abstract
BACKGROUND: The purpose of this study was to compare circulating tumor cells (CTCs)/circulating tumor microemboli (CTM) detection rates of the CellSearch and CTC-Biopsy systems in patients with gastric cancer (GC). We also investigated potential correlations between clinicopathological characteristics and prognosis in patients with GC.
MATERIAL AND METHODS: This prospective study was conducted at the Shandong Institute of Cancer Prevention and Control in China. Fifty-nine patients with GC and 22 healthy volunteers were recruited and their peripheral blood samples were examined by the CTC-Biopsy system and CellSearch system for CTC.
RESULTS: The rate of detection of CTCs/CTM was significantly higher with the CTC-Biopsy system than with the CellSearch system (59.32% vs. 27.12%, P<0.001). The Kappa value was 0.179, indicating poor consistency. CTCs detected with the CellSearch system in patients with stage III/IV GC was significantly correlated with neutrophil count (P=0.020), neutrophil/lymphocyte ratio (N/L ratio) (P=0.009), CA19-9 (P=0.049), tumor size (P=0.026), and the extent of vascular invasion (P=0.007). CTCs detected with the CTC-Biopsy system correlated with tumor differentiation (P=0.010). CTM in patients with stage I/II GC and stage II/IV GC correlated with CEA (P=0.004) and tumor differentiation (P=0.030), respectively. A CTC count >3 detected with the CellSearch system, and not the CTC-Biopsy system, correlated with reduced progression-free survival and overall survival.
CONCLUSIONS: The CTC-Biopsy system was superior to the CellSearch system for detecting CTCs in GC patients. CTM were detected with the CTC-Biopsy system but not with the CellSearch system. CTCs detected with the CellSearch system correlated with various clinicopathological factors and long-term survival outcomes.
Keywords: Neoplastic Cells, Circulating, Aged, 80 and over, Biopsy, Cell Count, healthy volunteers, Multivariate Analysis, Progression-Free Survival, Stomach
Background
Gastric cancer (GC) is the fourth most common cancer worldwide and the third most common cause of tumor-related deaths [1]. GC is an aggressive tumor, as almost 50% of patients suffer from tumor recurrence or metastasis after curative resection. The 5-year survival rate is less than 30% [2,3].
Circulating tumor cells (CTCs) are the cells shed from a primary tumor into the peripheral blood [4]. With the help of adhesion molecules, CTCs can adhere to form circulating tumor microemboli (CTM) [5]. CTCs and CTM may be responsible for the development of distant metastases in patients with malignant tumors [6,7]. In a study of patients with advanced GC, the number of CTCs detected in the peripheral blood after 6 weeks of chemotherapy was associated with the rate of disease control (
To detect CTCs, it is important to first separate tumor cells from blood cells. One of the most widely used method for separation and detection of CTCs is the CellSearch system [11,12]. Another technique, which is based on the principle of filtration and isolation of tumor cells according to cell size, allows for the separation of CTCs and CTM from whole blood using a membrane filter [13]. Our research group has developed the novel CTC-Biopsy detection system based on this filtration principle. The CTC-Biopsy system can differentiate peripheral blood tumor cells from normal cells based on tumor cell diameter and capacity of deformation. A filtration membrane was used to increase the yield of CTCs from the whole blood sample.
In this study, we compared the CTC detection rates of the CellSearch and CTC-Biopsy systems. We also analyzed the relationships among CTC, clinicopathological features, and prognosis in patients with GC.
Material and Methods
PATIENT SELECTION:
In this prospective study, patients with GC who were admitted to Shandong Cancer Hospital and Institute from May 2014 to December 2014 and met the inclusion criteria were recruited for the study.
The inclusion criteria were age >18 years, pathological diagnosis of GC, treatment-naïve status, and good performance status allowing for subsequent treatment and blood collection. Patients with benign stomach lesions or other malignancies were excluded from the study, as were patients receiving antitumor treatment.
During the same period, 22 healthy volunteers (age >18 years) were included as the negative controls, whose routine blood parameters, liver biochemistry, kidney function tests, tumor markers, and radiological imaging within the previous 3 months were normal. The study protocol was approved by the Ethics Committee of Shandong Cancer Prevention and Control Research Institute. Individuals who met the inclusion criteria signed written informed consent for enrollment in the study.
SAMPLE AND DATA COLLECTION:
Peripheral blood was collected from the patients, and the relevant clinical data were recorded. The initial 1 mL of collected blood was discarded to prevent epithelial cell contamination and the associated interference with the study results. About 7.5 mL of blood was collected into a CellSave blood preservation tube, which had an anticoagulant effect. Samples were processed by the CellSearch system and stored at room temperature. The blood samples were tested within 96 h.
To reduce the damage caused by venous blood sampling, 5 mL of peripheral blood was processed with the CTC-Biopsy system. Blood samples were collected in an EDTA anticoagulant blood tube (BD Vacutainer batch no: 367863) and submitted for analysis by the CTC-Biopsy system within 24 h. The peripheral blood of 22 healthy volunteers was collected and processed as described above.
CTC DETECTION WITH THE CELLSEARCH SYSTEM:
The CellSearch system was operated in strict accordance with the manufacturer’s instructions [14]. CTCs were defined as round or oval epithelial cells, expressing cell surface antigen epithelial cell adhesion molecule (EpCAM), cytokeratin (CK), and DAPI (4′,6-2-amino-2-benzene indole), without the expression of leukocyte common antigen (CD45): EpCAM+/CK+/DAPI+/CD45−. The results were analyzed independently by 2 experienced technicians. If there was any inconsistency, double-blind reanalysis was carried out by the assessment technician. Test results were considered positive if 1 or more CTCs were detected.
CTC DETECTION WITH THE CTC-BIOPSY SYSTEM:
CTCs were separated by a newly designed CTC-Biopsy system (Wuhan YZY Medical Science and Technology Co., Ltd., Wuhan, China). To maintain the cell morphology for analysis, 5 mL of blood sample was diluted to 8 mL with 0.2% paraformaldehyde and transferred to a centrifuge tube. The mixture was aerated and absorbed by the Pasteur tube and fixed at room temperature for 10 min. After fixation, the blood sample was filtered through a filter membrane with an aperture of 8 μm. Five kilopascals were applied to the filters. The cells remaining on the filter membrane were stained with Wright-Giemsa stain and dried at room temperature. After the test, the filter membrane was taken out, adhered to a slide, and dried at 50°C to 60°C for 30 min. The slide was then sealed and read.
CRITERIA FOR CTC DIAGNOSIS:
The criteria for judging malignant abnormal cells (CTCs) were as follows:
Based on the evaluation criteria proposed in previous studies, we considered samples that met ≥4 of the parameters described above as CTC [15–17]. A sample was also classified as CTC if it met criterion (6) and 2 additional criteria. Three or more cells were considered to be a CTC agglomerate, which we will refer to from here on as a CTM. The results were interpreted by 2 cytopathologists. All decisions were made after consensus was reached. If 1 or more CTCs were detected, the test was considered to have yielded positive results.
STATISTICAL ANALYSIS:
SPSS version 19.0 was used for statistical analysis. Consistency testing was used to compare the CellSearch and CTC-Biopsy systems in detecting peripheral blood CTCs in patients with GC. Continuous variables were expressed as mean±standard deviation, and the data conforming to a normal distribution with equal variance were tested by
Results
DEMOGRAPHIC DETAILS:
A total of 59 patients with GC and 22 healthy volunteers were included in this study. In the GC group, there were 49 men and 10 women, with a mean age of 57 years (Table 1).
CTC DETECTION IN HEALTHY VOLUNTEERS:
CTCs were not detected in the peripheral blood of any of the healthy volunteers by either the CellSearch or the CTC-Biopsy system.
COMPARISON BETWEEN THE CELLSEARCH AND CTC-BIOPSY SYSTEMS:
The CellSearch system did not detect CTM, and the CTC detection rate was 27.12% (16/59) (Table 2, Figure 1). The CTC/CTM detection rate was 59.32% (35/59) with the CTC-Biopsy system (Table 3, Figure 2). This difference was statistically significant (P<0.001) (Table 4). The Kappa coefficient value was 0.179, which confirmed that the consistency in results between systems was poor (Table 4).
CORRELATION BETWEEN THE PRESENCE OF CTCS AND CLINICOPATHOLOGICAL FACTORS OF PATIENTS WITH GC:
With the CellSearch system, a significant association was found between detectable CTCs and various clinicopathological factors such as neutrophil count, lymphocyte count, neutrophil/lymphocyte ratio, serum CA 19-9, distant metastasis, clinical stage, lymph node metastasis, tumor location, tumor size, and the extent of vascular invasion (P<0.05) (Table 5).
Although no statistically significant differences were found in patients with stage I/II GC (P>0.05), there was a significant correlation between detectable CTCs and various clinicopathological factors in patients with stage III/IV GC (P<0.05) (Table 5).
With the CTC-Biopsy system, there was no significant correlation between detectable CTC/CTM and clinicopathological factors (Table 6). However, subgroup analysis showed a significant correlation with neutrophil/lymphocyte ratio and serum CA19-9 in patients with stage I/II GC, and in patients with stage III/IV GC. Also, detectable CTCs were correlated with the degree of tumor differentiation (P<0.05) (Table 6).
CORRELATION BETWEEN CTMS DETECTED WITH THE CTC-BIOPSY SYSTEM AND CLINICOPATHOLOGICAL FACTORS:
Among the 59 patients with GC, a CTM was detected by the CTC-Biopsy system in 15 patients. There was no significant correlation between CTM detection and clinicopathological factors (P>0.05) (Table 7). A subgroup analysis of patients with stage I/II GC showed that CTM was correlated with serum CEA levels (P<0.05) (Table 7). In patients with stage III/IV GC, the CTM detected with the CTC-Biopsy system was correlated with the degree of tumor differentiation (P<0.05) (Table 7).
FACTORS AFFECTING 4-YEAR PROGRESSION-FREE SURVIVAL IN PATIENTS WITH GC WHO UNDERWENT SURGICAL/INTERVENTIONAL/CHEMORADIOTHERAPY TREATMENT:
The results of the univariate analysis showed that patients with GC with a CTC count >3, as measured with the CellSearch system, had significantly lower progression-free survival (PFS) than patients with fewer CTCs. No such association with PFS was observed for elevated CTC counts measured with the CTC-Biopsy system (Table 8). The results of univariate analysis also showed that lower PFS was significantly associated with advanced pathological stage, distant metastasis, lymph node metastasis, large tumor size, and vascular infiltration (Table 8).
The multivariate analysis showed that, with a CTC count > 3, advanced pathological stage and distant metastasis were independent factors associated with low PFS in patients with GC, as determined by the CellSearch system (Table 8).
FACTORS AFFECTING 4-YEAR OS IN PATIENTS WITH GC WHO UNDERWENT SURGICAL/INTERVENTIONAL/CHEMORADIOTHERAPY TREATMENT:
The results of univariate analysis showed that patients with GC with a CTC count >3, as measured with the CellSearch system, had significantly lower OS than patients with fewer CTCs. The same association was not found with the CTC-Biopsy system (Table 9). Additional factors associated with decreased OS in the univariate analysis were advanced pathological stage, distant metastasis, lymph node metastasis, large tumor size, and vascular infiltration (Table 9). In the multivariate analysis, distant metastasis and a CTC count >3, as measured with the CellSearch system, were independent predictors of lower OS in patients with GC (Table 9).
IMPACT OF CTC COUNT, AS DETECTED WITH THE CELLSEARCH SYSTEM, ON SURVIVAL IN PATIENTS WITH GC:
The 4-year PFS of patients in the CTC ≤3 group was significantly higher than that of patients in the CTC >3 group (P<0.001) (Figure 3). Similarly, the 4-year OS of patients in the CTC ≤3 group was significantly higher than that of patients in the CTC >3 group (P<0.001) (Figure 4).
Discussion
The presence of CTCs has been used as a “liquid pathology” index for tumor metastasis and to assess the risk of tumor recurrence. CTCs have also been used for the real-time detection of tumor response and for targeted therapies [12]. However, the concentration of CTCs in human peripheral blood is very low and varies significantly among individuals. Advanced technology is required to detect CTCs [13]. In this study, we used the CellSearch system, which is based on cell-surface immune recognition, and the CTC-Biopsy system, which is based on cell morphology and size, to detect CTCs in the peripheral blood of patients with GC.
Detection techniques that are based on epithelial markers, such as with the CellSearch system, cannot capture cells that do not express EpCAM and cytokeratin on the cell membrane. Galatea et al. used breast cancer cell lines in their study and found that the filtration method had a higher recovery rate for tumor cells than did CellSearch [18]. Another study on pancreatic cancer found a 40% CTC detection rate with the CellSearch system, while the CTC detection rate achieved using a technology based on the filtration principle reached 93% [19]. In a study on esophageal squamous cell carcinoma, Li et al. reported that the CTC detection rate of the CTC-Biopsy system (32.8%) was significantly higher than that of the CellSearch system (1.6%) [20]. A similar study on renal cancer found that the CTC detection rates by the CellSearch system and technology based on the filtration principle were 19.4% and 36.1%, respectively [21]. In the present study, the CTC detection rate of the CTC-Biopsy system was significantly higher than that of the CellSearch system in GC (59.32%
Recent studies have shown that CTCs are associated with advanced tumor stage and lymphatic vascular invasion [24,25]. In the present study, CTCs detected with the CellSearch system were positively correlated with the stage of disease (
CTMs are more invasive than CTCs [5]. Carlsson et al. found that the number of CTMs in patients with advanced lung cancer was much higher than that in patients with early lung cancer (0 to 184
Neutrophils have been found to be associated with tumor growth, metastasis, and tumor angiogenesis. Previous studies have found that the number of neutrophils in GC tumor tissue is increased and associated with low OS rates in patients with GC [28]. A study of 1220 nonsurgical patients with advanced GC found that patients with an elevated neutrophil/lymphocyte ratio had poor OS and that the neutrophil/lymphocyte ratio was an independent prognostic factor [29]. In patients with GC undergoing radical resection and postoperative adjuvant chemotherapy, preoperative neutrophil/lymphocyte ratio values were independent risk factors for OS and PFS [30]. In the present study, CTC count, as measured with the CellSearch system, was found to be correlated with neutrophils (
This study had some limitations. First, because of the constraints of our study design, we could not compare the recovery rate and specificity of the 2 systems for detection of GC and WBC cell lines. Also, owing to technical limitations, we could not use immunocytofluorescence or immunocytochemistry to verify the results of the CTC-Biopsy in the GC group. Hence, we could not identify false-positive cases detected by the CTC-Biopsy system. In the future, we intend to perform a more comprehensive study with the use of immunocytofluorescence or immunocytochemistry to verify the nature of the cells detected by the CTC-Biopsy system and to validate cell lines. Second, there was a poor correlation between the CTCs detected with the CTC-Biopsy system and the clinicopathological or prognostic factors of patients. Moreover, the correlations were different with the CellSearch system. We think that this may be related to the small number of patients in the experimental group and the short follow-up time. Therefore, to further clarify the significance of CTC detection in the prognostic evaluation of GC, additional large-sample, multi-center clinical trials are needed. Third, the identification criteria used by the CellSearch and CTC-Biopsy systems were not the same. Future experiments comparing these 2 systems with the same identification criteria are required to decrease the possibility of false-positive results.
Conclusions
In conclusion, the CTC-Biopsy system, which was designed based on the filtration principle, is more sensitive than the CellSearch system in the detection of CTCs. CTCs detected with the CellSearch system correlated with various clinicopathological factors and prognosis in GC patients. Future studies are required to validate the findings of this study.
Figures
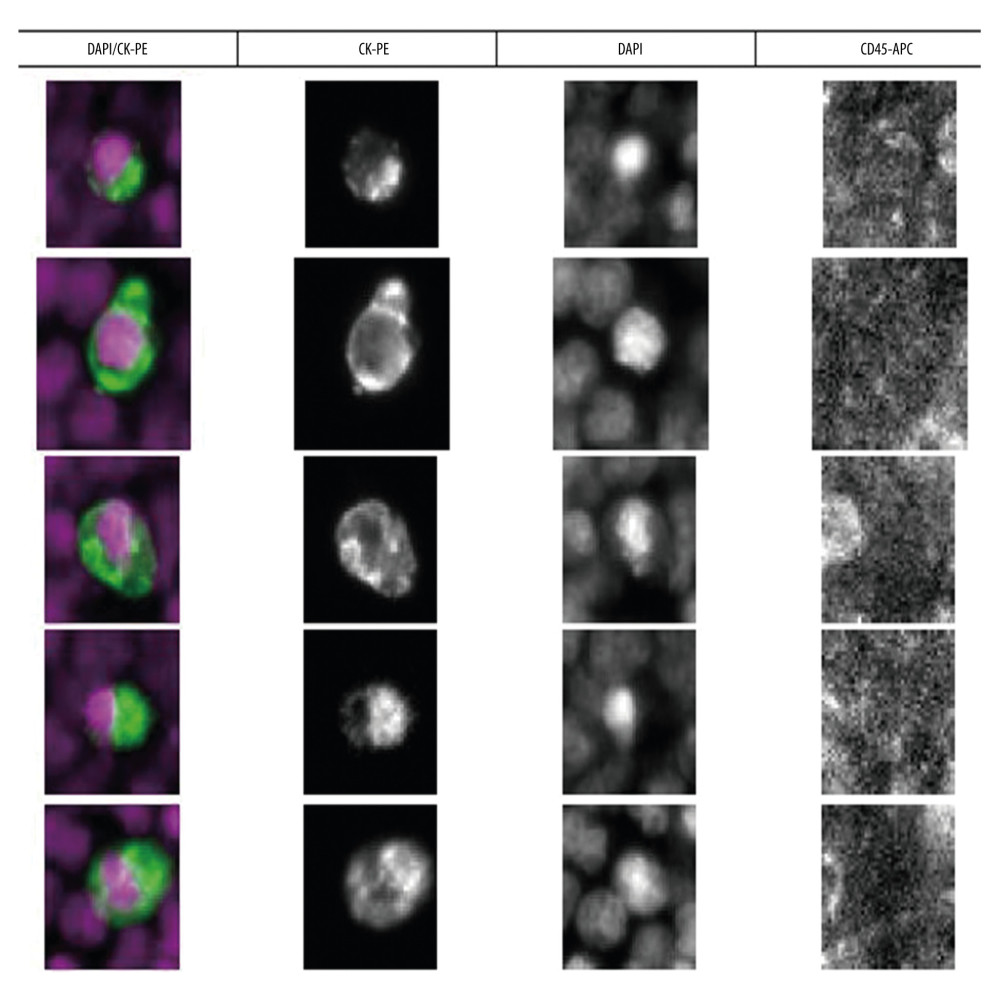 Figure 1. Circulating tumor cells (CTCs) were detected with the CellSearch system. In this system, CTCs were defined as circular or elliptical epithelial cells with specific cell surface antigen characteristics (EpCAM+/CK+/DAPI+/CD45−).
Figure 1. Circulating tumor cells (CTCs) were detected with the CellSearch system. In this system, CTCs were defined as circular or elliptical epithelial cells with specific cell surface antigen characteristics (EpCAM+/CK+/DAPI+/CD45−). 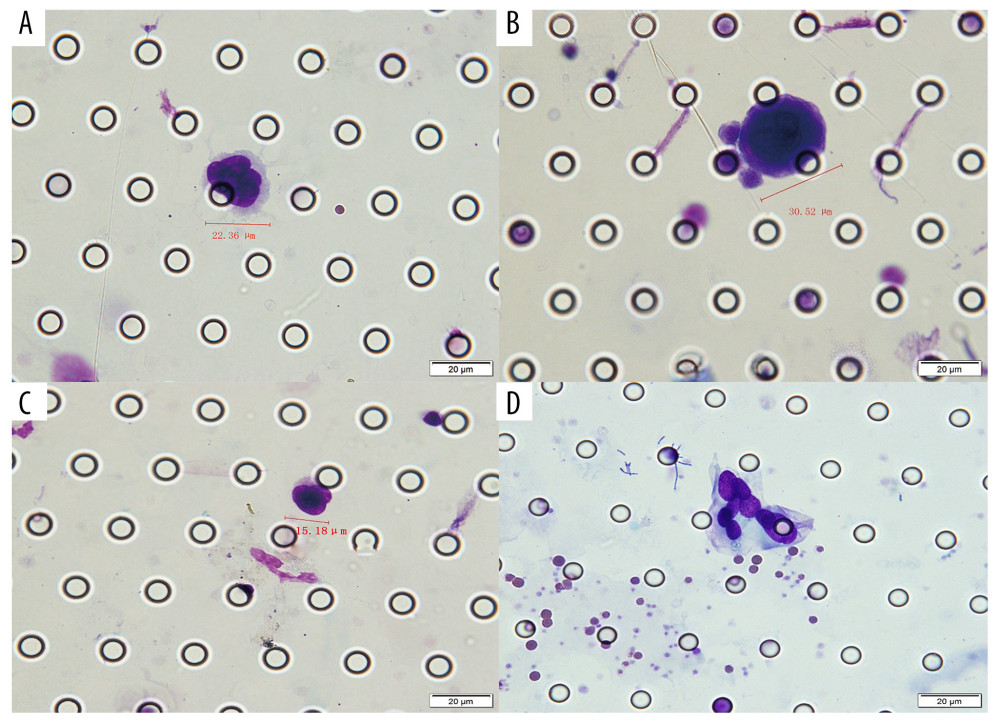 Figure 2. Circulating tumor cells (CTC)/circulating tumor microemboli (CTM) detected with the CTC-Biopsy system in patients with gastric cancer. Wright-Giemsa staining was performed for cytomorphological analysis. (A) CTC: nuclear-cytoplasmic ratio >0.8, irregular nuclear shape. (B) CTC: cell diameter >15 μm; abnormally large nucleoli. (C) CTC: thickened and wrinkled, with jagged nuclear membranes and side-shifted chromatin. (D) CTM: aggregation of tumor cells (≥3). All cells were analyzed under 40× magnification. Scale bar: 20 μm.
Figure 2. Circulating tumor cells (CTC)/circulating tumor microemboli (CTM) detected with the CTC-Biopsy system in patients with gastric cancer. Wright-Giemsa staining was performed for cytomorphological analysis. (A) CTC: nuclear-cytoplasmic ratio >0.8, irregular nuclear shape. (B) CTC: cell diameter >15 μm; abnormally large nucleoli. (C) CTC: thickened and wrinkled, with jagged nuclear membranes and side-shifted chromatin. (D) CTM: aggregation of tumor cells (≥3). All cells were analyzed under 40× magnification. Scale bar: 20 μm. 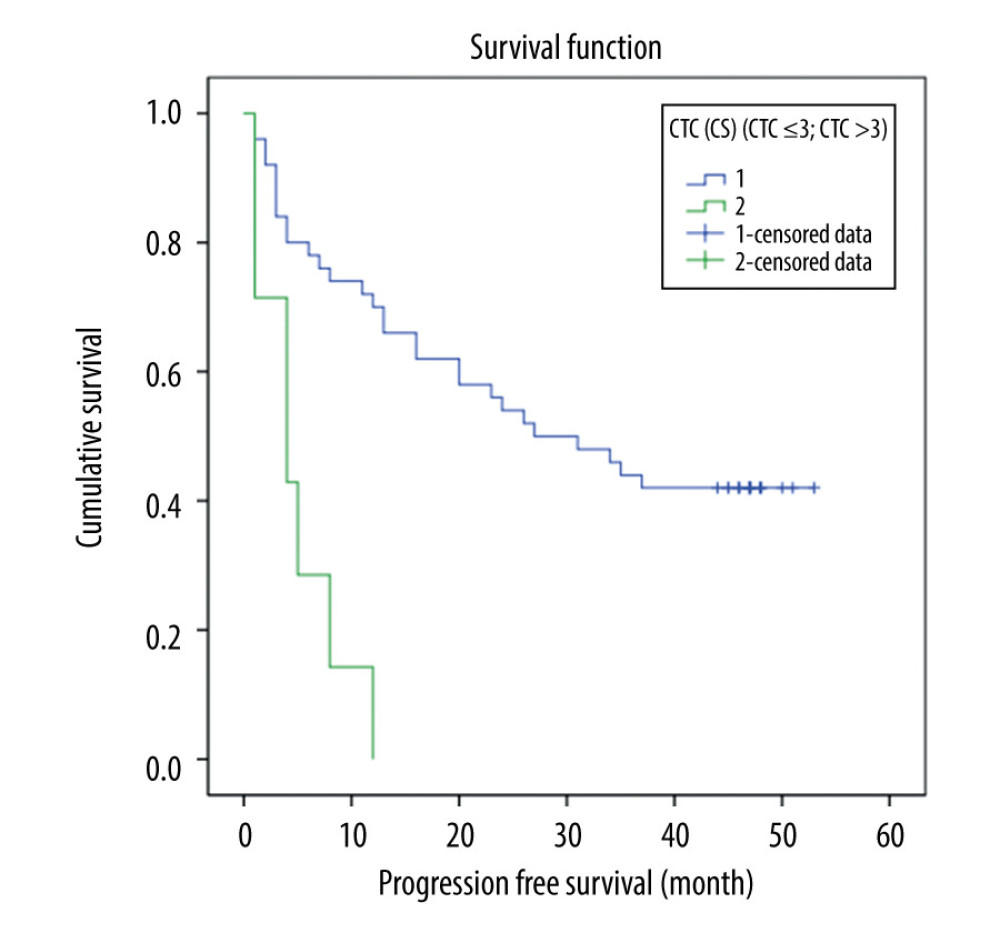 Figure 3. Correlation between circulating tumor cells (CTCs) detected with the CellSearch system and progression-free survival in 59 patients with gastric cancer (CTC ≤3 and CTC >3 group log-rank test, P<0.001).
Figure 3. Correlation between circulating tumor cells (CTCs) detected with the CellSearch system and progression-free survival in 59 patients with gastric cancer (CTC ≤3 and CTC >3 group log-rank test, P<0.001). 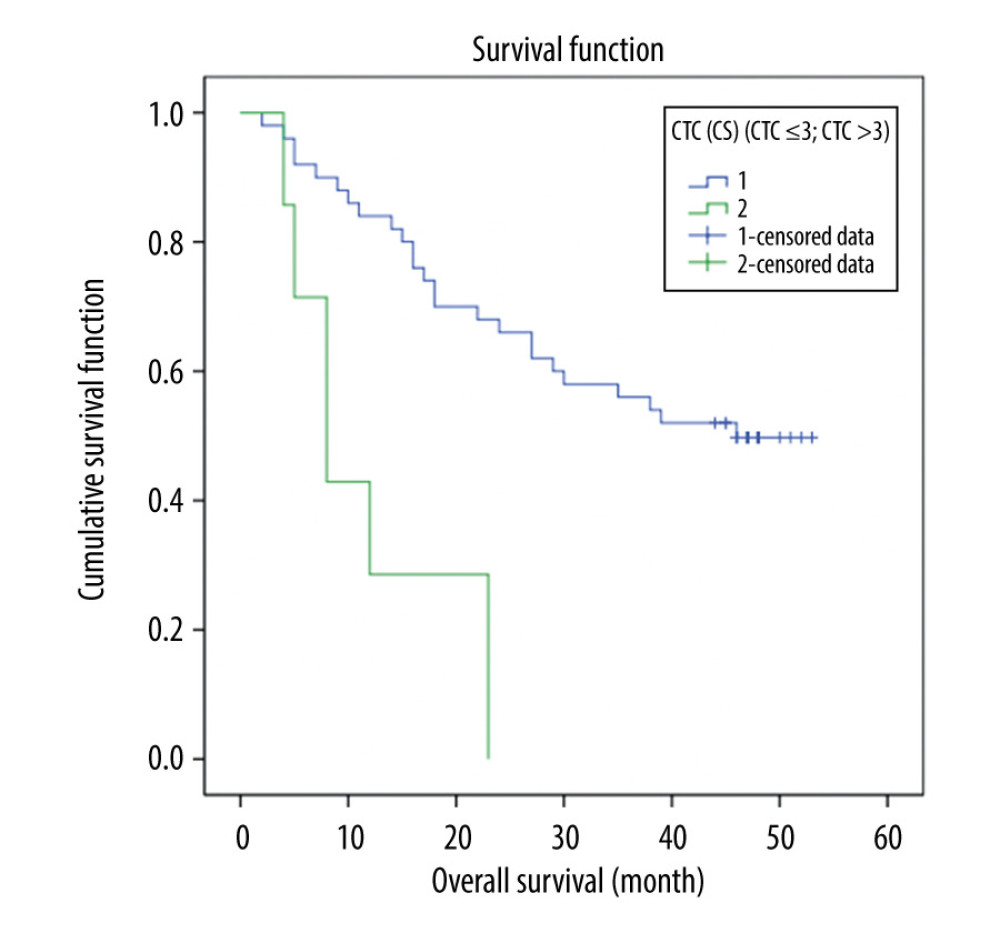 Figure 4. Correlation between circulating tumor cells (CTCs) detected with the CellSearch system and overall survival in 59 patients with gastric cancer (CTC ≤03 and CTC >3 group log-rank test, P<0.001).
Figure 4. Correlation between circulating tumor cells (CTCs) detected with the CellSearch system and overall survival in 59 patients with gastric cancer (CTC ≤03 and CTC >3 group log-rank test, P<0.001). Tables
Table 1. Baseline characteristics of the study population. Table 2. Circulating tumor cells detected with the CellSearch system in patients with gastric cancer.
Table 2. Circulating tumor cells detected with the CellSearch system in patients with gastric cancer.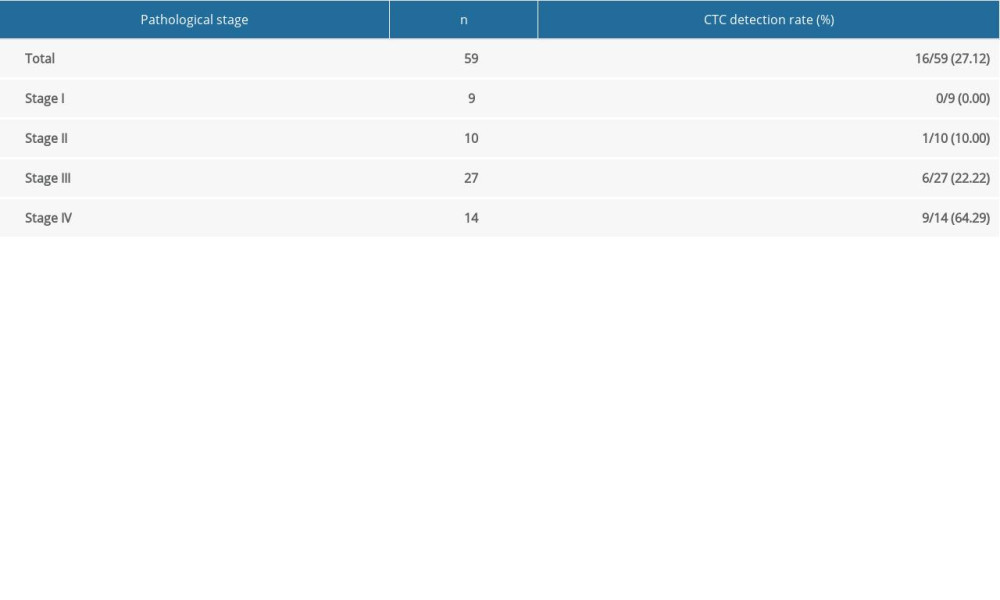 Table 3. Circulating tumor cells detected with the CTC-Biopsy system in patients with gastric cancer.
Table 3. Circulating tumor cells detected with the CTC-Biopsy system in patients with gastric cancer.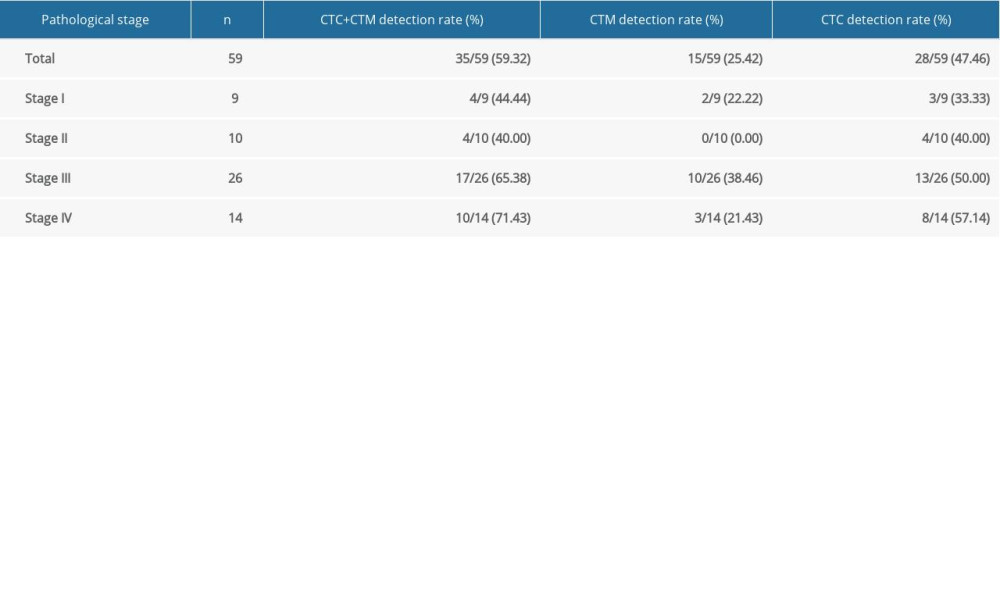 Table 4. Comparison of CellSearch and CTC-Biopsy systems in terms of circulating tumor cells detection rate.
Table 4. Comparison of CellSearch and CTC-Biopsy systems in terms of circulating tumor cells detection rate.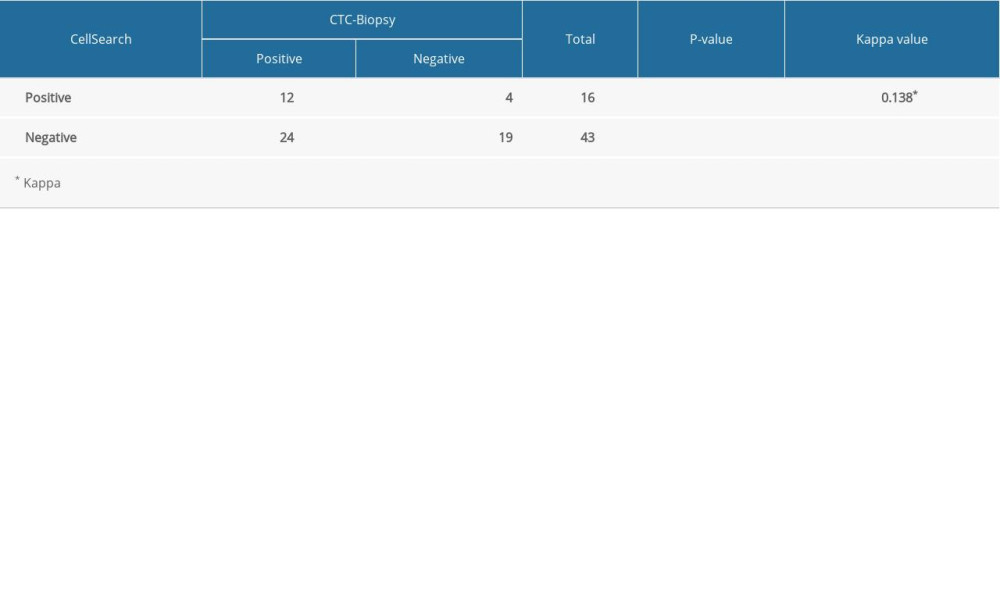 Table 5. Correlation between circulating tumor cells detected with the CellSearch system and clinicopathological factors.
Table 5. Correlation between circulating tumor cells detected with the CellSearch system and clinicopathological factors.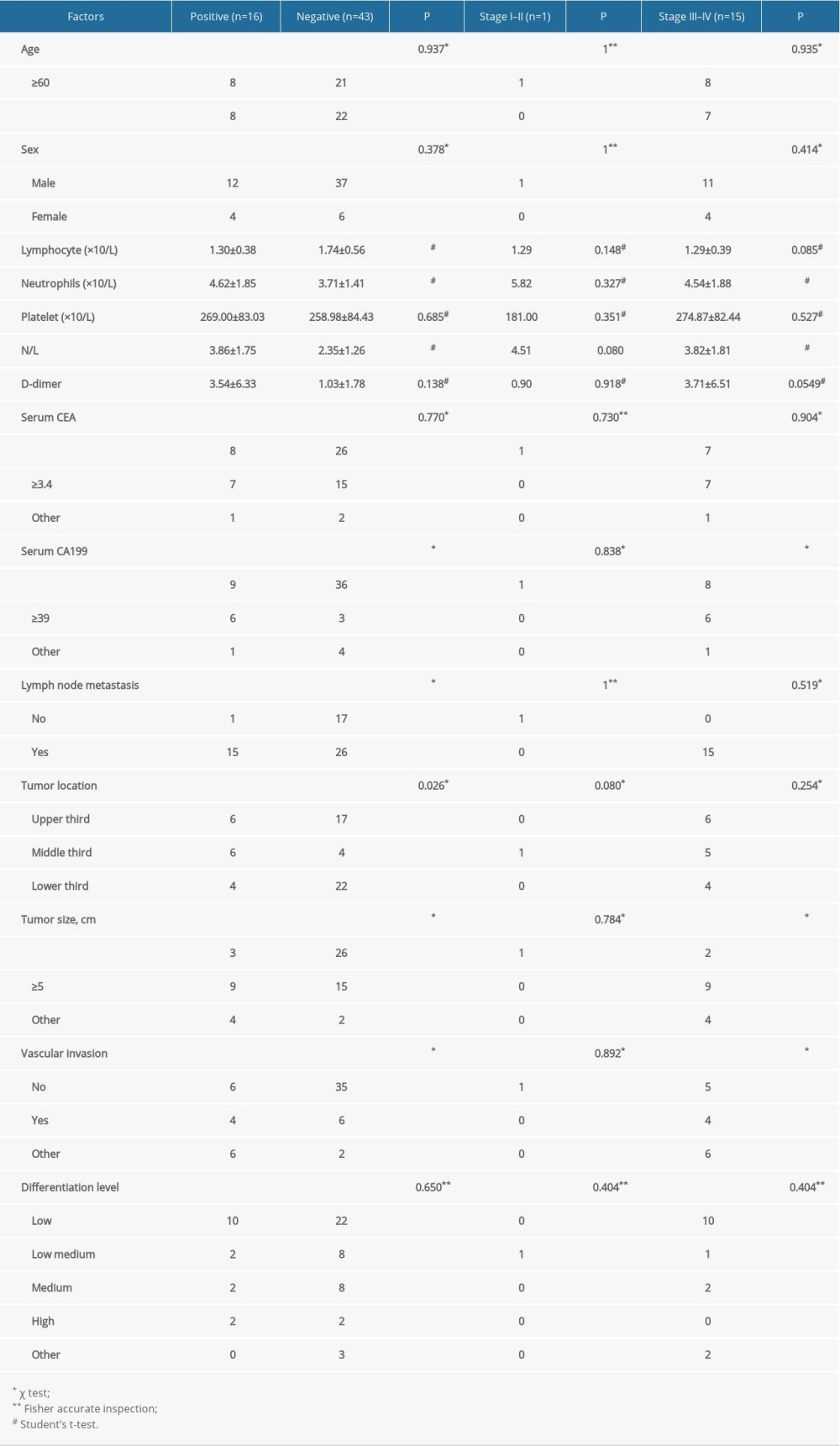 Table 6. Correlation between circulating tumor cells detected with the CTC-Biopsy system and clinicopathological factors.
Table 6. Correlation between circulating tumor cells detected with the CTC-Biopsy system and clinicopathological factors.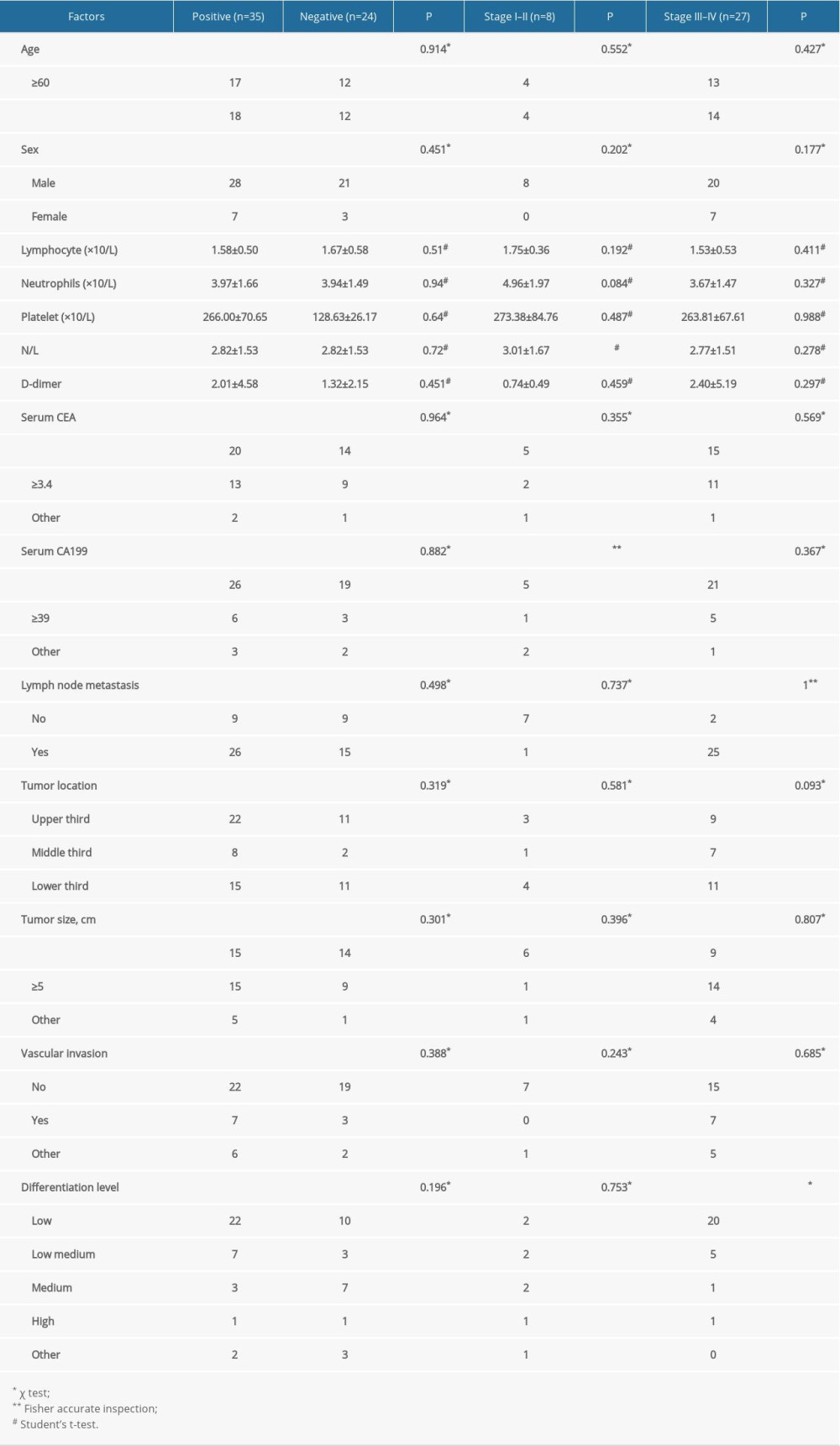 Table 7. Correlation between circulating tumor microemboli detected with the CTC-Biopsy system and clinicopathological factors.
Table 7. Correlation between circulating tumor microemboli detected with the CTC-Biopsy system and clinicopathological factors.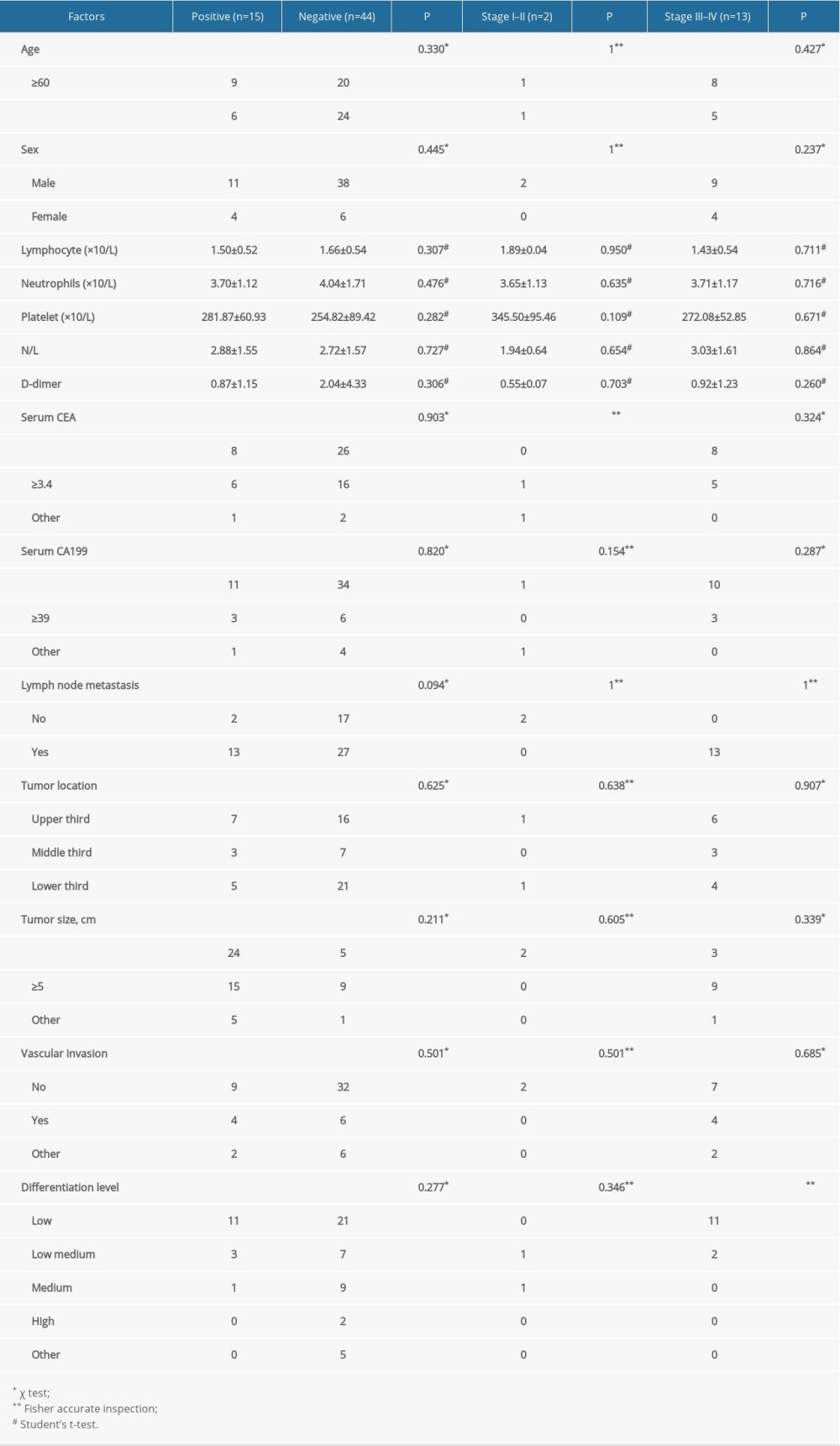 Table 8. Univariate and multivariate analysis of CellSearch-derived and other factors affecting progression-free survival in patients with gastric cancer.
Table 8. Univariate and multivariate analysis of CellSearch-derived and other factors affecting progression-free survival in patients with gastric cancer.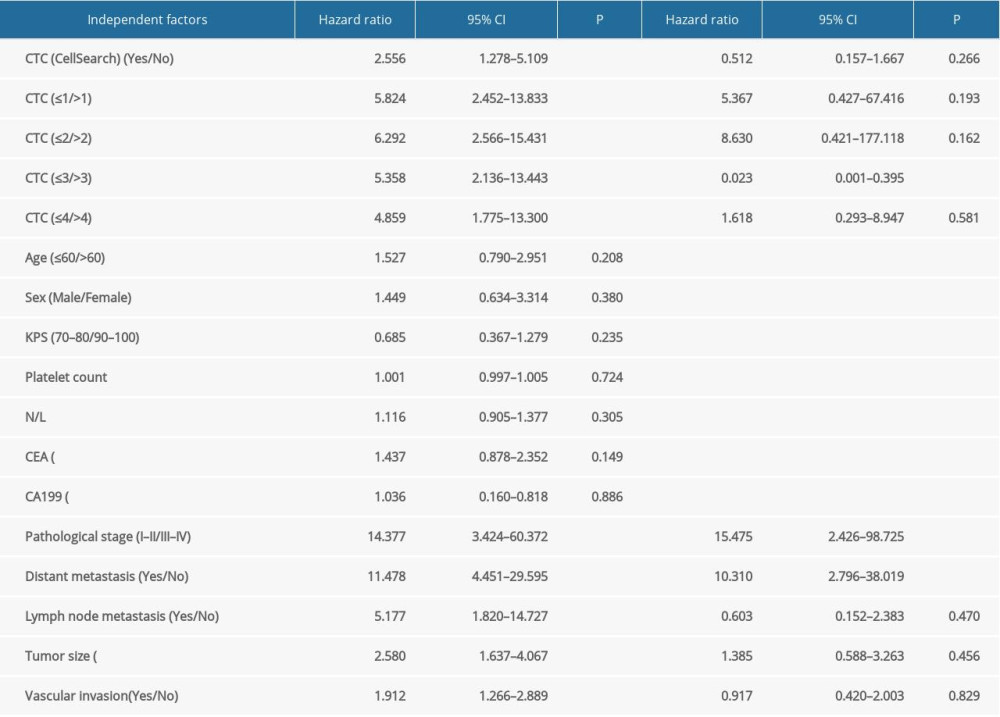 Table 9. Univariate and multivariate analyses of factors affecting overall survival in patients with gastric cancer.
Table 9. Univariate and multivariate analyses of factors affecting overall survival in patients with gastric cancer.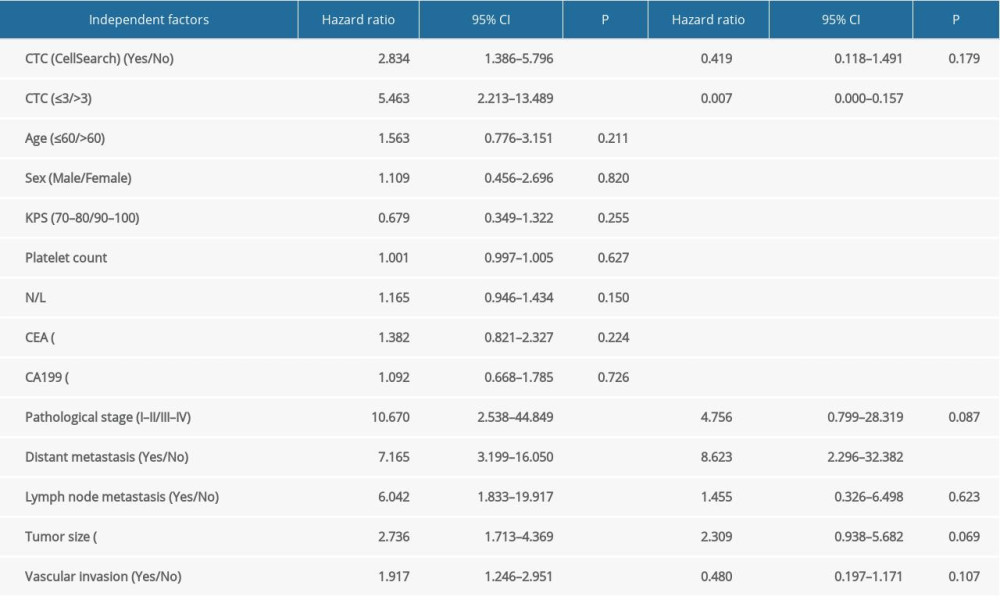
References
1. Karimi P, Islami F, Anandasabapathy S, Gastric cancer: Descriptive epidemiology, risk factors, screening, and prevention: Cancer Epidemiol Biomarkers, 2014; 23; 700-13
2. Duarte HO, Gomes J, Machado JC, Gastric cancer: Basic aspects: Helicobacter, 2018; e12523
3. Marrelli D, De Stefano A, de Manzoni G, Prediction of recurrence after radical surgery for gastric cancer: A scoring system obtained from a prospective multicenter study: Ann Surg, 2005; 241; 247-55
4. Liu Y, Gai J, Fu L, Effects of RSF-1 on proliferation and apoptosis of breast cancer cells: Oncol Lett, 2018; 16; 4279-84
5. Zhang ZY, Ge HY, Micrometastasis in gastric cancer: Cancer Lett, 2013; 336; 34-45
6. Duda DG, Ancukiewicz M, Isakoff SJ, Seeds and soil: Unraveling the role of local tumor stroma in distant metastasis: J Natl Cancer Inst, 2014; 106; dju187
7. Krebs MG, Metcalf RL, Carter L, Molecular analysis of circulating tumour cells-biology and biomarkers: Nat Rev Clin Oncol, 2014; 11; 129-44
8. Danila DC, Heller G, Gignac GA, Circulating tumor cell number and prognosis in progressive castration-resistant prostate cancer: Clin Cancer Res, 2007; 13; 7053-58
9. Yang C, Chen F, Wang S, Circulating tumor cells in gastrointestinal cancers: Current status and future perspectives: Front Oncol, 2019; 9; 1427
10. Vona G, Béroud C, Benachi A, Enrichment, immunomorphological, and genetic characterization of fetal cells circulating in maternal blood: Am J Pathol, 2002; 160; 51-58
11. Cristofanilli M, Budd GT, Ellis MJ, Circulating tumor cells, disease progression, and survival in metastatic breast cancer: N Engl J Med, 2004; 351; 781-91
12. Palmirotta R, Lovero D, Cafforio P, Liquid biopsy of cancer: A multimodal diagnostic tool in clinical oncology: Ther Adv Med Oncol, 2018; 10; 1758835918794630
13. Hong B, Zu Y, Detecting circulating tumor cells: Current challenges and new trends: Theranostics, 2013; 3; 377-94
14. Huebner H, Fasching PA, Gumbrecht W: BMC Cancer, 2018; 18; 204
15. Hofman V, Long E, Ilie M, Morphological analysis of circulating tumour cells in patients undergoing surgery for non-small cell lung carcinoma using the isolation by size of epithelial tumour cell (ISET) method: Cytopathology, 2012; 23; 30-38
16. Vona G, Sabile A, Louha M, Isolation by size of epithelial tumor cells: A new method for the immunomorphological and molecular characterization of circulatingtumor cells: Am J Pathol, 2000; 156; 57-63
17. Vona G, Béroud C, Benachi A, Enrichment, immunomorphological, and genetic characterization of fetal cells circulating in maternal blood: Am J Pathol, 2002; 160; 51-58
18. Kallergi G, Politaki E, Alkahtani S, Evaluation of isolation methods for circulating tumor cells (CTCs): Cell Physiol Biochem, 2016; 40; 411-19
19. Khoja L, Backen A, Sloane R, A pilot study to explore circulating tumour cells in pancreatic cancer as a novel biomarker: Br J Cancer, 2012; 106; 508-16
20. Li H, Song P, Zou B, Circulating tumor cell analyses in patients with esophageal squamous cell carcinoma using epithelial marker-dependent and -independent approaches: Medicine, 2015; 94; e1565
21. Bai M, Zou B, Wang Z, Comparison of two detection systems for circulating tumor cells among patients with renal cell carcinoma: Int Urol Nephrol, 2018; 50; 1801-9
22. Abdallah EA, Braun AC, Flores BCTCP, The potential clinical implications of circulating tumor cells and circulating tumor microemboli in gastric cancer: Oncologist, 2019; 24; e854-63
23. Zheng X, Fan L, Zhou P, Detection of circulating tumor cells and circulating tumor microemboli in gastric cancer: Transl Oncol, 2017; 10; 431-41
24. Wang L, Zhou S, Zhang W, Circulating tumor cells as an independent prognostic factor in advanced colorectal cancer: A retrospective study in 121 patients: Int J Colorectal Dis, 2019; 34; 589-97
25. Pan L, Yan G, Chen W, Distribution of circulating tumor cell phenotype in early cervical cancer: Cancer Manag Res, 2019; 11; 5531-36
26. Carlsson A, Nair VS, Luttgen MS, Circulating tumor microemboli diagnostics for patients with non-small-cell lung cancer: J Thorac Oncol, 2014; 9; 1111-19
27. Liu Y, Ling Y, Qi Q, Prognostic value of circulating tumor cells in advanced gastric cancer patients receiving chemotherapy: Mol Clin Oncol, 2017; 6; 235-42
28. Zhao JJ, Pan K, Wang W, The prognostic value of tumor-infiltrating neutrophils in gastric adenocarcinoma after resection: PLoS One, 2012; 7; e33655
29. Jin H, Sun J, Zhu K, The prognostic value of neutrophil-lymphocyte ratio is superior to derived neutrophil-lymphocyte ratio in advanced gastric cancer treated with preoperative chemotherapy and sequential R0 resection: A 5-year follow-up: OncoTargets Ther, 2017; 10; 2655-64
30. Aliustaoglu M, Bilici A, Ustaalioglu BB, The effect of peripheral blood values on prognosis of patients with locally advanced gastric cancer before treatment: Med Oncol, 2010; 27; 1060-65
Figures
Figure 1. Circulating tumor cells (CTCs) were detected with the CellSearch system. In this system, CTCs were defined as circular or elliptical epithelial cells with specific cell surface antigen characteristics (EpCAM+/CK+/DAPI+/CD45−).Figure 2. Circulating tumor cells (CTC)/circulating tumor microemboli (CTM) detected with the CTC-Biopsy system in patients with gastric cancer. Wright-Giemsa staining was performed for cytomorphological analysis. (A) CTC: nuclear-cytoplasmic ratio >0.8, irregular nuclear shape. (B) CTC: cell diameter >15 μm; abnormally large nucleoli. (C) CTC: thickened and wrinkled, with jagged nuclear membranes and side-shifted chromatin. (D) CTM: aggregation of tumor cells (≥3). All cells were analyzed under 40× magnification. Scale bar: 20 μm.Figure 3. Correlation between circulating tumor cells (CTCs) detected with the CellSearch system and progression-free survival in 59 patients with gastric cancer (CTC ≤3 and CTC >3 group log-rank test, P<0.001).Figure 4. Correlation between circulating tumor cells (CTCs) detected with the CellSearch system and overall survival in 59 patients with gastric cancer (CTC ≤03 and CTC >3 group log-rank test, P<0.001). Tables
Table 1. Baseline characteristics of the study population.Table 2. Circulating tumor cells detected with the CellSearch system in patients with gastric cancer.Table 3. Circulating tumor cells detected with the CTC-Biopsy system in patients with gastric cancer.Table 4. Comparison of CellSearch and CTC-Biopsy systems in terms of circulating tumor cells detection rate.Table 5. Correlation between circulating tumor cells detected with the CellSearch system and clinicopathological factors.Table 6. Correlation between circulating tumor cells detected with the CTC-Biopsy system and clinicopathological factors.Table 7. Correlation between circulating tumor microemboli detected with the CTC-Biopsy system and clinicopathological factors.Table 8. Univariate and multivariate analysis of CellSearch-derived and other factors affecting progression-free survival in patients with gastric cancer.Table 9. Univariate and multivariate analyses of factors affecting overall survival in patients with gastric cancer.Table 1. Baseline characteristics of the study population.Table 2. Circulating tumor cells detected with the CellSearch system in patients with gastric cancer.Table 3. Circulating tumor cells detected with the CTC-Biopsy system in patients with gastric cancer.Table 4. Comparison of CellSearch and CTC-Biopsy systems in terms of circulating tumor cells detection rate.Table 5. Correlation between circulating tumor cells detected with the CellSearch system and clinicopathological factors.Table 6. Correlation between circulating tumor cells detected with the CTC-Biopsy system and clinicopathological factors.Table 7. Correlation between circulating tumor microemboli detected with the CTC-Biopsy system and clinicopathological factors.Table 8. Univariate and multivariate analysis of CellSearch-derived and other factors affecting progression-free survival in patients with gastric cancer.Table 9. Univariate and multivariate analyses of factors affecting overall survival in patients with gastric cancer. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387