09 February 2022: Clinical Research
A Risk Prediction Model for Prolonged Length of Stay in Patients with Acute Exacerbations of Chronic Obstructive Pulmonary Disease: A Retrospective Study of 225 Patients in a Single Center in Kunming, China
Lifen Yang1ABCDEFG*, Meihua Li1BCD, Jingkui Shu2BCD, Yanxia Yang1BCD, Qian Huang3BCDDOI: 10.12659/MSM.934392
Med Sci Monit 2022; 28:e934392






Abstract
BACKGROUND: We aimed to develop an effective prediction model of prolonged length of stay (LOS) in patients with acute exacerbations of chronic obstructive pulmonary disease (AECOPD).
MATERIAL AND METHODS: We systematically enrolled 225 patients admitted for AECOPD to our hospital and divided them into a normal LOS group (≤7 days) and prolonged LOS group (>7 days). To analyze differences in laboratory data at different times, 3 logistic regression models were established. To develop the prediction model, all variables with statistical significance were included in the model. The area under the curve (AUC) was used to evaluate discrimination, and the Hosmer-Lemeshow test was used to assess the calibration of the model.
RESULTS: Factors found to be independently associated with the increased risk of prolonged LOS included the use of corticosteroids during hospitalization, elevated HCO₃⁻, decreased pH, and reductions in platelets (PLTs) and procalcitonin (PCT) between the fourth and first day of hospitalization. The risk prediction model including these factors had an AUC of 0.795, suggesting the good discrimination of our model. The Hosmer-Lemeshow test also showed good calibration of the model, which confirmed its good predictive performance.
CONCLUSIONS: A clinical prediction model was developed with good predictive performance, which could help clinicians identify patients with a higher risk of prolonged LOS, help shorten hospital stay, reduce the disease burden of patients, and improve the outcomes of AECOPD.
Keywords: Clinical Decision Rules, COPD, Severe Early-Onset, Acute Disease, Adrenal Cortex Hormones, Blood Platelets, China, Female, Humans, Hydrogen-Ion Concentration, Length of Stay, Male, procalcitonin, Pulmonary Disease, Chronic Obstructive, Risk Assessment
Background
Chronic obstructive pulmonary disease (COPD) is a chronic respiratory disorder characterized by persistent respiratory symptoms and airflow limitation. COPD is rarely reversible and can lead to chronic respiratory failure [1,2]. COPD remains the most prevalent disease-specific chronic respiratory disease, having a 5.9% relative increase in overall prevalence and killing of over 3 million people each year worldwide [3,4]. According to the World Health Organization, COPD is predicted to become the third leading cause of mortality worldwide by 2030 [5]. Acute exacerbation of COPD (AECOPD), which is characterized by episodes of worsening respiratory symptoms, has significant adverse consequences for patients [6,7]. Respiratory viruses and bacteria are the primary causes of AECOPD. Bacteria, such as
According to previous studies, prolonged LOS is associated with various clinical variables, such as advanced age, reduced body mass index (BMI), smoking history, presence of comorbidities, more severe AECOPD, higher prevalence of oxygen therapy, and use of mechanical ventilation [15–21]. Some vital sign parameters, such as greater respiratory rate on admission, systolic pressure > 140 mmHg, and diastolic pressure >90 mmHg, were also found to be related to prolonged LOS in patients with AECOPD [17,22]. Pathogen infection is also associated with prolonged AECOPD LOS [23–25]. As suggested by Mushlin et al, the medically required LOS for patients with AECOPD should be between 6 and 7 days based on clinical characteristics [26]. Crisafulli et al regarded over 7 days as extended LOS [15]. To the best of our knowledge, some models have been established to predict the risk of prolonged LOS in patients with AECOPD based on various predictors, including heart failure, diabetes, low serum albumin level, BMI, dyspnea, and physical activity level [14,17,20]. Whether there are other variables that can be used to build a valuable predictive model is as yet unknown.
Thus, we aimed to identify the predictors of prolonged LOS (defined as > 7 days) and tried to develop an effective prediction model using clinical and laboratory variables before and after admission, which may help clinicians to identify the patients who would require a prolonged stay and to develop corresponding interventions.
Material and Methods
STUDY DESIGN:
In this retrospective study, we systematically enrolled patients admitted for AECOPD to the First Hospital of Kunming. The inclusion criteria were: (1) patients aged ≥18 years and (2) patients who met the diagnostic criteria for COPD specified by the Global Initiative for Chronic Obstructive Lung Disease (GOLD) Initiative of 2017 [6]; specifically, COPD should be considered in any patient with the symptoms of dyspnea, chronic cough, or sputum production, and a post-bronchodilator forced expiratory volume in 1 s/forced vital capacity (FEV1/FVC) ratio <0.70 by spirometry, confirming the presence of persistent airflow limitation. AECOPD was defined as an acute worsening of respiratory symptoms that required additional therapy [6]. The exclusion criteria were: (1) patients with other respiratory diseases, such as pneumothorax or pulmonary embolism, asthma, pulmonary fibrosis, bronchiectasis, pulmonary tuberculosis sequelae, or pleural thickening; (2) patients with acute heart failure; (3) patients with extremely low immune function, severe infection, renal dysfunction, hepatobiliary diseases, pancreatic diseases, hyperthyroidism or hypothyroidism, malignant tumors, or blood system or connective tissue disorders; (4) patients with poor compliance who could not be contacted or were unwilling to make contact after discharge; (5) patients who took other investigational drugs within 1 month before our enrollment or were participating in other clinical studies; and (6) patients who were deemed unsuitable for this study by the physician in charge.
The study was approved by the Ethics Committee of our hospital (approval no. SLKY2018-53) and was conducted according to the requirements of the Good Clinical Practice guidelines and Declaration of Helsinki.
DATA COLLECTION:
Before admission, demographic and clinical data, including age, sex, BMI, history of drug and other allergies, surgery history, smoking and alcohol use, comorbidities (hypertension and diabetes), medication history (the use of systemic corticosteroids and antibiotics), home care medications (long-term oxygen therapy, short-acting β2-agonists, long-acting β2-agonists, and anticholinergics), season of COPD exacerbation (referring to the season of prior exacerbation in the last year), number of exacerbation attacks in the last year, and dyspnea grade were recorded. The dyspnea grade was evaluated by the modified Medical Research Council (mMRC) scale, which consists of a 5-level categorization, with a score of 2 as the symptomatic cutoff point. The severity of AECOPD was assessed by the Charlson weighted index of comorbidities, a method of categorizing comorbidities based on the International Classification of Diseases diagnosis codes. Each comorbidity category has an associated weight ranging from 1 to 6, based on the adjusted risk of mortality or resource use, and the sum of all the weights results in a single comorbidity score for an individual patient. The higher the score, the more likely the predicted outcome will result in mortality or higher resource use. On admission, all patients also underwent laboratory and microbial tests, and relevant variables, including white blood cells (WBCs), red blood cells (RBCs), packed-cell volume (PCV), hemoglobin (Hb), platelets (PLT), neutrophils (NEUT), lymphocytes (LY), pH, partial arterial carbon dioxide pressure (PaCO2), the ratio of partial arterial oxygen pressure to the fraction of inspired oxygen (PaO2/FiO2), HCO3−, base excess (BE), C-reactive protein (CRP), procalcitonin (PCT), amyloid, interleukin (IL)-6, and bacteria in sputum, were recorded. On the fourth day of admission, clinical and laboratory variables (corticosteroid and antibiotic use during hospitalization and laboratory variables as specified above, except bacteria in sputum) were collected. LOS was recorded at the time of discharge.
On admission, we collected sputum from spontaneous cough samples, which was processed by Gram staining and culture if sufficient (with >25 WBCs and <10 epithelial cells per field). In patients who did not provide spontaneous sputum samples, we obtained induced sputum production by inhalation of 5% hypertonic saline solution (via nebulization for 5 to 10 min).
LABORATORY AND MICROBIAL TESTS:
The laboratory tests conducted were blood cell analysis, arterial blood gas analysis, and infection markers test. The blood cell analysis for WBC, RBC, PCV, Hb, PLT, NEUT, and LY was carried out with a Sysmex XN-1000 automated hematology analyzer (Sysmex Corporation, Kobe, Japan). An ABL80 blood gas analyzer (Radiometer Medical A/S, Copenhagen, Denmark) was used for the arterial blood gas analysis to obtain data on pH, PaCO2, PaO2/FiO2, HCO3−, and BE. The infection markers test for CRP, PCT, amyloid, and IL-6 was performed using a Roche Cobas 8000 electrochemical analyzer (Roche Diagnostics, Mannheim, Germany).
The microbial test was a sputum culture. The sputum sample was homogenized with sputolysin and inoculated in blood agar, chocolate agar, and MacConkey agar media, which were incubated in 5% CO2 at 35 for 18 to 24 h. If no growth was observed after overnight incubation, the culture plates were incubated for an additional 24 h. Bacterial agents are classified as potentially pathogenic microorganisms (PPM) or non-PPM. Only when PPMs reached >106/colony forming units (CFUs) were they considered significant, while 105/CFU was regarded significant for
STATISTICAL ANALYSIS:
The included patients were divided into the normal LOS group (≤7 days) and the prolonged LOS group (>7 days). The Shapiro-Wilk test was used to test the normality of the quantitative data. Normally distributed quantitative data were described as mean±standard deviation, and the
Logistic stepwise regression analysis was performed to screen the variables. For differences in the laboratory data at different times, 3 logistic regression models were established. Age, sex, long-term home oxygen therapy, short-acting β2 agonists, COPD-exacerbated, autumn, and Charlson index were included in models 1, 2, and 3. In addition, laboratory data on admission was included in model 1, laboratory data on the fourth day of hospitalization was included in model 2, and changes in laboratory data between the fourth and first day of hospitalization was included in model 3. Then, the final model included all variables with statistical significance in models 1, 2, and 3 to develop a prediction model of prolonged LOS. The area under the curve (AUC) was used to evaluate the discrimination and the Hosmer-Lemeshow test was used to assess the calibration of the final model.
Data were statistically analyzed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA). Receiver operating characteristic (ROC) curves were plotted using R 4.0.2 (R foundation for Statistical Computing, Vienna, Austria).
Results
BASELINE DESCRIPTION:
In the present study, a total of 225 patients were enrolled and divided into a normal LOS group (≤7 days, n=73) and prolonged LOS group (>7 days, n=152). The median LOS was 7 days. Most patients (86.22%) were men and 78.67% of patients had a smoking history. The mean age was 71.23±8.43 years, and the mean BMI was 22.34±2.72 kg/m2. For comorbidities, 107 (47.56%) patients had hypertension, and 26 (11.56%) patients had diabetes. The most frequent medication history was antibiotic use. For home therapy, long-term home oxygen therapy was the most frequently used treatment, followed by short-acting β2 agonists. Concerning COPD exacerbation, most patients (56.89%) reported COPD exacerbation in winter. Nearly half of patients (48.44%) had 0 to 1 exacerbations within the last year.
DIFFERENCES IN BASELINE CHARACTERISTICS:
Based on the clinical and laboratory data collected at baseline, the univariate analysis suggested that age (t=−2.515, P=0.013), proportions of long-term home oxygen therapy (χ2=11.615, P<0.001), short-acting β2 agonists (χ2=6.426, P=0.011), and the incidence rate of autumn exacerbation (χ2=6.513, P=0.011) in the prolonged LOS group were all significantly higher than those in the normal LOS group. For laboratory data, the prolonged LOS group showed a significantly higher pH (t=−2.69, P=0.008), dyspnea grade (χ2=14.581, P<0.001), and Charlson index (χ2=7.769, P=0.005) but significantly lower PaCO2 (t=2.33, P=0.021) and HCO3− (t=2.23, P=0.027) compared with the normal LOS group (Table 1).
DIFFERENCES IN CHARACTERISTICS ON THE FOURTH DAY OF HOSPITALIZATION:
As shown in Table 2, analysis on the fourth day of hospitalization showed that PaO2/FiO2 (Z=−2.600, P=0.009), HCO3− (t=2.10, P=0.037), BE (Z=−2.112, P=0.035), and the proportion of corticosteroid use during hospitalization (χ2=14.060, P<0.001) in the prolonged LOS group were significantly higher than those in the normal LOS group.
DIFFERENCES IN CHARACTERISTIC CHANGES BETWEEN THE FOURTH AND FIRST DAY:
The results showed that changes in laboratory variables between the fourth and first day of hospitalization were similar between the prolonged LOS group and the normal LOS group (all P>0.05; Table 3).
VARIABLES ASSOCIATED WITH THE RISK OF PROLONGED LOS:
In multivariate regression model 1, which incorporated the laboratory data on admission, 1-year increase in age (day 1) was revealed to be associated with a 0.039-fold increase (OR 1.039, 95% CI 1.002–1.078) in the risk of prolonged LOS. Compared with patients with an mMRC scale (day 1) score of 0 to1, the risk of prolonged LOS increased 1.796-fold (OR 2.796, 95% CI 1.490–5.245) in those with scores of 2 to 4. In addition, the risk decreased 0.996-fold (OR 0.004, 95% CI 0.001–0.441) for every increase in pH (day 1), and the risk increased 0.077-fold (OR 1.077, 95% CI 1.006–1.153) for every 1 mmol/L increase in HCO3− (day 1) (Table 4).
In multivariate regression model 2, which included laboratory data on the fourth day of hospitalization, the risk of prolonged LOS increased 1.384-fold (OR 2.384, 95% CI 1.195–4.757) in patients whose exacerbations occurred in autumn (day 1). Compared with patients with mMRC scale (day 1) scores of 0 to 1, a 1.394-fold elevation (OR 2.394, 95% CI 1.274–4.501) in risk was shown in those with scale scores of 2 to 4. In addition, the risk increased by 2.007-fold (OR 3.007, 95% CI 1.539–5.877) for patients who used corticosteroids during hospitalization (day 4) (Table 4).
In multivariate regression model 3, which included changes in laboratory data between the first and the fourth day of hospitalization, the results demonstrated that long-term home oxygen therapy (day 1) raised the risk of prolonged LOS 1.396-fold (OR 2.396, 95% CI 1.310–4.383). For each point increase in the Charlson index (day 1), the risk increased 0.546-fold (OR 1.546, 95% CI 1.093–2.187). For each 1×109/L decrease in ΔPLT, the risk increased 0.006-fold (OR 1.006, 95% CI 1.000–1.012). In addition, the risk increased 1.119-fold (OR 2.119, 95% CI 1.185–3.790) for every 1 μg/L decrease in ΔPCT (Table 4).
DEVELOPMENT OF THE FINAL MODEL:
Variables with statistical significance in models 1, 2, and 3 were then included in the final prediction model. The model suggested that patients who used corticosteroids during hospitalization had a 2.514-fold increased risk (OR 3.514, 95% CI 1.677–7.362) of prolonged LOS. For every 1 mmol/L increase in HCO3−, the risk increased 0.069-fold (OR 1.069, 95% CI 1.000–1.142). For every increase in pH, the risk decreased 0.574-fold (OR 0.426, 95% CI 0.246–0.737). In addition, the risk increased 0.007-fold (OR 1.007, 95% CI 1.001–1.014) for every 1×109/L decrease in ΔPLT, and the risk increased 1.021-fold (OR 2.021, 95% CI 1.081–3.778) for every 1 μg/L decrease in ΔPCT (Table 5).
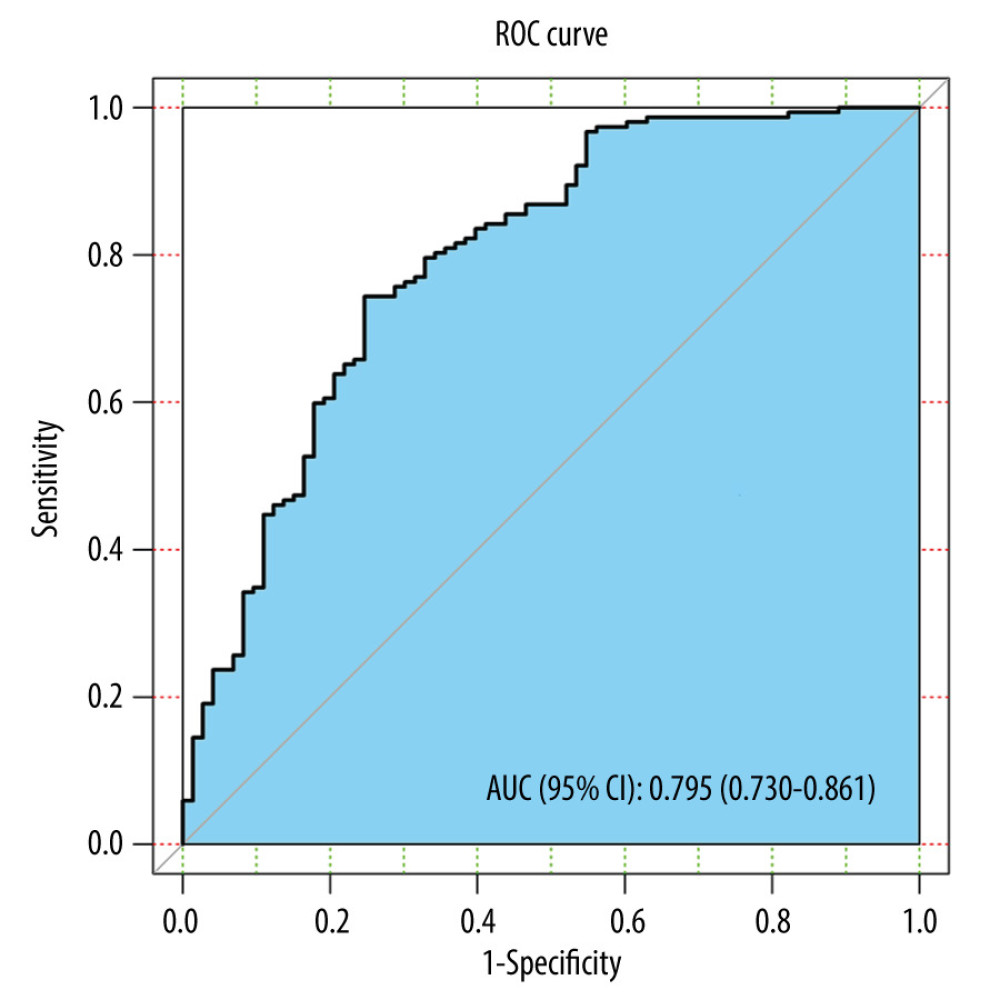
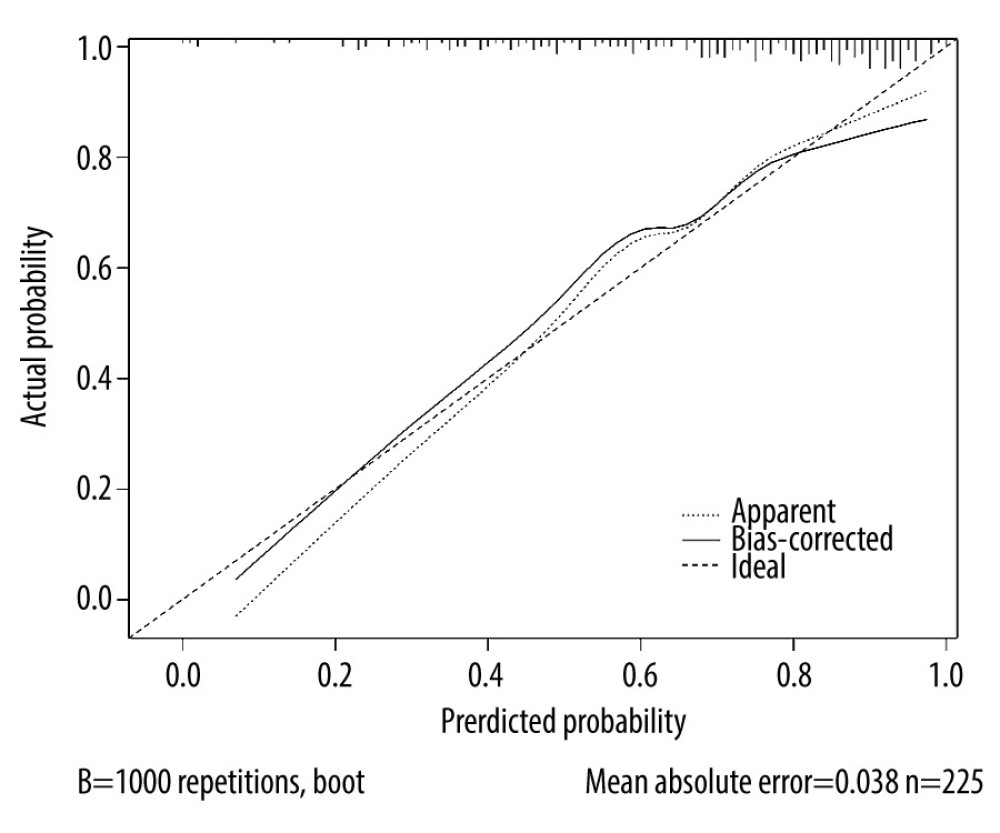
According to the ROC curve, the AUC of the combined prediction model was 0.795 (95% CI 0.730–0.861), with a sensitivity of 0.743 (95% CI, 0.674–0.813) and a specificity of 0.753 (95% CI, 0.65–0.852), which suggested the good discrimination of our model (Figure 1, Table 6). The results of the Hosmer-Lemeshow test (χ2=9.648, P=0.291) indicated the good calibration of the model. The calibration curve of the model is shown in Figure 2.
Discussion
In the present study, we aimed to develop a clinical prediction model for the risk of prolonged LOS >7 days in patients with AECOPD. Several factors were found to be independently associated with the increased risk of prolonged LOS, including use of corticosteroids during hospitalization, elevated HCO3−, decreased pH, and reduced changes in PLTs and PCT between the fourth and first day of hospitalization. A risk prediction model including these factors had an AUC of 0.795, suggesting the good discrimination of our model. The Hosmer-Lemeshow test also showed the good calibration of the model, confirming the model’s good predictive performance.
Owing to the clinical fact that 7 days was the median LOS of our study population, and based on previous studies that proposed the medically required LOS for patients with AECOPD should be between 6 and 7 days based on clinical characteristics [26] and over 7 days should be regarded as prolonged LOS [15], we chose the cutoff of 7 days for LOS in this study, although different cut-offs were used in other studies [14,17,19,20,27]. Further, the fourth day of hospitalization was selected to repeat the assessment of the same laboratory variables as those on the first day of hospitalization as well as corticosteroid and antibiotic use, because the efficacies of corticosteroids and antibiotics are generally evaluated 72 h after use in clinical practice, which was on the fourth day of hospitalization in this study. Moreover, in the present study, there were differences in the laboratory data between the fourth and first day of hospitalization.
The impact of HCO3− and pH at the time of admission on prolonged LOS have scarcely been investigated in patients with AECOPD. In the present study, an increase of HCO3− and a decrease of pH were associated with an increased risk of prolonged LOS. It was reported that a high PaCO2 measured in the Emergency Department was associated with prolonged LOS [20], which could support our findings in some way. According to Wang et al, PaCO2 and other blood-gas variables reflect the severity of respiratory failure [20]. Our results could be interpreted that due to upper respiratory tract obstruction, respiratory dysfunction, and carbon dioxide accumulation in the body, patients with COPD are prone to respiratory acidosis with an increase in HCO3− and a decrease in pH, which are associated with the occurrence of AECOPD and might contribute to a prolonged LOS. We recommend that clinicians should be cautious about a change in blood-gas variables, such as HCO3− and pH, in patients with COPD to identify those with a high risk of prolonged AECOPD LOS for early intervention.
We also found an association between the use of corticosteroids during hospitalization and the risk of prolonged LOS. The possible reason is that although the corticosteroids could inhibit the excessive inflammatory response, it could also lead to the spread of infection and other adverse effects, such as gastrointestinal bleeding and increased blood glucose [28,29]. Similarly, since the exacerbation of COPD and its treatment with corticosteroids can worsen comorbidities such as diabetes [30], it is understandable that a prolonged stay is needed to get these comorbid conditions under control [20]. Here, we suggested the proper use of corticosteroids during hospitalization to improve the outcome of AECOPD and shorten the hospital stay.
Currently, limited statistical models have been established that can effectively predict the risk of prolonged LOS in patients with AECOPD, which is based on varying definitions of prolonged LOS and different predictors [14,17,20]. There is no model to predict prolonged LOS for the Chinese population. In the present study, we developed a promising prediction model with good calibration and discrimination using data from a Chinese hospital comprising demographic, laboratory, and environmental variables. Increased knowledge of predictors and earlier prediction of the risk of prolonged LOS may help clinicians provide better and more timely treatment and intervention, which could shorten hospital stay, reduce the disease burden of patients, and improve the outcomes of AECOPD.
There are limitations in our study. First, the study may be limited by its retrospective design, and some important features, such as heart failure, stroke, need for mechanical ventilation, Intensive Care Unit admission, and even mortality, were not recorded in the hospital. Second, the sample size in our study was relatively small, and a prospective study with larger sample size is needed. Third, although the predictive ability of our model was good, external validation is preferred for improving the reliability of the model. Fourth, phenotyping of the groups was not comprehensive: the severity of AECOPD, the microbiological origin of AECOPD, and spirometric data were not available.
Conclusions
In the present study, we identified a group of predictors that were independently associated with prolonged LOS of more than 7 days. A clinical prediction model comprising these variables was then developed with good predictive performance. It may help clinicians identify patients with a higher risk of prolonged LOS and clarify which variables they should closely monitor when making treatment decisions to shorten hospital stay and improve the burden and outcomes of AECOPD for patients with COPD.
Tables
Table 1. Differences in baseline characteristics.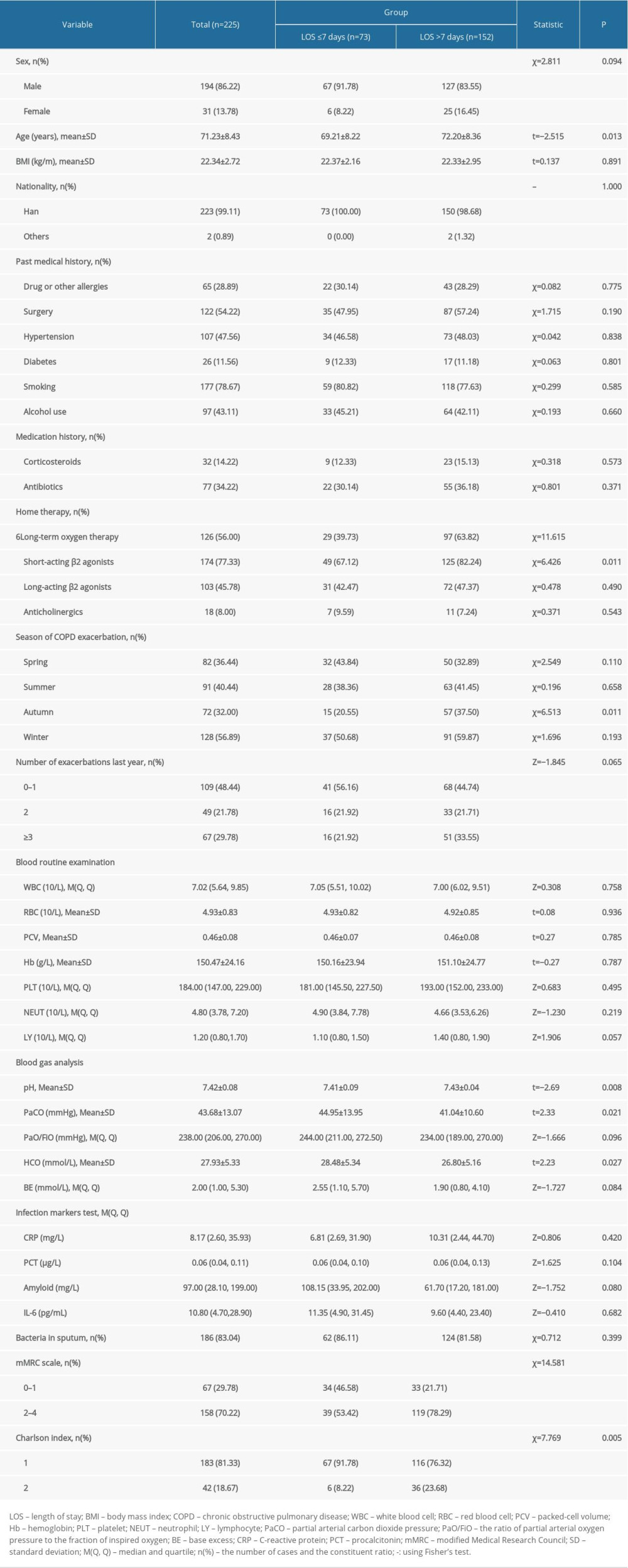 Table 2. Differences in characteristics on the fourth day of hospitalization.
Table 2. Differences in characteristics on the fourth day of hospitalization.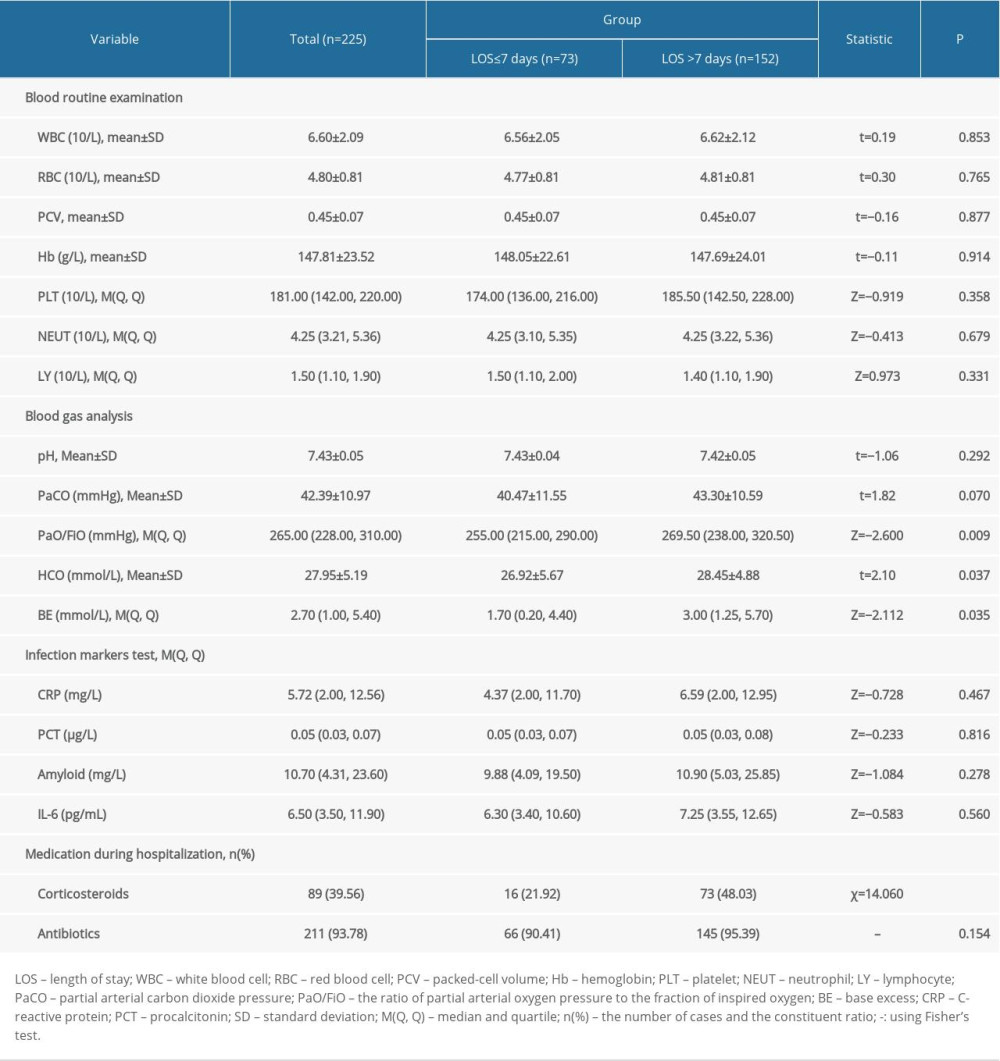 Table 3. Differences in characteristic changes between the fourth and first day.
Table 3. Differences in characteristic changes between the fourth and first day.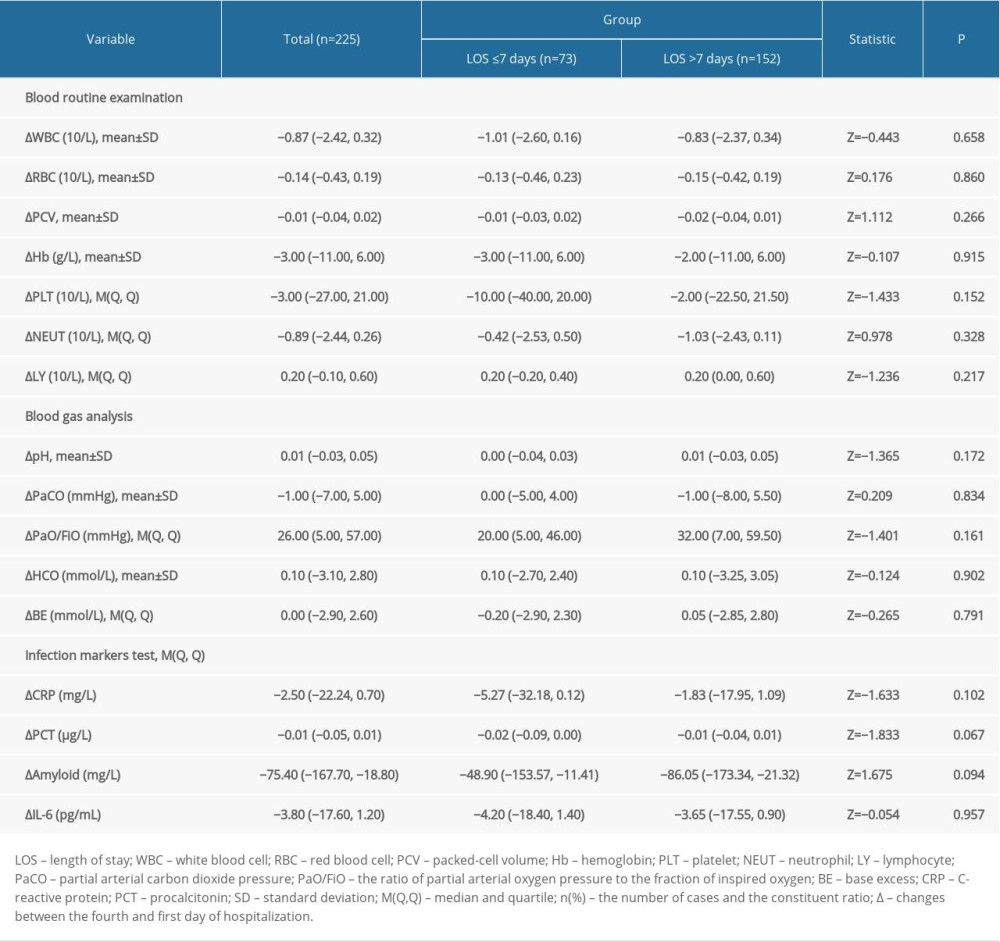 Table 4. Variables associated with the risk of prolonged LOS in models 1, 2, and 3.
Table 4. Variables associated with the risk of prolonged LOS in models 1, 2, and 3.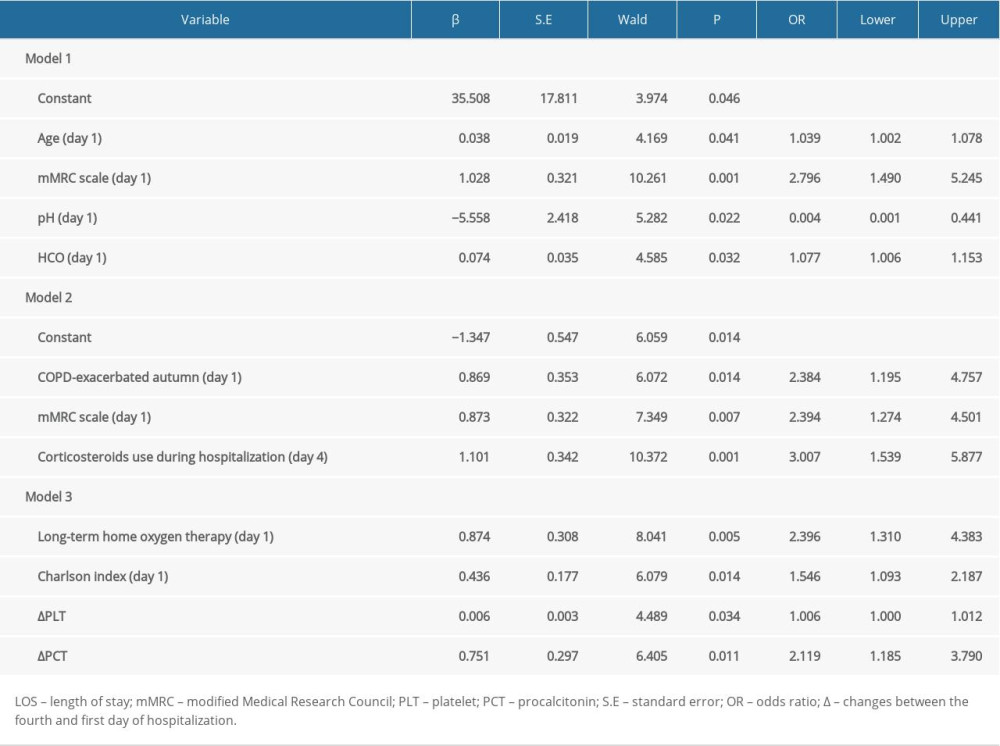 Table 5. Variables associated with the risk of prolonged LOS in the final model.
Table 5. Variables associated with the risk of prolonged LOS in the final model. Table 6. Predictive value of the predictors for prolonged LOS in the final model.
Table 6. Predictive value of the predictors for prolonged LOS in the final model.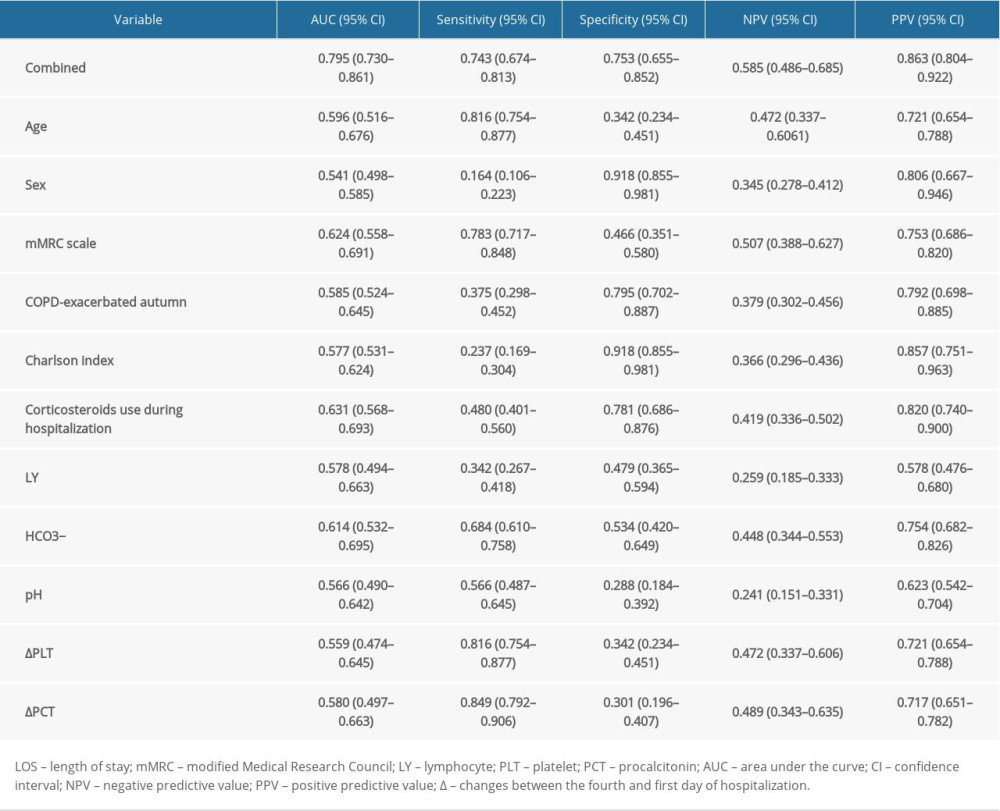
References
1. Labaki WW, Rosenberg SR, Chronic obstructive pulmonary disease: Ann Intern Med, 2020; 173; ITC17-32
2. Barnes PJ, Burney PG, Silverman EK, Chronic obstructive pulmonary disease: Nat Rev Dis Primers, 2015; 1; 15076
3. GBD Chronic Respiratory Disease Collaborators, Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017: Lancet Respir Med, 2020; 8; 585-96
4. Rabe KF, Watz H, Chronic obstructive pulmonary disease: Lancet, 2017; 389; 1931-40
5. Pollok J, van Agteren JE, Esterman AJ, Psychological therapies for the treatment of depression in chronic obstructive pulmonary disease: Cochrane Database Syst Rev, 2019; 3; CD012347
6. Vogelmeier CF, Criner GJ, Martinez FJ, Global Strategy for the diagnosis, management, and prevention of chronic obstructive lung disease. 2017 Report. GOLD Executive Summary: Am J Respir Crit Care Med, 2017; 195; 557-82
7. Wedzicha JA, Seemungal TA, COPD exacerbations: Defining their cause and prevention: Lancet, 2007; 370; 786-96
8. Whittaker Brown SA, Braman S, Recent advances in the management of acute exacerbations of chronic obstructive pulmonary disease: Med Clin North Am, 2020; 104; 615-30
9. Wedzicha JA, Singh R, Mackay AJ, Acute COPD exacerbations: Clin Chest Med, 2014; 35; 157-63
10. Ritchie AI, Wedzicha JA, Definition, causes, pathogenesis, and consequences of chronic obstructive pulmonary disease exacerbations: Clin Chest Med, 2020; 41; 421-38
11. Press VG, Konetzka RT, White SR, Insights about the economic impact of chronic obstructive pulmonary disease readmissions post implementation of the hospital readmission reduction program: Curr Opin Pulm Med, 2018; 24; 138-46
12. Niewoehner DE, The impact of severe exacerbations on quality of life and the clinical course of chronic obstructive pulmonary disease: Am J Med, 2006; 119; 38-45
13. Howcroft M, Walters EH, Wood-Baker R, Action plans with brief patient education for exacerbations in chronic obstructive pulmonary disease: Cochrane Database Syst Rev, 2016; 12; CD005074
14. Quintana JM, Unzurrunzaga A, Garcia-Gutierrez S, Predictors of hospital length of stay in patients with exacerbations of COPD: A cohort study: J Gen Intern Med, 2015; 30; 824-31
15. Crisafulli E, Ielpo A, Barbeta E, Clinical variables predicting the risk of a hospital stay for longer than 7 days in patients with severe acute exacerbations of chronic obstructive pulmonary disease: A prospective study: Respir Res, 2018; 19; 261
16. Diamantea F, Kostikas K, Bartziokas K, Prediction of hospitalization stay in COPD exacerbations: The AECOPD-F score: Respir Care, 2014; 59; 1679-86
17. Tsimogianni AM, Papiris SA, Stathopoulos GT, Predictors of outcome after exacerbation of chronic obstructive pulmonary disease: J Gen Intern Med, 2009; 24; 1043-48
18. Ruparel M, López-Campos JL, Castro-Acosta A, Understanding variation in length of hospital stay for COPD exacerbation: European COPD audit: ERJ Open Res, 2016; 2(1); 00034-2015
19. de la Iglesia F, Valiño P, Pita S, Factors predicting a hospital stay of over 3 days in patients with acute exacerbation of chronic obstructive pulmonary disease: J Intern Med, 2002; 251; 500-7
20. Wang Y, Stavem K, Dahl FA, Factors associated with a prolonged length of stay after acute exacerbation of chronic obstructive pulmonary disease (AECOPD): Int J Chron Obstruct Pulmon Dis, 2014; 9; 99-105
21. Agboado G, Peters J, Donkin L, Factors influencing the length of hospital stay among patients resident in Blackpool admitted with COPD: A cross-sectional study: BMJ Open, 2012; 2(5); e000869
22. Díaz-Peromingo JA, Grandes-Ibáńez J, Fandińo-Orgeira JM, Predicting factors contributing to length of stay in hospitalized chronic obstructive pulmonary disease (COPD) patients: The role of the emergency room: Acta Medica (Hradec Kralove), 2004; 47; 29-32
23. Estirado C, Ceccato A, Guerrero M, Microorganisms resistant to conventional antimicrobials in acute exacerbations of chronic obstructive pulmonary disease: Respir Res, 2018; 19; 119
24. Wilkinson TMA, Aris E, Bourne S, A prospective, observational cohort study of the seasonal dynamics of airway pathogens in the aetiology of exacerbations in COPD: Thorax, 2017; 72; 919-27
25. Liu H, Zheng D, Lin Y, Association of sputum microbiome with clinical outcome of initial antibiotic treatment in hospitalized patients with acute exacerbations of COPD: Pharmacol Res, 2020; 160; 105095
26. Mushlin AI, Black ER, Connolly CA, The necessary length of hospital stay for chronic pulmonary disease: JAMA, 1991; 266; 80-83
27. García-Sanz MT, González-Barcala FJ, Cánive-Gómez JC, Prolonged stay predictors in patients admitted with chronic obstructive pulmonary disease acute exacerbation: Lung India, 2018; 35; 316-20
28. Meijvis SC, Hardeman H, Remmelts HH, Dexamethasone and length of hospital stay in patients with community-acquired pneumonia: A randomised, double-blind, placebo-controlled trial: Lancet, 2011; 377; 2023-30
29. Caplan A, Fett N, Rosenbach M, Prevention and management of glucocorticoid-induced side effects: A comprehensive review: Gastrointestinal and endocrinologic side effects: J Am Acad Dermatol, 2017; 76; 11-16
30. Parappil A, Depczynski B, Collett P, Effect of comorbid diabetes on length of stay and risk of death in patients admitted with acute exacerbations of COPD: Respirology, 2010; 15; 918-22
Figures
Tables
Table 1. Differences in baseline characteristics.Table 2. Differences in characteristics on the fourth day of hospitalization.Table 3. Differences in characteristic changes between the fourth and first day.Table 4. Variables associated with the risk of prolonged LOS in models 1, 2, and 3.Table 5. Variables associated with the risk of prolonged LOS in the final model.Table 6. Predictive value of the predictors for prolonged LOS in the final model.Table 1. Differences in baseline characteristics.Table 2. Differences in characteristics on the fourth day of hospitalization.Table 3. Differences in characteristic changes between the fourth and first day.Table 4. Variables associated with the risk of prolonged LOS in models 1, 2, and 3.Table 5. Variables associated with the risk of prolonged LOS in the final model.Table 6. Predictive value of the predictors for prolonged LOS in the final model. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387