11 January 2024: Clinical Research
Predicting Acute Kidney Injury in Trauma Patients: Biomarkers as Early Indicators
Michal FrelichDOI: 10.12659/MSM.942271
Med Sci Monit 2024; 30:e942271






Abstract
BACKGROUND: Acute kidney injury (AKI) is a common cause of organ failure in patients after major trauma and is associated with increased morbidity and mortality. Early identification of patients at risk enables the implementation of a bundle of supportive care, which reduces the incidence of AKI. The primary objective of our study was to investigate whether the levels of biomarkers on admission predicted the onset of early AKI in patients with serious injuries.
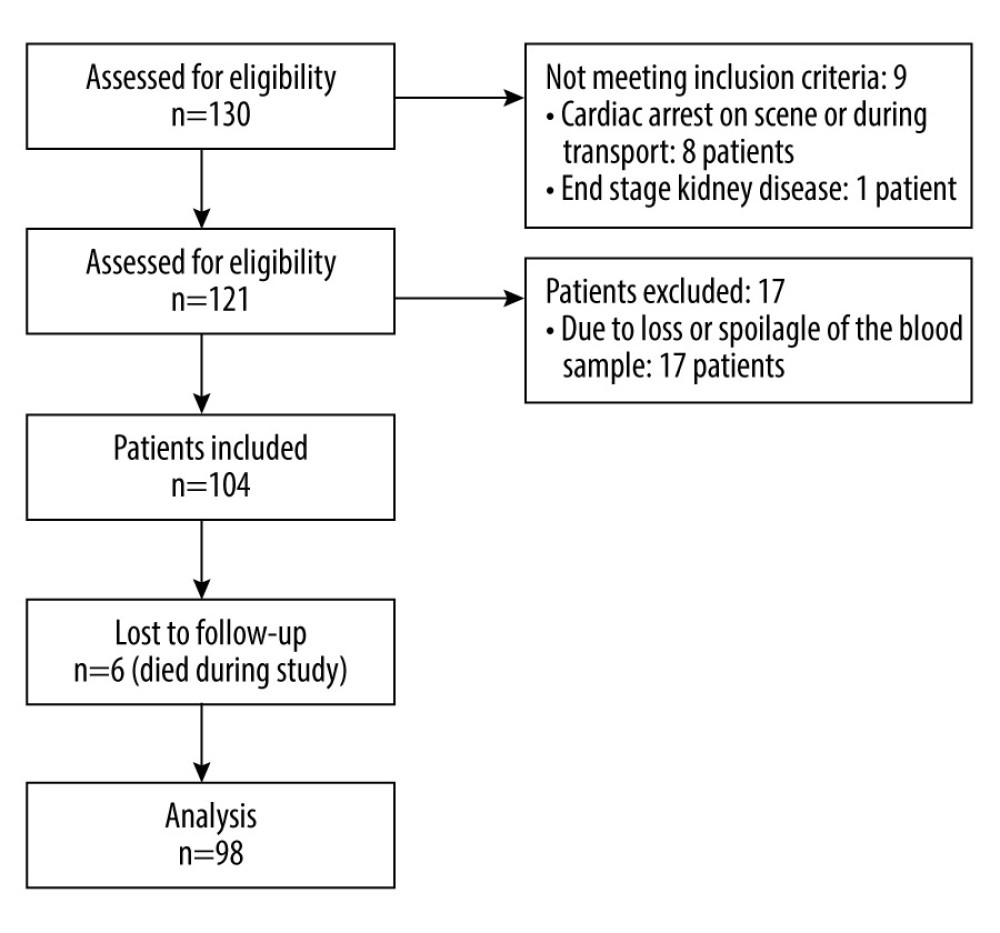
MATERIAL AND METHODS: This prospective observational study included 98 adult patients of both sexes with a serious injury (injury severity score >16). At admission, blood samples were taken, and creatinine, neutrophil gelatinase-associated lipocalin (NGAL), high mobility group box 1 (HMGB-1), and markers of rhabdomyolysis (creatine kinase, myoglobin) were evaluated. The patients were provided with standard resuscitation care, and the occurrence of AKI was monitored during the first 7 days after admission to the Intensive Care Unit, according to the Kidney Disease Improving Global Outcomes diagnostic criteria.
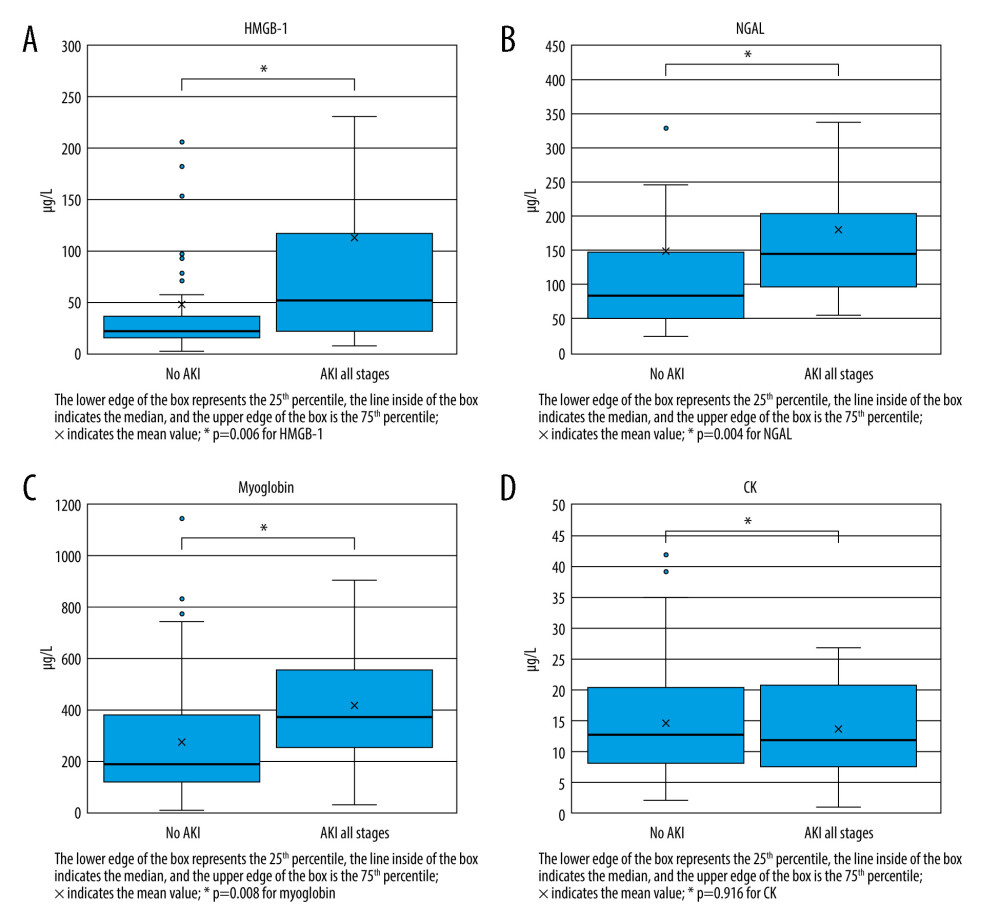
RESULTS: AKI occurred in 25 (25.5%) patients, in whom the admission levels of HMGB-1, NGAL, creatinine, and myoglobin were significantly higher than in non-AKI patients (48.3±98.4 vs 113.0±209.4 µg/L, P=0.006; 150.2±349.9 vs 181.4±152.2 µg/L, P=0.004; 83.1±20.8 vs 118.8±32.2 µmol/L, P<0.005; 2734.4±2214.5 vs 4182.3±2477.1 µg/L, P=0.008, respectively). Creatine kinase was 14.5±9.2 µkat/L in non-AKI patients and 13.7±7.9 µkat/L in AKI patients (P=0.916).
CONCLUSIONS: Admission levels of HMGB-1, NGAL, creatinine, and myoglobin predicted the risk of AKI in severely injured patients.
Keywords: Acute Kidney Injury, Multiple Trauma, biomarkers, adult, Female, Male, Humans, Creatinine, Lipocalin-2, Myoglobin, creatine kinase
Background
Acute kidney injury (AKI) is a common cause of organ failure in patients after major trauma, and it is independently associated with increased length of hospital stay and mortality [1–3]. Survivors of severe trauma with AKI can have variable recovery of kidney functions and be prone to developing chronic kidney disease (CKD) with late morbidity and mortality. AKI can also be a burden to the healthcare system, leading to substantially increased costs, especially those associated with renal replacement therapy. The incidence of trauma-induced AKI ranges from 1% to 50% depending on the definition of AKI and the study population [1,4]. The pathophysiology of post-traumatic AKI is complex; in addition to individual predisposition, the incidence of hemorrhage, tissue hypoxia, rhabdomyolysis, traumatic inflammation, second hits due to emergency surgery, and infections can impair renal function [5].
Within 45 min, severe injury and tissue hypoperfusion lead to a release of high mobility group box 1 (HMGB-1) into the blood circulation. HMBG-1, amphoterine, is a nuclear protein that interacts with nucleosomes, transcription factors, and histones. After trauma, it acts as an early trigger of sterile inflammation via activation of Toll-like receptor 4 and the receptor for advanced glycation end products. Activation of the systemic inflammatory response leads to a syndrome of multiorgan dysfunction, including AKI, the third leading cause of death in trauma patients after bleeding and traumatic brain injury [6,7]. Neutrophil gelatinase-associated lipocalin (NGAL) is a promising biomarker for the early detection of AKI [8]. Several studies have shown serum and urine NGAL levels to be useful as an early marker of AKI, particularly when the timing of the renal insult is known [9]. Rhabdomyolysis is characterized by the breakdown and necrosis of damaged skeletal muscle and subsequent release of its contents (eg, myoglobin and sarcoplasmic proteins) into the blood [10]. Several studies have reported rhabdomyolysis to be a risk factor for post-traumatic AKI, with increasing mortality. Myoglobin and creatine kinase (CK) are the most commonly used biomarkers for diagnosing and monitoring rhabdomyolysis severity. However, CK and myoglobin peaks are late markers of rhabdomyolysis severity, which makes them inappropriate for early prediction of AKI [11].
Even a mild renal injury or impairment of kidney function is a risk factor for excessive mortality. Therefore, it would be especially valuable to find biomarkers capable of predicting the risk of developing AKI early, ideally on admission [2,10]. The early prediction of trauma-induced AKI would allow the start of prophylactic interventions to limit kidney injury and improve the outcomes of severely injured patients [11].
The primary objective of our study was to investigate whether the admission levels of biomarkers of renal damage, specifically creatinine, NGAL, biomarker of activation of the systemic inflammatory response (HMGB-1), and markers of rhabdomyolysis (CK, myoglobin), can predict the onset of early AKI in patients with severe injury. The secondary objective was to assess the ability to predict AKI according to the mentioned markers within 24 h of admission. The tertiary objective was a comparison of admission levels of CK and myoglobin in the prediction of AKI.
Material and Methods
SAMPLE COLLECTION AND MEASUREMENTS:
Within 10 min of admission to the Emergency Department, in addition to standard laboratory tests, 2 blood samples were taken in collection tubes with ethylenediamine tetra acetic acid as an anticoagulant agent before the administration of any fluid resuscitation. The blood samples were immediately transferred to the central laboratory, centrifuged, and stored at −80°C. HMBG-1 was analyzed using the HMGB-1 ELISA test kit (Biovendor LM), and NGAL with the NGAL test reagent kit (Biovendor LM) at the conclusion of the study by a researcher who was blinded to all patients’ data. Other monitored laboratory parameters (creatinine, CK, and myoglobin) were evaluated within 1 h of sending the blood samples. The same tests were performed (except for HMGB-1) within 24 h of the patient’s admission to the hospital. Serum creatinine was collected every morning for 5 days into the patients’ Intensive Care Unit (ICU) stay. All measurements were performed in accordance with the manufacturers’ instructions. All data were collected and registered by an independent staff member using a case report form. This study closely followed the guidelines for Good Clinical Practice. All patients in the study underwent whole-body computed tomography with contrast agent to determine the injury severity in the initial phase of care immediately after the primary survey and stabilization of vital functions. The ISS was used as a measure of the degree of tissue injury [12].
DIAGNOSIS OF AKI:
AKI was assessed according to the Kidney Disease Improving Global Outcomes (KDIGO) classification based on the maximum creatinine level during the first 7 days of the ICU stay. The baseline creatinine level of trauma patients was unknown. As recommended in the KDIGO guidelines, we calculated the baseline creatinine value according to the Modification of Diet in Renal Disease formula, with a glomerular filtration rate of 75 mL/min per 1.73 m2. We also considered, according Tarazona et al, 2 other options to determine baseline creatinine: admission creatinine level and the lowest creatinine level over the first 5 days of admission or until discharge, whichever came first [11].
STATISTICAL ANALYSIS:
Quantitative variables were expressed according to distribution as means with standard deviation or medians with the interquartile range, and categorical variables as counts with percentages. The categorical variables were statistically analyzed using the Pearson’s chi-squared test or the Fisher’s exact test. Non-normally distributed variables were compared with the Mann-Whitney test and Wilcoxon signed-rank test, as appropriate. We made receiver operating characteristics (ROC) curves at 2 time points (at admission and after 24 h) for different thresholds of levels of biomarkers for the prediction of AKI. The value maximizing the Youden index (sensitivity+specificity-1) was considered to be the best threshold. Data were analyzed using IBM SPSS V26 software. A
Results
BIOMARKERS COLLECTED DURING ADMISSION:
The admission values for HMGB-1, NGAL, creatinine, and myoglobin were significantly higher in AKI patients than in non-AKI patients (48.3±98.4 vs 113.0±209.4 μg/L, P=0.006; 150.2±349.9 vs 181.4±152.2 μg/L, P=0.004; 83.1±20.8 vs 118.8±32.2 μmol/L, P<0.005; and 2734.4±2214.5 vs 4182.3±2477.1 μg/L, P=0.008, respectively; Table 2 and Figure 2). The level of CK on admission was not significantly different between non-AKI and AKI patients (14.5±9.2 μkat/L and 13.7±7.9 μkat/L, respectively; P=0.916). Patients with AKI also had higher initial ISS (P<0.0005) and lactate values (P<0.0005), as shown in Table 2.
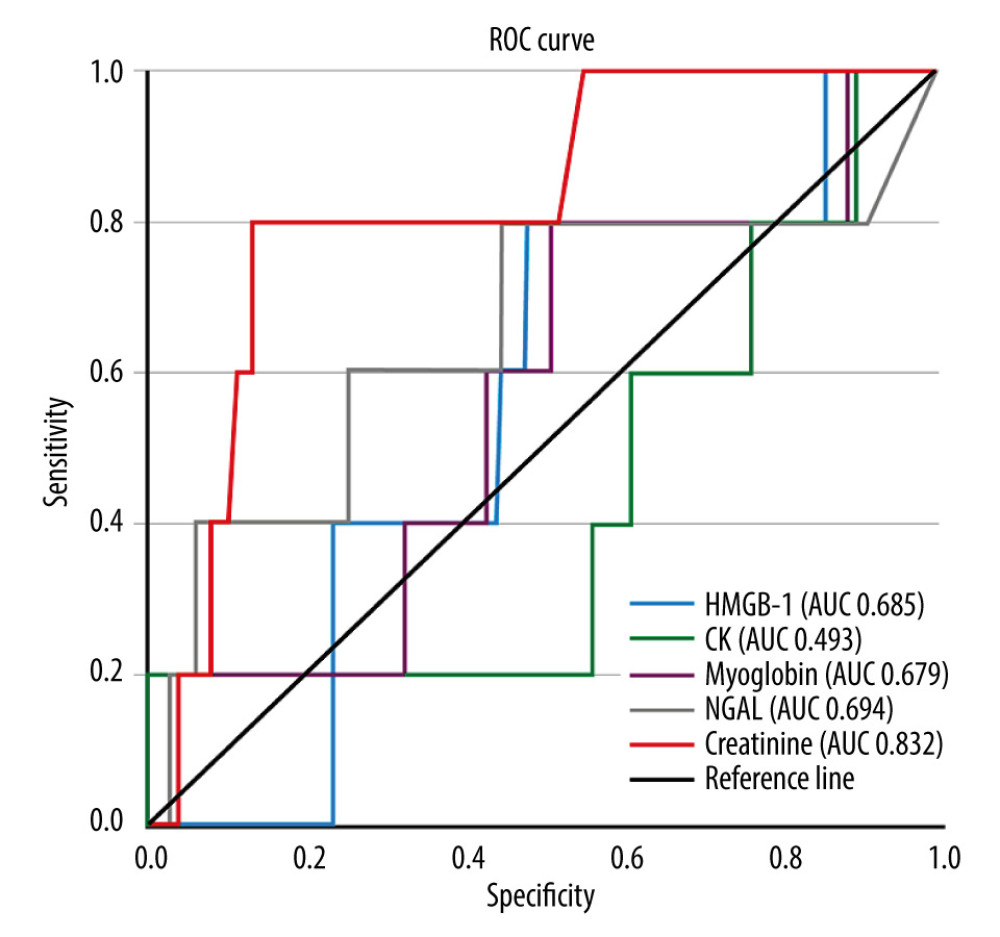
From the admission levels according to the area under the ROC curve (AUC), the most reliable predictors of AKI were creatinine and NGAL (AUC 0.83, 95% CI 0.74–0.93 and AUC 0.69, 95% CI 0.58–0.80, respectively). The creatinine level at admission had 76% sensitivity and 82% specificity for predicting AKI of any stage, with a cut-off level of 99 μmol/L. NGAL had 68% sensitivity and 69% specificity, with a cut-off level of 132.6 μg/L. On the basis of the AUC analysis, the HMGB-1 level at admission predicted AKI with a cut-off level of 59.7 μg/L, sensitivity of 48%, and specificity of 88% (AUC 0.69, 95% CI 0.56–0.82). This was followed by myoglobin (AUC 0.68, 95% CI 0.55–0.80), with a cut-off level of 3009.85, sensitivity of 72%, and specificity of 66%. The least sensitive admission biomarker in the prediction of AKI was CK (Figure 3 and Table 3).
BIOMARKERS COLLECTED 24 H AFTER ADMISSION:
The levels of NGAL, creatinine, and CK at 24 h after admission were higher in patients in the AKI group (Table 2). Of the biomarkers collected within 24 h of admission, the most reliable predictors of early AKI were creatinine (AUC 0.97, 95% CI 0.94–1.00) and NGAL (AUC 0.87, 95% CI 0.78–0.96). Creatinine predicted the occurrence of AKI with a sensitivity of 92% and specificity of 99%, with a cut-off >111 μmol/L. The sensitivity of NGAL to predict AKI was 80% and the specificity 88%, with a cut-off >126.5 μg/L. This was followed by myoglobin (AUC 0.81, 95% CI 0.70–0.92) with a sensitivity of 64%, specificity of 90%, and a cut-off >2654 μg/L. In the prediction of AKI according to biomarkers collected after 24 h, the least sensitive predictor was CK (AUC 0.66, 95% CI 0.54–0.78) with a sensitivity of 80%, specificity of 48%, and a cut-off >38.6 μkat/L (Table 3). According to statistical analysis of ROC curves, predictive values of NGAL, myoglobin, creatinine, and CK increased after collection in 24 h compared with admission values (P=0.01, P=0.013, P=0.002, and P=0.015, respectively).
Discussion
AKI can result from the actions of several renal aggressions after trauma, and it is very difficult to isolate the leading cause in clinical practice [5]. The delay in elevation of creatinine until approximately 24 to 48 h after AKI makes this standard renal function test inappropriate for the early diagnosis of AKI [13]. We conducted a prospective single-center observational study to evaluate the admission levels of NGAL, HMGB-1, creatinine, myoglobin, and CK for early prediction of AKI in patients with major trauma. Among the key findings of this study were that the admission values of HMGB-1, NGAL, creatinine, and myoglobin, but not CK, were significantly higher in patients who developed AKI during the 7-day stay in the ICU than in patients without this organ dysfunction. Second, the predictive value of the selected biomarkers increased when collected at 24 h. Third, of the monitored biomarkers of rhabdomyolysis, myoglobin was an earlier and more sensitive predictor of AKI onset in severely injured patients than was CK.
Early uncontrolled and protracted systemic inflammatory response syndrome has been reported to a be a risk factor for “sterile” organ failure, including AKI. In addition to blood loss and tissue hypoperfusion, a key mechanism leading to the triggering of a systemic inflammatory response is the release of HMBG-1 and other molecules into the bloodstream, collectively called damage-associated molecular patterns [7]. In our study, we observed significantly higher admission levels of HMGB-1 in patients who developed early AKI, with a cut-off of 59.7 μg/L for the prediction of AKI. These higher HMGB-1 levels in patients who developed AKI also corresponded with higher interleukin 6 levels. Recent studies reported that the level of HMGB-1 at 30 min after trauma correlates with the amplitude of immune activation and systemic inflammatory response syndrome; therefore, the values can be used to predict the risk of developing AKI [7]. However, in our study, the level of HMGB-1 had low sensitivity for predicting AKI, which we explain by the multifactorial etiology of the development of AKI in severely injured patients, in whom the high degree of systemic inflammatory response may not be the main cause of renal damage. Our results are in agreement with the work of Cohen et al, who demonstrated significantly higher levels of HMGB-1 in patients who developed acute lung injury and AKI than did patients who did not experience such organ failure. Interestingly, the same author demonstrated a correlation between higher HMGB-1 levels and coagulopathy, which may be another key factor in the pathogenesis of multiorgan failure [7].
NGAL, an iron-transporting protein covalently bound to gelatinase, is one of the most upregulated transcripts in the kidney very early after acute injury. Previous studies have reported that serum and urine NGAL levels are a useful tool for early detection of AKI, especially when the timing of the renal insult is known, such as with post-cardiac surgery or radiocontrast exposure [9]. In our study, serum NGAL levels on admission were higher in patients with early onset AKI than in patients without this organ dysfunction. After 24 h, the predictive value of NGAL increased, with an AUC of 0.87. Our results are in agreement with those of Makris et al, who reported that urinary NGAL taken on the first day of the injury is a reliable predictor of early AKI in multi-trauma patients [14]. Li et al achieved similar results with the determination of urinary NGAL to predict early AKI in patients with traumatic brain injury [15].
The ability to predict rhabdomyolysis-induced AKI is critical because the leakage of intracellular muscular components into the blood is thought to be one of the leading causes of AKI, and rhabdomyolysis has been suggested to contribute to 5% to 25% of all cases of AKI [16]. In our study, we demonstrated that, of the biomarkers of rhabdomyolysis, myoglobin was an earlier and more sensitive predictor of the onset of AKI in severely injured patients than was CK. Patients who developed AKI had a significantly increased level of myoglobin at admission than did patients without AKI, whereas the admission level of CK did not differ between the 2 groups of patients. The admission level of myoglobin >3010 predicted the occurrence of AKI with a sensitivity of 72% and specificity of 66%. There are several hypotheses to explain our results. First, the pathophysiology of rhabdomyolysis-induced AKI is thought to be triggered predominantly by myoglobin with direct renal toxicity, vasoconstriction, and tubular obstruction, whereas CK has no reported effect on the kidneys [11,16]. Therefore, admission myoglobin levels can more precisely reflect the renal toxicity of rhabdomyolysis. Second, unlike CK release, myoglobin release does not depend on lymphatic transport and is more quickly transported into the bloodstream, which makes it more accurate as an early marker for occurrence of AKI [11].
Our results are in agreement with those of Tarazona et al, who also demonstrated that admission myoglobin level was more accurate in the prediction of AKI after major trauma in their retrospective study of 857 trauma patients [11]. Other studies have shown an association of myoglobin and CK concentrations with the occurrence of AKI in patients with rhabdomyolysis, but these studies only assessed the peak concentrations of these biomarkers [11,17,18]. Although both peak values relate to the magnitude of intramuscular content release and, therefore, are surrogates of rhabdomyolysis severity, they occur only late after the trauma [16]. For this reason, they cannot be used for early prediction of post-traumatic AKI, which commonly develops within 48 h after trauma [5].
Early identification of patients at high risk of developing AKI is crucial, as it allows, according to the KDIGO guidelines, the implementation of a bundle of supportive measures intended to reduce the incidence of AKI. The key elements included in this bundle are close monitoring of serum creatinine and urine excretion, optimization of hemodynamic parameters and volume status, establishment of functional hemodynamic monitoring, discontinuation of all nephrotoxic agents, avoidance of hyperglycemia, and consideration of alternatives to radiocontrast agents [19,20]. Application of the bundle of preventive measures reduces the incidence of AKI in high-risk patients [20].
We acknowledge certain limitations in this study. First, this study enrolled patients from a single center. Data from a multicenter study would be more generalizable. In addition, optimal cut-offs are given for patients spending 38 min in the pre-hospital setting; thus, the results of our study may not match those of another trauma system with very different pre-hospital times. Furthermore, AKI was assessed from the level of creatinine only and not by considering the diuresis; therefore, the occurrence of AKI may be underestimated.
Conclusions
HMGB-1, NGAL, and myoglobin levels at admission can predict the risk of AKI in severely injured patients. Early identification of these patients allows the initiation of preventive measures aimed at reducing the occurrence of kidney dysfunction.
References
1. Perkins ZB, Captur G, Bird R, Trauma induced acute kidney injury: PLoS One, 2019; 14(1); e0211001
2. Harrois A, Libert N, Duranteau J, Acute kidney injury in trauma patients: Curr Opin Crit Care, 2017; 23(6); 447-56
3. Bihorac A, Delano MJ, Schold JD, Incidence, clinical predictors, genomics, and outcome of acute kidney injury among trauma patients: Ann Surg, 2010; 252(1); 158-65
4. Søvik S, Isachsen MS, Nordhuus KM, Acute kidney injury in trauma patients admitted to the ICU: A systematic review and meta-analysis: Intensive Care Med, 2019; 45(4); 407-19
5. Harrois A, Soyer B, Gauss TTraumabase Group, Prevalence and risk factors for acute kidney injury among trauma patients: A multicenter cohort study: Crit Care, 2018; 22(1); 344
6. Cohen MJ, Brohi K, Calfee CS, Early release of high mobility group box nuclear protein 1 after severe trauma in humans: Role of injury severity and tissue hypoperfusion: Crit Care, 2009; 13(6); R174
7. Vourc’h M, Roquilly A, Asehnoune K, Trauma-induced damage-associated molecular patterns-mediated remote organ injury and immunosuppression in the acutely ill patient: Front Immunol, 2018; 9; 1330
8. Devarajan P, NGAL in acute kidney injury: from serendipity to utility: Am J Kidney Dis, 2008; 52(3); 395-99
9. Cruz DN, de Cal M, Garzotto F, Plasma neutrophil gelatinase-associated lipocalin is an early biomarker for acute kidney injury in an adult ICU population: Intensive Care Med, 2010; 36(3); 444-51
10. Makris K, Spanou L, Acute kidney injury: Definition, pathophysiology and clinical phenotypes: Clin Biochem Rev, 2016; 37(2); 85-98
11. Tarazona V, Figueiredo S, Hamada S, Admission serum myoglobin and the development of acute kidney injury after major trauma: Ann Intensive Care, 2021; 11(1); 140
12. Baker SP, O’Neill B, Haddon W, Long WB, The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care: J Trauma, 1974; 14(3); 187-96
13. Katz N, Ronco C, Acute kidney stress – a useful term based on evolution in the understanding of acute kidney injury: Crit Care, 2016; 20; 23
14. Makris K, Markou N, Evodia E, Urinary neutrophil gelatinase-associated lipocalin (NGAL) as an early marker of acute kidney injury in critically ill multiple trauma patients: Clin Chem Lab Med, 2009; 47(1); 79-82
15. Li N, Zhao WG, Xu FL, Neutrophil gelatinase-associated lipocalin as an early marker of acute kidney injury in patients with traumatic brain injury: J Nephrol, 2013; 26(6); 1083-88
16. El-Abdellati E, Eyselbergs M, Sirimsi H, An observational study on rhabdomyolysis in the intensive care unit. Exploring its risk factors and main complication: acute kidney injury: Ann Intensive Care, 2013; 3(1); 8
17. Byerly S, Benjamin E, Biswas S, Peak creatinine kinase level is a key adjunct in the evaluation of critically ill trauma patients: Am J Surg, 2017; 214(2); 201-6
18. Raju NA, Rao SV, Joel JC, Predictive value of serum myoglobin and creatine phosphokinase for development of acute kidney injury in traumatic rhabdomyolysis: Indian J Crit Care Med, 2017; 21(12); 852-56
19. Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Update Work Group, KDIGO 2017 Clinical practice guideline update for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease-mineral and bone disorder (CKD-MBD): Kidney Int Suppl, 2017; 7; 1-59 Erratum in: Kidney Int Suppl. 2017;7(3):e1
20. Meersch M, Volmering S, Zarbock A, Prevention of acute kidney injury: Best Pract Res Clin Anaesthesiol, 2017; 31(3); 361-70
Figures
Tables
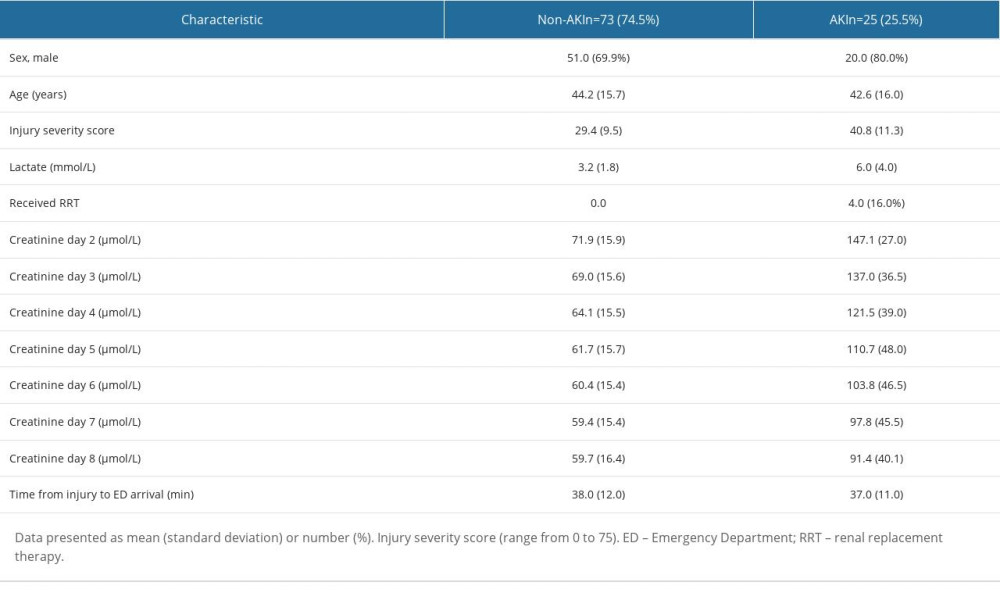 Table 1. General characteristics of the study population according to acute kidney injury (AKI) status.
Table 1. General characteristics of the study population according to acute kidney injury (AKI) status.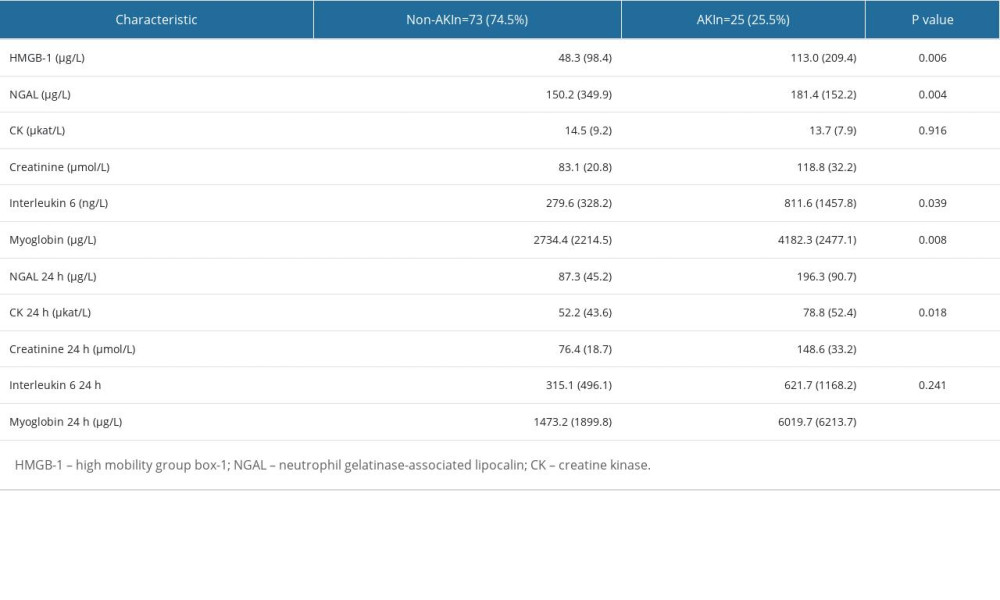 Table 2. Levels of biomarkers at 2 time points: admission and after 24 h.
Table 2. Levels of biomarkers at 2 time points: admission and after 24 h.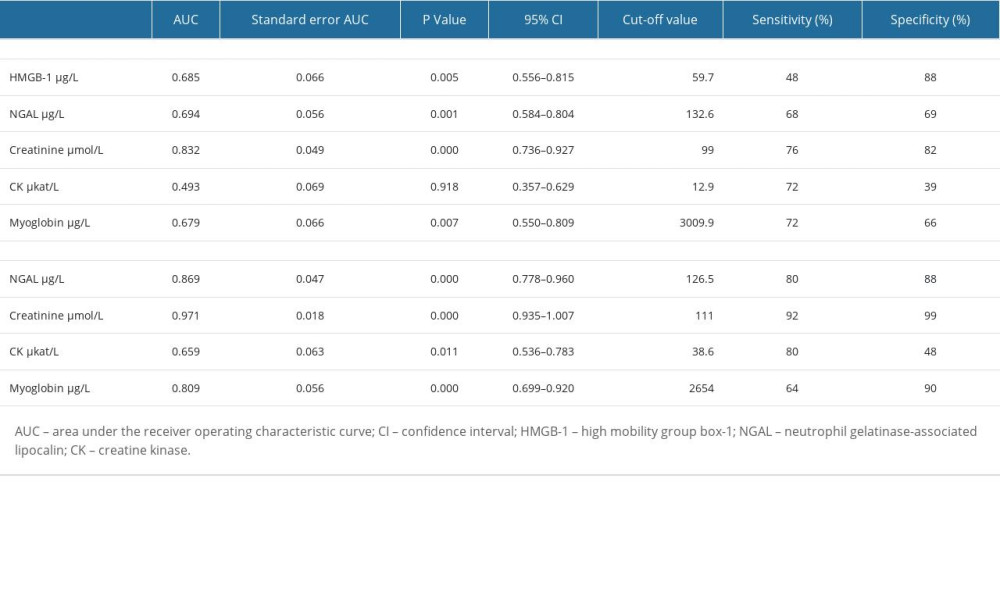 Table 3. Performance of admission biomarkers in predicting acute kidney injury (AKI).Table 1. General characteristics of the study population according to acute kidney injury (AKI) status.Table 2. Levels of biomarkers at 2 time points: admission and after 24 h.Table 3. Performance of admission biomarkers in predicting acute kidney injury (AKI).
Table 3. Performance of admission biomarkers in predicting acute kidney injury (AKI).Table 1. General characteristics of the study population according to acute kidney injury (AKI) status.Table 2. Levels of biomarkers at 2 time points: admission and after 24 h.Table 3. Performance of admission biomarkers in predicting acute kidney injury (AKI). In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387