04 September 2024: Clinical Research
Impact of COVID-19 on Sleep, Anxiety, and Depression Among Medical Call Center Staff: Insights from a January 2021 Study
Atakan YilmazDOI: 10.12659/MSM.945327
Med Sci Monit 2024; 30:e945327






Abstract
BACKGROUND: The COVID-19 outbreak emerged as a dual threat, effecting both the physical and mental well-being of healthcare staff. This study aimed to evaluate sleep quality using the Pittsburgh Sleep Quality Index (PSQI), levels of anxiety and depression using the Hospital Anxiety Depression Scale (HADS), and the significant influencing factors during COVID-19 pandemic in 284 workers in a medical call center in January 2021.
MATERIAL AND METHODS: Out of 443 pre-hospital care providers, 284 consented to participate. Data collection was done using an introductory information form, the PSQI for sleep quality, and the HADS for anxiety (HADS-A) and depression (HADS-D). Surveys were hosted on an online survey website and distributed via WhatsApp, with completed forms retrieved from the website.
RESULTS: Male sex (P=0.0001) and extended working hours in current workplace (P=0.017) were associated with higher HADS-A scores. Health problems, increased need for mental support, and poor job satisfaction correlated with lower HADS-D scores (P=0.025, P=0.005, P=0.0001, respectively) and higher PSQI scores (P=0.008, P=0.009, P=0.008, respectively). A moderately significant positive correlation was found between overall sleep quality and HADS-A (P=0.001, r=0.538) and HADS-D scores (P=0.001, r=0.493).
CONCLUSIONS: The pandemic significantly impacted the mental health and sleep quality of frontline healthcare personnel, necessitating the identification and mitigation of adverse psychosocial factors. Implementing and evaluating psychoeducational programs and establishing multidisciplinary mental health teams can provide for essential support and counseling, promoting the well-being of healthcare staff and ensuring effective emergency care.
Keywords: Anxiety, COVID-19, Depression, sleep quality, Health Personnel, Humans, Male, Female, adult, Surveys and Questionnaires, Call Centers, SARS-CoV-2, Middle Aged, Pandemics, Sleep, Mental Health, Job Satisfaction
Introduction
Caused by severe acute respiratory syndrome coronavirus 2, COVID-19 disease appeared in Wuhan, China, in December 2019 and was declared a pandemic by the World Health Organization in March 2020. By November 2021, as many as 628 million cases were detected worldwide, and the disease claimed the lives of almost 6.5 million people [1].
With the rapidly escalating number of cases of COVID-19 diagnosis, a wide range of measures were adopted to control and contain the further spread of the disease. Among these measures were lockdowns, mandatory wearing of masks, social distancing, regulations to allow working from home, obligatory quarantine practices for those coming from abroad, interruption of face-to-face education, and suspension of social activities such as theater, cinema, concert, and sports [2].
The physical symptoms, including shortness of breath, loss of taste and/or smell, headache, high fever, and others, brought by the pandemic may have also been accompanied by various psychosocial challenges. The most prevalent issues were xenophobia, financial challenges, separation from friends, and being away from loved ones during lockdown, in addition to fears of catching the disease, infecting the loved ones, losing them due to the disease, being stigmatized by society at large, and losing a job. All the aforementioned psychosocial factors coupled with sudden changes in daily routines can lead individuals to develop intense anxiety [3,4].
Individuals could also deny the pandemic and not comply with the precautions and regulations, depending on the psychosocial factors brought about by the disease [3]. Social media content also fueled public anxiety [5]. A study conducted in 2010 suggested that the anti-vaccination movement and negative news about the newly developed vaccines that appeared in the media during the H1N1 epidemic heightened concerns over the issue, deterring healthcare providers from being vaccinated [6]. In addition, the fact that a healthcare provider was also a member of his or her community should not go unnoticed. The burden that came with busy work in the frontline during the pandemic could have extended beyond physical symptoms and been followed by psychosocial effects [7]. Depression along with sleep and anxiety disorders came under close scrutiny in scholarly research focusing on the psychological effects experienced by healthcare staff involved in past epidemics, such as severe acute respiratory syndrome (SARS), Middle East respiratory syndrome, Ebola, and influenza [8]. In the SARS epidemic of 2003, for instance, depression and anxiety scores of healthcare staff working in high-risk zones were observed to be high even after 1 year [9]. In addition, depression rates were higher and sleep quality was lower in nurses working in a SARS unit, compared with that of their counterparts working in non-SARS units [10].
The need for healthcare staff in the COVID-19 pandemic became more prominent than the need for other service groups, as had been the case with previous epidemics such as SARS, Middle East respiratory syndrome, and influenza. A range of factors, such as working in the frontline, increased workload, fear of being infected and infecting relatives, social isolation, and limited access to medical and personal protective equipment, produced not only physical but also social and mental effects [11]. It is also documented that the COVID-19 breakout was responsible for the development of physical, social, and psychological disorders in pre-hospital care providers [12]. In a systematic review referring to the experiences of intensive care unit (ICU) nurses caring for patients with COVID-19, the findings revealed that ensuring the provision of high-quality patient care during the pandemic required a dedicated focus on addressing the psychological needs of and enhancing job satisfaction among ICU nurses [13].
By serving as the initial point of contact with infected and suspected cases, pre-hospital healthcare providers play a pivotal role in delivering care to patients outside the hospital setting. They are also tasked with transporting these patients to hospitals when required. It is thus essential to assess the impact of the COVID-19 pandemic on the sleep quality, anxiety, and depression status of pre-hospital healthcare providers. Understanding these aspects is crucial for ensuring timely and effective medical care, particularly during a pandemic, when the demand for healthcare services is heightened.
This study aimed to evaluate sleep quality and levels of anxiety and depression in 284 workers in a medical call center in January 2021.
In the research, we sought answers to the following questions:
Material and Methods
ETHICS STATEMENT:
This study was approved by the University Ethical Committee for Clinical Investigations (date: December 8, 2020; number: 23). Verbal consent was obtained from the pre-hospital care providers who volunteered to participate in the study. The principles outlined in the Declaration of Helsinki were followed.
STUDY DESIGN:
This descriptive and cross-sectional study was conducted from January 1 to 30, 2021, targeting healthcare staff affiliated with the pre-hospital care call center and its associated ambulance services. Of the 443 pre-hospital care providers approached, 284 voluntarily consented to participate in the study.
We intentionally did not create any inclusion criteria, allowing any healthcare staff expressing willingness to participate to be included in the study. However, individuals who took sick leave within the 1-month period following the initiation of the study and declined participation were excluded from the study.
INTRODUCTORY INFORMATION FORM:
Developed by the researchers to elicit sociodemographic attributes of the pre-hospital care providers, the introductory information form collected the following characteristics: age, sex, marital status, parenthood, education, profession, job satisfaction, physical health status, polymerase chain reaction (PCR) test status, history of mental health, years of work experience, work duration in the current department, and status of encountering, examining, or caring for patients with COVID-19.
PITTSBURGH SLEEP QUALITY INDEX (PSQI): The PSQI was originally developed by Buysse et al, and its adaptation to Turkish was performed by Agargun [14,15]. The Cronbach alpha value of the Turkish version of the PSQI administered in this study was 0.877. Broadly speaking, the PSQI is a 19-item self-rated scale that assesses sleep quality and disturbances over a 1-month time interval. Out of 24 items in total, 19 are rated by the participants themselves, and the last 5 items are rated by their roommates. A total of 18 items of the rated scale are divided into 7 sub-dimensions, including subjective sleep quality, sleep onset latency, sleep duration, habitual sleep efficiency, sleep disturbances, sleep medication use, and daytime dysfunction. Each sub-dimension is weighted between 0 (no trouble) and 3 (serious distress). The sum of the scores for the 7 sub-dimensions yields the global PSQI score, which ranges between 0 and 21. A global score of 5 or less is considered good sleep quality, and a score of greater than 5 signifies poor sleep quality [15].
HOSPITAL ANXIETY AND DEPRESSION SCALE (HADS): The HADS is a self-report questionnaire that was developed by Zigmond and Snaith to identify levels of anxiety (HADS-A) and depression (HADS-D) [16]. It has 14 items, each of which is scored between 0 and 3. Anxiety and depression are assessed with 7 questions each. The lowest and highest possible scores on each scale are 0 and 21, respectively, with high scores signaling increased anxiety and depression. According to this scale, adapted into Turkish by Aydemir et al, the cut-off value was specified as 7 for anxiety and 10 for depression in the Turkish population [17].
DATA COLLECTION:
The research data was collected through 3 tools: the introductory information form, which was designed by the researchers to collect sociodemographic attributes of the participants, the PSQI, which was used to measure sleep quality, and the HADS, which was used to measure anxiety and depression. The survey forms and scales were designed and hosted on a website (
STATISTICAL ANALYSIS:
All statistical analyses were performed using SPSS 25.0 (IBM Corp, Armonk, NY, USA). Continuous variables were defined by the mean±standard deviation and median (minimum-maximum values), and categorical variables were defined by number and percent. The Kolmogorov-Smirnov and Shapiro-Wilk tests were used for determination of normal distribution. The Mann-Whitney U test and Kruskal-Wallis variance analysis (post hoc: Mann-Whitney U test with Bonferroni Correction) were used for comparisons among groups. The Spearman correlation coefficient was used to examine the relationships between continuous variables. Key determinants were identified through the creation of multivariate regression models, wherein the variables reaching statistical significance in univariate analyses were considered. Categorical variables used when creating the models were turned into dummy variables and added to the models. Statistical significance was determined on the basis of
Results
ANALYSIS OF DEMOGRAPHICS OF PARTICIPANTS:
A cohort of 284 participants was recruited for this investigation. Nearly half of the study population fell within the age bracket of 26 to 35 years, and a majority of 158 individuals (55.6%) identified as female. Marriage status revealed that 195 participants (68.7%) were married, while 115 individuals (40.5%) did not have children. A substantial proportion of 225 participants (79.2%) reported no history of mental health issues. Notably, pre-hospital care workers, inclusive of paramedics, constituted the predominant demographic, representing 80% of the total study population (Table 1).
ANALYSIS OF DESCRIPTIVE CHARACTERISTICS OF PARTICIPANTS IN RELATION TO COVID-19:
Of the total participants, 261 (91.9%) reported encountering patients presenting symptoms consistent with COVID-19, and, notably, 230 participants (81%) reported having either examined or administered medical care to these patients. In the context of diagnostic measures, 190 participants (66.9%) reported undergoing a reverse transcription PCR test. Among those tested, 62 participants (21.8%) received a positive diagnosis for COVID-19 (Table 2).
ANALYSIS OF MEAN HADS-A, HADS-D, AND PSQI SCORES AMONG PARTICIPANTS:
The participants exhibited a mean HADS-A score of 12.11±4.87, with a median of 12, signifying the prevalence of anxiety symptoms. A considerable proportion or participants, 182 (64.1%), had HADS-A scores at or above 11. The mean HADS-D scores were 13.28±4.66, with a median of 13. An overwhelming majority of participants, 256 (90.1%), had HADS-D scores of 8 and above, highlighting a substantial prevalence of depressive symptoms within the cohort. Furthermore, HADS-A and HADS-D scores surpassed the established cut-off values in the majority of the study population (64.1% and 90.1%, respectively). The mean PSQI score was 8.47±3.06, with a median PSQI value of 8. Alarmingly, 255 participants (89.8%) scored 5 and above on the PSQI, indicating a prevalent incidence of poor sleep quality among the majority of the studied cohort (Table 3).
RELATIONSHIP BETWEEN HADS-A, HADS-D, AND PSQI SCORE AVERAGES AND DEMOGRAPHICS OF THE PARTICIPANTS:
The analysis of mean HADS-A scores across different age groups revealed a noteworthy distinction, specifically between participants aged 26 to 35 years and those aged 36 to 45 years, as well as between those aged 26 to 35 years and 46 years and older (
Comparisons according to profession yielded significant differences in HADS-A, HADS-D, and PSQI scores between paramedics and pre-hospital care providers, as well as between paramedics and other healthcare personnel (
Considering job satisfaction, the 3 delineated groups (satisfied, partially satisfied, and dissatisfied) exhibited significant differences in HADS-A and HADS-D scores (
In the context of COVID-19 diagnosis, no striking differences emerged in terms of HADS-A, HADS-D, and PSQI scores. Analysis of PSQI scores, when considering the role of treating or providing care to a COVID-19 patient, revealed no significant variations. However, in the examination of HADS-A and HADS-D, significantly lower scores were found among the participants involved in patient care than in those not engaged in such activities. Assessment of PCR test status demonstrated significantly lower HADS-A and HADS-D scores for the individuals tested, while those without a test yielded higher PSQI scores. Notably, HADS-D scores did not differ significantly based on PCR test outcomes. Conversely, the participants with negative PCR test results demonstrated significantly lower HADS-A scores than those without PCR testing. The PSQI analysis revealed significantly lower scores among those without a test than among those with either positive or negative test results (Table 4).
MULTIVARIATE REGRESSION ANALYSIS RESULTS FOR HAD-A, HAD-D, AND PSQI:
Multivariate regression models were constructed with the variables that were statistically significant in univariate analyses that we mentioned in Table 4. Accordingly, in Table 5, male sex and extended working hours in the current workplace correlated with higher HADS-A scores, whereas the presence of health issues, increased demand for mental support, and reduced levels of job satisfaction resulted in lower HADS-A scores (model 1 R2: 0.336). Similarly, health problems, an increased need for mental support, and poor job satisfaction were linked to lower HADS-D scores (model 2 R2: 0,264). In contrast, male sex exhibited a mitigating effect on PSQI scores, while the presence of health issues, heightened demand for mental support, and poor job satisfaction were associated with an increase in PSQI scores (model 3 R2: 0,228).
Finally, a moderately significant positive correlation was noted between overall sleep quality and HADS-A and HADS-D scores of the participants (
Discussion
We discovered a few important findings in our research. First, we found that sleep quality was poor and depression and anxiety were high among the participants. Second, we found that there was a relationship between the sex, health status, mental health status, job satisfaction, and working hours of the individuals and their anxiety scores. We also found that there was a relationship between the health status, mental health status, and job satisfaction of the participants and their depression scores. Finally, we found that there was a relationship between the sex, health status, mental health status, and job satisfaction of the individuals and their sleep quality. In this study, we aimed to investigate the sleep quality, anxiety, and depression status among pre-hospital care providers during the COVID-19 pandemic, as well as the significant influencing factors.
In our investigation, male healthcare staff exhibited higher susceptibility to anxiety, while female staff demonstrated a tendency toward poorer sleep quality, based on the obtained anxiety scores. Notably, there was no significant sex-related disparity in depression scores, which contrasts with prior studies that reported a more pronounced elevation in depressive and anxious symptoms among female healthcare staff [18–21]. Earlier research has recognized female sex as an independent risk factor for anxiety and depression [22,23]. On the other hand, another study documented that male sex was a significant factor influencing the anxiety levels of healthcare workers, corroborating the findings of our study’s multivariate regression analysis [24]. Due to a perception that the prevalence of COVID-19 was higher among men in the early stages of the pandemic, it is estimated that anxiety levels in male healthcare workers in our study were higher for this reason. Inconsistent with our findings, an investigation involving 964 Italian healthcare providers found female sex as a contributing factor to sleep disturbance [25]. Another study on 1306 Chinese frontline healthcare staff found poorer sleep quality in women, confirming the trends identified in our study [26]. That being said, it is crucial to acknowledge counter-arguments challenging the association between sex and anxiety, depression, and sleep quality [27–29]. Our (Turkish) societal structure, characterized by a patriarchal framework, places the primary responsibilities for working life and home economy on men. In certain segments, only male individuals in the family assume the role of the breadwinner. We thus hypothesize that male healthcare providers may have experienced heightened anxiety due to concerns about potential income loss during lockdown in the event of illness, fears of adverse economic and psychosocial effects on their family members in case of death, and apprehensions about infecting and losing loved ones. Conversely, traditional gender roles, where women are often perceived as primarily responsible for household chores and childcare after work, may have contributed to the observed poorer sleep quality among female healthcare than among their male counterparts.
Our analysis according to age group revealed a notable disparity in anxiety scores, particularly evident among participants aged 36 and older, who reported increased anxiety levels. This finding contradicts previous research [21], suggesting a tendency for anxiety to decrease with advancing age, a phenomenon attributed to increased experience and enhanced stress management capabilities in older individuals [12,30]. However, in our study, the relationship between the increase in anxiety level with increasing age may have been due to the fact that COVID-19 can be chronic and fatal, which increases especially with age. In contrast, other investigations presented varying perspectives. One study observed no significant distinction in sleep disturbance, anxiety, and depression between the general population and healthcare providers aged 36 to 44 years [31]. Conversely, another study noted more frequent sleep complaints among healthcare staff under the age of 30 years [20]. A survey-based study in Shanghai comparing the pre- and post-COVID-19 period among physicians aged 23 to 28 years revealed elevated levels of anxiety, depression, and fear of violence in the post-pandemic era [32]. An Iranian study found depression to be more prevalent between the ages of 41 to 55 years, associating this with factors such as decreased physical strength with advanced age, challenging working conditions, disrupted sleep cycles, and underlying diseases [33]. In line with these diverse findings, we believe that older healthcare staff in our society may experience heightened anxiety due to increasing responsibilities in family care with age, necessitating care for older family members with chronic diseases. Additionally, the surge in chronic diseases associated with aging might be another factor driving elevated anxiety levels.
Published reports indicate that occupational status is more closely associated with sleep quality than anxiety. Sleep problems are reported to be more prevalent among certain occupations, particularly nurses, which is attributed to their increased time spent with patients and frequent communication with patients and their relatives [28,29,34]. Our study also highlighted the direct relationship between sleep disturbances, anxiety, and depression. In the context of the present study, noteworthy differences in anxiety, depression, and sleep quality were identified between pre-hospital care providers and paramedics in ambulatory services, compared with that of other healthcare staff working in hospitals. While anxiety scores in physicians were higher than those in paramedics and pre-hospital care providers, this difference did not reach statistical significance. These findings corroborate the observations of Usul et al, who also reported elevated anxiety levels in pre-hospital care providers and paramedics [21]. The occupational groups primarily engaging with patients in ambulatory services in our country encompass pre-hospital care providers and paramedics. This being the case, anxiety and depression symptoms may have remained relatively lower, and sleep quality better, in these groups than in others, due to the proper use of personal protective equipment, a heightened awareness of pandemic conditions, and the consideration of each new patient as a potential COVID-19 case over the course of the pandemic.
The existing body of literature has demonstrated a correlation between comorbid conditions and sleep quality, anxiety, and depression [31], although research performed thus far has produced mixed results. Some investigations have established a close link between chronic diseases and sleep disturbances and anxiety [25], whereas others have reported associations between chronic disease status and anxiety, rather than depression [23]. Moreover, the presence of an underlying chronic disease has been identified as an independent risk factor for anxiety and depression [22]. In alignment with these varied findings, our study revealed a noteworthy distinction between individuals without health problems and those with a chronic disease concerning anxiety, depression, and sleep quality. The outcomes of our multivariate regression analysis indicate that the presence of health issues exerted a mitigating effect on anxiety and depression scores. Specifically, the participants without health problems reported increased anxiety, while those with a treated chronic disease had elevated depressive symptoms and poorer sleep quality. On the one hand, the elevated anxiety among healthy individuals may be attributed to the fear of contracting COVID-19. On the other hand, concerns about contagion and potential severity of COVID-19 progression in the presence of existing comorbidities may have caused those with chronic diseases to have greater depression and aggravating sleep quality.
No clear association was observed between the duration of working in the same department and depression or sleep quality. This is consistent with previous research findings, such as those reported by Yildirim et al, who found no significant correlations between parameters including professional title, workplace, working area, and working years with anxiety and depression [23]. In a study based in Italy, it was stated that the year of work experience was not related to the increase in the dimension of emotional exhaustion [35]. As per the findings from our multivariate regression analysis, years of experience within the current department was positively associated with elevated anxiety scores. This contradicts previous assertions suggesting that prolonged tenure in the same department may lead to lower stress levels, attributed to factors such as accumulated work experience, enhanced interpersonal skills, and steady income [12]. These results underscore the complexity of the relationship between work duration and mental health outcomes, suggesting that anxiety may be more influenced by certain factors associated with prolonged tenure, while depression and sleep quality may be influenced by other factors or show more nuanced relationships.
Wang et al [31] reported that a diagnosis of novel coronavirus infection among healthcare providers during the COVID-19 pandemic did not serve as a predictor for sleep quality. Consistent with this observation, our study found no significant disparity in sleep quality between individuals infected with COVID-19 and those without infection. Throughout the pandemic, the pre-hospital care call center experienced a surge in calls due to lockdowns and quarantine measures. Pre-hospital healthcare providers were constantly in the field responding to these calls, leading to irregular sleep patterns, irrespective of their COVID-19 infection status. We thus hypothesize that individuals facing increased work intensity, characterized by irregular sleep, may have already experienced poor sleep quality regardless of their infection status.
Previous research reported elevated stress levels in healthcare personnel who did not undergo PCR testing [36]. Yet a contrasting study involving 939 healthcare staff during the COVID-19 pandemic documented higher stress levels in healthcare workers who had been subject to PCR testing [37]. Consistent with this observation, Unal et al also noted increased stress levels in pre-hospital care providers who took PCR tests [12]. In our study, we observed higher anxiety and depression levels in individuals without PCR testing, leading us to speculate that the uncertainty regarding the COVID-19 infection status of those who did not undergo PCR testing contributed to elevated stress levels in this group.
The outcomes of our multivariate regression analysis demonstrate that job satisfaction is associated with lower anxiety and depression levels, while concurrently enhancing sleep quality. This aligns with existing literature, whereby several studies have affirmed the correlation between job satisfaction among healthcare staff and reduced stress levels [12]. In a Spanish study, it is mentioned that higher levels of job satisfaction were linked to a better quality of sleep and lower levels of anxiety [38]. Additionally, a study focusing on sleep quality among healthcare providers in a tertiary hospital noted that individuals reporting job dissatisfaction had lower sleep quality [39].
The findings of this article and their discussion should be considered within the framework of certain limitations. Foremost among these limitations is the time constraints imposed by the specified dates of our investigation. The emotional states of healthcare staff may have undergone fluctuations contingent upon the evolving dynamics of the pandemic. In addition, the restricted scope of our participant pool may have limited the broader applicability of our conclusions; therefore, the observed patterns may not be fully representative of the entire population of pre-hospital care providers. Finally, the reliance on self-reports through the use of forms and scales introduces a potential source of bias in our interpretation. The subjective nature of self-reporting may not result in an objective evaluation, introducing an element of subjectivity to the data. Despite these limitations, the insights gained from this study contribute valuable perspectives to the understanding of the mental health and sleep quality dynamics among pre-hospital care providers during the specified time frame.
Conclusions
The pandemic has had significant physiological and psychosocial effects on pre-hospital healthcare providers, making it essential to maintain their psychological well-being and sleep quality to ensure effective emergency care. Identifying and addressing the factors contributing to adverse psychosocial effects is crucial. Regular psychoeducational programs and psychosocial intervention studies should be implemented and assessed for their efficacy. Additionally, healthcare institutions should establish multidisciplinary mental health teams to provide comprehensive support and professional counseling, thereby mitigating negative effects and promoting the mental well-being of healthcare staff.
Tables
Table 1. Demographic characteristics of healthcare staff.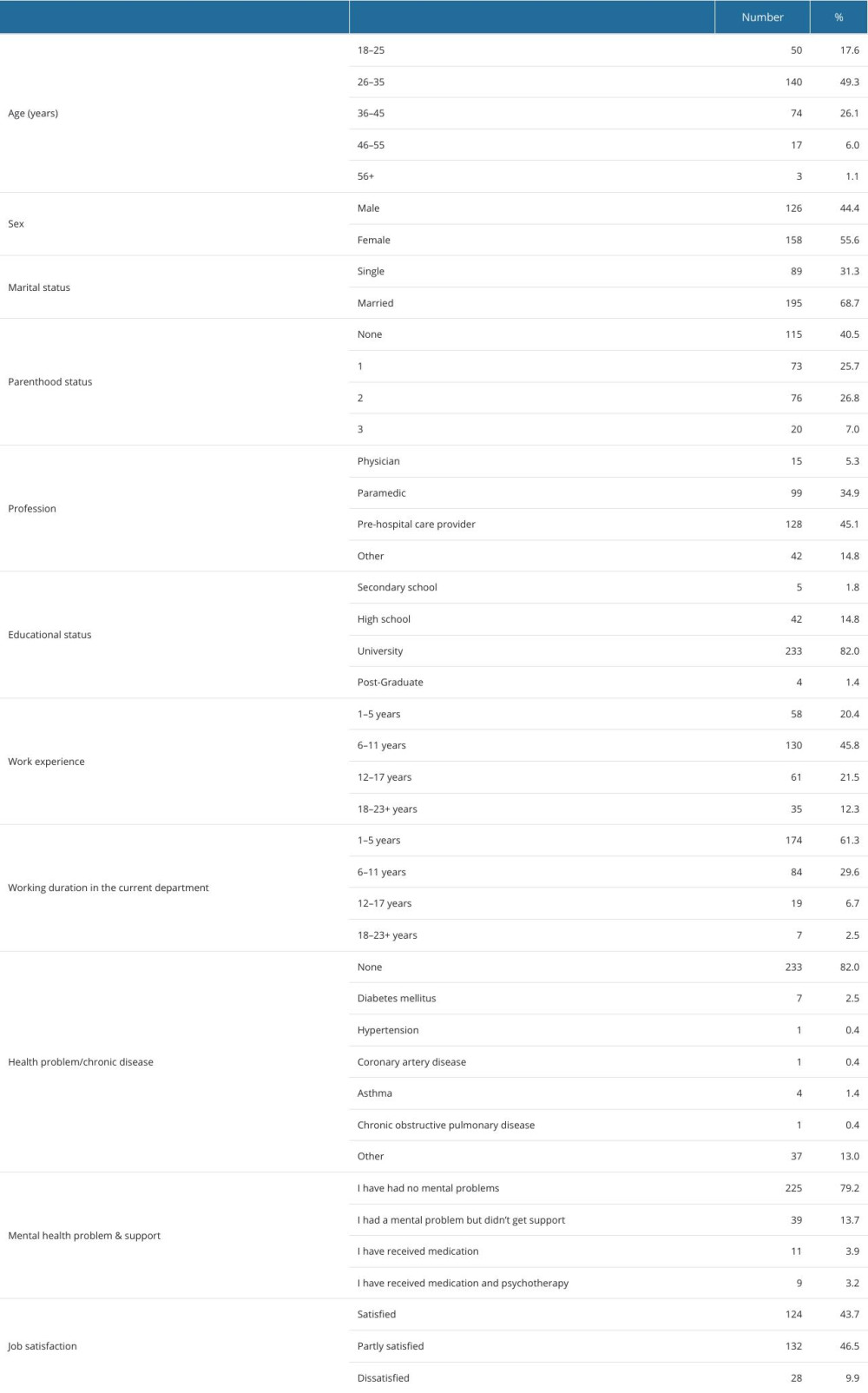 Table 2. Descriptive characteristics of healthcare providers in relation to COVID-19.
Table 2. Descriptive characteristics of healthcare providers in relation to COVID-19.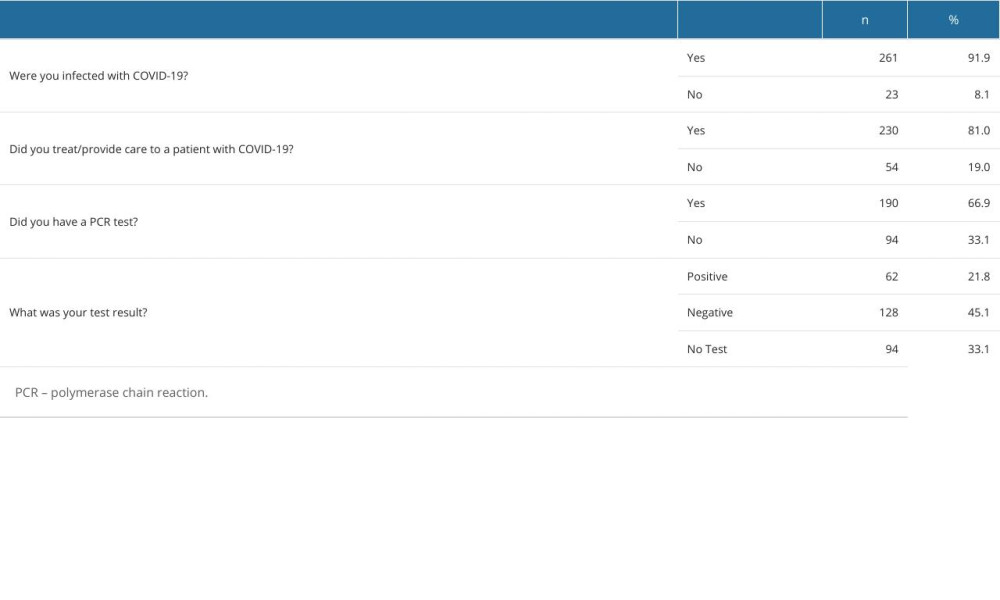 Table 3. Mean HADS and PSQI scores: depression, anxiety, and sleep quality status among healthcare staff.
Table 3. Mean HADS and PSQI scores: depression, anxiety, and sleep quality status among healthcare staff.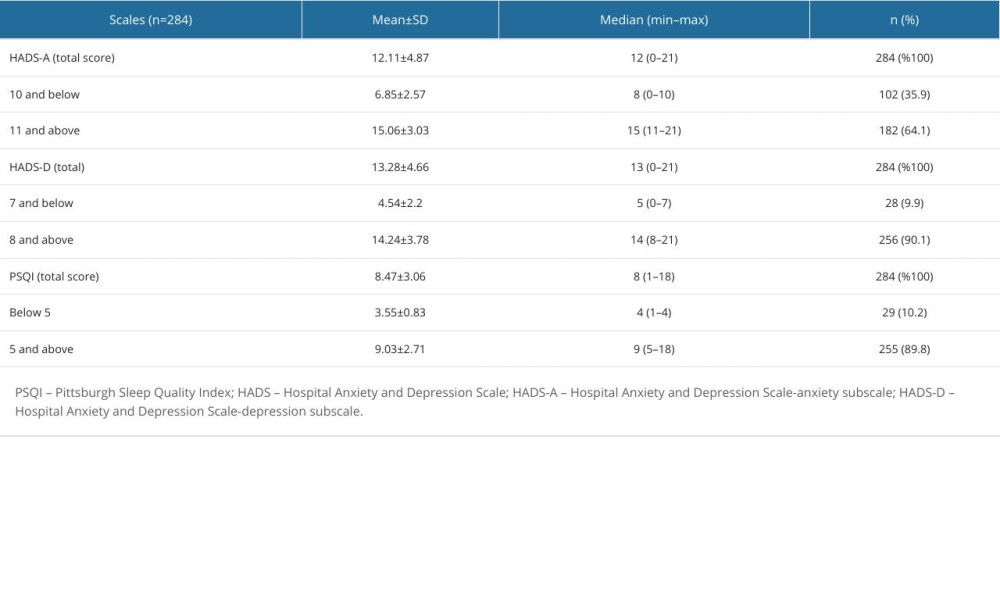 Table 4. Anxiety, depression, and PSQI score averages of healthcare staff by demographic characteristics.
Table 4. Anxiety, depression, and PSQI score averages of healthcare staff by demographic characteristics.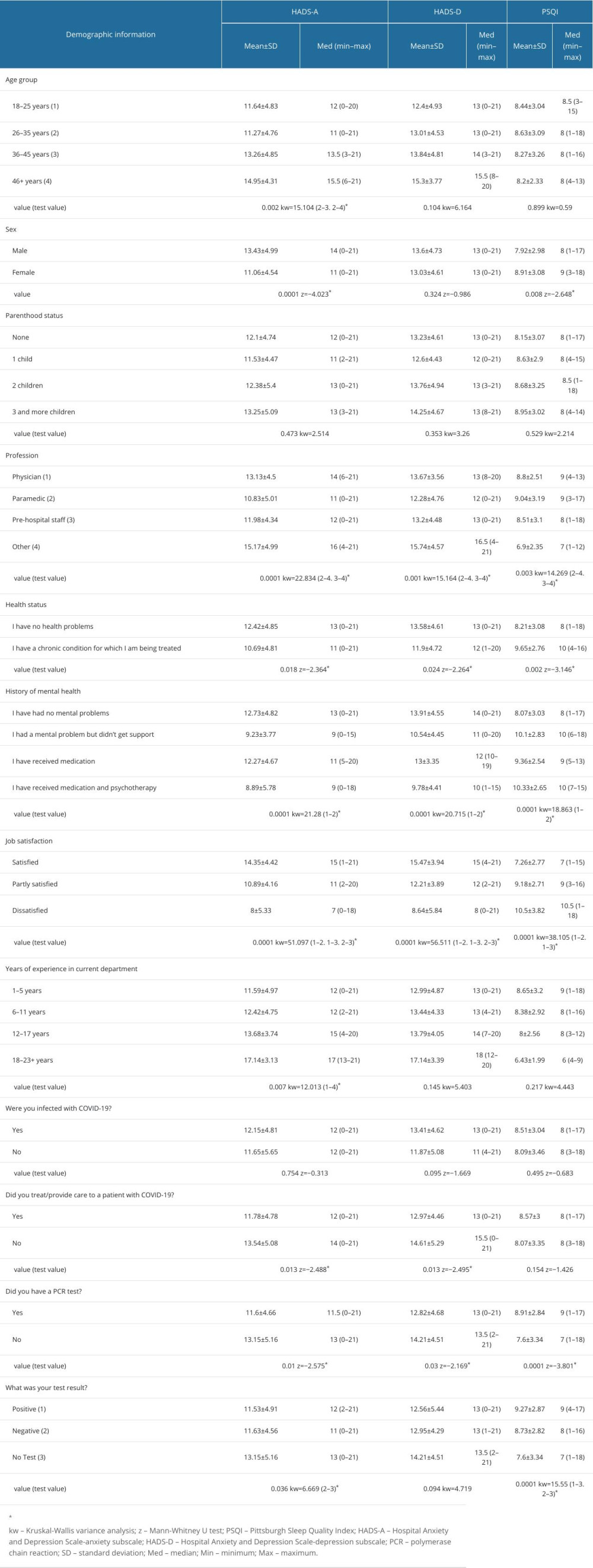 Table 5. Multivariate regression analysis results for HAD-A, HAD-D, and PSQI.
Table 5. Multivariate regression analysis results for HAD-A, HAD-D, and PSQI.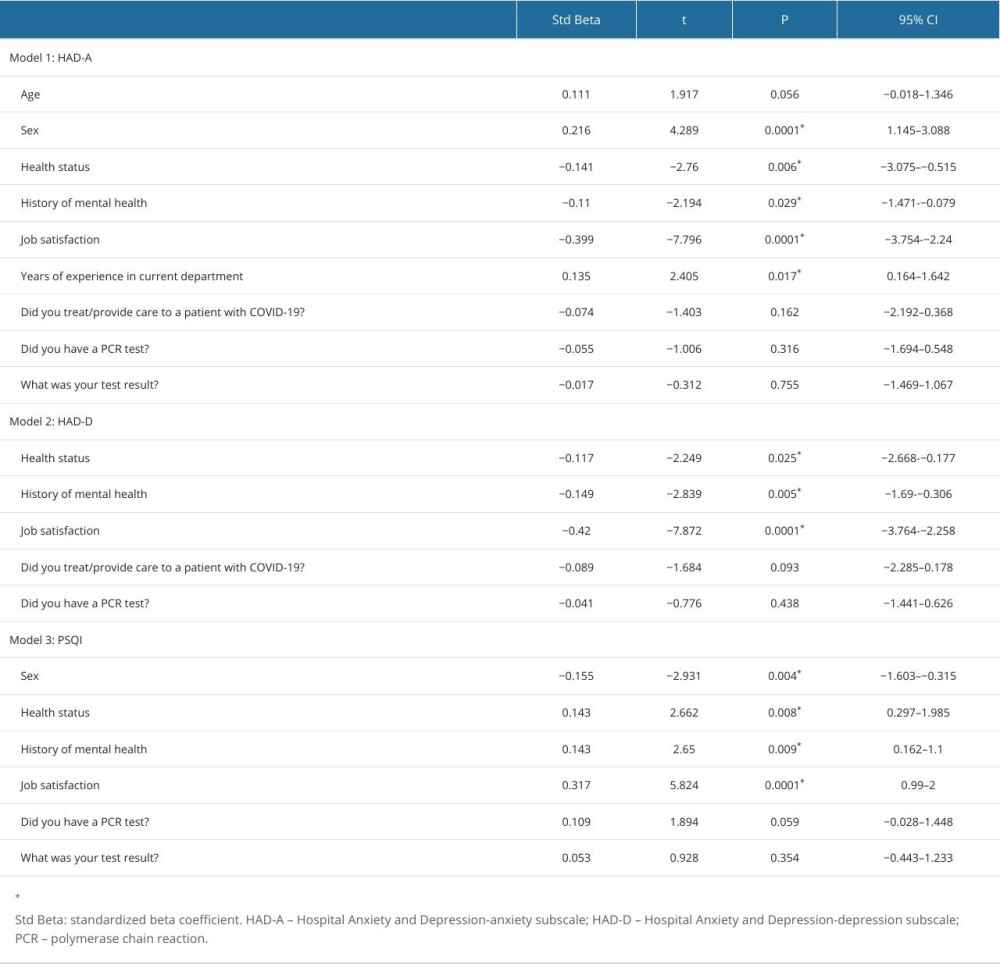
References
1. World Health Organization (WHO): COVID-19 Dashboard Available fromhttps://data.who.int/dashboards/covid19/
2. Girum T, Lentiro K, Geremew M, Migora B, Optimal strategies for COVID-19 prevention from global evidence achieved through social distancing, stay at home, travel restriction and lockdown: A systematic review: Arch Public Health, 2021; 79(1); 150
3. Taylor S, The psychology of pandemics: Annu Rev Clin Psychol, 2022; 18; 581-609
4. Choi EPH, Hui BPH, Wan EYF, Depression and anxiety in Hong Kong during COVID-19: Int J Environ Res Public Health, 2020; 17(10); 3740
5. Brailovskaia J, Miragall M, Margraf J, The relationship between social media use, anxiety and burden caused by coronavirus (COVID-19) in Spain: Curr Psychol, 2022; 41(10); 7441-47
6. Savas E, Tanriverdi D, Knowledge, attitudes and anxiety towards influenza A/H1N1 vaccination of healthcare workers in Turkey: BMC Infect Dis, 2010; 10; 281
7. Santarone K, McKenney M, Elkbuli A, Preserving mental health and resilience in frontline healthcare workers during COVID-19: Am J Emerg Med, 2020; 38(7); 1530-31
8. Preti E, Di Mattei V, Perego G, The psychological impact of epidemic and pandemic outbreaks on healthcare workers: Rapid review of the evidence: Curr Psychiatry Rep, 2020; 22(8); 43
9. Maunder R, Hunter J, Vincent L, The immediate psychological and occupational impact of the 2003 SARS outbreak in a teaching hospital: CMAJ, 2003; 168(10); 1245-51
10. Su TP, Lien TC, Yang CY, Prevalence of psychiatric morbidity and psychological adaptation of the nurses in a structured SARS caring unit during outbreak: A prospective and periodic assessment study in Taiwan: J Psychiatr Res, 2007; 41(1–2); 119-30
11. Pala SÇ, Metintas S, COVID-19 pandemisinde sağlık çalışanları: ESTÜDAM Halk Sağlığı Dergisi, 2020; 5; 156-68 [in Turkish]
12. Unal M, Yilmaz A, Yilmaz H, The impact of COVID-19 on social support perception and stress of prehospital care providers: Australas Emerg Care, 2022; 25(4); 334-40
13. Nikbakht Nasrabadi A, Abbasi S, Mardani A, Experiences of intensive care unit nurses working with COVID-19 patients: A systematic review and meta-synthesis of qualitative studies: Front Public Health, 2022; 10; 1034624
14. Buysse DJ, Reynolds CF, Monk TH, The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research: Psychiatry Res, 1989; 28(2); 193-213
15. Ağargün MY, Kara H, Anlar Ö, The validity and reliability of the Pittsburgh Sleep Quality Index: Turk J Psychiatry, 1996; 7(2); 107-15
16. Zigmond AS, Snaith RP, The hospital anxiety and depression scale: Acta Psychiatr Scand, 1983; 67(6); 361-70
17. Aydemir O, Güvenir T, Küey L, Reliability and validity of the Turkish version of Hospital Anxiety and Depression Scale: Turkish J Psychiatry, 1997; 8; 280-87
18. Luo M, Guo L, Yu M, Jiang W, Wang H, The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public – a systematic review and meta-analysis: Psychiatry Res, 2020; 291; 113190
19. Pappa S, Ntella V, Giannakas T, Giannakoulis VG, Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis [published correction appears in Brain Behav Immun. 2021;92:247]: Brain Behav Immun, 2020; 88; 901-7
20. Gupta B, Sharma V, Kumar N, Mahajan A, Anxiety and sleep disturbances among health care workers during the COVID-19 pandemic in India: Cross-sectional online survey: JMIR Public Health Surveill, 2020; 6(4); e24206
21. Usul E, Şan I, Bekgöz B, The effect of the COVID-19 pandemic on the anxiety level of emergency medical services professionals: Psychiatr Danub, 2020; 32(3–4); 563-69
22. Zhang WR, Wang K, Yin L, Mental health and psychosocial problems of medical health workers during the COVID-19 epidemic in China: Psychother Psychosom, 2020; 89(4); 242-50
23. Yildirim TT, Atas O, Asafov A, Psychological status of healthcare workers during the Covid-19 pandemic: J Coll Physicians Surg Pak, 2020; 30(6); 26-31
24. Şahin CU, Kulakaç N, Exploring anxiety levels in healthcare workers during COVID-19 pandemic: Turkey sample: Curr Psychol, 2022; 41(2); 1057-64
25. Proserpio P, Zambrelli E, Lanza A, Sleep disorders and mental health in hospital workers during the COVID-19 pandemic: A cross-sectional multicenter study in Northern Italy: Neurol Sci, 2022; 43(4); 2241-51
26. Qi J, Xu J, Li BZ, The evaluation of sleep disturbances for Chinese frontline medical workers under the outbreak of COVID-19: Sleep Med, 2020; 72; 1-4
27. Iskandarsyah A, Shabrina A, Djunaidi A, Siswadi AGP, Mental health, work satisfaction and, quality of life among healthcare professionals during the COVID-19 pandemic in an Indonesian sample: Psychol Res Behav Manag, 2021; 14; 1437-46
28. Wang S, Xie L, Xu Y, Sleep disturbances among medical workers during the outbreak of COVID-2019: Occup Med (Lond), 2020; 70(5); 364-69
29. Korkmaz S, Kazgan A, Çekiç S, The anxiety levels, quality of sleep and life and problem-solving skills in healthcare workers employed in COVID-19 services: J Clin Neurosci, 2020; 80; 131-36
30. Huang Y, Zhao N, Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey [published correction appears in Psychiatry Res. 2021;299:113803]: Psychiatry Res, 2020; 288; 112954
31. Wang W, Song W, Xia Z, Sleep disturbance and psychological profiles of medical staff and non-medical staff during the early outbreak of COVID-19 in Hubei Province, China: Front Psychiatry, 2020; 11; 733
32. Li W, Frank E, Zhao Z, Mental health of young physicians in China during the novel coronavirus disease 2019 outbreak: JAMA Netw Open, 2020; 3(6); e2010705
33. Sabbaghi M, Miri K, Kahi R, Nia MN, Investigation of stress, anxiety, and depression levels of Pre-Hospital Emergency Medicine personnel in eastern Iran during the COVID-19 pandemic: BMC Emerg Med, 2022; 22(1); 97
34. Oteir AO, Nazzal MS, Jaber AF, Depression, anxiety and insomnia among frontline healthcare workers amid the coronavirus pandemic (COVID-19) in Jordan: A cross-sectional study: BMJ Open, 2022; 12(1); e050078
35. Vitale E, Casolaro S, Anxiety, burnout and depression levels according to sex and years of work experience in Italian nurses engaged in the care of COVID-19 patients: J Evid Based Psychother, 2021; 21(1); 83-96
36. Erquicia J, Valls L, Barja A, Emotional impact of the COVID-19 pandemic on healthcare workers in one of the most important infection outbreaks in Europe: Med Clin (Engl Ed), 2020; 155(10); 434-40
37. Şahin MK, Aker S, Şahin G, Karabekiroğlu A, Prevalence of depression, anxiety, distress and insomnia and related factors in healthcare workers during COVID-19 pandemic in Turkey: J Community Health, 2020; 45(6); 1168-77
38. Andrés-Olivera P, García-Aparicio J, Lozano López MT, Impact on sleep quality, mood, anxiety, and personal satisfaction of doctors assigned to COVID-19 units: Int J Environ Res Public Health, 2022; 19(5); 2712
39. Tasdemir Yigitoglu G, Yilmaz A, Yilmaz H, The effect of COVID-19 on sleep quality, anxiety and depression on healthcare staff at a tertiary hospital in Turkey: Arch Psychiatr Nurs, 2021; 35(5); 504-10
Tables
Table 1. Demographic characteristics of healthcare staff.Table 2. Descriptive characteristics of healthcare providers in relation to COVID-19.Table 3. Mean HADS and PSQI scores: depression, anxiety, and sleep quality status among healthcare staff.Table 4. Anxiety, depression, and PSQI score averages of healthcare staff by demographic characteristics.Table 5. Multivariate regression analysis results for HAD-A, HAD-D, and PSQI. In Press
Clinical Research
Body Weight and Insulin Resistance Indicators Among ChildrenMed Sci Monit In Press; DOI: 10.12659/MSM.951434
Clinical Research
Comparison of Radiographic Cervical Sagittal Alignment Parameters in Patients With Nonspecific Neck Pain, D...Med Sci Monit In Press; DOI: 10.12659/MSM.952950
Clinical Research
Combined Fibrinogen and Urinary α1-Microglobulin as Predictors of Respiratory Tract Infection in Children w...Med Sci Monit In Press; DOI: 10.12659/MSM.951066
Database Analysis
Evaluation of Salivary Total Oxidant Status (TOS) and Total Antioxidant Status (TAS) in Orthodontic Patient...Med Sci Monit In Press; DOI: 10.12659/MSM.952052
Most Viewed Current Articles
17 Jan 2024 : Review article 14,175,576
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,756,620
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,465,966
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,651
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387