11 September 2024: Clinical Research
Prognostic Significance of the Advanced Lung Cancer Inflammation Index in Metastatic Small Cell Lung Cancer: A Retrospective Analysis of 96 Patients
Muslih ÜrünDOI: 10.12659/MSM.945752
Med Sci Monit 2024; 30:e945752






Abstract
BACKGROUND: The advanced lung cancer inflammation index (ALI) is regarded as a potential indicator of systemic inflammation. This retrospective study aimed to evaluate the prognostic role of the ALI in 96 patients with advanced small cell lung cancer (SCLC).
MATERIAL AND METHODS: This retrospective study included 96 patients who were diagnosed with extensive stage SCLC in a single institution between 2016 and 2022. The formula for ALI is body mass index (kg/m²)×serum albumin (g/dL)/neutrophil to lymphocyte ratio. Patients were divided into low inflammation (ALI ≥32.5) and high inflammation (ALI <32.5) groups. Kaplan-Meier analysis and Cox proportional analysis were conducted to assess the association between the ALI and patient prognosis.
RESULTS: Median age was 61 (range: 41-82) years. Median follow-up was 9 months, and median overall survival (OS) was 10 months (95% CI: 7.75-12.45). A lower ALI score (ALI <32.5) was correlated with a poorer OS than was a higher ALI score (median OS 7 months for ALI <32.5 95% CI: 4.6-9.3 vs 15 months for ALI ≥32.5, 95% CI: 10.6-19.3, P<0.001). In the multivariate analysis, ALI score, Eastern Cooperative Oncology Group performance status, brain metastasis, and bone metastasis were identified as independent prognostic factors.
CONCLUSIONS: ALI score is a substantial predictor of survival in SCLC as in other types of cancer types. Patients with a low ALI score have poorer survival. Assessment of ALI can identify lung cancer patients at high risk of poor prognosis and can be a useful prognostic marker in clinical practice.
Keywords: Lung, Small Cell Lung Carcinoma, Neutrophils, Lymphocytes, inflammation, Humans, Male, Female, Retrospective Studies, lung neoplasms, Middle Aged, Prognosis, Aged, adult, Aged, 80 and over, Kaplan-Meier Estimate, Proportional Hazards Models, Neoplasm Metastasis, Body Mass Index
Introduction
In 2020, approximately 1.8 million deaths worldwide were attributed to lung cancer [1]. Despite advancements in treatments, lung cancer still accounts for more deaths than the combined total of breast, prostate, colorectal, and brain cancers [2]. Small cell lung cancer (SCLC) comprises less than 20% of all lung cancer cases. Without intervention, survival for individuals with SCLC rarely extends beyond a few months. Nevertheless, SCLC exhibits a high responsiveness to dual chemotherapeutic regimens based on platinum compounds. Platinum-based chemotherapeutic regimens were standard therapy in first-line treatment because they extend survival, compared with the most effective palliative care [3]. For an extended period, the primary recommended treatment for individuals with extensive-stage SCLC was platinum plus etoposide. However, the currently favored treatment protocols incorporate immune checkpoint inhibitors that target the programmed death ligand 1, such as atezolizumab or durvalumab [4]. Currently, the established primary treatment for patients with extensive-stage SCLC involves a combination of platinum-based chemotherapy and immunotherapy utilizing durvalumab or atezolizumab, followed by maintenance immunotherapy, based on the results obtained from key studies such as CASPIAN [5,6] and IMPOWER [7,8]. This benefit of treatment can be seen even in patients with advanced disease, poor performance status, and severe organ dysfunction [9,10].
Upon diagnosis, around 30% of patients with SCLC will present with tumors confined to the hemithorax of origin, mediastinum, and supraclavicular lymph nodes. These patients are categorized as having limited-stage disease [11]. Despite being sensitive to initial chemotherapy, most patients with SCLC relapse within a year and have a limited response to second-line therapy [12]. Median overall survival (OS) is 15 to 20 months for patients with limited-stage disease and 8 to13 months for patients with extensive-stage disease [13].
The occurrence and development of cancer are significantly influenced by systemic inflammation [14]. Lung cancer frequently presents with systemic inflammation and compromised nutritional status [15,16]. Various signaling molecules and cytokines secreted by cancer cells trigger cachexia and cause progression. These signaling molecules lead to a decrease in muscle mass by suppressing muscle protein synthesis and increasing muscle proteolysis. Furthermore, oxidative stress, inflammation, energy imbalance, and hormonal changes significantly contribute to the development of cancer cachexia [17].
Cancer cells are characterized by inducing systemic inflammation in the host, which triggers the activation of oncogenic signaling pathways, ultimately resulting in the dissemination, growth, and metastasis of cancer [18]. Systemic inflammation is widely recognized as a detrimental prognostic factor, commonly linked with malnutrition, hypoalbuminemia, weight loss, and other manifestations of cancer cachexia [19]. Several relevant parameters, including C-reactive protein level, lactate dehydrogenase level, white blood cell count, absolute neutrophil count, and the neutrophil to lymphocyte ratio (NLR), have been explored as potential biomarkers of systemic inflammation in patients with cancer [19,20].
The advanced lung cancer inflammation index (ALI) was introduced in 2013 as a valuable prognostic indicator for metastatic non-small cell lung cancer (NSCLC) [21]. The assessment of the ALI, which incorporates indicators of the host’s nutritional and inflammatory status, holds promise as a potential reflection of cancer-induced systemic inflammation and cachexia. Therefore, it stands as an appealing candidate biomarker for assessing treatment efficacy in patients with cancer. While a low ALI score has been demonstrated as an independent poor prognostic factor in patients with advanced NSCLC [21,22], its predictive value remains unknown for patients with SCLC.
The identification of an effective prognostic and predictive index for survival in patients with cancer can help clinicians in their choice of treatment. Therefore, this retrospective study aimed to evaluate the prognostic role of the ALI in 96 patients with advanced SCLC.
Material and Methods
STUDY DESIGN AND ETHICAL ISSUES:
This retrospective study included patients who were followed and treated in the oncology clinic of Dursun Odabaşi Medical Center, Faculty of Medicine, Van Yüzüncü Yil University between 2016 and 2022. This study was conducted in accordance with the Declaration of Helsinki, and approval was granted by the Ethics Committee of Van Yüzüncü Yil University (ethics no: 2022/10–18). Patient consent was waived due to the retrospective observational design of the study.
PARTICIPANTS AND DATA COLLECTION:
Patients aged 18 years and above with a diagnosis of SCLC, extensive-stage disease at diagnosis, and no previous treatment were included. Patients below the age of 18, with more than one primary malignancy, limited-stage disease, or missing data were excluded. During the study period, in accordance with Turkish insurance regulations, immunotherapy was not eligible for reimbursement in our country. First-line chemotherapy was initiated for patients. While few patients underwent chemoimmunotherapy, they had to be excluded from the study. Height, weight, absolute lymphocyte count, absolute neutrophil count, platelet count, and serum albumin levels were retrieved from medical records from the date of diagnosis or the date closest to the date of diagnosis. Data records were eligible for inclusion if they were obtained within a maximum of 10 days before the date of diagnosis. The overall survival was calculated as the time from the date of diagnosis to either the date of death or the latest follow-up.
STATISTICAL ANALYSIS:
Descriptive statistics were presented as numbers and percentages for categorical variables and as median and ranges for continuous variables. The variables were investigated using visual (histogram, probability plots) and analytic methods (Kolmogorov-Smirnov, Shapiro-Wilk tests) to determine whether or not they were normally distributed. Due to the lack of normal distribution in the quantitative variables, a comparison between 2 independent groups was performed using the Mann-Whitney U test. The chi-square test and Fisher exact test were used, where appropriate, to compare the proportions in different groups. Survival curves were performed with the Kaplan-Meier method, and survivals were compared with the log-rank test. Prognostic factors for OS were investigated with Cox regression analysis. Statistically significant factors in univariate analysis were included in the backward stepwise regression model. ALI score is calculated as follows: ALI=body mass index (BMI)×albumin (g/dL)/NLR. BMI=weight (kg)/[height (m)]2. NLR=absolute neutrophil count/absolute lymphocyte count. The receiver operating characteristic curve was used to identify the optimal cut-off point for the ALI, comparing it with other clinical indicators for predicting survival. The optimal cut-off point for the ALI score was 32.5, with a sensitivity of 65.2% and a specificity of 72.6%. A
Results
PATIENT DEMOGRAPHICS AND CHARACTERISTICS:
The study included 96 patients. Table 1 summarizes the characteristics and results of the patients. The median age was 61 years (range: 41–82). Among them, 84 (87.5%) were male. All patients had a favorable Eastern Cooperative Oncology Group performance status (ECOG PS 0-2). Twenty percent of the patients had lymph node involvement, and 79.2% presented with at least 1 distant metastasis. The median follow-up duration was 9 months, and the median OS was 10 months (95% CI: 7.75–12.45).
ALI SCORE AND OVERALL SURVIVAL:
A lower ALI score (<32.5) was associated with a poorer OS than was a higher ALI score (median OS: 7 months for ALI <32.5 [95% CI: 4.6–9.3] vs 15 months for ALI ≥32.5 [95% CI: 10.6–19.3], P<0.001), as shown in Figure 1.
UNIVARIATE AND MULTIVARIATE ANALYSIS OF PROGNOSTIC FACTORS:
In the univariate analysis, ALI score less than 32.5, worse ECOG PS, lower weight, lower BMI, higher neutrophil count, higher NLR, higher platelet to lymphocyte ratio (PLR), and presence of brain, bone, and surrenal metastasis were found to be worse prognostic factors of OS, as shown in Table 2. In the multivariate analysis, ALI score, ECOG PS, brain metastasis, and bone metastasis were identified as independent prognostic factors, as shown in Table 2.
Discussion
In the present study, we demonstrated that the ALI score, a straightforward combination of anthropological and laboratory markers regularly evaluated in clinical settings, can predict the clinical benefit from chemotherapy in extensive-stage SCLC treated with platinum plus etoposide in the first-line treatment. Patients with an ALI score ≥32.5 had statistically significantly longer survival than those with an ALI score <32 (15 months vs 7 months, respectively).
Accumulating evidence has demonstrated that inflammatory and nutritional-based markers predict OS reliably in patients with cancer; however, it remains uncertain which specific marker is more suitable for which type of cancer. The variation of tumor-associated changes in inflammatory cells depends on the extent of the inflammatory response elicited by the tumor, and typically, a more intense inflammatory response correlates with a poorer prognosis. During the initial phases of tumor development, diverse inflammatory cells and proinflammatory cytokines become activated. These factors facilitate the formation of new blood vessels and lymphatic channels, creating a favorable tumor microenvironment that promotes tumor cell growth and differentiation [23]. In advanced stages, inflammation induced by cancer inhibits the activity of immune cells, consequently facilitating the spread of tumor cells [24,25]. Consequently, it is expected that inflammatory markers will serve as valuable prognostic biomarkers in cancer.
A study on patients with NSCLC identified a low lymphocyte count as an independent and unfavorable prognostic factor for disease-free survival [26]. The NLR has also been recognized as an indicator predicting survival outcomes in patients with NSCLC. However, it did not show any association with survival in individuals with SCLC [27]. In a study of patients with stage IV NSCLC, a high NLR, high PLR, and low lymphocyte to monocyte ratio were correlated with diminished survival [28]. Lochowski et al [29] demonstrated that elevated PLR was an independent prognostic factor for survival in patients with NSCLC who underwent surgery. A high neutrophil count and low lymphocyte count are indicative of a robust inflammatory response and a weakened immune response. A meta-analysis showed that NLR was a strong prognostic marker [30]. In another meta-analysis, a high PLR was associated with poor OS [31]. In our study, univariate analysis showed that among inflammatory markers, a high neutrophil count, high NLP, and high PLR were poor prognostic factors for survival, which was consistent with previous studies.
Several studies have confirmed that BMI and serum albumin levels are prognostic markers in patients with cancer [32,33]. Persistent systemic inflammation is associated with low body weight and hypoproteinemia [34,35]. In a research study involving individuals with inoperable NSCLC, weight loss and low serum albumin levels were associated with poor survival and were considered to be linked to persistent systemic inflammation [36]. A study found that low BMI and weight loss were associated with poor OS in patients with advanced lung cancer [37]. Our study findings revealed that low weight and low BMI were correlated with diminished survival outcomes in the univariate analysis, consistent with previous literature.
In a meta-analysis, the ALI score showed a prognostic value on the survival outcomes of patients with cancer, and a lower ALI score was associated with a less favorable prognosis (
Our study has several limitations. First, the retrospective design can introduce selection bias and limit the ability to establish causality. Second, the study was conducted at a single center, which can limit the generalizability of the findings to other populations and settings. Additionally, the sample size of 96 patients was relatively small.
Conclusions
ALI score is a significant predictor of survival in SCLC, as in other types of cancer types. Survival is worse in patients with a low ALI score. Assessment of ALI can identify lung cancer patients at high risk of poor prognosis and can be a useful prognostic marker in clinical practice. In the future, large, prospective, and well-designed studies are needed to confirm the prognostic properties of ALI and the relationship between the threshold value of ALI and tumor stage in this patient population.

References
1. Sung H, Ferlay J, Siegel RL, Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries: Cancer J Clin, 2021; 71(3); 209-49
2. Siegel RL, Miller KD, Fuchs HE, Jemal A, Cancer statistics, 2021: Cancer J Clin, 2021; 71(1); 7-33
3. Agra Y, Pelayo M, Sacristan M, Chemotherapy versus best supportive care for extensive small cell lung cancer: Cochrane Database Syst Rev, 2003(4); CD001990
4. NCC Network: Small cell lung cancer (Version 2.2024). [February 26, 2024]; Available from: https://www.nccn.org/professionals/physician_gls/pdf/sclc.pdf
5. Paz-Ares L, Dvorkin M, Chen Y, Durvalumab plus platinum-etoposide versus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN) : A randomised, controlled, open-label, phase 3 trial: Lancet, 2019; 394(10212); 1929-39
6. Goldman JW, Dvorkin M, Chen Y, Durvalumab, with or without tremelimumab, plus platinum-etoposide versus platinum-etoposide alone in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN) : Updated results from a randomised, controlled, open-label, phase 3 trial: Lancet Oncol, 2021; 22(1); 51-65
7. Horn L, Mansfield AS, Szczęsna A, First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer: N Engl J Med, 2018; 379(23); 2220-29
8. Liu SV, Reck M, Mansfield AS, Updated overall survival and PD-L1 subgroup analysis of patients with extensive-stage small-cell lung cancer treated with atezolizumab, carboplatin, and etoposide (IMpower133): J Clin Oncol, 2021; 39(6); 619-30
9. Giordano KF, Jatoi A, Adjei AA, Ramifications of severe organ dysfunction in newly diagnosed patients with small cell lung cancer: Contemporary experience from a single institution: Lung Cancer, 2005; 49(2); 209-15
10. Chen CR, Qi WX, Efficacy of addition immune checkpoint inhibitors to chemotherapy as first-line treatment for small cell lung cancer patients with liver or brain metastases: A systematic review and meta-analysis: Eur Rev Med Pharmacol Sci, 2022; 26(16); 5857-67
11. Murray N, Coy P, Pater JL, Importance of timing for thoracic irradiation in the combined modality treatment of limited-stage small-cell lung cancer. The National Cancer Institute of Canada Clinical Trials Group: J Clin Oncol, 1993; 11(2); 336-44
12. Rossi A, Tay R, Chiramel J, Current and future therapeutic approaches for the treatment of small cell lung cancer: Expert Rev Anticancer Ther, 2018; 18(5); 473-86
13. Lally BE, Urbanic JJ, Blackstock AW, Small cell lung cancer: Have we made any progress over the last 25 years?: Oncologist, 2007; 12(9); 1096-104
14. de Visser KE, Eichten A, Coussens LM, Paradoxical roles of the immune system during cancer development: Nat Rev Cancer, 2006; 6(1); 24-37
15. Madariaga MLL, Troschel FM, Best TD, Low thoracic skeletal muscle area predicts morbidity after pneumonectomy for lung cancer: Ann Thorac Surg, 2020; 109(3); 907-13
16. Alifano M, Mansuet-Lupo A, Lococo F, Systemic inflammation, nutritional status and tumor immune microenvironment determine outcome of resected non-small cell lung cancer: PLoS One, 2014; 9(9); e106914
17. Argilés JM, Busquets S, Stemmler B, López-Soriano FJ, Cancer cachexia: Understanding the molecular basis: Nat Rev Cancer, 2014; 14(11); 754-62
18. Hanahan D, Weinberg RA, Hallmarks of cancer: The next generation: Cell, 2011; 144(5); 646-74
19. Baracos VE, Martin L, Korc M, Cancer-associated cachexia: Nat Rev Dis Primers, 2018; 4; 17105
20. Menekse S, Kut E, Almuradova E, Elevated serum lactate dehydrogenase to albumin ratio is a useful poor prognostic predictor of nivolumab in patients with non-small cell lung cancer: Eur Rev Med Pharmacol Sci, 2023; 27(5 Suppl); 86-94
21. Jafri SH, Shi R, Mills G, Advance lung cancer inflammation index (ALI) at diagnosis is a prognostic marker in patients with metastatic non-small cell lung cancer (NSCLC): A retrospective review: BMC Cancer, 2013; 13; 158
22. Hua X, Chen J, Wu Y, Prognostic role of the advanced lung cancer inflammation index in cancer patients: A meta-analysis: World J Surg Oncol, 2019; 17(1); 177
23. Coussens LM, Werb Z, Inflammation and cancer: Nature, 2002; 420(6917); 860-67
24. Mantovani A, Allavena P, Sica A, Balkwill F, Cancer-related inflammation: Nature, 2008; 454(7203); 436-44
25. Balkwill F, Mantovani A, Inflammation and cancer: Back to Virchow?: Lancet, 2001; 357(9255); 539-45
26. Zhang J, Huang SH, Li H, Preoperative lymphocyte count is a favorable prognostic factor of disease-free survival in non-small-cell lung cancer: Med Oncol, 2013; 30(1); 352
27. Akinci Ozyurek B, Sahin Ozdemirel T, Prognostic value of the neutrophil to lymphocyte ratio (NLR) in lung cancer cases: Asian Pac J Cancer Prev, 2017; 18(5); 1417-21
28. Mandaliya H, Jones M, Oldmeadow C, Nordman , Prognostic biomarkers in stage IV non-small cell lung cancer (NSCLC): Neutrophil to lymphocyte ratio (NLR), lymphocyte to monocyte ratio (LMR), platelet to lymphocyte ratio (PLR) and advanced lung cancer inflammation index (ALI): Transl Lung Cancer Res, 2019; 8(6); 886-94
29. Łochowski M, Chałubińska-Fendler J, Zawadzka I, The prognostic significance of preoperative platelet-to-lymphocyte and neutrophil-to-lymphocyte ratios in patients operated for non-small cell lung cancer: Cancer Manag Res, 2021; 13; 7795-802
30. Wang Z, Zhan P, Lv Y, Prognostic role of pretreatment neutrophil-to-lymphocyte ratio in non-small cell lung cancer patients treated with systemic therapy: A meta-analysis: Transl Lung Cancer Res, 2019; 8(3); 214-26
31. Zhou H, Li J, Zhang Y, Platelet-lymphocyte ratio is a prognostic marker in small cell lung cancer – a systemic review and meta-analysis: Front Oncol, 2022; 12; 1086742
32. Han J, Zhou Y, Zheng Y, Positive effect of higher adult body mass index on overall survival of digestive system cancers except pancreatic cancer: A systematic review and meta-analysis: Biomed Res Int, 2017; 2017; 1049602
33. Gupta D, Lis CG, Pretreatment serum albumin as a predictor of cancer survival: A systematic review of the epidemiological literature: Nutr J, 2010; 9; 69
34. McMillan DC, Watson WS, O’Gorman P, Albumin concentrations are primarily determined by the body cell mass and the systemic inflammatory response in cancer patients with weight loss: Nutr Cancer, 2001; 39(2); 210-13
35. Don BR, Kaysen G, Serum albumin: Relationship to inflammation and nutrition: Semin Dial, 2004; 17(6); 432-37
36. Scott HR, McMillan DC, Forrest LM, The systemic inflammatory response, weight loss, performance status and survival in patients with inoperable non-small cell lung cancer: Br J Cancer, 2002; 87(3); 264-67
37. Oswalt C, Liu Y, Pang H, Associations between body mass index, weight loss and overall survival in patients with advanced lung cancer: J Cachexia Sarcopenia Muscle, 2022; 13(6); 2650-60
38. Seo BM, Choi J, Chang B, Clinical significance of the advanced lung cancer inflammation index in patients with limited-stage small cell lung cancer treated with chemoradiotherapy: Scie Rep, 2024; 14(1); 10347
39. He X, Zhou T, Yang Y, Advanced lung cancer inflammation index, a new prognostic score, predicts outcome in patients with small-cell lung cancer: Clin Lung Cancer, 2015; 16(6); e165-71
Tables
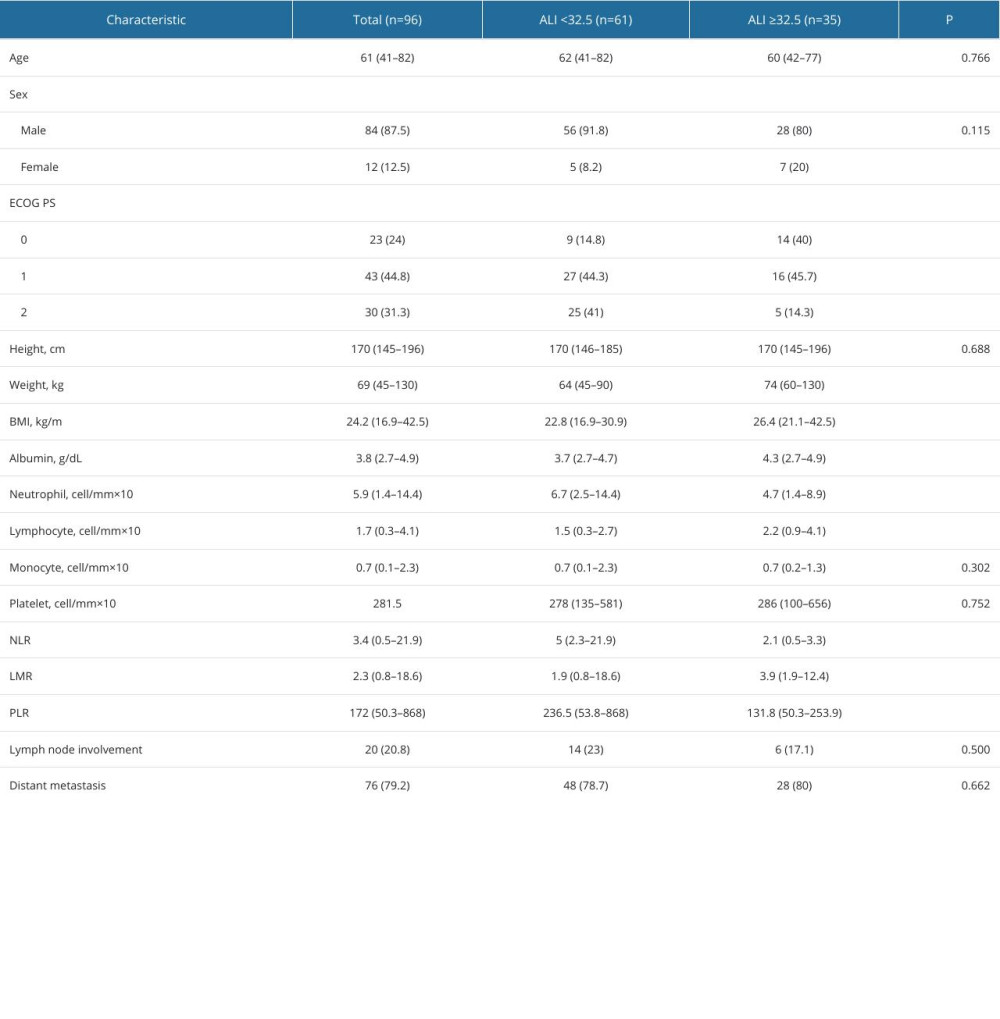 Table 1. Baseline characteristics and comparison by advanced lung cancer inflammation index (ALI) score.
Table 1. Baseline characteristics and comparison by advanced lung cancer inflammation index (ALI) score. Table 2. Prognostic factors for overall survival.Table 1. Baseline characteristics and comparison by advanced lung cancer inflammation index (ALI) score.Table 2. Prognostic factors for overall survival.
Table 2. Prognostic factors for overall survival.Table 1. Baseline characteristics and comparison by advanced lung cancer inflammation index (ALI) score.Table 2. Prognostic factors for overall survival. In Press
Clinical Research
Comparative Effectiveness of a Nurse-Led Care Model vs Usual Care in Rheumatoid Arthritis: A Longitudinal C...Med Sci Monit In Press; DOI: 10.12659/MSM.953211
Clinical Research
Impact of Treatment Modality on Pain, Sexual Function, and Psychological Well-Being in Patients With Bartho...Med Sci Monit In Press; DOI: 10.12659/MSM.952422
Clinical Research
Association Between Radiographic Knee Osteoarthritis, Pre-Fracture Mobility, and Hip Fracture Patterns in O...Med Sci Monit In Press; DOI: 10.12659/MSM.952678
Clinical Research
Association Between Total Cholesterol–to–High-Density Lipoprotein Ratio and Gestational Hypertension: A Cas...Med Sci Monit In Press; DOI: 10.12659/MSM.952395
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,084
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,757,530
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,116
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,768
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387