08 May 2023: Clinical Research
Evaluation of the One-Hour C-Propionate Breath Test in 49 Patients from a Single Center in Japan to Detect Vitamin B Deficiency
Yosuke SasakiDOI: 10.12659/MSM.940238
Med Sci Monit 2023; 29:e940238






Abstract
BACKGROUND: Given the unavailability of reliable biomarkers for vitamin B₁₂ (VB₁₂) deficiency in clinical settings, the usefulness of the ¹³C-propionate breath test (PBT), utilizing VB₁₂ as a coenzyme of methylmalonyl-CoA in propionate metabolism, as a diagnostic modality for VB₁₂ deficiency has been studied. However, a collection time of 2 h reduces its convenience. Hence, we evaluated the effectiveness of 1-h PBT for detecting VB₁₂ deficiency in 49 patients with suspected VB₁₂ deficiency.
MATERIAL AND METHODS: We collected 100-200 mL breath gas every 10 min until 1 h after the administration of 1 g of ¹³C-propionate from 49 patients (31 men, 18 women; median age, 70 years) with clinically suspected VB₁₂ deficiency and calculated the ¹³CO₂ recovered in the breath per hour as the recovery rate (RR [%dose/h]) from ¹³CO₂/¹²CO₂ using infrared isotope spectrometry. We compared the RRs between groups: (1) with serum VB₁₂ levels ≥145 pg/mL and <145 pg/mL, (2) with mean corpuscular volume ≤100 fL and >100 fL, and 3) pre- and post-VB₁₂ supplementation.
RESULTS: The RRs peaked within 30 min. The RRs at 20 min (RR20) and 30 min (RR30) were significantly lower in macrocytotic patients (41.28 vs 50.07, p=0.026 and 37.82 vs 43.93, P=0.003). The RR30 was higher in the supplemented patients (41.93 vs 32.84, P=0.024). There was no significant difference in RRs between the patients with normal and low serum VB₁₂ levels.
CONCLUSIONS: The 1-h PBT can be a diagnostic modality for VB₁₂ deficiency because 1 h is a sufficient collection time.
Keywords: Anemia, Anemia, Megaloblastic, Breath Tests, Propionates, vitamin B12, Aged, Female, Humans, Male, Carbon Isotopes, Japan, Vitamin B 12, Vitamin B 12 Deficiency
Background
Vitamin B12 (VB12) deficiency is known to cause various disorders, including megaloblastic anemia, cognitive defects, myelopathy, peripheral neuropathy, and loss of taste [1]. Furthermore, VB12 deficiency in older adults due to various causes, including adverse drug events or social isolation, is increasingly problematic because of the aging society [2,3]. As VB12 deficiency can be treated with VB12 supplementation, early diagnosis is crucial. However, there are challenges in the development of diagnostic methods for VB12 deficiency in Japan, such as the low reliability and unavailability of many biomarkers. Although many researchers have evaluated the association between serum VB12 levels and clinical symptoms, particularly cognitive function [4,5], many other studies have shown a poor association between VB12 and clinical symptoms [6,7]. Therefore, the measurement of other VB12 deficiency markers, such as serum homocysteine (HC) or methylmalonic acid (MMA), is required for the diagnosis of VB12 deficiency [8,9]. A systematic review of randomized controlled trials concluded that serum VB12 level is an effective biomarker for detecting change in VB12 intake. However, a systematic review pointed out the heterogeneity of serum VB12 levels among different studies [10]. The current guidelines recommend suspecting VB12 deficiency if patients have serum VB12 level <200 pg/mL and measuring plasma total HC or MMA levels to confirm the diagnosis [11]. Serum holotranscobalamin is also a promising candidate biomarker of VB12 deficiency; however, the unavailability and high costs of measuring these biomarkers hinder their use in clinical practice [11]. In addition, there are limited commercial methods for measuring serum MMA levels in Japan. Furthermore, the guidelines mention that there is no “gold-standard” test for the diagnosis of VB12 deficiency because there are no definitive cut-off values for HC or MMA levels, since a variety of methodologies are used to measure them [11]. Therefore, accessible noninvasive diagnostic modalities including screening tests are needed to better address VB12 deficiency in various clinical settings.
Utilizing the role of VB12 as a coenzyme of methylmalonyl-CoA in propionate metabolism to CO2 (Figure 1), the use of 13C-propionate breath test (PBT) as a noninvasive diagnostic modality for VB12 deficiency has been studied previously [12]. In the conventional PBT, the examiner collects 100–200 mL of breath gas every 10 min for 120 min after the administration of 13C-propionate. We believe that the collection time of 2 h for the convention PBT is too long and reduces the convenience for the participants; a collection period of 60 min appears to be sufficient to evaluate the propionate metabolism in patients with VB12 deficiency. Therefore, this study aimed to evaluate the usefulness of a 1-h PBT for detecting VB12 deficiency in patients with clinically suspected VB12 deficiency.
Material and Methods
PATIENTS:
We performed a 1-h PBT and collected blood samples from patients who visited the Department of General Medicine and Emergency Care, Toho University School of Medicine, Tokyo, Japan, between April 2014 and February 2023, with clinically suspected VB12 deficiency according to symptoms such as numbness, muscle cramps, cognitive dysfunction, or macrocytic anemia. The patients who underwent gastrectomy were excluded because gastrectomy causes altered intestinal excretion.
1-H PBT:
The patients were asked to fast for more than 8 h before the test. We collected 2.0 L of breath gas in the collecting bag before administering 13C-propionate. We asked the participants to drink 100 mL of 1 mg/mL 13C-propionate aqueous solution that we prepared immediately before administration to the participants. After the participants drank the aqueous solution containing 13C-propionate, we collected 100–200 mL of breath gas every 10 min until 60 min. We recorded the body weight and height of the participants immediately before the 1-h PBT to calculate the body surface area.
:
Because 13C-propionate is metabolized in the liver and finally exhaled as 13CO2 (Figure 1), we measured the 13CO2/12CO2 isotope ratio of the collected gas using infrared isotope spectrometry (POCone; Otsuka Electrics Co., Ltd., Hirakata, Japan). The detected 13CO2 levels in the exhaled gas were expressed as delta over base line per mil (Δ‰). We converted Δ‰ to 13CO2 recovered in the breath per hour (RR% dose/h), based on the body surface area (calculated as 0.0024265 × weight0.5378 × height0.3964 [m2]), and assumed CO2 excretion (VCO2) with reference to the previous study by Urita et al, as follows [12,13]:
where MW (molecular weight) is 97.07, VCO2 is 300 (BSA mmol/h), dose is 100 mg and APE (atom% excess) is 99.0% [13].
BLOOD TESTS:
We measured the serum VB12 level by chemiluminescent enzyme immunoassay (CLEIA) at SRL (Tokyo, Japan), hemoglobin level, and mean corpuscular volume (MCV) of all patients. In this study, we did not measure the serum MMA level due to the lack of access to serum MMA measurements in Japan and the high cost. Instead, we measured serum the VB12 level because we regarded it a feasible and somewhat reliable biomarker in light of the results of a previous systematic review of randomized control trials [10].
:
Because the lower limit of serum VB12 levels measured by CLEIA was 50 pg/mL, we could not analyze serum VB12 level as a continuous variable. Thus, we divided the patients into a VB12 deficiency group and a normal group. To avoid false-positive results, we defined VB12 deficiency as serum VB12 level <145 pg/mL, as the lowest cut-off value among those used in previous studies [14,15], and we defined macrocytosis as MCV >100 fL based on previous studies.
STATISTICAL ANALYSIS:
We compared the means or medians of the RRs between VB12 deficient patients (defined as serum VB12 levels <145 pg/mL) and normal patients (defined as serum VB12 ≥145 pg/mL). To compensate for the lack of asymptomatic healthy controls and comparison between 1-h PBT results and other biomarkers such as serum MMA, we additionally compared the RRs between macrocytic patients (defined as MCV >100 fL) and normocytic patients (MCV ≤100 fL) and between VB12-deficient patients before and after VB12 supplementation. We evaluated the normality of all variables using the Kolmogorov-Smirnov test and evaluated statistical differences between groups using the t test and Mann-Whitney U test for normally and non-normally distributed variables, respectively. Statistical significance was set at P<0.05. If patients received 1-h PBT before and after supplementation with VB12, we separately compared the results before and after supplementation. All statistical analyses were performed using R, version 4.2.0 [16].
Results
CLINICAL CHARACTERISTICS OF THE PARTICIPANTS:
We performed the 1-h PBT in 55 patients. Of them, 6 post-gastrectomy patients were excluded; hence, only 49 patients were finally evaluated. The median age was 70 years (range, 27–89 years). The median MCV was 93.5 fL (range, 78.3–135.6 fL). The frequencies of complaints or reasons for suspected VB12 deficiency are listed in Table 1.
:
Of the 49 patients, 20 (40.8%) had serum VB12 levels <145 pg/mL and were defined as having VB12 deficiency. The RRs were not significantly different between patients with VB12 deficiency and normal patients (Table 2, Figure 2).
COMPARISONS OF 1-H PBT BETWEEN MACROCYTIC AND NORMOCYTIC PATIENTS:
In the comparison of the RRs between 14/49 (28.6%) macrocytic, defined as MCV >100 fL, and 35 normocytic patients, the RR at 20 min after administration of 13C-propionate (RR20) and the RR at 30 min after administration of 13C-propionate (RR30) were significantly lower in macrocytic patients than in normocytic patients, with values of 41.28 vs 50.07 (P=0.026) and 37.82 vs 43.93 (P=0.003), respectively (Table 3, Figure 3, respectively).
COMPARISONS OF 1-H PBT BETWEEN PRE- AND POST-SUPPLEMENTATION:
Nine patients received the test before and after oral or intramuscular supplementation of VB12 for more than 3 months. We compared the RRs of 11 post-treatment data and 9 pre-treatment data (2 patients underwent the 1-h PBT twice after supplementation). As shown in Table 4 and Figure 4, the RRs at all time points were higher in the post-treatment group, although only the RR30 was significantly higher (mean: 41.93 vs 32.84, P=0.024).
Discussion
This study evaluated whether the 1-h PBT can be used as an easier, noninvasive method of diagnosis of VB12 deficiency by comparing the results of 1-h PBT results of patients with or without low serum VB12 levels, macrocytosis, and VB12 supplementation. We did not find a significant difference in RRs between the patients with normal and low serum VB12 levels; however, significant differences were found between the with and without macrocytosis groups and between the before and after VB12 supplementation groups. Furthermore, the RRs peaked within 30 min after propionate administration, suggesting that 1 h is sufficient for measuring the RRs.
The previous study on conventional PBT, performed by Wagner et al, comparing the RRs for 2 h between 26 participants who were at risk for VB12 deficiency and 32 healthy patients showed significantly lower RR10–30 in patients at risk of VB12 deficiency compared to healthy participants [12]. In the present study, we confirmed that the RRs peaked within 30 min after propionate administration, as reported by Wagner et al. Thus, we believe that 1 h, which is half the time for a conventional PBT, is sufficient for measuring the RRs. Besides the different measuring period (1 h vs 2 h), there are 2 other differences between the present study and the study by Wagner et al: (1) different reference biomarkers and (2) different comparison groups.
Because we could not measure the serum MMA level as mentioned above, we used serum VB12 level as a reference biomarker and defined serum VB12 deficiency as serum VB12 level <145 pg/mL; therefore, we did not find the expected difference in the 1-h PBT associated with low serum VB12 levels. We could not compare and analyze the association of PBT results and serum VB12 levels between our study and the study by Wagner et al because they did not directly analyze PBT results and serum VB12 levels [12]. As mentioned in the Background section above, many studies have pointed out that serum VB12 level is unreliable as a diagnostic marker for VB12 deficiency; therefore, serum MMA levels but not serum VB12 levels were used to diagnose deficiency in a previous study using PBT to diagnose VB12 deficiency [6]. Thus, we believe that the lack of changes in 1-h PBT associated with serum VB12 level was caused by the poor association between the serum VB12 level and actual VB12 deficiency rather than by the sensitivity of the 1-h PBT. Given the unreliability of serum VB12 levels in the diagnosis of VB12 deficiency, we intended to evaluate the diagnostic performance of 1-h PBT by comparing it with serum MMA levels; however, we did not go ahead with using serum MMA levels due to the lack of access to serum MMA measurement methods in Japan and the research cost, and we judged serum VB12 level to be a feasible and somewhat reliable biomarker according to the results of a previous systematic review of randomized control trials [10].
In this study, we evaluated the relationship between MCV, a marker of macrocytosis caused by megaloblastic anemia, a typical disease resulting from VB12 deficiency, and the RRs in 1-h PBT to compensate for the lack of comparison between 1-h PBT and other reliable biomarkers. As expected, the results showed that the RRs were significantly lower in the macrocytosis group 20–30 min after propionate administration.
For the same purpose of compensation, we additionally compared the RRs of post-treatment data and pre-treatment. As expected, the RR30 was significantly higher in the treated group. Although we cannot compare these findings with previous studies because no previous study on PBT evaluated the association between MCV and before and after treatment [12,17], we believe that the decrease in the RR in the macrocytosis group and the increase in the RR after VB12 supplementation reflect the propionate metabolic disturbances associated with VB12 deficiency, as in previous studies [12,17].
The present study has 3 major limitations: (1) As described above, we could not compare the findings of 1-h PBT with serum MMA levels due to lack of access to serum MMA measurement in Japan and the research cost. We believe that this is a major limitation that limits the significance of this study. To compensate for the lack of comparison between 1-h PBT and reliable biomarkers, we evaluated the relationship between MCV in this study. (2) However, this study did not exclude other causes of macrocytosis, such as folate deficiency, hypothyroidism, bone marrow disease, drug adverse effects, or alcoholic liver disease [14], nor did it determine the presence of iron-deficiency anemia, chronic inflammation, or thalassemia that cause low MCV [18]. Thus, the possibility of these comorbid conditions affecting the MCV values cannot be ignored. (3) We could not enroll asymptomatic healthy controls in this study because we could use the 1-h PBT only for patients with clinically suspected VB12 deficiency due to ethical restriction. Despite these limitations, since the peaks of the RRs were within 30 min after propionate administration, we believe that RR measurements for 1 h are sufficient to evaluate the abnormal propionate metabolism caused by VB12 deficiency. Therefore, the 1-h PBT may be a more convenient noninvasive diagnostic modality for VB12 deficiency than conventional PBT.
Conclusions
The 1-h PBT can be used as a convenient noninvasive diagnostic modality for VB12 deficiency because 1 h was found to be a sufficient collection time and expected differences were observed in comparisons between the groups with and without macrocytosis and before and after supplementation. Further studies comparing the 1-h PBT results with serum MMA levels are needed.
Figures
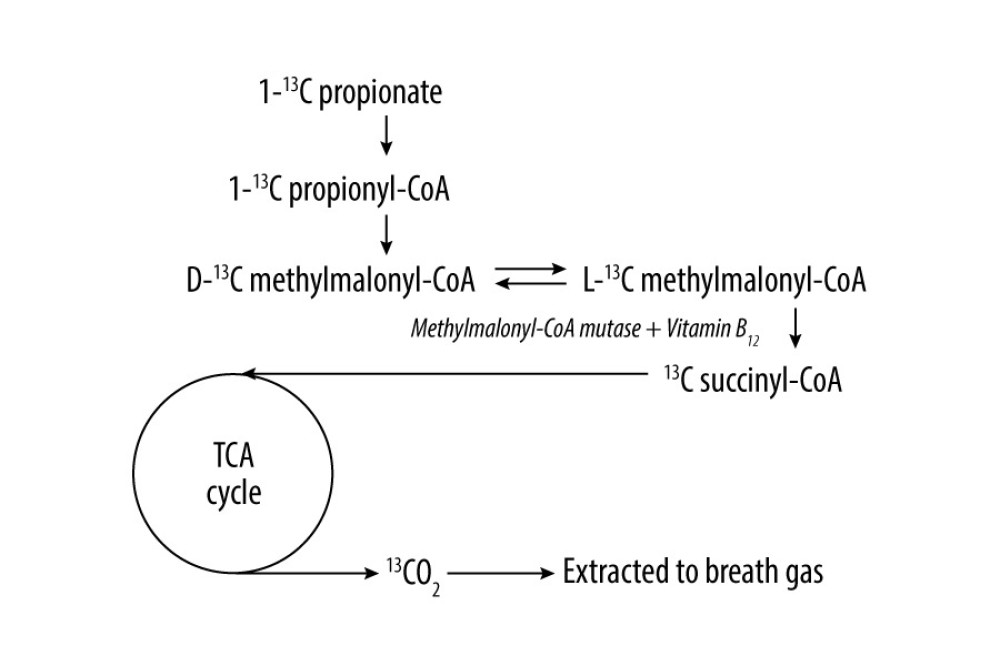 Figure 1. Propionate metabolism and measuring principle of the propionate breath test. Vitamin B12 functions as a coenzyme of methylmalonyl-CoA mutase in the conversion from L-methylmalonyl-CoA to succinyl-CoA in propionate metabolism. TCA – tricarboxylic acid.
Figure 1. Propionate metabolism and measuring principle of the propionate breath test. Vitamin B12 functions as a coenzyme of methylmalonyl-CoA mutase in the conversion from L-methylmalonyl-CoA to succinyl-CoA in propionate metabolism. TCA – tricarboxylic acid. 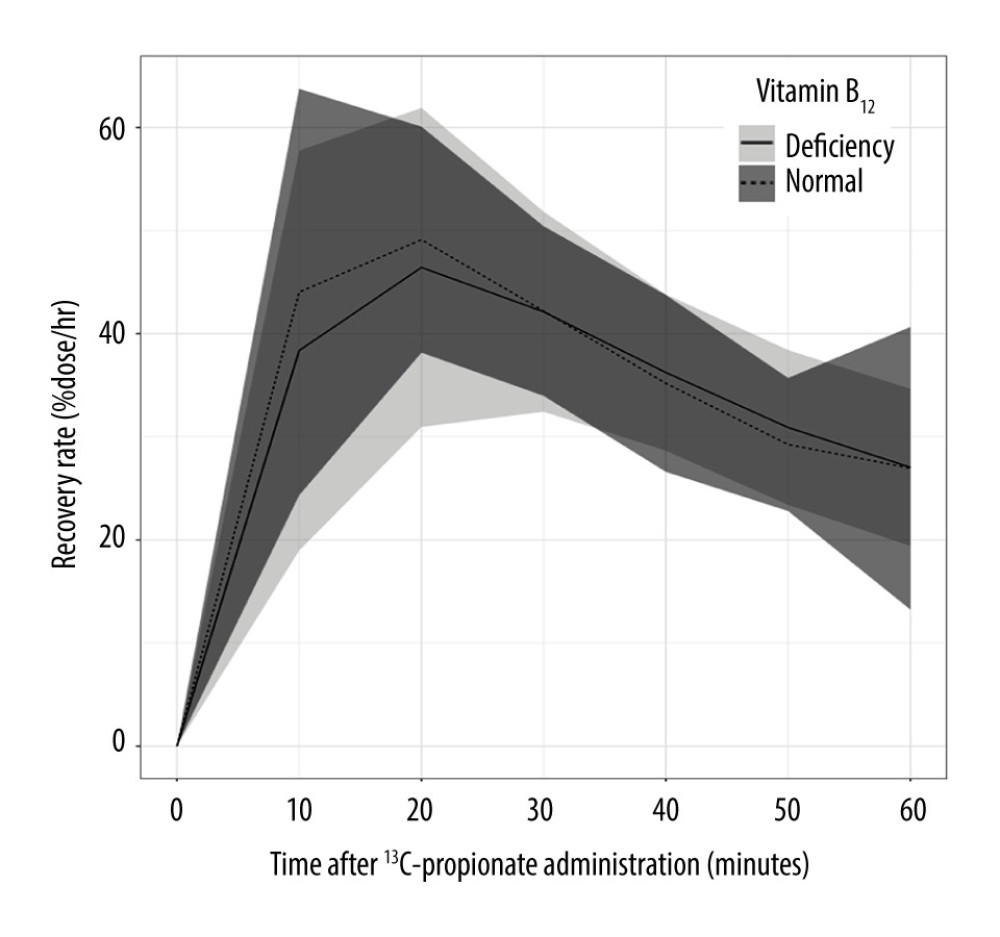 Figure 2. Comparisons of RRs from 1-h PBT between patients with normal and low serum VB12 levels. Horizontal axis and vertical axis indicate time (min) after 13C-propionate administration. and RR (%dose/h), respectively. VB12 deficiency was defined as serum VB12 level <145 pg/mL. The tinted area around each line indicates standard deviation. There were no significant differences of RRs between the 2 groups. PBT – 13C-propionate breath test; RR – 13C recovery rate; VB12 – vitamin B12.
Figure 2. Comparisons of RRs from 1-h PBT between patients with normal and low serum VB12 levels. Horizontal axis and vertical axis indicate time (min) after 13C-propionate administration. and RR (%dose/h), respectively. VB12 deficiency was defined as serum VB12 level <145 pg/mL. The tinted area around each line indicates standard deviation. There were no significant differences of RRs between the 2 groups. PBT – 13C-propionate breath test; RR – 13C recovery rate; VB12 – vitamin B12. 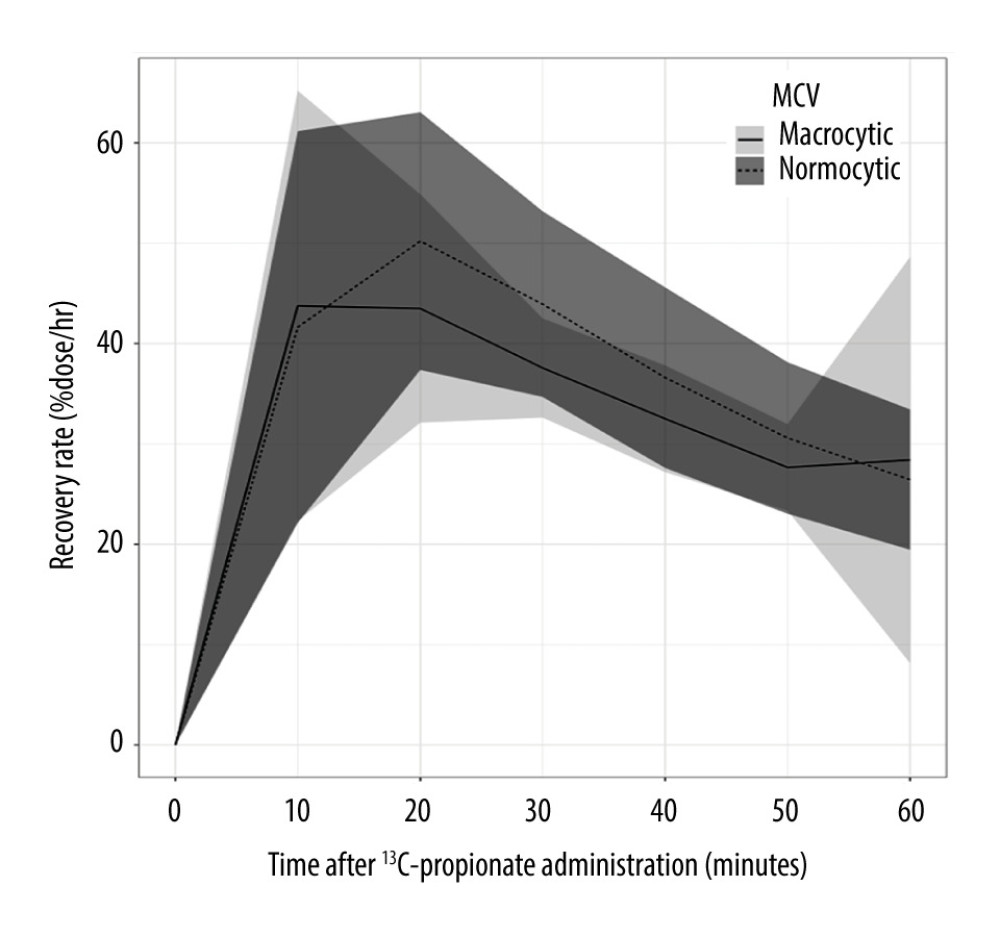 Figure 3. Comparisons of RRs in 1-h PBT between macrocytic and normocytic patients. Horizontal axis and vertical axis indicate time (min) after 13C-propionate administration. and RR (%dose/h), respectively. Macrocytosis is defined as MCV >100 fL. The tinted area around each line indicates standard deviation. RR20 and RR30 were significantly low in VB12 deficiency group compared than in the normal group. MCV – mean corpuscular volume; PBT – 13C-propionate breath test; RR – 13C recovery rate; RR20 – RR at 20 min after administration of 13C-propionate; RR30 – RR at 30 min after administration of 13C-propionate; VB12 – vitamin B12.
Figure 3. Comparisons of RRs in 1-h PBT between macrocytic and normocytic patients. Horizontal axis and vertical axis indicate time (min) after 13C-propionate administration. and RR (%dose/h), respectively. Macrocytosis is defined as MCV >100 fL. The tinted area around each line indicates standard deviation. RR20 and RR30 were significantly low in VB12 deficiency group compared than in the normal group. MCV – mean corpuscular volume; PBT – 13C-propionate breath test; RR – 13C recovery rate; RR20 – RR at 20 min after administration of 13C-propionate; RR30 – RR at 30 min after administration of 13C-propionate; VB12 – vitamin B12. 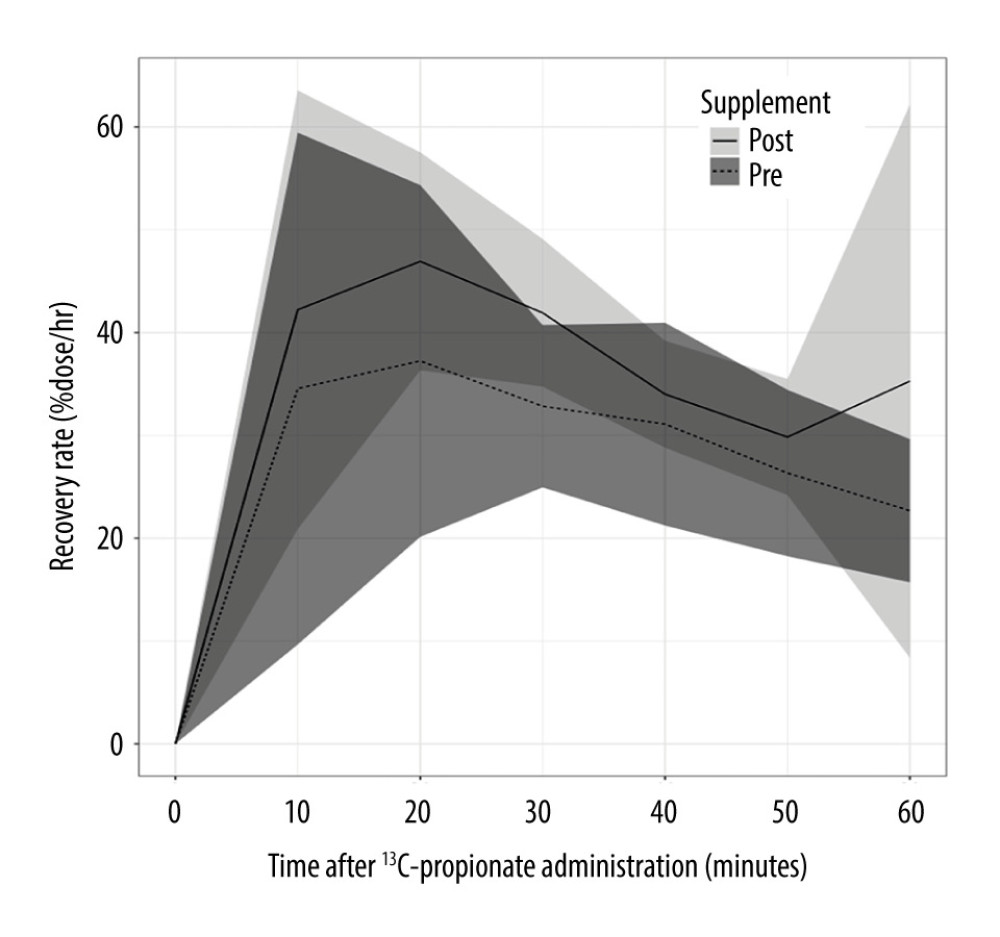 Figure 4. Comparisons of RRs in 1-h PBT between post- and pre-VB12 supplementation. Horizontal axis and vertical axis indicate time (min) after 13C-propionate administration and RR (%dose/h), respectively. The tinted area around each line indicates standard deviation. The RR30 was significantly higher in the post-supplement group than in the pre-supplement group. MCV – mean corpuscular volume; PBT – 13C-propionate breath test; RR – 13C recovery rate; RR30 – RR at 30 min after administration of 13C-propionate; VB12 – vitamin B12.
Figure 4. Comparisons of RRs in 1-h PBT between post- and pre-VB12 supplementation. Horizontal axis and vertical axis indicate time (min) after 13C-propionate administration and RR (%dose/h), respectively. The tinted area around each line indicates standard deviation. The RR30 was significantly higher in the post-supplement group than in the pre-supplement group. MCV – mean corpuscular volume; PBT – 13C-propionate breath test; RR – 13C recovery rate; RR30 – RR at 30 min after administration of 13C-propionate; VB12 – vitamin B12. Tables
Table 1. Complaints or reason for PBT of the participants.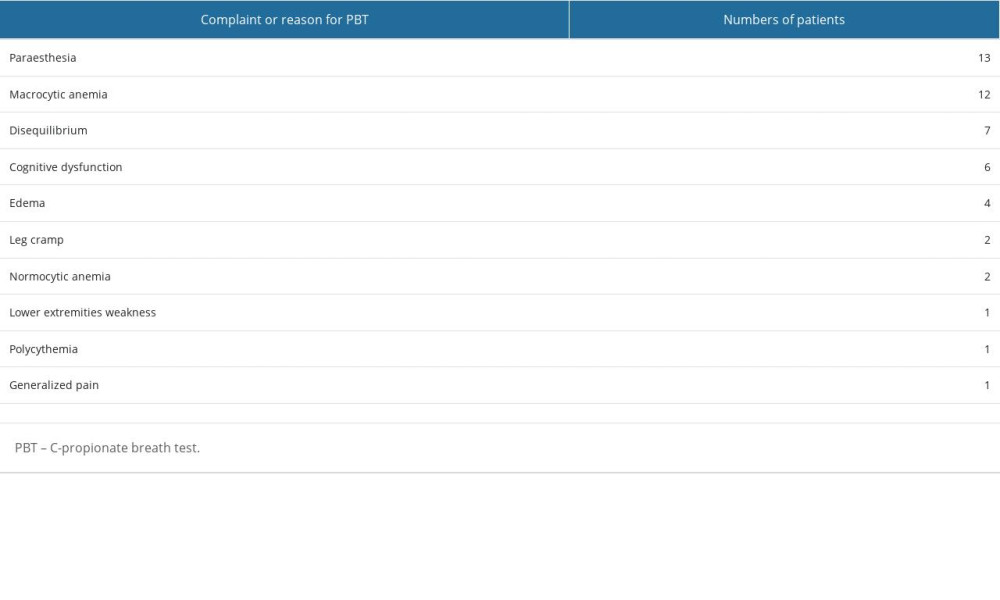 Table 2. Comparisons of RRs (%dose/h) from 1-h PBT between patients with normal and low serum VB12 levels.
Table 2. Comparisons of RRs (%dose/h) from 1-h PBT between patients with normal and low serum VB12 levels.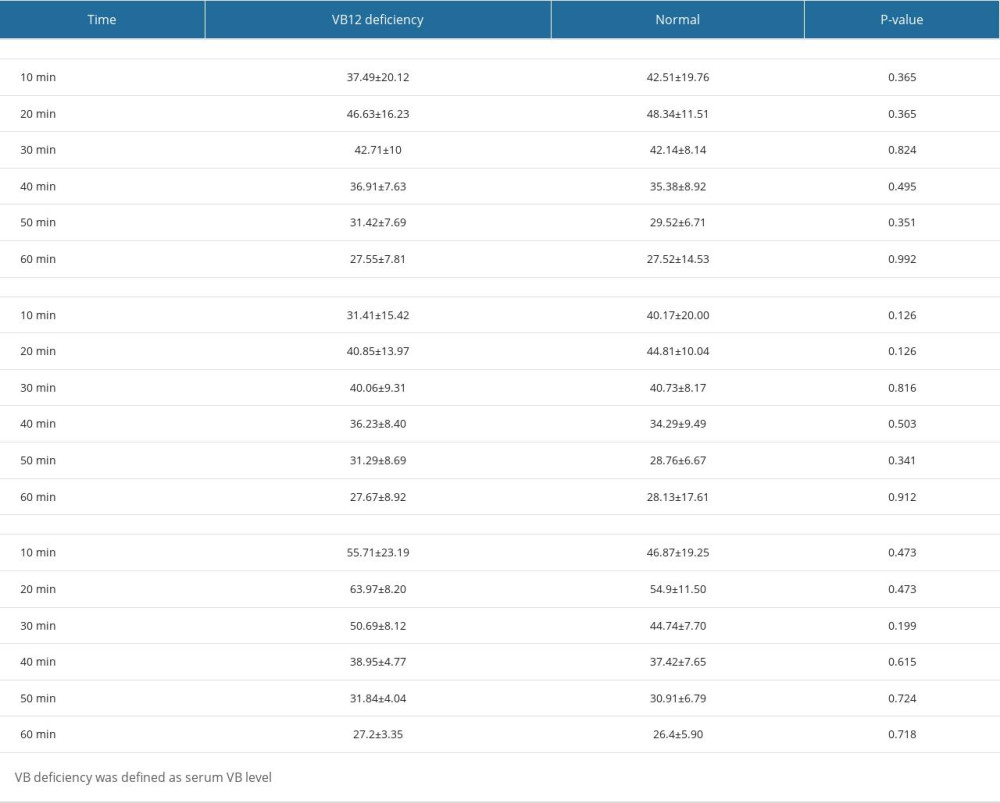 Table 3. Comparisons of RRs (%dose/h) from 1-h PBT between macrocytic and normocytic patients.
Table 3. Comparisons of RRs (%dose/h) from 1-h PBT between macrocytic and normocytic patients.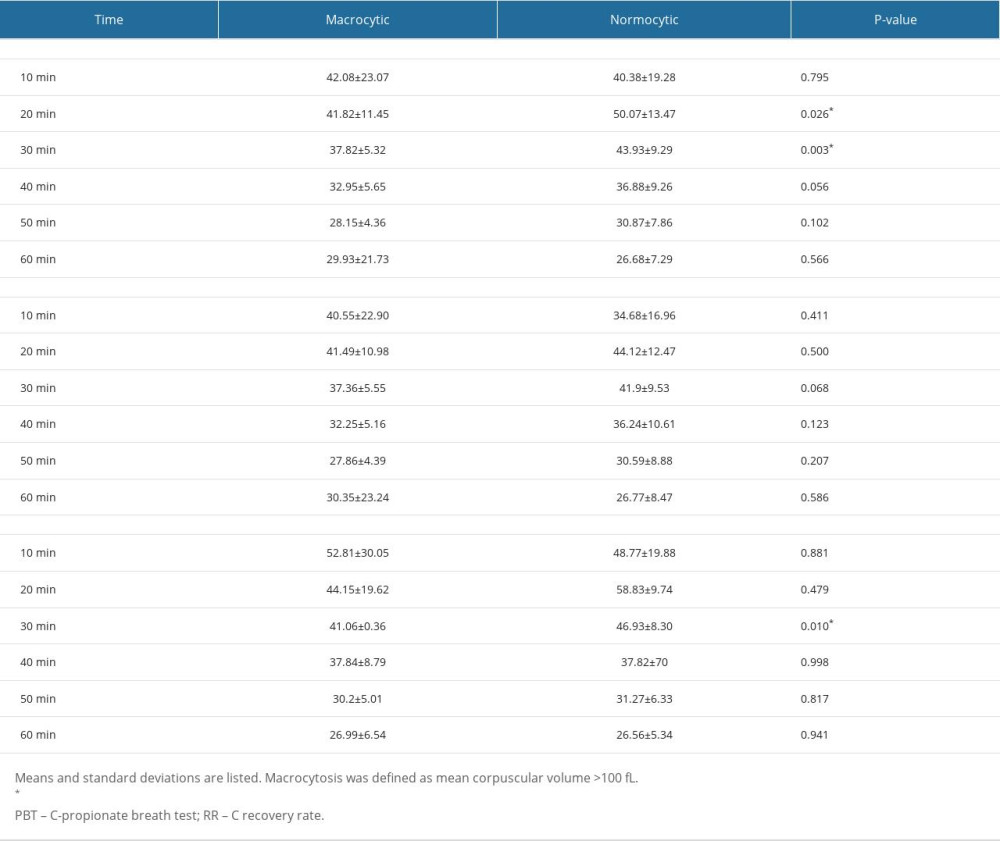 Table 4. Comparisons of RRs (%dose/h) from 1-h PBT between pre- and post- supplementation.
Table 4. Comparisons of RRs (%dose/h) from 1-h PBT between pre- and post- supplementation.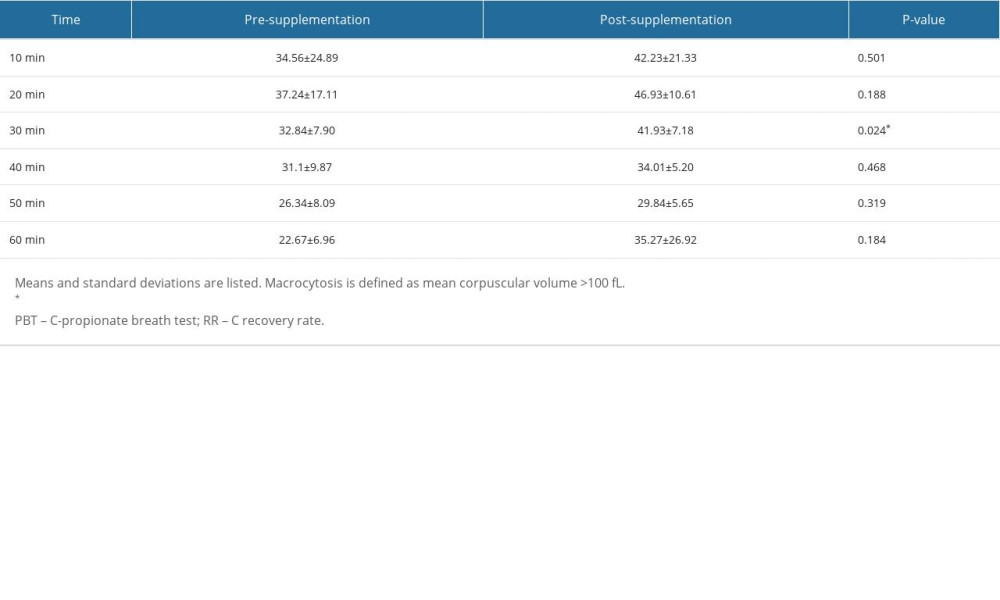
References
1. Stabler SP: N Engl J Med, 2013; 368; 149-60
2. Lam JR, Schneider JL, Zhao W, Corley DA, Proton pump inhibitor and histamine 2 receptor antagonist use and vitamin B 12 deficiency: JAMA, 2013; 310; 2435-42
3. Shigeta T, Sasaki Y, Maeda T, Pseudo-thrombotic microangiopathy caused by acquired cobalamin deficiency due to unintentional neglect: Intern Med, 2021; 60; 3833-37
4. Moore E, Mander A, Ames D: Int Psychogeriatr, 2012; 24; 541-56
5. Soh Y, Lee DH, Won CW: Medicine, 2020; 99; e21371
6. Health Quality Ontario: Ont Health Technol Assess Ser, 2013; 13; 1-45
7. Lambert D, Benhayoun S, Adjalla C, Alcoholic cirrhosis and cobalamin metabolism: Digestion, 1997; 58; 64-71
8. Smith AD, Refsum H, Vitamin B-12 and cognition in the elderly: Am J Clin Nutr, 2009; 89; 707S-11S
9. O’Leary F, Allman-Farinelli M, Samman S, Vitamin B 12 status, cognitive decline and dementia: A systematic review of prospective cohort studies: Br J Nutr, 2012; 108; 1948-61
10. Hoey L, Strain J, McNulty H, Studies of biomarker responses to intervention with vitamin B-12: A systematic review of randomized controlled trials: Am J Clin Nutr, 2009; 89; 1981S-96S
11. Devalia V, Hamilton MS, Molloy AM, Guidelines for the diagnosis and treatment of cobalamin and folate disorders: Br J Haematol, 2014; 166; 496-513
12. Wagner DA, Schatz R, Coston R: J Breath Res, 2011; 5; 046001
13. Urita Y, Watanabe T, Kawagoe N, Oxidation and absorption of glucose and fructose component ingested as a low glycemic sucrose-isomer isomaltulose (palatinose) in human: Indian J Appl Res, 2015; 5; 406-10
14. Nagao T, Hirokawa M, Diagnosis and treatment of macrocytic anemias in adults: J Gen Fam Med, 2017; 18; 200-4
15. Singh SJ, Dinkar A, Gupta P, Atam V: J Family Med Prim Care, 2022; 11; 2381-88
16. The R foundation: The R Project for statistical computing Available from: https://www.r-project.org/
17. Manoli I, Pass AR, Harrington EA: Genetics in Medicine, 2021; 23; 1522-33
18. DeLoughery TG, Microcytic anemia: N Engl J Med, 2014; 371; 1324-31
Figures
Figure 1. Propionate metabolism and measuring principle of the propionate breath test. Vitamin B12 functions as a coenzyme of methylmalonyl-CoA mutase in the conversion from L-methylmalonyl-CoA to succinyl-CoA in propionate metabolism. TCA – tricarboxylic acid.Figure 2. Comparisons of RRs from 1-h PBT between patients with normal and low serum VB12 levels. Horizontal axis and vertical axis indicate time (min) after 13C-propionate administration. and RR (%dose/h), respectively. VB12 deficiency was defined as serum VB12 level <145 pg/mL. The tinted area around each line indicates standard deviation. There were no significant differences of RRs between the 2 groups. PBT – 13C-propionate breath test; RR – 13C recovery rate; VB12 – vitamin B12.Figure 3. Comparisons of RRs in 1-h PBT between macrocytic and normocytic patients. Horizontal axis and vertical axis indicate time (min) after 13C-propionate administration. and RR (%dose/h), respectively. Macrocytosis is defined as MCV >100 fL. The tinted area around each line indicates standard deviation. RR20 and RR30 were significantly low in VB12 deficiency group compared than in the normal group. MCV – mean corpuscular volume; PBT – 13C-propionate breath test; RR – 13C recovery rate; RR20 – RR at 20 min after administration of 13C-propionate; RR30 – RR at 30 min after administration of 13C-propionate; VB12 – vitamin B12.Figure 4. Comparisons of RRs in 1-h PBT between post- and pre-VB12 supplementation. Horizontal axis and vertical axis indicate time (min) after 13C-propionate administration and RR (%dose/h), respectively. The tinted area around each line indicates standard deviation. The RR30 was significantly higher in the post-supplement group than in the pre-supplement group. MCV – mean corpuscular volume; PBT – 13C-propionate breath test; RR – 13C recovery rate; RR30 – RR at 30 min after administration of 13C-propionate; VB12 – vitamin B12. Tables
Table 1. Complaints or reason for PBT of the participants.Table 2. Comparisons of RRs (%dose/h) from 1-h PBT between patients with normal and low serum VB12 levels.Table 3. Comparisons of RRs (%dose/h) from 1-h PBT between macrocytic and normocytic patients.Table 4. Comparisons of RRs (%dose/h) from 1-h PBT between pre- and post- supplementation.Table 1. Complaints or reason for PBT of the participants.Table 2. Comparisons of RRs (%dose/h) from 1-h PBT between patients with normal and low serum VB12 levels.Table 3. Comparisons of RRs (%dose/h) from 1-h PBT between macrocytic and normocytic patients.Table 4. Comparisons of RRs (%dose/h) from 1-h PBT between pre- and post- supplementation. In Press
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Review article
Anisodus tanguticus in Cancer Research: A Review of Traditional Use, Phytochemistry, Extraction Methods, an...Med Sci Monit In Press; DOI: 10.12659/MSM.952999
Clinical Research
Nasal Mucociliary Clearance and Its Relationship With Disease Severity in Patients With Multiple SclerosisMed Sci Monit In Press; DOI: 10.12659/MSM.952850
Clinical Research
Modified Thoracoabdominal Nerves Block Through the Perichondrial Approach vs Subcostal Transversus Abdomini...Med Sci Monit In Press; DOI: 10.12659/MSM.953976
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,570
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,762,188
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,310
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,927
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387