25 March 2025: Clinical Research
Inflammatory Biomarkers in Smokers: Implications for Ligamentum Flavum Hypertrophy
Eyüp Çetin A 1*, Dilara Başgül Sagiri B 1, Eylem Burcu Kahraman Özlü D 1, Ezgi Akar BD 1, Eray Metin Güler DOI: 10.12659/MSM.947508
Med Sci Monit 2025; 31:e947508






Abstract
BACKGROUND: Ligamentum flavum (LF) hypertrophy is a key contributor to spinal pathologies such as lumbar and cervical disc herniations and spinal stenosis. Smoking, as a modifiable lifestyle factor, is implicated in systemic inflammation and oxidative stress, potentially exacerbating LF hypertrophy. This study aimed to compare the expression of alpha-1 antitrypsin (AAT), interleukin-1 beta (IL-1 beta), interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-alpha) in the lumbar ligamentum flavum from 27 smokers and 31 non-smokers.
MATERIAL AND METHODS: LF tissue samples were collected during spinal surgeries. Demographic, anthropometric, and clinical data were recorded. ELISA was used to quantify levels of AAT, IL-1β, IL-6, and TNF-α. Statistical analyses included t-tests, Mann-Whitney U tests, and receiver operating characteristic (ROC) curve analyses. Statistical significance was set at p<0.05.
RESULTS: Smokers exhibited significantly higher levels of IL-1β (p<0.001), IL-6 (p=0.004), and TNF-α (p<0.001), while AAT levels were significantly lower (p<0.001) compared to non-smokers. ROC analysis identified IL-1β (AUC=0.828; p<0.001) and TNF-α (AUC=0.801; p<0.001) as highly effective markers for distinguishing smokers from non-smokers, while IL-6 (AUC=0.730; p=0.003) showed moderate diagnostic accuracy. AAT (AUC=0.867; p<0.001) demonstrated excellent sensitivity (96.3%) for detecting smoking-related effects.
CONCLUSIONS: Smoking contributes significantly to systemic inflammation and oxidative stress, leading to biochemical changes that may drive LF hypertrophy. These findings underscore the importance of smoking cessation as a modifiable risk factor in the management of spinal pathologies.
Keywords: Ligamentum Flavum, Hypertrophy, Smoking, biomarkers, Spinal Cord Compression, Humans, Male, Female, Middle Aged, Interleukin-6, tumor necrosis factor-alpha, adult, Interleukin-1beta, inflammation, smokers, ROC Curve, alpha 1-Antitrypsin, Oxidative stress, Aged
Introduction
The ligamentum flavum (LF) is a key structural component of the spine, composed primarily of elastic fibers that maintain spinal stability and facilitate movement. However, hypertrophy or thickening of the LF is a major contributor to spinal pathologies such as lumbar and cervical disc herniations and spinal stenosis. Understanding whether LF thickening results from mechanical buckling or true hypertrophy involving cellular and extracellular matrix changes is critical for developing effective treatments [1].
Research has shown that both mechanical and biochemical factors contribute to LF hypertrophy. Wild-type transthyretin amyloidosis (ATTRwt) has been linked to significant amyloid deposition in lumbar LF tissue, highlighting systemic biochemical influences [2]. Additionally, N-acetylcysteine (NAC) has demonstrated potential in reducing oxidative stress-induced inflammation and fibrosis in hypertrophic LF cells [3]. ATTRwt deposition across all lumbar levels further emphasizes the importance of biochemical contributors to LF thickening [4].
LF ossification is also associated with thoracic myelopathy, a severe spinal cord compression disorder. Minimally invasive procedures like percutaneous full endoscopic posterior decompression have shown promise in managing ossified LF, underscoring the need for early diagnosis and targeted interventions [5–8]. Environmental factors, such as skeletal fluorosis, have also been implicated in LF ossification [9].
Preservation of the LF during spinal surgeries, such as percutaneous endoscopic lumbar interlaminar discectomy, may improve postoperative outcomes and reduce recurrence rates [10]. Studies analyzing LF in lumbar disc herniation and spinal stenosis patients reveal distinct biochemical and structural differences, offering insights into disease progression and treatment options [11].
Environmental and lifestyle factors, particularly smoking, have been recognized as significant contributors to LF hypertrophy and other spinal disorders. Nicotine promotes intervertebral disc degeneration through oxidative stress, inflammation, and apoptosis [12–14], explaining the clinical link between smoking and spinal degeneration [15]. Passive smoking also triggers early gene expression changes related to disc degeneration [16].
Smoking is a well-established risk factor for lumbar disc herniation, with evidence linking it to spinal degeneration and DNA damage [17,18]. Animal models have confirmed that chronic tobacco exposure leads to severe spinal degeneration [19]. Radiographic studies further support the association between smoking and cervical spine degeneration, emphasizing the need for smoking cessation as a preventive strategy [20].
Therefore, this study aimed to compare the expression of alpha-1 antitrypsin (AAT), interleukin-1 beta (IL-1 beta), interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-alpha) in the lumbar ligamentum flavum from 27 smokers and 31 non-smokers.
Material and Methods
STUDY DESIGN AND ETHICS APPROVAL:
This study was conducted at the Department of Neurosurgery, Haydarpaşa Numune Training and Research Hospital, utilizing tissue samples collected during spinal surgeries. Ethics approval was obtained from the Scientific Research Ethics Committee of the University of Health Sciences Hamidiye (Approval No: 14/25). Prior to participation, all patients provided written informed consent after being thoroughly informed about the study’s objectives, methodologies, potential risks, and their right to withdraw at any stage without any consequences.
The study was designed as a prospective cohort study to analyze the biochemical differences in the ligamentum flavum (LF) between smokers and non-smokers. A total of 58 patients were included in the study, with 27 classified as smokers and 31 as non-smokers. Ligamentum flavum tissue samples were obtained from patients who underwent surgical intervention for lumbar spinal stenosis and lumbar disc herniation as part of routine neurosurgical procedures. These samples were then subjected to biochemical analyses to determine potential differences between the groups based on smoking status.
STUDY POPULATION:
A total of 58 patients scheduled for lumbar spinal decompression or lumbar disc herniation surgery were included in the study. Among these, 27 patients were identified as smokers and 31 as non-smokers. Inclusion criteria required participants to be eligible for spinal surgery, to provide informed consent, and to have no contraindications for surgical intervention. Smoking status was primarily determined through self-reporting and, where possible, was corroborated using medical history records and biochemical markers such as serum cotinine levels.
To control for potential confounding factors, demographic and clinical data were collected for each participant, including age, sex, weight, height, body mass index (BMI), history of chronic diseases, alcohol consumption, and occupational exposure to heavy lifting. This information was systematically recorded to minimize potential biases in the biochemical analysis and ensure that any observed differences were attributable primarily to smoking status.
SAMPLE COLLECTION AND PROCESSING:
During each surgical procedure, ligamentum flavum tissue samples were carefully excised under sterile conditions to prevent contamination. Immediately after extraction, the tissue samples were snap-frozen in liquid nitrogen (Linde, Munich, Germany) and stored at −80°C in an ultra-low temperature freezer (Thermo Fisher Scientific, Waltham, MA, USA) to preserve biochemical integrity.
For biochemical analysis, tissue homogenization was performed using a standardized protocol in an ice-cold phosphate-buffered saline (PBS) solution at pH 7.4. The PBS solution was obtained from Sigma-Aldrich (St. Louis, MO, USA). Tissue homogenization was carried out under controlled laboratory conditions to maintain consistency across samples. Following homogenization, the samples were centrifuged at 12 000 g for 20 minutes at 4°C using a high-speed refrigerated centrifuge (Eppendorf 5417R, Hamburg, Germany). The supernatants were then carefully collected and stored at −80°C until further biochemical assessments were conducted.
BIOCHEMICAL ANALYSIS:
Quantification of inflammatory biomarkers, including alpha-1 antitrypsin (AAT), interleukin-1 beta (IL-1β), interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-α), was performed using enzyme-linked immunosorbent assay (ELISA) kits. The ELISA kits used in this study were obtained from Btlab (Shanghai, China) and included the following specific catalog numbers: AAT (Cat. No. E0753Hu), IL-1β (Cat. No. E0143Hu), IL-6 (Cat. No. E0090Hu), and TNF-α (Cat. No. E0082Hu). All assays were conducted according to the manufacturer’s instructions to ensure accuracy and reliability.
Each sample was analyzed in triplicate to enhance data reproducibility. Optical density (OD) readings were measured using a microplate reader (BioTek Synergy™, HTX Multimode Reader, U.S.A) at the specified wavelengths recommended by the manufacturer. Calibration curves were generated for each biomarker using standard solutions provided in the ELISA kits. To ensure internal assay validity, control samples with known biomarker concentrations were included in every batch. The inter- and intra-assay coefficient of variation (CV) was maintained below 10% to guarantee precision and consistency across the analyses.
STATISTICAL ANALYSIS:
All statistical analyses were performed using SPSS, version 27.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were expressed as mean±standard deviation (SD), median, minimum, maximum, frequency, and percentages as appropriate. The normality of data distribution was assessed using the Kolmogorov-Smirnov and Shapiro-Wilk tests.
For continuous variables exhibiting a normal distribution, independent sample t-tests were employed to compare differences between smokers and non-smokers. For variables that did not follow a normal distribution, the Mann-Whitney U test was applied. Categorical variables were analyzed using the chi-square test or Fisher’s exact test, depending on whether the chi-square assumptions were met.
To further evaluate the potential diagnostic value of the biochemical markers, receiver operating characteristic (ROC) curve analysis was conducted. This analysis was used to determine effect sizes, assess diagnostic accuracy, and establish optimal cut-off values for the inflammatory biomarkers. A p-value of less than 0.05 was considered statistically significant for all analyses.
Results
DEMOGRAPHIC CHARACTERISTICS:
A total of 58 patients undergoing lumbar spinal surgeries for decompression or disc herniation were included in the study. Among these, 27 were smokers (46.6%) and 31 were non-smokers (53.4%). The inclusion criteria required participants to be scheduled for spinal decompression or lumbar disc herniation surgeries, provide informed consent, and have no contraindications for surgery.
The participants’ average age was 50.5±13.8 years, ranging from 22 to 82 years, with a median age of 52 years. Smokers were significantly younger (mean: 44.3±11.1 years; median: 41.0) compared to non-smokers (mean: 55.9±13.8 years; median: 57.0; p=0.001).
ANTHROPOMETRIC MEASURES:
Table 1 summarizes the anthropometric data of the study population. Participants’ body weights ranged from 42 to 155 kg, with a mean of 78.3±17.5 kg and a median of 77 kg. Heights ranged from 150 to 188 cm, with a mean of 166.4±9.2 cm and a median of 166.5 cm.
The body mass index (BMI) varied from 16.4 to 51.8, with a mean value of 28.2±5.4 and a median of 27.1. Smokers had a significantly lower BMI (mean: 26.2±4.3; median: 25.4) compared to non-smokers (mean: 29.9±5.8; median: 29.4; p=0.008). These BMI differences highlight potential metabolic effects associated with smoking.
CLINICAL CHARACTERISTICS AND LIFESTYLE FACTORS:
The prevalence of chronic diseases was documented in 32.8% of participants, with 67.2% reporting no chronic illnesses. Although chronic disease prevalence was higher among non-smokers (38.7%) compared to smokers (25.9%), this difference was not statistically significant (p=0.301).
Alcohol consumption was reported by 10.3% of participants, with smokers showing a higher prevalence (18.5%) compared to non-smokers (3.2%). However, this difference did not reach statistical significance (p=0.056). Heavy lifting exposure, a known contributor to ligamentum flavum hypertrophy, was significantly more common in smokers (22.2%) compared to non-smokers (3.2%; p=0.027).
BIOCHEMICAL MARKERS:
The biochemical markers of inflammation demonstrated substantial variability between smokers and non-smokers. Table 2 provides a detailed comparison of these markers, which include IL-1β, IL-6, TNF-α, and AAT. IL-1β levels ranged from 202.5 to 907.8 pg/mL, with a mean of 503.3±182.6 pg/mL and a median of 475.5 pg/mL. Smokers exhibited significantly higher IL-1β levels (mean: 616.5±171.8 pg/mL; median: 624.1 pg/mL) compared to non-smokers (mean: 404.7±127.2 pg/mL; median: 385.8 pg/mL; p<0.001). IL-6 levels ranged from 55.9 to 190.3 pg/mL, with a mean of 107.7±31.5 pg/mL and a median of 104.9 pg/mL. Smokers had significantly elevated IL-6 levels (mean: 120.3±30.7 pg/mL; median: 114.8 pg/mL) compared to non-smokers (mean: 96.8±28.4 pg/mL; median: 89.2 pg/mL; p=0.004).
TNF-α levels ranged from 10.5 to 402.7 pg/mL, with a mean of 226.6±96.3 pg/mL and a median of 217.6 pg/mL. Smokers demonstrated significantly higher TNF-α levels (mean: 276.7±107.6 pg/mL; median: 304.0 pg/mL) compared to non-smokers (mean: 183.0±58.1 pg/mL; median: 175.3 pg/mL; p<0.001). AAT levels ranged from 0.31 to 4.92 pg/mL, with a mean of 1.69±1.28 pg/mL and a median of 1.11 pg/mL. Smokers had significantly lower AAT levels (mean: 0.88±0.53 pg/mL; median: 0.78 pg/mL) compared to non-smokers (mean: 2.40±1.33 pg/mL; median: 2.63 pg/mL; p<0.001).
The findings indicate that smoking is significantly associated with elevated inflammatory biomarkers (IL-1β, IL-6, TNF-α) and reduced anti-inflammatory markers (AAT). These results highlight the chronic inflammatory state induced by smoking, which may contribute to ligamentum flavum hypertrophy.
DEMOGRAPHIC AND GENDER DISTRIBUTION:
Table 2 provides a comparative analysis of demographic and sex distribution between smokers and non-smokers. Smokers were significantly younger than non-smokers. Smokers had a mean age of 44.3±11.1 years (median: 41.0), while non-smokers had a mean age of 55.9±13.8 years (median: 57.0). This difference was statistically significant (p=0.001), indicating that younger individuals in the study population were more likely to smoke. No statistically significant difference was observed in sex distribution between smokers and non-smokers. Females were slightly more prevalent among smokers (59.3%) compared to non-smokers (41.9%), but this difference was not statistically significant (p=0.188).
ANTHROPOMETRIC MEASURES:
The anthropometric characteristics of the study population are detailed in Table 2. Smokers had a mean body weight of 74.9±16.2 kg (median: 70.0), whereas non-smokers had a mean body weight of 81.3±18.3 kg (median: 78.0). The difference was not statistically significant (p=0.145). Smokers’ mean height was 168.5±7.4 cm (median: 168.0), and non-smokers’ mean height was 164.6±10.3 cm (median: 165.0). This difference was also not statistically significant (p=0.107). Smokers had a significantly lower BMI (mean: 26.2±4.3; median: 25.4) compared to non-smokers (mean: 29.9±5.8; median: 29.4; p=0.008). This suggests that smoking may be associated with lower body mass, potentially due to its metabolic effects.
CHRONIC DISEASES AND LIFESTYLE FACTORS:
The prevalence of chronic diseases was slightly lower among smokers (25.9%) compared to non-smokers (38.7%), but this difference was not statistically significant (p=0.301). Alcohol use was reported by 18.5% of smokers compared to 3.2% of non-smokers, but this difference was not statistically significant (p=0.056). Smokers were significantly more likely to report exposure to heavy lifting (22.2%) compared to non-smokers (3.2%; p=0.027). This finding suggests that occupational or lifestyle factors may compound the effects of smoking on ligamentum flavum hypertrophy.
LIGAMENTUM FLAVUM SIDE INVOLVEMENT:
No significant differences were observed in involvement of the right side (p=0.702), left side (p=0.847), or bilateral involvement (p=0.494) between smokers and non-smokers. This suggests that smoking does not preferentially affect the localization of ligamentum flavum hypertrophy.
BIOCHEMICAL MARKERS:
Table 2 highlights significant differences in inflammatory and anti-inflammatory biomarkers between smokers and non-smokers. Smokers had significantly higher IL-1β levels (mean: 616.5±171.8 pg/mL; median: 624.1) compared to non-smokers (mean: 404.7±127.2 pg/mL; median: 385.8; p<0.001). IL-6: Elevated IL-6 levels were observed in smokers (mean: 120.3±30.7 pg/mL; median: 114.8) compared to non-smokers (mean: 96.8±28.4 pg/mL; median: 89.2; p=0.004). TNF-α: TNF-α levels were significantly higher in smokers (mean: 276.7±107.6 pg/mL; median: 304.0) compared to non-smokers (mean: 183.0±58.1 pg/mL; median: 175.3; p<0.001). AAT: Anti-inflammatory AAT levels were significantly lower in smokers (mean: 0.88±0.53 pg/mL; median: 0.78) compared to non-smokers (mean: 2.40±1.33 pg/mL; median: 2.63; p<0.001).
KEY OBSERVATIONS:
Smokers demonstrated elevated levels of pro-inflammatory markers (IL-1β, IL-6, TNF-α) and lower levels of the anti-inflammatory marker (AAT). The significantly lower BMI in smokers supports the potential metabolic consequences of smoking, which may interact with systemic inflammation and ligamentum flavum hypertrophy. Heavy lifting exposure was notably more common among smokers, indicating the potential role of occupational stressors in exacerbating ligamentum flavum changes.
DIAGNOSTIC ACCURACY OF IL-1β:
The ability of IL-1β to differentiate between smokers and non-smokers was evaluated using ROC analysis. The area under the curve (AUC) for IL-1β was 0.828 (95% CI: 0.721–0.935, p<0.001), indicating a high level of diagnostic accuracy. An AUC above 0.8 suggests excellent discriminatory performance (Table 3, Figure 1).
At the optimized cut-off value of 510 pg/mL, the AUC slightly decreased to 0.790 (95% CI: 0.667–0.913, p<0.001). Despite the slight reduction, this threshold still demonstrated strong diagnostic performance. Sensitivity reflects the ability of IL-1β to correctly identify smokers. At the 510 pg/mL cut-off, 74.1% of smokers were correctly identified. Specificity indicates the ability to correctly classify non-smokers. Here, 83.9% of non-smokers were accurately identified as having IL-1β levels below the cut-off. PPV represents the probability that individuals with IL-1β levels >510 pg/mL are smokers. In this analysis, 80% of individuals exceeding the threshold were correctly identified as smokers. NPV indicates the probability that individuals with IL-1β levels ≤510 pg/mL are non-smokers. At the cut-off, 78.8% of participants below the threshold were correctly identified as non-smokers.
SIGNIFICANCE OF IL-1β AS A BIOMARKER:
IL-1β, a pro-inflammatory cytokine, plays a critical role in systemic inflammation, tissue remodeling, and cellular stress. Elevated IL-1β levels in smokers highlight the chronic inflammatory state induced by tobacco use, which may contribute to ligamentum flavum hypertrophy. The observed sensitivity and specificity values emphasize IL-1β’s potential as a reliable biomarker for smoking-related effects, with a low likelihood of false positives or negatives.
INTERPRETATION OF ROC ANALYSIS:
The ROC analysis provides an AUC of 0.828, indicating that IL-1β has an 82.8% probability of correctly distinguishing a randomly selected smoker from a non-smoker. The cut-off value of 510 pg/mL is a clinically actionable threshold, as smokers are significantly more likely to exhibit IL-1β levels exceeding this value due to heightened inflammatory responses.
CLINICAL UTILITY OF IL-1β:
The findings emphasize the utility of IL-1β as a biomarker for screening individuals at risk of smoking-related ligamentum flavum hypertrophy. Given its high sensitivity and specificity, IL-1β can serve as an effective tool for identifying smokers and assessing their risk for inflammation-related spinal changes.
DIAGNOSTIC ACCURACY OF IL-6:
The ROC curve analysis for IL-6 demonstrated moderate diagnostic accuracy in distinguishing smokers from non-smokers. The area under the curve (AUC) for IL-6 was 0.730 (95% CI: 0.598–0.862, p=0.003), indicating meaningful discriminatory capability, although not as strong as IL-1β. The optimized cut-off value for IL-6 was determined to be 102.5 pg/mL, where the AUC slightly increased to 0.744 (95% CI: 0.613–0.875, p=0.001) (Table 4, Figure 2).
DIAGNOSTIC PERFORMANCE AT THE 102.5 PG/ML CUT-OFF:
At this threshold, IL-6 correctly identified 77.8% of smokers, highlighting its value as a screening marker for individuals with smoking-related inflammation. The marker correctly classified 71.0% of non-smokers, though this reflects a moderate rate of false positives. Among participants with IL-6 levels >102.5 pg/mL, 70.0% were accurately identified as smokers. For IL-6 levels ≤102.5 pg/mL, 78.6% of participants were correctly classified as non-smokers.
DIAGNOSTIC ACCURACY OF TNF-α:
The ROC analysis for TNF-α revealed its robust diagnostic potential for differentiating smokers from non-smokers. The AUC for TNF-α was 0.768 (95% CI: 0.631–0.906, p<0.001), indicating good discriminatory power. At the optimized cut-off value of 260 pg/mL, the AUC increased further to 0.801 (95% CI: 0.679–0.923, p<0.001), reflecting strong diagnostic performance.
DIAGNOSTIC PERFORMANCE AT THE 260 PG/ML CUT-OFF:
At this threshold, TNF-α accurately identified 66.7% of smokers, a moderate sensitivity level balanced by its high specificity. TNF-α demonstrated excellent specificity, correctly excluding 93.5% of non-smokers, with minimal false positives. Among participants with TNF-α levels >260 pg/mL, 90.0% were confirmed as smokers, highlighting its utility in confirmatory testing. For TNF-α levels ≤260 pg/mL, 76.3% of individuals were accurately identified as non-smokers.
IL-6 INSIGHTS:
IL-6 is a key cytokine involved in inflammatory pathways and is often elevated in individuals with chronic conditions, including those affected by tobacco-related inflammation. While the AUC for IL-6 (0.730) is lower than that of IL-1β or TNF-α, its higher sensitivity (77.8%) makes it a valuable preliminary screening tool for identifying potential smokers.
TNF-α INSIGHTS:
TNF-α is a critical pro-inflammatory cytokine that plays a pivotal role in systemic inflammation and tissue remodeling. Its high specificity (93.5%) and PPV (90.0%) at the 260 pg/mL cut-off emphasize its reliability as a confirmatory marker for smoking-related inflammation. The robust diagnostic performance of TNF-α underscores its clinical relevance in identifying smoking-related inflammatory changes, particularly in ligamentum flavum hypertrophy.
CLINICAL RELEVANCE OF COMBINED MARKERS:
Combining IL-6 and TNF-α results may help clinicians achieve a balanced diagnostic strategy by leveraging IL-6’s higher sensitivity for initial screening and TNF-α’s higher specificity for confirmation. Together, these markers provide complementary insights into the chronic inflammatory state induced by smoking, supporting their clinical utility in evaluating ligamentum flavum hypertrophy and related spinal pathologies.
ROC ANALYSIS OF TNF-α:
The ROC curve analysis for TNF-α demonstrated strong discriminatory capability in distinguishing smokers from non-smokers. The area under the curve (AUC) for TNF-α was 0.768 (95% CI: 0.631–0.906, p<0.001), reflecting good diagnostic accuracy. When the cut-off value was optimized at 260 pg/mL, the AUC increased to 0.801 (95% CI: 0.679–0.923, p<0.001), underscoring the reliability of this marker (Table 5, Figure 3).
DIAGNOSTIC PERFORMANCE AT 260 PG/ML CUT-OFF:
At the 260 pg/mL threshold, TNF-α correctly identified 66.7% of smokers, highlighting its moderate sensitivity. This high specificity means that TNF-α reliably excluded 93.5% of non-smokers, with minimal false positives. Among participants with TNF-α levels >260 pg/mL, 90.0% were confirmed as smokers, indicating its strength as a confirmatory marker. For TNF-α levels ≤260 pg/mL, 76.3% of individuals were correctly identified as non-smokers, offering reliable exclusion of those without smoking-related inflammation.
BIOLOGICAL RELEVANCE OF TNF-α:
TNF-α is a critical pro-inflammatory cytokine involved in systemic inflammation, tissue remodeling, and immune responses. Elevated levels in smokers can be attributed to the chronic inflammatory states induced by smoking, leading to systemic effects such as ligamentum flavum hypertrophy, as observed in this study.
AUC INTERPRETATION:
The AUC of 0.768 indicates that TNF-α has a 76.8% probability of correctly classifying a randomly chosen smoker or non-smoker. At the optimized 260 pg/mL cut-off, the AUC improves to 0.801, emphasizing its strength as a diagnostic tool. This threshold effectively balances sensitivity and specificity, making it a practical and reliable marker for distinguishing smokers from non-smokers.
CLINICAL RELEVANCE OF THE 260 PG/ML THRESHOLD:
The optimized threshold of 260 pg/mL offers a strong balance between diagnostic accuracy and clinical applicability. TNF-α’s specificity of 93.5% ensures minimal false positives, making it an excellent confirmatory test. Although its sensitivity is moderate, it is sufficient for follow-up testing when combined with other markers like IL-6.
COMPARISON WITH IL-1β AND IL-6:
Compared to IL-1β and IL-6, TNF-α demonstrates higher specificity and PPV, making it more reliable for confirmatory testing rather than initial screening. Its moderate sensitivity indicates its limitations in detecting all smokers but ensures minimal false positives, reducing the risk of overdiagnosis. TNF-α has significant clinical utility as a biomarker for evaluating smoking-related inflammatory processes, particularly in the context of ligamentum flavum hypertrophy and other spinal pathologies. When combined with IL-6 (which has higher sensitivity), TNF-α can enhance overall diagnostic accuracy, allowing for effective screening and confirmation. This approach supports the use of multiple biomarkers to provide complementary diagnostic insights into smoking-induced inflammatory states.
ROC ANALYSIS OF TNF-α:
The ROC analysis for tumor necrosis factor-alpha (TNF-α) demonstrated strong discriminatory capability in distinguishing smokers from non-smokers. The AUC for TNF-α was 0.768 (95% CI: 0.631–0.906, p<0.001), indicating good diagnostic accuracy. When the cut-off value was optimized to 260 pg/mL, the AUC increased to 0.801 (95% CI: 0.679–0.923, p<0.001), underscoring the marker’s reliability (Table 6, Figure 4).
DIAGNOSTIC PERFORMANCE AT THE CUT-OFF VALUE (260 PG/ML):
At the threshold of 260 pg/mL, TNF-α successfully identified 66.7% of smokers at this cut-off value. Although moderate, this sensitivity is balanced by its high specificity. TNF-α exhibited high specificity, accurately identifying 93.5% of non-smokers. This minimizes false positives and enhances its clinical utility. Among individuals with TNF-α levels exceeding 260 pg/mL, 90.0% were confirmed as smokers, reflecting its effectiveness as a confirmatory biomarker. For TNF-α levels ≤260 pg/mL, 76.3% of individuals were correctly classified as non-smokers, offering reliable exclusion of individuals without smoking-related inflammation. TNF-α is a pro-inflammatory cytokine integral to processes such as inflammation, tissue remodeling, and immune regulation. Elevated TNF-α levels in smokers reflect the chronic inflammatory state induced by smoking, which contributes to systemic effects, including ligamentum flavum hypertrophy.
AUC INTERPRETATION AND CLINICAL RELEVANCE:
An AUC of 0.768 signifies that TNF-α has a 76.8% probability of correctly distinguishing between a smoker and a non-smoker when chosen randomly. With the cut-off value optimized at 260 pg/mL, the AUC improves to 0.801, highlighting its enhanced diagnostic ability. The 260 pg/mL cut-off value effectively balances sensitivity and specificity, making it a robust reference for distinguishing smokers from non-smokers. This threshold is particularly effective for confirming smoking status in individuals with elevated TNF-α levels.
COMPARISON WITH OTHER BIOMARKERS:
Compared to IL-1β and IL-6, TNF-α demonstrated higher specificity and higher PPV. At 93.5%, TNF-α reliably excludes non-smokers with minimal false positives, making it more suitable for confirmatory testing rather than initial screening. Its PPV of 90.0% indicates its superior utility in validating smoking status compared to other biomarkers. However, the moderate sensitivity of TNF-α underscores its limitations in detecting all smokers. This necessitates its use in conjunction with other biomarkers, such as IL-6, to improve overall diagnostic accuracy.
TNF-α has important clinical implications as a biomarker for evaluating smoking-related inflammatory responses, particularly in the context of ligamentum flavum hypertrophy and other spinal pathologies. When combined with IL-6 (which has higher sensitivity), TNF-α can provide a comprehensive diagnostic strategy by balancing sensitivity and specificity. This dual-marker approach could enable clinicians to effectively screen individuals at risk of smoking-induced inflammation, confirming the diagnoses with high specificity and minimizing false positives.
Discussion
This study shows the significant impact of smoking on ligamentum flavum (LF) hypertrophy by demonstrating its association with elevated levels of pro-inflammatory biomarkers (IL-1β, IL-6, TNF-α) and reduced levels of the anti-inflammatory protein alpha-1 antitrypsin (AAT). The findings suggest that smoking-induced systemic inflammation and oxidative stress contribute to LF hypertrophy, a key factor in spinal pathologies such as lumbar and cervical disc herniation and spinal stenosis. IL-1β and TNF-α emerged as robust confirmatory biomarkers for smoking-related inflammatory effects, with high discriminatory accuracy (AUC=0.828 and 0.801, respectively). IL-6, with moderate diagnostic accuracy (AUC=0.730) and high sensitivity, was identified as a useful screening tool. Furthermore, the study shows the diagnostic potential of AAT (AUC=0.867), emphasizing its role in detecting smoking-induced inflammation.
The significantly elevated levels of pro-inflammatory markers IL-1β, IL-6, and TNF-α in smokers, alongside reduced levels of the anti-inflammatory protein alpha-1 antitrypsin (AAT), reflect the systemic effects of smoking on tissue homeostasis. These findings align with previous studies identifying chronic inflammation and oxidative stress as mediators of spinal degeneration [17,19,20]. IL-1β is a key activator of the inflammasome pathway, which amplifies inflammatory cascades and tissue remodeling in response to chronic oxidative stress. Studies on spinal cord injuries have demonstrated that inhibition of inflammasome activation can protect against blood-spinal cord barrier disruption, reduce inflammatory cytokine release, and prevent excessive tissue fibrosis, suggesting a potential pathway for mitigating the inflammatory processes involved in ligamentum flavum hypertrophy [21]. Elevated IL-1β, a cytokine central to inflammation and tissue remodeling, has been linked to fibroblast activation in hypertrophic LF cells, exacerbating fibrosis and degradation [3,15]. Similarly, TNF-α is known to accelerate extracellular matrix degradation and fibrogenesis, contributing to LF hypertrophy [14]. The elevated levels of IL-6 observed in smokers further support its role as a mediator of fibrosis and inflammation in smoking-related spinal pathologies [6,13]. Conversely, the reduction in AAT levels suggests a diminished anti-inflammatory defense, compounding the effects of smoking-induced oxidative stress and inflammation [15]. Studies on curcumin’s anti-inflammatory properties demonstrate its ability to suppress TNF-α activation through modulation of the NF-κB pathway, offering insights into potential therapeutic strategies to mitigate smoking-induced inflammatory damage [22].
The diagnostic potential of IL-1β, TNF-α, IL-6, and AAT was evaluated using ROC curve analysis. IL-1β and TNF-α demonstrated strong discriminatory power, with AUC values of 0.828 and 0.801, respectively, making them robust confirmatory biomarkers for smoking-related inflammation. While IL-6 showed moderate diagnostic accuracy (AUC=0.730), its higher sensitivity (77.8%) supports its use as a screening tool. AAT, with an AUC of 0.867 and high sensitivity (96.3%), emerged as an effective indicator of smoking-induced inflammatory changes. These findings provide a foundation for integrating biomarker analysis into clinical practice for early detection and risk stratification.
The current findings are consistent with several studies investigating smoking’s role in spinal degeneration. Previous research has demonstrated strong associations between smoking and structural changes in spinal tissues, emphasizing the contributions of chronic inflammation and oxidative stress [17,19,20]. Smoking is also a well-established risk factor for lumbar disc herniation, with elevated inflammatory markers playing a pivotal role in disease progression [17,19,20].
Systemic contributors, such as transthyretin amyloidosis (ATTRwt), have also been implicated in LF hypertrophy through amyloid deposition [2,4]. While ATTRwt was not directly assessed in this study, the observed inflammatory markers in smokers may interact synergistically with conditions like ATTRwt to exacerbate LF hypertrophy. This potential interplay highlights the need for further research into the combined effects of smoking and systemic conditions on spinal pathologies.
These findings underscore the significant impact of smoking on spinal health, linking elevated pro-inflammatory markers and diminished anti-inflammatory defenses to LF hypertrophy. The diagnostic potential of IL-1β, TNF-α, IL-6, and AAT offers a promising avenue for personalized approaches to prevention and treatment. For instance, IL-1β and TNF-α could serve as confirmatory biomarkers, while IL-6 and AAT may be utilized as initial screening tools. Combining these markers may further enhance diagnostic accuracy.
Moreover, public health initiatives aimed at reducing smoking prevalence could significantly mitigate the burden of smoking-related spinal disorders. Smoking cessation emerges as a critical preventive strategy, with the potential to reduce systemic inflammation and its pathological consequences on the spine. Future research should explore the longitudinal impact of smoking cessation on biomarker levels and spinal health, as well as the efficacy of anti-inflammatory and antioxidant therapies in mitigating LF hypertrophy.
Despite its valuable insights, this study has several limitations. The sample size was relatively small, limiting the generalizability of the findings. Future research with larger cohorts is required to confirm these results and improve their applicability to diverse populations. The cross-sectional design precludes establishing a causal relationship between smoking and LF hypertrophy. Longitudinal studies are necessary to determine whether smoking cessation can reverse the observed biochemical and structural changes in LF tissues.
Methodological limitations include the reliance on self-reported smoking status, which may introduce recall bias. Although corroborated with biochemical markers where possible, discrepancies between self-reports and actual smoking habits could affect the accuracy of group assignments. The use of ELISA, while sensitive and reproducible, may not account for all potential confounders influencing biomarker levels. Additionally, the study focused on specific inflammatory markers and did not evaluate the potential synergistic effects of smoking with other systemic factors, such as amyloid deposition or genetic predispositions, on LF hypertrophy.
Conclusions
This study provides compelling evidence that smoking significantly contributes to ligamentum flavum (LF) hypertrophy by promoting a chronic inflammatory state, as demonstrated by elevated levels of IL-1β, IL-6, and TNF-α, and decreased levels of the anti-inflammatory protein alpha-1 antitrypsin (AAT). These findings suggest that smoking-induced oxidative stress and systemic inflammation play a pivotal role in the pathological remodeling of the LF, contributing to conditions such as lumbar spinal stenosis and disc herniation.
Biomarker analysis highlights IL-1β and TNF-α as highly effective confirmatory markers for smoking-related inflammation, with strong discriminatory accuracy (AUC=0.828 and 0.801, respectively), while IL-6 (AUC=0.730) emerges as a valuable screening tool. Notably, AAT (AUC=0.867) demonstrates exceptional sensitivity (96.3%) in detecting smoking-related inflammatory changes, reinforcing its potential as an early diagnostic marker.
Clinically, these results underscore the need for targeted smoking cessation strategies as part of spinal disorder prevention and management. Given that smoking exacerbates inflammatory pathways implicated in LF hypertrophy, proactive interventions – including cessation programs, anti-inflammatory therapies, and early biomarker screening – may mitigate disease progression and improve patient outcomes.
Future research should focus on longitudinal studies to establish causality between smoking cessation and biomarker normalization, as well as the efficacy of pharmacological interventions targeting IL-1β, IL-6, TNF-α, and AAT pathways. Integrating these biomarkers into routine clinical practice could enable personalized risk stratification and early intervention strategies for individuals at heightened risk of smoking-induced spinal degeneration.
In conclusion, smoking is a modifiable risk factor with profound biochemical implications for spinal health. Addressing its inflammatory consequences through prevention, early diagnosis, and tailored treatment approaches may significantly reduce the burden of LF hypertrophy and related spinal pathologies.
Figures
 Figure 1. ROC curve analysis of IL-1β levels for evaluating diagnostic accuracy between smokers and non-smokers.
Figure 1. ROC curve analysis of IL-1β levels for evaluating diagnostic accuracy between smokers and non-smokers.  Figure 2. Diagnostic accuracy of IL-6 Levels: ROC curve analysis comparing smokers and non-smokers.
Figure 2. Diagnostic accuracy of IL-6 Levels: ROC curve analysis comparing smokers and non-smokers.  Figure 3. Evaluation of TNF-α as a biomarker for smoking-related inflammation: ROC analysis.
Figure 3. Evaluation of TNF-α as a biomarker for smoking-related inflammation: ROC analysis.  Figure 4. ROC curve assessment of alpha-1 antitrypsin (AAT) for detecting smoking-induced biochemical changes in LF tissue.
Figure 4. ROC curve assessment of alpha-1 antitrypsin (AAT) for detecting smoking-induced biochemical changes in LF tissue. Tables
Table 1. Demographic and clinical characteristics of study participants, including BMI and smoking status.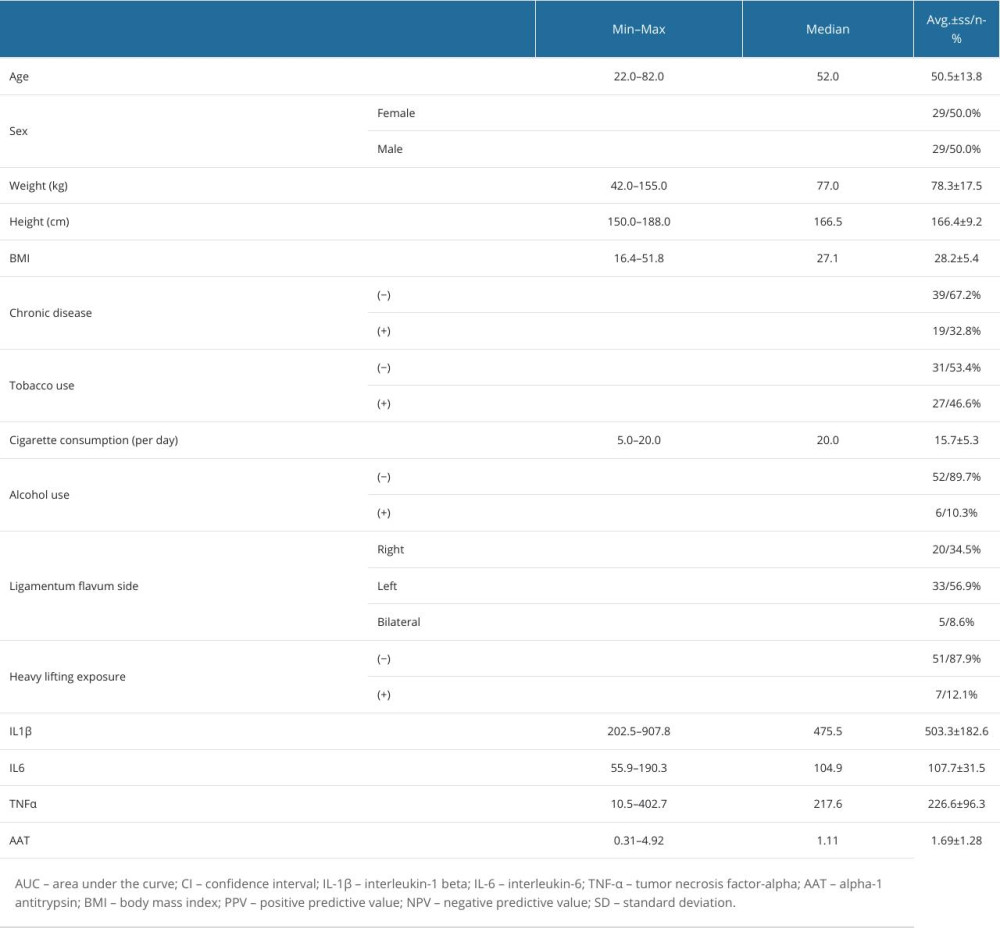 Table 2. Comparative analysis of demographic, clinical, and biochemical variables between smokers and non-smokers.
Table 2. Comparative analysis of demographic, clinical, and biochemical variables between smokers and non-smokers. Table 3. Diagnostic accuracy of IL-1β in differentiating smokers from non-smokers: ROC analysis results.
Table 3. Diagnostic accuracy of IL-1β in differentiating smokers from non-smokers: ROC analysis results. Table 4. Diagnostic performance of IL-6 levels in distinguishing smokers from non-smokers.
Table 4. Diagnostic performance of IL-6 levels in distinguishing smokers from non-smokers.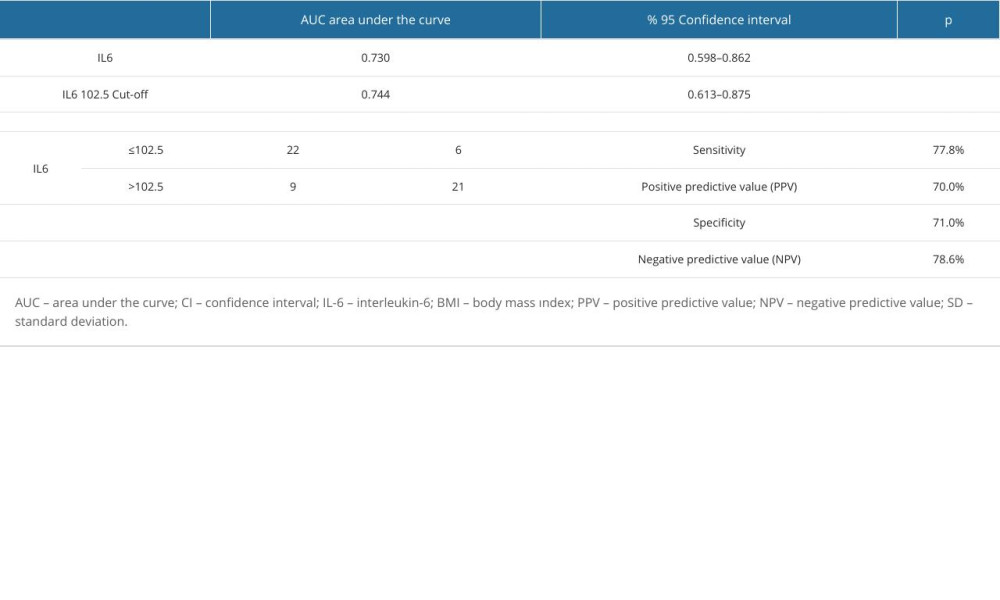 Table 5. ROC analysis of TNF-α as a biomarker for smoking-related inflammatory changes in LF tissue.
Table 5. ROC analysis of TNF-α as a biomarker for smoking-related inflammatory changes in LF tissue. Table 6. Diagnostic value of alpha-1 antitrypsin (AAT) levels in identifying smoking-induced LF hypertrophy.
Table 6. Diagnostic value of alpha-1 antitrypsin (AAT) levels in identifying smoking-induced LF hypertrophy.
References
1. Quencer RM, Smoker WRK, The “thickened” ligamentum flavum: Is it buckling or enlargement?: Am J Neuroradiol, 2010; 31(2); 181-90
2. George KM, Hernandez NS, Breton J, Increased thickness of lumbar spine ligamentum flavum in wild-type transthyretin amyloidosis: J Clin Neurosci, 2021; 84; 33-37
3. Hsu YC, Chuang HC, Tsai KL, Administration of N-acetylcysteine to regress the fibrogenic and proinflammatory effects of oxidative stress in hypertrophic ligamentum flavum cells: Oxid Med Cell Longev, 2022; 2022 1380353
4. Lee CH, Kuo YJ, Chang AP, Huang HM, The impact of amyloid deposits on ligamentum flavum hypertrophy: Insights from transthyretin amyloidosis research: Spine J, 2020; 20(12); 1916-22
5. Li X, An B, Gao H, Surgical results and prognostic factors following percutaneous full endoscopic posterior decompression for thoracic myelopathy caused by ossification of the ligamentum flavum: Sci Rep, 2020; 10(1); 1305
6. Sudhir G, Jayabalan SV, Gadde S, Analysis of factors influencing ligamentum flavum thickness in lumbar spine: A radiological study of 1070 disc levels in 214 patients: Clin Neurol Neurosurg, 2019; 182; 19-24
7. George KM, Dowd RS, Nail J, Wild-type transthyretin amyloidosis occurring in the ligamentum flavum of the cervicothoracic spine: World Neurosurg, 2020; 142; e325-e30
8. Li Z, Ren D, Zhao Y, Clinical characteristics and surgical outcome of thoracic myelopathy caused by ossification of the ligamentum flavum: A retrospective analysis of 85 cases: Spinal Cord, 2016; 54(3); 188-96
9. Wang W, Kong L, Zhao H, Thoracic ossification of ligamentum flavum caused by skeletal fluorosis: Eur Spine J, 2007; 16(8); 1119-28
10. Lee U, Kim CH, Kuo CC, Does preservation of ligamentum flavum in percutaneous endoscopic lumbar interlaminar discectomy improve clinical outcomes?: Neurospine, 2019; 16(1); 113-19
11. Aleksić V, Todorović J, Miladinović N, Ligamentum flavum analysis in patients with lumbar discus hernia and lumbar spinal stenosis: Sci Rep, 2023; 13(1); 3804
12. Mattar T, Costa AB, Appolonio PR, Thickness of the ligamentum flavum of the spine and its relationship with disc degeneration: Coluna/Columna, 2014; 13(2); 112-15
13. Iwahashi M, Matsuzaki H, Tokuhashi Y, Mechanism of intervertebral disc degeneration caused by nicotine in rabbits to explicate intervertebral disc disorders caused by smoking: Spine (Phila Pa 1976), 2002; 27(13); 1396-401
14. Akmal M, Kesani A, Anand B, Effect of nicotine on spinal disc cells: A cellular mechanism for disc degeneration: Spine, 2004; 29(5); 568-75
15. Chuang HC, Tsai KL, Tsai KJ, Oxidative stress mediates age-related hypertrophy of ligamentum flavum by inducing inflammation, fibrosis, and apoptosis through activating Akt and MAPK pathways: Aging (Albany NY), 2020; 12(23); 24168-83
16. Uei H, Matsuzaki H, Oda H, Gene expression changes in an early stage of intervertebral disc degeneration induced by passive cigarette smoking: Spine (Phila Pa 1976), 2006; 31(5); 510-14
17. Huang W, Qian Y, Zheng K, Is smoking a risk factor for lumbar disc herniation?: Eur Spine J, 2016; 25(1); 168-76
18. Nasto LA, Ngo K, Leme AS, Investigating the role of DNA damage in tobacco smoking-induced spine degeneration: Spine J, 2014; 14(3); 416-23
19. Wang D, Nasto LA, Roughley P, Spine degeneration in a murine model of chronic human tobacco smokers: Osteoarthritis Cartilage, 2012; 20(8); 896-905
20. Gore DR, Carrera GF, Glaeser ST, Smoking and degenerative changes of the cervical spine: a roentgenographic study: Spine J, 2006; 6(5); 557-60
21. Zhou X, Yang Y, Wu L, Brilliant Blue G inhibits inflammasome activation and reduces disruption of blood–spinal cord barrier induced by spinal cord injury in rats: Med Sci Monit, 2019; 25; 6359-66
22. Gao F, Shen J, Zhao L, Curcumin alleviates lipopolysaccharide (LPS)-activated neuroinflammation via modulation of miR-199b-5p/IκB kinase β (IKKβ)/nuclear factor kappa B (NF-κB) pathway in microglia: Med Sci Monit, 2019; 25; 9801-10
Figures
Figure 1. ROC curve analysis of IL-1β levels for evaluating diagnostic accuracy between smokers and non-smokers.Figure 2. Diagnostic accuracy of IL-6 Levels: ROC curve analysis comparing smokers and non-smokers.Figure 3. Evaluation of TNF-α as a biomarker for smoking-related inflammation: ROC analysis.Figure 4. ROC curve assessment of alpha-1 antitrypsin (AAT) for detecting smoking-induced biochemical changes in LF tissue. Tables
Table 1. Demographic and clinical characteristics of study participants, including BMI and smoking status.Table 2. Comparative analysis of demographic, clinical, and biochemical variables between smokers and non-smokers.Table 3. Diagnostic accuracy of IL-1β in differentiating smokers from non-smokers: ROC analysis results.Table 4. Diagnostic performance of IL-6 levels in distinguishing smokers from non-smokers.Table 5. ROC analysis of TNF-α as a biomarker for smoking-related inflammatory changes in LF tissue.Table 6. Diagnostic value of alpha-1 antitrypsin (AAT) levels in identifying smoking-induced LF hypertrophy.Table 1. Demographic and clinical characteristics of study participants, including BMI and smoking status.Table 2. Comparative analysis of demographic, clinical, and biochemical variables between smokers and non-smokers.Table 3. Diagnostic accuracy of IL-1β in differentiating smokers from non-smokers: ROC analysis results.Table 4. Diagnostic performance of IL-6 levels in distinguishing smokers from non-smokers.Table 5. ROC analysis of TNF-α as a biomarker for smoking-related inflammatory changes in LF tissue.Table 6. Diagnostic value of alpha-1 antitrypsin (AAT) levels in identifying smoking-induced LF hypertrophy. In Press
Clinical Research
Analysis of the Clinical Characteristics and Endoscopic Features of Phytobezoar-Induced Ulcers and Gastric ...Med Sci Monit In Press; DOI: 10.12659/MSM.952191
Clinical Research
Effect of Indirect Co-Culture With Gingival Mesenchymal Stem Cells on Cytokine Secretion in Primary Oral Sq...Med Sci Monit In Press; DOI: 10.12659/MSM.952439
Clinical Research
Comparison of Sleep Architecture in Individuals Aged 65 to 80 Years With and Without Mild Cognitive Impairm...Med Sci Monit In Press; DOI: 10.12659/MSM.952493
Clinical Research
Effects of Single-Bout Endurance Exercise Intensity on Peripheral Neurotrophic Factors in Patients With Isc...Med Sci Monit In Press; DOI: 10.12659/MSM.952089
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,514
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,760,677
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,264
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,906
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387