16 January 2023: Clinical Research
Usefulness of Detecting Brain-Derived Neurotrophic Factor in Intervertebral Disc Degeneration of the Lumbosacral Spine
Rafał StaszkiewiczABDEF, Dorian GładyszABDEF, Marcin GralewskiDEF, Kamil BryśEF, Michał GarczarekEF, Marcin GadzielińskiEF, Wiesław MarcolE, Dawid SobańskiB, Beniamin Oskar GrabarekACDEFDOI: 10.12659/MSM.938663
Med Sci Monit 2023; 29:e938663






Abstract
BACKGROUND: In determining the etiology of pain of discogenic origin, attention is paid to the role of neurotrophic factors, such as brain-derived neurotrophic factor (BDNF). Considering the potential role of BDNF in the etiology of pain during intervertebral disc degeneration (IVDD), this study aimed to assess changes in the number of BDNF-positive nerve fibers and levels of BDNF in IVDD of the lumbosacral spine in comparison to intervertebral discs (IVDs) of the control group (cadavers).
MATERIAL AND METHODS: The study group comprised 113 patients with IVDD of the lumbosacral spine. The control group consisted of 81 people (cadavers). We performed hematoxylin-eosin staining to assess IVD structures (degeneration), immunohistochemistry to determine the number of BDNF-positive nerve fibers, and an enzyme-linked immunosorbent assay and western blot to quantify BDNF levels in IVDs.
RESULTS: Levels of BDNF in the study group were significantly higher than in the control group (17.91±19.58 pg/mg; P<0.05). Furthermore, BDNF levels were significantly higher in the annulus fibrosus compared to the nucleus pulposus of the intervertebral disc (5.50±6.40 pg/mg; P<0.05). Neither the number of BDNF-positive nerves (P=0.359) nor BDNF concentration (P=0.706) were significantly correlated with the degree of perceived pain. The number of BDNF-positive fibers per 1 mm2 was not found to differ significantly according to the radiological degree of degeneration of the lumbosacral spine based on the Pfirrmann scale (P=0.735).
CONCLUSIONS: The level of BDNF expression may be indicative of IVD degeneration, although it does not predict the degree of this degeneration.
Keywords: BDNF Protein, Human, intervertebral disc degeneration, Humans, Brain-Derived Neurotrophic Factor, intervertebral disc, nucleus pulposus, Pain
Background
Intervertebral disc degeneration (IVDD) is a complex, progressive, and irreversible process in aging. Changes in disc structure contribute to the formation of radiculopathy, myelopathy, constriction of the intervertebral spaces, and disc herniation and spondylolisthesis [1]. Degeneration increases rapidly with age, especially in men, with about 10% of 50-year-olds and 60% of 70-year-olds presenting with severely degenerated discs. Spinal degeneration is known to progress rapidly during specific periods of human life. A recent study reported that the frequency of severe IVDD at any lumbar level significantly increases in people in their 20s, 30s, 50s, and 70s [2]. Progressive degeneration decreases the pH and oxygen concentration within the disc [3]. As a result of these changes, the development of intervertebral disc (IVD) calcification is observed, leading to reduction in the flow of nutrients and blood within the disc [4].
The first element of the IVD to be damaged due to the above changes is the nucleus pulposus. Due to metabolic dysregulation in IVDD, catabolism exceeds anabolism, leading to fibrosis and reduction in nucleus flexibility [5]. Fibrosis is accompanied by a change in the composition and quantity of proteoglycans, alongside a decrease in the number of cells resulting from apoptosis, causing dehydration [6]. Reducing the level of hydration causes deterioration of the ability to maintain correct pressure in the disc; as a result, it bulges and loses height [7]. Due to these progressive changes, conformational changes in elastin and collagen fibers forming the annulus fibrosus occur [8]. Old collagen fibers are denatured, and new ones are synthesized in the early degeneration process. Enzymatic activity plays a significant role in the denaturation and breakdown of collagen, fibronectin, and proteoglycans, with the most important being matrix metalloproteinases and cathepsins [9].
A 5-stage radiological classification system was created by Pfirrmann to assess the severity of IVD degeneration using magnetic resonance imaging (MRI) [10–12]. Grade 1 corresponds to IVD, which is homogeneous with bright, hyperintense white light intensity and normal height. In grade 2, the IVD is not homogeneous, but the hyperintense white signal is preserved. The nucleus pulposus (NP) and annulus fibrosus (AF) are clearly differentiated, and the IVD height is normal. At lesion grade 3, the IVD structure is heterogeneous, with intermittent gray signal intensity; the clear differentiation between AF and NP is lost at this stage, and the height of the IVD may be slightly reduced. Stage 4 presents an IVD that is heterogeneous, with hypointense dark gray signal intensity. It is not possible to distinguish between AF and NP at stage 4, and the height of the IVD is slightly to moderately reduced. Stage 5 shows degenerative changes with a heterogeneous IVD that presents with hypointense black signal intensity. Similar to stage 4, AF and NP cannot be distinguished at stage 5, and the disc space is collapsed [10–12].
At the molecular level, degeneration in IVD is expressed by the production of abnormal matrix components or by an increase in matrix degradation mediators, such as interleukin 1 (IL-1), tumor necrosis factor alpha (TNF-α), peroxide, nitric oxide, and matrix metalloproteinases (MMPs), and a reduction in the concentration of tissue inhibitors of metalloproteinases. It has been suggested that the inflammatory process and the resulting growth of nerve fibers into the fissures are the main causes of pain associated with IVDD, as mechanical pressure on a healthy disc does not cause pain compared to a disc affected by this disease [13]. In the etiology of pain of discogenic origin, attention is paid to the role of neurotrophic factors, which include classic neurotrophins, transforming growth factors, fibroblast growth factors, insulin-like growth factor, platelet-derived growth factor, neuropoietins, and a group of non-neuronal growth factors [14]. In a study of protein matrices, it was found that there is an elevated level of inflammatory factors, many of which are nociceptive, showing that degenerating and painful human IVDs release elevated levels of nerve growth factor (NGF) and brain-derived neurotrophic factor (BDNF; also known as ANON2 or BULN2), as well as ex vivo inflammatory and nociceptive factors, which induce neuronal plasticity and can actively diffuse, inducing neo-nephrosis and pain in vivo [15–18]. The BDNF protein is a neurotrophin synthesized in the cells of the central and peripheral nervous systems. It plays a role in the development and growth of neurons, memory processes, apoptosis, neurogenesis, and neuroregeneration [19]. It belongs to the family of neurotrophins (NTs), which are polypeptide growth factors [20]. Apart from BDNF, these include neurotrophin-3 (NT-3), NT-4, NT-7, and glial cell-derived neurotrophic factor, which are produced in the brain and other tissues [21].
Importantly, BDNF activity largely depends on the availability of other neurotrophic factors, such as NT-3 and NT-4/5, which, similar to BDNF, show neuroregenerative effects [15,22]. The synergistic interaction of NT-4/5 and BDNF in a cell culture of dopaminergic neurons has been demonstrated in vitro [23,24]. These factors, acting together, contribute to the survival of more than twice as many nerve cells as BDNF alone [23,24]. The same growth and neurotrophic factors can play an important role in modeling and producing pain, including discogenic pain, in the human body. For example, Maynard et al [23] confirmed the important role of neurotrophic factors in the induction and intensification of discogenic pain in the final, most advanced stage of IVDD.
Expression of BDNF messenger RNA (mRNA) in the peripheral nervous system increases at the time of damage, both in motor neurons and in Schwann cells located in the distal part of the stump of the severed nerve, but it only persists for the first few days after the damaging factor ceases [25]. BDNF also contributes to the increased migration of macrophages and mast cells into inflamed IVD, promoting repair processes in the damaged annulus fibrosus [26]. An experimental study showed that damage to peripheral nerves induces BDNF expression at the site of the damage, which promotes the regeneration of damaged neurons [27]. BDNF is produced in an inactive form called pro-BDNF, which undergoes enzymatic conversion by plasmin and the metalloproteinases MMP-2 and MMP-9 into a mature BDNF (mBDNF) protein [28]. Considering the potential role of BDNF in the etiology of pain during IVDD, this study aimed to assess changes in the number of BDNF-positive nerve fibers and levels of BDNF in the IVDD of the lumbosacral spine in comparison to IVDs of the control group.
Material and Methods
ETHICS:
This study was performed according to the 2013 Declaration of Helsinki guidelines on human experimentation. Data confidentiality and patient anonymity were maintained at all times. Patient-identifying information was deleted before the database was analyzed. Identifying patients individually in this article or in the database is impossible. Informed consent was obtained from all patients. Approval from the Bioethical Committee operating at the Regional Medical Chamber in Cracow (no. 162/KBL/OIL/2021) was obtained for this study. The issue of obtaining postmortem material for research is regulated by the Act of July 1, 2005, on the collection, storage, and transplantation of cells, tissues and organs (Journal of Laws of 2020, Item 2134). Article 5 of this Act is based on the construct of opting out, which means that, as a rule, it is permitted to collect tissues, cells, or organs from a human corpse unless the person from whom the tissues, cells, or organs are to be removed objected in this regard during their lifetime.
Article 5 of the Act of July 1, 2005, on the collection, storage and transplantation of cells, tissues and organs (Journal of Laws of 2020, Item 2134) states:
Information was obtained from the deceased’s family regarding the type of work performed, physical activity, and use of nonsteroidal anti-inflammatory drugs.
CHARACTERISTICS OF THE STUDY GROUP:
The study group included 113 patients (55 women, 48.68%; 58 men, 51.32%) diagnosed by a specialist surgeon as having symptomatic lumbosacral discopathy, which is an indication for surgical treatment. The ages of those included in the study ranged from 20 to 85 years, with a mean of 45.5±1.5 years. Body mass index (BMI) was determined for all patients. BMI in the range of 18.5–24.9 kg/m2 (normal) was found in 54 patients (37 women and 17 men), BMI in the range of 25.0–29.9 kg/m2 (overweight) in 42 patients (17 women and 15 men), and BMI of over 30 kg/m2 (obesity) in 17 patients (1 woman and 16 men).
Before admission to the Department of Neurosurgery, all patients who qualified for the study group were referred by a specialist doctor to the Neurosurgical Outpatient Clinic of the 5th Military Clinical Hospital with a polyclinic in Cracow. Surgical procedures were performed in this hospital and in the Voivodeship Hospital in Chrzanów in 2014–2020. Patients were allowed to choose which facility location and department they attended according to the principles of financing health services from public funds in Poland. Patients were recruited to this group according to the inclusion and exclusion criteria presented in Table 1.
NEUROLOGICAL EXAMINATION:
All patients in the study group underwent a complete neurological examination immediately before the procedure, which was supplemented with MRI (Signa Hde 1.5T General Electric Medical System Ltd., Warszawa, Poland) of the lumbosacral spine. The neurological examination consisted of an assessment of muscle strength, passive movements, muscle tension of the lower extremities, and reflexes (patellar, ankle, plantar, Babinski sign, and Rossolimo sign). Superficial and deep sensation (Lasègue test, Fajersztajn-Krzemicki sign, and Mackiewicz sign), gait and positioning, mobility, and pain of the lumbosacral spine were also assessed.
ANALYSIS OF THE DEGREE OF IVD DEGENERATION BY MRI:
MRI of the lumbosacral of the spine examination was performed in the SE T1, SE T1 fluid-attenuated inversion recovery, FSE T2, and short tau inversion recovery sequences in transverse and sagittal sections using 3-mm- and 4-mm-thick layers. For this purpose, 2 specialists in the field of neurosurgery (R.S. and D.G.) independently assessed the IVD using the Pfirrmann scale.
ASSESSMENT OF PAIN LEVEL: Pain intensity was assessed in all patients in the study group prior to surgery using the visual analogue scale (VAS) in the form of a ruler, on which the examined person indicated the degree of pain as a range from 0 (no pain) to 10 points (significant intense pain). The numerical value indicated by the patient on the VAS line was recorded in the database. The study was conducted in the morning at the same time of day under the same ambient conditions. Figure 1 shows the number of patients at each stage of radiological change in the section lumbosacral of the spine and each patient’s declared pain level.
CHARACTERISTICS OF THE CONTROL GROUP:
The control group contained 81 people (43 women, 53% and 38 men, 47%), with a mean age of 31.5±1.5 years. IVD samples were obtained from human cadavers during organ harvesting within 48 h from the confirmed moment of death.
BMI in the range of 18.5–24.9 (normal) was found in 23 participants (16 women and 17 men), 25.0–29.9 (overweight) in 40 patients (24 women and 16 men), and over 30 (obesity) in 18 participants (3 women and 15 men). Table 2 shows the inclusion and exclusion criteria for the control group.
IVD COLLECTION FROM THE STUDY GROUP AND CADAVERS (CONTROL):
IVD samples from the study group were collected during the microdiscectomy. The IVDs were collected using the
The first stage of the surgical procedure was to make an incision in the skin within the segment of the lumbosacral of the spine and to dissect the muscles adjacent to the spine. This allowed the researcher to reach the right segment of the spine and the spinal canal, known as bone access. Subsequently, the IVD sequester that had fallen into the spinal canal was removed, followed by the discectomy procedure (removal of the IVD). Blood that accumulated at the surgery site was drained during the postoperative procedure. The drainage was removed within 24 h of the operation.
A postmortem examination was performed for the control group after confirming donor qualification. The front surface of the lumbosacral spine section was exposed in a manner typical of a postmortem examination. Then, the appropriate IVD of the lumbosacral spine was removed using a flat sectional knife. The IVD was placed in a disposable zipper bag and labeled with the date of collection, section number, and initials of the donor’s name.
Due to the excellent quality of the preparations in the control group, 2 areas were distinguished for further study: the nucleus pulposus and the annulus fibrosus. IVDs were removed from the L1/L2 segment in 12 cases (14.81%), from the L2/L3 segment in 16 cases (19.75%), from the L3/L4 segment in 18 cases (22.22%), from the L4/L5 segment in 27 cases (33.33%), and from the L5/S1 segment in 8 cases (9.89%).
MOLECULAR ANALYSIS:
The IVDs collected from both groups for ELISA and western blot analysis were preserved in RNAlater (Thermo Fisher Scientific, Waltham, MA, USA; catalog number AM7020) and stored at −80°C until the start of BDNF expression assays. For immunofluorescence staining, the IVDs were protected using CRYOMATRIX medium (Thermo Fisher Scientific, Waltham, MA, USA; catalog number 6769006).
HISTOPATHOLOGICAL EVALUATION OF IVDS FROM THE STUDY AND CONTROL GROUPS:
All IVD samples obtained both at the time of microdiscectomy and from the deceased were evaluated histologically using hematoxylin-eosin (H&E) staining on paraffin sections 5 μm thick. For this purpose, we used an H&E staining kit (Abcam, Cambridge, MA, USA, catalog number ab245880), which included a bluing reagent, eosin Y solution, and hematoxylin (modified Lillie’s Mayer’s solution). First, we deparaffinized the scrap and hydrated it in deionized water. Then, the entire scrap was coated with hematoxylin (modified Lillie’s Mayer’s solution) and incubated with the reagent for 3–5 min. Then, excess dye was removed by washing the slide in distilled water. Next, we coated the slice with bluing reagent and incubated it with the reagent for 10–15 s. Subsequently, the slide was rinsed twice with distilled water. Further, the slide was immersed in absolute alcohol (96% ethanol; POL-AURA, Dywity, Poland; catalog number 13964800), and then the slide was covered with eosin Y reagent for 2–3 min. The slide was then rinsed with absolute alcohol and dehydrated with increasing concentrations of ethanol. Evaluation of each slide was always carried out by 2 independent investigators.
PREPARING IVDS FOR IMMUNOFLUORESCENT STAINING:
In the first stage, the IVDs were dehydrated for 24 h at 4°C using a 15% and 30% sucrose gradient. After dehydration, the IVD was frozen and embedded in a CRYOMATRIX medium (Thermo Fisher Scientific, Waltham, MA, USA; catalog number 6769006). The obtained blocks were cut on a frosting microtome (Leica Biosystems RM2235, Sydney, Australia) into sections 8- to 10-μm thick, then placed on a glass slide (Polysine® Menzel-Glaser, Thermo Fisher Scientific, Waltham, MA, USA) and stored at −20°C.
ANTIBODIES:
For immunofluorescent staining, we used a primary rabbit anti-BDNF antibody (Novus Biologicals, Centennial, CO, USA; catalog number NB100-98682; dilution 1: 200).
IMMUNOFLUORESCENT STAINING OF BDNF-POSITIVE NERVE FIBERS IN IVDS:
After thawing, the IVD preparations were rinsed for about 10 min in Tris buffer saline supplemented with 0.1% Tween 20 (TBST; Avantor International Ltd., Gdansk, Poland; catalog number J77500.K8), and then unspecific binding sites were blocked by incubation of samples in blocking solution (10% goat serum in TBST) for 30 min at room temperature (Thermo Fisher Scientific, Waltham, MA, USA; catalog number 50197Z). The preparations were then incubated for approximately 24 h in a refrigerator at 4°C with a primary rabbit anti-BDNF antibody solution (Novus Biologicals, Centennial, CO, USA; dilution 1: 200 in TBST). Following incubation, the samples were washed 3 times in a chilled PBS solution to remove an excess of unbound primary antibodies from the preparation.
In the third stage, the samples were treated with an anti-rabbit secondary antibody tagged with fluorescence AlexaFluor 568 dye (Thermo Fisher Scientific, Waltham, MA, USA; dilution of 1: 500) for 2 h at room temperature in a dark chamber. Excess of unbound secondary antibodies was washed away from the preparation with PBS (10 min at room temperature). The resulting preparations were washed 3 times for approximately 5 min with chilled PBS and then sealed in a Vectashield antifade mounting medium (Vector Laboratories, Newark, CA, USA; catalog number H-1000). The processed preparations were stored at 4°C in the dark. A sample that did not contain the primary rabbit anti-BDNF antibody served as a negative control in the assay. This indicator ensured that no unspecific or autofluorescence signals were present. A human HeLa cervical carcinoma cell line was used as a positive control.
QUANTITATIVE ASSESSMENT OF BDNF-POSITIVE NERVE FIBERS FROM THE OBTAINED MICROSCOPIC IMAGES:
The processed specimens were analyzed under fluorescence and confocal microscopy (Olympus, Tokyo, Japan). In the first step of the analysis, the sections containing the highest number of nerve fibers and/or immune-positive cells were identified and archived with a camera that captured digital images of the field of view. The labeled fibers or cells were counted at the point of their highest concentration in the next 2 to 4 sections, for a total of 10–20 fields of view (5 fields of view per section - center +4 circumferential, separated by 90°). Only cells with a clearly defined nucleus were counted to avoid double counting. The area of 1 field of view covered 0.0449 mm2. The final results were expressed as the arithmetic means per 1 mm2 of the surface area.
PREPARING THE IVDS FOR ELISA ASSAY:
Using a scalpel, IVD samples were cut into pieces approximately 1 mm in size, placed in a new test tube, and weighed. The weight of the sample was determined by subtracting the weight of the test tube from the weight of the sample in the test tube. The samples were incubated with a solution of 4M guanidine hydrochloride (Sigma Aldrich St. Louis, MO, USA, catalog number G3272), 1M sodium acetate (Sigma Aldrich St. Louis, MO, USA, catalog number S2889-250G), Triton 2% (Sigma Aldrich St. Louis, MO, USA, catalog number X100), and protease inhibitor cocktail (Sigma Aldrich St. Louis, MO, USA, catalog number P8340) for 12 h at 4°C on a laboratory cradle. The samples were then centrifuged (3000 rpm, 10 min) to obtain the supernatant, which was stored at −20°C.
ANTIBODIES: ELISA used a combination of 2 monoclonal antibodies (mAb BDNF-#1 and mAb BDNF-#9; Developmental Studies Hybridoma Bank, Iowa City, IA, USA) [29]. BDNF-#1 was conjugated with biotin using sulfo-NHS-LC-Biotin (Thermo Fisher Scientific, Waltham, MA, USA, catalog number 21435), whereas BDNF-#9 was conjugated with horseradish peroxidase (HRP) using a peroxidase labeling kit (Roche, Merck, Sigma Aldrich St. Louis, MO, USA, catalog number 11829696001) according to the manufacturer’s protocol.
ELISA ASSAY PROCEDURE:
In the first step of ELISA, 200 μl of 14 μg/ml biotin-conjugated BDNF-#1, which was diluted in phosphate buffered saline pH 7.6 (Merck, Sigma Aldrich St. Louis, MO, USA, catalog number P3744), was added to Pierce NeutrAvidin plates (Thermo Fisher Scientific, Waltham, MA, USA; catalog number 15509), and the samples were incubated for 2 h at room temperature. The plates were then washed 3 times with blocking buffer (1% bovine serum albumin (BS); Sigma Aldrich St. Louis, MO, USA, catalog number A2153) in PBS, followed by the addition of 150 μl of PBS.
In the next step, 50 μl of standards or diluted samples (1: 20) were added to the plate, and the whole sample was incubated for 3 h at room temperature on a rotary shaker. The samples were then washed 3 times with PBS, and then 200 μl of 1.25 μg/ml of HRP-conjugated mAb-#9 diluted in blocking buffer was added, and the samples were further incubated for 3 h on a rotary shaker. The plate was washed 3 times with phosphate buffer, and 100 μl of BM Chemiluminescence ELISA Substrate (buffered solution that contains luminol/4-iodophenol and buffered solution that contains a stabilized form of H2O2) (Roche, Merck, Sigma Aldrich St. Louis, MO, USA, catalog number 11582950001) was added. An M200PRO plate reader (Tecan, Männedorf, Switzerland) was used to evaluate absorbance at 540 nm. The standard was set using recombinant BDNF (Regeneron/Amgen) diluted in blocking buffer. A sample that did not contain the primary anti-BDNF antibody served as a negative control in the assay. This indicator ensured that no unspecific or autofluorescence signals were present. A human HeLa cervical carcinoma cell line was used as a positive control. All samples were analyzed in duplicate. Mean values were used for the analysis.
PREPARING THE IVDS FOR WESTERN BLOTTING:
The IVD samples stored in RNAlater solution were rinsed briefly with PBS and placed in a 2.0 ml tube. Then, 500 μl of radioimmunoprecipitation assay buffer (RIPA; Sigma Aldrich St. Louis, MO, USA, catalog number R0278) supplemented with protease and phosphatase inhibitor cocktail (Sigma Aldrich St. Louis, MO, USA, catalog number PP1010) was added. Samples were homogenized using a hand-held rotor/stator homogenizer (T18 Digital Ultra-Turrax, IKA Poland Ltd., Warsaw, Poland) until no solid fragments were visible. Thereafter, the tubes were placed on ice and mixed gently on a rocking plate for 1 h. Samples were centrifuged for 10 min (12000×g, +4°C) and supernatants were collected and stored at −80°C until further analyzed. After thawing, the total protein concentration was estimated in the preparations using the bicinchoninic acid assay KIT (BCA; Thermo Fisher, Waltham, MA, USA; catalog number 23225) according to the product’s guidelines. The protein concentrations ranged between 20 and 100 μg of total protein. All protein concentration measurements were calculated using a standard curve based on bovine serum albumin (BSA) standard solutions (involving a set of 6 standard points – 0, 250, 500, 1000, 1500, and 2000 μg/mL) (Sigma Aldrich St. Louis, MO, USA, catalog number A9576).
ANTIBODIES:
A western blot technique was used to evaluate the precursor BDNF (pro-BDNF) protein level in the IVD samples derived from the experimental and control groups. We used a primary mouse monoclonal IgG1 κ pro-BDNF antibody (Santa Cruz Biotech, Dallas, TX, USA; molecular weight 32 kDa; catalog number sc-65514; 1: 1000 dilution). HRP-conjugated goat anti-rabbit IgG (BioRad, Milan, Italy; catalog number 1706515; dilution 1: 3000) was used as the secondary antibody. As an endogenous control protein, glyceraldehyde 3-phosphate dehydrogenase (GAPDH; Santa Cruz Biotech, Dallas, Texas, USA; molecular weight 37 kDa; catalog number sc-25778; 1: 500 dilution) was used.
WESTERN BLOTTING PROCEDURE:
Equal amounts of protein (20 μg) were separated by sodium dodecyl sulfate polyacrylamide gel electrophoresis (POL-AURA, Dywity, Poland; catalog number PA-03-2962-D#25G). After electrophoresis, the proteins were transferred onto a polyvinylidene difluoride membrane (PVDF, 0.45 μm pore size, Thermo Fisher, Waltham, MA, USA; catalog number 88518).
The membrane was blocked using 1X Tris-buffered saline (TBS) containing 0.1% Tween-20 (Sigma Aldrich St. Louis, MO, USA, catalog number 91414) supplemented with 5% nonfat dry milk powder (Merck, Sigma Aldrich St. Louis, MO, USA, catalog number NIST1549A). Blocking was carried out at 4°C on a laboratory cradle overnight. Next, we added a primary mouse monoclonal IgG1 κ pro-BDNF antibody anti-BDNF antibody (Santa Cruz Biotech, Dallas, TX, USA; molecular weight 32 kDa; catalog number sc-65514) and incubated the whole thing overnight at 4°C with gentle shaking. The next day, after washing the membrane, incubation was performed with a secondary antibody, horseradish-peroxidase-conjugated goat anti-rabbit IgG (BioRad, Milan, Italy; catalog number 1706515; dilution 1: 3000). The optical density of each lane of the blot was measured using Kodak MI 4.5SE software (Kodak, Rochester, NY, USA). IVD samples to which a primary mouse monoclonal IgG1 κ pro-BDNF antibody anti-BDNF antibody was not added were used as a negative control. A human HeLa cervical carcinoma cell line was used as a positive control.
STATISTICAL ANALYSIS:
The statistical analysis was performed using the Statistica 13 PL program (StatSoft, Cracow, Poland) at a statistical significance threshold of
Results
RESULTS OF THE H&E STAINING:
H&E staining of IVDs obtained from the control group was carried out to assess whether features of IVD degeneration were present in the present samples, which allowed them to be classified as controls. On the other hand, degenerated IVDs show changes in the AP and NF structures and features of reduced IVD height (Figure 2).
DIFFERENCES IN THE NUMBER OF BDNF-POSITIVE NERVE FIBERS AND BDNF CONCENTRATIONS BETWEEN THE STUDY AND CONTROL GROUPS:
Based on the analysis, no statistically significant differences were found between the number of BDNF-positive fibers in the study and control groups. On the other hand, the concentration of BDNF was significantly higher in the test group compared to the control group (P=0.010; Table 3).
NUMBER OF BDNF-POSITIVE NERVES IN IVDD AND THEIR CONCENTRATION DEPENDING ON PAIN LEVEL: We did not find that the number of BDNF-positive nerves differed significantly according to the degree of perceived pain (P=0.359; one-way ANOVA test). The lowest number of nerve fibers was found in the group of patients reporting a perceived pain level of 6, and the highest at a level of 10. Similarly, the concentration of BDNF in the IVD was not shown to be correlated with the severity of pain in the study group (P=0.706; one-way ANOVA). The highest concentration of BDNF was found at level 4 pain intensity, and the lowest was found for patients who rated pain intensity at levels 2 or 3. The detailed results of the number of BDNF-positive fibers and their concentrations, based on pain intensity, are presented in Table 4.
ANALYSIS OF THE NUMBER OF BDNF-POSITIVE NERVES AND BDNF CONCENTRATIONS IN IVDD, DEPENDING ON THE VALUE OF THE PFIRRMANN SCALE: The number of BDNF-positive fibers per 1 mm2 and their concentration were not found to differ significantly according to the Pfirrmann scale (P=0.735 and 0.989, respectively; ANOVA variance analysis). The lowest BDNF concentration was recorded for the fifth degree of radiological advancement, whereas the highest was noted for the third degree of radiological degeneration (P=0.989). Detailed results on the number of BDNF-positive fibers and their concentration depending on the radiological degree of change are presented in Table 5.
EVALUATION OF THE CONCENTRATION OF BDNF IN THE NUCLEUS PULPOSUS AND THE ANNULUS FIBROSUS IN HUMAN CADAVER IVD: Due to the excellent quality of the IVD samples obtained from the control group, it was possible to compare the concentrations of BDNF in the nucleus pulposus and the annulus fibrosus. A significantly higher concentration of BDNF was found in the annulus fibrosus compared to the nucleus pulposus (P<0.001; Student’s t-test; Table 6).
THE RESULTS OF THE WESTERN BLOT ANALYSIS: Based on the obtained electropherograms, we confirmed the specificity of the antibodies used, as the molecular weight of the tagged proteins (GAPDH and pro-BDNF) matched the molecular weight specified by the antibody manufacturers (37 kDa and 32 kDa, respectively), and the presence of only 1 band for each protein was confirmed. In addition, the expression of GAPDH was constant in all samples tested; thus, this protein met the assumptions of endogenous control (overlay control). Pro-BDNF expression was noted in the control IVD- and in AP and NP. However, in degenerated IVDs, the highest expression of pro-BDNF was found when degenerative changes were advanced to levels 2 and 3 according to the Pfirrmann scale (Figure 3).
Discussion
Our analysis showed no statistically significant differences in the number of BDNF-positive nerve fibers in the degenerated IVDs compared to the IVDs collected from the control group. There were also no statistically significant differences between the number of BDNF-positive nerve fibers, the degree of radiological advancement of degenerative changes, or the severity of pain. The results indicate an increasing trend in both the number of nerve fibers and the concentration of BDNF with the progression of the degeneration process in IVDD, but only to a certain stage, at which it seems that the intercellular matrix still allows biochemical processes to take place. Therefore, the highest concentration of BDNF was recorded in the intermediate stages of radiological degeneration of the lumbosacral spine but not in the most advanced fifth stage.
Wilhelm et al confirmed the importance of BDNF in promoting the growth of peripheral nerves [30]. They showed that the administration of exogenous BDNF to the site of peripheral nerve damage in mice increased axon regeneration compared to mice that did not receive BDNF. Further, the inhibition of BDNF expression in the distal stump of the severed nerve did not affect the number of regenerating axons in its proximal segment [30]. By contrast, experimental studies in a rat model have shown that the administration of an anti-BDNF antibody to the site of nerve damage inhibits the proliferation of connective tissue and collagen fibers at the damaged area but does not suppress regeneration of damaged axons, which results in the inhibition of neuroblastoma formation [29,30]. The possibility of regeneration of peripheral nerves highlights the potential use of BDNF in supporting the treatment of peripheral nervous system damage. An experimental study confirmed that the use of combined therapy consisting of the simultaneous administration of 2 neurotrophic factors – BDNF and ciliary neurotrophic factor (CNTF) – led to increased efficiency in restoring the function of the damaged sciatic nerve in an experimental rat model compared to the use of either neurotrophin alone [31].
Depending on the location and extent of the damage to the nervous system, BDNF plays a different role. It supports neuronal growth, survival, and neurogenesis; can initiate compensatory processes that mitigate the harmful effects of injury, disease, or stress; and is involved in several trauma-induced maladaptive processes, including inflammatory or neuropathic pain [32]. In an experiment conducted on mice, Orita et al [33] showed that a BDNF-neutralizing antibody administered to damaged IVD using repeated injections significantly reduced the number of calcitonin gene-related peptide (CGRP)-positive neurons in the dorsal ganglia. Their results indicated a possible cause-and-effect relationship between the locally increased production of BDNF and the pathophysiology of discogenic pain. Henry et al [34] also emphasized the significant role of BDNF in the initiation and development of spine pain, linking the increase in BDNF concentration in the degenerating human disc with a preceding increase in the concentration of some pro-inflammatory cytokines, such as IL-1β and vascular endothelial growth factor (VEGF).
Khan et al [35] discussed the importance of searching for new biochemical markers to verify the severity of pain in the lumbar region, emphasizing the potential role of BDNF in this regard. Such analyses are important because they contribute to the development of personalized spine medicine and treatment. Kartha et al [36] conducted studies on the influence of vibration on the expression of BDNF and NGF in the IVDs of laboratory animals. They noted a several-fold increase in BDNF mRNA in discs damaged by vibration, which correlated with the severity of pain. Lee et al [37] conducted a study on a group of 25 patients with MRI-confirmed IVD of the lumbosacral spine in which they assessed the presence of BDNF. The presence of BDNF was found in 24 out of 25 degenerative human discs.
The results of our research turned out to be inconclusive. In this study, the concentration of BDNF in normal IVDs was significantly lower in women than in men. Additionally, the presence of this neurotrophic factor was not found at all in the area of the nucleus pulposus. However, the findings demonstrated the presence of a significantly higher concentration of BDNF within the annulus fibrosus than within the nucleus pulposus of healthy IVDs, which in itself is an interesting result. Fremont et al [38] examined the human IVDs of the lumbosacral spine obtained during lumbar microdiscectomy in a group of people with and without pain (as well as in a control group of discs obtained from human cadavers). They found that the penetration of free nerve endings into the deeper layers of human IVDs was demonstrated in the group of patients with pain symptoms compared to patients without pain symptoms and the control group.
One of limitations of our study is highlighted by the neuronal distribution of BDNF, which is not only limited to the cytosol where it is formed, but is also found in the vicinity of dendritic spines [16]. Further, various forms of BDNF are associated with particular stages of its production, such as precursor BDNF (pro-BDNF) or mature BDNF (mBDNF), which may not have been detectable by the antibodies we used. This limitation is further complicated by the fact that the BDNF gene contains as many as 11 exons and promoter sequences, which are switched on depending on the location and origin of individual cell types, allowing for the formation of many different transcripts. The regulation of the transcription of neurotrophic factors is, therefore, a complex and not yet fully understood process [39,40]. Further steps in the expression of the BDNF gene, such as at the mRNA polyadenylation site and modifications to the BDNF precursor protein, are also important in the formation of mature BDNF (mBDNF) protein [41,42].
Notably, the storage of IVD samples under low temperature did not affect the detection of BDNF-positive nerve fibers and assessment of BDNF levels in the samples. Indeed, appropriate cryoprotectants (Cryomatrix) and RNAlater stabilizing solution were used, which, according to the manufacturer’s recommendation, are suitable for preserving tissue material for RNA and protein analyses [43]. Positive and negative controls were appropriately included in each of the analyses to exclude false positives and false negatives. Probably also relevant is the fact that IVDs for the control group were collected postmortem. However, low temperature is a protective factor for biological material, and is routinely used in molecular biology. Zhang et al pointed out that the degenerative process within the IVD is the cause of the death of IVD-forming cells [41], thus depleting the pool of cells from which proteins can be extracted. There is also no way other than postmortem to obtain IVDs for the control group, and such a solution has already been described by other authors [42,44].
Nonetheless, the results we obtained are valuable and have clinical relevance. Indeed, we have shown that, in general, BDNF expression is higher in degenerative IVDs than in controls, but its concentration is not proportional to the severity of pain as determined by the patient’s VAS scale or the severity of degenerative changes on the Pfirrmann scale. At the same time, it should be remembered that the radiological classification of IVD degeneration on the Pfirrmann scale does not fully reflect the patient’s clinical condition. Thus, although IVD degenerative lesions were assigned a certain radiological grade, the patient’s condition and reported problems differed from those typical of the degree of degeneration. Thus, BDNF is a neurotrophic factor whose level of expression is indicative of IVD degeneration, without determining the degree of this degeneration. Perhaps increasing the number of individual subgroups would allow correlations between BDNF expression and IVD degenerative changes to be observed. Of course, further experiments are required. It would be important to determine the concentration of BDNF not only at the protein level but also at the mRNA transcriptome and micro-RNA levels. In doing so, the role of epigenetic mechanisms in the expression regulation of the gene that encodes BDNF protein could be assessed. Moreover, conducting a microarray experiment would allow for the selection of genes, signaling pathways, and cellular processes important for the degeneration of IVDs. A valuable supplement to these observations would be to study the frequency of polymorphic variants of the BDNF gene or to conduct next-generation sequencing (NGS), especially because in the case of some samples, no evidence of BDNF-positive nerve fibers or protein concentration in IVDs was found. The next step in the analysis could be to perform immunohistochemical staining to detect specific degenerated and healthy IVD proteins. It is also important to determine other neurotrophic factors and their relationships in the pathogenesis of IVDD.
Further research is required, as the available scientific reports indicate a significant role for BDNF in the etiology of discogenic spine pain. Moreover, in the next research stage, it will be essential to better understand the occurrence of discogenic pain to determine the concentration of other local factors related to the described phenomenon.
Conclusions
The analysis of the results of the presented research and our own experience allows us to conclude that the intensity of discogenic pain may be influenced by both the depth of invasion that individual nerve fibers reach in IVDD, which is subject to much greater axial compressive forces compared to healthy discs, and the phenomenon of the so-called sprouting of regenerating nerve fibers. The latter is intensified by the action of certain neurotrophic factors, which support the formation of a denser network of free nerve endings, located mainly in the peripheral areas of the human IVD. Thus, BDNF is a neurotrophic factor whose level of expression is indicative of IVD degeneration, although it does not predict the degree of this degeneration.
Figures
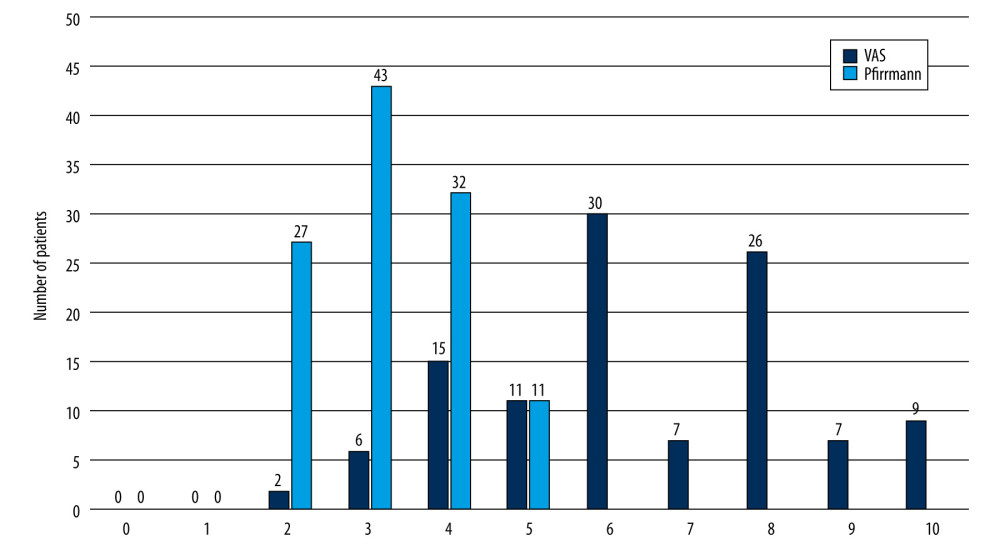 Figure 1. The number of patients declaring pain intensity in the range of 2–10 (according to the VAS) and whose radiological advancement of degenerative changes in the IVD was in the range of 2–5 (according to the Pfirrmann scale).
Figure 1. The number of patients declaring pain intensity in the range of 2–10 (according to the VAS) and whose radiological advancement of degenerative changes in the IVD was in the range of 2–5 (according to the Pfirrmann scale). ![Results of H&E staining of intervertebral disc in control group and experimental group (×50) [own picture]. (A) Healthy intervertebral disc; (B) degeneration intervertebral disc.](https://jours.isi-science.com/imageXml.php?i=medscimonit-29-e938663-g002.jpg&idArt=938663&w=1000) Figure 2. Results of H&E staining of intervertebral disc in control group and experimental group (×50) [own picture]. (A) Healthy intervertebral disc; (B) degeneration intervertebral disc.
Figure 2. Results of H&E staining of intervertebral disc in control group and experimental group (×50) [own picture]. (A) Healthy intervertebral disc; (B) degeneration intervertebral disc. 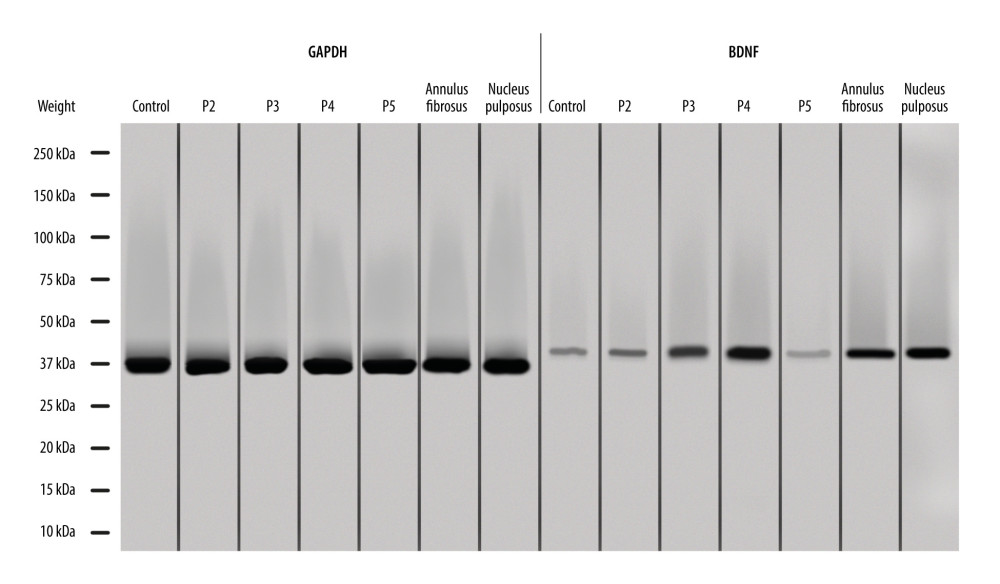 Figure 3. Expression of pro-BDNF in IVD obtained from the study and control groups, and annulus fibrosus, and nucleus pulposus from the control group obtained via the western blot technique. P – stage of radiological advancement of changes according to the Pfirrmann scale.
Figure 3. Expression of pro-BDNF in IVD obtained from the study and control groups, and annulus fibrosus, and nucleus pulposus from the control group obtained via the western blot technique. P – stage of radiological advancement of changes according to the Pfirrmann scale. Tables
Table 1. Inclusion and exclusion criteria for the study group.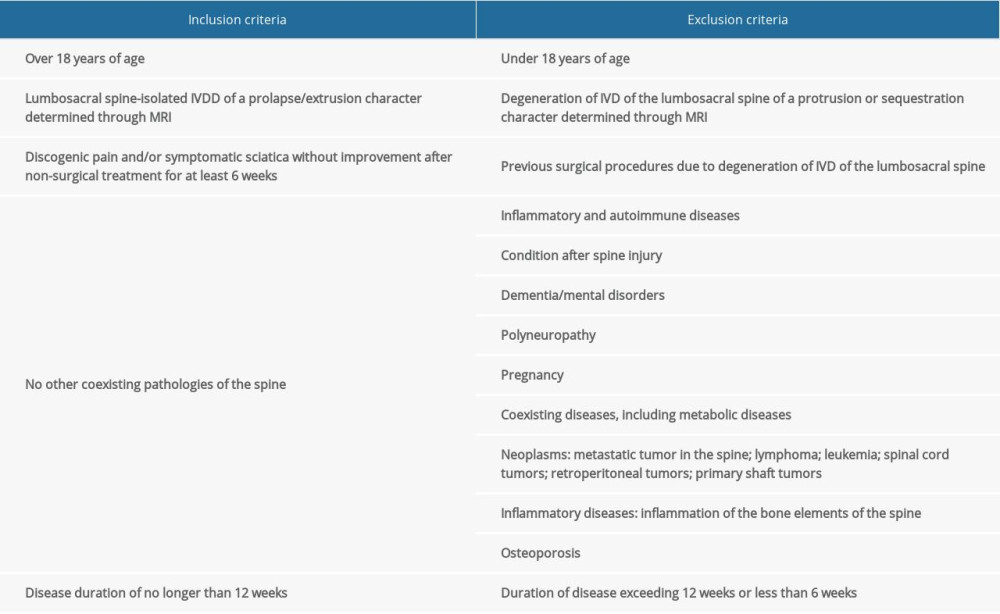 Table 2. Inclusion and exclusion criteria for the control group.
Table 2. Inclusion and exclusion criteria for the control group.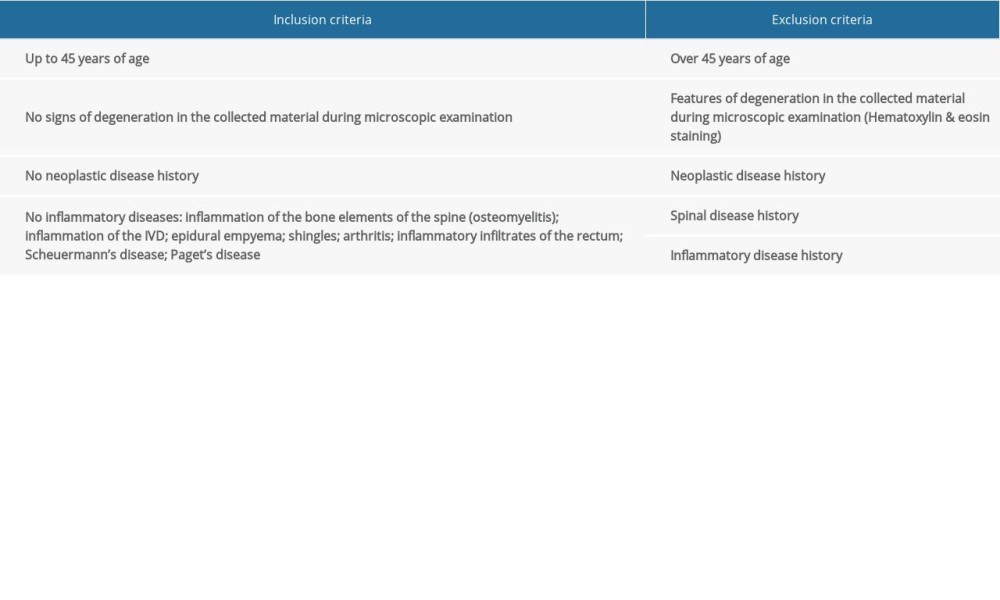 Table 3. Number of BDNF-positive fibers/1 mm2 and their concentration in the study and control group.
Table 3. Number of BDNF-positive fibers/1 mm2 and their concentration in the study and control group.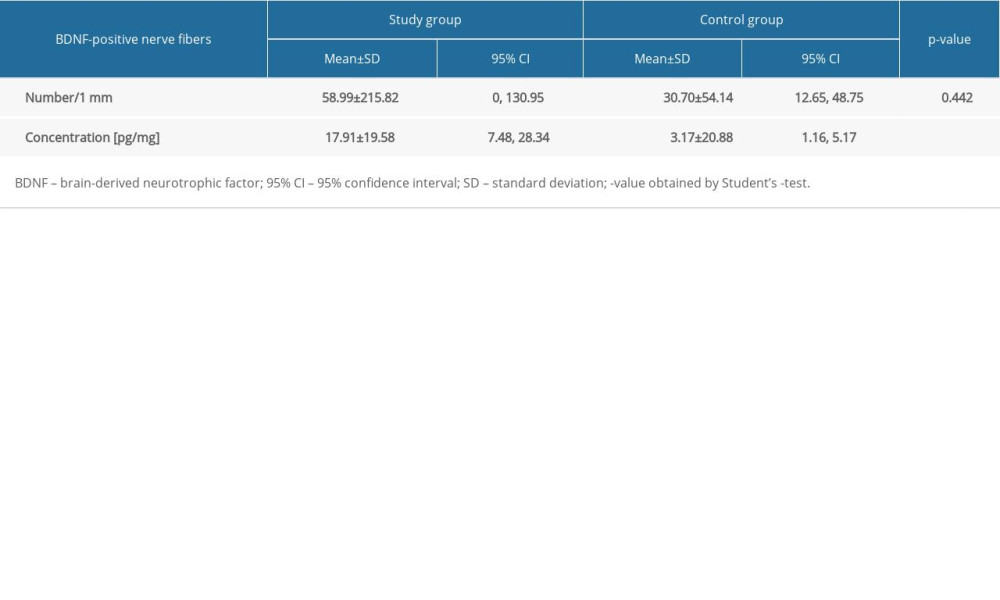 Table 4. Number of BDNF-positive fibers/1 mm2 and their concentration according to pain intensity.
Table 4. Number of BDNF-positive fibers/1 mm2 and their concentration according to pain intensity.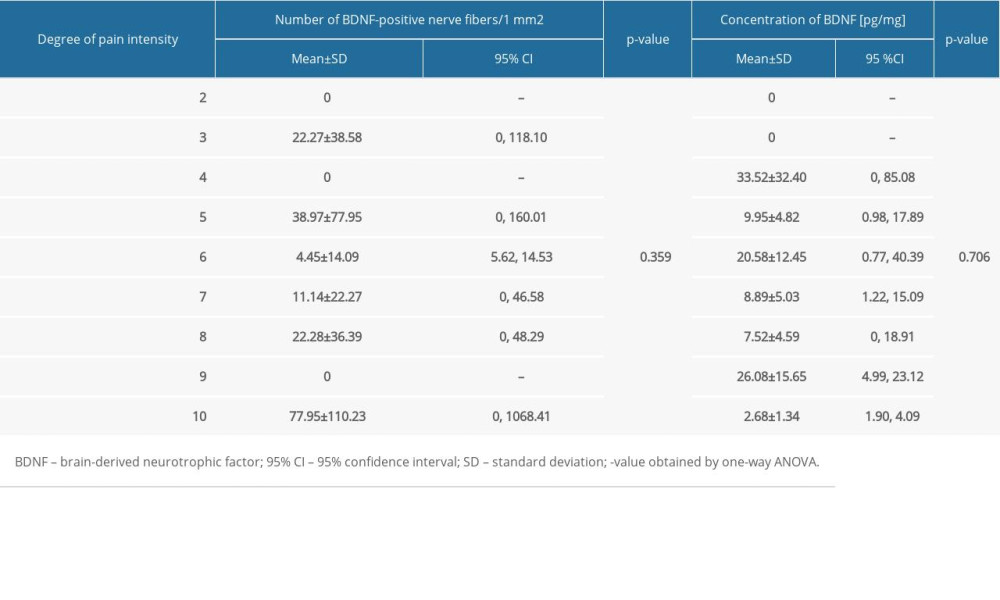 Table 5. Number of BDNF-positive fibers/1 mm2 and their concentrations according to the Pfirrmann scale obtained by immunofluorescence staining.
Table 5. Number of BDNF-positive fibers/1 mm2 and their concentrations according to the Pfirrmann scale obtained by immunofluorescence staining.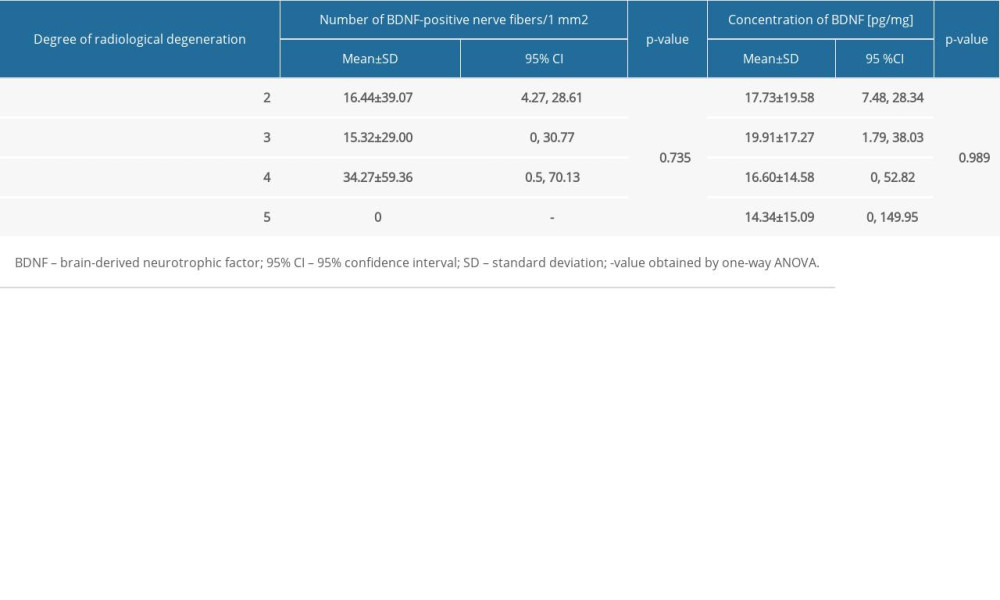 Table 6. Changes in the concentration of BDNF in annulus fibrosus and nucleus pulposus in the control group.
Table 6. Changes in the concentration of BDNF in annulus fibrosus and nucleus pulposus in the control group.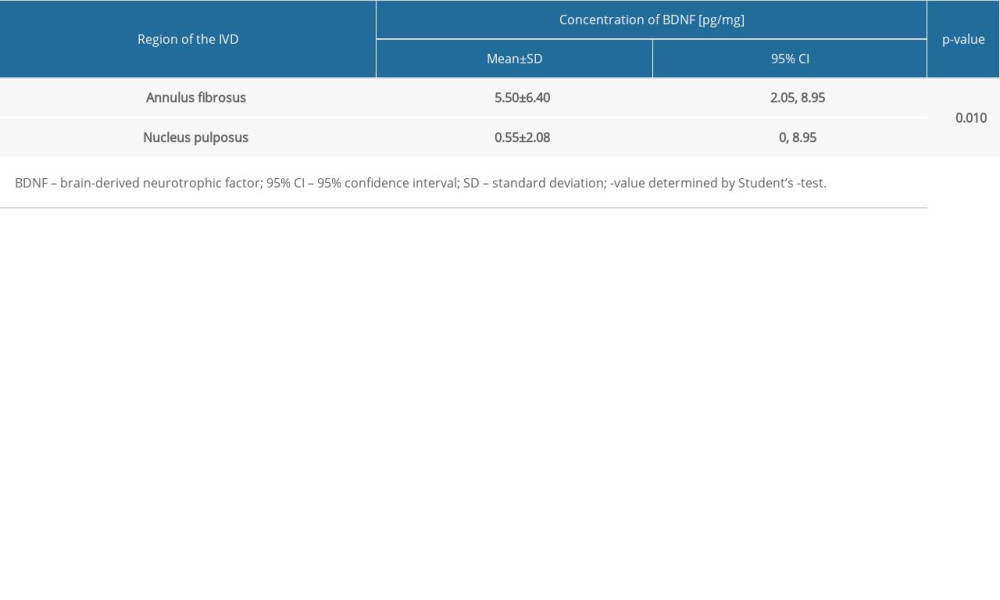
References
1. Francisco V, Pino J, González-Gay MÁ, A new immunometabolic perspective of intervertebral disc degeneration: Nat Rev Rheumatol, 2022; 18(1); 47-60
2. Ekşi MŞ, Orhun Ö, Yaşar AH, At what speed does spinal degeneration gear up?: Aging Paradigm in patients with low back pain: Clin Neurol Neurosurg, 2022; 215; 107187
3. Ashinsky B, Smith HE, Mauck RL, Gullbrand SE, Intervertebral disc degeneration and regeneration: A motion segment perspective: Eur Cell Mater, 2021; 41; 370-80
4. Su Q, Li Y, Feng X, Association and histological characteristics of endplate injury and intervertebral disc degeneration in a rat model: Injury, 2021; 52(8); 2084-94
5. Radcliff K, Zigler J, Braxton E, Final long-term reporting from a randomized controlled IDE trial for lumbar artificial discs in single-level degenerative disc disease: 7-year results: Int J Spine Surg, 2021; 15(4); 612-32
6. Gübitz R, Lange T, Gosheger G, Influence of age, BMI, gender and lumbar level on T1ρ magnetic resonance imaging of lumbar discs in healthy asymptomatic adults: RöFo-Fortschritte Auf Dem Gebiet Der Röntgenstrahlen Und Der Bildgebenden Verfahren, 2018; 190; 144-51, copyright Georg Thieme Verlag KG
7. Patil S, Al Kahtani A, Baeshen H, Face validity and psychometric evaluation of the available oral health-related quality of life instruments: A systematic review: Oral Health Prev Dent, 2020; 18(1); 409-16
8. Cyril D, Giugni A, Bangar SS, Elastic fibers in the intervertebral disc: From form to function and toward regeneration: Int J Mol Sci, 2022; 23(16); 8931
9. Brown S, Rodrigues S, Sharp C, Staying connected: Structural integration at the intervertebral disc-vertebra interface of human lumbar spines: Eur Spine J, 2017; 26(1); 248-58
10. Pfirrmann CW, Metzdorf A, Zanetti M, Magnetic resonance classification of lumbar intervertebral disc degeneration: Spine (Phila Pa 1976), 2001; 26(17); 1873-78
11. Yu LP, Qian WW, Yin GY, MRI assessment of lumbar intervertebral disc degeneration with lumbar degenerative disease using the Pfirrmann grading systems: PLoS One, 2012; 7(12); e48074
12. Hasanović-Vučković S, Jusufbegović M, Vegar-Zubović S, Assessment of lumbar spine disc degeneration in coherence to Pfirrman grades and oswestry disability index: J Health Sci, 2020; 10(3); 191-95
13. Lyu FJ, Cui H, Pan H, Painful intervertebral disc degeneration and inflammation: from laboratory evidence to clinical interventions: Bone Res, 2021; 9(1); 1-14
14. Morel L, Domingues O, Zimmer J, Michel T, Revisiting the role of neurotrophic factors in inflammation: Cells, 2020; 9(4); 865
15. de León A, Gibon J, Barker PA, NGF-dependent and BDNF-dependent DRG sensory neurons deploy distinct degenerative signaling mechanisms: eNeuro, 2021; 8(1) ENEURO.0277-20.202
16. Colucci-D’Amato L, Speranza L, Volpicelli F, Neurotrophic factor BDNF, physiological functions and therapeutic potential in depression, neurodegeneration and brain cancer: Int J Mol Sci, 2020; 21(20); 7777
17. Kalliolias GD, Ivashkiv LB, TNF biology, pathogenic mechanisms and emerging therapeutic strategies: Nat Rev Rheumatol, 2016; 12(1); 49-62
18. Staszkiewicz R, Bolechala F, Wieczorek J, Changes in essential and trace elements content in degenerating human intervertebral discs do not correspond to patients’ clinical status: Česká a Slovenská Neurologie a Neurochirurgie, 2019; 82/115(2); 203-8
19. Małczyńska P, Piotrowicz Z, Drabarek D, Rola mózgowego czynnika neurotroficznego (BDNF) w procesach neurodegeneracji oraz w mechanizmach neuroregeneracji wywołanej wzmożoną aktywnością fizyczną: Postępy Biochemii, 2019; 65(1); 2-8 [in Polish]
20. García-Suárez PC, Rentería I, Plaisance EP, The effects of interval training on peripheral brain derived neurotrophic factor (BDNF) in young adults: A systematic review and meta-analysis: Sci Rep, 2021; 11(1); 1-14
21. Messina OD, Vidal Wilman M, Vidal Neira LF, Nutrition, osteoarthritis and cartilage metabolism: Aging Clin Exp Res, 2019; 31(6); 807-13
22. Wu SY, Pan BS, Tsai SF, BDNF reverses aging-related microglial activation: J Neuroinflammation, 2020; 17(1); 210
23. Maynard KR, Hobbs JW, Sukumar M, Bdnf mRNA splice variants differentially impact CA1 and CA3 dendrite complexity and spine morphology in the hippocampus: Brain Structure Funct, 2017; 222(7); 3295-307
24. Barker PA, Mantyh P, Arendt-Nielsen L, Nerve growth factor signaling and its contribution to pain: J Pain Res, 2020; 13; 1223
25. Li R, Li D-H, Zhang H-Y, Growth factors-based therapeutic strategies and their underlying signaling mechanisms for peripheral nerve regeneration: Acta Pharmacol Sin, 2020; 41(10); 1289-300
26. Cartelli D, Cavaletti G, Lauria G, Meregalli C, Ubiquitin proteasome system and microtubules are master regulators of central and peripheral nervous system axon degeneration: Cells, 2022; 11(8); 1358
27. Jara JS, Agger S, Hollis ER, Functional electrical stimulation and the modulation of the axon regeneration program: Front Cell Dev Biol, 2020; 8; 736
28. Fang F, Yang W, Florio JB, Synuclein impairs trafficking and signaling of BDNF in a mouse model of Parkinson’s disease: Sci Rep, 2017; 7(1); 1-13
29. Wilhelm JC, Xu M, Cucoranu D, Cooperative roles of BDNF expression in neurons and Schwann cells are modulated by exercise to facilitate nerve regeneration: J Neurosci, 2012; 32(14); 5002-9
30. Guevara YMV, Yoshikawa H, Saito I, Effect of local application of an antibody against brain-derived neurotrophic factor on neuroma formation after transection of the inferior alveolar nerve in the rat: Neuroreport, 2014; 25(13); 1069
31. Jiang YX, Dong ZY, Wang JW, Efficacy of endoscopic radiofrequency ablation for treatment of reflux hypersensitivity: A study based on Rome IV criteria: Gastroenterol Res Pract, 2022; 2022; 4145810
32. Smith PA, BDNF: No gain without pain?: Neuroscience, 2014; 283; 107-23
33. Orita S, Eguchi Y, Kamoda H, Brain-derived neurotrophic factor inhibition at the punctured intervertebral disc downregulates the production of calcitonin gene-related peptide in dorsal root ganglia in rats: Spine, 2011; 36(21); 1737-43
34. Henry N, Clouet J, Le Bideau J, Innovative strategies for intervertebral disc regenerative medicine: from cell therapies to multiscale delivery systems: Biotechnol Adv, 2018; 36(1); 281-94
35. Khan AN, Jacobsen HE, Khan J, Inflammatory biomarkers of low back pain and disc degeneration: A review: Ann NY Acad Sci, 2017; 1410(1); 68-84
36. Kartha S, Zeeman ME, Baig HA, Upregulation of BDNF & NGF in cervical intervertebral discs exposed to painful whole-body vibration: Spine, 2014; 39(19); 1542
37. Lee RS, Kayser MV, Ali SY, Calcium phosphate microcrystal deposition in the human intervertebral disc: J Anat, 2006; 208(1); 13-19
38. Freemont AJ, Watkins A, Le Maitre C, Nerve growth factor expression and innervation of the painful intervertebral disc: J Pathol, 2002; 197(3); 286-92
39. Colliva A, Tongiorgi E, Distinct role of 5′ UTR sequences in dendritic trafficking of BDNF mRNA: Additional mechanisms for the BDNF splice variants spatial code: Mol Brain, 2021; 14(1); 1-13
40. Ghafouri-Fard S, Khoshbakht T, Taheri M, Ghanbari M, A concise review on the role of BDNF-AS in human disorders: Biomed Pharmacother, 2021; 142; 112051
41. Zhang F, Zhao X, Shen H, Zhang C, Molecular mechanisms of cell death in intervertebral disc degeneration (review): Int J Mol Med, 2016; 37(6); 1439-48
42. Xiaogang M, Quanshan H, Liping Z, Kaken H, The expression of cytokine and its significance for the intervertebral disks of Kazakhs: J Clin Lab Anal, 2017; 31(5); e22087
43. Filippiadis DK, Tutton S, Mazioti A, Kelekis A, Percutaneous image-guided ablation of bone and soft tissue tumours: A review of available techniques and protective measures: Insights Imaging, 2014; 5(3); 339-46
44. Nakazawa KR, Walter BA, Laudier DM, Accumulation and localization of macrophage phenotypes with human intervertebral disc degeneration: Spine J, 2018; 18(2); 343-56
Figures
Figure 1. The number of patients declaring pain intensity in the range of 2–10 (according to the VAS) and whose radiological advancement of degenerative changes in the IVD was in the range of 2–5 (according to the Pfirrmann scale).Figure 2. Results of H&E staining of intervertebral disc in control group and experimental group (×50) [own picture]. (A) Healthy intervertebral disc; (B) degeneration intervertebral disc.Figure 3. Expression of pro-BDNF in IVD obtained from the study and control groups, and annulus fibrosus, and nucleus pulposus from the control group obtained via the western blot technique. P – stage of radiological advancement of changes according to the Pfirrmann scale. Tables
Table 1. Inclusion and exclusion criteria for the study group.Table 2. Inclusion and exclusion criteria for the control group.Table 3. Number of BDNF-positive fibers/1 mm2 and their concentration in the study and control group.Table 4. Number of BDNF-positive fibers/1 mm2 and their concentration according to pain intensity.Table 5. Number of BDNF-positive fibers/1 mm2 and their concentrations according to the Pfirrmann scale obtained by immunofluorescence staining.Table 6. Changes in the concentration of BDNF in annulus fibrosus and nucleus pulposus in the control group.Table 1. Inclusion and exclusion criteria for the study group.Table 2. Inclusion and exclusion criteria for the control group.Table 3. Number of BDNF-positive fibers/1 mm2 and their concentration in the study and control group.Table 4. Number of BDNF-positive fibers/1 mm2 and their concentration according to pain intensity.Table 5. Number of BDNF-positive fibers/1 mm2 and their concentrations according to the Pfirrmann scale obtained by immunofluorescence staining.Table 6. Changes in the concentration of BDNF in annulus fibrosus and nucleus pulposus in the control group. In Press
Clinical Research
Comparative Effectiveness of a Nurse-Led Care Model vs Usual Care in Rheumatoid Arthritis: A Longitudinal C...Med Sci Monit In Press; DOI: 10.12659/MSM.953211
Clinical Research
Impact of Treatment Modality on Pain, Sexual Function, and Psychological Well-Being in Patients With Bartho...Med Sci Monit In Press; DOI: 10.12659/MSM.952422
Clinical Research
Association Between Radiographic Knee Osteoarthritis, Pre-Fracture Mobility, and Hip Fracture Patterns in O...Med Sci Monit In Press; DOI: 10.12659/MSM.952678
Clinical Research
Association Between Total Cholesterol–to–High-Density Lipoprotein Ratio and Gestational Hypertension: A Cas...Med Sci Monit In Press; DOI: 10.12659/MSM.952395
Most Viewed Current Articles
17 Jan 2024 : Review article 14,176,084
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
13 Nov 2021 : Clinical Research 3,757,530
Acceptance of COVID-19 Vaccination and Its Associated Factors Among Cancer Patients Attending the Oncology ...DOI :10.12659/MSM.932788
Med Sci Monit 2021; 27:e932788
14 Dec 2022 : Clinical Research 2,466,116
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research 708,768
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387